1
MINISTÉRIO DA EDUCAÇÃO
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
PÓS-GRADUAÇÃO CIÊNCIAS DA SAÚDE
EFEITOS DA SINTOMATOLOGIA DEPRESSIVA NA MOBILIDADE DE
IDOSOS DE UM CENTRO URBANO DO NORDESTE BRASILEIRO
CRISTIANO DOS SANTOS GOMES
NATAL
2013

2
MINISTÉRIO DA EDUCAÇÃO
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
PÓS-GRADUAÇÃO CIÊNCIAS DA SAÚDE
EFEITOS DA SINTOMATOLOGIA DEPRESSIVA NA MOBILIDADE DE
IDOSOS DE UM CENTRO URBANO DO NORDESTE BRASILEIRO
Dissertação de mestrado apresentada à Universidade
Federal do Rio Grande do Norte – Programa de Pós-
Graduação em Ciências da Saúde, para obtenção do
título de mestre.
Orientador: Prof. Dr. Ricardo Oliveira Guerra
Natal/RN
2013


3
MINISTÉRIO DA EDUCAÇÃO
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
PÓS-GRADUAÇÃO CIÊNCIAS DA SAÚDE
Coordenadora do Programa de Pós- Graduação em Ciências da Saúde
Profª Drª Ivonete Batista Araújo

4
AGRADECIMENTOS
Aos idosos participantes dessa pesquisa por sua disponibilidade e
presteza na ocasião das entrevistas, mesmo em meio a tantas situações
adversas.
Aos colegas do laboratório 07 do Departamento de Fisioterapia pelas
experiências, aflições e aprendizados compartilhados diariamente nesses dois
anos e pelo companheirismo de sempre. Em especial Juliana Fernandes,
Mayle e Juliana Souza, parceiras desde a graduação.
A Profª Draª Aline Freire pelo apoio e disponibilidade nos inúmeros
momentos de dúvida no decorrer desse processo de formação.
Ao estimado Prof.º Dr. Ricardo Oliveira Guerra pela paciência de Jó e
sabedoria de Salomão na hora de transmitir seus valiosos ensinamentos.
A minha mãe, Dona Maria Salete que com sua infinita garra e dedicação
sempre lutou pelo meu crescimento enquanto pessoa, cidadão e profissional.
Palavras nunca serão suficientes para descrever quão grato e feliz estou
nesse momento.

5
RESUMO
O processo de envelhecimento da humanidade é um fenômeno mundial
e nas últimas décadas a população brasileira tem acompanhado essa
tendência. No entanto, este fenômeno somente pode ser considerado como
uma real conquista em termos sócios demográficos na medida em que se
agregue qualidade aos anos adicionais de vida para a população. Em
populações idosas, a incapacidade funcional e os sintomas depressivos
tornaram-se importantes conceitos tanto por suas consequências para a saúde
pública, quanto pelo impacto na qualidade de vida dessas populações. Este
estudo tem como objetivo verificar se há associação entre os sintomas
depressivos e o desempenho funcional de idosos comunitários. Foram
avaliados 313 idosos de um centro urbano do nordeste brasileiro através das
baterias de testes; Center for Epidemiologic Studies Depression – CES-D e
Short Physical Performance Battery - SPPB; além de variáveis relacionadas ao
estado físico, condições crônicas, função cognitiva e características sócio
demográficas. Foram utilizadas medidas de correlação e aplicado método de
análise multivariada para construir um modelo explicativo da influência da
sintomatologia depressiva no desempenho funcional. Os resultados revelaram
que as mulheres apresentaram mais sintomas depressivos (p< 0.01) e pior
desempenho funcional (p< 0.01) que os homens. Os indivíduos com
sintomatologia depressiva apresentaram pior desempenho funcional,
especialmente as mulheres. A idade, o sexo feminino, o estado de saúde
percebido, o nível de função cognitiva e o Índice de massa corporal foram
identificados como fatores associados ao desempenho funcional na amostra
estudada. Os resultados deste estudo permitem inferir a relação de associação
entre sintomas depressivos e desempenho funcional em uma população de
idosos de um centro urbano no nordeste do Brasil. Estes resultados fornecem
informações úteis para intervenções terapêuticas adequadas voltadas para a
prevenção do declínio na mobilidade em idosos.
Palavras Chave: Idosos, depressão, mobilidade

6
LISTA DE FIGURAS
Figura 01: Localização do bairro das Rocas.
Figura 02: Fluxograma de seleção da amostra

7
LISTA DE QUADROS
Quadro 01: Modelo conceitual proposto para descrever o processo de
incapacidade.
Quadro 02: Quadro de variáveis independentes
Quadro 03: Quadro de variáveis dependentes

8
LISTA DE TABELAS
Table 1. Sociodemographic and clinical characteristics of the sample.
Table 2.Short Physical Performance Battery scores among subjects with and
without depressive symptoms.
Table 3. Results of linear regression analysis

9
SUMÁRIO
1. INTRODUÇÃO.....................................................................................................pg 10
1.1 Desempenho funcional.....................................................................................pg 10
1.2 Sintomas Depressivos.......................................................................................pg 11
2. JUSTIFICATIVA.....................................................................................................pg 13
3. OBJETIVOS...........................................................................................................pg 15
4. MÉTODO..............................................................................................................pg 16
4.1. Natureza do Estudo..........................................................................................pg 16
4.2. População e Amostra........................................................................................pg 16
4.3. Cálculo do tamanho amostral...........................................................................pg 17
4.4 Critérios de inclusão..........................................................................................pg 17
4.5. Procedimento para coleta de dados.................................................................pg 18
4.5.1. Treinamento dos entrevistadores.................................................................pg 18
4.5.2 Estudo Piloto..................................................................................................pg 18
4.5.3. Recrutamento da amostra.............................................................................pg 19
4.5.4. Coleta de Dados ............................................................................................pg 19
4.6. Variáveis do estudo............................................................................................pg 20
4.6.1. Variáveis independentes...............................................................................pg 20
4.6.2. Variáveis Dependentes.................................................................................pg 21
4.7. Instrumentos Utilizados – Questionários ........................................................pg 21
4.8. Aspectos Éticos..................................................................................... ...........pg 23
5. RESULTADOS.......................................................................................................pg 24
6. COMENTÁRIOS, CRÍTICAS E SUGESTÕES.............................................................pg 40
7. REFERÊNCIAS BIBLIOGRÁFICAS...........................................................................pg 42
ANEXOS......................................................................................................................pg 45

10
1. INTRODUÇÃO
O processo de envelhecimento da população é um fenômeno mundial[1] e
nas últimas décadas o Brasil tem acompanhado essa tendência demográfica.
De acordo com projeções recentes, a população de 65 anos ou mais passará
de 3,1% do total de brasileiros em 1970 para cerca de 19% em 2050[2]. No
entanto, o aumento da expectativa de vida na população brasileira só poderá
ser considerado como uma real conquista do bem-estar social, na medida em
que se agregue qualidade aos anos adicionais de vida[3]
O crescimento demográfico da população idosa brasileira vem sendo
acompanhado por aumento na prevalência de doenças crônico degenerativas e
incapacidades[4]. Outra característica importante desse grupo etário observada
na segunda metade do século XX foi um acelerado processo de urbanização,
em apenas 40 anos houve uma transição de uma população eminentemente
rural para eminentemente urbana[5]. As condições socioeconômicas
vivenciadas por essa população muitas vezes são precárias, e consideradas
como principais motores propulsores de eventos estressantes podendo
culminar em quadros depressivos[6], o que resulta em novas demandas aos
sistemas de saúde[3, 7].
Quando se pensa na elaboração de uma nova política de cuidado para o
idoso baseada na qualidade de vida, o desempenho funcional ocupa lugar
peculiar, pois expressa as habilidades físicas e mentais necessárias à vida
independente e autônoma[8].
1.1. Desempenho funcional
Em populações idosas, a incapacidade funcional tornou-se um importante
conceito tanto por suas conseqüências em saúde pública, quanto pelo impacto
na qualidade de vida dessas populações, podendo resultar em desfechos
adversos e aumento no custo de saúde [9]. A perda de independência funcional,
comum no processo de envelhecimento humano, tem grande impacto na
qualidade de vida dos idosos e resulta em ônus social e econômico [10]. Com o

11
avançar da idade, a capacidade funcional em realizar tarefas avançadas e
básicas da vida diária incluindo tarefas domésticas, de auto-cuidado e outras
atividades consideradas importantes para a qualidade de vida tornam-se
progressivamente limitadas[9]. Devido a este fato, a prevenção da incapacidade
tem emergido como um importante tópico para gerontologia e medicina
geriátrica [10].
Geralmente, a incapacidade em idosos é medida através de auto-relato de
funcionalidade em diferentes atividades da vida diária[11]. Entretanto, medidas
eficazes e eficientes de avaliação do desempenho físico em idosos têm sido
desenvolvidas[12].
Considerando que medidas de desempenho físico refletem limitações na
funcionalidade e que essas limitações podem levar a incapacidade, foi
desenvolvida uma bateria de testes que incluem tarefas relacionadas à função
dos membros inferiores, com o intuito de prover informações a respeito de todo
o espectro de funcionalidade. Assim, Guralnik et al. desenvolveu uma bateria
de testes denominada Short Physical Performance Battery (SPPB)[13] como
uma medida do desempenho funcional dos membros inferiores em uma
população de indivíduos idosos comunitários. O baixo desempenho físico nos
membros inferiores tem sido apontado como um forte fator de risco para a
incidência de incapacidade, hospitalização, institucionalização e mortalidade [14,
15].
1.2 Sintomas depressivos:
A depressão é um dos problemas de saúde mental mais comum entre os
idosos[16], e a prevalência global estimada de sintomas depressivos entre
idosos comunitários é de 15%[17]. O interesse pelo tema depressão em idosos
tem crescido com o aumento do percentual dos mesmos, na população, e
pelas dificuldades encontradas por profissionais da área de saúde em
diagnosticar e tratar esses pacientes[18]. A dificuldade no diagnóstico se
apresenta pela presença de problemas físicos coexistentes, fazendo com que,
freqüentemente, os profissionais de saúde encarem os sintomas depressivos
como manifestações normais do envelhecimento[19, 20].
12
Na população idosa os sintomas depressivos se apresentam de forma
peculiar, e são caracterizados por alterações do humor, com sentimentos de
tristeza, baixa auto-estima, pensamentos negativos recorrentes e
desesperança. Também podem ser observadas, diminuição do sono, perda de
prazer nas atividades habituais, irritabilidade, fadiga e perda de energia. [19]
Ainda que a depressão acarrete várias alterações, ela não apresenta
taxas muito elevadas de mortalidade, porém, possui um grande peso na
incapacidade. Os sintomas depressivos estão relacionados com co-morbidades
físicas, baixos níveis de qualidade de vida e incapacidade funcional[21, 22].
Alguns autores propõem o envolvimento de mecanismos
comportamentais e biológicos para explicar essa associação entre depressão e
aspectos relacionados à funcionalidade em idosos, no entanto os achados na
literatura a respeito desses mecanismos ainda não são conclusivos[23-25]. Nesse
sentido, sintomas comuns da depressão, como insônia, ganho ou perda de
peso, podem ter efeitos deletérios ao longo do tempo, resultando em
incapacidade. Além disso, a depressão também pode reduzir a motivação, que,
por sua vez, pode levar a comportamentos prejudiciais à saúde, como a
inatividade física e a ausência de cuidados médicos adequados. Por fim, o
sofrimento psíquico decorrente da depressão pode alterar a função neural,
hormonal e imunológica, aumentando assim a susceptibilidade à doença e
posterior declínio de diversos aspectos da saúde física[26,27].

13
2. JUSTIFICATIVA
No último século a população mundial passou por um processo de
transição demográfica sendo expressa de forma robusta no crescimento da
população idosa. Este processo parece ser resultado de avanços nas ciências
médicas, da melhoria de condições socioeconômicas, e do acesso aos serviços
de saúde em diversos países do mudo. O aumento da população idosa trouxe
consigo uma série de novas realidades que chamam a atenção dos
profissionais de saúde e estudiosos da área de envelhecimento, dentre elas
destaca-se os quadro de redução progressiva da mobilidade ao longo dos
anos.
A mobilidade é considerada do ponto de vista conceitual, a habilidade
para mover-se no seu próprio ambiente. O declínio da mobilidade é um dos
primeiros estágios do processo de incapacidade, que se estende desde o
aparecimento de doenças crônicas até a perda de independência funcional e
autonomia. A perda da mobilidade tem consequências para a qualidade de
vida, com forte impacto sobre a saúde física e mental, e na capacidade de
realizar atividades instrumentais e básicas da vida diária, que aumenta o risco
de institucionalização e mortalidade.
Modelos conceituais propostos por estudiosos para descrever o
processo de desenvolvimento da incapacidade (Quadro abaixo) apontam a
deficiência de órgãos e sistemas, como estágios iniciais que repercutem nas
atividades da vida diária e na incapacidade no sentido mais amplo do ponto de
vista social. Desta forma, podemos supor que aspectos importantes como a
mobilidade no sentido de deficiência, poderá ser agravada por diversos fatores
de risco entre os quais, estados comportamentais como a depressão,
influenciam de forma direta ou indiretamente no agravo do declínio da
mobilidade.

14
Quadro 01: Modelo conceitual proposto para descrever o processo de
incapacidade.
Atualmente a depressão é apontada como uma das patologias mais
prevalentes no campo da saúde mental, em populações idosas, os estados
depressivos são resultados do acúmulo de eventos estressores ao longo do
curso da vida, agravados pelas perdas sociais inerentes a esta população. A
busca do entendimento das relações existentes entre a redução da mobilidade
e os sintomas depressivos tem sua relevância devido a sua associação com
desfechos adversos à saúde em idosos.
Estudos epidemiológicos de caráter observacional em populações
idosas com características socioeconômicas desfavoráveis permitem a análise
dos fatores associados ao declínio do desempenho físico neste contingente. Os
resultados de estudos desta natureza ajudam na elaboração de possíveis
intervenções de prevenção em nível individual e comunitário. Essa perspectiva
de prevenção deverá ser complementar ao desenvolvimento de projetos de
assistência a idosos.

15
3. OBJETIVOS
Geral:
Investigar se há associação entre os sintomas depressivos e o
desempenho funcional de pessoas idosas de um centro urbano do
nordeste brasileiro.
Específicos:
Estimar as diferenças entre homens e mulheres relacionadas aos
sintomas depressivos e desempenho funcional.
Verificar se há diferenças no desempenho funcional entre aqueles
indivíduos que apresentam sintomas depressivos e aqueles não
apresentam esses sintomas.
Identificar fatores associados aos escores obtidos no teste de
desempenho funcional

16
4. MÉTODOS
4.1 Natureza do Estudo
O presente estudo caracteriza-se por ser de natureza epidemiológica, do
tipo transversal e faz parte de um estudo maior denominado “Carga alostática,
Fragilidade e Função física em idosos residentes da comunidade”.
4.2. População e Amostra
O universo desse estudo é constituído por homens e mulheres idosos com
idade igual ou superior a 65 anos, residentes no bairro das Rocas (Figura 1),
localizados no distrito leste da Cidade de Natal, capital do estado do Rio
Grande do Norte.
Figura 1. Localização do Bairro Rocas. Fonte: Mapa elaborado pela SEMURB – Secretaria Municipal de Meio Ambiente e Urbanismo, 2009.
De acordo com a estrutura etária da população e a população total
residente no bairro no ano 2008 (IBGE 2008), temos como total da população
nas Rocas, 11.061 habitantes, destes 1.056 são indivíduos com 65 anos ou
17
mais, correspondendo a aproximadamente 10% da população total que reside
neste bairro.
4.3. Cálculo do tamanho amostral
Este estudo fez parte de um projeto maior denominado “Carga alostática,
fragilidade e função física em idosos residentes na comunidade” que deu
origem a uma tese de doutorado. Portanto, para fins de cálculo do tamanho
amostral foi considerado que a probabilidade de torna-se frágil entre aqueles
com alta Carga Alostatica é o dobro daqueles com baixa Carga Alostática,
sendo a proporção da população com alta Carga Alostática igual a B=0,33. Foi
admitido um α=0,05 para erros do tipo I, e β=0.80 para erros do tipo II. Dessa
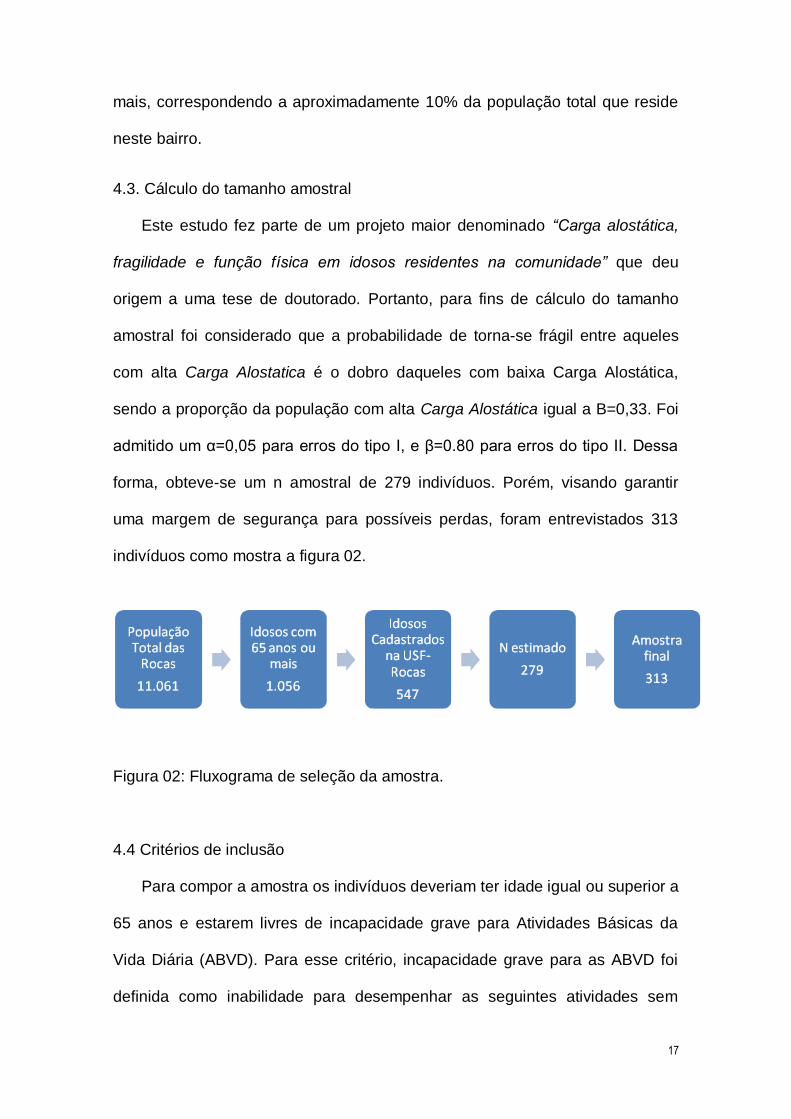
forma, obteve-se um n amostral de 279 indivíduos. Porém, visando garantir
uma margem de segurança para possíveis perdas, foram entrevistados 313
indivíduos como mostra a figura 02.
Figura 02: Fluxograma de seleção da amostra.
4.4 Critérios de inclusão
Para compor a amostra os indivíduos deveriam ter idade igual ou superior a
65 anos e estarem livres de incapacidade grave para Atividades Básicas da
Vida Diária (ABVD). Para esse critério, incapacidade grave para as ABVD foi
definida como inabilidade para desempenhar as seguintes atividades sem

18
ajuda: tomar banho, levantar da cama, comer, vestir-se ou usar o banheiro.
Aqueles que relataram ter alguma dificuldade, mas que eram capazes de
realizar essas atividades foram incluídos no estudo.
Além disso, os participantes deveriam estar cadastrados na Estratégia
Saúde da Família, vinculado a Unidade de Saúde da Família (USF-Rocas).
Foram excluídos aqueles que não completaram todas as fases da pesquisa,
desistindo da sua participação na ocasião da entrevista e aqueles que
obtiveram pontuação insuficiente no teste de rastreio cognitivo.
4.5. Procedimento para coleta de dados
A coleta de dados foi realizada no domicílio dos idosos, por
entrevistadores previamente treinados.
4.5.1. Treinamento dos entrevistadores:
Os entrevistadores eram fisioterapeutas e foram submetidos a um
treinamento prévio quanto aos instrumentos da pesquisa, seguindo uma
padronização dos protocolos, através de vídeos, além de ter sido realizado um
estudo piloto para calibração e validação dos instrumentos.
4.5.2 Estudo Piloto:
Um estudo piloto foi realizado no ano de 2009, nos meses de outubro a
dezembro, com o objetivo de testar os questionários e instrumentos a serem
utilizados, e verificar a confiabilidade das medidas[28] .

19
4.5.3. Recrutamento da amostra:
Para recrutamento da amostra os pesquisadores receberam uma lista com
o nome de todos os idosos residentes no bairro das Rocas e que estavam
cadastrados na Unidade Saúde da Família Rocas, com idade a partir de 65
anos de ambos os sexos e que não estavam restritos ao leito, ficando nosso
universo restrito a 547 idosos.
Utilizando os dados da distribuição etária da população, foi feita a
distribuição da amostra proporcional para cada faixa etária (65-69 anos; 70-74
anos; 75-79 anos; 80 anos ou mais).
Os participantes foram contatados pelos entrevistadores em seus
domicílios. Nesse momento, foram explicados todos os procedimentos da
pesquisa, bem como os seus objetivos. Aqueles que aceitaram participar do
estudo e estavam de acordo com os critérios de inclusão propostos assinaram
um Termo de Consentimento Livre e Esclarecido (Anexo 1).
4.5.4. Coleta de Dados:
A coleta de dados constituiu-se da entrevista, realizada no domicílio do
participante, onde o mesmo respondeu ao questionário (ANEXO 2). Foram
também feitas as medidas antropométricas, e o SPPB (Short Physical
Performance Batery).

20
4.6. Variáveis do estudo
4.6.1. Variáveis independentes
Quadro 02: Quadro das Variáveis independentes
Nome Descrição Tipo
Idade Idade do idoso em anos Quantitativa
contínua
Sexo Masculino e feminino Categórica
nominal
Situação Socioeconômica
Escolaridade
Não alfabetizado; ensino fundamental
incompleto; ensino fundamental
completo; ensino médio incompleto;
ensino médio completo; ensino
superior incompleto; ensino superior
completo
Categórica
ordinal
Renda Ganho mensal de acordo com a
moeda local (em Real)
Quantitativa
contínua
História
Profissional
Profissão desempenhada a maior
parte da vida
Categórica
nominal
Situação Familiar
Estado civil Solteiro, Casado, Viúvo,
separado/divorciado, Religioso
Categórica
Nominal
Número de
pessoas que
convive
Número de pessoas que convivem
com o idoso
Quantitativa
ordinal
Relação
Familiar
Tipo de relação familiar das pessoas
que convivem com os idosos
Categórica
nominal
Hábitos de Vida
Alcoolismo Hábito etilista: bebe, nunca bebeu Categórica
nominal
Tabagismo Habitos tabagistas: fuma, já fumou,
não fuma
Categórica
nominal
Atividade física Prática de atividade física Categórica
nominal
Condições de Saúde
Doenças
crônicas
Presença de doenças crônicas:
0 a 1; 2 ou mais
Categórica
ordinal
Auto-relato de
saúde
Excelente; muito boa; boa; mais ou
menos; ruim
Categórica
ordinal
Sintomas Avaliado pela CES-D Categórica

21
Depressivos >16: com sintomas depressivos
<16: sem sintomas depressivos
ordinal
Declínio
Cognitivo
Medido pela PCL (Prova Cognitiva de
Leganes)
Categórica
ordinal
4.6.2. Variáveis Dependentes
Quadro 3: Quadro da Variáveis Dependentes
Nome Descrição Tipo
Desempenho Físico
Desempenho
dos membros
inferiores
(SPPB)
Soma dos escores de:
Equilíbrio em pé (0 - 4)
Velocidade da marcha (0 – 4)
Levantar/sentar da cadeira (0 – 4)
Quantitativa
discreta
4.7. Instrumentos Utilizados – Questionários e Exames
Desempenho Físico:
Short Physical Performance Batery (SPPB): instrumento utilizado para medir o
desempenho funcional desenvolvido por Guralnik et al, 1994[13]. Inclui três
testes relacionados à função dos membros inferiores: equilíbrio, marcha e
sentar/levantar da cadeira. Cada teste tem pontuação de 0 a 4, onde zero
representa o pior desempenho. O teste de equilíbrio é composto por três
tarefas hierárquicas: a posição dos pés lado a lado, a posição semi-tandem
(calcanhar de um pé ao lado do hálux do outro pé) e tandem (calcanhar de um
pé a frente do hálux do outro pé). O teste da marcha constitui uma caminha na
velocidade habitual por um percurso de 3 ou 4 metros onde é registrado o
tempo de execução. O teste é repetido duas vezes onde o menor tempo é
considerado para pontuação. O teste levantar da cadeira constitui uma medida
indireta da força dos membros inferiores, onde é solicitado ao participante
levantar e sentar da cadeira cinco vezes consecutivas, com os braços cruzados

22
sobre o tronco, o mais rápido que ele for capaz de executar. O escore total do
teste varia de 0 a 12 pontos, onde zero representa o pior desempenho e 12, o
melhor.
Sintomas Depressivos:
Sintomas Depressivos: avaliado pela escala de pressão do Center for
Epidemiological Studies (CES-D). Essa escala é utilizada para o rastreio dos
sintomas depressivos e foi validada para a população brasileira por Batistone et
al em 2007[29], composta por 20 itens sobre humor, sintomas somáticos,
interações com os outros e funcionamento motor. Estes itens comportam a
avaliação da frequência de sintomas depressivos vividos na semana anterior a
entrevista. As respostas são pontuadas de acordo com uma ordem de
freqüência de sintomas (0=nunca ou raramente, 1=às vezes, 2=frequentemente
e 3=maioria das vezes ou sempre), e o escore final varia de 0 a 60 pontos.
Quanto maior a pontuação do indivíduo mais sintomas depressivos ele
apresenta.
Declínio Cognitivo:
Medido através da Prova Cognitiva de Leganés (PCL). A Prova Cognitiva
de Leganés é um teste de rastreio cognitivo desenvolvido em por Zunzunegui
et al 2000[30], na cidade de Leganés, na Espanha. O teste possui 32 questões,
agrupadas em 07 categorias: orientação temporal (3 pontos); orientação
espacial (2 pontos); informações pessoais (3 pontos); teste de nomeação (6
pontos); memória imediata (6 pontos); memória tardia (6 pontos); memória
lógica (3 pontos). Pontuações ≤ 22 foram considerados com déficit cognitivo.

23
4.8 Aspectos éticos da pesquisa
Este estudo foi submetido ao Comitê de Ética em Pesquisa da
Universidade Federal do Rio Grande do Norte (UFRN) como parte do estudo
“Carga alostática, Fragilidade e Funcionalidade em idosos”, obtendo o parecer
CEP/HUOL 481/10 de acordo com a resolução 196/96 do Conselho Nacional
de Saúde.(Anexo 03)

24
5. RESULTADOS
Os resultados e discussão do presente estudo estão apresentados no
formato de artigo, contando a colaboração dos professores Ricardo Oliveira
Guerra e Álvaro Campos Cavalcanti Maciel, e de alunos de pós-graduação em
Fisioterapia e Ciências da Saúde da Universidade Federal do Rio Grande do
Norte.
O artigo foi escrito na língua inglesa, e submetido à revista Archives of
Gerontology and Geriatrics tendo como título: DEPRESSIVE SYMPTOMS AND
FUNCTIONAL DECLINE IN AN ELDERLY SAMPLE OF URBAN CENTER IN
NORTHEASTERN BRAZIL. Este manuscrito apresenta os principais resultados
e análise dos dados do projeto de dissertação.

25
Artigo
DEPRESSIVE SYMPTOMS AND FUNCTIONAL DECLINE IN AN ELDERLY
SAMPLE OF URBAN CENTER IN NORTHEASTERN BRAZIL.
Cristiano dos Santos Gomes1 Álvaro Cavalcante Maciel2 Aline do Nascimento Falcão
Freire3 Mayle de Andrade Moreira4 Marília de Oliveira Ribeiro2 Ricardo Oliveira
Guerra5
1- Physiotherapist, Master of Health Sciences, Universidade Federal do Rio Grande
do Norte, Brazil.
2- Adjunct Profesor, Department of Physiotherapy, Universidade Federal do Rio
Grande do Norte, Brazil.
3- Physiotherapist, Department of Physiotherapy, Universidade Federal do Rio
Grande do Norte, Brazil.
4- Physiotherapist, Master of Physiotherapy, Universidade Federal do Rio Grande do
Norte, Brazil.
5- Associate Profesor, Department of Physiotherapy, Universidade Federal do Rio
Grande do Norte, Brazil.

26
ABSTRACT
Objective: To examine the association between depressive symptoms and functional
status in elderly people living in an urban center in northeastern Brazil. Methods: In
this cross-sectional, observational, analytic study, 313 community-dwelling elderly
(age ≥ 65 years) individuals of both sexes who resided in Natal, Rio Grande do
Norte, were evaluated. The Brazilian version of the Center for Epidemiologic Studies
Depression Scale was used to screen for depressive symptoms. Physical
performance was assessed using the Short Physical Performance Battery. A
multivariate linear regression model adjusted for clinical and socioeconomic variables
was used to analyze the association between depressive symptoms and functional
performance. Results: Our findings showed that the presence of depressive
symptoms influenced functional performance, even when analyses controlled for
variables such as age, sex, poor perceived health, cognitive status, and body mass
index. Conclusion: The results of this study reinforce the association between
depressive symptoms and functional performance in an elderly population in an
urban center in northeastern Brazil. These findings provide useful information for the
identification of potential targets for research and therapeutic interventions aimed at
preventing a decline in mobility in elderly individuals.
Key words: Depression; mobility; Functional Performance; elderly;

27
INTRODUCTION
Despite the difficulty of diagnosing depression in elderly individuals due to
coexisting age-related cognitive disorders[1], this condition is considered to be one of
the most prevalent psychiatric disorders in elderly populations[2]. Depressive
symptoms in elderly patients have been shown to affect many aspects of health,
such as cognitive function[3], inflammatory biomarkers[4], quality of life[5], and physical
health[6]. However, the greatest impact of depression in such patients is related to
functional disability, as this condition is associated with low levels of physical activity
that lead to deficits in mobility and physical performance[7-9]. Some authors have
explained this association through the involvement of behavioral and biological
mechanisms[10, 11], such as reduced motivation arising from depressive states that
may contribute to sedentary behavior[12]. Nevertheless, the mechanisms underlying
the causal relationship between depressive symptoms and functional decline in
elderly individuals are complex and involve neural, hormonal, and immunological
changes[13].
The decline in mobility is an important parameter in the assessment of initial
processes leading to disability in elderly individuals. Objective measures, such as the
short physical performance battery (SPPB) developed by Guralnik et al. [14], can
estimate the risk of disability in elderly community residents, thereby enabling the
design of effective strategies for the prevention of physical immobility in this
population.
Population studies in developed countries[9, 15-20] have revealed the importance
of the impact of depressive symptomatology on physical performance in older
people. In Brazil, where population aging has accelerated in recent decades, few
studies have examined depressive symptoms and functional status in elderly
populations [17–20]. Regional cultural diversity and variation in socioeconomic
conditions in Brazil may lead to differences in the effects of population aging on
mental and physical health. Many elderly individuals live under poor socioeconomic
conditions in mid-sized cities, such as most cities in northeastern Brazil. This study
aimed to determine if there is association between depressive symptoms and
functional status in elderly people living in an urban center in northeastern Brazil.
Because various socioeconomic and cultural factors determine the presence of
depressive symptoms, we hypothesized that depressive states in elderly people

28
living in regions with highly contrasting social conditions would influence functional
performance.
SUBJECTS AND METHODS
In this observational, analytical, cross-sectional study, 313 elderly (age ≥ 65
years) Brazilians of both sexes who lived in the community of Natal, Rio Grande do
Norte, were evaluated. The following inclusion criteria were adopted: Study
participants should be free of severe disability in basic activities of daily living,
defined as the self-reported inability to perform the following activities without help:
bathing, getting out of bed, eating, dressing, and/or using the bathroom. Also the
participants should be registered at the Family Health Strategy, linked to the Family
Health Unit. We excluded data from participants who did not complete all phases of
the research from analyses during the interview or those with poor cognitive
performance.
Sample size calculation was performed with consideration that the probability
of physical performance loss was two-fold higher among those with (vs. without)
depressive symptoms. The proportion of the population with depressive
symptomatology (B) was determined to be 0.33. Calculation allowed for type I (α =
0.05) and type II (β = 0.80) errors.
A pilot study was conducted to standardize, calibrate, and validate protocols
and tools to be used in this research[21]. Five previously trained professionals
evaluated subjects during home visits. All goals and procedures of the research were
explained during these visits, and eligible individuals who agreed to participate
signed informed consent forms.
This study was approved by the Ethics Committee of the Federal University of
Rio Grande do Norte as part of the study "Biomarkers of stress, function and frailty in
an elderly population" (CEP/HUOL 481/10), according to resolution 196/96 of the
National Health Council.

29
Measures
The assessment protocol consisted of self-reported questions about
socioeconomic characteristics, such as participants’ age, sex, income, and
educational level; lifestyle habits such as drinking, smoking, and physical activity; and
clinical characteristics such as cognitive function, depression, body mass index and
chronic conditions.
Cognitive decline was measured by the Prueba Cognitiva Leganés a cognitive
screening test developed by Zunzunegui et al.[22] and validated in Portuguese by
Caldas et al.[23]. This instrument contains 32 items grouped in seven categories:
temporal orientation (3 points), spatial orientation (2 points), personal information (3
points), naming test (6 points), immediate memory (6 points), delayed recall (6
points), and logical memory (3 points). Scores less than 22 points reveal cognitive
decline.
Performance was measured using the SPPB, which was developed by
Guralnik et al. in 1994[14] and adapted for Brazilian cultural settings by Nakano in
2007[24]. The SPPB consists of a series of tests that measure balance, gait speed,
and lower limb strength. Each domain has range 0-4 points, which can total 12
points, the more points the better the functional performance.
The Brazilian version of the Center for Epidemiologic Studies Depression
Scale (CES-D)[25] was used to screen depressive symptoms. This 20-item instrument
solicits information about respondents’ mood, somatic symptoms, interactions with
others, and motor function. Responses to items are structured by the frequency with
which the respondent experienced depressive symptoms in the week prior to the
interview (0 = never or rarely, 1 = sometimes, 2 = often, 3 = most of the time or
always), with final scores ranging from 0 to 60 points[12]. The cutoff score of ≥16,
originally proposed by Radloff[26], was used to indicate the presence of depressive
symptoms.
Statistical Analysis
Data were analyzed using SPSS software (version 20.0; SPSS Inc., Chicago,
IL, USA) with a significance level of 5% (α = 0.05). First, the Kolmogorov-Smirnov
test was used to verify the normality of the data. Descriptive statistics (means,
standard deviations, absolute and relative frequencies) were calculated. The

30
independent samples t-test (a parametric test used in case of Gaussian distribution)
and chi-squared (a non- parametric test used in case of non-Gaussian distribution)
test were used to compare measures between men and women. Associations
between depression and functional performance were examined using the Pearson
correlation coefficient. The Mann–Whitney test was used to compare mean functional
performance in individuals with and without depressive symptoms, once SPPB data
presented non-Gaussean distribution. Linear regression analysis was performed to
examine the effects of multiple factors on physical performance, using three models.
The model 01 included only the CES-D, in the model 2 sociodemographic variables
as sex and age we included, and in the model 3, the variables PCL, self-reported
health and Body mass index were considered.
RESULTS
We evaluated 313 elderly individuals [210 (67%) women, 103 (33%) men]. All
individuals were included. Table 1 shows the main clinical and socioeconomic
characteristics of study participants. Most (52.4%) women were widowed or
separated, whereas the majority (77.7%) of men was married. Men had a higher
mean educational level (years of education) than did women (p = 0.013). Most
(74.3%) participants reported negative perceptions of their health status and 61.3%
reported having two or more chronic conditions.
The mean cognitive performance score was 27.07 ± 3.80 for the total sample,
and this score did not differ significantly between men and women (p = 0.813). The
prevalence of depressive symptoms was 39.6%; 9.26% of participants reporting
depressive symptoms were men and 30.33% were women.
Negative association was observed between depressive symptomatology and
functional performance (p < 0,001). Individuals who reported depressive symptoms
had worse physical performance scores than those who did not (p = 0.001). Lower
limb strength was the only performance parameter that was not significantly lower in
men with (vs. without) depressive symptoms (p = 0.402). Women had lower mean
scores than men for all components of the SPPB (Table 2).
Table 3 shows the results of multiple linear regression analysis. We have built
three explanation models, which the final model with social and anthropometrics

31
variables shows best values (R2= 0.34; p <0.001) to explain the effect on functional
performance adjusted by depressive symptoms.
DISCUSSION
Outcomes from distinct studies have revealed associations between
depressive states and declining physical function in older adults, and these
relationships are reciprocal and mutually reinforcing over time[13, 15, 26, 27]. The
mechanisms and factors underlying these interactions remain unclear, so depressive
symptoms that often accompany clinical conditions such as Diabetes, Heart
diseases, obesity, neurological disorders, can influence the reduction of mobility.18,28
Studies using a variety of methodologies have found that the incidence of
depressive disorders is high in elderly community-dwelling Brazilians[17, 29,30]. Using a
CES-D cutoff score of 16 points, we determined that 39.6% of our sample had
depressive symptoms. The sociodemographic characteristics of the study population
may have contributed to this result. Socioeconomic conditions and health status in
Latin America aging people, mainly accounted for gender differences are associated
with the prevalence of depression. Additionally, poor health and hunger during
childhood, as well as illiteracy or lack of education are related with depression in both
men and women[31]. Results from the SABE study using variables from life course
approach, revealed a stronger association between depression and lower extremity
limitations was found in Latin America elders[32]. Previous findings from our research
group has previously established associations of sociodemographic factors related to
mobility and functional capacity with depressive symptoms and poor perception of
health status in the elderly population of northeastern Brazil [19, 33-35]. Other factors are
related to the presence of depressive symptoms and the social environment in which
older people live, as well as the participation in social support networks, have been
identified as determinants of physical activity levels and physical mobility[11,36].
Our findings revealed that the presence of depressive symptoms influenced
functional performance in elderly community residents in an urban center in
northeastern Brazil, reinforcing the findings of studies conducted in southeastern
Brazil that have demonstrated an association between depressive symptoms and
disability in instrumental activities of daily living (IADL), and the association between
depressive symptoms and worse outcomes of gait speed measured by test Get Up

32
and Go, even in the presence of Socioeconomic and cultural differences between
these regions.[37-39] This effect was observed in an explanatory model adjusted for
sociodemographic factors, such as age and cognitive status, and anthropometric
measures, such as body mass index. These data allow us to infer that objective
measures of mobility (SPPB) are partly influenced by depression, i.e., elderly
Brazilians living in socially unfavorable conditions may experience a decline in
mobility due to circumstances arising from emotional disturbance. Potential
explanations for this relationship are related to various aspects of personal motivation
and levels of ability and functional performance, which represent an initial step in the
process of disability in elderly individuals.
Gender differences about functional limitations are more frequently observed
in older women and the causes of this statement can be explained by diverse
approaches. Decline in functional performance in aging may originally related to
biologic variables as muscle fiber type-specific characteristics, circulating hormone
concentrations, skeletal muscle mass and strength, and it is different between men
and women[40]. Factors intrinsic to the aging process, such as sarcopenia and gait
disturbances, also have strong effects on the development of disability and declining
mobility in elderly people[39]. Functional loss can be assessed using objective
measures of walking speed, lower-limb strength, and balance[42,43]. These
parameters are included in SPPB, and it presents a good reliability and validity in
different aging populations, and it is easy to understand and to using[44]. Within of
SPPB parameters, walking speed is a particularly good predictor of functional
disability[42]. Deficits in gait speed may be due to the age-related development of
sarcopenia, which predominantly affects the lower extremities, causing changes in
muscle activity patterns and reducing muscle strength and power. These effects on
gait are most pronounced in women[43, 45]. In our sample, we observed a lower
average gait speed in subjects with depressive symptoms, especially in women.
However, in contrast to these findings in the literature, a recent longitudinal study
reveals that gait speed predicts depressive symptoms in men[46].
Several limitations of this study should be considered. The cross-sectional
nature of our study prevented us from establishing causality between variables.
Moreover, individuals with temporary or intermittent depressive symptomatology,
rather than depressive disorders, were likely included in our study sample. These
individuals may have been evaluated at a time when their reactions to stressful

33
events led to a temporary increase in depressive symptoms. Nevertheless, the
stronger relationship between depression and functional performance adjusted by
variables such as perceived health status, suggests that social determinants can be
involved as predictors of mental and physical health in Brazilians elders.
CONCLUSION
The results of this study reinforce the association between depressive
symptoms and functional performance in an elderly population in a large urban
center with unfavorable socioeconomic aspects. Our findings provide useful
information for the identification of potential targets for research and therapeutic
interventions aimed at preventing a decline in mobility in elderly individuals.

34
Table 1. Sociodemographic and clinical characteristics of the sample
Variable Total (n = 313) Men (n = 103) n (%)
Women (n = 210) p
Marital status <0.001 Single 49 (15.7) 11 (10.7) 38 (18.1) Married 142 (45.4) 80 (77.7) 62 (29.5) Widowed/divorced 122 (39.0) 12 (11.6) 110 (52.4)
Monthly income (basic wage) 0.013 <1 19 (6.1) 1 (1.0) 18 (8.6) 1–3 257 (82.1) 83 (80.6) 174 (82.9) 4–5 26 (8.3) 13 (12.6) 13 (6.2) >5 11 (3.5) 6 (5.8) 5 (2.4)
Self-reported health 0.003 Excellent/very good 20 (6.4) 13 (12.6) 7 (3.3) Good 63 (20.1) 27 (26.6) 36 (17.1) almost bad/bad 230(73.4) 63 (61.2) 167 (79.5)
Number of chronic conditions 0.077 0 44 (14.1) 20 (19.4) 24 (11.4) 1 77 (24.6) 28 (27.2) 49 (23.3) ≥2 192 (61.3) 55 (53.4) 137 (65.2)
Comorbidities Hypertension 205 (65.5) 62 (60.2) 163 (68.1) 0.167 Diabetes 91 (29.1) 29 (28.2) 62 (29.5) 0.802 Arthritis/osteoarthritis 146 (46.6) 32 (32.1) 114 (54.3) <0.001
Depression 43 (23.4) 6 (5.8) 37 (17.6) 0.004 Mean ± SD Age 74.44±0.68 75.33±0.64 74.74±0.48 0.914 Years of education 4.81 ± 3.89 5.59 ± 4.46 4.43 ± 3.52 0.013 Total SPPB score 8.32 ± 2.70 9.33 ± 2.32 7.82 ±2.74) <0.001 Total CES-D score 14.34 ± 11.35 12.16 ± 9.55 16.31 ±11.92) <0.001 Total PCL score 27.07 ± 3.80 27.14 ± 3.78 27.03 ±3.81) 0.813 BMI 26.66 ± 4.67 25.80 ± 3.68 27.52 ±5.76) <0.001
SD, standard deviation; SPPB, Short Physical Performance Battery; CES-D, Center for Epidemiologic Studies Depression Scale; PCL, Prueba Cognitiva Leganés; BMI, Body mass index.

35
Table 2 .Short Physical Performance Battery scores among subjects with and without depressive symptoms
SPPB variable (mean ± SD)
Balance Gait speed Strength MMII Total score
Depressive symptoms
Total Men Women Total Men Women Total Men Women Total Men Women
No 3.53 ± 0.89* 3.79 ± 0.52* 3.35 ± 1.04* 3.03 ± 0.97* 3.32 ± 0.90* 2.84 ± 0.97* 2.32 ± 1.22* 2.64 ± 1.09 2.12 ± 1.27* 8.92 ± 2.40* 9.78 ± 1.83* 8.35 ± 2.56*
Yes 3.02 ± 1.22 3.17 ± 1.10 2.97 ± 1.26 2.59 ± 1.02 2.86 ± 1.12 2.51 ± 0.98 1.79 ± 1.35 2.17 ± 1.60 1.67 ± 1.25 7.42 ± 2.90 8.20 ± 3.01 7.18 ± 2.84
SPPB, Short Physical Performance Battery; SD, standard deviation; MMII, lower limbs . Presence of depressive symptoms was
determined using the Center for Epidemiologic Studies Depression Scale. *p ≤ 0.05.

36
Table 3. Results of linear regression analysis, with SPPB as dependent
variable.
Variable Model 1 Model 2 Model 3
β p β p β P
CES-D -0.244 <0.001 -0.186 <0.001 -0.102 0.044
Age -0.408 <0.001 -0.379 <0.001
Sex+ -0.197 <0.001 -0.143 0.003
Self-reported health++ 0.242 <0.001
PCL 0.117 0.015
Body mass índex
-0.108 0.025
R2 0.059 0.271 0.348
Constant 9,1 22,7 23,4
F 19,2 37,6 26,74
CES-D, Center for Epidemiological Studies Depression Scale; PCL, Prueba Cognitiva de Leganés. + Sex (0-man; 1- woman) ++ Self-reported health (0-bad;1-more or less; 2- good)
REFERENCES
37
1. Ávila, R. and C.M. de Campos Bottino, Atualização sobre alterações cognitivas em idosos com síndrome depressiva Rev Bras Psiquiatr, 2006. 28(4): p. 316-20.
2. Oliveira, D., L. Gomes, and R.F. Oliveira, Prevalência de depressão em idosos que frequentam centros de convivência. Rev Saúde Pública, 2006. 40(4): p. 734-6.
3. Sikkes, S.A., et al., Do instrumental activities of daily living predict dementia at 1- and 2-year follow-up? Findings from the Development of Screening guidelines and diagnostic Criteria for Predementia Alzheimer's disease study. J Am Geriatr Soc, 2011. 59(12): p. 2273-81.
4. Looper, K., et al., History of depressive episodes as a risk factor for illness severity in early inflammatory arthritis. J Psychosom Res, 2011. 71(1): p. 28-31.
5. Duivis, H.E., et al., Depressive symptoms, health behaviors, and subsequent inflammation in patients with coronary heart disease: prospective findings from the heart and soul study. Am J Psychiatry, 2011. 168(9): p. 913-20.
6. Chen, C.M., et al., Trajectories of depression and their relationship with health status and social service use. Arch Gerontol Geriatr, 2011. 53(2): p. e118-24.
7. Everson-Rose, S.A., et al., Do depressive symptoms predict declines in physical performance in an elderly, biracial population? Psychosom Med, 2005. 67(4): p. 609-15.
8. Hassmen, P., N. Koivula, and A. Uutela, Physical exercise and psychological well-being: a population study in Finland. Prev Med, 2000. 30(1): p. 17-25.
9. Lindwall, M., et al., Depression and exercise in elderly men and women: findings from the Swedish national study on aging and care. J Aging Phys Act, 2007. 15(1): p. 41-55.
10. Cronin-Stubbs, D., et al., Six-year effect of depressive symptoms on the course of physical disability in community-living older adults. Arch Intern Med, 2000. 160(20): p. 3074-80.
11. Ostir, G.V., et al., The Effect of Depressive Symptoms on the Association Between Functional Status and Social Participation. Soc Indic Res, 2007. 80(2): p. 379-392.
12. Matthews, M.M., et al., Depressive symptoms and physical performance in the lifestyle interventions and independence for elders pilot study. J Am Geriatr Soc, 2011. 59(3): p. 495-500.
13. Barry, L.C., et al., Longitudinal association between depressive symptoms and disability burden among older persons. J Gerontol A Biol Sci Med Sci, 2009. 64(12): p. 1325-32.
14. Guralnik, J.M., et al., A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. Journal of gerontology, 1994. 49(2): p. M85-M94.
15. Bruce, M.L., et al., The impact of depressive symptomatology on physical disability: MacArthur Studies of Successful Aging. Am J Public Health, 1994. 84(11): p. 1796-9.
16. Katon, W. and P. Ciechanowski, Impact of major depression on chronic medical illness. J Psychosom Res, 2002. 53(4): p. 859-63.
17. Barcelos-Ferreira, R., et al., Clinically significant depressive symptoms and associated factors in community elderly subjects from Sao Paulo, Brazil. Am J Geriatr Psychiatry, 2009. 17(7): p. 582-90.
18. Hoffmann, E.J., et al., Sintomas depressivos e fatores associados entre idosos residentes em uma comunidade no norte de Minas Gerais, Brasil. J Bras Psiquiatr, 2010. 59(3): p. 190-7.
19. Maciel, A.C.C. and R.O. Guerra, Prevalência e fatores associados à sintomatologia depressiva em idosos residentes no Nordeste do Brasil. J Bras Psiquiatr, 2006. 55(1): p. 26-33.
20. Reichert, C.L., et al., Physical activity and depressive symptoms in community-dwelling elders from southern Brazil. Rev Bras Psiquiatr, 2011. 33(2): p. 165-70.

38
21. Freire, A.N., et al., Validity and reliability of the short physical performance battery in two diverse older adult populations in Quebec and Brazil. Journal of aging and health, 2012. 24(5): p. 863-878.
22. Zunzunegui, M.V., et al., Development of simple cognitive function measures in a community dwelling population of elderly in Spain. Int J Geriatr Psychiatry, 2000. 15(2): p. 130-40.
23. Caldas, V.V., et al., Translation, cultural adaptation and psychometric evaluation of the Leganes cognitive test in a low educated elderly Brazilian population. Arq Neuropsiquiatr, 2012. 70(1): p. 22-7.
24. Nakano, M.M., Versão brasileira da Short Physical Performance Battery SPPB: adaptação cultural e estudo da confiabilidade. 2007, Universidade Estadual de Campinas.
25. Batistoni, S.S., A.L. Neri, and A.P. Cupertino, [Validity of the Center for Epidemiological Studies Depression Scale among Brazilian elderly]. Rev Saude Publica, 2007. 41(4): p. 598-605.
26. Radloff, L.S., The CES-D scale A self-report depression scale for research in the general population. Applied psychological measurement, 1977. 1(3): p. 385-401.
27. Gayman, M.D., R.J. Turner, and M. Cui, Physical limitations and depressive symptoms: exploring the nature of the association. J Gerontol B Psychol Sci Soc Sci, 2008. 63(4): p. S219-S228.
28. Suassuna, P.D.; Veras, R.P.; Lourenço, R.A.; Caldas, C.P. Factors associated with depressive symptoms in elderly assisted in a Geriatric outpatient clinic Rev. Bras. Geriatr. Gerontol., Rio de Janeiro, 2012; 15(4):643-650
29. Costa, E., et al., Prevalence of International Classification of Diseases, 10th Revision common mental disorders in the elderly in a Brazilian community: The Bambui Health Ageing Study. Am J Geriatr Psychiatry, 2007. 15(1): p. 17-27.
30. Ormel, J., et al., Temporal and reciprocal relationship between IADL/ADL disability and depressive symptoms in late life. J Gerontol B Psychol Sci Soc Sci, 2002. 57(4): p. P338-47.
31. Alvarado, B.E., et al., Social and gender inequalities in depressive symptoms among urban older adults of latin america and the Caribbean. J Gerontol B Psychol Sci Soc Sci, 2007. 62(4): p. S226-36.
32. Alvarado, B.E., R.O. Guerra, and M.V. Zunzunegui, Gender differences in lower extremity function in Latin American elders: seeking explanations from a life-course perspective. J Aging Health, 2007. 19(6): p. 1004-24.
33. Abate, M., et al., Frailty in the elderly: the physical dimension. Eura Medicophys, 2007. 43(3): p. 407-15.
34. Gazalle, F.K., et al., Sintomas depressivos e fatores associados em população idosa no Sul do Brasil. Rev Saúde Pública, 2004. 38(3): p. 365-71.
35. Maciel, A.C.C.G., R. O. Rev. bras. fisioter. Vol. 9, No. 1 (2005), 17-23, Fatores Associados à Alteração da Mobilidade em Idosos Residentes na Comunidade. Rev. bras. fisiotera. , 2005. 9(1).
36. Maciel, A.C.C.G., R.O., Influência dos fatores biopsicossociais sobre a capacidade funcional de idosos. Rev Bras Epidemiol, 2007. 10(2): p. 178-89.

39
37. ARTERBURN D, WESTBROOK EO, LUDMAN EJ, OPERSKALSKI B, LINDE JA, ROHDE P, JEFFERY RW, SIMON GE.RELATIONSHIP BETWEEN OBESITY, DEPRESSION, AND DISABILITY IN MIDDLE-AGED WOMEN. JUL;6(3):E197-E206. EPUB 2012 MAR 3.
38. TENG, C.T.; HUMES, E.C.; DEMETRIO, F.N. DEPRESSION AND MEDICAL COMORBIDITY REV. PSIQ.CLÍN. 32 (3); 149-159, 2005.
39. SANTOS KLEYTON T., FERNANDES MARCOS H., REIS LUCIANA A., COQUEIRO RAILDO S.,
ROCHA SAULO V.. DEPRESSIVE SYMPTOMS AND MOTOR PERFORMANCE IN THE
ELDERLY: A POPULATION BASED STUDY. REV. BRAS. FISIOTER. AUG; 16( 4 ): 295-300.
40. Verdijk, L.B., et al., Characteristics of muscle fiber type are predictive of skeletal muscle mass and strength in elderly men. J Am Geriatr Soc, 2010. 58(11): p. 2069-75.
41. Spolito, G., et al., Relações entre o bem-estar subjetivo e a funcionalidade em idosos em seguimento ambulatorial. Rev Bras Fisioter, 2010. 14(1): p. 81-9.
42. Guralnik, J.M., et al., Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci, 2000. 55(4): p. M221-31.
43. Lang, T., et al., Sarcopenia: etiology, clinical consequences, intervention, and assessment. Osteoporos Int, 2009. 21(4): p. 543-59.
44. Freire, A.N., et al., Validity and reliability of the short physical performance battery in two diverse older adult populations in Quebec and Brazil. J Aging Health, 2012. 24(5): p. 863-78.
45. Graf, A., et al., The effect of walking speed on lower-extremity joint powers among elderly adults who exhibit low physical performance. Arch Phys Med Rehabil, 2005. 86(11): p. 2177-83.
46. Sanders, J.B., et al., Do depressive symptoms and gait speed impairment predict each other's incidence? A 16-year prospective study in the community. J Am Geriatr Soc, 2012. 60(9): p. 1673-80.

40
6. COMENTÁRIOS, CRÍTICAS E SUGESTÕES
A presente dissertação permaneceu fiel à proposta inicial avaliando as
relações existentes entre os sintomas depressivos e a mobilidade de idosos
comunitários de um centro urbano do nordeste brasileiro. Apesar do caráter
transversal desse estudo não permitir o estabelecimento de relações de
causalidade, o conhecimento das associações entre sintomatologia depressiva
e desempenho funcional em populações idosas brasileiras é fundamental para
o planejamento de estratégias eficazes de prevenção e tratamento, seja da
depressão como da autonomia funcional.
Essa pesquisa contribui de forma significativa para a o entendimento de
nosso tema principal e permite a diversos profissionais de saúde, de áreas
diferentes, a exemplo de médicos, enfermeiros, educadores físicos e
fisioterapeutas, repensarem suas práticas e adotarem novos métodos a fim de
prover qualidade ao processo de envelhecimento experimentado na população
brasileira.
A experiência vivenciada no decorrer destes dois anos de execução do
projeto permitiu a evolução no domínio das ferramentas utilizadas na
metodologia cientifica, conhecimento este imprescindível para minha formação,
enquanto pesquisador, e futura carreira docente que pretendo trilhar. Os
créditos oferecidos pelo programa associados a estudos independentes
propiciaram um aprofundamento no método e conhecimento científico,
ressaltando a relevância da prática baseada em evidências. A participação no
Grupo de Estudos em Epidemiologia e Fisioterapia Geriátrica da UFRN
(GEEFG-UFRN) e a atuação no programa de docência assistida despertaram
ainda mais o interesse pela busca do conhecimento e a importância de sua
transmissão aos profissionais em formação nos cursos de graduação em
Fisioterapia e áreas afins.
Durante o curso de mestrado foi produzido um artigo científico, um
estudo epidemiológico submetido à Revista Archives of Geriatrics and
Gerontology (B1). Além disso os seguintes trabalhos foram apresentados em
congressos:

41
“ DEPRESSÃO E FUNCIONALIDADE EM IDOSOS RESIDENTES NA
CIDADE DE SANTA CRUZ – RN” XVIII congresso brasileiro de
geriatria e gerontologia realizado de 22 a 25 de maio de 2012 no Rio de
Janeiro.
“ENVELHECIMENTO E DESEMPENHO FUNCIONAL EM IDOSOS
RESIDENTES NA CIDADE DE NATAL/RN.” III Congresso internacional
de envelhecimento humano realizado de 13 a 15 de junho de 2013 em
Campina Grande –PB.
“PERFIL DE FRAGILIDADE DE IDOSOS DE UM CENTRO URBANO
DO NORDESTE BRASILEIRO” III Congresso internacional de
envelhecimento humano realizado de 13 a 15 de junho de 2013 em
Campina Grande –PB.
“AVALIAÇÃO DA CAPACIDADE FÍSICA ATRAVÉS DA SHORT
PHYSICAL PERFORMANCE BATTERY EM IDOSOS RESIDENTES NA
COMUNIDADE DO MUNICÍPIO DE NATAL-RN” III Congresso
internacional de envelhecimento humano realizado de 13 a 15 de junho
de 2013 em Campina Grande –PB.
“RELAÇÃO ENTRE A PERCEPÇÃO SUBJETIVA DE SAÚDE E A
SINTOMATOLOGIA DEPRESSIVA EM IDOSOS RESIDENTES NA
COMUNIDADE DO MUNICÍPIO DE NATAL-RN” III Congresso
internacional de envelhecimento humano realizado de 13 a 15 de junho
de 2013 em Campina Grande –PB.
“ A VELOCIDADE DA MARCHA PODE IDENTIFICAR IDOSOS COM
MEDO DE CAIR?” III Congresso internacional de envelhecimento
humano realizado de 13 a 15 de junho de 2013 em Campina Grande –
PB.

42
7. REFERÊNCIAS 1. Santos-Filho, S.D., et al., O interesse científico no estudo do
envelhecimento e prevenção em ciências biomédicas. Revista Brasileira
de Ciências do Envelhecimento Humano, 2006. 3(2).
2. Carvalho, J.A.M.d. and L.L. Rodríguez-Wong, A transição da estrutura
etária da população brasileira na primeira metade do século XXI; The
changing age distribution of the Brazilian population in the first half of the
21st century. Cad. saúde pública, 2008. 24(3): p. 597-605.
3. Veras, R., Envelhecimento populacional contemporâneo: demandas,
desafios e inovações. Rev Saúde Pública, 2009. 43(3): p. 548-54.
4. Veras, R., Fórum. Envelhecimento populacional e as informações de
saúde do PNAD: demandas e desafios contemporâneos. Introdução;
Forum. Population aging and health information from the National
Household Sample Survey: contemporary demands and challenges.
Introduction. Cad. saúde pública, 2007. 23(10): p. 2463-2466.
5. Nasri, F., O envelhecimento populacional no Brasil; The aging population
in Brazil. Einstein (São Paulo), 2008. 6(supl. 1): p. S4-S6.
6. Kraaij, V., E. Arensman, and P. Spinhoven, Negative Life Events and
Depression in Elderly Persons A Meta-Analysis. The Journals of
Gerontology Series B: Psychological Sciences and Social Sciences,
2002. 57(1): p. P87-P94.
7. de Oliveira Santos, M.I.P. and R.H. Griep, Capacidade funcional de
idosos atendidos em um programa do SUS em Belém (PA). 2013.
8. Paloma Andrade Pinheiro, T.D.E.-R.O.P., Raildo da Silva Coqueiro, and
A.R.B. Marcos Henrique Fernandes, MOTOR PERFORMANCE OF THE
ELDERLY IN NORTHEAST BRAZIL: DIFFERENCES WITH AGE AND
SEX. Rev Esc Enferm USP, 2013.
9. Topinkova, E., Aging, disability and frailty. Ann Nutr Metab, 2008. 52
Suppl 1: p. 6-11.
10. Ensrud, K.E., et al., A comparison of frailty indexes for the prediction of
falls, disability, fractures, and mortality in older men. J Am Geriatr Soc,
2009. 57(3): p. 492-8.

43
11. Dong, X., et al., Physical function decline and the risk of elder self-
neglect in a community-dwelling population. The Gerontologist, 2010.
50(3): p. 316-326.
12. Guralnik, J.M., et al., Lower extremity function and subsequent disability:
consistency across studies, predictive models, and value of gait speed
alone compared with the short physical performance battery. J Gerontol
A Biol Sci Med Sci, 2000. 55(4): p. M221-31.
13. Guralnik, J.M., et al., A short physical performance battery assessing
lower extremity function: association with self-reported disability and
prediction of mortality and nursing home admission. Journal of
gerontology, 1994. 49(2): p. M85-M94.
14. Ferrucci, L., et al., Characteristics of nondisabled older persons who
perform poorly in objective tests of lower extremity function. J Am Geriatr
Soc, 2000. 48(9): p. 1102-10.
15. Tolea, M.I., et al., Sex-specific correlates of walking speed in a wide age-
ranged population. J Gerontol B Psychol Sci Soc Sci, 2010. 65B(2): p.
174-84.
16. Lim, Y.-H., et al., Air Pollution and Symptoms of Depression in Elderly
Adults. Environmental Health Perspectives, 2012. 120(7): p. 1023.
17. Maglione, J.E., et al., Depressive Symptoms and Subjective and
Objective Sleep in Community‐Dwelling Older Women. Journal of the
American Geriatrics Society, 2012. 60(4): p. 635-643.
18. Ávila, R. and C.M. de Campos Bottino, Atualização sobre alterações
cognitivas em idosos com síndrome depressiva Rev Bras Psiquiatr,
2006. 28(4): p. 316-20.
19. Gazalle, F.K., et al., Sintomas depressivos e fatores associados em
população idosa no Sul do Brasil. Rev Saúde Pública, 2004. 38(3): p.
365-71.
20. Gumarães, J.M.N. and C.P. Caldas, A influência da atividade física nos
quadros depressivos de pessoas idosas: uma revisão sistemática. Rev.
bras. epidemiol, 2006. 9(4): p. 481-492.
21. Covinsky, K.E., et al., Depressive Symptoms in Middle Age and the
Development of Later‐Life Functional Limitations: The Long‐Term Effect
44
of Depressive Symptoms. Journal of the American Geriatrics Society,
2010. 58(3): p. 551-556.
22. Prina, A.M., et al., The association between depressive symptoms and
non-psychiatric hospitalisation in older adults. PloS one, 2012. 7(4): p.
e34821.
23. Ostir, G.V., et al., The Effect of Depressive Symptoms on the Association
Between Functional Status and Social Participation. Soc Indic Res, 2007.
80(2): p. 379-392.
24. Gomes, G.A.O., et al., Comparação entre idosos que sofreram quedas
segundo desempenho físico e número de ocorrências. Rev Bras Fisioter,
2009. 13(5): p. 430-7.
25. Cronin-Stubbs, D., et al., Six-year effect of depressive symptoms on the
course of physical disability in community-living older adults. Arch Intern
Med, 2000. 160(20): p. 3074-80.
26. Lewis, G. and R. Araya, Classification, disability and the public health
agenda. Br Med Bull, 2001. 57: p. 3-15.
27. Barry, L.C., et al., Longitudinal association between depressive
symptoms and disability burden among older persons. J Gerontol A Biol
Sci Med Sci, 2009. 64(12): p. 1325-32.
28. Freire, A.N., et al., Validity and reliability of the short physical
performance battery in two diverse older adult populations in Quebec
and Brazil. Journal of aging and health, 2012. 24(5): p. 863-878.
29. Batistoni, S.S., A.L. Neri, and A.P. Cupertino, [Validity of the Center for
Epidemiological Studies Depression Scale among Brazilian elderly]. Rev
Saude Publica, 2007. 41(4): p. 598-605.
30. Zunzunegui, M.V., et al., Development of simple cognitive function
measures in a community dwelling population of elderly in Spain. Int J
Geriatr Psychiatry, 2000. 15(2): p. 130-40.

45
ANEXOS
ANEXO 01
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
TÍTULO DA PEQUISA: CARGA ALOSTÁTICA, FRAGILIDADE E
FUNCIONALIDADE EM IDOSOS
INVESTIGADORES: Aline do Nascimento Falcão Freire
Prof Orientador Ricardo Oliveira Guerra
NOME DO PARTICIPANTE:
_______________________________________________________________
Este termo de consentimento livre e esclarecido poderá conter palavras que
você não entende. Peça a uma pessoa da equipe de estudo para explicar
qualquer palavra ou informação que você não tenha entendido claramente.
OBJETIVO DO ESTUDO
Você está sendo convidado a participar de um estudo de caráter
transversal. O objetivo desse estudo é analisar as relações associativas entre
carga alostática, através dos fatores sociais estressores e marcadores
biológicos do estresse, com a fragilidade e o estado funcional de populações
idosas residentes na comunidade.
DESENHO DO ESTUDO
A população selecionada para participar das atividades será composta
por idosos de ambos os sexos, com idade acima de 65 anos, residente na
comunidade na cidade de Natal/RN.
PROCEDIMENTOS
Se você concordar em participar do estudo, será submetido a uma
avaliação utilizando alguns questionários. Primeiramente, responderá ao
questionário contendo informações sobre o curso de vida, estado de saúde,

46
nível cognitivo, incapacidade funcional. Após, será dadas as orientações para a
coleta da saliva, urina e sangue a ser realizada nos dias consecutivos.
CUSTOS
Todos os serviços profissionais exigidos como parte deste estudo serão
gratuitos.
CONFIDENCIALIDADE
Sua identidade será preservada em todas as situações que envolvam
discussão, apresentação e/ou publicação dos resultados da pesquisa. Somente
suas iniciais identificarão as informações coletadas sobre você. Os registros
que identificam você e este termo de consentimento poderão ser inspecionados
pela Pró-Reitoria de Pesquisa e Pós-Graduação da UFRN, além do Comitê de
Ética em Pesquisa do Hospital Universitário Onofre Lopes. Não haverá
qualquer forma de gratificação pela participação no experimento e os
resultados obtidos a partir dele serão propriedade exclusiva dos pesquisadores,
podendo ser divulgados de quaisquer formas (escrita e oral), a critério dos
mesmos.
PARTICIPAÇÃO/RETIRADA VOLUNTÁRIA DO ESTUDO
Sua participação é voluntária. Você é livre para aceitar participar deste
estudo ou poderá retirar-se a qualquer momento.
QUEM CONTACTAR EM CASO DE DÚVIDA
Se você tiver alguma dúvida sobre este estudo ou algum problema
relacionado à pesquisa, deverá entrar em contato com a investigadora do
estudo, Aline do Nascimento Falcão Freire, rua dos Tororós, n 2310, Lagoa
Nova; telefone (84) 8804-5941; e-mail: [email protected].
Dúvidas a respeito da ética dessa pesquisa poderão ser questionadas
ao Comitê de Ética em Pesquisa do Hospital Universitário Onofre Lopes no
endereço Av. Nilo Peçanha nº 620, Petrópolis, Natal/RN, CEP: 59012-300,
telefone:3342-5003.
*Não assine nem date este formulário a menos que você tenha tido a
oportunidade de esclarecer suas dúvidas e tenha recebido respostas
satisfatórias a todas as suas perguntas.

47
CONSENTIMENTO INFORMADO
Li e entendi as informações acima. Perguntei e discuti os detalhes do estudo
com uma pessoa da equipe de pesquisa. Concordo em participar deste estudo
baseado nas informações fornecidas. Entendo que receberei uma cópia
assinada e datada deste termo de consentimento.
Participante da pesquisa:
Nome:_______________________________________________________
Data:____/____/____
____________________________________________________________
Assinatura
Pesquisador responsável:
Nome: Professor Doutor Ricardo Oliveira Guerra
Endereço: Centro de Ciências da Saúde – Departamento de Fisioterapia
Av. Senador Salgado Filho, 300, Campus Universitário, CEP: 59078-970, Natal-
RN, 2ª andar.
Telefone: 3342-2002.
E-mail: [email protected]
Assinatura
Comitê de Ética em Pesquisa do Hospital Universitário Onofre Lopes:

48
Av. Nilo Peçanha, nº 620, Petrópolis, CEP: 59012-300, Natal-RN, telefone:
3342-5003.
ANEXO 02
I) IDENTIFICAÇÃO ENTREVISTA I
ENTREVISTADOR
Identificação do Entrevistador (No.) Data da entrevista:
2 0
Ano Mês Dia
PARTICIPANTE
Identificação do participante(No.)
Lugar Rocas Santarém Soledade
ADMINISTRATIVO
(Não escrever nada no espaço sombreado;reservado ao verificador-coordenador
Entrevista completa 1 □ sim 2 □ não
Identificação do entrevistador (No.)
Código do questionário 1 □sim 2 □ não
Identificação do revisor (nº)
Data da realização da entrevista Hora que iniciou Hora que terminou
Ano Mês Dia H(24h) Min. H(24h) Min.
Assinou consentimento 1 □ sim 2 □ não

49
II) INFORMAÇÕES PESSOAIS
Identificação do participante (No.)
Conhecendo
Nome completo
Endereço completo
No. do telefone
Pessoa de contato
Relação com o participante
Nome completo
No. do telefone
III) Dados demográficos
1 Data de nascimento do participante
Ano Mês Dia
2 Idade do participante
3 Sexo do participante (Colocar sem perguntar)
1 □ Homem
2 □ Mulher
4 Qual é o seu estado civil? 1 Solteiro (a)
2 Casado ou vive com cônguje
3 Viúvo (a)
4 Separado/divorciado

50
5 Religioso
5 Quantos anos você vive em:
*Rocas ; *Santarém; *Soledade
Anos
IV) ESCOLARIDADE
1 Quantos anos você estudou?
2 Você sabe ler e escrever? 1 Não, nem sei ler nem escrver
2 Entendo o que leio mas não sei escrver
3 Sim, sei ler e escrever
3 Qual o seu nível de escolaridade? 1 0-4 anos
2 5-8 anos
3 1º grau incompleto
4 1ª grau completo
5 2º grau incompleto
6 2º grau completo
7 Nível superior
8 Pós-graduação
9 Não sei
V) RENDAS
1 Quais são suas rendas? 1 Aponsentadoria ou pensão
2 Ajuda de familiares em outro país
3 Ajuda de familiares aqui
4 Renda de alugel ou de empresas
5 Recebe ajuda do governo (ajuda social)

51
6 Outras, especifique ___________
7 Nenhuma
8 Não sei
9 Não tenho resposta
2 Qual sua renda mensal? 1 Nenhum
2 Menos que 1 salário
3 1 a 3 salários
4 4 a 5 salários
5 Mais de 5 salários
3 Você acha que sua renda é satisfatória para suas
necessidades?
1 Muito bem
2 Conveniente
3 Não muito bem
4 Não é sufuciente
VI) DOENÇAS CRÔNICAS
“Eu vou fazer algumas perguntas sobre a sua saúde”
1 Você diria que sua saúde é excelente, muito boa, boa,
mais ou menos, ou ruim?
1 Excelente
2 muito boa
3 Boa
4 mais ou menos (passável)
5 Ruim
6 Não sei
7 Não tenho resposta
2 Algum médico ou enfermeiro disse que você tem pressão
alta ou sofre de hipertensão?
Se uma outra pessoa responder pelo participante, referir
de quem é a resposta.
1 sim
2 Não
3 Não sei
4 Não tenho resposta

52
3 Algum médico ou enfermeiro já lhe disse que você sofre
de diabetes, ou tem um nível elevado de açúcar no
sangue?
1 Sim
2 Não
3 Não sei
4 Não tenho resposta
4 Algum médico ou enfermeiro disse que você sofre de
câncer ou de um tumor maligno, ou de um câncer na
pele?
1 Sim
2 Não
3 Não sei
4 Não tenho resposta
5 Algum médico ou enfermeiro já lhe disse que você sofre
de alguma doença pulmonar crônica, como bronquite
crônica, enfisema ou asma?
1 Sim
2 Não
3 Não sei
4 Não tenho resposta
6 Algum médico ou enfermeiro já lhe disse que você teve
um ataque cardíaco, doença coronária, sofre de angina,
de insuficiência cardíaca ou outros problemas cardíacos?
1 Sim
2 Não
3 Não sei
4 Não tenho resposta
7 Algum médico ou enfermeiro já lhe disse que você sofreu
de embolia cerebral, de acidente vascular cerebral (AVC),
de um ataque ou trombose?
1 Sim
2 Não
3 Não sei
4 Não tenho resposta
8 Algum médico ou enfermeiro disse que você sofre de
reumatismo, de artrite ou artrose?
1 sim
2 não
3 Não sei
4 não tenho resposta
9 Algum médico ou enfermeiro disse que você sofre de
depressão?
1 Sim
2 Não
3 Não sei
4 Não tenho resposta

53
10 Algum médico ou enfermeiro disse que você sofre de
alguma doença? (não mencionar nenhuma)
Qual :_________
1 Sim
2 Não
3 Não sei
4 Não tenho resposta
11. Perdeu peso sem intenção de 5kg ou mais nos últimos
anos?
1 Sim
2 Não
3 Não sei
4 Não tenho resposta
VII) SINTOMAS DEPRESSIVOS
« Agora eu vou ler algumas frases para você e você me diz se teve ou se sentiu durante última semana.
Tem que me dizer se foi frequente , ou se foi alguns dias, ou no inicio ou no fim da semana.»
« Para as respostas você deve me dizer de que maneira sentiu se nunca, se as vezes, se frequentemente,
se todo dia, se alguns dias, durante a última semana. »
Ler cada questão completamente incluindo todas as categorias de respostas.
Raramente
ou nunca
(menos que
1 dia)
Poucas
vezes
(1-2
dias)
Ás
vezes
(3-4
dias)
Quase
sempre ou
sempre (5-
7 dias)
1 Eu me chateei por coisas que normalmente não me chateavam
2 Não tive vontade de comer; estava sem apetite
3 Sinto que não consegui me livrar da tristeza mesmo com ajuda da
família e dos amigos
4 Eu me senti tão bem quanto as outras pessoas
5 Eu tive problemas para manter a concentração (prestar atenção) no
que estava fazendo
6 Eu me senti deprimido
7 Sinto que tudo que fiz foi muito custoso
8 Eu me senti com esperança em relação ao futuro
9 Eu pensei que minha vida tem sido um fracasso

54
10 Eu me senti com medo
11 Meu sono esteve agitado
12 Eu estive feliz
13 Eu conversei menos que o meu normal
14 Eu me senti sozinho
15 As pessoas não foram amigáveis
16 Eu me diverti
17 Eu tive crises de choro
18 Eu me senti triste
19 Eu senti que as pessoas não gostam de mim
20 Eu me sinto desanimado
VIII) DECLINIO COGNITIVO(PCL)
« As vezes, as pessoas se queixam de problemas de memória, o que fazer para ter uma boa memória.
Nós vamos fazer um teste e vamos compor uma série de questões que vai nos ajudar a detectar os
problemas de memória. Se você está de acordo pode responder algumas perguntas? » SIM NÃO
“Você deve responder essas perguntas sozinhas sem ajuda de outra pessoa
Qual é a data de hoje?
Ano mês dia
Correto 1 Incorreto 0
Que horas são?
(+ / - 2 horas)
:
H Min
Correto 1 Incorreto 0
Que dia da semana estamos? Correto 1 Incorreto 0
Qual é o seu endereço
completo?
Correto 1
Incorreto 0
Em que bairro nos estamos? Correto 1 Incorreto 0
Que idade você tem? Correto 1 Incorreto 0
Qual é sua data de nascimento?
Correto 1 Incorreto 0

55
Ano Mês Dia
Qual é a idade e o nome do(a)
filho (a) mais novo da sua mãe?
Correto 1 Incorreto 0
Total ________ ________
“Nesse momento vou mostrar algumas imagens e vou lhe perguntar o que elas representam para você.”
Mostre as imagens ao participante e marque se a resposta é correta ou não.
Vaca Correto 1 Incorreto 0
Barco/navio Correto 1 Incorreto 0
Colher Correto 1 Incorreto 0
Avião Correto 1 Incorreto 0
Garrafa Correto 1 Incorreto 0
Caminhão Correto 1 Incorreto 0
Total ________ ________
“Agora vou repetir todos os objetos para você olhar. Daqui a pouco vou lhe perguntar quais os objetos
que você viu.
Você pode me dizer os objetos que você viu, por favor.”
Vaca Correto 1 Incorreto 0
Barco/navio Correto 1 Incorreto 0
Colher Correto 1 Incorreto 0
Avião Correto 1 Incorreto 0
Garrafa Correto 1 Incorreto 0
Caminhão Correto 1 Incorreto 0
Total ________ ________
“Vou lhe contar uma história. Você vai ficar atenta, porque só vou contar uma vez. Quando eu terminar
depois de alguns segundos vou lhe perguntar e quero que você repita o que aprendeu. A história é (ler
lentamente):
Três crianças estavam sozinhas em casa quando começou a incendiar. Um bravo bombeiro chegou a
tempo entrou pela janela, entrou dentro de casa e levou as crianças para um lugar seguro. Salvo alguns
cortes e arranhões as crianças ficaram sans e salvas.”

56
(Peça ao participante depois de 2 minutos para dizer o que ela entendeu da história)
Três crianças Correto 1 Incorreto 0
Incendio Correto 1 Incorreto 0
Bombeiro que entrou Correto 1 Incorreto 0
Crianças foram socorridas Correto 1 Incorreto 0
Cortes e arranhões Correto 1 Incorreto 0
Sans e salvas Correto 1 Incorreto 0
Total ________ ________
5 minutos depois de mostrar as imagens (durante essse tempo, você pode medir a pressão arterial do
participante)
“Você pode repetir os objetos que você viu a poucos minutos?”
Vaca Correto 1 Incorreto 0
Barco/navio Correto 1 Incorreto 0
Colher Correto 1 Incorreto 0
Avião Correto 1 Incorreto 0
Garrafa Correto 1 Incorreto 0
Caminhão Correto 1 Incorreto 0
Total ________ ________
TOTAL SCORE:

57
Anexo 03- Certificado do comitê de ética
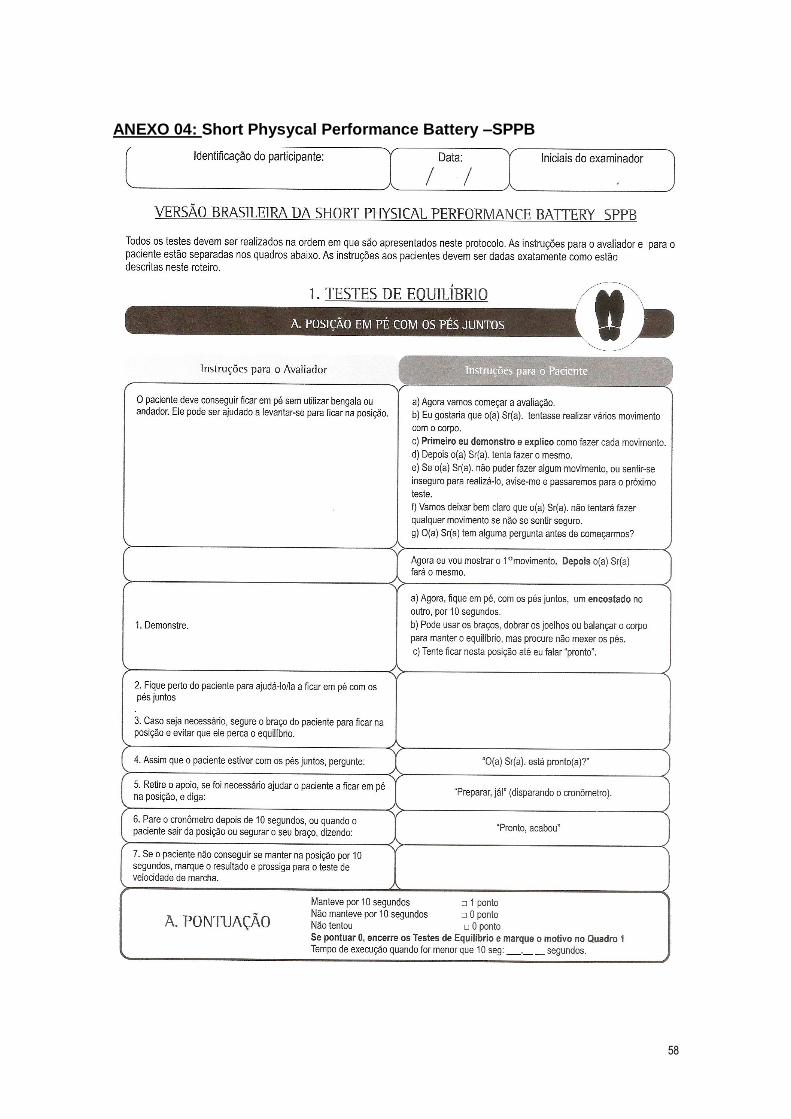
58
ANEXO 04: Short Physycal Performance Battery –SPPB

59

60

61

62

63

64

65
ANEXO 05
All Articles and Material should be submitted on-line via the Archives of Gerontology and Geriatrics submission system http://ees.elsevier.com/agg/ Please contact the Editorial Offices at [email protected] for general queries
Submission Checklist It is hoped that this list will be useful during the final checking of an article prior to sending it to the journal's Editor for Review. Please consult this Guide for Authors for further details of any item.
Ensure that the following items are present
• One Author designated as Corresponding Author • E-Mail address • Full postal address • Telephone number including country dialing code • Keywords • Original artwork (high-quality prints) • All figure captions • Any supplementary materials
Further Considerations • All references mentioned in the Reference list are cited in the text, and vice versa • Permission has been obtained for use of copyrighted material from other sources (including the Web) • Colour figures are clearly marked as being intended for colour reproduction on the Web (free of charge) and in print or to be reproduced in colour on the Web (free of charge) and in black-and-white in print • If only colour on the Web is required, black and white versions of the figures are also supplied for printing purposes
For any further information please visit our customer support site at http://support.elsevier.com.
Online-only Publication
Archives of Gerontology and Geriatrics offers authors the opportunity to select online-only publication as their preferred option for publishing their paper in the journal, rather than print publication. If authors wish to do this, their paper will be published online on ScienceDirect as a paginated and fully citable electronic article. It will be listed in the contents page of a printed issue and the full citation and abstract will be published in print. The citation and abstract of the paper will also still appear in the usual abstracting and indexing databases.
Authors will be asked to select which publication option they would prefer when submitting their paper to the Editorial Office.
Submission of articles Submission of an article implies that the work described has not been published previously (except in the form of an abstract or as part of a published lecture or academic thesis), that it is not under consideration for publication elsewhere,

66
that its publication is approved by all Authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, without the written consent of the Publisher.
Upon acceptance of an article, authors will be asked to sign a "Journal Publishing Agreement" (for more information on this and copyright see http://authors.elsevier.com). Acceptance of the agreement will ensure the widest possible dissemination of information. An email will be sent to the corresponding author confirming receipt of the manuscript together with a "Journal Publishing Agreement" form.
If excerpts from other copyrighted works are included, the author(s) must obtain written permission from the copyright owners and credit the source(s) in the article. Elsevier has preprinted forms for use by authors in these cases: contact Elsevier's Rights Department, Philadelphia, PA, USA: Tel. (+1) 215 238 7869; email [email protected]. Requests may also be completed online via the Elsevier homepage (http://www.elsevier.com/locate/permissions).
Funding body agreements and policies
Elsevier has established agreements and developed policies to allow authors who publish in Elsevier journals to comply with potential manuscript archiving requirements as specified as conditions of their grant awards. To learn more about existing agreements and policies please visit http://www.elsevier.com/fundingbodies
Types of papers
(1) Original papers reporting results of fundamental research in the fields defined in Aims and Scope
(2) Systematic Reviews, Non systematic review articles which give a valuable survey and synthesis based upon a critical interpretation of the recent research data or hypotheses will also be considered. We also welcome reviews by investigators of a series of their own studies where findings from several papers can be presented as a coherent whole advancing knowledge in a particular area. Such reviews may relate to both experimental studies and cohort profiles detailing the study provenance and its main findings.
(3) Study protocols that describe complex samples or experimental methods realting to the fields defined in Aims and Scope are welcome.
Presentation of manuscript Please write your text in good English (US-English spelling). Italics are not to be used for expressions of Latin origin, for example, in vivo, et al., per se. Use decimal points (not commas), use a space for thousands (10 000 and above).
Language Editing Available Authors who require information about language editing and copyediting services pre- and post-submission please visit http://www.elsevier.com/wps/find/authorshome.authors/languagepolishing or our customer support site at http://support.elsevier.com for more information. Please note Elsevier neither endorses nor takes responsibility for any products, goods or services offered by outside vendors through our services or in any advertising. For more information please refer to our Terms and
67
Conditionshttp://www.elsevier.com/wps/find/termsconditions.cws_home/termsconditions
Provide the following data on the title page (in the order given).
Title. Concise and informative, no more than 40 words. Titles are often used in abstracting and indexing systems. Avoid abbreviations and formulae where possible.
ShortTitle. No more than 60 characters including spaces to be used as a running head.
Author names and affiliations. Where the family name may be ambiguous (e.g., a double name), please indicate this clearly. Present the Authors' affiliation addresses (where the actual work was done) below the names. Indicate all affiliations with a lower-case superscript letter immediately after the Author's name and in front of the appropriate address. Provide the full postal address of each affiliation, including the country name, and, if available, the e-mail address of each Author.
Corresponding Author. Clearly indicate who is willing to handle correspondence at all stages of refereeing and publication, also post-publication. Ensure that telephone and fax numbers (with country and area code) are provided in addition to the e-mail address and the complete postal address.
All authors should have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted.
Acknowledgements. All contributors who do not meet the criteria for authorship as defined above should be listed in an acknowledgements section. Examples of those who might be acknowledged include a person who provided purely technical help, writing assistance, or a department chair who provided only general support. Authors should disclose whether they had any writing assistance and identify the entity that paid for this assistance. This should be listed at the end of the manuscript
Present/permanent address. If an Author has moved since the work described in the article was done, or was visiting at the time, a "Present address" (or "Permanent address") may be indicated as a footnote to that Author's name. The address at which the Author actually did the work must be retained as the main, affiliation address. Superscript Arabic numerals are used for such footnotes.
Abstract. A concise and factual abstract is required (maximum length 250 words). For original articles and systematic reviews the abstract should be structured to state briefly the purpose of the research, the materials and methods, the principal results and major conclusions. An abstract is often presented separate from the article, so it must be able to stand alone. References should therefore be avoided, but if essential, they must be cited in full, without reference to the reference list. Non-standard or uncommon abbreviations should be avoided, but if essential they must be defined at their first mention in the abstract itself.

68
Keywords. Immediately after the abstract, provide a maximum of 6 keywords, avoiding general and plural terms and multiple concepts (avoid, for example, "and", "of"). Be sparing with abbreviations: only abbreviations firmly established in the field may be eligible. These keywords will be used for indexing purposes.
Conflict of interest. At the end of the text, under a subheading "Conflict of interest statement" all authors must disclose any financial and personal relationships with other people or organisations that could inappropriately influence (bias) their work. Examples of potential conflicts of interest include employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, and grants or other funding.
Role of the funding source. All sources of funding should be declared as an acknowledgement at the end of the text. Authors should declare the role of study sponsors, if any, in the study design, in the collection, analysis and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication. If the study sponsors had no such involvement, the authors should so state.
Arrangement of the article
There are no specific word limits for articles: authors should be as concise as possible. Provide the short title as a running head centered at the top of the page and number all pages centered at the bottom of the pages except the Title Page.
Subdivision of the article. Divide your article into clearly defined and numbered sections. Subsections should be numbered 1.1 (then 1.1.1, 1.1.2), 1.2, etc. (the abstract is not included in section numbering). Use this numbering also for internal cross-referencing: do not just refer to "the text". Any subsection may be given a brief heading. Each heading should appear on its own separate line.
Introduction. State the objectives of the work and provide an adequate background.
Materials and methods. Provide sufficient detail to allow the work to be reproduced. Methods already published should be indicated by a reference: only relevant modifications should be described.
Results. Results should be clear and concise.
Discussion. This should explore the significance of the results of the work, not repeat them.
Conclusions. The main conclusions of the study may be presented in a short Conclusions section, which may stand alone or form a subsection of a Discussion or Results and Discussion section.
Appendices. If there is more than one appendix, they should be identified as A, B, etc. Formulae and equations in appendices should be given separate numbering: (Eq. A.1), (Eq. A.2), etc.; in a subsequent appendix, (Eq. B.1) and so forth.
References
Responsibility for the accuracy of bibliographic citations lies entirely with the Authors.

69
Reference style
Text: Citations in the text should follow the referencing style used by the American Psychological Association. You are referred to the Publication Manual of the American Psychological Association, Sixth Edition, ISBN 978-1-4338-0561-5, copies of which may be ordered from http://books.apa.org/books.cfm?id=4200067 or APA Order Dept., P.O.B. 2710, Hyattsville, MD 20784, USA or APA, 3 Henrietta Street, London, WC3E 8LU, UK. Details concerning this referencing style can also be found at http://linguistics.byu.edu/faculty/henrichsenl/apa/apa01.html.
List: references should be arranged first alphabetically and then further sorted chronologically if necessary. More than one reference from the same author(s) in the same year must be identified by the letters 'a', 'b', 'c', etc., placed after the year of publication.
Examples: Reference to a journal publication: Van der Geer, J., Hanraads, J. A. J., & Lupton, R. A. (2010). The art of writing a scientific article. Journal of Scientific Communications, 163, 51-59.
Reference to a book: Strunk, W., Jr., & White, E. B. (2000). The elements of style. (4th ed.). New York: Longman, (Chapter 4).
Reference to a chapter in an edited book: Mettam, G. R., & Adams, L. B. (2009). How to prepare an electronic version of your article. In B. S. Jones, & R. Z. Smith (Eds.), Introduction to the electronic age (pp. 281-304). New York: E-Publishing Inc.
References written in non-English language: These should be distinguished by writing at the end of the reference: (in Portuguese), (in Norwegian) etc. Journal names like BJOC cannot be used: the official abbreviated name of the journal should be given
Figure captions, tables, figures, schemes. Present these, in this order, at the end of the article. They are described in more detail below. High-resolution graphics files must always be provided separate from the main text file (see Preparation of illustrations http://www.elsevier.com/wps/find/authorsview.authors/authorartworkinstructions).
Text graphics. Present incidental graphics not suitable for mention as figures, plates or schemes at the end of the article and number them "Graphic 1", etc. Their precise position in the text can then be defined similarly (both on the manuscript and in the file). See further under the section, Preparation of Electronic Illustrations. Ensure that high-resolution graphics files are provided, even if the graphic appears as part of your normal wordprocessed text file.
Footnotes. Footnotes should be used sparingly. Number them consecutively throughout the article, using superscript Arabic numbers. Many wordprocessors build footnotes into the text, and this feature may be used. Should this not be the case, indicate the position of footnotes in the text and present the footnotes

70
themselves on a separate sheet at the end of the article. Do not include footnotes in the Reference list.
Table footnotes. Indicate each footnote in a table with a superscript lowercase letter.
Tables. Number tables consecutively in accordance with their appearance in the text. Place footnotes to tables below the table body and indicate them with superscript lowercase letters. Avoid vertical rules. Be sparing in the use of tables and ensure that the data presented in tables do not duplicate results described elsewhere in the article.
Nomenclature and units. Follow internationally accepted rules and conventions: use the international system of units (SI). If other quantities are mentioned, give their equivalent in SI.
Preparation of supplementary data. Elsevier now accepts electronic supplementary material (e-components) to support and enhance your scientific research. Supplementary files offer the Author additional possibilities to publish supporting applications, movies, animation sequences, high-resolution images, background datasets, sound clips and more. Supplementary files supplied will be published online alongside the electronic version of your article in Elsevier Web products, including ScienceDirect: http://www.sciencedirect.com. In order to ensure that your submitted material is directly usable, please ensure that data is provided in one of our recommended file formats. Authors should submit the material in electronic format together with the article and supply a concise and descriptive caption for each file. For more detailed instructions please visit our artwork instruction pages athttp://www.elsevier.com/wps/find/authorsview.authors/authorartworkinstructions
Randomised controlled trials All randomised controlled trials submitted for publication in Complementary Therapies in Medicine should include a completed Consolidated Standards of Reporting Trials (CONSORT) flow chart. Please refer to the CONSORT statement website at http://www.consort-statement.org for more information. Archives of Gerontology and Geriatrics has adopted the proposal from the International Committee of Medical Journal Editors (ICMJE) which require, as a condition of consideration for publication of clinical trials, registration in a public trials registry. Trials must register at or before the onset of patient enrolment. The clinical trial registration number should be included at the end of the abstract of the article. For this purpose, a clinical trial is defined as any research study that prospectively assigns human participants or groups of humans to one or more health-related interventions to evaluate the effects of health outcomes. Health-related interventions include any intervention used to modify a biomedical or health-related outcome (for example drugs, surgical procedures, devices, behavioural treatments, dietary interventions, and process-of-care changes). Health outcomes include any biomedical or health-related measures obtained in patients or participants, including pharmacokinetic measures and adverse events. Purely observational studies (those in which the assignment of the medical intervention is not at the discretion of the investigator) will not require registration. Further information can be found at http://www.icmje.org.

71
Disclosure of clinical trial results
In line with the position of the International Committee of Medical Journal Editors, the Journal is willing to consider manuscripts which include results posted in the same clinical trials registry in which primary registration resides. It will not consider such postings to be prior publication, providing the results posted are presented in the form of a brief structured (500 words) abstract or table. However, divulging results in other circumstances (eg, investors' meetings) is strongly discouraged and may jeopardise consideration of the manuscript. Authors should fully disclose all postings in registries of results of the same or closely related work.
Ethics Work on human beings that is submitted to Archives of Gerontology and Geriatrics should comply with the principles laid down in the Declaration of Helsinki; Recommendations guiding physicians in biomedical research involving human subjects. Adopted by the 18th World Medical Assembly, Helsinki, Finland, June 1964, amended by the 29th World Medical Assembly, Tokyo, Japan, October 1975, the 35th World Medical Assembly, Venice, Italy, October 1983, and the 41st World Medical Assembly, Hong Kong, September 1989. The manuscript should contain a statement that the work has been approved by the appropriate ethical committees related to the institution(s) in which it was performed and that subjects gave informed consent to the work. Studies involving experiments with animals must state that their care was in accordance with institution guidelines. Patients' and volunteers' names, initials, and hospital numbers should not be used.
Changes to Authorship This policy concerns the addition, deletion, or rearrangement of author names in the authorship of accepted manuscripts: Before the accepted manuscript is published in an online issue: Requests to add or remove an author, or to rearrange the author names, must be sent to the Journal Manager from the corresponding author of the accepted manuscript and must include: (a) the reason the name should be added or removed, or the author names rearranged and (b) written confirmation (e-mail, fax, letter) from all authors that they agree with the addition, removal or rearrangement. In the case of addition or removal of authors, this includes confirmation from the author being added or removed. Requests that are not sent by the corresponding author will be forwarded by the Journal Manager to the corresponding author, who must follow the procedure as described above. Note that: (1) Journal Managers will inform the Journal Editors of any such requests and (2) publication of the accepted manuscript in an online issue is suspended until authorship has been agreed. After the accepted manuscript is published in an online issue: Any requests to add, delete, or rearrange author names in an article published in an online issue will follow the same policies as noted above and result in a corrigendum.
Preparation of electronic illustrations
Submitting your artwork in an electronic format helps us to produce your work to the best possible standards, ensuring accuracy, clarity and a high level of detail.
General points
• Make sure you use uniform lettering and sizing of your original artwork.

72
• Save text in illustrations as "graphics" or enclose the font. • Only use the following fonts in your illustrations: Arial, Courier, Helvetica, Times, Symbol. • Number the illustrations according to their sequence in the text. • Use a logical naming convention for your artwork files, and supply a separate listing of the files and the software used. • Provide captions to illustrations separately. • Produce images near to the desired size of the printed version.
A detailed guide on electronic artwork is available on our website: http://authors.elsevier.com/artwork
Formats Regardless of the application used, when your electronic artwork is finalised, please "save as" or convert the images to one of the following formats (Note the resolution requirements for line drawings, halftones, and line/halftone combinations given below.):
EPS: Vector drawings. Embed the font or save the text as "graphics". TIFF: Colour or greyscale photographs (halftones): always use a minimum of 300 dpi. TIFF: Bitmapped line drawings: use a minimum of 1000 dpi., TIFF: Combinations bitmapped line/half-tone (colour or greyscale): a minimum of 500 dpi is required. DOC, XLS or PPT: If your electronic artwork is created in any of these Microsoft Office applications please supply "as is". Please do not: • Supply embedded graphics in your (spreadsheet, presentation) document; • Supply files that are optimised for screen use (like GIF, BMP, PICT, WPG); the resolution is too low; • Supply files that are too low in resolution; • Submit graphics that are disproportionately large for the content.
Captions Ensure that each illustration has a caption. Supply captions on a separate sheet, not attached to the figure. A caption should comprise a brief title (not on the figure itself) and a description of the illustration. Keep text in the illustrations themselves to a minimum but explain all symbols and abbreviations used.
Line drawings Supply high-quality printouts on white paper produced with black ink. The lettering and symbols, as well as other details, should have proportionate dimensions, so as not to become illegible or unclear after possible reduction; in general, the figures should be designed for a reduction factor of two to three. The degree of reduction will be determined by the Publisher. Illustrations will not be enlarged. Consider the page format of the journal when designing the illustrations.
Patient Details Unless you have written permission from the patient (or, where applicable, the next of kin), the personal details of any patient included in any part of the article and in any supplementary materials (including all illustrations and videos) must

73
be removed before submission. For further information seehttp://www.elsevier.com/patientphotographs
Colour illustrations Please make sure that artwork files are in an acceptable format (TIFF, EPS or MS Office files) and with the correct resolution. If, together with your accepted article, you submit usable color figures then Elsevier will ensure, at no additional charge that these figures will appear in color on the Web (e.g., ScienceDirect and other sites) regardless of whether or not these illustrations are reproduced in color in the printed version. For color reproduction in print, you will receive information regarding the costs from Elsevier after receipt of your accepted article. Please indicate your preference for color in print or on the Web only. For further information on the preparation of electronic artwork, please see http://www.elsevier.com/artworkinstructions.Please note: Because of technical complications which can arise by converting color figures to "gray scale" (for the printed version should you not opt for color in print) please submit in addition usable black and white versions of all the color illustrations.
Proofs One set of page proofs in PDF format will be sent by e-mail to the corresponding author (if we do not have an e-mail address then paper proofs will be sent by post). Elsevier now sends PDF proofs which can be annotated; for this you will need to download Adobe Reader version 7 available free from Adobe. Instructions on how to annotate PDF files will accompany the proofs. The exact system requirements are given at the Adobe siteIf you do not wish to use the PDF annotations function, you may list the corrections (including replies to the Query Form) and return to Elsevier in an e-mail. Please list your corrections quoting line number. If, for any reason, this is not possible, then mark the corrections and any other comments (including replies to the Query Form) on a printout of your proof and return by fax, or scan the pages and e-mail, or by post. Please use this proof only for checking the typesetting, editing, completeness and correctness of the text, tables and figures. Significant changes to the article as accepted for publication will only be considered at this stage with permission from the Editor. We will do everything possible to get your article published quickly and accurately. Therefore, it is important to ensure that all of your corrections are sent back to us in one communication: please check carefully before replying, as inclusion of any subsequent corrections cannot be guaranteed. Proofreading is solely your responsibility. Note that Elsevier may proceed with the publication of your article if no response is received.
Author enquiries
For enquiries relating to the submission of articles (including electronic submission where available) please visithttp://www.elsevier.com/wps/find/authorshome.authors . Author's can also their track accepted articles and set up e-mail alerts to inform you of when an article's status has changed, as well as detailed artwork guidelines, copyright information, frequently asked questions and more. Or contact the Editorial Office [email protected]
Open Access This journal offers authors two choices to publish their research;

74
1. Open Access • Articles are freely available to both subscribers and the wider public with permitted reuse • An Open Access publication fee is payable by authors or their research funder 2. Subscription • Articles are made available to subscribers as well as developing countries and patient groups through our access programs (http://www.elsevier.com/access) • No Open Access publication fee
All articles published Open Access will be immediately and permanently free for everyone to read and download. Permitted reuse is defined by your choice of one of the following Creative Commons user licenses:
Creative Commons Attribution-Non Commercial-ShareAlike (CC BY-NC-SA): for non-commercial purposes, lets others distribute and copy the article, to create extracts, abstracts and other revised versions, adaptations or derivative works of or from an article (such as a translation), to include in a collective work (such as an anthology), to text and data mine the article, as long as they credit the author(s), do not represent the author as endorsing their adaptation of the article, do not modify the article in such a way as to damage the author ’s honor or reputation, and license their new adaptations or creations under identical terms (CC BY NC SA).
Creative Commons Attribution-NonCommercial-NoDerivs (CC-BY-NC-ND): for non-commercial purposes, lets others distribute and copy the article, and to include in a collective work (such as an anthology), as long as they credit the author(s) and provided they do not alter or modify the article.
Elsevier has established agreements with funding bodies. This ensures authors can comply with funding body Open Access requirements, including specific user licenses, such as CC-BY. Some authors may also be reimbursed for associated publication fees. Funding bodies. If you need to comply with your funding body policy you can apply for the CC-BY license after your manuscript is accepted for publication.
To provide Open Access, this journal has a publication fee which needs to be met by the authors or their research funders for each article published Open Access. Your publication choice will have no effect on the peer review process or acceptance of submitted articles.
The Open Access publication fee for this journal is$USD 2,500, excluding taxes. Learn more aboutLearn more about Elseviers pricing policy.
Offprints The corresponding author, at no cost, will be provided with a PDF file of the article via e-mail. For an extra charge, paper offprints can be ordered via the offprint order form which is sent once the article is accepted for publication. The PDF file is a watermarked version of the published article and includes a cover sheet with the journal cover image and a disclaimer outlining the terms and conditions of use.
© 2013 Elsevier Ltd. All rights reserved.

75
This journal and the individual contributions contained in it are protected under copyright by Elsevier Ltd, and the following terms and conditions apply to their use:
Photocopying
Single photocopies of single articles may be made for personal use as allowed by national copyright laws. Permission of the Publisher and payment of a fee is required for all other photocopying, including multiple or systematic copying, copying for advertising or promotional purposes, resale, and all forms of document delivery. Special rates are available for educational institutions that wish to make photocopies for non-profit educational classroom use. For information on how to seek permission visit www.elsevier.com/permissions or call: (+44) 1865 843830 (UK) / (+1) 215 239 3804 (USA).
Derivative Works
Subscribers may reproduce tables of contents or prepare lists of articles including abstracts for internal circulation within their institutions. Permission of the Publisher is required for resale or distribution outside the institution. Permission of the Publisher is required for all other derivative works, including compilations and translations (please consult www.elsevier.com/permissions).
AudioSlides The journal encourages authors to create an AudioSlides presentation with their published article. AudioSlides are brief, webinar-style presentations that are shown next to the online article on ScienceDirect. This gives authors the opportunity to summarize their research in their own words and to help readers understand what the paper is about. More information and examples are available at http://www.elsevier.com/audioslides. Authors of this journal will automatically receive an invitation e-mail to create an AudioSlides presentation after acceptance of their paper.
Electronic Storage or Usage
Permission of the Publisher is required to store or use electronically any material contained in this journal, including any article or part of an article (please consult www.elsevier.com/permissions). Except as outlined above, no part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without prior written permission of the Publisher.
Notice No responsibility is assumed by the Publisher for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions or ideas contained in the material herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of it by its manufacturer.
Recommended