Effect of Ion Pairing on In Vitro Transcorneal Permeabilityof a �9-Tetrahydrocannabinol Prodrug: Potentialin Glaucoma Therapy
TUSHAR HINGORANI,1 WASEEM GUL,2,3,4 MAHMOUD ELSOHLY,2,3,4 MICHAEL A. REPKA,1,2,3 SOUMYAJIT MAJUMDAR1,2,3
1Department of Pharmaceutics, School of Pharmacy, The University of Mississippi, University, Mississippi 38677
2Research Institute of Pharmaceutical Sciences, The University of Mississippi, University, Mississippi 38677
3National Center for Natural Product Research, The University of Mississippi, University, Mississippi 38677
4ElSohly Laboratories, Inc., Oxford, Mississippi 38655
Received 21 February 2011; revised 10 August 2011; accepted 27 September 2011
Published online 11 October 2011 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/jps.22791
ABSTRACT: The aim of the present study was to evaluate and improve the in vitrotranscorneal permeability characteristics of �9-tetrahydrocannabinol (THC) through prodrugderivatization and formulation approaches. In vitro corneal permeability of THC and itshemisuccinate (THC-HS) and hemiglutarate (THC-HG) ester prodrugs and WIN 55-212-2(WIN), a synthetic cannabinoid, was determined using isolated rabbit cornea. The formula-tions studied included hydroxypropyl beta cyclodextrin (HP$CD) or randomly methylated betacyclodextrin (RM$CD), as well as prodrug–ion-pair complexes with L-arginine or tromethamine.Corneal permeability of WIN was found to be two-fold higher than THC in the presenceof HP$CD. THC-HS and THC-HG exhibited pH-dependent permeability. In the presence ofHP$CD, at pH 5 (donor solution pH), both prodrugs exhibited six-fold higher permeability com-pared with THC. However, permeability of the prodrugs was about three-fold lower than that ofTHC at pH 7.4. RM$CD, at pH 7.4, led to a significant improvement in permeability. Formationof ion-pair complexes markedly improved the solubility and permeability of THC-HG (seven-fold and threefold greater permeability compared with THC and WIN, respectively) at pH 7.4.The in vitro results demonstrate that the use of an ion-pair complex of THC-HG could be aneffective strategy for topical delivery of THC. © 2011 Wiley Periodicals, Inc. and the AmericanPharmacists Association J Pharm Sci 101:616–626, 2012Keywords: absorption; drug transport; formulation; passive diffusion/transport; permeability
INTRODUCTION
In 1971, Hepler and Frank1 published a report thatlinked marijuana smoking to a significant drop in
Abbreviations used: BCH, 2-aminobicyclo-[2,2,1]-heptane-2-carboxylic acid; CB1, cannabinoid receptor type 1; CB2, cannabi-noid receptor type 2; DPBS, Dulbecco’s phosphate buffered saline;HP$CD, hydroxypropyl beta cyclodextrin; IOP, intraocular pres-sure; IPBS, isotonic phosphate buffered saline; RM$CD, randomlymethylated beta cyclodextrin; THC, �9-tetrahydrocannabinol;THC-HS, �9-tetrahydrocannabinol hemisuccinate; THC-HG, �9-tetrahydrocannabinol hemiglutarate; THC-HG–ARG, ion pair of�9-tetrahydrocannabinol hemiglutarate and L-arginine; THC-HG–TRIS, ion pair of �9-tetrahydrocannabinol hemiglutarate andtromethamine; WIN, WIN 55-212-2.
Correspondence to: Soumyajit Majumdar (Telephone: +662-915-3793; Fax: +662-915-1177; E-mail: [email protected])Journal of Pharmaceutical Sciences, Vol. 101, 616–626 (2012)© 2011 Wiley Periodicals, Inc. and the American Pharmacists Association
intraocular pressure (IOP). Because of its implica-tions in the treatment of glaucoma, this report stim-ulated intense research toward identification of theconstituents responsible for this pharmacological ac-tion. It was established that �9-tetrahydrocannabinol(THC, Fig. 1a), a primary active constituent of mar-ijuana, is one of the components responsible for theIOP lowering effects.2 During the course of further in-vestigations, a reduction in IOP was observed whenTHC was administered either orally or intravenouslybut not when applied topically.3,4 This lack of topicalactivity, although some reports did demonstrate thattopical delivery of THC significantly lowered IOP,5 ledresearchers to conclude that the IOP lowering mech-anism of THC was probably because of its centrallyacting hypotensive effect and not due to activation oflocal ocular receptors.
616 JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012

ENHANCED TRANSCORNEAL PERMEATION OF THC PRODRUG 617
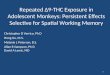
Figure 1. Chemical structures of (a) �9-tetrahydrocannabinol (THC), (B) �9-tetrahydrocannbinol hemisuccinate (THC-HS), (c) �9-tetrahydrocannbinol hemiglutarate(THC-HG), (d) WIN 55-212-2 (WIN).
However, recent studies suggest that THC canlower IOP and act as a neuroprotective agent bybinding to the cannabinoid receptors expressed inthe ocular tissues. In the 1990s, two cannabinoid re-ceptors type 1 and 2, CB1 and CB2, were identifiedand cloned.6 THC acts as an agonist for both CB1and CB2 receptors. Affinity values for the CB1 andCB2 receptors are 5.05 and 3.13 nM, respectively,7
whereas the half-maximal effective concentration val-ues for the CB1 and CB2 receptors are 6 and 0.4 nM,respectively.8 Although the distribution of cannabi-noid receptors in the body, since their identifica-tion, has been largely delineated, only recently havecannabinoid receptors been identified in the oculartissues. CB1 receptors are expressed in the trabec-ular meshwork, iris, ciliary body, and the retina,9–12
whereas CB2 receptors have been found in the retinaand trabecular meshwork.13 These locally expressedcannabinoid receptors are now believed to be involvedin the IOP lowering and neuroprotective activity of anumber of endocannabinoid and synthetic cannabi-noid derivatives.
There are two major pathways for the drainageof aqueous humor from the anterior ocular seg-ment: drainage through the Schlemm’s canal or theuveoscleral route. Activation of the CB1 receptorsin the ciliary muscle, by CB1 receptor agonists, in-duces contraction of the ciliary muscle.14 Contractionof the ciliary muscle leads to widening of the inter-cellular spaces in the trabecular meshwork and en-hances outflow of aqueous humor.15 Recently, bimato-prost, a prostaglandin analog that enhances uveoscle-ral outflow, has been shown to contract the humanciliary muscle through CB1-mediated mechanism.16
Furthermore, activation of CB1 receptors leads tofragmentation and reduction of actin stress fibersin the trabecular meshwork, further enhancing out-flow of aqueous humor.9 Thus, THC can reduce IOPthrough the local CB1/CB2 receptors. This can alsobe inferred from a previous clinical study. Merrittet al.5 demonstrated that 0.1% THC in mineral oilwhen given topically led to a 5.4 mm drop in IOP butwas accompanied with a 12 mm drop in systolic bloodpressure. A 10 mm drop in systolic blood pressure,
following systemic THC administration, should be as-sociated with less than a 1 mm drop in IOP.17 Also,0.05% THC in mineral oil, topically administered, ledto a 4.8 mm drop in IOP with no systemic hypotensiveeffect. Thus, these data suggest that topical THC isprobably acting locally through the ocular cannabi-noid receptors to reduce the IOP, and not through thesystemic pathway.
In glaucoma, a reduction in IOP is often not enoughto prevent or arrest the development or progressionof glaucoma-related optic neuropathy.18,19 Vision losscontinues even after significant IOP reduction hasbeen achieved. It has been suggested that neuroglialcell cytotoxicity in the optic nerve and retina leadsto visual field loss in glaucoma.20 Neuroglial cell tox-icity impairs macroglial glutamate metabolism andcauses microglia to release inflammatory cytokinesfollowing ischemia because of compression or vascu-lar occlusion. The released glutamate acts on recep-tors, including the N-methyl-D-aspartate subtype, onthe retinal ganglion cells to induce calcium influx andthe release of toxic reactive oxygen species, leading toapoptosis.20 Recent studies have demonstrated thatCB2 or nonspecific CB1/CB2 agonists were able toprotect retinal cells from oxidative stress but specificCB1 agonists had no effect.21 Intravitreally adminis-tered THC has been demonstrated to act as a neuro-protective in a rat model of glaucoma.20,22 Hampsonet al.23 also reported that the neuroprotective activ-ity of THC could also be independent of CB1 receptoractivation. Although the mechanism of neuroprotec-tion of THC is not yet clearly understood, it could bedue to the activation of CB2 receptors, its antioxidanteffect, or some other mechanism.23–25 The current ev-idence clearly suggests that THC possesses both IOPlowering and neuroprotectant activity, which are in-dependent of each other.
Although significant efforts have been directed to-ward understanding the pharmacology of THC, de-sign of effective topical delivery strategies for THChas not seen much activity. In 1977, Green et al.26
published a paper comparing corneal penetration ofTHC from different oils and found that light mineraloil was the best of the four vehicles tested. The study
DOI 10.1002/jps JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012

618 HINGORANI ET AL.
reported a 20% drop in IOP of normotensive rabbitswhen a 50:L dose (0.1%, w/w THC) was adminis-tered topically. However, plasma drug concentrationswere not reported. All further pharmacological stud-ies, with THC administered topically, were carried outusing light mineral oil as the vehicle. However, THCbeing a highly lipophilic molecule, with an aqueoussolubility of only 1–2 :g/mL and a log P of 6.3,27 itseffective partitioning from the oily vehicle into thetear film would be a suspect. Kearse and Green28 com-pared in vitro corneal permeability of THC from dif-ferent vehicles and observed that the permeability ofTHC from light mineral oil was only 1.86 × 10−8 cm/s.Thus, the lack of topical activity observed in the ear-lier in vivo reports could be due to the ineffective deliv-ery of THC to the target ocular tissues rather than ab-sence of local pharmacological activity. When higherdoses were administered, to increase the amount ofTHC permeating across the cornea, systemic side ef-fects were observed. Thus, development of a formu-lation that can effectively deliver THC across thecornea is needed prior to its evaluation for therapeuticactivity.
The aim of the current project was to improve theaqueous solubility and in vitro permeability of THCemploying complex formation and prodrug derivati-zation strategies. Dicarboxylic acid esters are com-monly used promoieties in prodrug derivatizationapproaches. These ester prodrugs exhibit higheraqueous solubility because they are ionized at phys-iological pH values. The THC hemisuccinate ester(THC-HS, Fig. 1b) and THC hemiglutarate ester(THC-HG, Fig. 1c) prodrugs were synthesized andevaluated for transcorneal permeability. The effect ofcyclodextrins and counterion adduct/complex forma-tion on the solubility and corneal permeability of THCand/or the two prodrugs were studied.
MATERIALS
Chemicals
Hydroxypropyl beta cyclodextrin (HP$CD), ran-domly methylated beta cyclodextrin (RM$CD),2-aminobicyclo-[2,2,1]-heptane-2-carboxylic acid(BCH), L-arginine (ARG), and Sigmacote R© wereobtained from Sigma (St. Louis, Missouri). WIN-55-212-2 (WIN) was purchased from Tocris Bioscience(Ellisville, Missouri). All other chemicals were ob-tained from Fisher Scientific (St. Louis, Missouri).All solvents used for analysis were of high pressureliquid chromatography (HPLC) grade.
Animal Tissues
Recently, we have evaluated the effect of storageon corneas obtained from ocular globes preserved in
Hank’s balanced salt solution and found the corneasto be equivalent to freshly excised corneas.29 Both ac-tive and passive transport processes in the preservedcorneas are intact for 24 h. Whole eye globes of al-bino New Zealand white rabbits were obtained fromPel Freez Biologicals (Rogers, Arkansas). Eyes wereshipped overnight in Hank’s balanced salt solutionover wet ice and used immediately on receipt.
METHODS
Preparation of Dicarboxylic Acid Ester Prodrugs
Dicarboxylic acid prodrugs (THC-HS and THC-HG)were synthesized and characterized according to pre-viously published procedures.30
Solubility of the Prodrugs
Solubility in Buffers
As THC binds to plastic, all experiments were car-ried out in plastic vials/tubes coated with Sigmacote R©
(Sigma) or borosilicate glass vials were used.31 Spe-cific measured quantities of stock solutions of THC-HS or THC-HG were transferred to the borosilicateglass or coated plastic vials and the organic sol-vent was evaporated using a stream of nitrogen gas.Dulbecco’s phosphate-buffered saline (DPBS) or iso-tonic phosphate-buffered saline (IPBS) was thenadded to the vials and the resulting mixture was son-icated for 10 min to dislodge the drug sticking to con-tainer walls and allowed to equilibrate for 24 h at 25◦Cin a shaking water bath at 75 shakes per minute. Theresulting suspension was centrifuged at 16,000g ina Fisher Scientific acuSpin micro17R centrifuge for10 min using silicon-coated centrifuge tubes. The su-pernatant was collected and analyzed by HPLC.
Solubility in Cyclodextrins
Solubility of THC-HS and THC-HG in a 2.5% solu-tion of HP$CD or RM$CD in DPBS or IPBS was de-termined using methods described under solubility ofTHC-HS/THC-HG in buffer solutions.
Solubility in Presence of L-Arginine/Tromethamine
Formation of an ion-pair complex with a hydrophiliccounterion could lead to an improvement in the solu-bility of the drug. Aliquots of stock solutions of THC-HS and THC-HG were transferred to glass vials andthe organic solvent was evaporated using a streamof nitrogen gas. L-Arginine or tromethamine (TRIS)in IPBS was then added to specific concentrationsof the prodrug. The prodrug THC-HS/THC-HG andthe counterion ARG/TRIS were added in increasingconcentrations, keeping the ratio of drug–counterion
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012 DOI 10.1002/jps

ENHANCED TRANSCORNEAL PERMEATION OF THC PRODRUG 619
constant (1:2). The combinations were then processedfor solubility determination following the same meth-ods as described under solubility of the prodrugs inbuffer solutions.
In Vitro Transcorneal Permeability Studies
Excess THC, THC-HS, THC-HG, and WIN were equi-librated in DPBS containing 2.5% HP$CD or RM$CD(pH adjusted to 5, 6, and 7.4) for 24 h at 25◦C ina shaking water bath. The supernatant containingthe drug–cyclodextrin complex was used in the trans-port studies. Donor solutions were analyzed for drugcontent at the beginning and after completion of thein vitro permeability studies. Receiver solution for allpermeability studies with cyclodextrin formulationsconsisted of 2.5% HP$CD solution in DPBS with pHadjusted to 7.4.
Transcorneal permeability of the ion-pair com-plexes of THC-HG with L-arginine (THC-HG–ARG)and tromethamine (THC-HG–TRIS) was also studied.THC-HG (1 mM) was equilibrated with ARG (2 mM) orTRIS (2 mM) in IPBS at 25◦C for 24 h in a shaking wa-ter bath. The supernatants were collected, analyzed,and used as the donor solution. For the studies in-vestigating permeability of the ion-pair formulations,receiver medium consisted of 2.5% HP$CD solutionin IPBS with pH adjusted to 7.4.
Eyes were used immediately upon receipt.Corneas were excised, following previously publishedprotocols.32 Briefly, an incision was made about2 mm from the corneal–scleral junction and thecornea was excised by cutting radially along thesclera. The 2 mm scleral portions help in easy mount-ing of the cornea. The excised corneas were im-mediately mounted between standard, 9 mm, side-by-side diffusion cells (PermeGear Inc., Hellertown,Pennsylvania). The half-cell facing the epitheliallayer was termed as the donor compartment. A circu-lating water bath was used to maintain the temper-ature at 34◦C during the transport studies. The vol-ume of the receiver solution (3.2 mL) was maintainedslightly higher than that of the donor solution (3 mLdrug solution) to maintain the natural curvature ofthe cornea. Both chambers were stirred continuouslyusing magnetic stirrers. Aliquots, 600 :L, were with-drawn every 30 min for 3 h and immediately replacedwith an equal volume of the receiver solution. Sam-ples were analyzed following the method described inthe Analytical Method section.
Involvement of Amino Acid Transporter
Amino acid transporters have been identified onthe rabbit/human cornea and are functionally active.ARG is a substrate for amino acid transporter B0,+,a sodium and energy-dependent transporter and is
specifically inhibited by BCH. The THC-HG–ARGadduct could be conveyed across the cornea by B0,+.Permeability of THC-HG–ARG complex was thus de-termined in the presence of 5 mM BCH to evaluateinvolvement of B0,+ in the transport process.
Stability in Ocular Tissue Homogenates
Tissue Preparation
Aqueous and vitreous humor were used as suchand without any dilution. They were centrifuged at16,000g for 10 min at 4◦C and the supernatant wasused. Other ocular tissues used in this study werehomogenized in ice-cold DPBS, on an ice bath, usingTISSUEMISER (Fisher Scientific). The homogenatewas then centrifuged at 16,000g at 4◦C for 15 min.Protein content in the supernatant was determinedaccording to the method of Bradford32 and was stan-dardized to 1 mg/mL.
Hydrolysis Procedure
The standardized homogenates were equilibrated for30 min at 37◦C to activate the enzymes. To 1.98 mLof the supernatant, 20:L of THC-HG (1 mg/mL) inethanol was added and mixed. Samples were with-drawn at predetermined time intervals. Bioconver-sion of THC-HG–ARG and THC-HG–TRIS complexto THC in aqueous humor was also evaluated. To0.95 mL of aqueous humor, 50 :L of THC-HG–ARGor THC-HG–TRIS complex (1:2) was added. Samples,200 :L, were withdrawn at specific time intervals. Anequal volume of ice-cold methanol was added to thealiquoted samples, to arrest the reaction, and cen-trifuged at 16,000g for 10 min. The supernatant wascollected and taken for analysis.
Analytical Method
Samples were analyzed using a Waters (Mildford,Massachusetts) HPLC system consisting of Waters600 pump controller, refrigerated Waters 717 plusautosampler, Waters 2487 UV detector, and Agilent(Santa Clara, California) 3395 integrator. Primarystock solutions of THC, THC-HS, and THC-HG wereprepared in hexane and stored at −15◦C. For thepreparation of standards, a known amount of stockwas taken and hexane was evaporated using nitro-gen gas. Standards were reconstituted using mobilephase. Mobile phase consisted of an 85:15 mixture ofmethanol and 0.84% (v/v) glacial acetic acid. A Phe-nomenex (Torrance, California) Luna PFP (2), 4.6 ×250 mm, column was used. Analytes were detectedat 226 nm. For quantification of THC, THC-HS, andTHC-HG, a standard curve was constructed with alinear range of 0.1–5 :g/mL. Injection volume was
DOI 10.1002/jps JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012

620 HINGORANI ET AL.
100 :L. Samples from the permeation studies wereinjected as such, whereas the solubility study sam-ples were diluted appropriately, in mobile phase, be-fore being injected. The standard curve generated hadcoefficient of determination values (r2) greater than0.9999. Retention times for the analytes were as fol-lows: THC (10.1 min), THC-HS (13 min), and THC-HG (14.3 min). Limit of detection and quantificationswere 5 and 50 ng/mL, respectively.
Data Analysis
Flux was calculated from the plot of cumulativeamount of drug (Dcum) in the receiver phase with re-spect to time (Eq. 1). Flux values were normalized todonor concentration (Cd) to calculate drug permeabil-ity (Eq. 2).
Flux (J) = dDcum/dt (1)
Permeability (P) = Flux/Cd (2)
All experiments were carried out at least in tripli-cate. Data obtained were subjected to statistical anal-ysis using analysis of variance. Variance between thegroups was checked using Levenes’ test. Statisticaldifference between groups was checked using Tukey’shonestly significant difference test. A p value of 0.05or less was considered to signify statistically signifi-cant difference.
RESULTS
Solubility
Solubility in Buffers
Solubility of the prodrugs, THC-HS and THC-HG, inIPBS or DPBS (Table 1) was found to be markedlyhigher than the reported solubility of THC (1–2:g/mL) in water.27 THC-HS and THC-HG demonstratedsignificantly higher solubility in IPBS (9.8 ± 0.9 and18.8 ± 3.1:g/mL, respectively) compared with that inDPBS (5.4 ± 0.3 and 4.3 ± 0.2:g/mL, respectively).
Solubility in Cyclodextrins
Solubility of the prodrugs (THC-HS and THC-HG)was significantly improved in the presence of cy-clodextrins (Table 1). A significant difference betweenthe solubility of THC-HS in the presence of HP$CD(144.9 ± 23.4:g/mL) and RM$CD (197.5 ± 57.9:g/mL) was not observed in IPBS. With both HP$CD(418.9 ± 13.8:g/mL) and RM$CD (430.2 ± 75.2:g/mL), THC-HS demonstrated a twofold higher solu-bility in DBPS compared with that in IPBS. THC-HG solubility in the presence of the cyclodextrins was
Table 1. Solubility of THC-HS and THC-HG in IPBS and DPBSas such or IPBS and DPBS containing 2.5% HP$CD or RM$CD at25◦C
Prodrug Buffer Cyclodextrin (2.5%) Solubility (:g/mL)
THC-HS – 9.8 ± 0.9IPBS HP$CD 144.9 ± 23.4
RM$CD 197.5 ± 57.9– 5.4 ± 0.3
DPBS HP$CD 418.9 ± 13.8RM$CD 430.2 ± 75.2
THC-HG – 18.8 ± 3.1IPBS HP$CD 899.9 ± 27.5
RM$CD 857.7 ± 49.4– 4.3 ± 0.2
DPBS HP$CD 678.5 ± 84.2RM$CD 910.6 ± 62.8
Results are depicted as mean ±SD (n = 3).
about 1.5-fold to twofold higher compared with THC-HS in DPBS containing HP$CD or RM$CD. Solubil-ity of THC-HG in IPBS was independent of the cy-clodextrin used. However, in DPBS, higher solubil-ity in RM$CD was observed compared with HP$CD(Table 1).
Solubility in Presence of ARG/TRIS
As THC-HS and THC-HG demonstrated higher aque-ous solubility in IPBS compared with DPBS (Table 1),ion-pairing studies with ARG and TRIS were carriedout in IPBS only. Preliminary studies demonstratedthat THC-HS was unstable in the presence of ARGand TRIS in IPBS. At the end of the 24 h equilibra-tion period, THC-HS was completely converted intoTHC (data not presented). Solubility of THC-HG inIPBS was found to increase linearly with increasingconcentrations of ARG or TRIS (Table 2). At the high-est concentration studied, the solubility of THC-HG(4 mM) with ARG (8 mM) was found to be 1716.5 ±49.5:g/mL. Aqueous solubility of THC-HG (4 mM)with TRIS (8 mM) was found to be 1158.4 ± 39.9:g/mL. With a further increase in the concentrations ofARG or TRIS, the solution pH was observed to in-crease above pH 10 and was not investigated anyfurther.
Corneal Permeation
Transcorneal permeability of THC (0.15 mM) acrossisolated rabbit cornea at pH 7.4 was found to be 5.57 ×10−6 cm/s (Fig. 2). DPBS containing 2.5% HP$CD wasused to prepare the donor solution. Decrease in donorsolution pH to 5 did not produce any significant effecton the corneal permeability of THC. When the concen-tration of HP$CD in the donor solution was increasedfrom 2.5% to 30%, keeping the drug concentrationconstant, THC permeating into the receiver chamber
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012 DOI 10.1002/jps

ENHANCED TRANSCORNEAL PERMEATION OF THC PRODRUG 621
Table 2. Solubility of THC-HG in IPBS, and the resulting solution pH, as a function of increasing concentrations of THC-HG andL-Arginine/Tromethamine while maintaining the ratio of drug– counterion constant (1:2), at 25◦C
Counterion THC-HG (mM) Counterion (mM) pH Concentration of THC-HG in Solution (:g/mL)
L-Arginine 1 2 7.4 423.4 ± 52.22 4 7.9 795.5 ± 51.13 6 8.4 1154.9 ± 47.54 8 8.9 1716.5 ± 49.1
Tromethamine 1 2 7.5 219.3 ± 16.92 4 7.6 517.2 ± 46.53 6 7.7 868.5 ± 80.54 8 7.8 1158.4 ± 39.9
Results are depicted as mean ±SD (n = 3).
was found to be below the detection limit (<0.05:g/mL). WIN, a synthetic CB1/CB2 agonist, which hasbeen demonstrated to reduce IOP when applied top-ically, exhibited twofold higher corneal permeabilitycompared with THC. Permeability of WIN across thecornea, such as THC, was also found to be pH inde-pendent. When the concentration of HP$CD in thedonor solution was increased from 2.5% to 30%, keep-ing the concentration of WIN constant, a 10-fold de-crease in corneal permeability of WIN was observed.Replacing HP$CD with RM$CD (2.5%) in the donorsolution led to a twofold improvement in the in vitrocorneal permeability of THC but did not affect the per-meability of WIN. Expectedly, THC-HS and THC-HGdemonstrated pH-dependent permeability across thecornea. At pH 5 (donor solution pH), permeability ofTHC-HS and THC-HG was about sixfold higher com-pared with the permeability of THC in 2.5% HP$CDin DPBS (Fig. 3). An increase in the donor solutionpH significantly decreased the permeability of THC-HS and THC-HG. Compared with the permeability ofTHC in 2.5% HP$CD (pH 7.4), permeability of THC-HS and THC-HG was about twofold higher at pH 6and about threefold lower at pH 7.4 (Fig. 3). This is
Figure 2. Permeability of THC and WIN at 34◦C acrossisolated rabbit cornea. The legends indicate the donor so-lution pH and composition. Receiver solution used in thesestudies was DPBS containing 2.5% HP$CD (pH 7.4). Re-sults are depicted as a mean ±SD (n = 3). ∗p < 0.05; ∗∗ND,THC concentrations could not be detected in the presenceof 30% HP$CD.
probably because the prodrugs are ionized at physio-logical pH values (pKa of THC-HG is 3.6 ± 0.4). Forall permeability studies involving cyclodextrin formu-lations, DPBS containing 2.5% HP$CD was used asthe receiver solution.
To shield the negative charge on the prodrugs,permeability of THC-HS and THC-HG was evalu-ated in the presence of ARG and TRIS because theyare positively charged at physiological pH values. Atphysiological pH (pH 7.4), THC-HG–ARG and THC-HG–TRIS were found to be almost sevenfold morepermeable compared with the permeability of THCin 2.5% HP$CD (Fig. 4 & 5). This was about three-fold higher compared with the corneal permeabilityof WIN at pH 7.4. IPBS containing 2.5% HP$CD wasused as the receiver solution in these studies for de-termining the permeability of the ion pairs. Donorconcentrations (in terms of THC) and flux values forall the formulations have been reported in Table 3.
Analysis of the donor solution samples collected atthe start and end of the permeation studies indicatedthat THC-HS and THC-HG, in all formulations stud-ied, remained intact for the duration of the in vitropermeability studies.
Figure 3. Permeability of THC-HS and THC-HG (interms of total THC) at 34◦C across isolated cornea. Thelegends indicate the donor solution pH and composition.Receiver solution used in these studies was DPBS contain-ing 2.5% HP$CD (pH 7.4). Results are depicted as a mean±SD (n = 3). ∗p < 0.05.
DOI 10.1002/jps JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012

622 HINGORANI ET AL.
Figure 4. Comparative permeability (in terms of to-tal THC) of THC, WIN, THC-HG–ARG complex, THC-HG–ARG complex + BCH, and THC-HG–TRIS complex at34◦C across isolated rabbit corneas. The legends indicatethe donor solution pH and composition. Receiver mediumwas 2.5% HP$CD in DPBS (pH 7.4) for THC and WIN,whereas for the ion-pair complexes the receiver solutionwas IPBS containing 2.5% HP$CD (pH 7.4). Results aredepicted as a mean ±SD (n = 3). ∗p < 0.05.
Involvement of Amino Acid Transporter
2-Aminobicyclo-[2,2,1]-heptane-2-carboxylic acid isan L-amino acid transporter inhibitor. There was nosignificant difference in the permeability of the THC-HG–ARG complex in the presence of 5 mM BCH.
Stability in Corneal Homogenates
Apparent first-order enzyme-mediated degradationrate constants (after adjusting for buffer-mediatedhydrolysis) and half-life of THC-HG in aqueous hu-mor, vitreous humor, and other ocular tissue ho-mogenates (1 mg/mL) have been depicted in Table 4.THC-HG was rapidly converted to THC in the aque-ous humor (t1/2, 25 ± 2.1 min) and the retina choroid(t1/2, 36.7 ± 1.2 min). Bioconversion of THC-HG inaqueous humor was not affected by the presence ofARG or TRIS.
DISCUSSION
Establishing effective delivery of a drug to the targettissues is a prerequisite to clinical studies evaluatingpharmacological response. However, all previous clin-ical studies evaluating topical effectiveness of THC inglaucoma used light mineral oil-based formulations,a vehicle from which in vitro corneal permeabilityof THC is reported to be 1.86 × 10−8 cm/s.28 Thus,inefficient delivery of THC to the target ocular tis-sues could be responsible for the sporadic evidencewith respect to the efficacy of topically administeredTHC on IOP. In the present investigation, prodrugand formulation approaches to improve the aqueoussolubility and transcorneal permeability of THC werestudied.
Cyclodextrins have been widely used as complexforming agents to improve the solubility and perme-ability of many hydrophobic drug candidates.33 Astheir discovery, cyclodextrins have been used in nu-merous marketed products. Of these, HP$CD whenused up to 12.5% (w/v) has been shown to be safeand well tolerated when administered topically to theeye.34 It has also been demonstrated that HP$CD onlytransports the drug molecule to the surface of themembrane and does not itself permeate through themembrane in any significant quantities.34 RM$CDhas also been used by researchers in ophthalmic drugdelivery.35 When used at high concentrations, bothHP$CD and RM$CD have been shown to affect tightjunction integrity.36,37 However, in vitro corneal per-meability studies demonstrate that use of HP$CDup to concentrations of 5% (w/v) does not affect thetight junctions.37 Concentration-dependent effect ofRM$CD on corneal tight junctions has not been re-ported as yet. Thus, some of the observed enhance-ment in corneal permeability in the presence of thecyclodextrins could have resulted from the interactionof the cyclodextrins with the corneal tight junctions
Figure 5. Cumulative transport of THC, THC-HS, and THC-HG (in terms of total THC)from cyclodextrin and ion pair-based formulations across isolated rabbit corneas at 34◦C, as afunction of time. The donor solution (Don) and receiver medium (Rec) pH and composition areindicated in the legends. Results are depicted as a mean ±SD (n = 3). ∗p < 0.05.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012 DOI 10.1002/jps

ENHANCED TRANSCORNEAL PERMEATION OF THC PRODRUG 623
Table 3. Donor concentrations and flux of THC, THC-HS, and THC-HG (in terms of total THC) and WIN in different vehicles at34◦C across isolated rabbit cornea
Drug Donor pH Donor VehicleDonor Concentration
(:g/mL)Flux [:g/(cm2 min) ×
10−2]Predicted Maximum Fluxa
[:g/(cm2 min) × 10−2]
THC 5 2.5% HP$CD in DPBS 40.7 ± 0.7 1.7 ± 0.2 –7.4 2.5% HP$CD in DPBS 46.8 ± 2.9 1.6 ± 0.1 –7.4 30% HP$CD in DPBS 40.1 ± 0.7 No drug detected –7.4 2.5% RM$CD in DPBS 19.9 ± 0.9 1.5 ± 0.2 –
WIN 5 2.5% HP$CD in DPBS 73.3 ± 2.8 5.4 ± 0.3 –7.4 2.5% HP$CD in DPBS 86.3 ± 12.4 5.7 ± 0.6 –7.4 30% HP$CD in DPBS 97.2 ± 0.4 0.8 ± 0.1 –7.4 2.5% RM$CD in DPBS 238.3 ± 17.5 13.2 ± 0.6 –
THC-HS 5 2.5% HP$CD in DPBS 64.3 ± 4.3 14.9 ± 0.9 –6 2.5% HP$CD in DPBS 29.8 ± 2.9 1.5 ± 0.1 –
7.4 2.5% HP$CD in DPBS 73.1 ± 0.7 0.9 ± 0.5 5.1 ± 3.77.4 2.5% RM$CD in DPBS 103.5 ± 12.9 3.5 ± 0.1 14.7 ± 0.5
THC-HG 5 2.5% HP$CD in DPBS 53.8 ± 3.1 11.4 ± 1.1 –6 2.5% HP$CD in DPBS 30.1 ± 1.5 1.7 ± 0.2 –
7.4 2.5% HP$CD in DPBS 30.9 ± 1.9 0.3 ± 0.1 6.5 ± 2.17.4 2.5% RM$CD in DPBS 30.1 ± 0.4 1.9 ± 0.2 56.3 ± 6.17.6 2 mM L-arginine in IPBS 78.9 ± 8.1 14.9 ± 0.9 79.9 ± 11.97.6 2 mM L-arginine + BCH in IPBS 71.6 ± 6.5 13.4 ±0.9 –7.6 2 mM tromethamine in IPBS 71.9 ± 2.2 17.1 ± 2.6 51.9 ± 9.1
aMaximum flux values were calculated theoretically by multiplying observed permeability with maximum solubility values depicted in Tables 1 and2. Maximum values have not been presented for formulations wherein maximum solubility was not calculated.
Results are depicted as mean ±SD (n = 3).
also, besides enhanced solubility and greater avail-ability of the drug at the corneal surface.
Permeability of THC from 2.5% HP$CD solutions inDPBS was found to be about 300-fold higher comparedwith the permeability of THC from light mineral oil-based formulations. Incidentally, when Kearse andGreen28 used 30% HP$CD as the vehicle, transcornealpermeability of THC was observed to be only 3.3 ×10−8 cm/s. Thus, permeability of THC from the 2.5%HP$CD drug saturated solution in this study wasabout 200 times higher compared with the permeabil-ity value reported by Kearse and Green.28 Consistentwith this observation, when the concentration of cy-clodextrin was increased to 30%, from 2.5% in thecurrent study, while keeping the drug concentrationconstant, a dramatic decrease in corneal permeabil-ity was observed (Fig. 2). Our results thus demon-strate that the presence of excess amounts of free cy-clodextrins (use of unsaturated drug cyclodextrin so-lutions) results in decreased permeability. WIN alsodemonstrated a similar phenomenon (Fig. 2). Thus,the presence of excess cyclodextrin probably leads toa decrease in the free drug concentration availablefor permeation. Interestingly, the use of RM$CD im-proved permeability of THC by almost twofold.
However, even after such dramatic improvements,corneal permeability of THC only equaled the perme-ability of WIN, which is about five times more potentthan THC. Thus, the relatively hydrophilic THC-HSand THC-HG prodrugs were evaluated as a means tofurther improve transcorneal permeability.
Aqueous solubilities of THC-HS and THC-HG werefound to be significantly higher in IPBS than inDPBS (Table 1). This could be due to the higher ionicstrength of DPBS, compared with IPBS, which couldinhibit ionization of the prodrugs and thus aqueoussolubility. Use of cyclodextrins significantly improvedthe aqueous solubility of THC-HS and THC-HG inboth IPBS and DPBS (Table 1). However, aqueoussolubility of THC-HS in HP$CD or RM$CD in DPBSwas found to be higher than that in IPBS. The in-creased solubility in DBPS could be due to the pres-ence of higher concentrations of unionized THC-HSin DPBS, which may demonstrate higher affinity forthe cyclodextrins. Alternatively, stability of THC-HSin DPBS could be higher compared with that in IPBS,resulting in higher solubility. Generally, THC-HGdemonstrated higher solubility compared with THC-HS. This is probably because THC-HG is significantlymore stable than THC-HS, especially at higher pH
Table 4. Apparent first- order rate constants (k∗) and half lives (t1/2) of THC-HG in ocular tissue homogenates
Cornea Aqueous Humor Iris–Ciliary Body Vitreous Humor Retina Choroid
THC-HG k∗ × 103 (min−1) 9.7 ± 0.6 28.1 ± 0.1 14.7 ± 1.9 4.8 ± 0.2 18.9 ± 0.7t1/2 (min) 71 ± 1.2 25 ± 2.1 47.5 ± 5.1 144.7 ± 5.3 36.7 ± 1.2
Results are depicted as mean ± SD (n = 3).
DOI 10.1002/jps JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012

624 HINGORANI ET AL.
values. The solubility studies involved a 24 h equili-bration period and would thus be exposed to signifi-cant hydrolysis.30
THC-HS and THC-HG demonstrated pH-dependent corneal permeability. At pH 5 (donorsolution pH), the permeability of the prodrugs wasabout fivefold higher compared with THC, in HP$CD.Corneal permeability decreased threefold when thedonor solution pH was 7.4, probably due to ionizationof the prodrugs. Dicarboxylic acids are commonlyused as promoieties in prodrug derivatization ap-proaches to increase the solubility of water-insolubledrugs, but their acidic pKa values keep them in theionized state at physiological pH values. When orallyadministered, the gastrointestinal tract possesses alarge surface area and allows prolonged contact time.Also, endogenous ligands could form complexes withionized drugs when given orally. Thus, even ionizeddrugs can be absorbed on oral administration over aperiod of time. In contrast, when a drug is instilledtopically, it has to overcome the limited surface areaavailable for absorption and also faces an extremelyshort contact time. Moreover, the mucus lining thecorneal epithelial cells is negatively charged andwould thus repel the negatively charged prodrugs,leading to decreased permeability. A soluble, union-ized, and highly permeable molecule is thus mostfavorable for ocular delivery.
Ion-pairing agents have been used to neutralize thecharge on ionic drugs and prodrugs and to improve oc-ular permeability.38,39 ARG carries a positive chargeat physiological pH and was thus chosen to form anion-pair complex. TRIS is a primary amine and is pos-itively charged at pH 7.4. TRIS has been successfullyused as a counterion for preparing ophthalmic ke-torolac formulations (Acular R©, Allergan Inc.(Irvine,California))
THC-HS was found to be highly unstable in thepresence of the cationic counterions. At the end ofthe 24 h equilibration period with ARG and TRIS,the prodrug was completely converted to THC at allconcentrations studied. Further studies of THC-HSwith counterions were discontinued. The maximumaqueous solubility values reported for THC-HG are539.56:g/mL at pH 8 and 411.3:g/mL at pH 9.30
Improved aqueous solubility of THC-HG with ARG(1.7 mg/mL at pH 8.9, Table 2) and TRIS (1.2 mg/mL,pH 7.8, Table 2) in IPBS suggests formation of ionpairs. All further studies with counterions were car-ried out with THC-HG.
At physiological pH values, THC-HG–ARG andTHC-HG–TRIS ion pair complexes in IPBS weresevenfold more permeable compared with THC in2.5% HP$CD in DPBS. The ion-pair complexesdemonstrated almost a 1000-fold improvement overthe reported permeability of THC from light min-eral oil-based formulations. Three amino acid trans-
porters LAT1, ASCT1, and B0,+ have been shownto be present and functionally active on the cornealepithelium.40–42 ARG utilizes the B0,+ system to per-meate through the cornea. B0,+ transports aminoacids may be neutral or positively charged. Althoughboth L and D amino acids are transported, L is morepreferred.32 The amino acid transporter B0,+ is knownto accept a wide range of substrates and possiblycould tolerate significant structural modifications totheir substrates. The increased corneal permeabilityof THC-HG–ARG could be because of the involvementof the B0,+ system. However, permeability of THCfrom the THC-HG–ARG complex was not inhibitedby BCH, indicating that the improvement in physico-chemical properties was responsible for the observedimprovement in permeability. Alternatively, it couldbe speculated that the improvement in permeabilitycould also be due to the positively charged counteri-ons neutralizing the negative charge on the mucouslayer covering the corneal epithelium.
Although prodrug derivatization and complex for-mation improve solubility and corneal permeabil-ity, the prodrug has to revert back to the parentdrug once it reaches the site of action in order toelicit pharmacological response. Our results demon-strate that THC-HG undergoes rapid bioconversionto THC in the aqueous humor, retina, and iris ciliary(Table 4).
The present study has thus led to the developmentof a topical drug delivery system, which improved thesolubility and permeability of THC. The THC pro-drugs, especially THC-HG, can thus be formulatedas 0.05% topical solutions for future preclinical stud-ies exploring their utility in glaucoma. Consideringthe promising data obtained with the cyclodextrinsin this study, the inclusion complex formed betweenTHC-HG and HP$CD/RM$CD will be characterizedin the near future, in a manner similar to our previ-ous studies with THC-HS.43
ACKNOWLEDGMENTS
This publication was partially supported by grants(#1R41EY020042 and #2R42GM067304-02) from theNational Institutes of Health to ElSohly Laborato-ries, Inc. (Oxford, Mississippi). The project was alsopartially supported by grant number 5P20RR021929from the National Center for Research Resources/NIH. The content is solely the responsibility of theauthors and does not necessarily represent the offi-cial views of the National Institutes of Health.
REFERENCES
1. Hepler RS, Frank IR. 1971. Marihuana smoking and intraoc-ular pressure. JAMA 217(10):1392.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012 DOI 10.1002/jps

ENHANCED TRANSCORNEAL PERMEATION OF THC PRODRUG 625
2. Elsohly MA, Harland E, Murphy JC, Wirth P, Waller CW.1981. Cannabinoids in glaucoma: A primary screening proce-dure. J Clin Pharmacol 21(Suppl 8–9):472S–478S.
3. Green K, Roth M. 1982. Ocular effects of topical administra-tion of delta 9-tetrahydrocannabinol in man. Arch Ophthalmol100(2):265–267.
4. Merritt JC, Perry DD, Russell DN, Jones BF. 1981. Topicaldelta 9-tetrahydrocannabinol and aqueous dynamics in glau-coma. J Clin Pharmacol 21(Suppl 8–9):467S–471S.
5. Merritt JC, Olsen JL, Armstrong JR, McKinnon SM. 1981.Topical delta 9-tetrahydrocannabinol in hypertensive glauco-mas. J Pharm Pharmacol 33(1):40–41.
6. Montero C, Campillo NE, Goya P, Paez JA. 2005. Homologymodels of the cannabinoid CB1 and CB2 receptors. A dockinganalysis study. Eur J Med Chem 40(1):75–83.
7. Pertwee RG. 2008. The diverse CB1 and CB2 re-ceptor pharmacology of three plant cannabinoids:Delta9-tetrahydrocannabinol, cannabidiol and delta9-tetrahydrocannabivarin. Br J Pharmacol 153(2):199–215.
8. Ryberg E, Larsson N, Sjogren S, Hjorth S, Hermansson NO,Leonova J, Elebring T, Nilsson K, Drmota T, Greasley PJ.2007. The orphan receptor GPR55 is a novel cannabinoid re-ceptor. Br J Pharmacol 152(7):1092–1101.
9. Kumar A, Song ZH. 2006. CB1 cannabinoid receptor-mediatedchanges of trabecular meshwork cellular properties. Mol Vis12:290–297.
10. Porcella A, Maxia C, Gessa GL, Pani L. 2000. The human eyeexpresses high levels of CB1 cannabinoid receptor mRNA andprotein. Eur J Neurosci 12(3):1123–1127.
11. Stamer WD, Golightly SF, Hosohata Y, Ryan EP, PorterAC, Varga E, Noecker RJ, Felder CC, Yamamura HI.2001. Cannabinoid CB(1) receptor expression, activationand detection of endogenous ligand in trabecular meshworkand ciliary process tissues. Eur J Pharmacol 431(3):277–286.
12. Straiker AJ, Maguire G, Mackie K, Lindsey J. 1999. Localiza-tion of cannabinoid CB1 receptors in the human anterior eyeand retina. Invest Ophthalmol Vis Sci 40(10):2442–2448.
13. He F, Song ZH. 2007. Molecular and cellular changes inducedby the activation of CB2 cannabinoid receptors in trabecularmeshwork cells. Mol Vis 13:1348–1356.
14. Lograno MD, Romano MR. 2004. Cannabinoid agonists in-duce contractile responses through Gi/o-dependent activationof phospholipase C in the bovine ciliary muscle. Eur J Phar-macol 494(1):55–62.
15. Llobet A, Gasull X, Gual A. 2003. Understanding trabecularmeshwork physiology: A key to the control of intraocular pres-sure? News Physiol Sci 18:205–209.
16. Romano MR, Lograno MD. 2007. Evidence for the involvementof cannabinoid CB1 receptors in the bimatoprost-induced con-tractions on the human isolated ciliary muscle. Invest Oph-thalmol Vis Sci 48(8):3677–3682.
17. Klein BE, Klein R, Knudtson MD. 2005. Intraocular pres-sure and systemic blood pressure: Longitudinal perspective:The Beaver Dam Eye Study. Br J Ophthalmol 89(3):284–287.
18. Schwartz M, Yoles E. 1999. Optic nerve degeneration and po-tential neuroprotection: Implications for glaucoma. Eur J Oph-thalmol 9(Suppl 1):S9–S11.
19. Levin LA, Peeples P. 2008. History of neuroprotection and ra-tionale as a therapy for glaucoma. Am J Manag Care 14(Suppl1):S11–S14.
20. El-Remessy AB, Khalil IE, Matragoon S, Abou-Mohamed G,Tsai NJ, Roon P, Caldwell RB, Caldwell RW, Green K, Liou GI.2003. Neuroprotective effect of (-)delta9-tetrahydrocannabinoland cannabidiol in N-methyl-D-aspartate-induced retinalneurotoxicity: Involvement of peroxynitrite. Am J Pathol163(5):1997–2008.
21. Wei Y, Wang X, Wang L. 2009. Presence and regulation ofcannabinoid receptors in human retinal pigment epithelialcells. Mol Vis 15:1243–1251.
22. Crandall J, Matragoon S, Khalifa YM, Borlongan C, Tsai NT,Caldwell RB, Liou GI. 2007. Neuroprotective and intraocularpressure-lowering effects of (-)delta9-tetrahydrocannabinol ina rat model of glaucoma. Ophthalmic Res 39(2):69–75.
23. Hampson AJ, Grimaldi M, Axelrod J, Wink D. 1998. Cannabid-iol and (-)delta9-tetrahydrocannabinol are neuroprotective an-tioxidants. Proc Natl Acad Sci U S A 95(14):8268–8273.
24. Garcia-Arencibia M, Gonzalez S, de Lago E, Ramos JA,Mechoulam R, Fernandez-Ruiz J. 2007. Evaluation of the neu-roprotective effect of cannabinoids in a rat model of Parkin-son’s disease: Importance of antioxidant and cannabinoidreceptor-independent properties. Brain Res 1134(1):162–170.
25. Han KH, Lim S, Ryu J, Lee CW, Kim Y, Kang JH, Kang SS,Ahn YK, Park CS, Kim JJ. 2009. CB1 and CB2 cannabinoidreceptors differentially regulate the production of reactive oxy-gen species by macrophages. Cardiovasc Res 84(3):378–386.
26. Green K, Bigger JF, Kim K, Bowman K. 1977. Cannabi-noid penetration and chronic effects in the eye. Exp Eye Res24(2):197–205.
27. Jarho P, Pate DW, Brenneisen R, Jarvinen T. 1998.Hydroxypropyl-beta-cyclodextrin and its combination withhydroxypropyl-methylcellulose increases aqueous solubility ofdelta9-tetrahydrocannabinol. Life Sci 63(26):PL381–PL384.
28. Kearse EC, Green K. 2000. Effect of vehicle upon in vitrotranscorneal permeability and intracorneal content of delta9-tetrahydrocannabinol. Curr Eye Res 20(6):496–501.
29. Majumdar S, Hingorani T, Srirangam R. Evaluation of activeand passive transport processes in corneas extracted from pre-served rabbit eyes. J Pharm Sci 99(4):1921–1930.
30. Thumma S, Majumdar S, Elsohly MA, Gul W, RepkaMA. 2008. Preformulation studies of a prodrug of delta9-tetrahydrocannabinol. AAPS PharmSciTech 9(3):982–990.
31. Christophersen AS. 1986. Tetrahydrocannabinol stability inwhole blood: Plastic versus glass containers. J Anal Toxicol10(4):129–131.
32. Majumdar S, Hingorani T, Srirangam R, Gadepalli RS,Rimoldi JM, Repka MA. 2009. Transcorneal permeation ofL- and D-aspartate ester prodrugs of acyclovir: Delineation ofpassive diffusion versus transporter involvement. Pharm Res26(5):1261–1269.
33. Stella VJ, He Q. 2008. Cyclodextrins. Toxicol Pathol36(1):30–42.
34. Loftsson T, Stefansson E. 1997. Effect of cyclodextrins ontopical drug delivery to the eye. Drug Dev Ind Pharm23(5):473–481.
35. Loftsson T, Stefansson E. 2002. Cyclodextrins in eye drop for-mulations: Enhanced topical delivery of corticosteroids to theeye. Acta Ophthalmol Scand 80(2):144–150.
36. Lambert D, O’Neill CA, Padfield PJ. 2007. Methyl-beta-cyclodextrin increases permeability of Caco-2 cell monolay-ers by displacing specific claudins from cholesterol rich do-mains associated with tight junctions. Cell Physiol Biochem20(5):495–506.
37. Tirucherai GS, Mitra AK. 2003. Effect of hydroxypropyl betacyclodextrin complexation on aqueous solubility, stability, andcorneal permeation of acyl ester prodrugs of ganciclovir. AAPSPharmSciTech 4(3):E45.
38. Conroy CW, Buck RH. 1992. Influence of ion pairing salts onthe transcorneal permeability of ionized sulfonamides. J OculPharmacol 8(3):233–240.
39. Ivaturi VD, Kim SK. 2009. Enhanced permeation ofmethotrexate in vitro by ion pair formation with L-arginine.J Pharm Sci 98(10):3633–3639.
40. Hatanaka T, Haramura M, Fei YJ, Miyauchi S, Bridges CC,Ganapathy PS, Smith SB, Ganapathy V, Ganapathy ME. 2004.
DOI 10.1002/jps JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012

626 HINGORANI ET AL.
Transport of amino acid-based prodrugs by the Na+- and Cl(-)-coupled amino acid transporter ATB0,+ and expression of thetransporter in tissues amenable for drug delivery. J PharmacolExp Ther 308(3):1138–1147.
41. Jain-Vakkalagadda B, Dey S, Pal D, Mitra AK. 2003. Identifi-cation and functional characterization of a Na+-independentlarge neutral amino acid transporter, LAT1, in humanand rabbit cornea. Invest Ophthalmol Vis Sci 44(7):2919–2927.
42. Jain-Vakkalagadda B, Pal D, Gunda S, Nashed Y, GanapathyV, Mitra AK. 2004. Identification of a Na+-dependent cationicand neutral amino acid transporter, B(0,+), in human andrabbit cornea. Mol Pharm 1(5):338–346.
43. Upadhye SB, Kulkarni SJ, Majumdar S, Avery MA, GulW,TB:break/ Elsohly MA, Repka MA. Preparation and char-acterization of inclusion complexes of a hemisuccinate esterprodrug of delta(9)-tetrahydrocannabinol with modified beta-cyclodextrins. AAPS PharmSciTech 11:509–517.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 101, NO. 2, FEBRUARY 2012 DOI 10.1002/jps
Recommended