SHORT COMMUNICATION
A validated GC–MS method for the determinationof D9-tetrahydrocannabinol and 11-nor-D9-tetrahydrocannabinol-9-carboxylic acid in bile samples
Ioannis Papoutsis • Panagiota Nikolaou • Artemisia Dona • Constantinos Pistos •
Maria Stefanidou • Chara Spiliopoulou • Sotirios Athanaselis
Received: 21 October 2011 / Accepted: 9 November 2011 / Published online: 3 December 2011
� Japanese Association of Forensic Toxicology and Springer 2011
Abstract We present a validated gas chromatography-
mass spectrometry method for the determination of D9-tet-
rahydrocannabinol and 11-nor-D9-tetrahydrocannabinol-9-
carboxylic acid in bile samples. The method includes protein
precipitation with acetonitrile after enzymatic hydrolysis,
and solid-phase extraction followed by silylation using
N,O-bis(trimethylsilyl)trifluoroacetamide with 1% trimeth-
ylchlorosilane. The limit of detection was 0.30 ng/ml and the
limit of quantitation was 1.00 ng/ml. The calibration curves
were linear within the dynamic range of 1.00–500 ng/ml
(R2 C 0.993) and the absolute recovery for both analytes
was higher than 87.5%. Accuracy and precision were less
than 8.8% and 8.2%, respectively. The developed method
was applied for the analysis of bile samples obtained from 21
forensic cases.
Keywords D9-Tetrahydrocannabinol � 11-Nor-D9-
tetrahydrocannabinol-9-carboxylic acid � Bile � GC–MS
Introduction
Cannabis, the most commonly used illicit drug throughout
the world [1], is often implicated in forensic cases like deaths
of drug addicts, driving under the influence of drugs, acci-
dents, and others. The increasing use of cannabis threatens
road safety because it is known to be a causative factor in
some traffic accidents [2–6]. D9-Tetrahydrocannabinol
(THC) is the main psychoactive constituent of the plant
Cannabis sativa [7, 8] and it has a complex pharmacokinetic
profile due to its high lipid solubility, protein binding and
large distribution volume [3, 9]. THC is extensively metab-
olized primarily to 11-hydroxy-D9-tetrahydrocannabinol
(THC-OH), which is further metabolized to the carbox-
ylic acid metabolite 11-nor-D9-tetrahydrocannabinol-9-car-
boxylic acid (THCCOOH) [10–13]. The concentrations of
THC and its metabolites in biological samples correlate
with recent drug use and impaired human performance or
behavior; quantification of THC in blood is absolutely nec-
essary in cases of accidents where victims or other involved
persons are affected by cannabis [2, 11, 14]. Generally,
plasma or whole blood concentrations of cannabinoids are
required for the evaluation of driving ability under the
influence of cannabis, for monitoring drug addicts under
rehabilitation, and for the investigation of forensic cases
[8, 12, 15]. In forensic cases, analysis of alternative matrices,
such as bile, may be required especially when urine or blood
samples are not available or cannabinoid blood concentra-
tion data do not provide adequate answers to questions
posed by the investigation [12]. The bile concentrations of
drugs, including cannabinoids, are generally severalfold
higher than the respective blood concentrations, so determi-
nation of cannabinoids in bile remains an important post-
mortem tool for documenting chronic cannabinoid use [16].
Many analytical methods for determining cannabinoids
in different biological matrices have been developed.
Immunoassays are generally used for screening of urine
samples for cannabis use, but the chromatographic confir-
mation of positive results is mandatory [13]. For this
purpose, gas chromatography (GC) [7, 11, 14, 15, 17–19]
or liquid chromatography (LC) [2, 4, 5, 8, 12, 13, 20–25]
methods using mainly mass spectrometry (MS) and MS/
MS detectors have been used for the determination of THC
I. Papoutsis � P. Nikolaou (&) � A. Dona � C. Pistos �M. Stefanidou � C. Spiliopoulou � S. Athanaselis
Department of Forensic Medicine and Toxicology,
School of Medicine, National and Kapodistrian University
of Athens, 75 Mikras Asias, 115 27 Athens, Greece
e-mail: [email protected]
123
Forensic Toxicol (2012) 30:51–58
DOI 10.1007/s11419-011-0126-1

and its metabolites in blood [2, 4, 5, 8, 11, 12, 14, 17, 19,
20, 22, 24, 25] or plasma [7, 13, 15, 18, 21], urine [11, 13,
19–21], oral fluid [20], and tissues [18, 23, 26]. To our
knowledge, there is no validated method published con-
cerning the determination of THC and its carboxylic acid
metabolite THCCOOH in bile samples that could be used
for the study of the distribution of cannabinoids and the
establishment of cannabis use. The aim of this study was
the development, optimization, and validation of a GC–MS
method for the determination of THC and THCCOOH
concentrations in bile. The developed method was suc-
cessfully applied in the analysis of bile samples from dead
drug addicts during the investigation of the respective
forensic cases.
Materials and methods
Chemicals and reagents
Methanolic standard stock solutions of THC (1.0 mg/ml),
THCCOOH (0.1 mg/ml), THC-d3 (0.1 mg/ml) and THC-
COOH-d3 (1.0 mg/ml) were purchased from LGC Pro-
mochem (Molsheim, France) and all standards were
[99.9% pure. Bond Elut LRC Certify II Solid Phase
Extraction (SPE) columns were obtained from Varian
(Houten, Netherlands). N,O-bis(trimethylsilyl)trifluoroace-
tamide (BSTFA) with 1% trimethylchlorosilane (TMCS),
pentafluoropropionic anhydride (PFPA) 99%, 2,2,3,3,3-
pentafluoro-1-propanol (PFPOH) 97%, methyl iodide
(CH3I) 99%, and b-glucuronidase (from Helix pomatia,
400,000 units/g) were purchased from Sigma-Aldrich
(Steinheim, Germany). The stock enzyme was diluted with
1.0 M acetate buffer (pH 5.0) to prepare the working
b-glucuronidase solution (100,000 units/ml). All solvents
(methanol, hexane, ethyl acetate, acetone, acetonitrile,
isooctane, acetic acid) were HPLC grade and were pur-
chased from Merck (Darmstadt, Germany). Drug-free bile
samples, verified as negative for drugs by GC–MS, were
pooled and used for the preparation of spiked calibrators
and quality control (QC) samples.
Preparation of standard solutions
Combined stock solutions of THC and THCCOOH were
diluted with methanol to prepare seven calibrator working
solutions (0.02, 0.10, 0.20, 0.50, 1.50, 4.00, and 10.0 lg/ml).
Bile samples for calibration curves were prepared by
spiking pooled drug-free bile (950 ll) with 50 ll of the
above-mentioned working solutions, yielding concentra-
tions for each analyte of 1.00, 5.00, 10.0, 25.0, 75.0, 200,
and 500 ng/ml. QC working solutions were prepared at
concentrations of 0.06, 2.00, and 8.00 lg/ml. Blank bile
samples (950 ll) were fortified with 50 ll of the appro-
priate QC working solutions to give low (3.00 ng/ml),
medium (100 ng/ml), and high (400 ng/ml) concentration
QC samples for each analyte. A working internal standard
solution containing THC-d3 and THCCOOH-d3 at con-
centrations of 0.50 lg/ml was prepared by mixing the
appropriate volumes of the corresponding stock solutions
and then by diluting with methanol. Fresh working solu-
tions were prepared on each day of analysis.
Sample preparation
A volume of 50 ll of the mixed working internal standard
solution (0.50 lg/ml) was added to the calibrator, QC, and
real bile samples (1.0 ml). All samples were vortex-mixed
for 15 s. As a result, all calibrators, QC, and real samples
contained 25.0 ng/ml of THC-d3 and THCCOOH-d3.
Subsequently, 1 ml of 0.1 M acetate buffer (pH 7.0) and
200 ll of working b-glucuronidase solution were added,
the tubes were capped, vortex-mixed for 15 s, and stored at
37�C for 16 h. Following the enzymatic hydrolysis, pro-
teins were precipitated with 3.0 ml of acetonitrile, added
dropwise while vortex mixing. Then the samples were
centrifuged at 2000 rpm for 5 min, the supernatant was
decanted into a clean glass tube, and the solvent was
evaporated under a gentle stream of N2 at 40�C to
approximately 0.5 ml. The pH of all samples was adjusted
to 7 with the addition of 5.0 ml of a mixture of 0.1 M
acetate buffer (pH 7.0) with methanol (95:5, v/v, mixture
A). Bond Elut LRC Certify II SPE columns were condi-
tioned with 2 ml of methanol and 2 ml of mixture A prior
to sample loading. The samples were applied to the col-
umns at a flow rate of approximately 1.0 ml/min. The
columns were washed subsequently with 2 ml of mixture A
and 100 ll of acetone, and they were dried under high
vacuum (C10 mmHg) for 3 min. THC was eluted twice
with 2.0 ml of a freshly prepared mixture of hexane:ethyl
acetate (90:10, v/v). The THC eluates were collected in
clean tubes and evaporated to dryness under a gentle
stream of N2 at 40�C. Then the columns were washed again
with 3.0 ml of methanol 50% and 100 ll of ethyl acetate
and they were dried under high vacuum (C10 mmHg) for
3 min. THCCOOH was eluted twice with 2.0 ml of a
freshly prepared mixture of hexane:ethyl acetate:acetic
acid (90:10:1, v/v/v). The THCCOOH eluates were also
collected in clean tubes and evaporated to dryness under a
gentle stream of N2 at 40�C. All the residues were deriv-
atized by adding 30 ll of acetonitrile and 30 ll of BSTFA
with 1% TMCS, vortex mixing, and heating at 70�C for
30 min. After cooling the tubes, the samples were injected
(1.0 ll) into the GC–MS system.
52 Forensic Toxicol (2012) 30:51–58
123

GC–MS conditions and apparatus
Chromatographic analysis was performed on an Agilent
6890N/5975 GC–MS system, equipped with an HP-5MS
column (30 m 9 0.25 mm i.d., 0.25 lm film thickness).
Helium was used as carrier gas at a flow rate of 1.0 ml/min.
Injections were carried out in the splitless mode using an
Agilent 7683B autosampler system. The initial column
temperature of 150�C with 1-min hold was increased at a
rate of 30�C/min to the final column temperature of 300�C
and held for 11 min. The injector, ion source, and interface
temperatures were maintained at 280, 230, and 280�C,
respectively. The above GC conditions were chosen after
optimization of the developed GC–MS method. The mass
spectrometer was operated in electron-impact ionization
(EI, 70 eV) and selective ion monitoring (SIM) modes for
this assay. The mass fragments used for the qualitative
analysis of analytes were m/z 371, 386, and 303 for THC
(374 for THC-d3), and 371, 473, and 488 for THCCOOH
(374 for THCCOOH-d3). For quantification, mass fragment
m/z 371 was used for THC and THCCOOH, and m/z 374
was used for the deuterated analogs.
The pH meter used was a 691 digital model (Metrohm,
Switzerland) with a glass electrode. An evaporator using
nitrogen (Reacti-Vap Pierce, Model 18780, Rochford, IL,
USA), a furnace (J.P. Selecta, Spain), and a cooled cen-
trifuge (Sigma 4K10, Germany) were also used.
Results and discussion
Method development and optimization
We developed and optimized a sensitive, selective, and
specific GC–MS method for the determination of THC and
THCCOOH in bile samples. The developed method
includes enzymatic hydrolysis using b-glucuronidase prior
to protein precipitation with acetonitrile and SPE using
Bond Elut LRC Certify II columns followed by silylation
using BSTFA with 1% TMCS in acetonitrile environment.
In most GC–MS methods, a derivatization step is
required to increase stability and improve the chromato-
graphic performance of the cannabinoids during analysis.
This part of the sample preparation is not needed in LC
methods [2, 4, 5, 8, 12, 13, 20–25], and the cannabinoids
may be analyzed directly. However, LC-MS-MS instru-
mentation is not widely available for routine analysis in
forensic laboratories worldwide, and it remains a more
expensive analytical technique when compared with
GC–MS. Furthermore, in some previously published
methods [14, 15, 21] the compound identification criteria
were not fulfilled as only one characteristic transition ion
was monitored [21], or in some GC–MS–MS [14] and
GC–MS methods using chemical ionization [15], two
qualifier ions required in addition to the primary ion were
not provided for identification.
During the development and optimization of the GC–MS
method, a derivatization procedure was preferred and dif-
ferent reagents (BSTFA with 1% TMCS, CH3I, PFPA with
PFPOH) were tested. Derivatization of both analytes was
achieved using all the reagents tested. Silylation resulted in
increased sensitivity, so the conditions of this derivatization
reaction (e.g., solvent environment, temperature, time) were
optimized. Conditions of acetonitrile environment, tem-
perature of 70�C, and time duration of 30 min were optimal
for silylation of the cannabinoids. Furthermore, different
chromatographic conditions were tested and the optimal
values were selected according to the peak areas of both
silylated analytes and their resolution.
Optimization of the extraction procedure was also per-
formed. The previously published methods for the determi-
nation of THC and THCCOOH in biological fluids use either
SPE [2, 5, 7, 8, 11, 13, 15, 17, 20, 21, 24, 25] or liquid–liquid
extraction (LLE) [12, 14, 22, 23]. When the LLE technique
was tested using different organic solvents (hexane, ethyl
acetate, and isooctane) or a mixture of hexane:ethyl acetate
(60:40, 70:30, 80:20, and 90:10, v/v) at different pH values
(4.0, 5.0, 6.0, and 7.0), there were many interferences from
endogenous compounds, so the matrix effect influenced the
derivatization of both analytes and reduced the recovery of
the method. In our study, SPE was chosen for sample prep-
aration, because it ensures a rapid, reproducible, and simple
process that gives clean extracts suitable for a derivatization
procedure. Bond Elut LRC Certify II SPE columns were
selected in this study due to their chemical properties
(nonpolar and strong anion exchange) and for their suit-
ability for the analysis of acidic drugs. When these columns
were tested, a low matrix effect was observed and the
recovery results were high for both analytes ([85%). Dif-
ferent ratios of the eluting solvent mixture of hexane:ethyl
acetate for THC (70:30, 80:20, 90:10, and 95:5, v/v) and
hexane:ethyl acetate:acetic acid for THCCOOH (70:30:1,
80:20:1, 90:10:1, and 95:5:1, v/v/v) were evaluated. It was
found that the eluting mixtures of hexane:ethyl acetate
(90:10, v/v) and hexane:ethyl acetate:acetic acid (90:10:1,
v/v/v) gave very good cleanup of the bile samples, and they
gave high and reproducible extraction efficiency values for
THC and THCCOOH, respectively.
Method validation
The combination of protein precipitation and SPE, prior to
silylation, proved to be useful for the determination
of THC and THCCOOH concentrations in bile. The
developed method was validated in terms of selectivity,
specificity, linearity, limit of detection (LOD), limit of
Forensic Toxicol (2012) 30:51–58 53
123

quantification (LOQ), recovery, precision, accuracy, and
robustness according to international guidelines regarding
bioanalytical method validation [27, 28].
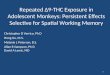
The selectivity of the method was adequate with minimal
matrix effects for all blank bile samples (n = 6); no inter-
ference from endogenous compounds was observed at the
retention times of the analytes. A representative SIM chro-
matogram of a blank bile sample is shown in Fig. 1.
The specificity study found that bile concentrations of
1000 ng/ml of the selected drugs and their metabolites
[cocaine, ecgonine methylester, benzoyloecgonine, mor-
phine, codeine, 6-acetyl-morphine, diazepam, nordiazepam,
alprazolam, bromazepam, 7-amino-flunitrazepam, metha-
done, buprenorphine, nor-buprenorphine, amphetamine,
methamphetamine, 3,4-methylenedioxymethamphetamine
(MDMA), 3,4-methylenedioxyamphetamine (MDA), keta-
mine, ephedrine, amitriptyline, biperiden, phenobarbital,
and clomipramine] do not interfere with the accurate
determination of both analytes in bile.
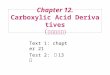
The LOD and LOQ for each analyte were determined as
the lowest bile concentration yielding signal-to-noise ratios
of at least 3:1 (0.30 ng/ml) and 10:1 (1.00 ng/ml),
respectively. A representative SIM chromatogram of a
spiked bile sample at the LOQ concentration (1.00 ng/ml)
is shown in Fig. 2. LOD and LOQ values were also cal-
culated from the residual standard deviation of the
regression line (sb) of the calibration curve and its slope
(a) according to the following equations: LOD = 3.3(sb/a)
and LOQ = 10(sb/a) and the results are presented in
Table 1.
Fig. 1 SIM chromatogram of a
blank bile sample
54 Forensic Toxicol (2012) 30:51–58
123

Linearity was determined by the calculation of the
regression line using the method of least-squares with a
weighting factor of 1/x2. The linear dynamic range for both
analytes of 1.00–500 ng/ml and the correlation coefficients
(R2) exceeded 0.993 and 0.994 for THC and THCCOOH,
respectively. The linearity results are summarized in
Table 1.
Precision and accuracy of the developed method
(intraday n = 6 and interday n = 36) were calculated by
analyzing three QC levels within the linear range of the
analytes (3.00, 100, and 400 ng/ml for both analytes).
Precision was expressed as the relative standard deviation
(% RSD). Accuracy of the method was calculated as the
percentage difference from the expected concentration
Fig. 2 SIM chromatogram of a
spiked bile sample at the LOQ
concentration (1.00 ng/ml)
Table 1 Linearity results of the developed method for the determination of THC and THCCOOH in bile samples
Analyte Concentration range (ng/ml) % RSD of slopes (n = 6) R2 LOD (ng/ml) 3.3(sb/a) LOQ (ng/ml) 10(sb/a)
THC 1.00–500 3.1 C0.993 0.29 0.88
THCCOOH 1.00–500 2.8 C0.994 0.27 0.82
Forensic Toxicol (2012) 30:51–58 55
123

(% Er). Intraday and interday accuracies were in the ranges
of -8.5 to 7.8% and -9.3 to 8.8%, respectively, while
intraday and interday precisions were less than 6.3% and
8.2%. The results are presented in Table 2.
The absolute recovery values of THC and THCCOOH
were evaluated by comparing the peak areas of the spiked
bile samples at three QC levels with the relative areas of
standard methanolic solutions (at the same concentrations)
that were derivatized and injected directly into the GC–MS.
The absolute recovery for each compound, at each con-
centration, was calculated by using the following equation.
% absolute recovery ¼ peak area of extract/ðmean peak area of standard solutionÞ � 100
The absolute recovery at three QC levels was found to
be higher than 87.5% and 92.6% for THC and THCCOOH,
respectively.
Robustness of the entire method was studied by
changing several parameters of the procedure (pH of
samples was adjusted to 7.5 and 6.5 instead of 7.0, deriv-
atization temperature 75 and 65�C instead of 70�C, and the
ratio of the solvents in the elution mixture for THC: 93:7,
Table 2 Intraday and interday accuracy and precision of the developed method for the determination of THC and THCCOOH in bile at three
quality control (QC) concentrations
Analyte QC concentration (ng/ml) Intraday (n = 6) Interday (n = 36)
Accuracy (% Er) Precision (% RSD) Accuracy (% Er) Precision (% RSD)
THC 3.00 -8.5 3.9 -7.8 7.5
100 6.3 4.6 -5.9 6.4
400 -7.9 6.3 6.9 8.2
THCCOOH 3.00 -6.1 5.1 -9.3 8.1
100 7.8 3.7 8.8 6.6
400 -3.9 4.3 -7.4 7.3
Table 3 Concentrations and ratios of THC and THCCOOH in bile and postmortem blood samples
Forensic case THC (ng/ml) THCCOOH (ng/ml)
Bile Blood Ratio Cbile/Cblood Bile Blood Ratio Cbile/Cblood
1 a a – 31.8 1.06 30.0
2 a a – 65.9 a –
3 a a – 180.9 4.59 39.4
4 a a – 150.3 a –
5 15.2 2.66 5.7 252.6 8.54 29.6
6 17.0 2.44 7.0 419.2 4.26 98.4
7 8.40 3.10 2.7 469.0 17.7 26.5
8 2.56 a – 63.0 1.64 38.4
9 a a – 7.29 a –
10 2.17 15.1 0.1 141.6 2.51 56.4
11 2.88 1.56 1.8 226.0 9.37 24.1
12 54.5 24.1 2.3 1126 27.0 41.7
13 a a – 510.8 18.9 27.0
14 a a – 3.44 a –
15 3.01 1.88 1.6 212.6 8.14 26.1
16 2.69 a – 83.7 2.72 30.8
17 2.55 4.25 0.6 114.9 3.57 32.2
18 a a – 29.4 a –
19 a a – 18.6 a –
20 13.8 4.32 3.2 381.9 10.7 35.7
21 3.85 a – 136.2 3.02 45.1
a Not detected
56 Forensic Toxicol (2012) 30:51–58
123

v/v instead of 90:10, v/v, and for THCCOOH: 93:7:1, v/v/v
instead of 90:10:1, v/v/v) as well as GC parameters
(temperature rate, 29.5�C/min; flow rate of carrier gas,
0.97 ml/min; injector temperature, 277�C; and 3% lower
detector voltage). Neither a single parameter nor a com-
bination of the ones changed showed a significant influence
on the results of the method, which proved to be suffi-
ciently robust.
Method application
The developed GC–MS method was proved to be sensitive,
selective, and specific for the determination of THC and
THCCOOH in bile samples during the investigation of
forensic cases. The method was applied for bile samples
(n = 21) after positive screening in urine for the presence
of cannabinoids. THC and THCCOOH bile concentrations
are presented in Table 3. In all cases studied, postmortem
blood samples were also available and were analyzed for
THC and THCCOOH according to the modified method of
Schroeder et al. [11]. The results are shown in Table 3.
When THCCOOH and/or THC were present in blood
samples, their presence was always confirmed in bile
samples. In some cases (2, 4, 8, 9, 14, 16, 18, 19, and 21),
THC and THCCOOH were not detected in blood, but THC
or THCCOOH was detected in bile. The bile-to-blood
cannabinoid concentration ratios were also calculated
(Table 3). The THC ratio varied from 0.1 to 7.0, whereas
the THCCOOH ratio varied from 24.1 to 98.4.
Conclusions
We present a validated, sensitive, and selective method for
the determination of THC and its major metabolite THC-
COOH in bile samples, using gas chromatographic separa-
tion with electron-ionization mass spectrometry detection,
which showed a satisfactory overall analytical performance.
The developed method combined protein precipitation with
SPE, after enzymatic hydrolysis, and provided a thorough
cleanup of the matrix to minimize any endogenous or
exogenous interference, in combination with high recovery,
excellent precision, and accuracy in the linear dynamic
range. The method was successfully applied to bile samples.
Bile concentrations of THC and THCCOOH are generally
severalfold higher than the respective blood concentrations.
This method permits measurement of low concentrations in
bile samples and it provides reliable analytical data that are
prerequisite for correct interpretation of toxicological find-
ings in the evaluation of scientific studies or in the investi-
gation of forensic cases during daily routine work. Bile
could be suggested as the specimen of choice for detecting
cannabis use when the blood cannabinoid concentration is
very low or as an alternative sample especially in cases
where blood samples are not available.
Acknowledgments The authors thank Athanasia Kokkinari and
Christina Paraskevopoulou for their technical assistance in this study.
This research was financially supported by the Special Research
Account of the University of Athens.
References
1. United Nations Office on Drugs and Crime (2011) World Drug
Report. http://www.unodc.org/unodc/en/data-and-analysis/WDR-
2011.html
2. Jamey C, Szwarc E, Tracqui A, Ludes B (2008) Determination of
cannabinoids in whole blood by UPLC-MS-MS. J Anal Toxicol
32:349–354
3. Jones AW, Holmgren A, Kugelberg FC (2008) Driving under the
influence of cannabis: a 10-year study of age and gender differ-
ences in the concentrations of tetrahydrocannabinol in blood.
Addiction 103:452–461
4. Schwope DM, Scheidweiler KB, Huestis MA (2011) Direct
quantification of cannabinoid glucuronides in whole blood by
liquid chromatography-tandem mass spectrometry. Anal Bioanal
Chem 401:1273–1283
5. Konig S, Aebi B, Lanz S, Gasser M, Weinmann W (2011)
On-line SPE LC-MS/MS for the quantification of D9-tetrahy-
drocannabinol (THC) and its two major metabolites in human
peripheral blood by liquid chromatography tandem mass spec-
trometry. Anal Bioanal Chem 400:9–16
6. Athanaselis S, Papadodima S, Maravelias C, Spiliopoulou (2009)
Driving under the influence of cannabis. In: Paterson SE, Allan
LK (eds) Road traffic: safety, modeling and impacts. Nova Sci-
ence, New York, pp 1–13
7. Lowe RH, Karchner EL, Schwilke EW, Barnes AJ, Huestis MA
(2007) Simultaneous quantification of D9-tetrahydrocannabinol,
11-hydroxy-D9-tetrahydrocannabinol, and 11-nor-D9-tetrahydro-
cannabinol-9-carboxylic acid in human plasma using two-
dimensional gas chromatography, cryofocusing, and electron
impact-mass spectrometry. J Chromatogr A 1163:318–327
8. Jagerdeo E, Schaff JE, Montgomery MA, LeBeau MA (2009) A
semi-automated solid-phase extraction liquid chromatography/
tandem mass spectrometry method for the analysis of tetrahy-
drocannabinol and metabolites in whole blood. Rapid Commun
Mass Spectrom 23:2697–2705
9. Holland MG, Schwope DM, Stoppacher R, Gillen SB, Huestis
MA (2011) Postmortem redistribution of D9-tetrahydrocannabinol
(THC), 11-hydroxy-THC (11-OH-THC), and 11-nor-9-carboxy-
THC (THCCOOH). Forensic Sci Int. doi:10.1016/j.forensiint.
2011.06.028
10. Baselt RC (2004) Disposition of toxic drugs and chemicals in
Man, 7th edn. Biomedical Publications, California, pp 1083–1088
11. Schroeder JL, Marinetti LJ, Smith RK, Brewer WE, Clelland BL,
Morgan SL (2008) The analysis of D9-tetrahydrocannabinol and
metabolite in whole blood and 11-nor- D9-tetrahydrocannabinol-
9-carboxylic acid in urine using disposable pipette extraction
with confirmation and quantification by gas chromatography-
mass spectrometry. J Anal Toxicol 32:659–666
12. Fernandez MMR, Boeck GD, Wood M, Lopez-Rivadulla M,
Samyn N (2008) Simultaneous analysis of THC and its metabo-
lites in blood using liquid chromatography-tandem mass spec-
trometry. J Chromatogr B 875:465–470
13. Mercolini L, Musenga A, Comin I, Baccini C, Conti M,
Raggi MA (2008) Determination of plasma and urine levels of
Forensic Toxicol (2012) 30:51–58 57
123

D9-tetrahydrocannabinol and its main metabolite by liquid chro-
matography after solid-phase extraction. J Pharm Biomed Anal
47:156–163
14. Thomas A, Widmer C, Hopfgartner G, Staub C (2007) Fast gas
chromatography and negative-ion chemical ionization tandem
mass spectrometry for forensic analysis of cannabinoids in whole
blood. J Pharm Biomed Anal 45:495–503
15. Goodwin RS, Gustafson RA, Barnes A, Nebro W, Moolchan ET,
Huestis MA (2006) D9-Tetrahydrocannabinol, 11-hydroxy- D9-
tetrahydrocannabinol and 11-nor-9-carboxy- D9-tetrahydrocan-
nabinol in human plasma after controlled oral administration of
cannabinoids. Ther Drug Monit 28:545–551
16. Vanbinst R, Koenig J, Di Fagio V, Hassoun A (2002) Bile analysis
of drugs in postmortem cases. Forensic Sci Int 128:35–40
17. Scurlock RD, Ohlson GB, Worthen DK (2006) The detection of
D9-tetrahydrocannabinol (THC) and 11-nor-9-carboxy- D9-tetra-
hydrocannabinol (THCA) in whole blood using two-dimensional
gas chromatography and EI-mass spectrometry. J Anal Toxicol
30:262–266
18. Brunet B, Doucet C, Venisse N, Hauet T, Hebrard W, Papet Y,
Mauco G, Mura P (2006) Validation of large white pig as an
animal model for the study of cannabinoids metabolism: appli-
cation to the study of THC distribution in tissues. Forensic Sci Int
161:169–174
19. Lin DL, Lin RL (2005) Distribution of 11-nor-9-carboxy-delta9-
tetrahydrocannabinol in traffic fatality cases. J Anal Toxicol
29:58–61
20. Teixeira H, Verstraete A, Proenca P, Corte-Real F, Monsanto P,
Vieira DN (2007) Validated method for the simultaneous deter-
mination of D9-THC and D9-THC-COOH in oral fluid, urine
and whole blood using solid-phase extraction and liquid
chromatography-mass spectrometry with electrospray ionization.
Forensic Sci Int 170:148–155
21. Grauwiler SB, Scholer A, Drewe J (2007) Development of a
LC/MS/MS method for the analysis of cannabinoids in human
EDTA-plasma and urine after small doses of Cannabis sativaextracts. J Chromatogr B 850:515–522
22. Oiestad EL, Johansen U, Oiestad AM, Christophersen AS (2011)
Drug screening of whole blood by ultra-performance liquid
chromatography-tandem mass spectrometry. J Anal Toxicol
35:280–293
23. Gronewold A, Skopp G (2011) A preliminary investigation on the
distribution of cannabinoids in man. Forensic Sci Int 210:7–11
24. Elian AA, Hackett J (2009) Solid-phase extraction and analysis of
THC and carboxy-THC from whole blood using a novel fluori-
nated solid-phase extraction sorbent and fast liquid chromatog-
raphy-tandem mass spectrometry. J Anal Toxicol 33:461–468
25. Coulter C, Miller E, Crompton K, Moore C (2008) Tetrahydro-
cannabinol and two of its metabolites in whole blood using liquid
chromatography-tandem mass spectrometry. J Anal Toxicol
32:653–658
26. Bailey JR, Cunny HC, Paule MG, Slikker WJ (1987) Fetal dispo-
sition on delta 9-tetrahydrocannabinol (THC) during late pregnancy
in the rhesus monkey. Toxicol Appl Pharmacol 90:315–321
27. Guidance for Industry: FDA bioanalytical method validation,
guidelines US Dept. of Health and Human Services, Food and
Drug Administration (FDA), Centre for Drug Evaluation and
Research (CDER), 2001
28. Guidelines for validation of analytical procedures: methodology
step 4 international conference on harmonization of technical
requirements for registration of pharmaceuticals for human use,
ICH harmonized tripartite guideline, 2005
58 Forensic Toxicol (2012) 30:51–58
123
Recommended