Case Report
Carcinoma showing thymus-like differentiation (CASTLE) withneuroendocrine differentiation
Manabu Yamazaki,1 Satoshi Fujii,1 Hiroyuki Daiko,2 Ryuichi Hayashi2 and Atsushi Ochiai1
1Pathology Division, Research Center for Innovative Oncology and 2Department of Head and Neck Surgery, NationalCancer Center Hospital East, Chiba, Japan
Carcinoma showing thymus-like differentiation (CASTLE) isa rare malignant neoplasm that histologically resemblesthymic carcinoma and arises in the thyroid gland oradjacent soft tissue of the neck. Herein is reported thecase of a 62-year-old male patient with CASTLE exhibitingneuroendocrine differentiation, who was treated with totalpharyngolaryngo-esophagectomy and total thyroidectomy.Gross examination of the surgical specimen showed agrayish-white, solid, lobulated tumor, mainly locatedbetween the trachea and esophagus, and involving thelower part of the left thyroid lobe. Histologically, the tumorconsisted of epithelial cell nests separated by thick fibroussepta. The tumor cells were polygonal in shape, and con-tained pale cytoplasm and a vesicular nucleus with promi-nent nucleoli. There were few mitotic figures. Rosette-likearrangements that suggested neuroendocrine differentia-tion were observed in part of the tumor. The tumor cellswere positive for CD5 and neuroendocrine markers includ-ing synaptophysin and chromogranin A.
Key words: carcinoma showing thymus-like differentiation,CASTLE, neuroendocrine differentiation
Carcinoma showing thymus-like differentiation (CASTLE) is arare malignant tumor of the neck that histologically resemblesthymic carcinoma.1 Miyauchi et al. first reported three casesof intrathyroidal tumor that resembled primary squamous cellcarcinoma of the thyroid gland but which had a favorableoutcome, as ‘intrathyroidal epithelial thymoma’,2 and Chanand Rosai later designated this type of tumor as CASTLE.3
CASTLE has been postulated to originate from cervicalectopic thymus or branchial pouch remnants. The majority of
tumors occur in the thyroid gland, usually in the lower portion,but they rarely arise in extrathyroidal soft tissue of the neck.1
The histopathology of CASTLE is characterized by an expan-sive growth pattern, thick fibrous bands dividing the tumornests, the presence of lymphocytes, and rare or infrequentmitoses.4 Although, to our knowledge, approximately 30cases of CASTLE have been reported in the English-language literature,2–17 neuroendocrine differentiation inCASTLE has not been described in detail. We report a caseof CASTLE with neuroendocrine differentiation that waslocated in cervical soft tissue and involved adjacent organs,and which required differential diagnosis from other tumorsderived from the thyroid gland and upper aerodigestive tract.
CLINICAL SUMMARY
A 62-year-old Japanese man who had a 6 month history ofcough and sputum consulted a physician, and a lump in hisneck was detected. The patient had never experienced painor dysphagia. He was referred to the Department of Headand Neck Surgery, National Cancer Center Hospital East. CTindicated a well-demarcated cervical mass located on the leftdorsal aspect of the trachea that was connected to the infe-rior portion of the left lobe of the thyroid gland, and thetrachea was displaced to the right (Fig. 1). Radiological evi-dence suggested thyroid cancer. The results of laboratoryexamination were unremarkable. Fine-needle aspirationcytology showed a few clusters of epithelial cells containinglarge nuclei and scant cytoplasm against a clear background,suggesting malignant tumor, but these findings wereinsufficient for cytological evidence indicating papillarythyroid carcinoma or follicular neoplasms. A preoperativeclinical diagnosis of thyroid cancer was made, and totalpharyngolaryngo-esophagectomy combined with total thy-roidectomy was performed and followed by reconstructionwith a free jejunal graft.
Correspondence: Atsushi Ochiai, MD, PhD, Pathology Division,Research Center for Innovative Oncology, National Cancer CenterHospital East, 6-5-1 Kashiwanoha, Kashiwa, Chiba 277-8577,Japan. Email: [email protected]
Received 23 April 2008. Accepted for publication 22 July 2008.© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology
Pathology International 2008; 58: 775–779 doi:10.1111/j.1440-1827.2008.02310.x
PATHOLOGICAL FINDINGS
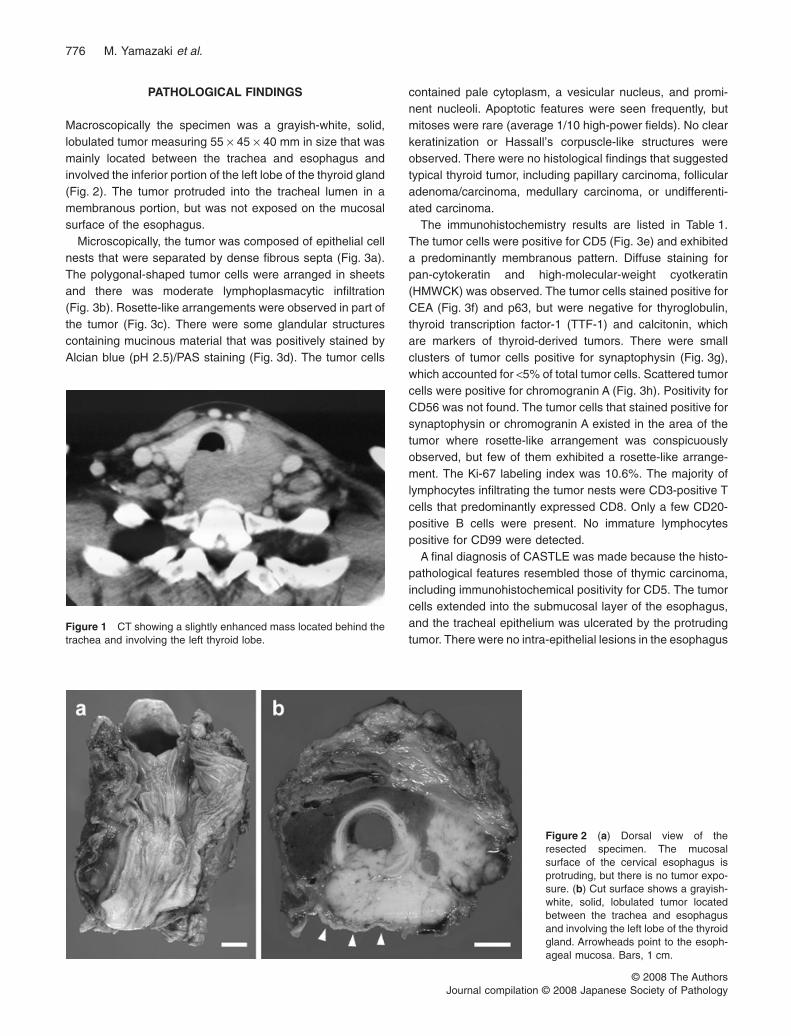
Macroscopically the specimen was a grayish-white, solid,lobulated tumor measuring 55 ¥ 45 ¥ 40 mm in size that wasmainly located between the trachea and esophagus andinvolved the inferior portion of the left lobe of the thyroid gland(Fig. 2). The tumor protruded into the tracheal lumen in amembranous portion, but was not exposed on the mucosalsurface of the esophagus.
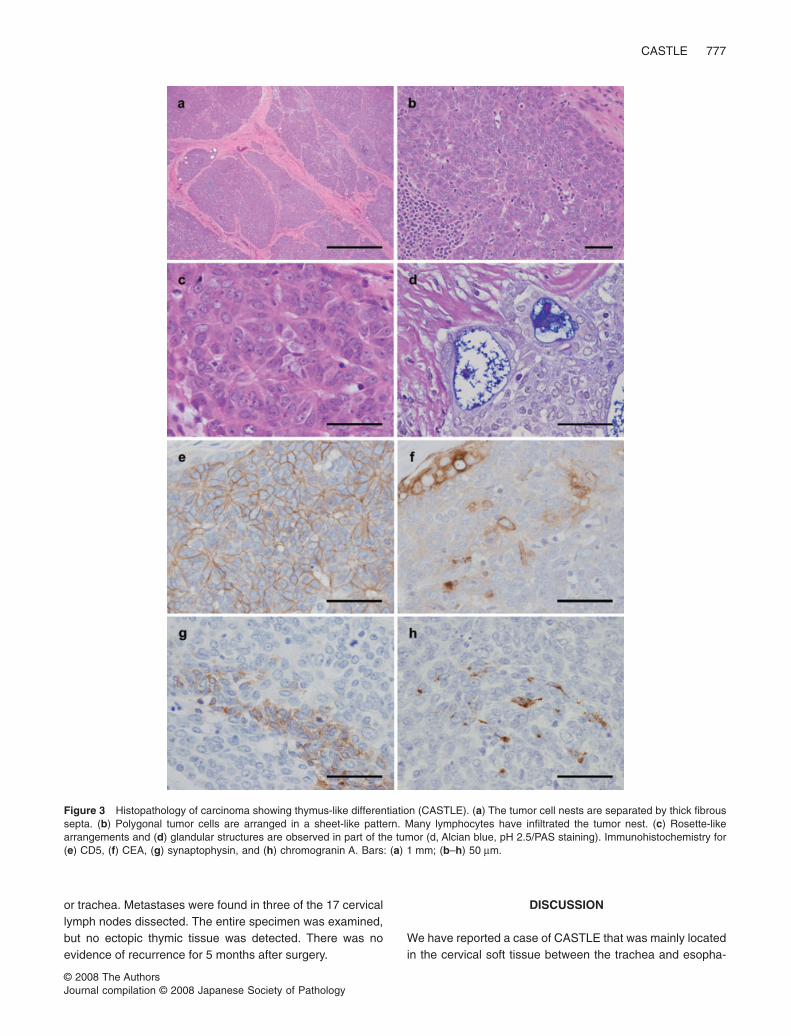
Microscopically, the tumor was composed of epithelial cellnests that were separated by dense fibrous septa (Fig. 3a).The polygonal-shaped tumor cells were arranged in sheetsand there was moderate lymphoplasmacytic infiltration(Fig. 3b). Rosette-like arrangements were observed in part ofthe tumor (Fig. 3c). There were some glandular structurescontaining mucinous material that was positively stained byAlcian blue (pH 2.5)/PAS staining (Fig. 3d). The tumor cells
contained pale cytoplasm, a vesicular nucleus, and promi-nent nucleoli. Apoptotic features were seen frequently, butmitoses were rare (average 1/10 high-power fields). No clearkeratinization or Hassall’s corpuscle-like structures wereobserved. There were no histological findings that suggestedtypical thyroid tumor, including papillary carcinoma, follicularadenoma/carcinoma, medullary carcinoma, or undifferenti-ated carcinoma.
The immunohistochemistry results are listed in Table 1.The tumor cells were positive for CD5 (Fig. 3e) and exhibiteda predominantly membranous pattern. Diffuse staining forpan-cytokeratin and high-molecular-weight cyotkeratin(HMWCK) was observed. The tumor cells stained positive forCEA (Fig. 3f) and p63, but were negative for thyroglobulin,thyroid transcription factor-1 (TTF-1) and calcitonin, whichare markers of thyroid-derived tumors. There were smallclusters of tumor cells positive for synaptophysin (Fig. 3g),which accounted for <5% of total tumor cells. Scattered tumorcells were positive for chromogranin A (Fig. 3h). Positivity forCD56 was not found. The tumor cells that stained positive forsynaptophysin or chromogranin A existed in the area of thetumor where rosette-like arrangement was conspicuouslyobserved, but few of them exhibited a rosette-like arrange-ment. The Ki-67 labeling index was 10.6%. The majority oflymphocytes infiltrating the tumor nests were CD3-positive Tcells that predominantly expressed CD8. Only a few CD20-positive B cells were present. No immature lymphocytespositive for CD99 were detected.
A final diagnosis of CASTLE was made because the histo-pathological features resembled those of thymic carcinoma,including immunohistochemical positivity for CD5. The tumorcells extended into the submucosal layer of the esophagus,and the tracheal epithelium was ulcerated by the protrudingtumor. There were no intra-epithelial lesions in the esophagus
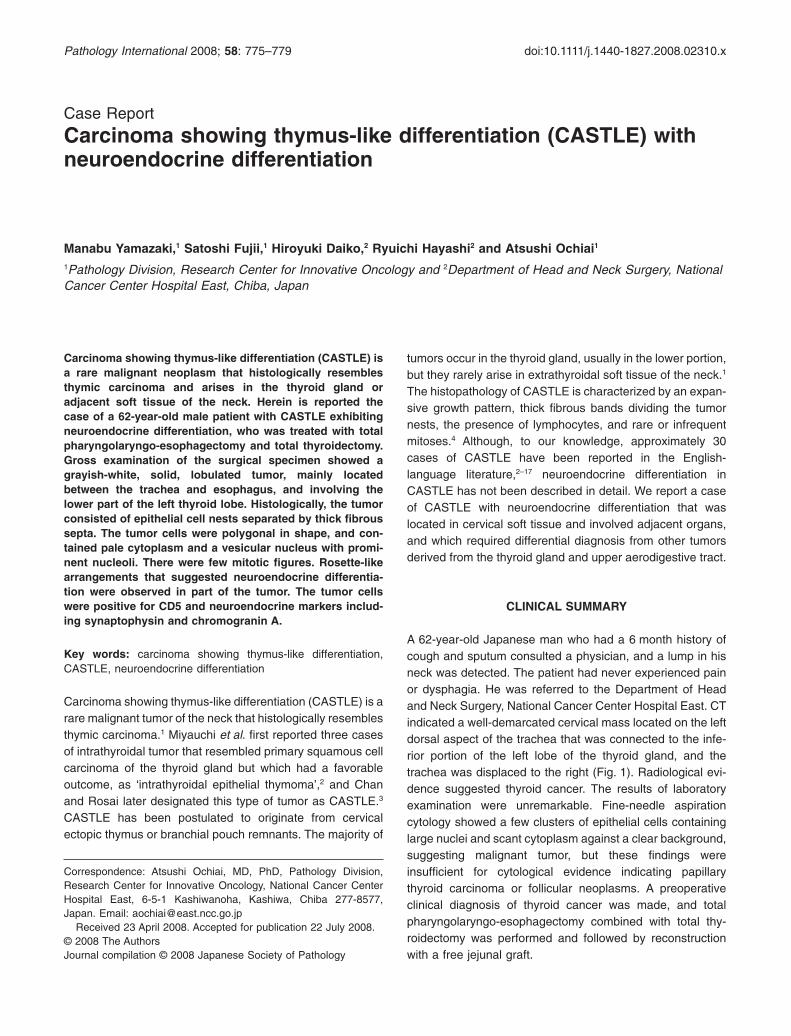
Figure 1 CT showing a slightly enhanced mass located behind thetrachea and involving the left thyroid lobe.
Figure 2 (a) Dorsal view of theresected specimen. The mucosalsurface of the cervical esophagus isprotruding, but there is no tumor expo-sure. (b) Cut surface shows a grayish-white, solid, lobulated tumor locatedbetween the trachea and esophagusand involving the left lobe of the thyroidgland. Arrowheads point to the esoph-ageal mucosa. Bars, 1 cm.
776 M. Yamazaki et al.
© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology
or trachea. Metastases were found in three of the 17 cervicallymph nodes dissected. The entire specimen was examined,but no ectopic thymic tissue was detected. There was noevidence of recurrence for 5 months after surgery.
DISCUSSION
We have reported a case of CASTLE that was mainly locatedin the cervical soft tissue between the trachea and esopha-
Figure 3 Histopathology of carcinoma showing thymus-like differentiation (CASTLE). (a) The tumor cell nests are separated by thick fibroussepta. (b) Polygonal tumor cells are arranged in a sheet-like pattern. Many lymphocytes have infiltrated the tumor nest. (c) Rosette-likearrangements and (d) glandular structures are observed in part of the tumor (d, Alcian blue, pH 2.5/PAS staining). Immunohistochemistry for(e) CD5, (f) CEA, (g) synaptophysin, and (h) chromogranin A. Bars: (a) 1 mm; (b–h) 50 mm.
CASTLE 777
© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology

gus. Primary squamous cell carcinoma or undifferentiatedcarcinoma of the thyroid gland, squamous cell carcinoma ofthe upper aerodigestive tract, and metastatic carcinoma fromother organs, in addition to CASTLE were included in thedifferential diagnosis on histopathology. Squamous cell car-cinoma and undifferentiated carcinoma of the thyroid glandwere less probable because clear keratinization is generallyobserved in squamous cell carcinoma of the thyroid glandand cytological pleomorphism is more prominent in un-differentiated carcinoma of the thyroid gland. Moreover,these carcinomas have a more aggressive clinical course.The distinctive growth pattern, lacking a connection with theesophageal mucosa despite extensive involvement of theesophagus by the tumor, ruled out primary esophageal car-cinoma. Metastatic carcinoma was ruled out based on theresults of the systemic examinations. Although the histologi-cal architecture of this CASTLE tumor apparently resembledthat of orthotopic type B3 thymoma, nuclear atypia observedin this tumor was prominent and there was no involvementof CD99-positive immature lymphocytes. CASTLE was firstreported as ‘intrathyroidal epithelial thymoma’ by Miyauchiet al.2 Chan and Rosai have noted that CASTLE had a morehistological resemblance to thymic carcinoma (so-called typeII malignant thymoma) than thymoma in view of its markednuclear atypia.3
CASTLE tumors are relatively indolent, and grow lessrapidly compared with squamous cell carcinoma of the thy-roid.2 A recent clinicopathological study of 22 patients whounderwent curative surgery found 5 and 10 year cause-specific survival rates of 90% and 82%, respectively.18 Butsome cases involving locoregional recurrence and/or distantmetastasis pursued a rapid fatal course.9–11 These reportsindicate variation in the malignancy of CASTLE. A meta-analysis suggested that patients with nodal metastasis havea high risk of recurrence.6 Nodal metastasis and extrathyroi-dal extension appear to be predictors of a poorer outcome.18
The outcome of orthotopic thymic carcinoma is known to belargely dependent on the histological subtype.19 Tumors with
low-grade histology, such as squamous cell carcinoma andbasaloid carcinoma, have a better prognosis than tumorswith high-grade histology, including lymphoepithelial-like car-cinoma.19 Further investigation is needed to elucidatewhether there are any histological variations in CASTLErelated to the malignancy.
Immunohistochemistry using several markers was helpfulin making the differential diagnosis between CASTLE andother tumors of the thyroid gland and upper aerodigestivetract. CD5 is a surface glycoprotein expressed on mature Tcells and a subset of B cells.20 Thymic carcinoma cells arealso known to be positive for CD5 and it is a useful marker fordifferentiating thymic carcinoma from thymoma.21,22 Immuno-histochemistry for CD5 is positive in the majority of CASTLEtumors.12,13,18 Reimann et al. demonstrated that CD5 was notpositive in all cases of squamous cell carcinoma, poorlydifferentiated carcinoma, or follicular adenoma/carcinoma ofthe thyroid, or in most cases of papillary thyroid carcinoma.13
Other head and neck tumors, including squamous cell carci-noma of the larynx, salivary gland tumors, and parathyroidgland tumors are negative for CD5.12 Ito et al. reported sen-sitivity and specificity for CD5 immunohistochemistry for thediagnosis of CASTLE as 82% and 100%, respectively.18 It isreported that expression of HMWCK, CEA and p63 inCASTLE are evidence of thymic origin and are useful diag-nostic markers to distinguish CASTLE from other thyroidneoplasms.13
Expression of neuroendocrine markers in CASTLE alsosupports the idea that CASTLE is of thymic origin. In thepresent case a few tumor cells were stained positive forsynaptophysin or chromogranin A, but few of these cellsformed rosette-like structures. To date, positivity for chromog-ranin A or neuron-specific enolase has each been reported inonly one case,4,14 while negative results for both markerswere found in several other cases of CASTLE.15–17 Neuroen-docrine markers such as synaptophysin, chromogranin A andneuron-specific enolase are positive in thymic carcinoma infocal or dispersed distribution.23,24 Several neuroendocrine
Table 1 Panel of antibodies used in the present study
Antigen Type Clone Source Dilution Retrieval Result
CD5 RbM SP19 Ventana, Tucson, AZ, USA Pre-diluted Mw +Pan-cytokeratin M AE1/AE3 Novocastra, Newcastle, UK 1:50 Mw +HMWCK M 34bE12 Dako, Glostrup, Denmark 1:50 Mw +CEA P – Dako 1:400 none +p63 M 4A4 Lab Vision, Fremont, CA, USA 1:400 none +Synaptophysin P – Dako 1:400 Mw +Chromogranin A M LK2H10 Ventana Pre-diluted Mw +CD56 M NCC-Lu-243 Nippon Kayaku, Tokyo, Japan 1:25 Mw -Thyroid transcription factor-1 M 8G7G3/1 Dako 1:50 Mw -Thyroglobulin P – Dako 1:5000 none -Calcitonin P – Dako 1:5000 none -Ki-67 M MIB1 Dako 1:50 Mw +: 10.6%
HMWCK, high-molecular-weight cytokeratin; M, mouse monoclonal antibody; Mw, microwave; P, rabbit polyclonal antibody; RbM, rabbit monoclonalantibody.
778 M. Yamazaki et al.
© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology

markers including synaptophysin and chromogranin A arepreferentially expressed in medullary thymic epithelial cellsand Hassall’s corpuscles in human thymus.25 Thymicmicroenvironment, under neuroendocrine control, playsimportant roles in T-cell differentiation.26
In summary, we have reported a case of CASTLE withneuroendocrine differentiation located in the soft tissue of theneck that needed to be differentiated from other tumors of thethyroid gland and upper aerodigestive tract.
REFERENCES
1 DeLellis RA, Lloyd RV, Heitz PU, Eng C, eds. World HealthOrganization Classification of Tumours. Pathology and GeneticsTumours of Endocrine Organs. Lyon: IARC Press, 2004.
2 Miyauchi A, Kuma K, Matsuzuka F et al. Intrathyroidal epithelialthymoma: An entity distinct from squamous cell carcinoma ofthe thyroid. World J Surg 1985; 9: 128–35.
3 Chan JKC, Rosai J. Tumors of the neck showing thymic orrelated branchial pouch differentiation: A unifying concept. HumPathol 1991; 22: 349–67.
4 Asa SL, Dardick I, Van Nostrand AW, Bailey DJ, Gullane PJ.Primary thyroid thymoma: A distinct clinicopathologic entity.Hum Pathol 1988; 19: 1463–7.
5 Watanabe I, Tezuka F, Yamaguchi M, Sagawa J, Kaise N.Thymic carcinoma of the thyroid. Pathol Int 1996; 46: 450–56.
6 Roka S, Kornek G, Schuller J, Ortmann E, Feichtinger J,Armbruster C. Carcinoma showing thymic-like elements: A raremalignancy of the thyroid gland. Br J Surg 2004; 91: 142–5.
7 Luo CM, Hsueh C, Chen TM. Extrathyroid carcinoma showingthymus-like differentiation (CASTLE) tumor: A new case reportand review of literature. Head Neck 2005; 27: 927–33.
8 Piacentini MG, Romano F, De Fina S et al. Carcinoma of theneck showing thymic-like elements (CASTLE): Report of acase and review of the literature. Int J Surg Pathol 2006; 14:171–5.
9 Kakudo K, Mori I, Tamaoki N, Watanabe K. Carcinoma of pos-sible thymic origin presenting as a thyroid mass: A new sub-group of squamous cell carcinoma of the thyroid. J Surg Oncol1988; 38: 187–92.
10 Mizukami Y, Kurumaya H, Yamada T et al. Thymic carcinomainvolving the thyroid gland: Report of two cases. Hum Pathol1995; 26: 576–9.
11 Kusada N, Hara Y, Kobayashi S et al. A case of aggressivecarcinoma showing thymus-like differentiation with distantmetastases. Thyroid 2005; 15: 1383–8.
12 Dorfman DM, Shahsafaei A, Miyauchi A. Intrathyroidal epithelialthymoma (ITET)/carcinoma showing thymus-like differentiation(CASTLE) exhibits CD5 immunoreactivity: New evidence forthymic differentiation. Histopathology 1998; 32: 104–9.
13 Reimann JD, Dorfman DM, Nose V. Carcinoma showingthymus-like differentiation of the thyroid (CASTLE): A compara-tive study: Evidence of thymic differentiation and solid cell nestorigin. Am J Surg Pathol 2006; 30: 994–1001.
14 Alifano M, Boudaya MS, Dinu C, Kadiri H, Regnard JF. Carci-noma showing thymus-like elements invading the trachea.J Thorac Cardiovasc Surg 2006; 132: 191–2.
15 Ahuja AT, Chan ES, Allen PW, Lau KY, King W, Metreweli C.Carcinoma showing thymiclike differentiation (CASTLE tumor).AJNR Am J Neuroradiol 1998; 19: 1225–8.
16 Kwon Y, Hong EK, Koo HL et al. Clinicopathological and immu-nohistochemical studies of thymic-related tumours in thyroidgland: Report of five cases. Histopathology 2006; 48: 312–15.
17 Damiani S, Filotico M, Eusebi V. Carcinoma of the thyroidshowing thymoma-like features. Virchows Arch A Pathol AnatHistopathol 1991; 418: 463–6.
18 Ito Y, Miyauchi A, Nakamura Y, Miya A, Kobayashi K, Kakudo K.Clinicopathologic significance of intrathyroidal epithelialthymoma/carcinoma showing thymus-like differentiation: A col-laborative study with Member Institutes of The Japanese Societyof Thyroid Surgery. Am J Clin Pathol 2007; 127: 230–36.
19 Suster S, Rosai J. Thymic carcinoma. A clinicopathologic studyof 60 cases. Cancer 1991; 67: 1025–32.
20 Bikah G, Lynd FM, Aruffo AA, Ledbetter JA, Bondada S. A rolefor CD5 in cognate interactions between T cells and B cells, andidentification of a novel ligand for CD5. Int Immunol 1998; 10:1185–96.
21 Berezowski K, Grimes MM, Gal A, Kornstein MJ. CD5 immu-noreactivity of epithelial cells in thymic carcinoma and CASTLEusing paraffin-embedded tissue. Am J Clin Pathol 1996; 106:483–6.
22 Dorfman DM, Shahsafaei A, Chan JKC. Thymic carcinomas, butnot thymomas and carcinomas of other sites, show CD5 immu-noreactivity. Am J Surg Pathol 1997; 21: 936–40.
23 Lauriola L, Erlandson RA, Rosai J. Neuroendocrine differentia-tion is a common feature of thymic carcinoma. Am J Surg Pathol1998; 22: 1059–66.
24 Hishima T, Fukayama M, Hayashi Y et al. Neuroendocrine dif-ferentiation in thymic epithelial tumors with special reference tothymic carcinoma and atypical thymoma. Hum Pathol 1998; 29:330–38.
25 Bai M, Papoudou-Bai A, Karatzias G et al. Immunohistochemi-cal expression patterns of neural and neuroendocrine markers,the neural growth factor receptors and the beta-tubulin II and IVisotypes in human thymus. Anticancer Res 2008; 28: 295–303.
26 Savino W, Dardenne M. Neuroendocrine control of thymusphysiology. Endocr Rev 2000; 21: 412–43.
CASTLE 779
© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology
Recommended