Annexures
227
Annexure – I
Ethical Clearance of KLE Univeristy of Higher Education Belgaum
Annexures
228
Annexure – II
Plant Authentication Certificate
Annexures
229
Annexure – III
Animal Ethical Committee Clearance Certificate

Annexures
230
Annexure – IV
Ethical Clearnce certificate: BMK Ayurveda college & Hospital, Belgaum
Annexures
231
Annexures
232
Annexure - V
PRIOR INFORMED CONSENT FORM
Traditional Knowledge Dear Traditional Knowledge holder (s),
This research project ‘Role of Traditional Medicines in Reproductive Health’ is being
conducted by the research fellow Dr. Pushpa Kotur, under the mandate of RMRC
(ICMR) with the intention of documenting and developing the knowledge of herbal
practice. The initiative health will help in reducing the erosion of knowledge, increase
the social esteem of the grassroots innovators and knowledge providers and it will help
India become an innovative society. We strive to obtain the written consent and
authorization from all innovators/knowledge providers to disclose and/or add value to
innovation/traditional knowledge documented for the research project.
Reference No.:_________________________________________________________
Name of the Knowledge Holder: __________________________________________
Title of Traditional Knowledge/ Herbal practice:_____________________________
How did you know about the knowledge/practice?
a) Elders b) Self explored c) Family tradition d) Community
Please fill section A and C for box a, b, c and section B & C for box d
SECTION - A
A. Can your address be shared with those interested in your knowledge?
Yes No
B. Can your traditional knowledge be displayed/published on the Internet/ Scientific
journal?
Yes No
C. if yes, to what extent can your knowledge be shared?
a. Partial disclosure
OR
b. Full disclosure
D. Would you appreciate if further research is conducted on your traditional
knowledge?
If yes, please specify _____________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
Annexures
233
SECTION – B
A. Name of the community’s authorized leader
i. Elected _________________________
ii. Traditional ______________________
B. Can your address be shared with those interested in your knowledge?
Yes/ No
C. Can your traditional knowledge be displayed/published on the Internet/ Scientific
journal?
Yes No
D. If Yes, to what extent your knowledge be shared?
a) Partial disclosure
OR
b) Full disclosure
E. Whether the consent of the local community has been taken while submitting the
community traditional knowledge?
Yes No
F. To what extent specific traditional knowledge/ community knowledge is known and
or practical within or among the concerned communities?
(a)
(b)
G. Has the concerned community been informed of the improvement made in the
traditional knowledge belonging to them?
Yes No
Annexures
234
DECLARATION
I/ We have read this Prior Information Consent form and have understood the
implication of the various choices described in the explanatory note; I/ We have
voluntarily decided to select the option/options which I/ We have ticked above in
the section A and / or Section B. I/ We understand that if the Innovation /
Traditional Knowledge/ ideas provided to you is already well known and is in
public domain, then the restriction on its diffusion and application will not apply. I/
We further assure the researcher that all the information given above is true the b
my/our knowledge and belief.
_________________________
Signature
Name and Address of the Community/ Traditional Knowledge Holder:
_________________________________________________________________
_________________________________________________________________
__________________________________________________________________
_____________________
Signature
Name and Address of the of the Authorized Leader
_________________________________________________________________
_________________________________________________________________
__________________________________________________________________
_____________________
Signature
Name and Address of the Witness/collaborator
_________________________________________________________________
_________________________________________________________________
__________________________________________________________________
____________________________
Signature of theWitness
Date:__________________
Annexures
235
Annexure – VI
Questionnaire: Collection of Information from Traditional Practioner
Interview Schedule for Traditional Healers / Vaidyas
1. Name of the Practitioner / Vaidya / Local Healer:
______________________________________________________________________
2. Complete Address:
______________________________________________________________________
3. Age: Occupation:
4. Economical Status:
5. No. of Children:
Male Female
6. Place of Practice:
______________________________________________________________________
__
7. Experience (in years):
______________________________________________________________________
___
8. Practice Learnt by:
a. From forefathers
b. From others (Specify) _________________________________
c. By reading Books and gathering information.
d. Any other
9. Reason to start Practice:
a. Family business
b. Hobby / Interest
c. Any other
10. Is this your full time profession? Yes / No
11. Average no. of Patients treated per week
a. About 5 patients
b. 5 to 10 patients
c. 10 to 20 patients
d. More than 20 patients
12 Diseases you generally treat
a. ____________________ e. ____________________
b. ____________________ f. ____________________
c. ____________________ g. ____________________
d. ____________________ h. ____________________
Photo
Annexures
236
13. Are you specialized in treating particular disease?
________________________________________________________________
14. What type of people come to you for treatment?
15. How do you diagnose the condition? Explain methods of diagnosis.
16. In which phase of the disease your treatment is useful?
a. Emergency b. Acute c. chronic
17. From where do you collect the medicinal plants used by you? Do you follow
particular method of collection?
Please mention if particular season / time of the day for collection of the plants.
________________________________________________________________
________________________________________________________________
________________________________________________________________
19. How do you procure the medicinal plants used by you?
20. Which type of the plants do you procure? Wild Cultivated
21. Do you use stored or fresh medicinal plants? Fresh Stored
22. How do you store medicinal plants?
23. Have you ever thought of cultivating the plants used by you? If the your answer is
yes what are the conditions required to grow these plants?
________________________________________________________________
________________________________________________________________
24. Do you process / purify before prescribing the medicine? What are the dosages of
the medicines?
25 Which part of the plants do you use? What are the dosages of the medicines?
Disease Plant used Part of the plant Processing Details Dose
Annexures
237
26. Do you prescribe any animal product for treatment / prevention of diseases
Yes/No
If your answer is yes please provide the details
________________________________________________________________
________________________________________________________________
27. Do you advise any dietary or other restrictions to the patient during the course of
treatment? Please provide details.
________________________________________________________________
________________________________________________________________
28. What is the outcome of your treatment?
a. Good b. Very good c. Excellent d. Not so good
29. Have you observed any side effects, interactions of any of the medicinal Plant? If
the answer is yes in which type of patients it is more common and how do you tackle
them?
________________________________________________________________
________________________________________________________________
30. Do you use same medicinal dose/ mode of preparation for all age groups?
________________________________________________________________
________________________________________________________________
31. Do you get the plants in sufficient quantity for your practice? Yes/ No If no please
provide the reasons.
________________________________________________________________
________________________________________________________________
32. Do you get medicinal plants in sufficient quantity?
33. Do you document or keep records of your patients? Do you follow them regularly?
Yes/No
34. Do you want to preserve the heritage of herbal medicine?
Yes/No
35. Are you ready to share/teach the knowledge of herbal medicine to others?
Yes/No
36. What kind of remuneration you are getting from the patients?
37. Do you use any herbal product or medicine to keep yourself healthy and fit
(prevention)?
Annexures
238
Annexure – VII
Data Analysis Sheet
Sl.
No.
Plant
(Local
Name)
Specimen
Number
Part used &
condition
(Fresh/dry)
Quantity Preparation &
Utilization
Dose &
Duration
Disease Miscellaneous
Signature of the Interviewer Date
Annexures
239
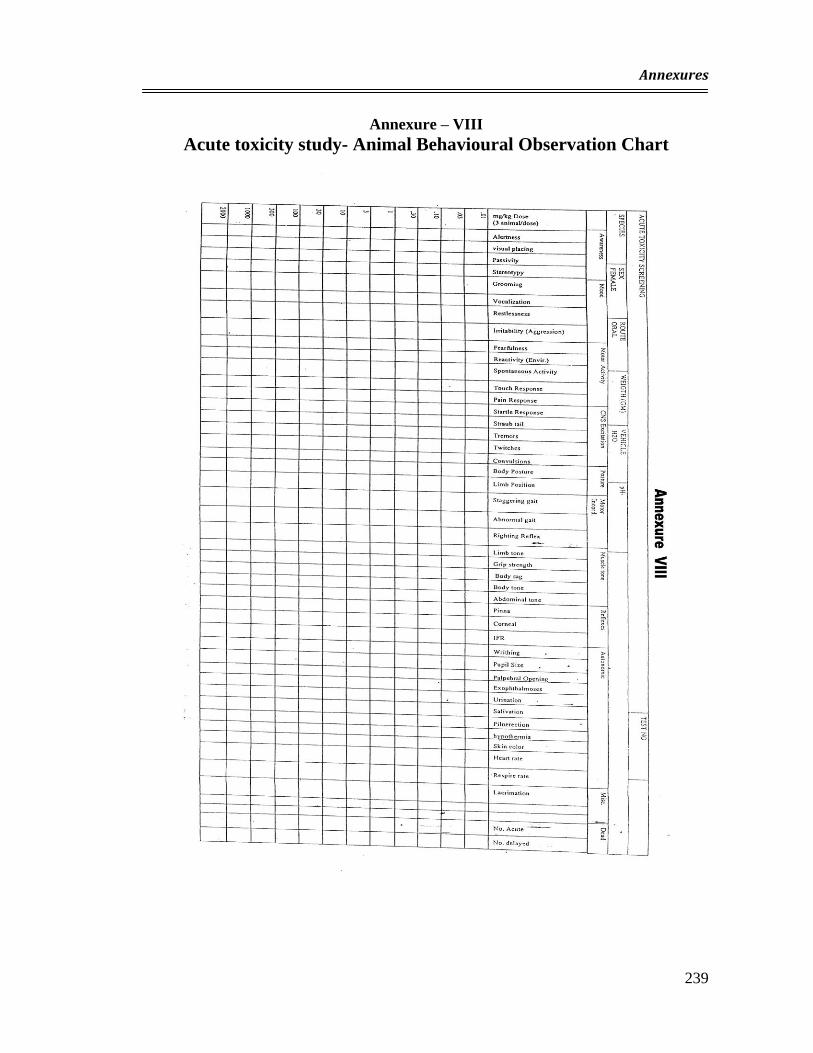
Annexure – VIII
Acute toxicity study- Animal Behavioural Observation Chart
Annexures
240
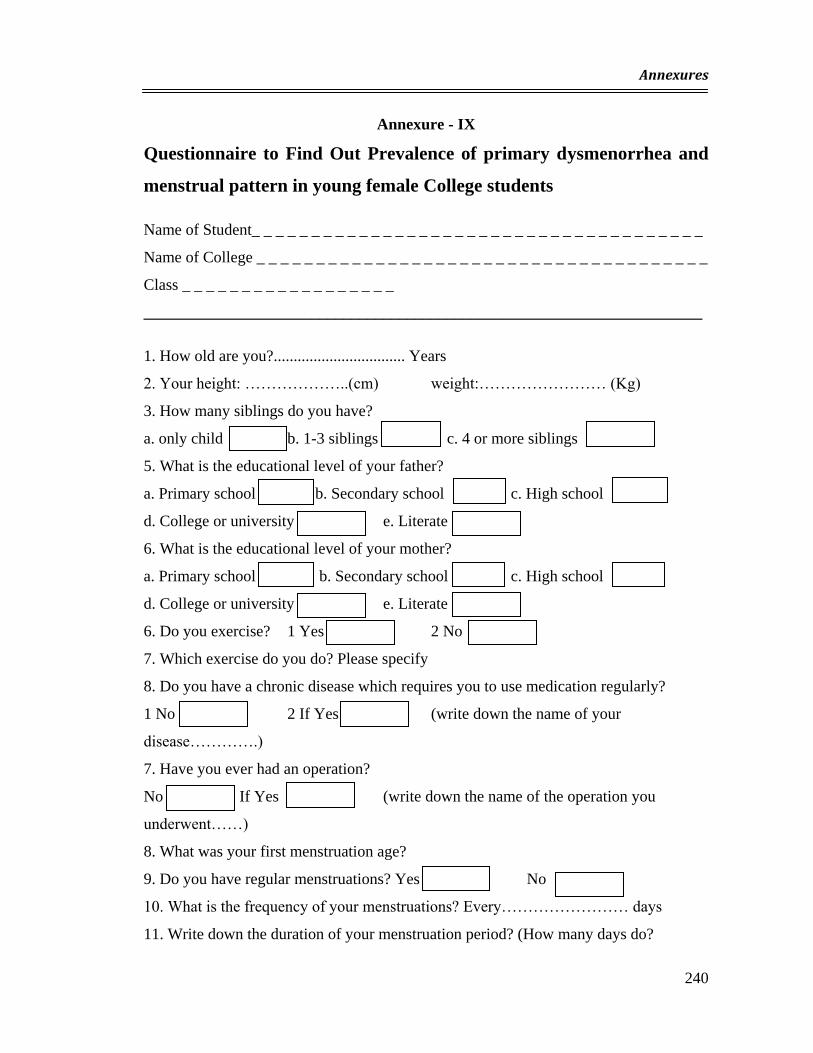
Annexure - IX
Questionnaire to Find Out Prevalence of primary dysmenorrhea and
menstrual pattern in young female College students
Name of Student_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Name of College _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Class _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
______________________________________________________________________
1. How old are you?................................. Years
2. Your height: ………………..(cm) weight:…………………… (Kg)
3. How many siblings do you have?
a. only child b. 1-3 siblings c. 4 or more siblings
5. What is the educational level of your father?
a. Primary school b. Secondary school c. High school
d. College or university e. Literate
6. What is the educational level of your mother?
a. Primary school b. Secondary school c. High school
d. College or university e. Literate
6. Do you exercise? 1 Yes 2 No
7. Which exercise do you do? Please specify
8. Do you have a chronic disease which requires you to use medication regularly?
1 No 2 If Yes (write down the name of your
disease………….)
7. Have you ever had an operation?
No If Yes (write down the name of the operation you
underwent……)
8. What was your first menstruation age?
9. Do you have regular menstruations? Yes No
10. What is the frequency of your menstruations? Every…………………… days
11. Write down the duration of your menstruation period? (How many days do?
Annexures
241
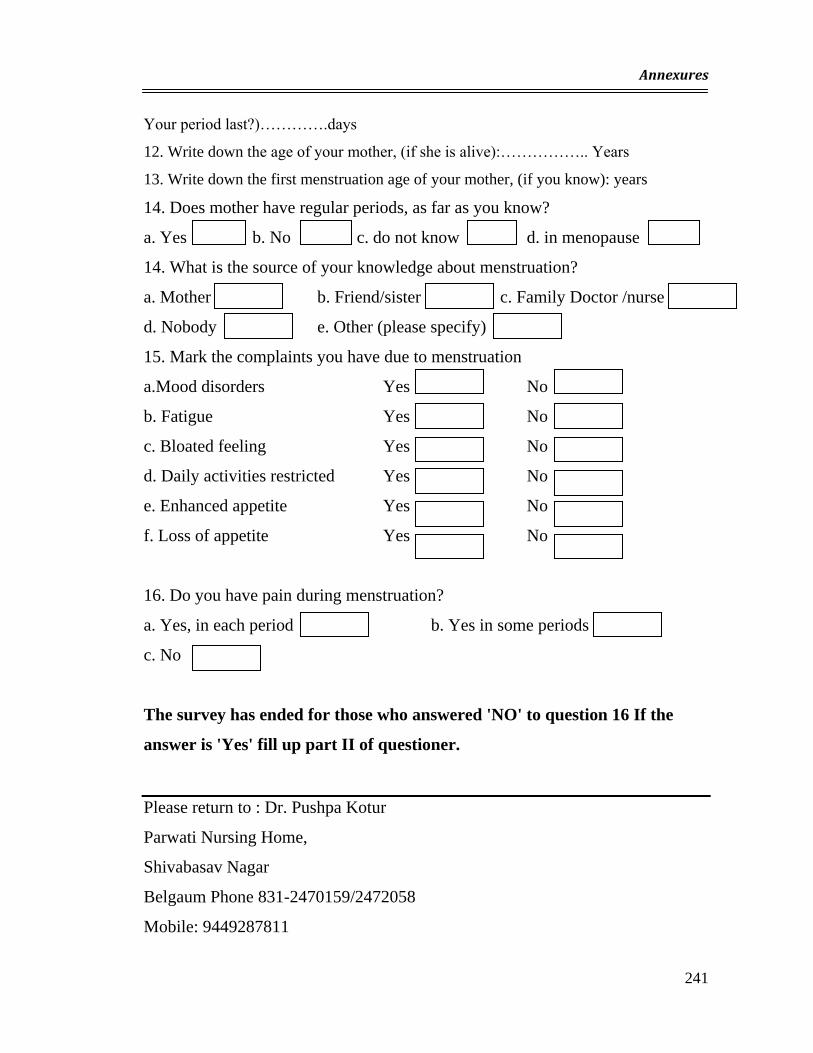
Your period last?)………….days
12. Write down the age of your mother, (if she is alive):…………….. Years
13. Write down the first menstruation age of your mother, (if you know): years
14. Does mother have regular periods, as far as you know?
a. Yes b. No c. do not know d. in menopause
14. What is the source of your knowledge about menstruation?
a. Mother b. Friend/sister c. Family Doctor /nurse
d. Nobody e. Other (please specify)
15. Mark the complaints you have due to menstruation
a.Mood disorders Yes No
b. Fatigue Yes No
c. Bloated feeling Yes No
d. Daily activities restricted Yes No
e. Enhanced appetite Yes No
f. Loss of appetite Yes No
16. Do you have pain during menstruation?
a. Yes, in each period b. Yes in some periods
c. No
The survey has ended for those who answered 'NO' to question 16 If the
answer is 'Yes' fill up part II of questioner.
Please return to : Dr. Pushpa Kotur
Parwati Nursing Home,
Shivabasav Nagar
Belgaum Phone 831-2470159/2472058
Mobile: 9449287811
Annexures
242
Part II Questainner : (The survey continues for those who answered YES)
17. Since when have you been having painful menstruation?
a. Since my first period b. For the last………..... months
c. For the last ……………..years
18. On which day of your period does the pain start?..........................
19. How long does it last?
a. 1 day b. 2 days c. 3days d.4 days /more
20. Do you take analgesic drug for menstrual pain?
No If Yes (indicate the name of the drug:…………)
21. Does your menstruation pattern change when you take analgesic drug?
No If Yes (Please specify the change: …………….)
22. Have you ever seen a doctor for menstrual pain? Yes No
23. Have you ever missed any school day due to menstrual pain in the last year?
a. Never b.1 day c.2days
d. 3-4 days e. 5-6 days f. 7 days or more
24. Have you ever missed any examinations due to menstrual pain in the last year?
a. Never b. Once c. Twice d. Three times or more
25. How do you evaluate your school performance when you have painful
menstruation?
a. Very poor b. Poor c. Average
d. Good e. Very good
26. How do you evaluate your life performance when you have painful menstruation?
a. Very poor b. Poor c. Average
d. Good D e. Very good
27. How would you rate your menstrual pain on a scale from 1 to 10?
Please indicate 0 1 2 3 4 5 6 7 8 9 10
Please return to : Dr. Pushpa Kotur
Parwati Nursing Home, Shivabasav Nagar
Belgaum Phone 831-2470159/2472058, Mobile: 9449287811
Annexures
243
Annexures
244
Annexures
245
Annexures
246
Annexure - XI
INFORMED CONSENT FORM
Investigator: Dr. Pushpa Kotur
Name of the participant;
Mrs / Mr.____________________________________________________ Age
_____________Y rs.
Reg. No. ___________________________
I, Dr. Pushpa Kotur, research fellow, KLE University, Belgaum, request you to be a
participant in the research study titled 'Role-of Traditional Medicine in Reproductive
Health' conducted by me (as a requirement to be fulfilled as a part of my Ph.D.
programme).I request you to read this form and ask questions ,if you have any, regarding
the study prior to signing this form. I am herewith submitting details of the research
protocol as follows:
Aim of The Study: to evaluate the herbal medicines used by the traditional healers in rural
area of Belgaum District.
Purpose of research:
1. To document and develop knowledge of herbal practice and their effective use in
reproductive health care.
2. To evaluate advantages, efficacy, and safety of these herbal practice
Procedure involved:
You will be examined and investigated for your reproductive l1ealth problems. During this
procedure your blood and urine sample may be required to diagnose the nature of disease.
You may be subjected for ultrasonic examination to confirm the diagnosis. Further you will
be offered the herbal medicine to treat your disease/ disorder as per the formulation of the
traditional healer's directions. During the course of treatment you may be advised dietary
restrictions or other form of restrictions.
Once the course of the treatment is over you will be again interviewed to find out the
outcome of the treatment modality. Again you may be subjected to examination and
investigations to document the efficiency, safety of the treatment modality.
Potential risks and discomfort: I would like to quation you that you may be sensitive to
the herbal medicine; more so if you are using some other drugs for the treatment of the
same or some other disease/ disorder because there may be risk of drug interaction in
such situations. Hence I request you to inform us regarding the drugs other than medicine
prescribed by us being used by you during the course of this treatment.
Benefits of participating this research project:
Please note that you will be treated under the supervision of the expert qualified medical
personnel although you have opted for traditional herbal medicine. If you have any side
effects of the herbal medicines, they will be promptly treated, free of cost, in a scientific
manner.
You will be helping to document and apply this knowledge of herbal medicine in a
scientific manner to treat other patients with similar problems in the community.
Annexures
247
New Information:
Any new information collected will be told to you as and when required.
Privacy and confidentiality:
I would like to assure you the privacy and confidentiality will be respected and any
information provided by you or collected during the study will be kept strictly confidential.
Injury as a result of participation:
I will like to state that there will neither be any compensation to you and your relatives nor
there any monitory benefits for the damage incurred during the course of study.
Costs of participation in this research:
Please note that participation is free of cost.
Reimbursement for any expenditure for participation:
There will not be any reimbursement for any of your expenditure.
Withdrawal for any expenses for participation in research:
Please note that to start with the as participation is voluntary so is the decision to withdraw.
I would assure you that such step will not alter the participant's management by any of the
staff of the institution. Kindly note that researcher can remove you from the study if such
circumstances arise.
Whom to contact:
Kindly feel yourself free to enquire about any queries or information regarding the research
project during the study or even thereafter. If required you can contact following persons:
Dr. Pushpa. P. Kotur.
Research fellow, KLE University, Belgaum.
44/Sector 2, Shivabasav Nagar, Belgaum. Phone 9449287811
Dr. S. D. Kholkute. Dy. Director, Regional Medical Research Centre (ICMR), Belgaum
Cell : 9448366539
Dr. B. Srinivasa Prasad. Principal, K.L.E.S. B. M. Kankanwadi Ayurveda Medical College,
Belgaum
Cell :9448569289
Signature of the participant/legally authorized person:
Participant's name:
Signature:
Witness name:
Signature:
Date: Place:
Annexures
248
Annexure - XII
PHASE III A: LIMITED CLINICAL EVALUATION OF HIBISCUS
ROSA SINENSIS L. (WHITE FLOWERS) USED FOR THE
TREATMENT OF VULVO VAGINITIS
PROFORMA
I. Personal History
Intials of the Patient: Age:
Address:
Occupation:
II. Gynaecological complaints:
1. Menstrual Disorders: Duration
a. Menorrhagia b. Hypomenorrhoea
c. Dysmenorrhoea d. Premenstrual Symptoms
e. Menstrual Irregularities:
i. Metrorrhagia
ii. polymenorrhoea
iii. oligermenorrhoea
2. White discharge P/V
3. Blood Stained Discharge
4. Infertility.:
Primary Secondary .
5. Other complaints
Annexures
249
II . Present Menstrual History:
III . Past Menstrual History:
IV . Obstetric History:
1. No.of Deliveries : FTND PTD
2. No. of Abortions:
3. Causes of Abortions :
4. Last Delivery:
5. Underwent Sterilisation:
6. How many Years Back?
V . Past History :
1. H/O Similar Complaints:
2. Duration of Complaints:
3. Diagnosis :
4. Investigations :
5. Treatment Taken :
VI . Medical History :
1. Tuberculosis : 2. Thyroid Disorder:
3. Bleeding Disorder: 4. Hypertension:
5. H/O taking Treatment Duration
Medicines— 1.
2.
3.
4.
6. H/O Surgery in the past
Type of Surgery:
Annexures
250
When?
Post- Operative Medicines:
VII .General Physical Examination:
HT. WT. Nutritional Status:
Temp.: Pulse Resp. Rate:
B.P.: Oedema: Anaemia:
VIII . Systemic Examination:
Cardiovascular
Respiratory:
Per Abdominal:
Per Speculum:
Per Vaginal :
P/R.
IX . Provisional Clinical Diagnosis :
X. Investigations :
Before Treatment After Treatment
1. Hb%
2. T/C
3. Diff Count.
Annexures
251
4. ESR.
5. Urine Analysis
6. RBS
7. BUN.
8. Serum Creatinine
9. Ultrasonography:
10. Pap Smear:
11. Vaginal Smear:
PH
KOH : Fishy Odour Yes No
Wet Smear Trichomoniasis Candidiasis
12. Culture Sensitivity:
High Vaginal Swab
Cervical swab
XI .Final Diagnosis:
XII . Treatment :
Herbal
Conventional : Required Not required
XII . Reassessment and Follow Up:
1. Vaginal Smear:
PH
KOH : Fishy Odour Yes No
Wet Smear Trichomoniasis Candidiasis
2. Culture Sensitivity:
High Vaginal Swab
Cervical swab
Annexures
252
Annexure - XIII
PHASE III B: LIMITED CLINICAL EVALUATION OF LEAVES
AND STEMS OF OCIMUM BASILICUM L. USED FOR THE
TREATMENT DYSMENORRHOEA.
PROFORMA
I. Personal History
Intials of the Patient: Age:
Address:
Occupation:
II. Gynaecological complaints:
1 Menstrual Disorders: Duration
a. Menorrhagia b. Hypomenorrhoea
c. Dysmenorrhoea d. Premenstrual Symptoms
e. Menstrual Irregularities:
i. Metrorrhagia
ii. polymenorrhoea
iii. oligermenorrhoea
2. White discharge P/V
3. Blood Stained Discharge
4. Infertility.:
Primary Secondary .
5 Other complaints
II . Present Menstrual History:
Annexures
253
III . Past Menstrual History:
IV . Obstetric History:
7. No.of Deliveries : FTND PTD
8. No. of Abortions:
9. Causes of Abortions :
10. Last Delivery:
11. Underwent Sterilisation:
12. How many Years Back?
V . Past History :
6. H/O Similar Complaints:
7. Duration of Complaints:
8. Diagnosis :
9. Investigations :
10. Treatment Taken :
VI . Medical History :
2. Tuberculosis : 2. Thyroid Disorder:
4. Bleeding Disorder: 4. Hypertension:
5. H/O taking Treatment Duration
Medicines— 1.
2.
3.
4.
6. H/O Surgery in the past
Type of Surgery:
When?
Post- Operative Medicines:
Annexures
254
VII .General Physical Examination:
HT. WT. Nutritional Status:
Temp.: Pulse Resp. Rate:
B.P.: Oedema: Anaemia:
VIII . Systemic Examination:
Cardiovascular
Respiratory:
Per Abdominal:
Per Speculum:
Per Vaginal :
P/R.
IX . Provisional Clinical Diagnosis :
X. Investigations :
Before Treatment After Treatment
13. Hb%
14. T/C
15. Diff Count.
16. ESR.
17. Urine Analysis
18. RBS
19. BUN.
Annexures
255
20. Serum Creatinine
21. Ultrasonography:
XI .Final Diagnosis:
XII . Treatment :
Herbal
Conventional : Required Not required
XII . Reassessment and Follow Up:
VAS Score:
PBLAC Score :
Hb% :
Side Effects: Acceptance

Annexures
256
Annexure – XIV
Visual Analysis Scale (VAS) Score Chart
Annexures
257
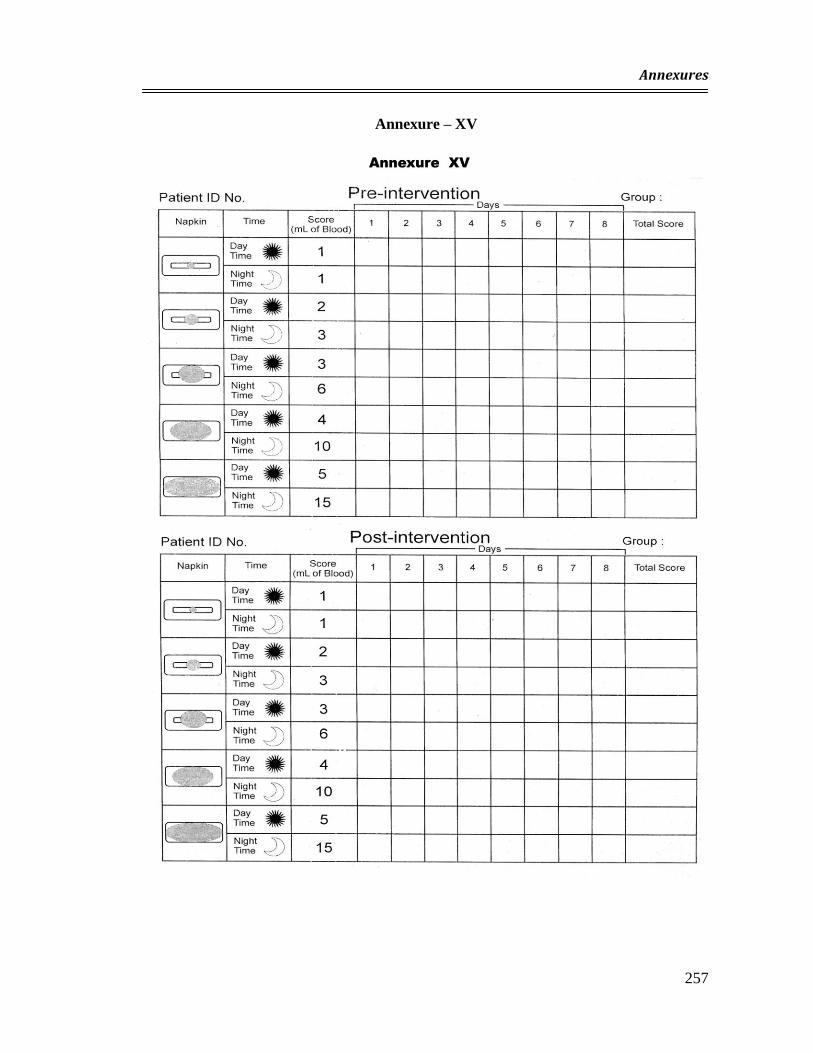
Annexure – XV
Annexures
258
PHASE III-C: LIMITED CLINICAL EVALUATION OF HIBISCUS
ROSA SINENSIS L. (RED FLOWERS) USED FOR THE
TREATMENT OF DYSFUNCTIONAL UTERINE BLEEDING.
PROFORMA
I. Personal History
Intials of the Patient:
Age:
Address:
Occupation:
II. Gynaecological complaints:
1. Menstrual Disorders: Duration
a. Menorrhagia b.Hypomenorrhoea
c Dysmenorrhoea d. Premenstrual Symptoms
e. Menstrual Irregularities:
i) polymenorrhoea ii) oligermenorrhoea
f. Metrorrhagia
2. White discharge P/V
3. Blood Stained Discharge
4. Infertility.:
Primary Secondary
.
5. Other complaints
Annexures
259
II . Present Menstrual History:
III . Past Menstrual History:
IV . Obstetric History:
1. No.of Deliveries : FTND PTD
2. No. of Abortions:
3. Causes of Abortions :
4. Last Delivery:
5. Underwent Sterilisation:
6. How many Years Back?
V . Past History :
1. H/O Similar Complaints:
2. Duration of Complaints:
3. Diagnosis :
4. Investigations :
5. Treatment Taken :
VI . Medical History :
1. Tuberculosis : 2. Thyroid Disorder:
3. Bleeding Disorder: 4. Hypertension:
5. H/O taking Treatment Duration
Medicines— 1.
2.
3.
4.
Annexures
260
6. H/O Surgery in the past
Type of Surgery:
When?
Post- Operative Medicines:
VII .General Physical Examination:
HT. WT. Nutritional Status:
Temp.: Pulse Resp. Rate:
B.P.: Oedema: Anaemia:
VIII . Systemic Examination:
Cardiovascular
Respiratory:
Per Abdominal:
Per Speculum:
Per Vaginal :
P/R.
IX . Provisional Clinical Diagnosis :
X. Investigations :
Before Treatment After Treatment
1. Hb%
2. T/C
3. Diff Count.
4. ESR.
Annexures
261
5. Urine Analysis
6. RBS
7. BUN.
8. Serum Creatinine
9. Ultrasonography:
10. Pap Smear:
11. Endometrial Biopsy
XI .Final Diagnosis:
XII . Treatment :
Herbal
Conventional :
XII . Reassessment and Follow Up:
PBLAC Score :
Hb% :
Side Effects:
Acceptance
Recommended