Exacerbation of COPDExacerbation of COPD
Tamsil SyafiuddinTamsil Syafiuddin
20052005
AECBAECB

Outline of discussion• Diagosis of COPD• Diagnosis acute exacerbation of COPD• Impact of acute exacerbation COPD• Treatment of acute exaerbation COPD

Definition of Definition of CChronic hronic OObstructive bstructive PPulmonary ulmonary DDisease (isease (COPDCOPD))
• COPD is a disease state characterized by airflow limitation that is not fully reversible
• The airflow limitation is usually both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases.
R. A. Pauwels et al. AJCCM 2001; 163:1256-76NHLBI/WHO Global Initiative (GOLD)

DIAGNOSIS OF COPDDIAGNOSIS OF COPD
• A diagnosis of COPD should be considered in any patient who has symptoms of cough, sputum production, or dyspnea, and/or a history of exposure to risk factors for the disease.
• The diagnosis is confirmed by spirometrie
R. A. Pauwels et al. AJCCM 2001; 163:1256-76NHLBI/WHO Global Initiative (GOLD)

How to Diagnosis/How to thing
Data:
Analysis
Planning
Lung/COPD ?
Heart/LVF?
Cough ?Dyspnoe ?Wheezing ?Age?
Risk factors?
Radiologic examinations?
Spirometri
PEFR
Data

• Pathogenic bacteria are found in 50 - 80% of patients experiencing AECB.
AECBAECB
R. A. Pauwels et al. AJCCM 2001; 163:1256-76NHLBI/WHO Global Initiative (GOLD)

Importance of ExacerbationsImportance of Exacerbations
1Burrows. NEJM 1969; 280:397-4042Miravitlles. Respir Med 1999; 93:173-179
• Exacerbations are the most common observable cause of death in prospective studies1
• COPD patients suffered mean of 2 AE/year, with a high drug use; 10% required admission2

Causative Pathogens in LRTI I
H. influenzae S. pneumoniae Branhamella catarrhalis Mycoplasma/Chlamydia?
Purulent Bronchitis
Advanced Clinical Disease Klebsiella spp. Proteus spp. Enterobacter spp. P. aeruginosa

Infective Exacerbationsof Chronic Bronchitis
Relation betweenBacteriologic Etiology
and Lung FunctionJörg Eller, MD; Anja Ede, MD; Tom Schaberg, PhD;
Michael S. Niedermann, MD, FCCP; Harald Mauch, MD; and Hartmut Lode, MDChest 1998;113:1542-1548

•Study objective: Possible relationship between functional respirat. impairment (FEV1) and pathogens in AECB
•Setting: 6 pneumology units in Spain
•Patients: 91 with AECB
•Interventions: Quantitative sputum cultures (106 pathogens, <10 squ. cells, >25 granuloc.)
Relationship Between Bacterial Flora in Sputum and Functional Impairment in Patients With
Acute Exacerbations of COPD
Miravitlles M et al. Chest 1999;116:40

•Results: FEV1 <50%, was associated with a high risk of P. aeruginosa or H. influenzae isolation (OR; 6.62)
•Conclusions: Pat. with the greatest degree of functional impairment presented a higher probability
of P. aeruginosa or H. influenzae
Relationship Between Bacterial Flora in Sputum and Functional Impairment in Patients With Acute Exacerbations of
COPD
Miravitlles M et al. Chest 1999;116:40

Mira
vitll
es M
et a
l. C
hest
199
9;11
6:40

Changes in Bronchial Inflammation during acute exacerbations of chronic
bronchitis
S. Gompertz, C. O‘Brien, D.L. Bayley, S.L.Hill R.A. Stockley
Europ Respir J 2001; 17:1112-1119

Inflammatory mediators at presentation
Mucoid Purulentbronchitics bronchitics
MPO units x mL-1 0.48 (0.37-0.69) 0.62 (0.42-1.50)+NE nM 0.0 (0.0-0.0) 7.6 (0.8-13.8)***IL8 nM 2.4 (07-4.7) 5.5 (2.8-12.6)***LTB4 nM 3.4 (1.1-11.3) 7.1 (4.6-15.2)+Albumin ratio % 0.4 (0.3-0.9) 1.4 (0.7)-3.1)***
Data are presented as median (interquartile range). MPO:myeloperoxidase; NE: neutrophil elastase; IL-8 interleukin-8; LTB4:leukotriene B4; +: p < 0.025;***: p < 0.001

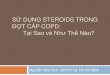
The Vicious Circle of Respiratory Decline in Chronic Bronchitis

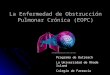
Breathing in COPD

Normal Alveolar Emptying

Alveolar Emptying in COPD
In COPD, airflow is limited because alveoli lose their elasticity, supportive structures are lost, and small airways are narrowed

Breathing in COPD

Air Trapping Air Trapping Occurs in patients with COPDOccurs in patients with COPD Results in an increase in the work of breathing Results in an increase in the work of breathing Places respiratory muscles at a mechanical disadvantagePlaces respiratory muscles at a mechanical disadvantage Contributes to the sensation of breathlessness (dyspnea)Contributes to the sensation of breathlessness (dyspnea)
NormalNormal HyperinflationHyperinflation
Images courtesy of Denis O’Donnell, Queen’s University, Kingston, CanadaImages courtesy of Denis O’Donnell, Queen’s University, Kingston, Canada

Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)
TreatmentTreatment

The 3 major goals of the comprehensive The 3 major goals of the comprehensive treatment of COPDtreatment of COPD : :
•Lessen airflow limitationLessen airflow limitation
•Prevent and treat secondary medical complications Prevent and treat secondary medical complications (eg, hypoxemia, infection) (eg, hypoxemia, infection)
•Decrease respiratory symptoms and improve QoLDecrease respiratory symptoms and improve QoL

The goal of the treatment of COPD The goal of the treatment of COPD
to improve to improve daily livingdaily living and and quality of lifequality of life by by
preventingpreventing symptoms symptoms and and exacerbationsexacerbations
optimal lung functionoptimal lung function

•Smoking cessation is the most important thing to improve COPD symptoms
preventingpreventing symptoms symptoms and and exacerbationsexacerbations

Acute exacerbation of COPD is one of the major reasons for hospital admission in the
United States.

Bronchodilators
• Inhaled beta2 agonists are the treatment of choice for acute exacerbations of COPD
•Usually delivered via a nebulizer
•Adding Xanthin to the combination of bronchodilators can be beneficial
• Inhaled anticholinergic agent is also usually added.
•Corticosteroids are used if do not improve sufficiently after trying other drugs or who develop an exacerbation.
Sharma S, Graham L, Pulmonary and Critical Care Medicine, University of Manitoba, Lung and Airway, 2004

Hospitalized :Hospitalized :
•develop severe develop severe respiratory dysfunctionrespiratory dysfunction•serious serious respiratory diseases (eg, pneumonia, acute respiratory diseases (eg, pneumonia, acute
bronchitis)bronchitis)
The purpose of hospitalization is to The purpose of hospitalization is to treat symptomstreat symptoms and and to to preventprevent further deterioration/lung functions. further deterioration/lung functions.

This therapy is most beneficial for people This therapy is most beneficial for people whose exacerbations are characterized by at whose exacerbations are characterized by at
least 2 of the following (ie, Winnipeg criteria): least 2 of the following (ie, Winnipeg criteria):
•increased shortness of breath,increased shortness of breath,• increased sputum production, increased sputum production,
•and increased sputum purulence.and increased sputum purulence.
AntibioticsAntibiotics

American Thoracic Society Proposed Classification of
AECBsType Core organisms Features
Uncomplicated H. influenzae, S. pneumoniae <4 exacerbations per yearM. catarrhalis, H. parainfluenzae No comorbidity
Complicated Increased risk of drug-resistant <64 years oldS. pneumoniae and Gram- <4 exacerbations per year negative bacilliComorbidityCost of failure greater
Suppurative Risk of P. aeruginosa Chronic steroid useFEV1 <35% of predicted
American Thoracic Society. Am J Respir Crit Care Med 2001,

Winnipeg criteria for AECBWinnipeg criteria for AECB
Typ I Typ II Typ III*Dyspnoe
Sputum purulent
Sputum volume
Anthonisen et al. Ann Intern Med 1987

American Thoracic Society Proposed Treatment
Guidelines for AECBsType Agent
Uncomplicated New macrolide (azithromycin, clarithromycin), cephalosporin (cefuroxime, cefpodoxime, cefprozil) doxycycline
Complicated Fluoroquinolone, amoxicillin/claculanic
Suppurative Ciprofloxacin
American Thoracic Society. Am J Respir Crit Care Med 2001,

General guidelines that are used in determining the ideal time to begin ventilatory support are as follows:
•progressive worsening of respiratory acidosis and/or an altered mental state.
•significant hypoxemia despite supplemental oxygen.
Assisted ventilation/ICUAssisted ventilation/ICU

Admitted to the intensive care unit (ICU) if require the following symptoms:
•Confusion
•Lethargy
•Respiratory muscle fatigue
•Worsening hypoxemia (not enough oxygen in the blood)
•Respiratory acidosis (retention of carbon dioxide in the blood)

How to Diagnosis/How to thing
Data:
Analysis
Planning
Lung/COPD ?
Heart/LVF?
Cough ?Dyspnoe ?Wheezing ?Age?
Risk factors?
Radiologic examinations?
Spirometri
PEFR
Data

Missed diagnosis COPD




Recommended