Clinical Gastroenterology and Hepatology 2014;12:870–877
Factors That Affect Accuracy of a-Fetoprotein Test in Detectionof Hepatocellular Carcinoma in Patients With Cirrhosis
Purva Gopal,* Adam C. Yopp,‡,§ Akbar K. Waljee,k,¶ Jason Chiang,# Mahendra Nehra,#
Pragathi Kandunoori,# and Amit G. Singal§,#,**
*Department of Pathology, ‡Department of Surgery, §Harold C Simmons Cancer Center, #Department of Internal Medicine,**Department of Clinical Sciences, University of Texas Southwestern Medical Center, Dallas, Texas; kDepartment of InternalMedicine, University of Michigan, Ann Arbor, Michigan; and ¶Center for Clinical Management Research, Ann Arbor VeteransAffairs Healthcare Systems, Ann Arbor, Michigan
BACKGROUND & AIMS:
Measurements of a-fetoprotein (AFP) detect hepatocellular carcinoma (HCC) with low levels ofsensitivity and specificity, and therefore are not recommended for use in liver cancer surveil-lance. However, AFP levels might accurately detect HCC in subgroups of patients. We performeda retrospective case-control study to identify features of patients with cirrhosis in whom levelsof AFP correlated with HCC.METHODS:
We collected data from patients with cirrhosis, with (n [ 452) or without (n [ 676) HCC,diagnosed at Parkland Hospital in Dallas, Texas, from January 2005 through June 2012. Wedetermined sensitivities and specificities with which different levels of AFP identified thosewith HCC; multivariate logistic regression was used to associate accurate identification of HCCwith patient features (age, sex, race/ethnicity, alcohol intake, smoking, etiology of cirrhosis,presence of decompensation, and laboratory test results). We assessed the overall accuracy ofthese factors in detecting HCC using receiver operator characteristic curve analysis and theDelong method. We calculated levels of AFP that detect HCC with the highest levels of sensitivityand specificity in subgroups using receiver operator characteristic analysis.RESULTS:
Themost common etiologies of cirrhosis were hepatitis C virus (HCV) infection (60%) and alcoholinduced (22%). Nearly 11%of patientswere human immunodeficiency virus (HIV)-positive. Levelsof AFP greater than 20 ng/mL detected HCC with 70.1% sensitivity and 89.8% specificity. This AFPlevel identified patients with HCC with a c-statistic of 0.87 (95% confidence interval, 0.85–0.89); itwas significantly more accurate in HCV-negative patients than in HCV-positive patients (c-statistic,0.89 vs 0.83; P[ .007). AFP levels of 59 ng/mL or greatermost accurately detected HCC in patientswith HCV-associated cirrhosis; levels of AFP of 11 ng/mL or greater accurately identified HCC inHCV-negative patients. The level of AFP identified early stage HCC with a c-statistic of 0.62 (95%confidence interval, 0.58–0.66), and had a significantly higher level of accuracy for HIV-positivepatients than for HIV-negative patients (c-statistic, 0.81 vs 0.59; P < .001).CONCLUSIONS:
Based on a retrospective analysis of data from patients with cirrhosis, with or without HCC, AFPlevel most accurately detects HCC in patients without HCV infection. It detects HCC with a highlevel of accuracy in patients with cirrhosis and HIV infection.Keywords: Biomarkers; Liver Disease; AIDS; Screening.
Abbreviations used in this paper: AASLD, American Association for the Studyof Liver Diseases; AFP, a-fetoprotein; ALT, alanine aminotransferase; AST,aspartate aminotransferase; CI, confidence interval; HBV, hepatitis B virus;HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HIV, human immu-nodeficiency virus; NAFLD, nonalcoholic fatty liver disease; NASH, nonalco-holic steatohepatitis; OR, odds ratio; ROC, receiver operator characteristic.
© 2014 by the AGA Institute1542-3565/$36.00
http://dx.doi.org/10.1016/j.cgh.2013.09.053
See related article, El-Serag HB et al, on page1249 in Gastroenterology.
Hepatocellular carcinoma (HCC) is the fifth mostcommon cause of cancer and the third leading
cause of cancer-related death worldwide.1 Within theUnited States and Europe, its incidence is increasingrapidly, largely driven by the current epidemic of hepati-tis C virus (HCV) and nonalcoholic fatty liver disease(NAFLD) cases.2 Prognosis for patients with HCC
depends on tumor stage at diagnosis, with curative op-tions available only for patients diagnosed at an earlystage.

May 2014 Predictors of AFP for Detection of HCC 871
Surveillance with ultrasound alone at 6-month intervalsis recommended in patients with cirrhosis to detect HCC atan early stage.3 However, ultrasound remains operator-dependent, with a large gap between its efficacy and itseffectiveness in clinical practice, creating a need for effec-tive complementary biomarkers.4–7 a-fetoprotein (AFP),the best-studied serologic test, is attractive for surveillancebecause it is relatively inexpensive and easily obtainable.However, the most recent guidelines from the AmericanAssociation for the Study of Liver Diseases (AASLD) nolonger recommend using AFP, citing poor sensitivity andspecificity of AFP for early stage HCC. At a cut-off value of20 ng/mL, the most commonly used cut-off value in clin-ical practice, AFP has a sensitivity and specificity ofapproximately 60% and 80% for HCC, respectively.8
However, most studies have assumed that AFP per-forms equally well in all patients, independent of liverdisease etiology or severity. AFP has been shown to beincreased in several states of liver injury, including acuteliver failure, suggesting decreased specificity in cases withhigh cell turnover.9,10 Furthermore, the specificity of AFPmay vary by patient characteristics, such as sex andrace.6,10–12 Many of the prior studies were limited by arelatively small sample size, inclusion of patients withonly HCV or hepatitis B virus (HBV) infection, and theinclusion of patients without cirrhosis.10,13,14 However,the majority of HCC patients in the United States andEurope have underlying cirrhosis at the time of diag-nosis,2,15 and the inclusion of patients withmilder degreesof liver disease, who carry a low risk of HCC, may haveunfairly biased results of prior studies, so the accuracy ofAFP has been underestimated. Therefore, the primary aimof our study was to identify determinants for sensitivity,specificity, and overall accuracy of AFP in a cohort ofpatients with cirrhosis. A secondary aim of our study wasto define new potential cut-off values for AFP in the sub-groups of patients in whom accuracy varies.
Methods
Study Population
We conducted a retrospective case-control study ofcirrhotic patients with and without HCC at Parkland Me-morial Health and Hospital System, the safety-net systemfor Dallas County. With 11 primary care clinics in low-income neighborhoods, the Parkland Memorial Health andHospital System cares for a large proportion of patientswith cirrhosis as well as patients with HCC in Dallas County.Furthermore, Parkland Hospital is one of the few safety-nethospitals with an integrated electronic medical record forthe hospital and clinics, including primary care clinics.
We included all patients diagnosedwith HCC at ParklandHospital between January 2005 and June 2012. As previ-ously described, patientswere identifiedbya combination ofInternational Classification of Diseases, 9th revision, codesfor HCC (155.0 or 155.2), a prospectively maintained list of
patients seen in a multidisciplinary liver tumor clinic, andtumor conference presentation lists.16 Two authors (A.G.S.andA.C.Y.) adjudicatedallHCCcases to confirmthat theymetdiagnostic criteria, based on AASLD guidelines.We excludedpatientswhodidnot have anAFP level beforeHCCdiagnosis.
Our control population consisted of patients withcirrhosis who were seen at Parkland Hospital betweenJanuary 2010 and July 2011. Patients initially were identifiedusing a previously validated combination of InternationalClassification of Diseases, 9th revision, codes.17 Patientswere required to have at least one outpatient appointmentduring this time period to suggest that Parkland Hospitalwas their medical home. We excluded patients with anysuspicious liver mass on imaging and those who did nothave an AFP test during the study period (January 2010–July2011). Patients were required to have at least 6 months offollow-up evaluation to confirm the absence of HCC. Thisstudy was approved by the Institutional Review Board of theUniversity of Texas Southwestern Medical Center.
Data Collection
Patient demographics, clinical history, laboratory data,and imaging results were obtained through review ofcomputerized and paper medical records. Two in-vestigators (A.G.S. and A.C.Y.) independently extracted in-formation regarding HCC patients using standardizedforms, with discrepancies resolved through consensus.Similarly, 2 investigators (M.N. and P.K.) independentlyextracted information regarding non-HCC patients usingstandardized forms, with a third investigator (A.G.S.)available to resolve discrepancies. Age, sex, race/ethnicity,and lifetime alcohol and smoking history were recorded,with active alcohol abuse defined as drinkingmore than 40g/day of alcohol. Data regarding liver disease includedunderlying etiology and the presence of decompensation(ascites or encephalopathy). We classified patients ac-cording to etiology of liver disease, including HCV, HBV,alcohol-related liver disease, NAFLD, and other. Laboratorydata of interest included platelet count, creatinine, aspar-tate aminotransferase (AST), alanine aminotransferase(ALT), bilirubin, albumin, international normalized ratio,and AFP. We assessed the latest laboratory values betweenJanuary 2010 and July 2011 in non-HCC patients and thelaboratory values before diagnosis in those with HCC. Tu-mor characteristics were determined by imaging studies,which all had been interpreted by radiologists at ourinstitution. Early stage HCC was defined using the Milancriteria (1 tumor <5 cm or 2–3 tumors each <3 cm indiameter, without vascular invasion or distantmetastases).
Statistical Analysis
Demographics and clinical features were comparedbetween patients with and without HCC using the Fisherexact test and the Mann–Whitney rank-sum test forcategoric and continuous variables, respectively.

872 Gopal et al Clinical Gastroenterology and Hepatology Vol. 12, No. 5
We determined the sensitivity, specificity, positivepredictive value, and negative predictive value of AFP forthe detection of HCC. We dichotomized AFP at a cut-offvalue of 20 ng/mL because this is the most commonlyreported and used cut-off value in clinical practice. Weassessed overall accuracy, indicating the degree of correctclassification, by the c-statistic using receiver operatorcharacteristic (ROC) curve analysis. A c-statistic rangesfrom 0 to 1, with 1 indicating perfect prediction and 0.5indicating prediction by chance alone; values between 0.7and 0.8 generally are considered acceptable.18
We determined predictors of sensitivity and specificityusing the Fisher exact test and the Mann-Whitney rank-sum tests for categoric and continuous variables, respec-tively. We assessed the following potential independentvariables: age, sex, race, ethnicity, body mass index, eti-ology of liver disease, presence of hepatic decompensa-tion, human immunodeficiency virus (HIV) serostatus,platelet count, creatinine, albumin, AST level, bilirubin,international normalized ratio, and tumor stage. Variablessignificant on univariate analysis were included in multi-variate logistic regression analysis. After Bonferroniadjustment, P values of .05 and .025 were consideredsignificant for univariate and multivariate analyses,respectively. We used the Delong method to comparec-statistics between groups and to identify predictors ofoverall accuracy. Finally, we determined new optimalcut-off values to maximize sensitivity and specificity inthese subgroups using ROC curve analysis. All data anal-ysis was conducted using Stata 11 (College Station, TX).
Results
Patient Characteristics
Between January 2005 and June 2012, there were457 patients with cirrhosis who were diagnosed withHCC. We excluded 5 patients who did not have an AFPlevel before HCC diagnosis. Between January 2010 andJuly 2011, there were 914 patients with cirrhosis whowere seen in an outpatient setting at Parkland Hospital,of whom 238 patients were excluded for a lack of AFPlevel or insufficient follow-up duration.
The baseline characteristics of the remaining 1128patients (452 HCC and 676 non-HCC) are shown inTable 1. The median age of patients was 55 years, andthe majority of patients were men, with a higher pro-portion of men among HCC patients (78% vs 66%; P <.001). Our population was racially diverse, with 31%non-Hispanic Caucasians, 37% Hispanic Caucasians, and27% African Americans. Non-HCC patients were signifi-cantly more likely to be non-Hispanic Caucasian thanthose with HCC (34% vs 26%; P ¼ .01). The most com-mon etiologies of cirrhosis were HCV (60%), alcohol-induced liver disease (22%), and NAFLD (10%). Asexpected, HCV cirrhosis was significantly more commonamong HCC patients than non-HCC patients (70% vs
54%; P < .001). Nearly 11% of patients with known HIVserostatus were HIV positive. Of the 80 HIV-positivepatients, 59 (74%) had HCV co-infection and 14 (18%)had HBV co-infection.
The majority (53%) of patients had Child–Pugh Bcirrhosis, and another 32%hadChild–PughA cirrhosis. Themedian AFP level was 198 ng/mL in the HCC patients and 4ng/mL in non-HCC patients. The HCC cohort was diversewith respect to tumor stage, with 150 (33%) patientshaving early stage tumors, as defined by Milan criteria.
Performance Characteristics of a-Fetoprotein
Table 2 shows the performance characteristics of AFPat a cut-off value of 20 ng/mL. The sensitivity and speci-ficity of AFP values greater than 20 ng/mL for the detec-tion of HCC were 70.1% and 89.8%, respectively. AFPhad high positive and negative predictive values of 82.2%and 81.5%, respectively, although the proportion ofHCC patients in our study (40%) was substantially higherthan that seen in usual clinical settings. The sensitivity ofAFP, at a cut-off value of 20 ng/mL, for detection of earlystage HCC was significantly lower at 49.3%.
Predictors of specificity (ie, the proportion of patientswith an AFP level <20 ng/mL among those without HCC)included black race, HCV etiology, and AST level greaterthan 40 U/L on univariate analysis. On multivariateanalysis, black race (odds ratio [OR], 0.47; 95% confi-dence interval [CI], 0.27–0.81), HCV etiology (OR, 0.18;95% CI, 0.08–0.41), and increased AST levels (OR, 0.06;95% CI, 0.01–0.42) were associated with lower specificity(Table 3). Although only 7% of Caucasians and 8% ofHispanic patients had increased AFP levels in the absenceof HCC, false-positive AFP results were found in 20% ofAfrican Americans. AFP levels greater than 20 ng/mLachieved a very high specificity in the other 2 subgroups,with a specificity of 98% among non-HCV patients and99% among patients with normal AST levels.
Predictors of sensitivity (ie, the proportion of patientswith an AFP level >20 ng/mL among those with HCC) onunivariate analysis included early tumor stage, HIV sta-tus, viral etiology, AST level greater than 40 U/L, plateletcount greater than 100,000/mL, and bilirubin levelgreater than 2 mg/dL. On multivariate analysis, HIVstatus (OR, 4.50; 95% CI, 1.44–14.1) was associatedsignificantly with higher sensitivity, and early tumorstage (OR, 0.25; 95% CI, 0.15–0.43) was associatedwith lower sensitivity (Table 3). AFP had a sensitivity of86% in HIV-positive patients, compared with 67% inHIV-negative patients.
Subgroup analyses, excluding HIV-positive patients,were performed for predictors of sensitivity and speci-ficity. Predictors of specificity on multivariate analysiscontinued to include black race (OR, 0.43; 95% CI,0.24–0.77), HCV etiology (OR, 0.20; 95% CI, 0.09–0.45),and increased AST levels (OR, 0.07; 95% CI, 0.01–0.50).Predictors of sensitivity were similar except viral
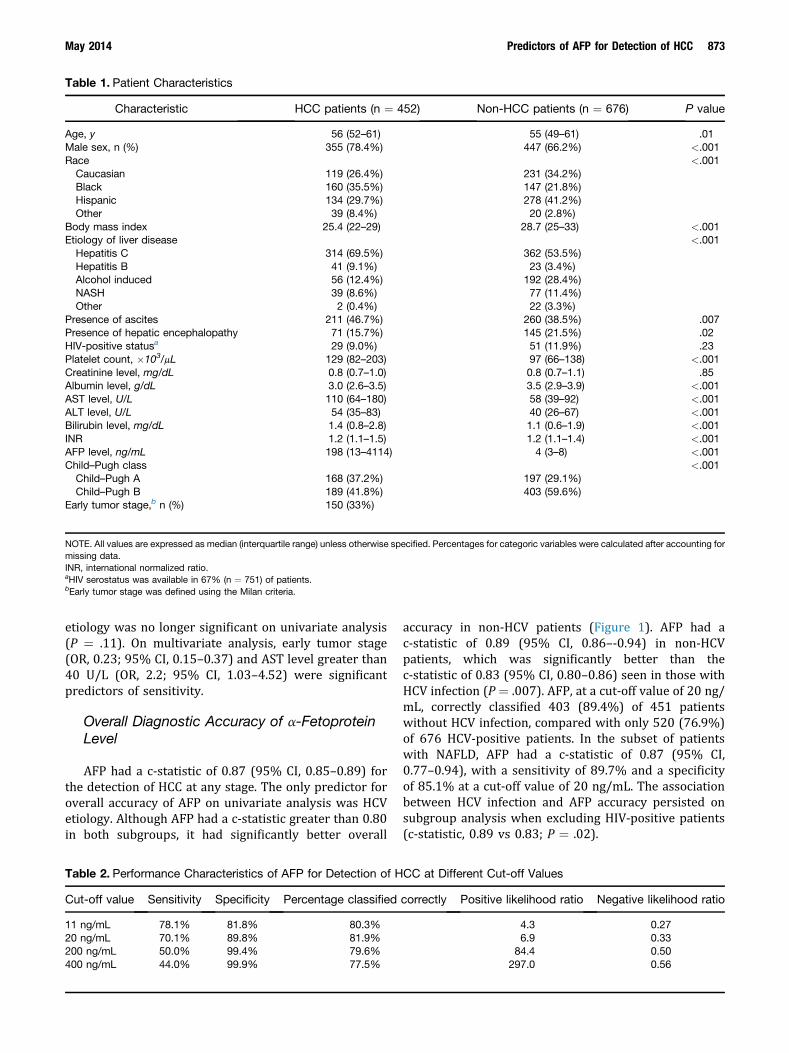
Table 1. Patient Characteristics
Characteristic HCC patients (n ¼ 452) Non-HCC patients (n ¼ 676) P value
Age, y 56 (52–61) 55 (49–61) .01Male sex, n (%) 355 (78.4%) 447 (66.2%) <.001Race <.001
Caucasian 119 (26.4%) 231 (34.2%)Black 160 (35.5%) 147 (21.8%)Hispanic 134 (29.7%) 278 (41.2%)Other 39 (8.4%) 20 (2.8%)
Body mass index 25.4 (22–29) 28.7 (25–33) <.001Etiology of liver disease <.001
Hepatitis C 314 (69.5%) 362 (53.5%)Hepatitis B 41 (9.1%) 23 (3.4%)Alcohol induced 56 (12.4%) 192 (28.4%)NASH 39 (8.6%) 77 (11.4%)Other 2 (0.4%) 22 (3.3%)
Presence of ascites 211 (46.7%) 260 (38.5%) .007Presence of hepatic encephalopathy 71 (15.7%) 145 (21.5%) .02HIV-positive statusa 29 (9.0%) 51 (11.9%) .23Platelet count, �103/mL 129 (82–203) 97 (66–138) <.001Creatinine level, mg/dL 0.8 (0.7–1.0) 0.8 (0.7–1.1) .85Albumin level, g/dL 3.0 (2.6–3.5) 3.5 (2.9–3.9) <.001AST level, U/L 110 (64–180) 58 (39–92) <.001ALT level, U/L 54 (35–83) 40 (26–67) <.001Bilirubin level, mg/dL 1.4 (0.8–2.8) 1.1 (0.6–1.9) <.001INR 1.2 (1.1–1.5) 1.2 (1.1–1.4) <.001AFP level, ng/mL 198 (13–4114) 4 (3–8) <.001Child–Pugh class <.001
Child–Pugh A 168 (37.2%) 197 (29.1%)Child–Pugh B 189 (41.8%) 403 (59.6%)
Early tumor stage,b n (%) 150 (33%)
NOTE. All values are expressed as median (interquartile range) unless otherwise specified. Percentages for categoric variables were calculated after accounting formissing data.INR, international normalized ratio.aHIV serostatus was available in 67% (n ¼ 751) of patients.bEarly tumor stage was defined using the Milan criteria.
May 2014 Predictors of AFP for Detection of HCC 873
etiology was no longer significant on univariate analysis(P ¼ .11). On multivariate analysis, early tumor stage(OR, 0.23; 95% CI, 0.15–0.37) and AST level greater than40 U/L (OR, 2.2; 95% CI, 1.03–4.52) were significantpredictors of sensitivity.
Overall Diagnostic Accuracy of a-FetoproteinLevel
AFP had a c-statistic of 0.87 (95% CI, 0.85–0.89) forthe detection of HCC at any stage. The only predictor foroverall accuracy of AFP on univariate analysis was HCVetiology. Although AFP had a c-statistic greater than 0.80in both subgroups, it had significantly better overall
Table 2. Performance Characteristics of AFP for Detection of H
Cut-off value Sensitivity Specificity Percentage classified
11 ng/mL 78.1% 81.8% 80.3%20 ng/mL 70.1% 89.8% 81.9%200 ng/mL 50.0% 99.4% 79.6%400 ng/mL 44.0% 99.9% 77.5%
accuracy in non-HCV patients (Figure 1). AFP had ac-statistic of 0.89 (95% CI, 0.86–-0.94) in non-HCVpatients, which was significantly better than thec-statistic of 0.83 (95% CI, 0.80–0.86) seen in those withHCV infection (P ¼ .007). AFP, at a cut-off value of 20 ng/mL, correctly classified 403 (89.4%) of 451 patientswithout HCV infection, compared with only 520 (76.9%)of 676 HCV-positive patients. In the subset of patientswith NAFLD, AFP had a c-statistic of 0.87 (95% CI,0.77–0.94), with a sensitivity of 89.7% and a specificityof 85.1% at a cut-off value of 20 ng/mL. The associationbetween HCV infection and AFP accuracy persisted onsubgroup analysis when excluding HIV-positive patients(c-statistic, 0.89 vs 0.83; P ¼ .02).
CC at Different Cut-off Values
correctly Positive likelihood ratio Negative likelihood ratio
4.3 0.276.9 0.33
84.4 0.50297.0 0.56
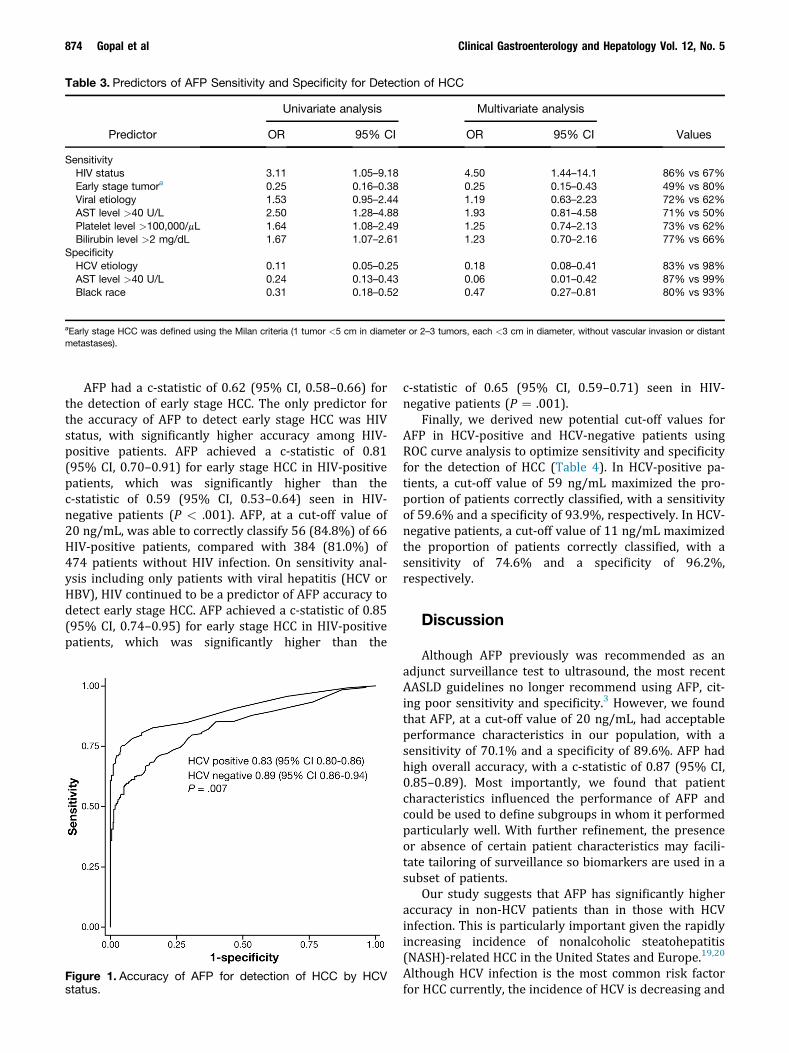
Table 3. Predictors of AFP Sensitivity and Specificity for Detection of HCC
Predictor
Univariate analysis Multivariate analysis
ValuesOR 95% CI OR 95% CI
SensitivityHIV status 3.11 1.05–9.18 4.50 1.44–14.1 86% vs 67%Early stage tumora 0.25 0.16–0.38 0.25 0.15–0.43 49% vs 80%Viral etiology 1.53 0.95–2.44 1.19 0.63–2.23 72% vs 62%AST level >40 U/L 2.50 1.28–4.88 1.93 0.81–4.58 71% vs 50%Platelet level >100,000/mL 1.64 1.08–2.49 1.25 0.74–2.13 73% vs 62%Bilirubin level >2 mg/dL 1.67 1.07–2.61 1.23 0.70–2.16 77% vs 66%
SpecificityHCV etiology 0.11 0.05–0.25 0.18 0.08–0.41 83% vs 98%AST level >40 U/L 0.24 0.13–0.43 0.06 0.01–0.42 87% vs 99%Black race 0.31 0.18–0.52 0.47 0.27–0.81 80% vs 93%
aEarly stage HCC was defined using the Milan criteria (1 tumor <5 cm in diameter or 2–3 tumors, each <3 cm in diameter, without vascular invasion or distantmetastases).
874 Gopal et al Clinical Gastroenterology and Hepatology Vol. 12, No. 5
AFP had a c-statistic of 0.62 (95% CI, 0.58–0.66) forthe detection of early stage HCC. The only predictor forthe accuracy of AFP to detect early stage HCC was HIVstatus, with significantly higher accuracy among HIV-positive patients. AFP achieved a c-statistic of 0.81(95% CI, 0.70–0.91) for early stage HCC in HIV-positivepatients, which was significantly higher than thec-statistic of 0.59 (95% CI, 0.53–0.64) seen in HIV-negative patients (P < .001). AFP, at a cut-off value of20 ng/mL, was able to correctly classify 56 (84.8%) of 66HIV-positive patients, compared with 384 (81.0%) of474 patients without HIV infection. On sensitivity anal-ysis including only patients with viral hepatitis (HCV orHBV), HIV continued to be a predictor of AFP accuracy todetect early stage HCC. AFP achieved a c-statistic of 0.85(95% CI, 0.74–0.95) for early stage HCC in HIV-positivepatients, which was significantly higher than the
Figure 1. Accuracy of AFP for detection of HCC by HCVstatus.
c-statistic of 0.65 (95% CI, 0.59–0.71) seen in HIV-negative patients (P ¼ .001).
Finally, we derived new potential cut-off values forAFP in HCV-positive and HCV-negative patients usingROC curve analysis to optimize sensitivity and specificityfor the detection of HCC (Table 4). In HCV-positive pa-tients, a cut-off value of 59 ng/mL maximized the pro-portion of patients correctly classified, with a sensitivityof 59.6% and a specificity of 93.9%, respectively. In HCV-negative patients, a cut-off value of 11 ng/mL maximizedthe proportion of patients correctly classified, with asensitivity of 74.6% and a specificity of 96.2%,respectively.
Discussion
Although AFP previously was recommended as anadjunct surveillance test to ultrasound, the most recentAASLD guidelines no longer recommend using AFP, cit-ing poor sensitivity and specificity.3 However, we foundthat AFP, at a cut-off value of 20 ng/mL, had acceptableperformance characteristics in our population, with asensitivity of 70.1% and a specificity of 89.6%. AFP hadhigh overall accuracy, with a c-statistic of 0.87 (95% CI,0.85–0.89). Most importantly, we found that patientcharacteristics influenced the performance of AFP andcould be used to define subgroups in whom it performedparticularly well. With further refinement, the presenceor absence of certain patient characteristics may facili-tate tailoring of surveillance so biomarkers are used in asubset of patients.
Our study suggests that AFP has significantly higheraccuracy in non-HCV patients than in those with HCVinfection. This is particularly important given the rapidlyincreasing incidence of nonalcoholic steatohepatitis(NASH)-related HCC in the United States and Europe.19,20
Although HCV infection is the most common risk factorfor HCC currently, the incidence of HCV is decreasing and
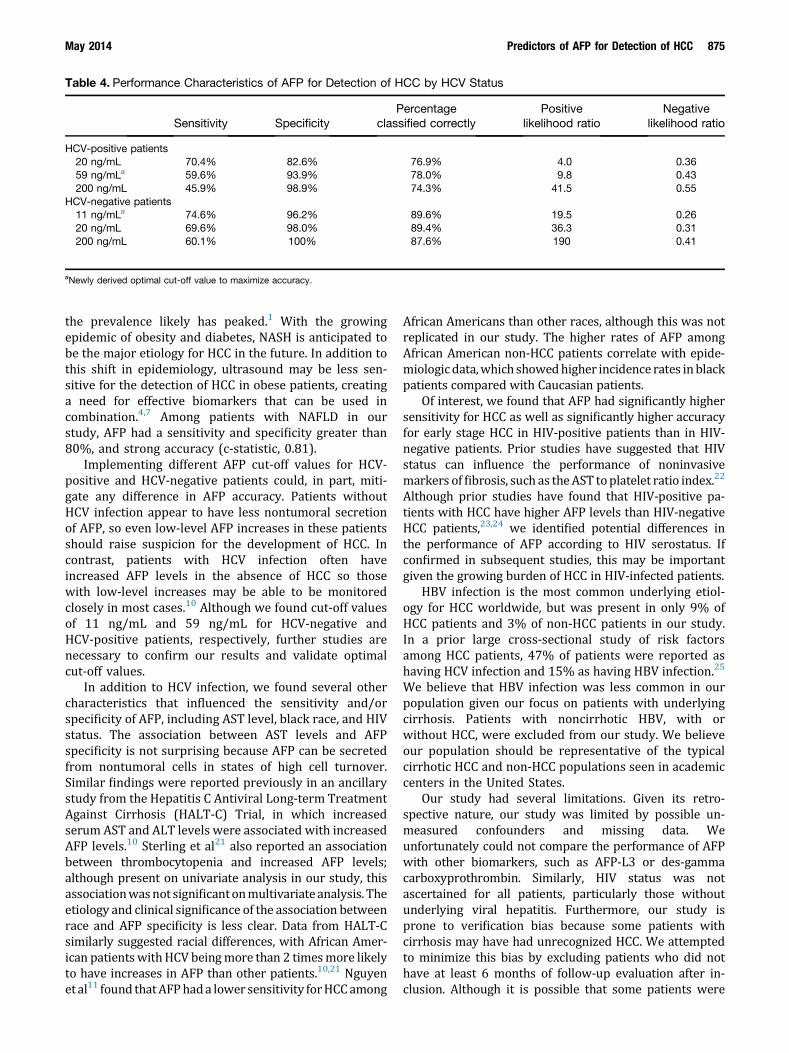
Table 4. Performance Characteristics of AFP for Detection of HCC by HCV Status
Sensitivity SpecificityPercentage
classified correctlyPositive
likelihood ratioNegative
likelihood ratio
HCV-positive patients20 ng/mL 70.4% 82.6% 76.9% 4.0 0.3659 ng/mLa 59.6% 93.9% 78.0% 9.8 0.43200 ng/mL 45.9% 98.9% 74.3% 41.5 0.55
HCV-negative patients11 ng/mLa 74.6% 96.2% 89.6% 19.5 0.2620 ng/mL 69.6% 98.0% 89.4% 36.3 0.31200 ng/mL 60.1% 100% 87.6% 190 0.41
aNewly derived optimal cut-off value to maximize accuracy.
May 2014 Predictors of AFP for Detection of HCC 875
the prevalence likely has peaked.1 With the growingepidemic of obesity and diabetes, NASH is anticipated tobe the major etiology for HCC in the future. In addition tothis shift in epidemiology, ultrasound may be less sen-sitive for the detection of HCC in obese patients, creatinga need for effective biomarkers that can be used incombination.4,7 Among patients with NAFLD in ourstudy, AFP had a sensitivity and specificity greater than80%, and strong accuracy (c-statistic, 0.81).
Implementing different AFP cut-off values for HCV-positive and HCV-negative patients could, in part, miti-gate any difference in AFP accuracy. Patients withoutHCV infection appear to have less nontumoral secretionof AFP, so even low-level AFP increases in these patientsshould raise suspicion for the development of HCC. Incontrast, patients with HCV infection often haveincreased AFP levels in the absence of HCC so thosewith low-level increases may be able to be monitoredclosely in most cases.10 Although we found cut-off valuesof 11 ng/mL and 59 ng/mL for HCV-negative andHCV-positive patients, respectively, further studies arenecessary to confirm our results and validate optimalcut-off values.
In addition to HCV infection, we found several othercharacteristics that influenced the sensitivity and/orspecificity of AFP, including AST level, black race, and HIVstatus. The association between AST levels and AFPspecificity is not surprising because AFP can be secretedfrom nontumoral cells in states of high cell turnover.Similar findings were reported previously in an ancillarystudy from the Hepatitis C Antiviral Long-term TreatmentAgainst Cirrhosis (HALT-C) Trial, in which increasedserum AST and ALT levels were associated with increasedAFP levels.10 Sterling et al21 also reported an associationbetween thrombocytopenia and increased AFP levels;although present on univariate analysis in our study, thisassociationwasnot significantonmultivariateanalysis. Theetiology and clinical significance of the association betweenrace and AFP specificity is less clear. Data from HALT-Csimilarly suggested racial differences, with African Amer-ican patientswithHCV beingmore than 2 timesmore likelyto have increases in AFP than other patients.10,21 Nguyenetal11 found thatAFPhada lower sensitivity forHCCamong
African Americans than other races, although this was notreplicated in our study. The higher rates of AFP amongAfrican American non-HCC patients correlate with epide-miologicdata,which showedhigher incidence rates inblackpatients compared with Caucasian patients.
Of interest, we found that AFP had significantly highersensitivity for HCC as well as significantly higher accuracyfor early stage HCC in HIV-positive patients than in HIV-negative patients. Prior studies have suggested that HIVstatus can influence the performance of noninvasivemarkers offibrosis, such as theAST toplatelet ratio index.22
Although prior studies have found that HIV-positive pa-tients with HCC have higher AFP levels than HIV-negativeHCC patients,23,24 we identified potential differences inthe performance of AFP according to HIV serostatus. Ifconfirmed in subsequent studies, this may be importantgiven the growing burden of HCC in HIV-infected patients.
HBV infection is the most common underlying etiol-ogy for HCC worldwide, but was present in only 9% ofHCC patients and 3% of non-HCC patients in our study.In a prior large cross-sectional study of risk factorsamong HCC patients, 47% of patients were reported ashaving HCV infection and 15% as having HBV infection.25
We believe that HBV infection was less common in ourpopulation given our focus on patients with underlyingcirrhosis. Patients with noncirrhotic HBV, with orwithout HCC, were excluded from our study. We believeour population should be representative of the typicalcirrhotic HCC and non-HCC populations seen in academiccenters in the United States.
Our study had several limitations. Given its retro-spective nature, our study was limited by possible un-measured confounders and missing data. Weunfortunately could not compare the performance of AFPwith other biomarkers, such as AFP-L3 or des-gammacarboxyprothrombin. Similarly, HIV status was notascertained for all patients, particularly those withoutunderlying viral hepatitis. Furthermore, our study isprone to verification bias because some patients withcirrhosis may have had unrecognized HCC. We attemptedto minimize this bias by excluding patients who did nothave at least 6 months of follow-up evaluation after in-clusion. Although it is possible that some patients were

876 Gopal et al Clinical Gastroenterology and Hepatology Vol. 12, No. 5
diagnosed with HCC at outside institutions, we believethis was unlikely given that Parkland Hospital, as thesafety-net health system for Dallas County, is the onlyoption for indigent patients. Another limitation of ourstudy was that we only assessed the accuracy of AFP atone point in time. It is likely that longitudinal assessmentof AFP levels, including changes over time, may alter itsperformance characteristics.26,27 Finally, our study is notgeneralizable to groups not represented in this study,including Asian patients. Overall, we believe that ourstudy’s limitations outweigh its notable strengths,including its well-characterized cohort who all had un-derlying cirrhosis, its racially diverse population includingboth African American and Hispanic patients, and itsrelatively large sample size.
In conclusion, we found that several patient charac-teristics influence the performance of AFP for thedetection of HCC in patients with cirrhosis. The higheraccuracy of AFP for detecting HCC among patientswithout HCV infection is particularly important given theincreasing incidence of NASH in the United States andEurope. A lower AFP cut-off value should be used in thissubgroup of patients to maximize its sensitivity andspecificity. Further studies, specifically focusing on pa-tients with NASH, are necessary to confirm our findingsand further define the benefit of AFP when used incombination with ultrasound.
References
1. El-Serag HB. Epidemiology of viral hepatitis and hepatocellularcarcinoma. Gastroenterology 2012;142:1264–1273.
2. El-Serag HB, Lau M, Eschbach K, et al. Epidemiology of he-patocellular carcinoma in Hispanics in the United States. ArchIntern Med 2007;167:1983–1989.
3. Bruix J, Sherman M. Management of hepatocellular carcinoma:an update. Hepatology 2010;53:1–35.
4. Finberg HJ. Whither (wither?) the ultrasound specialist?J Ultrasound Med 2004;23:1543–1547.
5. Singal A, Volk ML, Waljee A, et al. Meta-analysis: surveillancewith ultrasound for early-stage hepatocellular carcinoma in pa-tients with cirrhosis. Aliment Pharmacol Ther 2009;30:37–47.
6. Singal AG, Conjeevaram HS, Volk ML, et al. Effectiveness ofhepatocellular carcinoma surveillance in patients with cirrhosis.Cancer Epidemiol Biomarkers Prev 2012;21:793–799.
7. Singal AG, Nehra M, Adams-Huet B, et al. Detection of hepa-tocellular carcinoma at advanced stages among patients in theHALT-C trial: where did surveillance fail? Am J Gastroenterol2013;108:425–432.
8. Gupta S, Bent S, Kohlwes J. Test characteristics of alpha-fetoprotein for detecting hepatocellular carcinoma in patientswith hepatitis C. A systematic review and critical analysis. AnnIntern Med 2003;139:46–50.
9. Takikawa Y, Suzuki K. Is AFP a new reliable marker of liverregeneration in acute hepatic failure? J Gastroenterol 2002;37:681–682.
10. Di Bisceglie AM, Sterling RK, Chung RT, et al. Serum alpha-fetoprotein levels in patients with advanced hepatitis C: resultsfrom the HALT-C Trial. J Hepatol 2005;43:434–441.
11. Nguyen MH, Garcia RT, Simpson PW, et al. Racial differences ineffectiveness of alpha-fetoprotein for diagnosis of hepatocellular
carcinoma in hepatitis C virus cirrhosis. Hepatology 2002;36:410–417.
12. VolkML,HernandezJC, SuGL, et al. Risk factors for hepatocellularcarcinoma may impair the performance of biomarkers: a compar-ison of AFP, DCP, and AFP-L3. Cancer Biomark 2007;3:79–87.
13. Cedrone A, Covino M, Caturelli E, et al. Utility of alpha-fetoprotein (AFP) in the screening of patients with virus-relatedchronic liver disease: does different viral etiology influenceAFP levels in HCC? A study in 350 western patients. Hep-atogastroenterology 2000;47:1654–1658.
14. Trevisani F, D’Intino PE, Morselli-Labate AM, et al. Serum alpha-fetoprotein for diagnosis of hepatocellular carcinoma in patientswith chronic liver disease: influence of HBsAg and anti-HCVstatus. J Hepatol 2001;34:570–575.
15. Yang JD, Kim WR, Coelho R, et al. Cirrhosis is present in mostpatients with hepatitis B and hepatocellular carcinoma. ClinGastroenterol Hepatol 2011;9:64–70.
16. Singal AG, Yopp AC, Gupta S, et al. Failure rates in the hepa-tocellular carcinoma surveillance process. Cancer Prev Res(Phila) 2012;5:1124–1130.
17. Nehra MS, Ma Y, Clark C, et al. Use of administrative claimsdata for identifying patients with cirrhosis. J Clin Gastroenterol2013;47:e50–e54.
18. Mossman D, Somoza E. ROC curves, test accuracy, and thedescription of diagnostic tests. J Neuropsychiatry Clin Neurosci1991;3:330–333.
19. Bellentani S, Scaglioni F, Marino M, et al. Epidemiology of non-alcoholic fatty liver disease. Dig Dis 2010;28:155–161.
20. Starley BQ, Calcagno CJ, Harrison SA. Nonalcoholic fatty liverdisease and hepatocellular carcinoma: a weighty connection.Hepatology 2010;51:1820–1832.
21. Sterling RK, Wright EC, Morgan TR, et al. Frequency of elevatedhepatocellular carcinoma (HCC) biomarkers in patients withadvanced hepatitis C. Am J Gastroenterol 2012;107:64–74.
22. Singal AG, Thomassen LV, Gretch DR, et al. Use of the AST toplatelet ratio index in HCV/HIV co-infected patients. AlimentPharmacol Ther 2011;33:566–577.
23. Brau N, Fox RK, Xiao P, et al. Presentation and outcome ofhepatocellular carcinoma in HIV-infected patients: a U.S.Canadian multicenter study. J Hepatol 2007;47:527–537.
24. Yopp AC, Subramanian M, Jain MK, et al. Presentation, treat-ment, and clinical outcomes of patients with hepatocellularcarcinoma, with and without human immunodeficiency virusinfection. Clin Gastroenterol Hepatol 2012;10:1284–1290.
25. Di Bisceglie AM, Lyra AC, Schwartz M, et al. Hepatitis C-relatedhepatocellular carcinoma in the United States: influence ofethnic status. Am J Gastroenterol 2003;98:2060–2063.
26. Lee E, Edward S, Singal AG, et al. Improving screening for he-patocellular carcinoma by incorporating data on levels of alpha-fetoprotein, over time. Clin Gastroenterol Hepatol 2013;11:437–440.
27. Singal AG, Mukherjee A, Elmunzer BJ, et al. Machine learningalgorithms outperform conventional regression models in pre-dicting development of hepatocellular carcinoma. Am J Gas-troenterol 2013;108:1723–1730.
Reprint requestsAddress requests for reprints to: Amit G. Singal, MD, MS, Dedman Scholar ofClinical Care, Division of Digestive and Liver Diseases, University of TexasSouthwestern, 5959 Harry Hines Boulevard, PO Box 1, Suite 420, Dallas, Texas75390-8887. e-mail: [email protected]; fax: (214) 645-6114.

May 2014 Predictors of AFP for Detection of HCC 877
Conflicts of interestThe authors disclose no conflicts.
FundingSupported by UT-STAR, National Institutes of Health/National Center forAdvancing Translational Science (KL2 TR000453), National Institutes of Health/National Center for Advancing Translational Science (UL1-TR000451), and anAmerican College of Gastroenterology Junior Faculty Development Award
(A.G.S.); and funded by a Veterans Affairs Health Services Research & Devel-opment Career Development Award 1IK2HX000775 (A.K.W.). The content issolely the responsibility of the authors and does not necessarily represent theofficial views of UT-STAR, the University of Texas Southwestern MedicalCenter and its affiliated academic and health care centers, the National Centerfor Advancing Translational Sciences, the Veterans Affairs, or the National In-stitutes of Health. No funding bodies had any role in the study design, datacollection and analysis, decision to publish, or preparation of the manuscript.
Recommended

















