Efficacy of Ultrasound-assisted Stress TestingUsing a Hand-carried Ultrasound Device for
Diagnosis of Coronary Artery DiseaseYutaka Hirano, MD, Hisakazu Uehara, MD, Hajime Nakamura, MD,Shin-ichirou Ikuta, MD, Manabu Nakano, MD, Seita Akiyama, MD,
and Kinji Ishikawa, MD, Osaka, Japan
Background: Exercise echocardiography is an effectivemeans of noninvasively detecting coronary artery dis-ease (CAD), and hand-carried cardiac ultrasound (HCU)devices are now being used to diagnose CAD in emer-gency rooms and at bedsides.Objective: To compare the efficacies of exercise echo-cardiography with an HCU device (EchoCG-HCU) andexercise electrocardiography (ECG) in the diagnosis ofCAD.Methods: Fifty-eight patients underwent symptom-lim-ited treadmill exercise testing. Two-dimensional echo-cardiographic images were obtained from standardparasternal and apical windows at rest and immediately
after exercise using an HCU device (180 PLUS SonoSitedoi:10.1016/j.echo.2006.01.006
536
Inc, Bothell, Wash). Wall motion was scored for each of16 left ventricular segments using a 5-point gradingsystem. The development of new or worsening wallmotion was considered to be indicative of ischemia.Results: When identifying CAD using exercise ECG, thesensitivity ws 63%, the specificity was 72%, and thediagnostic accuracy was 69%. By comparison, with exer-cise EchoCG-HCU the sensitivity was 68%, the specificitywas 90%, and the diagnostic accuracy was 83%. More-over, the specificity of exercise EchoCG-HCU was signif-icantly higher than that of exercise ECG (p < .05).Conclusion: Exercise EchoCG-HCU is at least as use-ful as exercise ECG for diagnosing CAD. (J Am Soc
Echocardiogr 2006;19:536-539.)Although exercise echocardiography (EchoCG) isreportedly useful for diagnosing coronary artery dis-ease (CAD),1-4 in Japan there are few hospitals inwhich exercise EchoCG is performed, often becausethere is not enough space in the exercise room for astandard EchoCG machine. Recently, however, hand-carried ultrasound (HCU) devices have been appliedfor the diagnosis of CAD, and a number of studies haveconfirmed its usefulness as a screening device.5-11 Inthis study, we compared the diagnostic efficacy ofexercise electrocardiography (ECG) with that of exer-cise EchoCG using an HCU device (EchoCG-HCU).
METHODS
In all, 97 consecutive patients with chest pain who under-went treadmill exercise ECG in our hospital between August2003 and January 2004 were enrolled for this study. Ex-cluded were patients with valvular heart disease, cardiomy-
From the Department of Cardiology, Kinki University School ofMedicine.Reprint requests: Yutaka Hirano, MD, Department of Cardiology,Kinki University School of Medicine, 377-2 Ohnohigashi, Osaka-sayama, Osaka 589-8511 Japan (E-mail: [email protected]).0894-7317/$32.00Copyright 2006 by the American Society of Echocardiography.
opathy, unstable angina pectoris, or myocardial infarction.Patients underwent symptom-limited treadmill exercisetesting using a modified Ellestad or modified Naughtonprotocol. All examinations were initiated at 1 PM withoutchanging the patients’ medications. Before exercise, 2-di-mensional (2D) EchoCG images obtained from theparasternal long- and short-axis views and the apical 4- and2-chamber views were recorded using a HCU device (180Plus, SonoSite Inc, Bothell, Wash) (width 19 � diameter6.3 � height 34 cm; 2.6 kg) coupled to a digital video-camera (DCR-TRV18, SONY Co Ltd, Tokyo, Japan) andstored on digital videotape. During the treadmill exercise,blood pressure and 12-channel ECGs were recorded everyminute. The criterion for CAD was S-T segment depressionof more than 0.1 mV at 80 milliseconds after the J-point.Exercise was discontinued if the patient had chest pain orleg fatigue, if the heart rate reached the target heart rate,or if the ECG showed S-T segment depression of morethan 0.2 mV at 80 milliseconds after the J-point. Immedi-ately after exercise, the patients were placed in the leftdecubitus position and ECGs and EchoCG-HCUs wererecorded. Left ventricular regional wall motion was sub-sequently analyzed using the 16-segment model12 of theAmerican Society of Echocardiography with 5 gradesranging from normokinesis to dyskinesis. The criterion forCAD was the onset of new wall-motion abnormalities.Segments were assigned to the territories of 3 coronaryarteries (left anterior descending, left circumflex, and
right) according to the vascular distribution of the seg-
Journal of the American Society of EchocardiographyVolume 19 Number 5 Hirano et al 537
ments.13 In addition, within 2 weeks after exercise,coronary angiography was performed using Judkin’s tech-nique. Significant coronary stenosis was defined as greaterthan 75% lumenal diameter stenosis of a coronary artery.
Wall motion was evaluated by two independent, experi-enced echocardiographers (physicians) who were not in-formed of the results of treadmill ECG and coronary angiog-raphy. Whenever a disagreement occurred, a third observer(physician) reviewed the images, and the differences wereresolved by consensus. The duration of time for imageacquisition for all views was measured.
Patients were fully informed about all of the tests, includ-ing their usefulness, limitations, and possible complications,and informed consent was obtained from all.
Statistical Analysis
All measured values are expressed as means � SD. Thesensitivity, specificity, and diagnostic accuracy of exerciseECG and EchoCG-HCU were compared using the �2 test andFisher direct probability calculations. Heart rates and bloodpressures were compared using Student t test. Values of Pless than .05 were considered significant.
RESULTS
Of the 97 patients who underwent exercise ECG andexercise EchoCG-HCU, 6 were excluded from analysisbecause of the poor image quality of their EchoCGfindings. Of the 91 remaining patients, 58 underwentcoronary angiography within 2 weeks after their exer-cise test. The patient backgrounds are shown in Table:
Table Patient characteristics
Male:female 42:16Site of coronary artery stenosis
LAD 14LCX 9RCA 7
Single-vessel disease 10Multivessel disease 9Coronary risk factor (%)
DM 14 (24)HT 43 (74)Hyperlipidemia 18 (31)Smoking 16 (28)
Drug therapy (%)�-blockers 13 (22)Ca antagonists 29 (50)Nitrates 8 (14)ACE-I 10 (17)ARB 12 (21)Antiplatelet agents 18 (31)Statins 15 (26)
Ca, Calcium; ACE-I, angiotensin-converting enzyme inhibitors; ARB, an-giotensin receptor blockers; DM, diabetes mellitus; HT, hypertension; LAD,left anterior descending coronary artery; LCX, left circumflex artery; RCA,right coronary artery.
10 had 1-vessel disease, 9 had multivessel disease, and
39 had no significant stenosis. The stenotic sites werewithin the left anterior descending coronary artery in14 patients, the left circumflex artery in 9 patients, andthe right coronary artery in 7 patients. Exercise wasended because of leg fatigue in 22 patients (37.9%),ECG changes in 5 patients (8.6%), chest pain in 3patients (5.2%), dyspnea in 1 patient (1.7%), and theachievement of the target heart rate in 28 patients(48.3%). Heart rates were significantly increased byexercise (74 � 15-143 � 22/min; P � .01), as wereboth the systolic and diastolic blood pressures (138 �21-200 � 23 mm Hg and 79 � 19-84 � 20 mm Hg,respectively; P � .01).
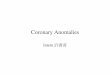
Among the 19 patients with CAD, wall-motionabnormalities were detected with exerciseEchoCG-HCU in 13, and significant ECG changeswere observed in 12. Conversely, among the 39patients without CAD, wall-motion abnormalitieswere not detected with exercise EchoCG-HCU in35, and significant ECG changes were not ob-served in 28. Thus, the sensitivity, specificity, anddiagnostic accuracy of exercise ECG in the diag-nosis of CAD were 63% (12/19), 72% (28/39), and69% (40/58), respectively. When wall motion wasevaluated using an HCU device in the diagnosis ofCAD, the sensitivity, specificity, and diagnosticaccuracy were 68% (13/19), 90% (35/39), and 83%(48/58), respectively. Note that the specificitywas significantly higher with EchoCG-HCU (P �.05) (Figure). When diagnosing CAD, the sensitiv-ity of EchoCG-HCU was 60% (6/10) among pa-tients with 1-vessel disease and 78% (7/9) amongthose with multivessel disease; with respect to theaffected coronary artery, the sensitivities were71%, 56%, and 71% for the left anterior descend-ing, left circumflex, and right coronary arteries,respectively. The time required to start recordingusing the HCU device was 15 � 5 seconds, and thetotal time required to record images for all views
Figure Sensitivity, specificity, and diagnostic accuracy ofexercise electrocardiography (ECG) and exercise echocar-diography (Echo) using hand-carried ultrasound.
was 40 � 7 seconds.

Journal of the American Society of Echocardiography538 Hirano et al May 2006
DISCUSSION
Exercise ECG has long been used to diagnoseCAD, although its diagnostic accuracy is not high.Gianrossi et al14 performed a meta-analysis involv-ing 147 studies (24,074 patients) and reportedthat the sensitivity and specificity of exercise ECGin the diagnosis of CAD were 68% and 77%,respectively. Exercise EchoCG is another tech-nique available for noninvasively detecting CADand has been shown to be more accurate thanexercise ECG.2-4 In Japan, however, exercise ECGis still used to diagnose CAD because a standardEchoCG machine is often too large to be placed inthe small exercise rooms and because standardEchoCG machines are often being used for routineexamination, making them unavailable for exer-cise EchoCG. On the other hand, Rugolotto et al5
recently reported that an HCU device is adequatefor focused assessment of cardiac anatomy andfunction, and Spencer et al6 demonstrated that thecombination of physical examination and the find-ings on an HCU device is better than physicalexamination alone for diagnosing CAD. In addi-tion, Decara et al7 tested the feasibility of teachingmedical students to use HCU devices to makebedside cardiac diagnoses and compared the ac-curacy of their HCU and physical examinations.They found that instructing fourth-year medicalstudents on the use of an HCU device is feasibleand results in significantly more accurate bedsidediagnoses. Finally, Vourvouri et al8 reported thatan HCU device could be used to effectively screenfor left ventricular hypertrophy in patients withhypertension.
We have shown here that an HCU device is alsouseful for diagnosing exercise-induced ischemia inpatients with CAD. Obtaining useful 2D EchoCGrecordings immediately after exercise requiresconsiderable skill; images often are not of suffi-cient quality to make a diagnosis, even with astandard EchoCG machine. But we have nowdemonstrated that EchoCG-HCU can be done withat least the same sensitivity and diagnostic accu-racy as is achieved with exercise ECG. Indeed, wefound that the specificity of EchoCG-HCU wassignificantly higher than ECG in the diagnosis ofCAD, although there was no significant increase insensitivity, perhaps because of inadequate imagequality.
The HCU device used in this study makes use oftissue harmonic imaging, but no satisfactory 2DEchoCG images could be directly stored. Whenpoor EchoCG imaging makes evaluation of wallmotion difficult, other examinations such as do-butamine stress EchoCG and myocardial scintigra-phy should be performed. In addition, we used
semiquantitative scoring to evaluate wall motion.In the future, quantitative evaluation of wall mo-tion using color kinesis or Doppler tissue imagingmay be necessary, even when the HCU device iscombined with exercise.
Limitations
Diagnosis of CAD using exercise EchoCG is facili-tated by display on a quad screen, an approachcommonly used in Europe and the United States.1 Itwas impossible, however, to configure a digital quadscreen display with the HCU device used in ourstudy. In addition, because no 2D echocardiogramscould be stored on the HCU device used, theinstrument was connected to a digital video device,and wall motion recorded on digital videotape wasregenerated for evaluation. Operator experiencemay compensate the limitations in imaging usingHCU devices. We have reported that formal stressecho accuracy in our institution is the same as theexpert readers.15 Finally, a larger number of patientswill be needed for a definitive evaluation of theefficacy of digital exercise EchoCG using HCU de-vices in the diagnosis of CAD.
Conclusion
Investigation of wall motion using EchoCG-HCUbefore and immediately after treadmill exercise isat least as effective for diagnosing CAD as exerciseECG.
REFERENCES
1. Armstrong WF. Stress echocardiography for detection of cor-onary artery disease. Circulation 1991;84:I43-9.
2. Ryan T, Vasey CG, Presti CF, O’Donnell JA, Feigenbaum H,Armstrong WF. Exercise echocardiography: detection of cor-onary artery disease in patients with normal left ventricularwall motion at rest. J Am Coll Cardiol 1988;11:993-9.
3. Sawada SG, Judson WE, Ryan T, Armstrong WF, FeigenbaumH. Upright bicycle exercise echocardiography after coronaryartery bypass grafting. Am J Cardiol 1989;64:1123-9.
4. Quinones MA, Verani MS, Haichin RM, Mahmarian JJ,Suarez J, Zoghbi WA. Exercise echocardiography versus 201Tlsingle-photon emission computed tomography in evaluationof coronary artery disease: analysis of 292 patients. Circulation1992;85:1026-31.
5. Rugolotto M, Hu BS, Liang DH, Schnittger I. Rapid assess-ment of cardiac anatomy and function with a new hand-carriedultrasound device (OptiGo): a comparison with standardechocardiography. Eur J Echocardiogr 2001;2:262-9.
6. Spencer KT, Anderson AS, Bhargava A, Bales AC, SorrentinoM, Furlong K, et al. Physician-performed point-of-care echo-cardiography using a laptop platform compared with physicalexamination in the cardiovascular patient. J Am Coll Cardiol2001;37:2013-8.
7. Decara JM, Kirkpatrick JN, Spencer KT, Ward RP, Kasza K,Furlong K, et al. Use of hand-carried ultrasound devices toaugment the accuracy of medical student bedside cardiacdiagnoses. J Am Soc Echocardiogr 2005;18:257-63.
8. Vourvouri EC, Poldermans D, Schinkel AF, Koroleva LY,
Sozzi FB, Parharidis GE, et al. Left ventricular hypertrophy
Journal of the American Society of EchocardiographyVolume 19 Number 5 Hirano et al 539
screening using a hand-held ultrasound device. Eur Heart J2002;23:1516-21.
9. Googkin GM, Spevack DM, Tunick PA, Kronzon I. Howuseful is hand-carried bedside echocardiography in critically illpatients? J Am Coll Cardiol 2001;37:2019-22.
10. Quiles J, Garcia-Fernandez MA, Almeida PB, Perez-David E,Bermejo J, Moreno M, et al. Portable spectral Doppler echo-cardiographic device: overcoming limitations. Heart 2003;89:1014-8.
11. Gorcsan J II, Pandey P, ElifSade L. Influsence of hand-carriedultrasound on bedside patient treatment decisions for consul-tative cardiology. J Am Soc Echocardiogr 2004;17:50-5.
12. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R,Feigenbaum H, et al. Recommendations for quantitation of
the left ventricle by two-dimensional echocardiography:American Society of Echocardiography committee onstandards, subcommittee on quantitation of two-dimensionalechocardiograms. J Am Soc Echocardiogr 1989;2:358-67.
13. Segar DS, Brown SE, Sawada SG, Ryan T, Feigenbaum H.Dobutamine stress echocardiography: correlation with coro-nary lesion severity as determined by quantitative angiogra-phy. J Am Coll Cardiol 1992;19:1197-202.
14. Gianrossi R, Detrano R, Mulvihill D, Lehmann K, Dubach P,Colombo A, et al. Exercise-induced ST depression in thediagnosis of coronary artery disease: a meta-analysis. Circula-tion 1989;80:87-98.
15. Hirano Y, Ozasa Y, Yamamoto T, Uehara H, Yamada S,Nakagawa K, et al. Hyperventilation and cold-pressor stressechocardiography for noninvasive diagnosis of coronary artery
spasm. J Am Soc Echocardiogr 2001;14:626-633.Recommended