FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
Agradecimentos
Quero agradecer a todos aqueles que me apoiaram e que de alguma forma
contribuíram para a realização deste trabalho: aos meus colegas da Unidade de
Genética Molecular. Ao professor Doutor Mário Sousa pela sua orientação e
disponibilidade, à Dra. Rosário Santos por me ter possibilitado a realização da minha
tese na Unidade de Genética Molecular, e especialmente ao Dr. Jorge Oliveira por
todo o seu apoio, conselhos e disponibilidade.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
ABSTRACT:
Cornelia de Lange Syndrome [CdLS (MIM#122470)] is a rare multisystemic disorder,
characterized by a typical phenotype that includes distinctive facial dysmorphism,
hirsutism, growth and psychomotor developmental delay, limb defects, multiple organ
system problems such as frequent gastrointestinal and congenital heart defects. CdLS
is essentially caused by defects in NIPBL and SMC1A genes (~50% and 5% of cases,
respectively), but less frequently mutations have been also described in other genes
(SMC3, HDCA8, RAD21). This genetic heterogeneity in CdLS is partially explained by
a close functional relationship at the cellular level, since all these genes encode for
proteins involved in the sister chromatid cohesion complex. The molecular and clinical
characterization of CdLS patients was initiated at the national level in 2005. This initial
part of the work enabled the detailed characterization of thirteen CdLS patients with
novel NIPBL mutations, and the development of a locus specific database for this gene
(Oliveira et al., 2010).
The present work intended to unfold new molecular findings in the remaining 40 CdLS
patients of our cohort. Molecularly unresolved patients were also analyzed by other
techniques such as multiplex ligation-dependent probe amplification technique for
NIPBL gene, and by high resolution melting curve analysis (hrMCA) for SMC1A. The
analysis of NIPBL gene identified eight mutations previously reported in the literature
(including a case with suspected somatic mosaicism), three novel mutations (c.86del,
c.6983C>G and c.7307C>T) and two large deletions. The development of hrMCA
applied to SMC1A is a fast and cost-effective scanning method, and allowed the
identification of one mutation (c.1487G>A).
Overall, mutations in SMC1A and NIPBL have been identified in 51% of the
Portuguese CdLS patients studied by our group. The combination of different
experimental procedure was essential for attaining an enhanced mutation detection
rate in CdLS. Considering the distinct gene mutation detection rates a flowchart is
proposed for the genetic molecular diagnostic of CdLS. Due to recent discovery of new
genes involved in the disease, and considering that several patients are still
molecularly uncharacterized, its plausible that in a near future new genetics causes for
CdLS will be identified.
Keywords: Cornelia de Lange, CdLS, NIPBL, SMC1A, hrMCA, MLPA, Cohesin,
Mutation screening
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
RESUMO:
A Síndrome Cornélia de Lange [CdLS (MIM#122470)] é uma doença multissistémica
rara, caracterizada por um fenótipo típico que inclui um dismorfismo facial
característico, hirsutismo, atraso no crescimento e desenvolvimento psicomotor,
defeitos nos membros, problemas associados a múltiplos sistemas de órgãos, sendo
os mais frequentes problemas cardíacos, e refluxo gastrointestinal. A CdLS está
associada a defeitos nos genes NIPBL e SMC1A genes (identificados em ~50% e 5%
dos doentes, respectivamente), mas outras mutações mais raras foram descritos em
outros genes (SMC3, HDCA8, RAD21). A heterogeneidade genética nesta síndrome é
explicada ao nível celular, pela proximidade funcional das proteínas codificadas por
estes genes, estando envolvidas no complexo das coesinas que unem os cromatídeos
irmãos. Em 2005, iniciou-se em Portugal a caracterização clínica e molecular dos
doentes com CdLS. A parte inicial deste projecto permitiu a descrição detalhada de
treze doentes com novas mutações no gene NIPBL e o desenvolvimento de uma base
de dados de mutações específica para este locus (Oliveira et al., 2010).
Com a realização desta dissertação de mestrado pretende-se contribuir na
caracterização molecular dos restantes 40 doentes Portugueses do grupo de estudo.
Os casos não esclarecidos molecularmente foram analisados por outras técnicas
nomeadamente, multiplex ligation-dependent probe amplification technique aplicada ao
gene NIPBL, e por high resolution melting curve analysis (hrMCA) desenvolvida para o
gene SMC1A. A análise do gene NIPBL permitiu a identificação de oito mutações
anteriormente descritas na literatura (incluindo um caso com suspeita de mosaicismo
somático), três novas mutações (c.86del, c.6983C>G e c.7307C>T), bem como duas
grandes delecções neste gene. O desenvolvimento da técnica hrMCA aplicada ao
gene SMC1A demonstrou ser eficaz, tratando-se de um método rápido e rentável,
tendo permitido a identificação de uma mutação (c.1487G>A).
Considerando todos os dados obtidos, foram identificadas mutações em 51% dos
doentes Portugueses com CdLS. A utilização de diferentes técnicas moleculares foi
essencial para atingir uma taxa de detecção de mutações mais elevada. Devido à
recente descoberta de dois genes envolvidos na doença, (HDCA8, RAD21), e
existindo ainda uma percentagem razoável de casos sem mutação identificada, é
possível que novas causas genéticas de CdLS sejam identificadas neste doentes.
Palavras-Chave: Cornelia de Lange, CdLS, NIPBL, SMC1A, Coesina, hrMCA, MLPA,
rastreio de mutações
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
Index
1. Introduction ..................................................................................................... 1
1.1. Cornelia de Lange Syndrome .................................................................. 1
1.1.1. History and Nomenclature ................................................................ 1
1.1.2. Clinical features ................................................................................ 2
1.1.3. Etiology............................................................................................. 3
1.2. Biochemistry basis of CdLS - the cohesin complex .................................. 3
1.3. Genetics of CdLS .................................................................................... 6
1.3.1. NIPBL gene ...................................................................................... 6
1.3.2. SMC1A gene .................................................................................... 7
1.3.3. SMC3 gene ...................................................................................... 9
1.3.4. HDAC8 gene .................................................................................... 9
2. Objectives ..................................................................................................... 10
3. Materials and Methods ................................................................................. 11
3.1. Patients ................................................................................................. 11
3.2. Preparation of biological samples .......................................................... 12
3.2.1. DNA extraction method ................................................................... 12
3.2.2. RNA extraction method ................................................................... 12
3.2.3. Nucleic acid quantification .............................................................. 12
3.2.4. RNA conversion to cDNA ............................................................... 13
3.2.5. Aliquots preparation ........................................................................ 13
3.3. DNA amplification by PCR ..................................................................... 13
3.3.1. Oligonucleotides design .................................................................. 14
3.3.2. PCR mixture and thermocycling profiles ......................................... 15
3.4. Agarose gel electrophoresis .................................................................. 17
3.5. PCR purification ..................................................................................... 18
3.6. Sanger Sequencing ............................................................................... 18
3.6.1. Sequencing reaction ....................................................................... 18
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
3.6.2. Sequencing PCR purification .......................................................... 19
3.6.3. Sequencing analysis ....................................................................... 19
3.7. Multiplex ligation probe amplification ..................................................... 19
3.8. High Resolution Melting Curve Analysis ................................................ 20
3.9. Bioinformatics and databases ................................................................ 22
3.9.1. Missense mutations analysis .......................................................... 22
3.9.2. Algorithms for evaluating splicing.................................................... 22
4. Results ......................................................................................................... 24
4.1. NIPBL gene sequencing ........................................................................ 24
4.1.1. Mutations causing premature stop codons. ..................................... 27
4.1.2. In-frame deletion ............................................................................. 28
4.1.3. Missense mutations ........................................................................ 28
4.1.4. Splicing mutations .......................................................................... 31
4.1.5. Variant with unknown significance .................................................. 32
4.2. Large mutations detected in NIPBL gene ............................................... 33
4.3. Mutation screening for SMC1A gene ..................................................... 34
5. Discussion .................................................................................................... 38
5.1. Mutations identified in NIPBL ................................................................. 38
5.1.1. Detection of large NIPBL deletions by MLPA .................................. 40
5.1.2. Somatic mosaicism ......................................................................... 41
5.1.3. Novel silent polymorphism .............................................................. 42
5.2. Implementation of hrMCA for SMC1A .................................................... 42
5.3. Mutation detection rate .......................................................................... 43
5.4. Bioinformatic tools and databases ......................................................... 44
5.5. Procedure for the molecular diagnostic of CdLS patients ....................... 45
5.6. Future perspectives ............................................................................... 47
6. Bibliography .................................................................................................. 48
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
Tables and Figures Index
Figure 1.1 – Schematic representation of the cohesin complex……………………4
Table 1.1- Members and regulators of the cohesin complex……………………….5
Figure 1.2 – NIPBL-LOVD database content analysis………………………………7
Table 3.1: PCR program for NIPBL amplification…………………………………..16
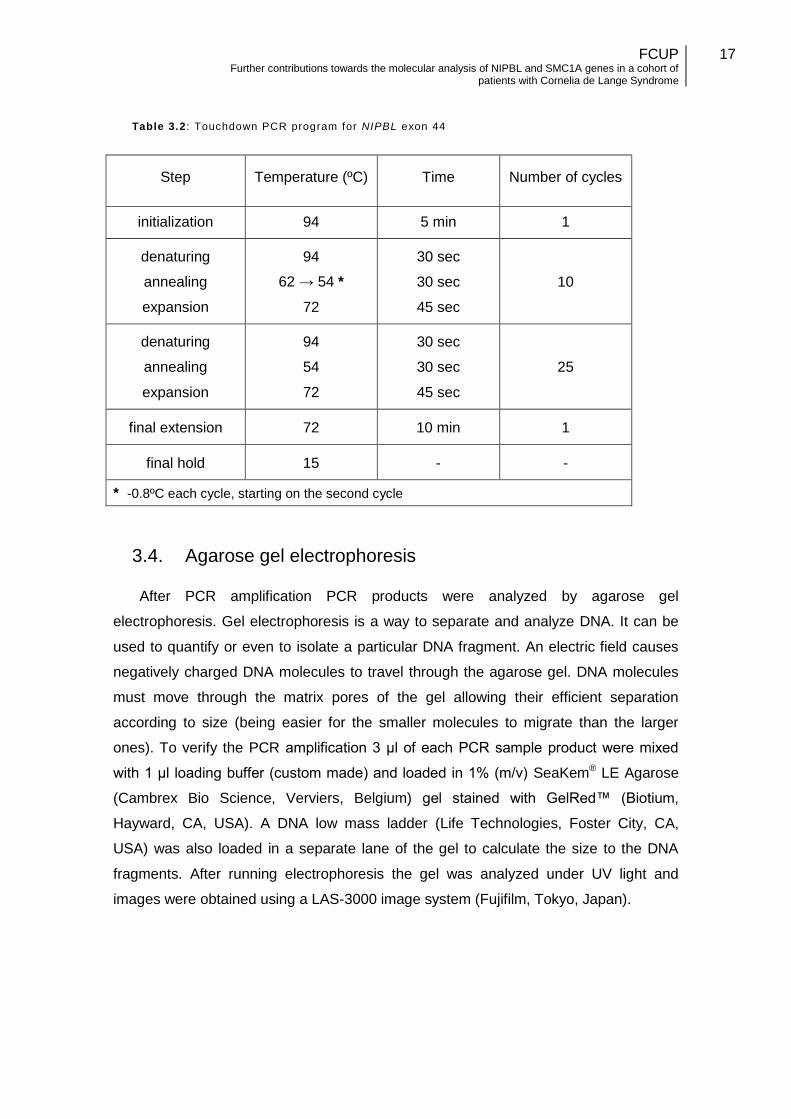
Table 3.2: Touchdown PCR program for NIPBL exon 44…………………………17
Table 3.3: High Resolution Melting Curve Analysis for SMC1A gene……………21
Figure 4.1: Screening for NIPBL gene mutations by sequencing…………………24
Table 4.1: Mutations found in NIPBL gene………………………………………………...25
Figure 4.2: Representation of the NIPBL gene……………………………………………26
Figure 4.3: Sequencing electropherogram of a novel small deletion……………….…..27
Figure 4.4: Suspected mosaicism mutation c.1885C>T…………………………….……28
Figure 4.5: Sequencing electropherograms of two missense mutations………….……29
Table 4.2: Evaluation of missense variant in terms of pathogenicity……………………30
Figure 4.6: Protein sequence alignments of delagin from several organisms………….30
Figure 4.7: Evaluation of P46 splicing mutation c.64+1G>A……………………………..31
Figure 4.8: Evaluation of patient P20 splicing mutation c.6763+5G>T…………………32
Figure 4.9: Variation detected in patient P44………………………………………………33
Figure 4.10: cDNA electropherogram analysis……………………………………………33
Figure 4.11: Screening of NIPBL mutations by MLPA……………………………………33
Figure 4.12: MLPA results of patient P32………………………………………………….34
Figure 4.13: Strategy for SMC1A mutation screening by hrMCA………………………35 Figure 4.14: Normalized High Resolut ion Melting Curves, for amplicons of exons 1 to 6a……………………………………………………………………………………………….35
Figure 4.15: Normalized High Resolution Melting Curves, for amplicons of exons 6b to 25………………………………………………………………………………………………36
Figure 4.16: SMC1A missense mutation, detected through High Resolution Melting Curve Analysis………………………………………………………………………….........37
Figure 5.1: Representation of the NIPBL gene, with the distribution of all known point and small del/ins mutations throughout the gene…………………………………………39
Table 5.1: Overall results of the genetic analysis of NIPBL and SMC1A genes in the Portuguese CdLS patient cohort…………………………………………………………….44
Figure 5.2: Flowchart for a proposed procedure for the genetic molecular diagnostic of CdLS……………………………………………………………………………………………46
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
Abreviations:
cDNA - Complementary DNA
CdLS - Cornelia de Lange Syndrome
dATP - Deoxyadenosine triphosphate
cCTP - Deoxycytidine triphosphate
dGTP - Deoxyguanosine triphosphate
dTTP - Deoxythymidine triphosphate
dNTP - Deoxyribonucleotide
DNA - Deoxyribonucleic acid
dbSNP - Single Nucleotide Polymorphism Database
gDNA - genomic DNA
hrMCA - High Resolution Melting Curve Analysis
MLPA - Multiplex Ligand Probe Amplification
RNA - Ribonucleic Acid
LSDB - Locus Specific Database
NCBI - National Center for Biotechnology Information
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
1
1. Introduction
1.1. Cornelia de Lange Syndrome
Cornelia de Lange Syndrome (CdLS) is a rare, multisystemic developmental
disorder that can be characterized by a typical phenotype, although it can be highly
variable between affected individuals, depending on the severity (Krantz et al., 2004). It
has an estimated prevalence of about 1:10 000 individuals (Kline et al., 2007).
However, since additional patients with milder CdLS phenotypes have been reported in
the literature its actual incidence and prevalence may be more common than initially
suspected.
1.1.1. History and Nomenclature
The first known description of CdLS was made by Vrolik in 1849, who reported a
case as an extreme example of oligodactily (Oostra et al., 1994). In 1916, a German
physician named Winfried Brachmann made a detailed description of a case of a
patient that had died from pneumonia at 19 days of age, which presented CdLS
features (symmetric monodactyly, antecubital webbing, dwarfism, cervical ribs, and
hirsutism) (Deardorff et al., 2011; Johns et al., 2012). Seventeen years later, Cornelia
Catharina de Lange, a Dutch pediatrician described two unrelated patients that shared
similar features. Both cases had mental retardation, microcephaly and unusual facies
that resembled each other. She described these cases in detail and proposed a
diagnostic criteria, reporting these cases as typus degenerativus amstelodamensis
(Amsterdam type degeneration), after the city that she worked in (de Lange 1933;
Kumar et al., 1985).
This syndrome is usually known as Cornelia de Lange Syndrome, honoring the
pediatrician’s contribution to the characterization of the disorder, but can be also known
as Brachmann de Lange syndrome, Amsterdam type degeneration or Amsterdam
dwarfism (Johns et al., 2012).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
2
1.1.2. Clinical features
CdLS phenotype includes distinctive facial dysmorphic features, hirsutism, growth
and psychomotor developmental delay, limb abnormalities, and relatively frequent
gastrointestinal and congenital heart defects (Krantz et al., 2004; Tonkin et al., 2004).
This syndrome is usually sporadic, but there are some familial occurrences reported in
about 1% of cases (Lalatta et al., 2007).
The characteristic dysmorphic facial features, are the most consistent and
recognizable clinical findings in CdLS (Liu and Krantz, 2009). This include arched
eyebrows with synophrys (and sometimes a severe ptosis), short neck, hirsute
forehead, long and thick eyelashes, and a long and smooth philtrum (Kline et al., 2007).
Ears may be lowset and posteriorly rotated, and the mid face flattened with depressed
nasal bridge. The patients can also have upper thin lips, high palate, broadly spaced
teeth and micrognatia (Liu and Krantz, 2009).
Limb defects help to corroborate a CdLS diagnosis (Kline et al., 2007). These
findings can range from small hands and feet, to severe anomalies of the upper limbs.
The majority of CdLS cases can have brachydactyly and clinodactyly, a shorter first
metacarpal, and proximally placed thumbs, while the most severe cases can have
oligodactyly, ulnar deficiencies or absent forearms (Kline et al., 2007; Krantz et al.,
2004).
Growth and developmental delay is usually observed, with patients having small
stature, microcephaly, mental and/or learning disabilities, especially speech and
language problems (Bork et al., 2004; Liu and Krantz, 2009).
Multiple organ systems can be involved in CdLS, but the mostly affected include
the gastrointestinal system (especially the presence of gastroesophageal reflux
disease), hearing, genitourinary system, ocular system, heart and diaphragm. Besides
limb defects other orthopedic complications may occur (Kline et al., 2007; Dorsettt and
Krantz, 2009).
Most patients have behavioral problems that can be caused or enhanced by the
disease physical complications. Common behavioral and neurological problems that
have been reported in CdLS patients include autistic behavior, self injurious tendencies,
obsessive compulsive behavior, attention deficit disorder, and depression (Liu and
Krantz, 2009).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
3
The variability of the CdLS phenotype expression been shown since the earliest
reports of this syndrome. While the most severe cases of CdLS have many of the
symptoms described above, in the mildest forms the patients usually have mild to
moderate mental disability and (at least at a young age) typical facial characteristics,
without other substantial structural differences. This implies that the brain is the most
sensitive organ to this condition (Dorsettt and Krantz, 2009). This variation between
affected individuals has led to the development of scoring systems that help to
establish a genotype-phenotype correlation, and to anticipate care measures that will
be needed by each patient (Kline et al., 2007).
1.1.3. Etiology
CdLS is a genetically heterogeneous syndrome since five genes have been
reported as implicated in this disease. The majority of patients have de novo dominant
mutations in NIPBL gene (40-60% of patients) (Russo et al., 2012). This explains the
reason why the bulk of patients have a sporadic inheritance pattern and there are only
a few familial cases. In addition, a limited number of patients have been described as
having mutations in other genes such as SMC1A and SMC3 (~5% and <1% of patients
respectively). All of these encode for proteins involved in the Cohesin sister chromatid
cohesion (Galendari et al., 2011).
Very recently, another gene involved in the cohesion complex, HDAC8, has been
reported as causing CdLS but mutations were identified in a very small percentage of
patients (Deardorff et al., 2012a). A closely related gene, RAD21, has also been found
to cause a cohesinopathy with several overlapping features with CdLS (Deardorff et al.,
2012b). Other unidentified genes are thought to be involved with this syndrome since
many patients are still molecularly unresolved (Russo et al., 2012). Considering the
importance of the cohesin complex to this syndrome, this subject will be covered in
more detailed in the next section of this Introduction.
1.2. Biochemistry basis of CdLS - the cohesin complex
Cohesin complex has a crucial role in cell division by regulating sister chromatid
cohesion during mitosis and meiosis. During the last years several studies have
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
4
demonstrated that this complex, together with their key regulators, has other essential
functions during cell cycle progression. These include: i) DNA double strand repair in
G2 phase, ii) gene expression by determining the amount of elongating RNA
polymerases on genes (Fay et al., 2011) and thereby, iii) contributing for maintaining
the genome’s stability (reviewed by Horsfield et al., 2012).
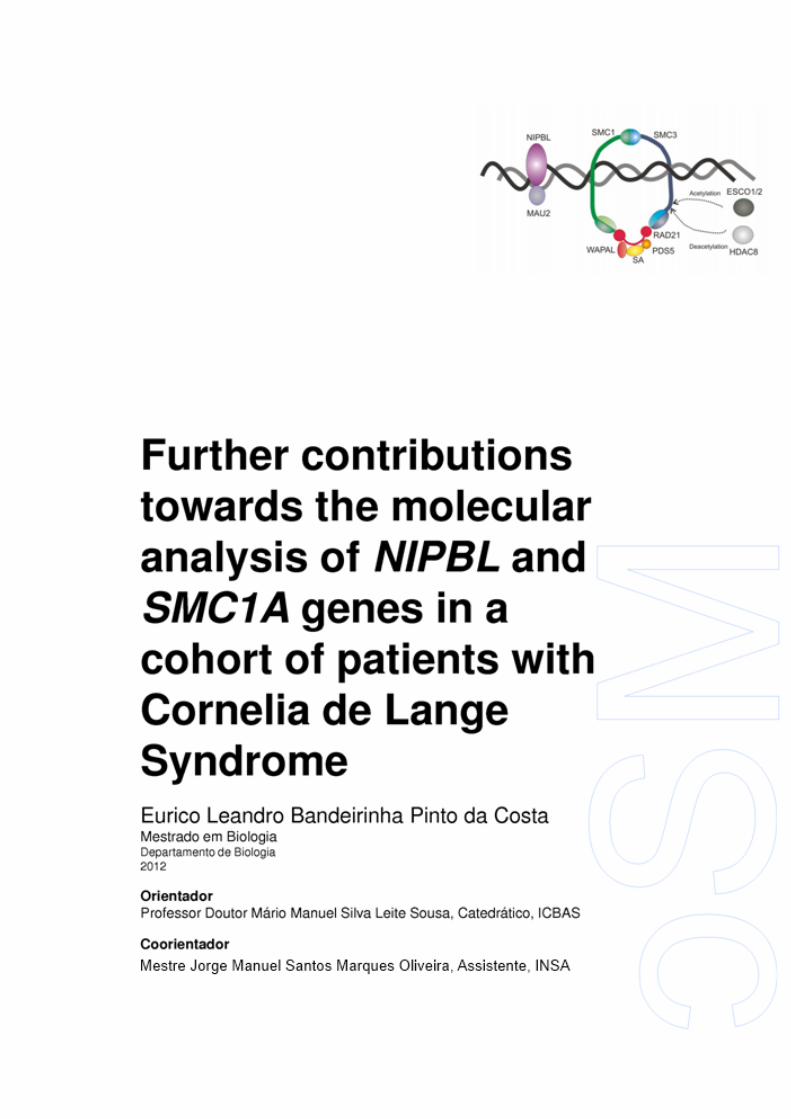
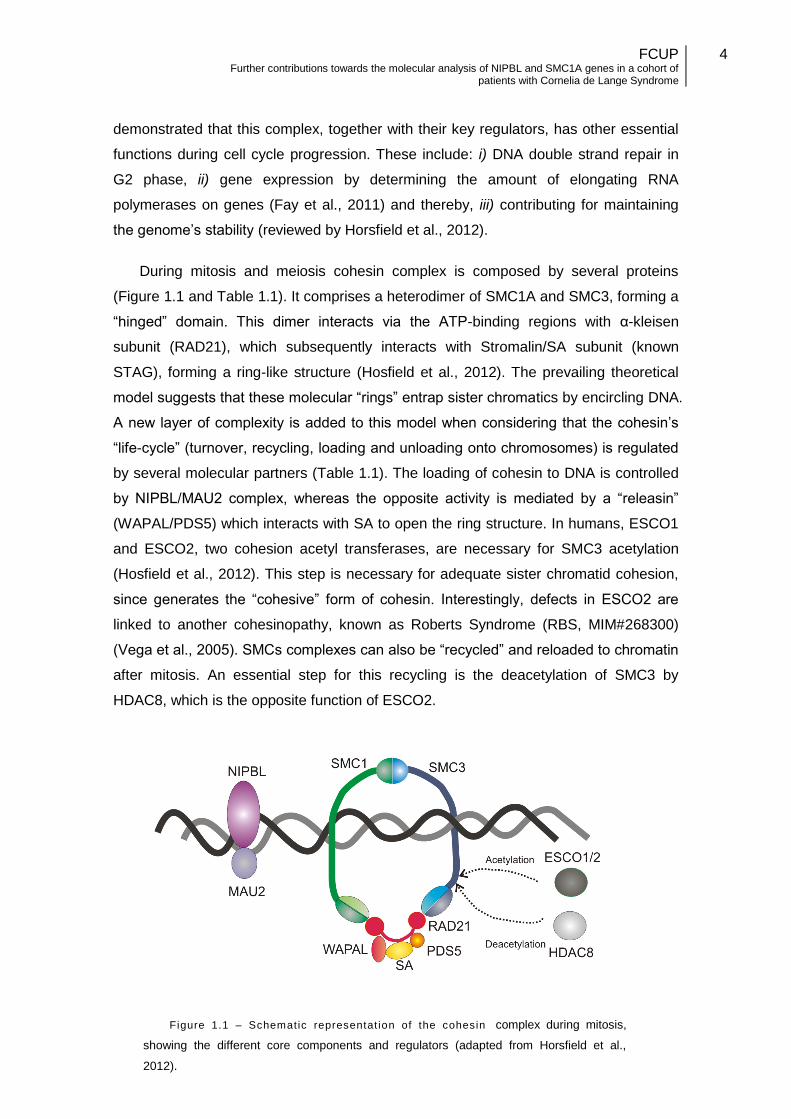
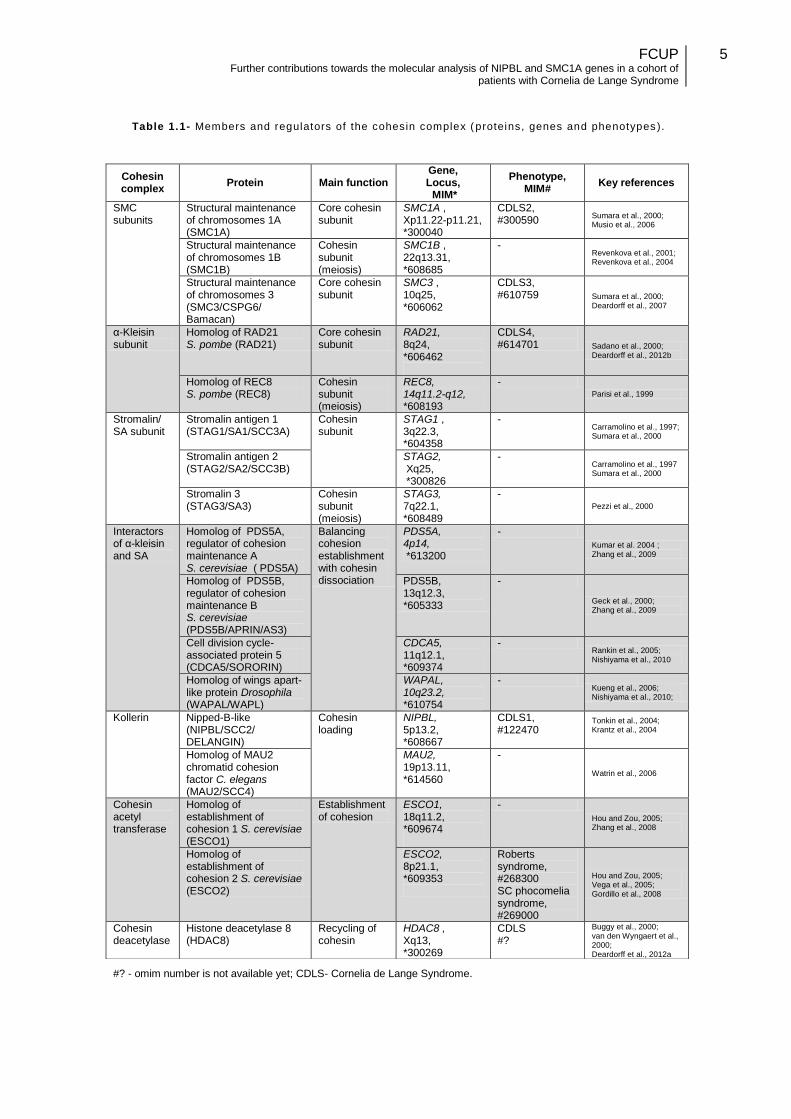
During mitosis and meiosis cohesin complex is composed by several proteins
(Figure 1.1 and Table 1.1). It comprises a heterodimer of SMC1A and SMC3, forming a
“hinged” domain. This dimer interacts via the ATP-binding regions with α-kleisen
subunit (RAD21), which subsequently interacts with Stromalin/SA subunit (known
STAG), forming a ring-like structure (Hosfield et al., 2012). The prevailing theoretical
model suggests that these molecular “rings” entrap sister chromatics by encircling DNA.
A new layer of complexity is added to this model when considering that the cohesin’s
“life-cycle” (turnover, recycling, loading and unloading onto chromosomes) is regulated
by several molecular partners (Table 1.1). The loading of cohesin to DNA is controlled
by NIPBL/MAU2 complex, whereas the opposite activity is mediated by a “releasin”
(WAPAL/PDS5) which interacts with SA to open the ring structure. In humans, ESCO1
and ESCO2, two cohesion acetyl transferases, are necessary for SMC3 acetylation
(Hosfield et al., 2012). This step is necessary for adequate sister chromatid cohesion,
since generates the “cohesive” form of cohesin. Interestingly, defects in ESCO2 are
linked to another cohesinopathy, known as Roberts Syndrome (RBS, MIM#268300)
(Vega et al., 2005). SMCs complexes can also be “recycled” and reloaded to chromatin
after mitosis. An essential step for this recycling is the deacetylation of SMC3 by
HDAC8, which is the opposite function of ESCO2.
Figure 1.1 – Schematic representat ion of the cohesin complex during mitosis,
showing the different core components and regulators (adapted from Horsfield et al.,
2012).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
5
Table 1.1- Members and regulators of the cohesin complex (proteins, genes and phenotypes ).
#? - omim number is not available yet; CDLS- Cornelia de Lange Syndrome.
Cohesin complex
Protein Main function Gene, Locus, MIM*
Phenotype, MIM#
Key references
SMC subunits
Structural maintenance of chromosomes 1A (SMC1A)
Core cohesin subunit
SMC1A , Xp11.22-p11.21, *300040
CDLS2, #300590
Sumara et al., 2000; Musio et al., 2006
Structural maintenance of chromosomes 1B (SMC1B)
Cohesin subunit (meiosis)
SMC1B , 22q13.31, *608685
- Revenkova et al., 2001; Revenkova et al., 2004
Structural maintenance of chromosomes 3 (SMC3/CSPG6/ Bamacan)
Core cohesin subunit
SMC3 , 10q25, *606062
CDLS3, #610759 Sumara et al., 2000;
Deardorff et al., 2007
α-Kleisin subunit
Homolog of RAD21 S. pombe (RAD21)
Core cohesin subunit
RAD21, 8q24, *606462
CDLS4, #614701 Sadano et al., 2000;
Deardorff et al., 2012b
Homolog of REC8 S. pombe (REC8)
Cohesin subunit (meiosis)
REC8, 14q11.2-q12, *608193
- Parisi et al., 1999
Stromalin/ SA subunit
Stromalin antigen 1 (STAG1/SA1/SCC3A)
Cohesin subunit
STAG1 , 3q22.3, *604358
- Carramolino et al., 1997; Sumara et al., 2000
Stromalin antigen 2 (STAG2/SA2/SCC3B)
STAG2, Xq25, *300826
- Carramolino et al., 1997 Sumara et al., 2000
Stromalin 3 (STAG3/SA3)
Cohesin subunit (meiosis)
STAG3, 7q22.1, *608489
- Pezzi et al., 2000
Interactors of α-kleisin and SA
Homolog of PDS5A, regulator of cohesion maintenance A S. cerevisiae ( PDS5A)
Balancing cohesion establishment with cohesin dissociation
PDS5A, 4p14, *613200
-
Kumar et al. 2004 ; Zhang et al., 2009
Homolog of PDS5B, regulator of cohesion maintenance B S. cerevisiae (PDS5B/APRIN/AS3)
PDS5B, 13q12.3, *605333
-
Geck et al., 2000; Zhang et al., 2009
Cell division cycle-associated protein 5 (CDCA5/SORORIN)
CDCA5, 11q12.1, *609374
- Rankin et al., 2005; Nishiyama et al., 2010
Homolog of wings apart-like protein Drosophila (WAPAL/WAPL)
WAPAL, 10q23.2, *610754
- Kueng et al., 2006; Nishiyama et al., 2010;
Kollerin Nipped-B-like (NIPBL/SCC2/ DELANGIN)
Cohesin loading
NIPBL, 5p13.2, *608667
CDLS1, #122470
Tonkin et al., 2004; Krantz et al., 2004
Homolog of MAU2 chromatid cohesion factor C. elegans (MAU2/SCC4)
MAU2, 19p13.11, *614560
-
Watrin et al., 2006
Cohesin acetyl transferase
Homolog of establishment of cohesion 1 S. cerevisiae (ESCO1)
Establishment of cohesion
ESCO1, 18q11.2, *609674
-
Hou and Zou, 2005; Zhang et al., 2008
Homolog of establishment of cohesion 2 S. cerevisiae (ESCO2)
ESCO2, 8p21.1, *609353
Roberts syndrome, #268300 SC phocomelia syndrome, #269000
Hou and Zou, 2005; Vega et al., 2005; Gordillo et al., 2008
Cohesin deacetylase
Histone deacetylase 8 (HDAC8)
Recycling of cohesin
HDAC8 , Xq13, *300269
CDLS #?
Buggy et al., 2000; van den Wyngaert et al., 2000; Deardorff et al., 2012a
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
6
1.3. Genetics of CdLS
1.3.1. NIPBL gene
It was in 2004 that NIPBL (MIM*608667), the first gene responsible for CdLS was
found by two independent groups (Krantz et al., 2004; Tonkin et al., 2004). This gene
was found through genome-wide linkage exclusion analysis in affected families, in
patients with de novo translocations and deletions, that allowed the identification of a
candidate genomic region for CdLS. Using distinct approaches both works identified
mutations in a gene named as NIPBL (Nipped-B like, MIM*608667) as causative of the
disease (Krantz et al., 2004; Tonkin et al., 2004).
The human NIPBL gene is located in chromosome 5, (5p13.1) and spans over
190Kbp. The open reading frame (ORF) of NIPBL starts in exon 2, and continues to
exon 47 (Tonkin et al., 2004). This gene encodes for delangin, a protein which contains
a highly conserved armadillo domain with several HEAT-repeats, a protein-protein
interaction motif (Selicorni et al., 2008), a glutamine-rich domain, and a predicted
bipartite nuclear localization signal (Yan et al., 2006; Braunholz et al., 2012). This
protein has two isoforms: delangin-A (the mainly expressed form), a long form with
2804 amino acids, and delangin-B, the shorter form with 2697 amino acids (Tonkin et
al., 2004). It is involved in cohesin complex loading, mediating chromatin modifications
through recruitment of histone deacetylases. NIPBL was identified as the human
homologue of Drosophila melanogaster Nipped-B gene, a chromosomal adherin
involved in chromatid cohesion and also acting as a transcriptional regulator in Yeast
(SCC2) (Bhuiyan et al., 2006). Further studies have demonstrated that the human
protein is a regulator of the cohesin complex required for binding of the cohesin
complex (Braunholz et al., 2012; Dorsett et al., 2007). NIPBL-mutated cells from CdLS
patients have shown a reduced capacity to tolerate DNA damage (Revenkova et al.,
2009).
Nearly half of CdLS cases are caused by mutations in NIPBL gene, being the
major causative gene for this syndrome. Mutations in this gene can cause mild to
severe forms of the disease (Galendari et al., 2011). Genotype-phenotype correlations
studies indicate that severe NIPBL mutations (originating premature termination
codons) usually cause more severe forms than missense mutations (Dorsettt and
Krantz, 2009).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
7
0
2
4
6
8
10
12
14
16
18
20
5'U
TR-1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
47-3
'UTR
Distribution of mutations NIPBL gene
Total mutations (count) Mutations [(count/exon size)*100]
56
In 2010, Oliveira et al., reported the creation of a locus specific database (LSDB)
for the NIPBL gene, which contained mutational and clinical data reported in all peer
review papers. An analysis of the mutations in the database was made, and all
mutations types were found in NIPBL: small deletions (27.6% of cases), missense
changes (21.1%), nonsense mutations (17.3%), mutations affecting splicing (17.1%),
small duplications (13.6%), insertions (1.5%) and insertion/deletions (1.5%). Statistical
analysis suggested that patients with nonsense mutations or out-of-frame
deletions/duplications/insertions more often presented a severe phenotype than those
with less detrimental effect on the protein (Oliveira et al., 2010).
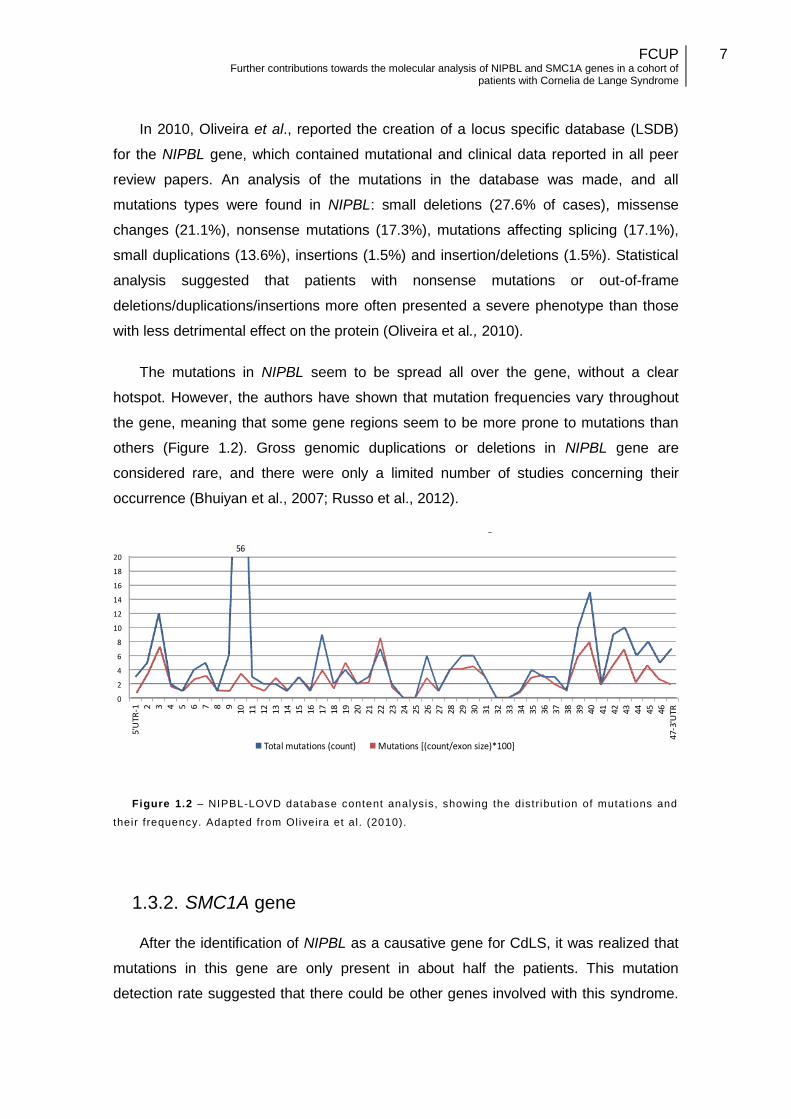
The mutations in NIPBL seem to be spread all over the gene, without a clear
hotspot. However, the authors have shown that mutation frequencies vary throughout
the gene, meaning that some gene regions seem to be more prone to mutations than
others (Figure 1.2). Gross genomic duplications or deletions in NIPBL gene are
considered rare, and there were only a limited number of studies concerning their
occurrence (Bhuiyan et al., 2007; Russo et al., 2012).
Figure 1.2 – NIPBL-LOVD database content analysis, showing the distribut ion of mutat ions and
their frequency. Adapted from Oliveira et al. (2010).
1.3.2. SMC1A gene
After the identification of NIPBL as a causative gene for CdLS, it was realized that
mutations in this gene are only present in about half the patients. This mutation
detection rate suggested that there could be other genes involved with this syndrome.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
8
The variability of the clinical findings between patients also supported this hypothesis.
Since NIPBL is involved in the cohesion complex, other genes encoding proteins linked
to the cohesion complex were studied in patients with CdLS or CdLS-like phenotype.
In 2006, mutations in the SMC1A gene (structural maintenance of chromosomes
1A, MIM #300590) was found to cause an X-linked form of CdLS patients (Musio et al.,
2006). Mutations were found in three affected males of the same family and in an
unrelated patient, without NIPBL mutations (Musio et al., 2006). The SMC1A gene is
located in chromosome Xp11.22, with a size of 48Kbp, and has 25 exons (all of them
coding). The SMC1A gene encodes for a protein with 1233 aminoacids, which is one of
the four subunits of the cohesion complex. It is involved in genome stability and DNA
repair (Musio et al., 2006; Watrin and Peters, 2006). Interestingly, the majority of
patients with SMC1A mutations are females (Deardorff et al., 2007). While in normal
females the SMC1A gene escapes X-inactivation and both copies are expressed,
males are hemizygous for SMC1A since it is not located in the pseudoautosomal
region. Affected females should express a normal copy of the gene, leading to the
suggestion that SMC1A mutations are dominant-negative (Liu and Krantz, 2009;
Hoppman-Chaney et al., 2011).
X-linked CdLS patients seem to have a milder phenotype than the “classic” form,
especially the female patients, having a milder dysmorphism, and a mild or no growth
delay, and absence of microcephaly (Musio et al., 2006; Bork et al., 2007). Less severe
cases result in a phenotype that approaches that of apparently nonsyndromic mental
retardation (Revenkova et al., 2009), although severe phenotypes in this gene have
also been reported (Hoppman-Chaney et al., 2011). Male patients seem to have a
severer phenotype than females, more similar with a “typical” CdLS. (Musio et al.,
2006; Maninni et al., 2010).
A LSDB for SMC1A gene was also developed (Oliveira et al., 2010). Most
mutations reported were substitutions (~84%), and the remaining are small deletions
(~16%). The majority of the mutations reported in this database have a de novo origin.
The mutations appear spread over the gene, without a clear mutational hotspot
(http://www.lovd.nl/SMC1A, last accessed 15 September 2012).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
9
1.3.3. SMC3 gene
The discovery that mutations in the X-linked SMC1A gene result in CdLS
suggested that other members of the cohesin complex may contribute to the etiology of
CdLS. In 2007, Deardorff and collaborators screened 115 CdLS patients that were
negative for mutations in NIPBL, for mutations in genes encoding for subunits of the
cohesin complex (SMC1A and SMC3). There was only one mutation found in SMC3
gene so far, in two unrelated patients. It is a small deletion in exon 9 that results in the
loss of a single amino acid. (Deardorff et al., 2007; Revenkova et al., 2009).
The SMC3 gene (MIM#610759), or structural maintenance of chromosomes 3, is
located on chromosome 10q25.2, and it has a size of 37Kbp, and 29 exons (all of them
coding). This gene encodes for the SMC3 protein, with 1217 aminoacids, and like
SMC1A, is one of the subunits of the cohesion complex (Deardorff et al., 2007;
Revenkova et al., 2009). Patients with mutations in SMC3 present a mild variant of the
CdLS phenotype, with very mild facial features, and no absence or reduction of limbs
or digits, and no other major structural anomalies in contrast to classical CdLS
phenotype (Deardorff et al., 2007).
1.3.4. HDAC8 gene
The involvement of HDAC8 in CdLS was discovered very recently by Deardorff and
co-workers (2012a). His group characterized this gene product as a SMC3 deacetylase,
and also detected six loss-of-function mutations in HDAC8 (Deardorff et al., 2012a).
The HDAC8 gene (MIM#601639), or histone deacetylase 8, is located in
chromosome Xq13.1, has a size of 243.6 Kbp, and contains a total of 61 exons. In the
cohesion complex, the HDAC8 protein is the SMC3 deacetylase. The SMC3 protein is
acetylated by ESCO2 during S-phase to establish cohesiveness of chromatin-loaded
cohesion, and HDAC8 protein deacetylates SMC3 during anaphase. The loss of
HDAC8 activity in increased SMC3 acetylation and inefficient dissolution of the ‘used’
cohesin complex released from chromatin in both prophase and anaphase. Deardorff
and team suggested that this defects lead to impaired embryonic development which
can give rise to CdLS. (Deardorff et al., 2012a).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
10
2. Objectives
The molecular and clinical characterization of CdLS patients was initiated at the
national level in 2005 with the research project entitled: “Caracterização clínica,
epidemiológica e molecular dos doentes com o Síndrome de Cornelia de Lange em
Portugal”, supported by the Instituto de Genética Médica Dr. Jacinto Magalhães. Our
team of molecular and clinical geneticists gathered mutational and clinical data on a
total of 53 Portuguese CdLS patients (this includes more recent cases). Thirteen of
those patients, with novel NIPBL mutations, were initially reported together with the
development of a LSDB (Oliveira et al., 2010). The present work intended to unfold
new molecular findings in the remaining Portuguese CdLS patients. In brief, the main
objectives of the present work were the following:
i) Report the molecular characterization of the remaining CdLS patients with
NIPBL mutations.
ii) Apply Multiplex Ligation-dependent Probe Amplification technique (for
NIPBL) in the group of CdLS patients that remained molecularly unresolved
after NIPBL gene sequencing.
iii) Set up a fast and cost-effective screening method for point mutations in
SMC1A gene by High resolution melting curve analysis.
iv) Optimize the molecular diagnostic procedure of CdLS patients.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
11
3. Materials and Methods
3.1. Patients
Forty CdLS Patients were included in this work, recruited in two distinct phases:
i) Research project (2005-2010).
The criteria for inclusion were a diagnosis of CdLS confirmed by a clinical
geneticist, a normal karyotype and guardian informed consent. A clinical protocol
designed for a previous study (Dias et al., 2008) was used by clinical geneticists to
assess the patients. This protocol includes information on prenatal, birth and postnatal
history, an evaluation of 50 phenotypical features, behavior, development and
multisystem involvement. A diagnostic severity score was also included in the protocol
formulary. This scoring system described by Kline and collaborators (2007), classifies
CdLS patients as mild, moderate or severe, according to the number and type of
abnormalities (Annex I). From the 53 patients (from 51 different families) initially
referred, 26 patients were recruited for this work. Fourteen were excluded for one of
the following criteria: insufficient DNA for analysis (deceased patients, n=2), insufficient
clinical data (incomplete/lacking clinical protocol information, n=2), patients with low
severity score (with “Cornelia-like” features but not reaching the mild phenotype, n=10).
Thirteen of these patients (from 12 different families) were previously published by our
group (Oliveira et al., 2010) and thus, will not be included in the results section of this
work.
ii) Clinical requests for CdLS molecular studies (2010-2012).
Fourteen new CdLS cases were referred for molecular studies. Together with the
biological samples a specific request form was used to collect as most as possible
information concerning their phenotype. The clinical classification of patients was
based on the information retrieved from this test request form and was validated by a
clinical geneticist using the score system proposed by Kline et al. (2007).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
12
3.2. Preparation of biological samples
3.2.1. DNA extraction method
Genomic DNA (gDNA) was extracted from peripheral blood samples, collected
from the patients and available parents in EDTA anticoagulant tubes, using salting out
method (Miller et al., 1988). Since this method does not requires the use of toxic
chemicals it is a good alternative to the phenol/chloroform extraction. Salting-out is
based on the principle that proteins and other cellular contaminants are less soluble at
higher salt concentrations due to their relative hidrophobicity and will precipitate in a
saturated salt solution while the DNA does not.
3.2.2. RNA extraction method
One of the major concerns in manipulating RNAs, are the ribonuclease enzymes
present in cells and tissues that can rapidly destroy these nucleic acids. Thus, it is
important to avoid sample contamination with ribonucleases. Nuclease-free pipette tips
and reagents were used and all micropipettes (used exclusive for RNA extraction),
were cleaned with RNase AWAY™ (Life Technologies, Foster City, CA, USA). Total
mRNA purification was made from peripheral blood sample in EDTA anticoagulant tube,
using the commercial kit PerfectPure™ RNA Purification System (5 PRIME, Hamburg,
Germany) following the manufacturer protocol.
3.2.3. Nucleic acid quantification
After the nucleic acid extraction, purity and concentration were determined through
spectrophotometric absorbances at the wavelengths of 260 nm (A260) and 280 nm
(A280). A 2 µl sample was quantified in a Nanodrop spectophtometer (Thermo
Scientific), with two independent measures. A260 is used to measure DNA (1U A260 =
50 ng/μl) and RNA (1U A260 = 40 ng/μl) concentrations, while A280 is used to
measure protein concentration. The A260/A280 ratio is used to determine the purity of
nucleic acids. A pure DNA and RNA sample would have a ratio of ~1.8 and ~2.0
respectively, while a protein contaminated sample has a lower ratio (Maniatis et al.,
1982) (Glasel, 1995).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
13
3.2.4. RNA conversion to cDNA
Since RNA is so easily degraded, it was more convenient to convert it to cDNA
(complementary DNA). The High-Capacity cDNA Archive Kit (Life Technologies, Foster
City, CA, USA) was used for the conversion, following the manufacturer protocol. This
was made through a reverse transcription reaction (RT reaction), using MultiScribe™
Reverse Transcriptase (Life Technologies, Foster City, CA, USA) enzyme, and random
(examer) primers. The RNA template was mixed with the kit reagent mixture, and
placed in a thermocycler, and placed 10 minutes at 25ºC and 120 minutes at 37ºC.
3.2.5. Aliquots preparation
The gDNA samples were aliquoted at 100 μg/ml and 50 μg/ml concentrations for
PCR (section 3.3), and for high resolution melting curve analysis (hrMCA) (section 3.8)
use, respectively. This step was essentially done to preserve the original stock sample
for future analysis, and to set the same gDNA concentration between all samples. This
is not only useful to optimize the PCR but also critical for MLPA (section 3.6) and
hrMCA techniques by prevent bias and allowing accurate results. The aliquots and
original samples were stored at 4ºC until use, thus avoiding freeze-thaw of the samples
at lower temperatures).
3.3. DNA amplification by PCR
The polymerase chain reaction (PCR) is an in vitro technique used in molecular
biology, to amplify a target sequence (amplicon) of DNA exponentially. Besides the
DNA template being amplified, the PCR mixture needs several components, including:
Oligonucleotide sequences (primer pair) with a sequence complementary to
the 3' (3 prime) ends of each of the sense and anti-sense strand of the DNA
target region.
Deoxynucleotide triphosphates - dATP, dCTP, dGTP and dTTP (dNTPs).
DNA polymerase, (such as the thermostable Taq polymerase).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
14
Buffer solution that enables the suitable activity and stability of the DNA
polymerase.
Divalent cations (like Mg2+) and monovalent cation (like K+).
This technique consists of cycles of: denaturation (separation of double strand
DNA into single stranded DNA), annealing (primers pair with DNA complementary
sequence), and extension (enzymatic replication of the DNA). This is done by
repeatedly heating and cooling the reaction mixture. The DNA polymerase uses a
single DNA strand to create a new complementary DNA strand in the site targeted by
the pair of primers. The new DNA is itself used as a template for replication, creating a
chain reaction in which the DNA template is exponentially amplified. Besides the cycle
phase, there are some PCR programs that use a preliminary first denaturing step,
heating the sample for heat-activated enzymes, or to help denature the target DNA
better. A final extension (or final elongation) step can also be used to make sure that
the single-stranded DNA is entirely extended (Maniatis et al., 1982).
3.3.1. Oligonucleotides design
Primer design is a critical step for a successful PCR approach. When designing
primers several parameters should be considered (Burpo, 2001):
The primer sequences should be unique to target only a region of DNA, and
avoid annealing at a similar sequence.
Primers with long repeats of a single nucleotide should be avoided (loop
formations can occur).
Primers should not anneal with other primers or themselves (formation of
primer dimers could contaminate the sample).
Primers should be located at least 30-40 bases upstream of the region of
interest in the sequence read.
Optimal primer GC content between 40-60%
NIPBL gene
The mainly expressed isoform of the NIPBL gene (transcript with the accession
number NM_133433.3) has a total of 47 exons, 46 of which are coding (exon 1 is non-
coding). A total of fifty-four primer pairs were used to completely cover the coding and
flanking regions of the gene. In addition to the primers described by Krantz et al. (2004),
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
15
used for exon 10 and exons 39 to 47 of NIPBL gene, custom primers were designed for
the remaining gene regions (exons 2 to 9 and 11 to 38, Annex II.a).
SMC1A gene
According to the transcript with accession number NM_006306.2, SMC1A gene
has a total of 25 exons. Twenty six primer pairs were designed and used to cover the
coding and flanking intronic regions of the gene (Annex II.b). The primers designed
were optimized for hrMCA technique, with smaller amplicons, and without M13
universal tail.
Primer Express (Life Technologies, Foster City, CA, USA) software was used for
primer design. Besides speeding up this process the application allowed to
standardization of experimental conditions. Primers were chosen to have the same
annealing temperature (58-60ºC). In the case of NIPBL gene approach primers
incorporated a M13 universal primers tail sequence. Since the M13-tailed sequences
are not present in the Human genome, primers are not fully complementary (at their 5’).
These M13 universal primers are useful for downstream applications (such as Sanger
sequencing) since the same sequencing primer can be used for all amplicons. In order
to exclude primers more susceptible to primer-dimer formation, Fast PCR software
(Kalendar and Schulman, 2009) was used. Finally, primer-BLAST (Ye et al., 2012,
accessed at http://www.ncbi.nlm.nih.gov/tools/primer-blast/) algorithm was used to
check for primer specificity.
3.3.2. PCR mixture and thermocycling profiles
The NIPBL PCR mixture (for all primer pairs) was prepared with the following
reagents:
10 μl of PCR Master Mix 2x (Cat No # M7505, Promega, Fitchburg, WI, USA)
7 μl dH2O (nuclease free)
1 μl Forward Primer + 1 μl Reverse Primer (primers at 10 pmol/μl)
1 μl gDNA (100 ng/l)
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
16
Then, the PCR mixture samples were homogenized and placed in a thermocycler
(Veriti® Thermal Cycler 96-well, Life Technologies, Foster City, CA, USA), to run one of
the NIPBL programs.
While all the other exons use the same PCR program (Table 3.1) with only
differences in annealing temperatures, exon 44 primer pair had to be performed using
a different thermocycler profile. This is mainly due to the particular base pair
composition of this amplicon, which is particular prone to nonspecific amplification and
a high background. Also, it was difficult to find a new alternative primer pair. To
overcome this problem, a Touchdown PCR program (Table 3.2) was used for exon 44.
This particular type of PCR increases the specificity of primer annealing by initiating at
with higher annealing temperatures and by gradually reducing it. Higher temperatures
result in greater specificity for the binding between the primer and the targeted DNA
template, but low amplification yield. As cycle-by-cycle the annealing temperature
lowers resulting in less specificity but increasing the efficiency of amplification. Due to
the exponential amplification nature of PCR, the amplified (specific) sequences during
the first cycles will out-compete the nonspecific sequences that may be result at lower
temperatures.
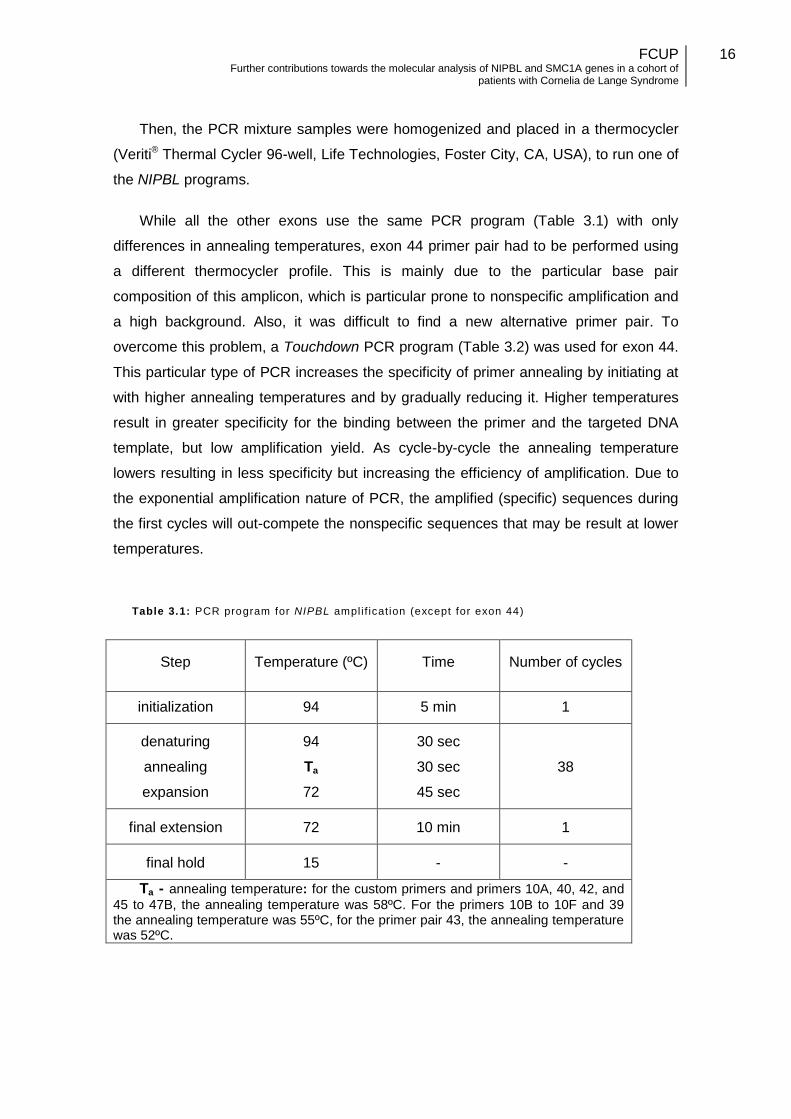
Table 3.1: PCR program for NIPBL ampli f icat ion (except for exon 44)
Step Temperature (ºC) Time Number of cycles
initialization 94 5 min 1
denaturing
annealing
expansion
94
Ta
72
30 sec
30 sec
45 sec
38
final extension 72 10 min 1
final hold 15 - -
Ta - annealing temperature: for the custom primers and primers 10A, 40, 42, and
45 to 47B, the annealing temperature was 58ºC. For the primers 10B to 10F and 39 the annealing temperature was 55ºC, for the primer pair 43, the annealing temperature was 52ºC.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
17
Table 3.2 : Touchdown PCR program for NIPBL exon 44
Step Temperature (ºC) Time Number of cycles
initialization 94 5 min 1
denaturing
annealing
expansion
94
62 → 54 *
72
30 sec
30 sec
45 sec
10
denaturing
annealing
expansion
94
54
72
30 sec
30 sec
45 sec
25
final extension 72 10 min 1
final hold 15 - -
* -0.8ºC each cycle, starting on the second cycle
3.4. Agarose gel electrophoresis
After PCR amplification PCR products were analyzed by agarose gel
electrophoresis. Gel electrophoresis is a way to separate and analyze DNA. It can be
used to quantify or even to isolate a particular DNA fragment. An electric field causes
negatively charged DNA molecules to travel through the agarose gel. DNA molecules
must move through the matrix pores of the gel allowing their efficient separation
according to size (being easier for the smaller molecules to migrate than the larger
ones). To verify the PCR amplification 3 μl of each PCR sample product were mixed
with 1 μl loading buffer (custom made) and loaded in 1% (m/v) SeaKem® LE Agarose
(Cambrex Bio Science, Verviers, Belgium) gel stained with GelRed™ (Biotium,
Hayward, CA, USA). A DNA low mass ladder (Life Technologies, Foster City, CA,
USA) was also loaded in a separate lane of the gel to calculate the size to the DNA
fragments. After running electrophoresis the gel was analyzed under UV light and
images were obtained using a LAS-3000 image system (Fujifilm, Tokyo, Japan).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
18
3.5. PCR purification
The PCR product was purified using the ExoSAP-IT® (Affimetrix, Santa Clara, CA,
USA) enzymatic treatment. ExoSAP-IT® is a mixture of shrimp alkaline phosphatase
and exonuclease that degrade primers and dephosphorylate dNTPs, improving the
quality of the sequences resulting from PCR product.
In this procedure 2 μl of ExoSAP-IT® was added to 8 μl of PCR product (for each
amplicon) and this mixture was placed for 30 minutes at 37ºC followed by 15 minutes
at 85ºC (enzyme inactivation step).
3.6. Sanger Sequencing
Purified PCR products were sequenced by dye-terminator cycle sequencing. In this
type of sequencing, there are 4 (one for each base) chain terminator ddNTPs
(dideoxynucleotide-tri-phosphate) tagged with fluorescent dyes that emit light in
different wavelengths. These ddNTPs are mixed in lower concentration with dNTPs
and when a DNA polymerase incorporates a ddNTP instead of a dNTP the chain
extension is prematurely ended. This will produce a series of DNA fragments with
different lengths that are terminated with a specific base. Cycle sequencing products
must be cleaned of primers, excess dNTP’s, enzymes and buffer components before
proceeding for electrophoresis. Currently this analysis is carried out in multi-capillary
automated sequencers that can efficiently analyze several samples at the same time.
Briefly, samples are injected into the capillaries loaded with a special polymer (used as
a separation matrix) by means of an electric potential difference. This capillary
electrophoresis resolves each dye labeled DNA fragments with high efficiency (1 bp
difference). At the end of the capillary a laser-induced fluorescent system is used to
excite each fluorochrome and the resulting light is detected. Finally the software
converts all the fluorescence signals into an electropherogram.
3.6.1. Sequencing reaction
This sequencing reaction is an asymmetric PCR carried out using only one primer,
resulting in the amplification of only one DNA strand of the double-stranded DNA
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
19
template. This means that to sequence both DNA strands two independent sequencing
reactions are needed for each amplicon (one for each of the primer pair).
Sequencing reactions were prepared with BigDye® Terminator Cycle Sequencing
Kit v1.1 (Life Technologies, Foster City, CA, USA), using a mixture of 2 μl big-dye, 2 μl
dH2O, 1 μl primer (at 5 pmol/μl) and 5 μl purified PCR products. The M13 Universal
primers (Forward and Reverse) were used in the sequencing reaction (instead of the
PCR primers) for the M13-tailed primers. For amplicons without M13-tailed primers, the
initial PCR primers were used.
3.6.2. Sequencing PCR purification
After cycle sequencing, the samples were purified by Performa® DTR Ultra 96-
Well Plates (Edge Bio, Gaithersburg, MA, USA). The samples were transfered into the
Performa® well plates, that were centrifuged at 850 rcf in an Eppendorf 5804 R Plate
Centrifuge (Eppendorf, Hamburg, Germany). These columns have a hydrated gel
matrix that purified the samples of dye terminators, dNTPs, primers, and buffer.
3.6.3. Sequencing analysis
The fragments were separated by size through capillarity electrophoresis in 3130xl
ABI Genetic Analyser (Life Technologies, Foster City, CA, USA) and sequence
analysis was performed using SeqScape® v2.5 software (Life Technologies, Foster
City, CA, USA). Identified sequence variants were confirmed in a secondary
confirmatory PCR of the affected amplicon, in the patient and parents (if available).
3.7. Multiplex ligation probe amplification
The multiplex ligation-dependent probe amplification (MLPA) is a semi-quantitative
technique that uses a primer pair to amplify several target DNA locations, by using
probes. This technique allows the detection of gross deletions and duplications in the
target DNA sequence. Each of the probes is composed of two oligonucleotides that
target adjacent sites. One of them has a tail sequence complementary to the forward
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
20
primer, and the other to the reverse primer. Only when both oligonucleotides are
hybridized with their respective target sequence, they can be ligated into a complete
probe. Each of the complete probes has a unique size, which can be identified by
capillarity electrophoresis. By using reference samples it is possible to compare the
relative quantity of each of the fragments.
The MLPA analysis was performed using commercial kits P141 and P142 (MRC-
Holland, Amsterdam, the Netherlands), that contain probes for all NIPBL exons. First, a
mixture was prepared with the DNA samples and the NIPBL probes, and subsequently
heated to denature followed by overnight hybridization. After this period a DNA ligase is
added to the mixture to uphold probes’ ligation. These ligation products are finally
amplified by PCR. Final MLPA products were separated by capillary electrophoresis,
using a 3130xl ABI Genetic Analyser (Life Technologies, Foster City, CA, USA).
Results were analyzed using GeneMarker® software (SoftGenetics LLC, State College,
PA, USA). The population normalization method was used and data was plotted using
probe ratio.
3.8. High Resolution Melting Curve Analysis
The hrMCA is a technique used to detect sequence variants in double stranded
DNA samples. During gDNA amplification by PCR, an intercalating fluorescent dye is
added at a saturating concentration, and its incorporation and binding to double
stranded DNA causes it to become florescent. The changes in fluorescence are
detected by an optical system during real-time. After the PCR step, the specific hrMCA
thermocycling profile is initiated, samples are heated from between two temperature
(such as from 50 to 95ºC) in a precise and uniform way. When the specific melting
temperature of the amplicon is reached, the two DNA strands separate (melt) from
each other, releasing the intercalated dye which loses its fluorescence. Since the
melting temperature of an amplicon depends on its DNA composition, a single base
pair change in the sequence will shift the temperature at which the melting occurs. By
comparing melting curve profiles of wild type controls and from patients it is possible to
identify sequence variants. This technique was used to detect variants in SMC1A gene,
and for population screening in some NIPBL variants.
The PCR and subsequently hrMCA were prepared with the following reagents:
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
21
10 μl of PCR Master Mix 2x (Promega Cat No # M7505)
6 μl dH2O (nuclease free)
1 μl EvagreenTM (Biotium, Hayward, CA, USA)
1 μl Forward Primer + 1 μl Reverse Primer (primers at 5 pmol/μl)
1 μl gDNA (50 ng/l)
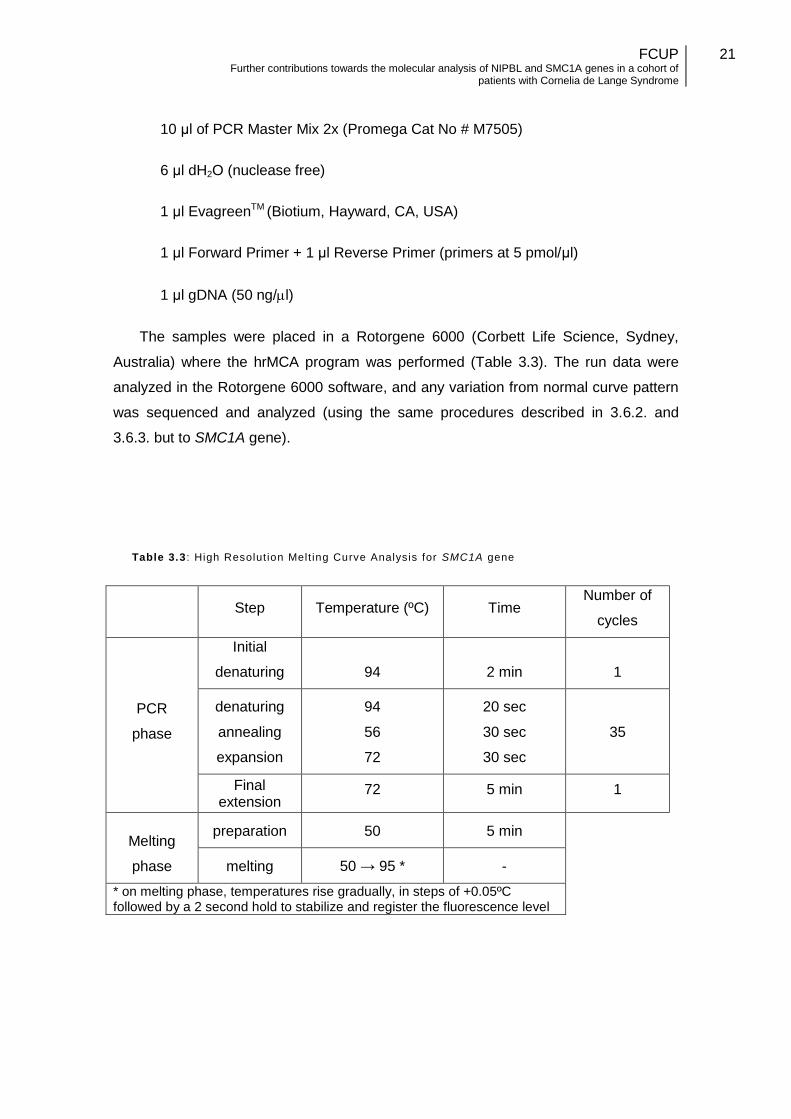
The samples were placed in a Rotorgene 6000 (Corbett Life Science, Sydney,
Australia) where the hrMCA program was performed (Table 3.3). The run data were
analyzed in the Rotorgene 6000 software, and any variation from normal curve pattern
was sequenced and analyzed (using the same procedures described in 3.6.2. and
3.6.3. but to SMC1A gene).
Table 3.3 : High Resolut ion Melt ing Curve Analysis for SMC1A gene
Step Temperature (ºC) Time Number of
cycles
PCR
phase
Initial
denaturing 94 2 min 1
denaturing
annealing
expansion
94
56
72
20 sec
30 sec
30 sec
35
Final extension
72 5 min 1
Melting
phase
preparation 50 5 min
melting 50 → 95 * -
* on melting phase, temperatures rise gradually, in steps of +0.05ºC followed by a 2 second hold to stabilize and register the fluorescence level
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
22
3.9. Bioinformatics and databases
The variations discovered through the different techniques, were analyzed with the
aid of Alamut 3.0 (Interactive Biosoftware, Rouen, France) mutation interpretation
software, and the locus specific mutation databases (LSDB) for NIPBL and SMC1A
genes (http://www.lovd.nl/CDLS). These databases use the Leiden Open Variation
database (LOVD) software platform, enabling a Web-based listing and curation of
sequence variations associated with phenotypical information.
3.9.1. Missense mutations analysis
The bioinformatic analysis of the pathogenicity was made with the help of the
commercial software Alamut version 3.0 (Interactive Biosoftware, Rouen, France), and
three other tools:
PolyPhen version 2. This software gives a score to the impact of
substitutions on the structure and function of protein, with a range of
values from: 0 to 1.000, with the higher value more likely to be
pathogenic (Adzhubei et al., 2010).
SIFT is a sequence homology-based tool that predicts whether an
amino acid substitution in a protein will have a phenotypic effect. The
score ranges from 0 to 1. The substitution is predicted damaging is the
score is <= 0.05, and tolerated if the score is > 0.05 (Pauline and
Henikoff, 2003).
Grantham's distance compares wild type with mutated aminoacids, by
using physical and chemical parameters (volume, weight, polarity, and
carbon-composition). The score range from 0 to 215, with higher value
indicates larger difference.
3.9.2. Algorithms for evaluating splicing
The splicing mutations found were analyzed through five different methods,
integrated in the Alamut 3.0 (Interactive Biosoftware, Rouen, France) Splicing
Prediction Module:
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
23
SpliceSiteFinder-like method is based on position weight matrices
computed from a set of human constitutive exon/intron junctions for donor
and acceptor sites.
MaxEntScan method uses the Maximum Entropy principle (Yeo et al.,
2004).
NNSPLICE is a method based on neural networks (Reese et al., 1997).
GeneSplicer uses several techniques to detect splice sites, among which
the Markov models (Pertea et al., 2001).
Human Splicing Finder method is based on position weight matrices
with position-dependent logic (Desmet et al., 2009).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
24
4. Results
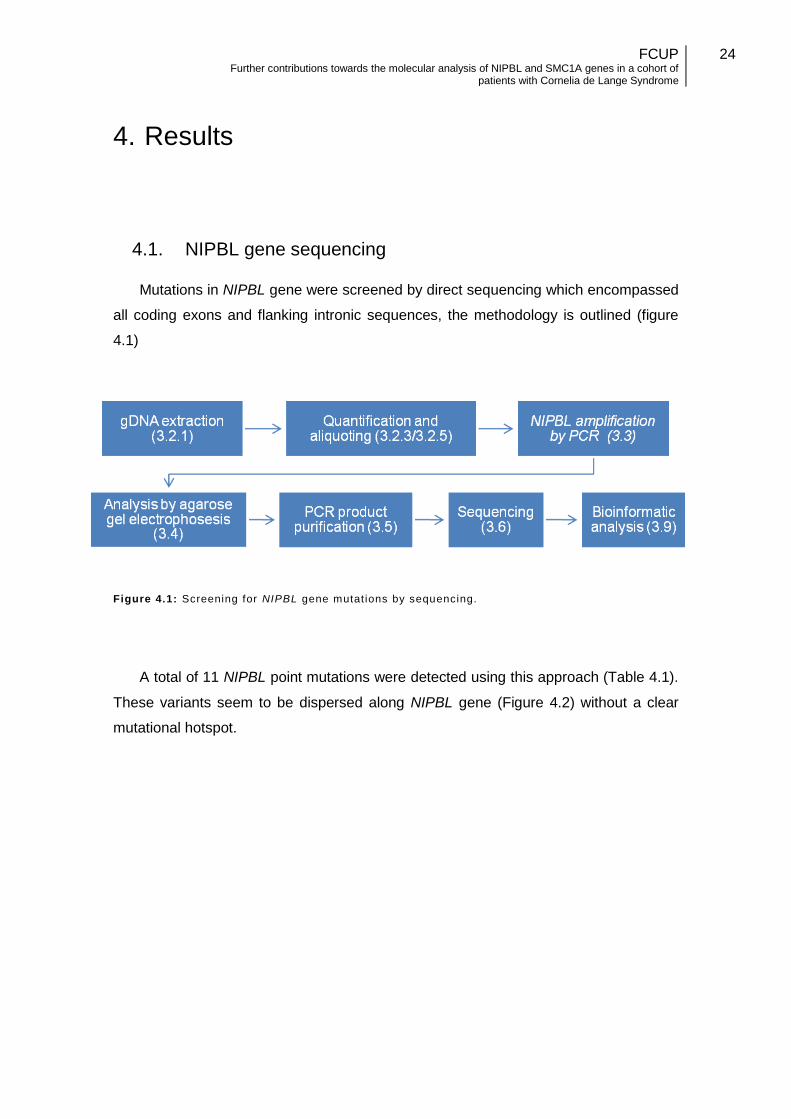
4.1. NIPBL gene sequencing
Mutations in NIPBL gene were screened by direct sequencing which encompassed
all coding exons and flanking intronic sequences, the methodology is outlined (figure
4.1)
Figure 4.1: Screening for NIPBL gene mutat ions by sequencing.
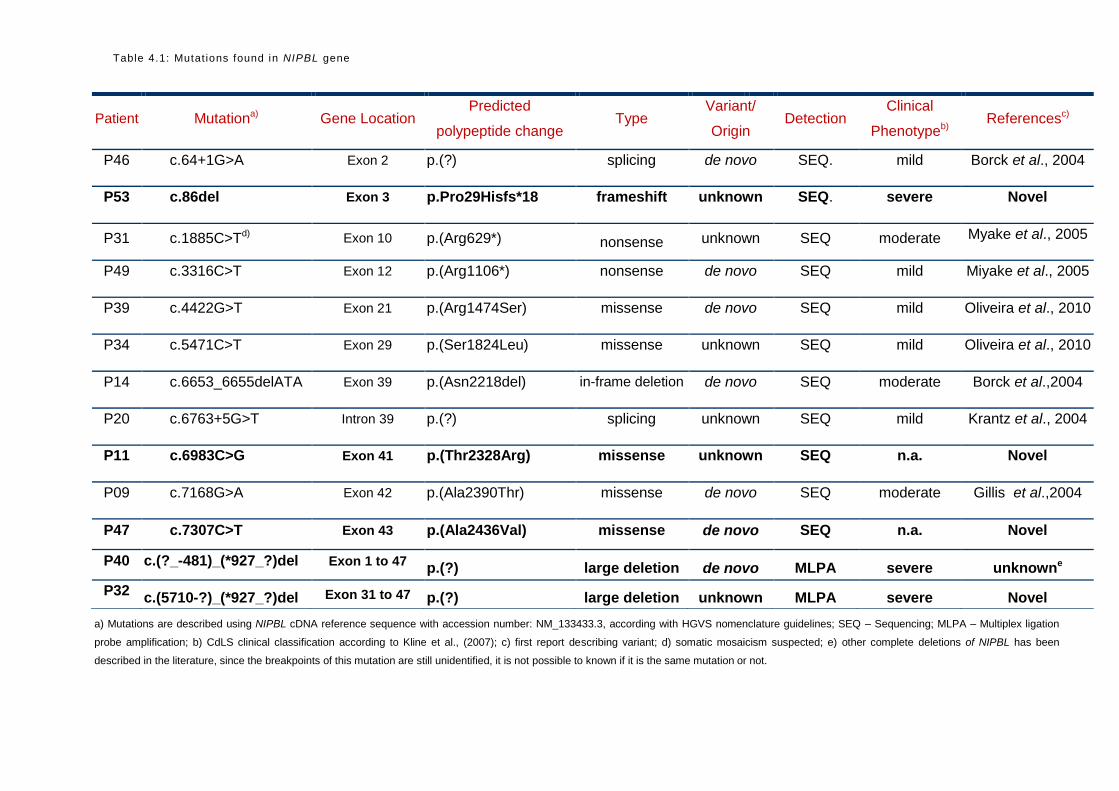
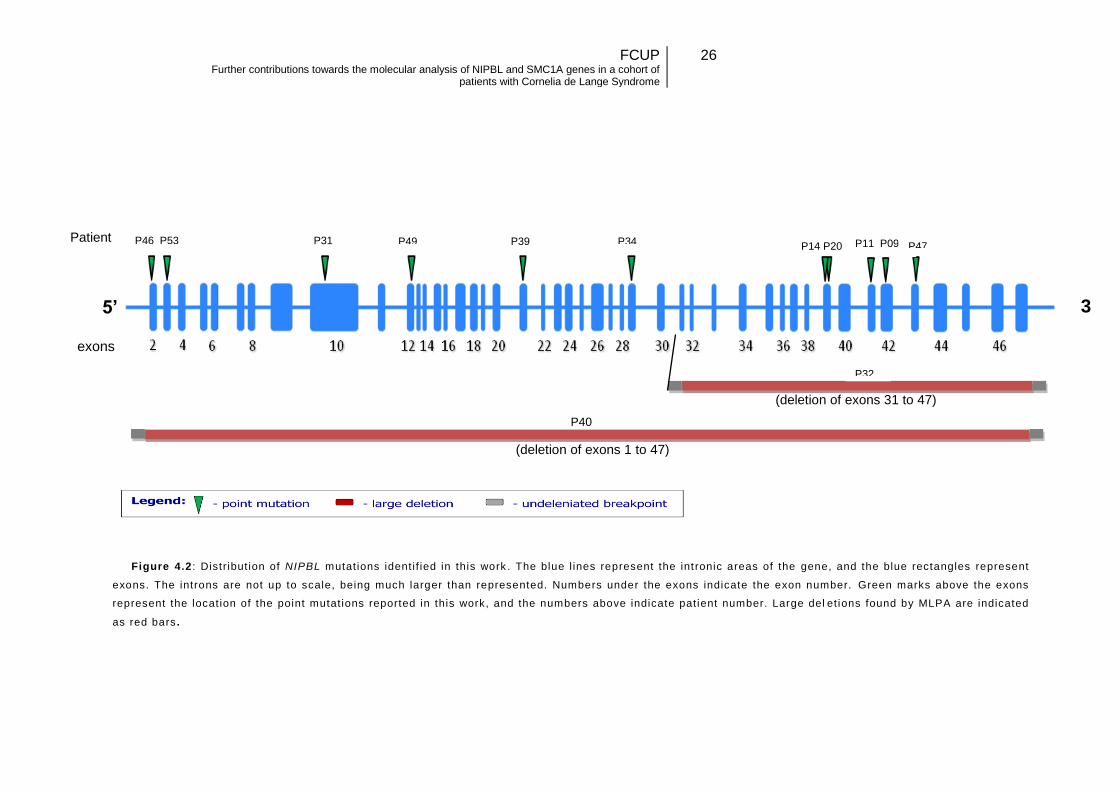
A total of 11 NIPBL point mutations were detected using this approach (Table 4.1).
These variants seem to be dispersed along NIPBL gene (Figure 4.2) without a clear
mutational hotspot.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
25
a) Mutations are described using NIPBL cDNA reference sequence with accession number: NM_133433.3, according with HGVS nomenclature guidelines; SEQ – Sequencing; MLPA – Multiplex ligation
probe amplification; b) CdLS clinical classification according to Kline et al., (2007); c) first report describing variant; d) somatic mosaicism suspected; e) other complete deletions of NIPBL has been
described in the literature, since the breakpoints of this mutation are still unidentified, it is not possible to known if it is the same mutation or not.
Patient Mutationa) Gene Location Predicted
polypeptide change Type
Variant/
Origin Detection
Clinical
Phenotypeb) Referencesc)
P46 c.64+1G>A Exon 2 p.(?) splicing de novo SEQ. mild Borck et al., 2004
P53 c.86del Exon 3 p.Pro29Hisfs*18 frameshift unknown SEQ. severe Novel
P31 c.1885C>Td) Exon 10 p.(Arg629*) nonsense unknown SEQ moderate Myake et al., 2005
P49 c.3316C>T Exon 12 p.(Arg1106*) nonsense de novo SEQ mild Miyake et al., 2005
P39 c.4422G>T Exon 21 p.(Arg1474Ser) missense de novo SEQ mild Oliveira et al., 2010
P34 c.5471C>T Exon 29 p.(Ser1824Leu) missense unknown SEQ mild Oliveira et al., 2010
P14 c.6653_6655delATA Exon 39 p.(Asn2218del) in-frame deletion de novo SEQ moderate Borck et al.,2004
P20 c.6763+5G>T Intron 39 p.(?) splicing unknown SEQ mild Krantz et al., 2004
P11 c.6983C>G Exon 41 p.(Thr2328Arg) missense unknown SEQ n.a. Novel
P09 c.7168G>A Exon 42 p.(Ala2390Thr) missense de novo SEQ moderate Gillis et al.,2004
P47 c.7307C>T Exon 43 p.(Ala2436Val) missense de novo SEQ n.a. Novel
P40 c.(?_-481)_(*927_?)del Exon 1 to 47 p.(?) large deletion de novo MLPA severe unknowne
P32 c.(5710-?)_(*927_?)del Exon 31 to 47 p.(?) large deletion unknown MLPA severe Novel
Table 4.1: Mutat ions found in NIPBL gene
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
26
5’ 3
’ exons
Patient
Figure 4.2 : Distribut ion of NIPBL mutat ions ident i f ied in this work . The blue l ines represent the int ronic areas of the gene, and the blue rectangles represent
exons. The introns are not up to scale, being much larger than represented. Numbers under the exons indicate the exon number. Green marks above the exons
represent the locat ion of the point mutat ions reported in this work, and the numbers above indicate pat ient number. Large del et ions found by MLPA are indicated
as red bars .
13
P40
(deletion of exons 31 to 47)
(deletion of exons 1 to 47)
P46 P53 P31 P49 P39 P34 P14 P20 P11 P09 P47
P32
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
27
4.1.1. Mutations causing premature stop codons
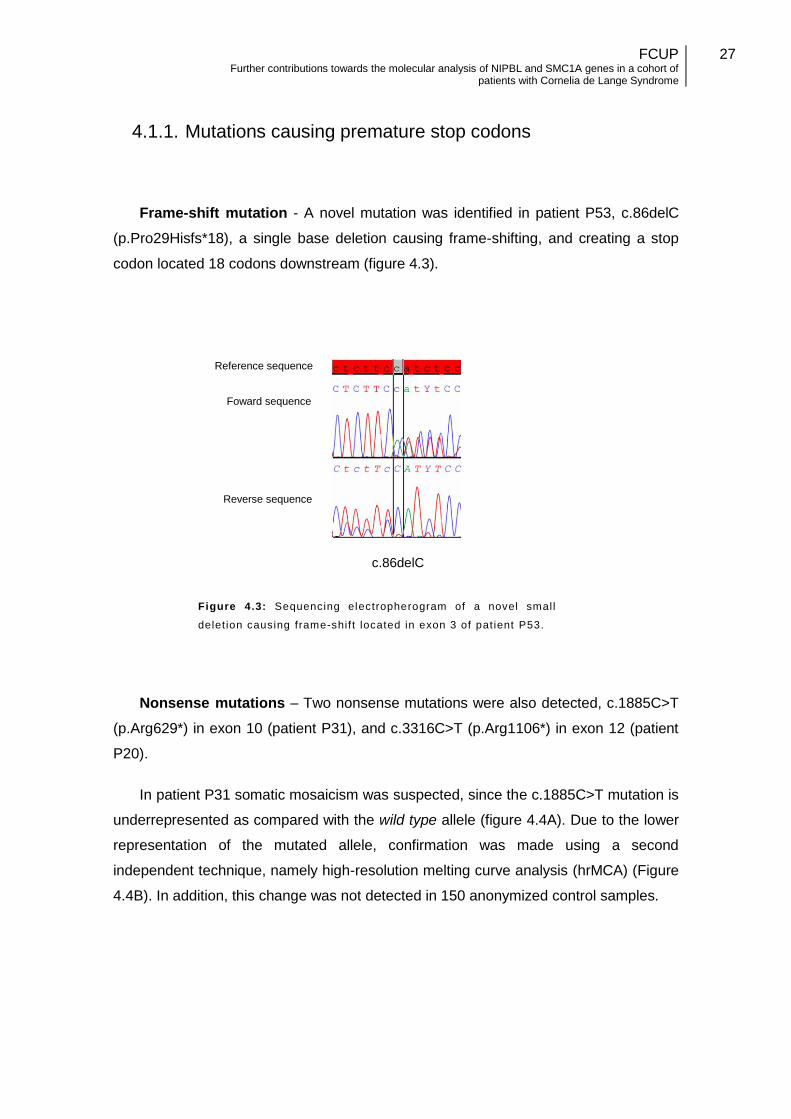
Frame-shift mutation - A novel mutation was identified in patient P53, c.86delC
(p.Pro29Hisfs*18), a single base deletion causing frame-shifting, and creating a stop
codon located 18 codons downstream (figure 4.3).
Figure 4.3: Sequencing electropherogram of a novel small
delet ion causing frame-shif t located in exon 3 of pat ient P53.
Nonsense mutations – Two nonsense mutations were also detected, c.1885C>T
(p.Arg629*) in exon 10 (patient P31), and c.3316C>T (p.Arg1106*) in exon 12 (patient
P20).
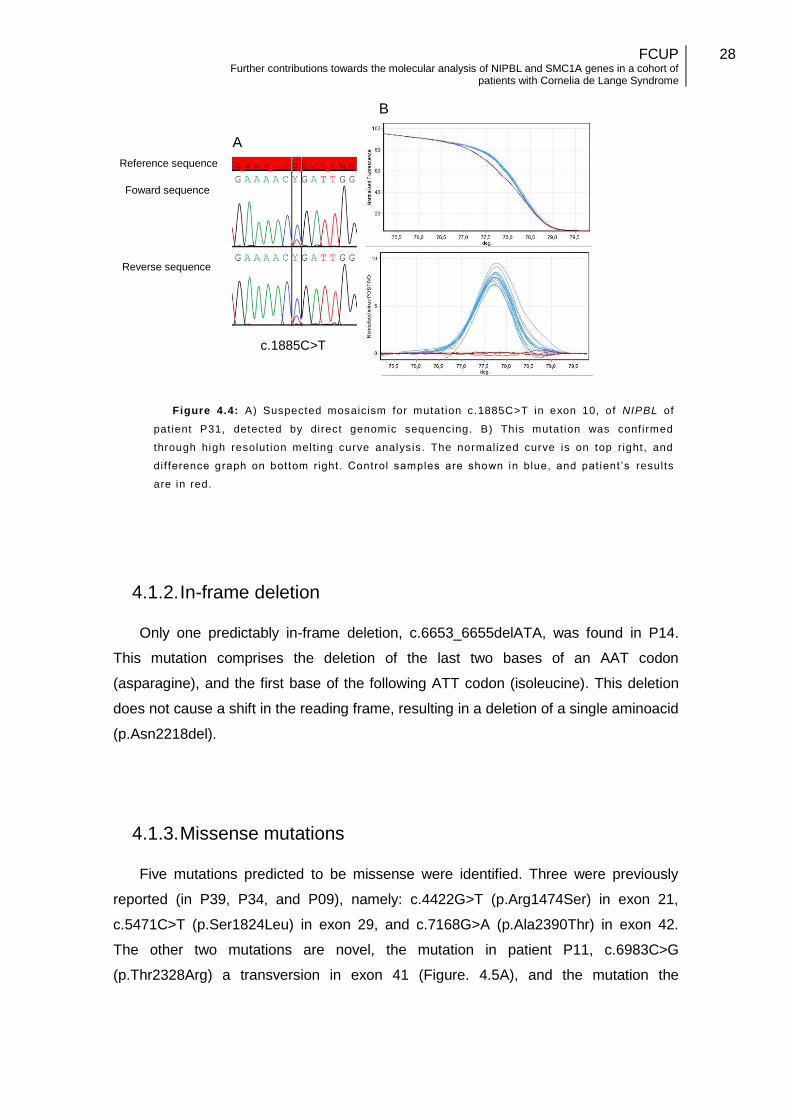
In patient P31 somatic mosaicism was suspected, since the c.1885C>T mutation is
underrepresented as compared with the wild type allele (figure 4.4A). Due to the lower
representation of the mutated allele, confirmation was made using a second
independent technique, namely high-resolution melting curve analysis (hrMCA) (Figure
4.4B). In addition, this change was not detected in 150 anonymized control samples.
c.86delC
Reference sequence
Foward sequence
Reverse sequence
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
28
4.1.2. In-frame deletion
Only one predictably in-frame deletion, c.6653_6655delATA, was found in P14.
This mutation comprises the deletion of the last two bases of an AAT codon
(asparagine), and the first base of the following ATT codon (isoleucine). This deletion
does not cause a shift in the reading frame, resulting in a deletion of a single aminoacid
(p.Asn2218del).
4.1.3. Missense mutations
Five mutations predicted to be missense were identified. Three were previously
reported (in P39, P34, and P09), namely: c.4422G>T (p.Arg1474Ser) in exon 21,
c.5471C>T (p.Ser1824Leu) in exon 29, and c.7168G>A (p.Ala2390Thr) in exon 42.
The other two mutations are novel, the mutation in patient P11, c.6983C>G
(p.Thr2328Arg) a transversion in exon 41 (Figure. 4.5A), and the mutation the
Figure 4.4: A) Suspected mosaicism for mutat ion c.1885C>T in exon 10, of NIPBL of
pat ient P31, detected by direct genomic sequencing. B) This mutat ion was conf irmed
through high resolut ion melt ing curve analysis. The normalized curve is on top right, and
dif ference graph on bottom right. Control samples are shown in blue, and pat ient ’s results
are in red.
c.1885C>T
Reference sequence
Foward sequence
Reverse sequence
A
B
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
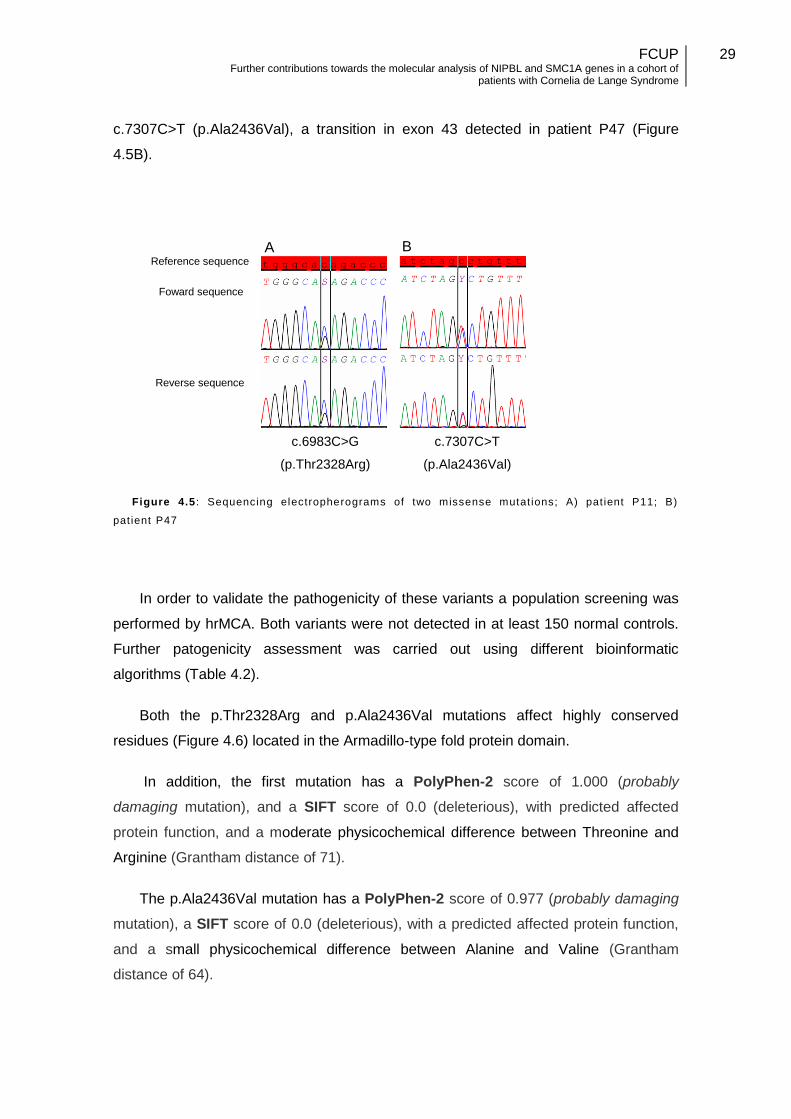
29
c.7307C>T (p.Ala2436Val), a transition in exon 43 detected in patient P47 (Figure
4.5B).
Figure 4.5 : Sequencing electropherograms of two missense mutat ions; A) pat ient P11; B)
pat ient P47
In order to validate the pathogenicity of these variants a population screening was
performed by hrMCA. Both variants were not detected in at least 150 normal controls.
Further patogenicity assessment was carried out using different bioinformatic
algorithms (Table 4.2).
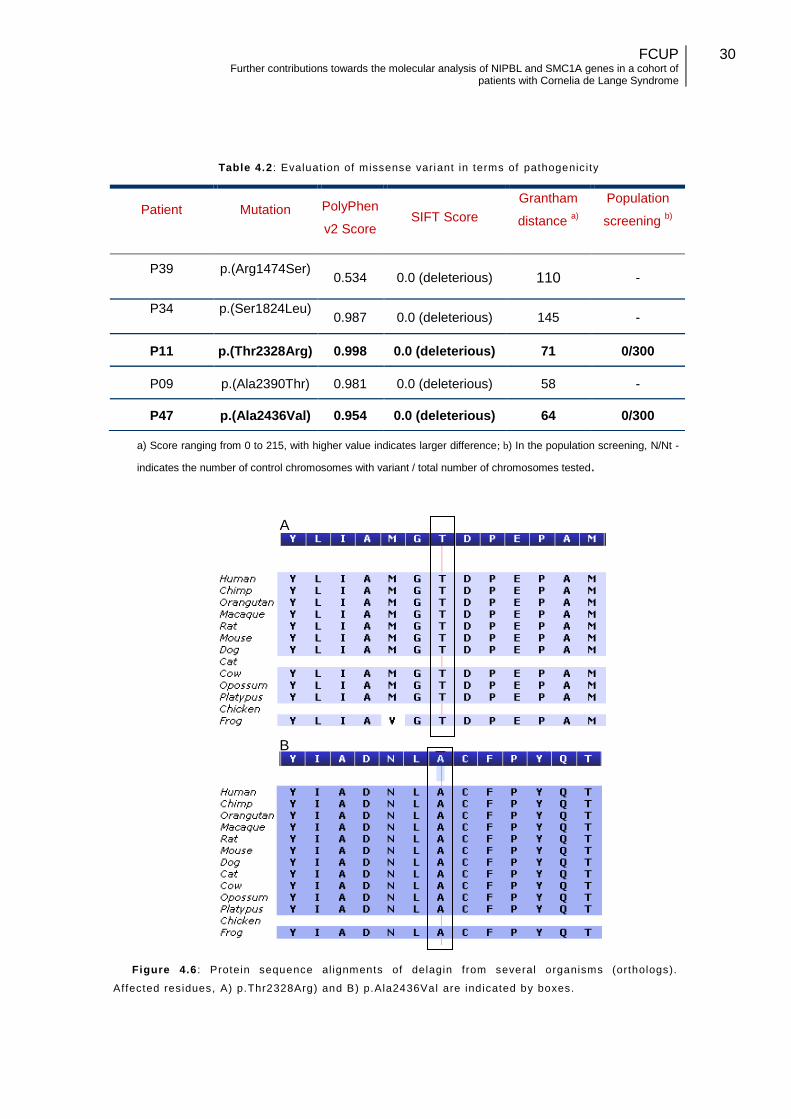
Both the p.Thr2328Arg and p.Ala2436Val mutations affect highly conserved
residues (Figure 4.6) located in the Armadillo-type fold protein domain.
In addition, the first mutation has a PolyPhen-2 score of 1.000 (probably
damaging mutation), and a SIFT score of 0.0 (deleterious), with predicted affected
protein function, and a moderate physicochemical difference between Threonine and
Arginine (Grantham distance of 71).
The p.Ala2436Val mutation has a PolyPhen-2 score of 0.977 (probably damaging
mutation), a SIFT score of 0.0 (deleterious), with a predicted affected protein function,
and a small physicochemical difference between Alanine and Valine (Grantham
distance of 64).
c.6983C>G
(p.Thr2328Arg)
Reference sequence
Foward sequence
Reverse sequence
A B
c.7307C>T
(p.Ala2436Val)
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
30
Table 4.2 : Evaluat ion of missense variant in terms of pathogenicity
a) Score ranging from 0 to 215, with higher value indicates larger difference; b) In the population screening, N/Nt -
indicates the number of control chromosomes with variant / total number of chromosomes tested.
Figure 4.6 : Protein sequence al ignments of delagin from several organisms (orthologs).
Affected residues, A) p.Thr2328Arg) and B) p.Ala2436Val are indicated by boxes.
Patient Mutation PolyPhen
v2 Score SIFT Score
Grantham
distance a)
Population
screening b)
P39 p.(Arg1474Ser) 0.534 0.0 (deleterious) 110 -
P34 p.(Ser1824Leu) 0.987 0.0 (deleterious) 145 -
P11 p.(Thr2328Arg) 0.998 0.0 (deleterious) 71 0/300
P09 p.(Ala2390Thr) 0.981 0.0 (deleterious) 58 -
P47 p.(Ala2436Val) 0.954 0.0 (deleterious) 64 0/300
A
B
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
31
The bioinformatic analysis results support the pathogenicity of the three previously
described mutations, and suggests that the two novel mutations are also pathogenic.
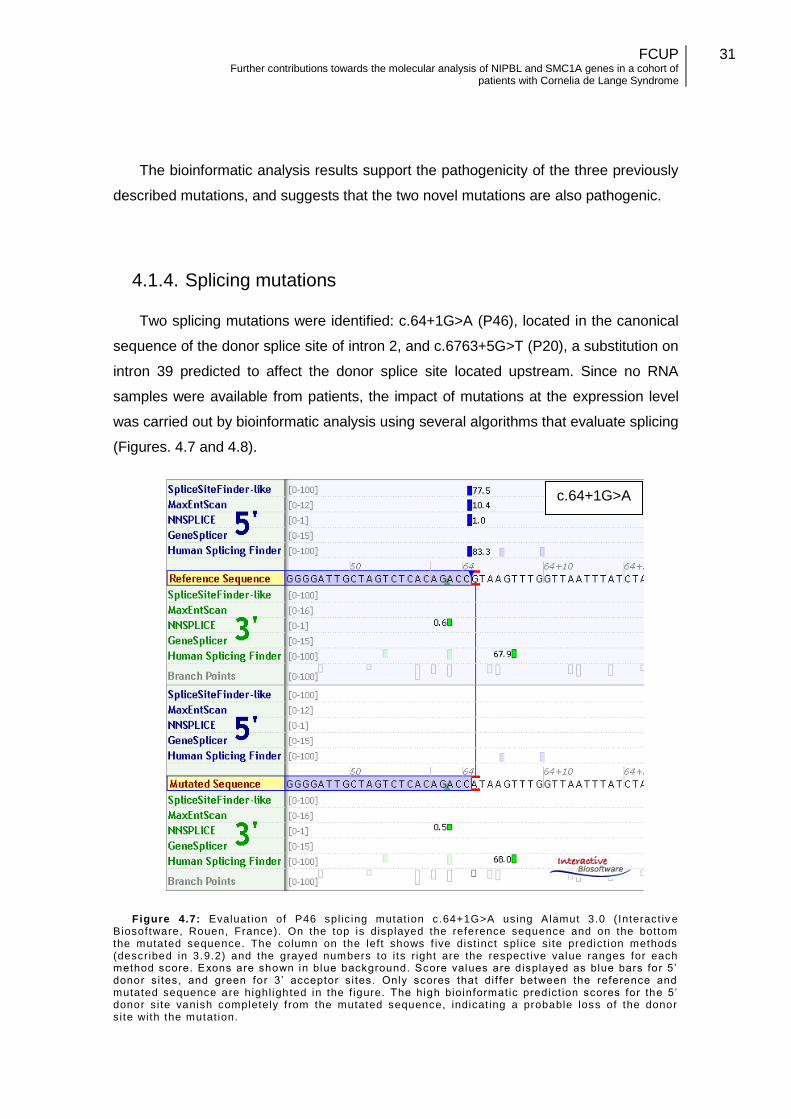
4.1.4. Splicing mutations
Two splicing mutations were identified: c.64+1G>A (P46), located in the canonical
sequence of the donor splice site of intron 2, and c.6763+5G>T (P20), a substitution on
intron 39 predicted to affect the donor splice site located upstream. Since no RNA
samples were available from patients, the impact of mutations at the expression level
was carried out by bioinformatic analysis using several algorithms that evaluate splicing
(Figures. 4.7 and 4.8).
Figure 4.7: Evaluat ion of P46 spl ic ing mutat ion c.64+1G>A using Alamut 3.0 ( Interact iv e Biosoftware, Rouen, France). On the top is displayed the reference sequence and on the bottom the mutated sequence. The column on the left shows f ive dist inct spl ice site predict ion methods (described in 3.9.2) and the grayed numbers to i ts r ight are the respect ive value ranges for each method score. Exons are shown in blue background. Score values are displayed as blue bars for 5 ’ donor sites, and green for 3’ acceptor si tes. Only scores that dif fer between the reference and mutated sequence are highl ighted in the f igure. The high bioinformatic predict ion scores for the 5’ donor site vanish completely from the mutated sequence, indicat ing a probable loss of the donor site with the mutat ion.
c.64+1G>A
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
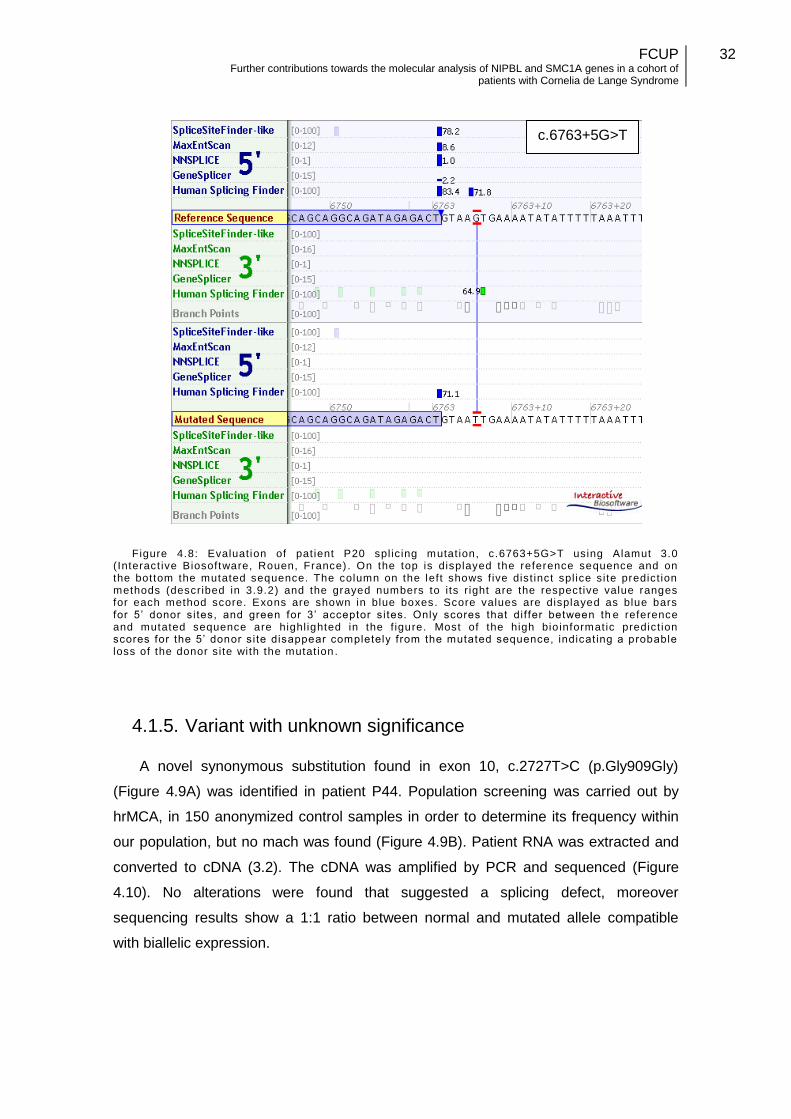
32
Figure 4.8: Evaluat ion of pat ient P20 spl ic ing mutat ion, c.6763+5G>T using Alamut 3.0 (Interact ive Biosoftware, Rouen, France) . On the top is displayed the reference sequence and on the bottom the mutated sequence. The column on the left shows f ive dist inct spl ice site predict ion methods (described in 3.9.2) and the grayed numbers to i ts r ight are the respect ive value ranges for each method score. Exons are shown in blue boxes. Score values are displayed as blue bars for 5’ donor sites, and green for 3’ acceptor si tes. Only scores that dif fer between th e reference and mutated sequence are highl ighted in the f igure. Most of the high bioinformatic predict ion scores for the 5’ donor site disappear completely from the mutated sequence, indicat ing a probable loss of the donor site with the mutat ion .
4.1.5. Variant with unknown significance
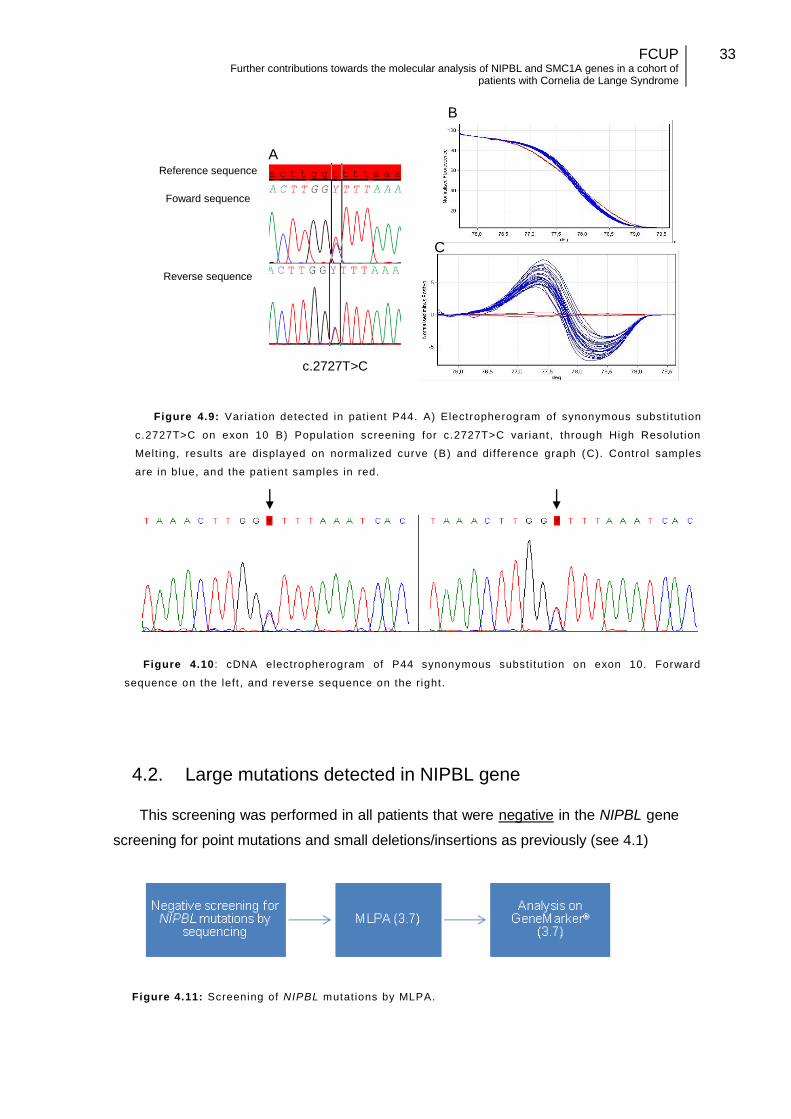
A novel synonymous substitution found in exon 10, c.2727T>C (p.Gly909Gly)
(Figure 4.9A) was identified in patient P44. Population screening was carried out by
hrMCA, in 150 anonymized control samples in order to determine its frequency within
our population, but no mach was found (Figure 4.9B). Patient RNA was extracted and
converted to cDNA (3.2). The cDNA was amplified by PCR and sequenced (Figure
4.10). No alterations were found that suggested a splicing defect, moreover
sequencing results show a 1:1 ratio between normal and mutated allele compatible
with biallelic expression.
c.6763+5G>T
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
33
.
4.2. Large mutations detected in NIPBL gene
This screening was performed in all patients that were negative in the NIPBL gene
screening for point mutations and small deletions/insertions as previously (see 4.1)
Figure 4.11: Screening of NIPBL mutat ions by MLPA.
c.2727T>C
Figure 4.9: Variat ion detected in pat ient P44. A) Electropherogram of synonymous subst i tut ion
c.2727T>C on exon 10 B) Populat ion screening for c.2727T>C variant, through High Resolut ion
Melt ing, results are displayed on normalized curve (B) and dif ference graph (C). Control samples
are in blue, and the pat ient samples in red.
Figure 4.10 : cDNA electropherogram of P44 synonymous subst i tut ion on exon 10. Forward
sequence on the left , and reverse sequence on the right.
Reference sequence
Foward sequence
Reverse sequence
A
B
C
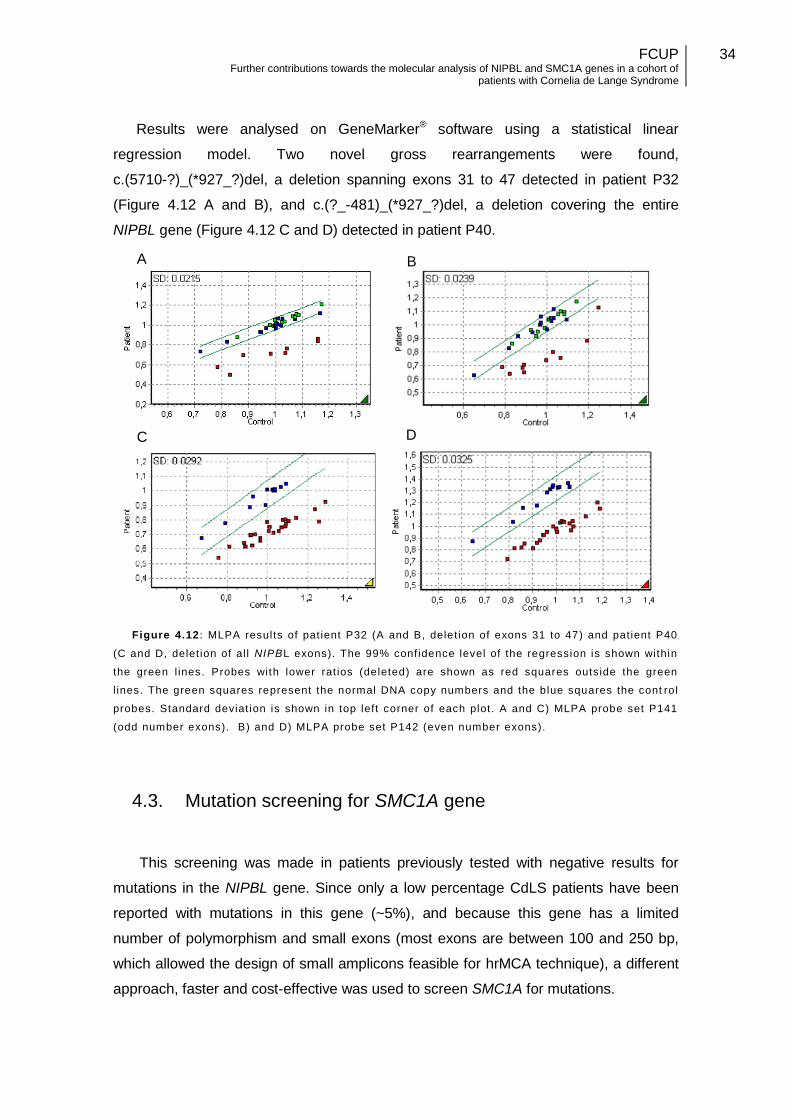
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
34
Results were analysed on GeneMarker® software using a statistical linear
regression model. Two novel gross rearrangements were found,
c.(5710-?)_(*927_?)del, a deletion spanning exons 31 to 47 detected in patient P32
(Figure 4.12 A and B), and c.(?_-481)_(*927_?)del, a deletion covering the entire
NIPBL gene (Figure 4.12 C and D) detected in patient P40.
Figure 4.12 : MLPA results of pat ient P32 (A and B, delet ion of exons 31 to 47) and pat ient P40
(C and D, delet ion of al l NIPBL exons). The 99% confidence level of the regression is shown within
the green l ines. Probes with lower rat ios (deleted) are shown as red squares outside the green
l ines. The green squares represent the normal DNA copy numbers and the blue squares the cont rol
probes. Standard deviat ion is shown in top left corner of each plot. A and C) MLPA probe set P141
(odd number exons). B) and D) MLPA probe set P142 (even number exons).
4.3. Mutation screening for SMC1A gene
This screening was made in patients previously tested with negative results for
mutations in the NIPBL gene. Since only a low percentage CdLS patients have been
reported with mutations in this gene (~5%), and because this gene has a limited
number of polymorphism and small exons (most exons are between 100 and 250 bp,
which allowed the design of small amplicons feasible for hrMCA technique), a different
approach, faster and cost-effective was used to screen SMC1A for mutations.
A B
C D
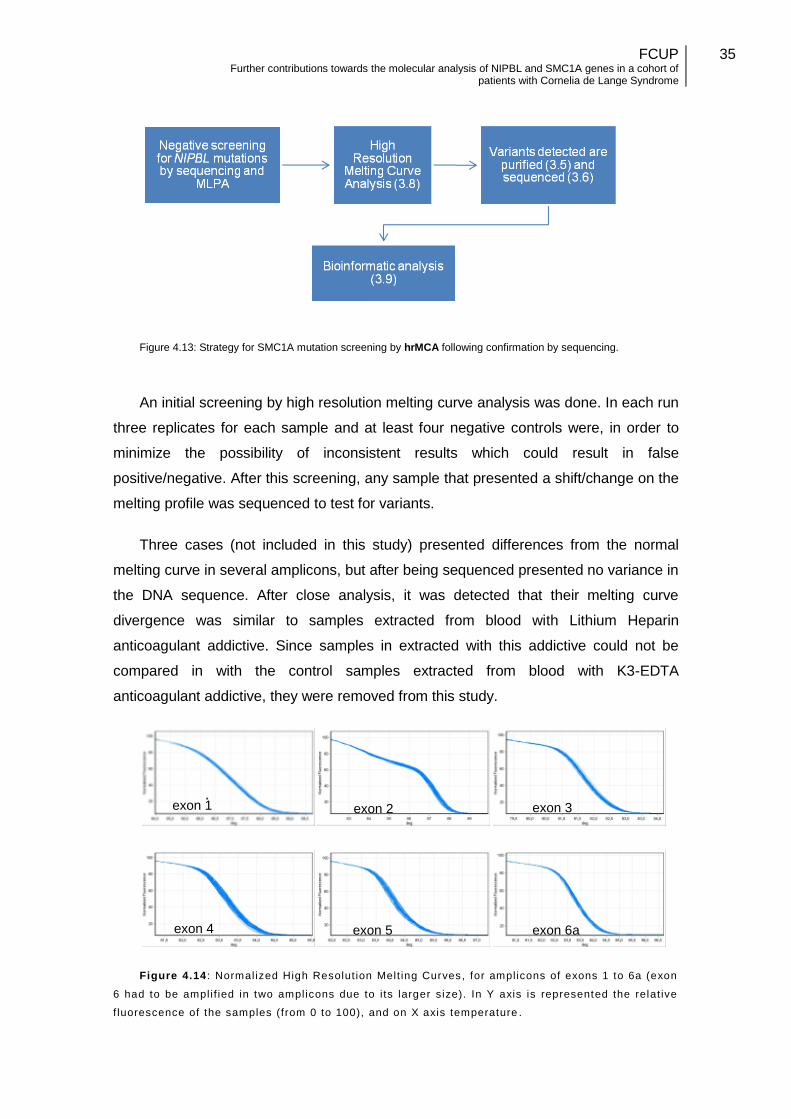
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
35
Figure 4.13: Strategy for SMC1A mutation screening by hrMCA following confirmation by sequencing.
An initial screening by high resolution melting curve analysis was done. In each run
three replicates for each sample and at least four negative controls were, in order to
minimize the possibility of inconsistent results which could result in false
positive/negative. After this screening, any sample that presented a shift/change on the
melting profile was sequenced to test for variants.
Three cases (not included in this study) presented differences from the normal
melting curve in several amplicons, but after being sequenced presented no variance in
the DNA sequence. After close analysis, it was detected that their melting curve
divergence was similar to samples extracted from blood with Lithium Heparin
anticoagulant addictive. Since samples in extracted with this addictive could not be
compared in with the control samples extracted from blood with K3-EDTA
anticoagulant addictive, they were removed from this study.
Figure 4.14 : Normalized High Resolut ion Melt ing Curves, for amplicons of exons 1 to 6a (exon
6 had to be ampli f ied in two amplicons due to i ts larger size). In Y axis is represented the relat ive
f luorescence of the samples (from 0 to 100), and on X axis temperature .
exon 1
exon 4
exon 3
exon 5 exon 6a
exon 2
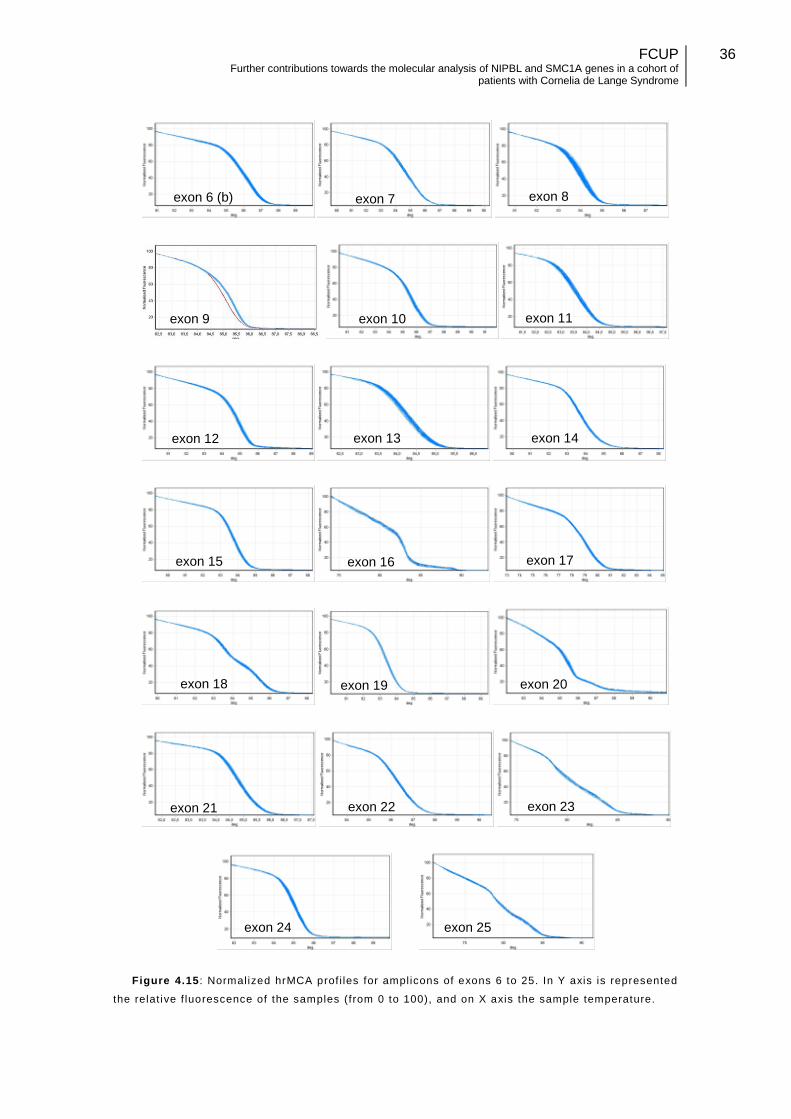
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
36
Figure 4.15 : Normalized hrMCA prof i les for amplicons of exons 6 to 25. In Y axis is represented
the relat ive f luorescence of the samples (from 0 to 100), and on X axis the sample temperature.
exon 9 exon 11
exon 12
exon 22 exon 23
exon 24 exon 25
exon 6 (b) exon 8 exon 7
exon 13 exon 14
exon 15 exon 16 exon 17
exon 18 exon 19 exon 20
exon 21
exon 10
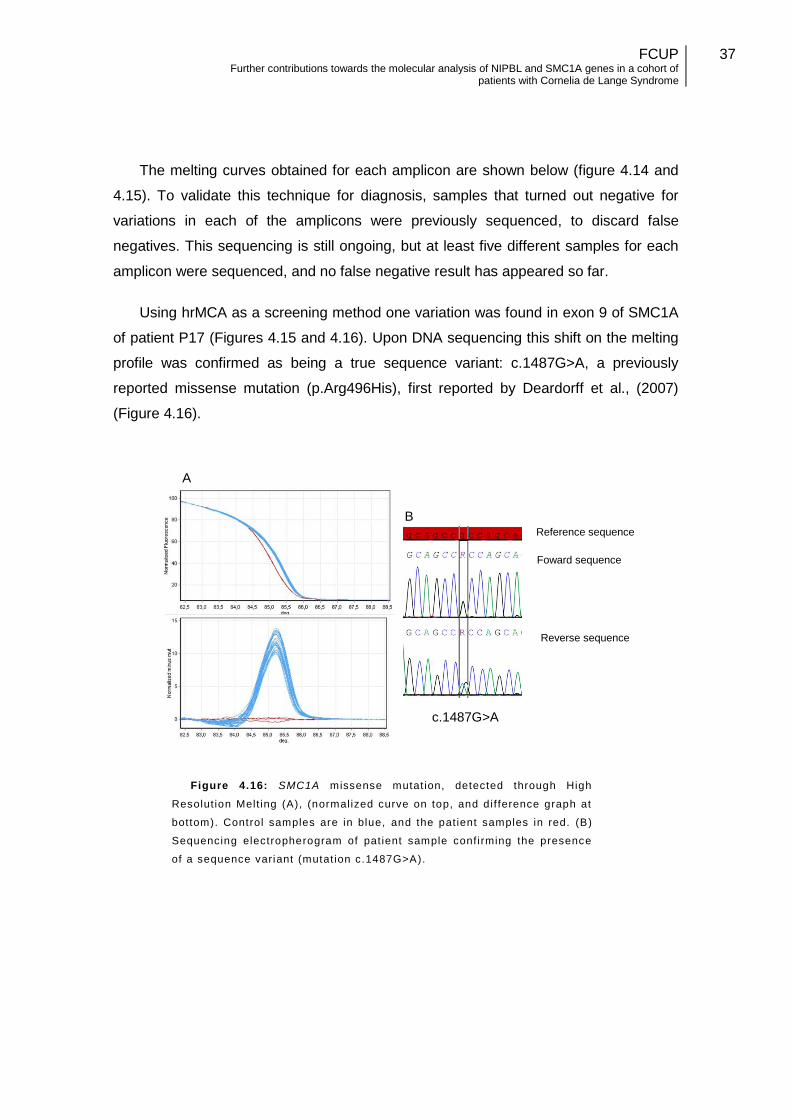
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
37
The melting curves obtained for each amplicon are shown below (figure 4.14 and
4.15). To validate this technique for diagnosis, samples that turned out negative for
variations in each of the amplicons were previously sequenced, to discard false
negatives. This sequencing is still ongoing, but at least five different samples for each
amplicon were sequenced, and no false negative result has appeared so far.
Using hrMCA as a screening method one variation was found in exon 9 of SMC1A
of patient P17 (Figures 4.15 and 4.16). Upon DNA sequencing this shift on the melting
profile was confirmed as being a true sequence variant: c.1487G>A, a previously
reported missense mutation (p.Arg496His), first reported by Deardorff et al., (2007)
(Figure 4.16).
Figure 4.16: SMC1A missense mutat ion, detected through High
Resolut ion Melt ing (A), (normalized curve on top, and dif ference graph at
bottom). Control samples are in blue, and the pat ient samples in red. (B)
Sequencing electropherogram of pat ient sample conf irming the presence
of a sequence variant (mutat ion c.1487G>A).
c.1487G>A
B
A
Reference sequence
Foward sequence
Reverse sequence
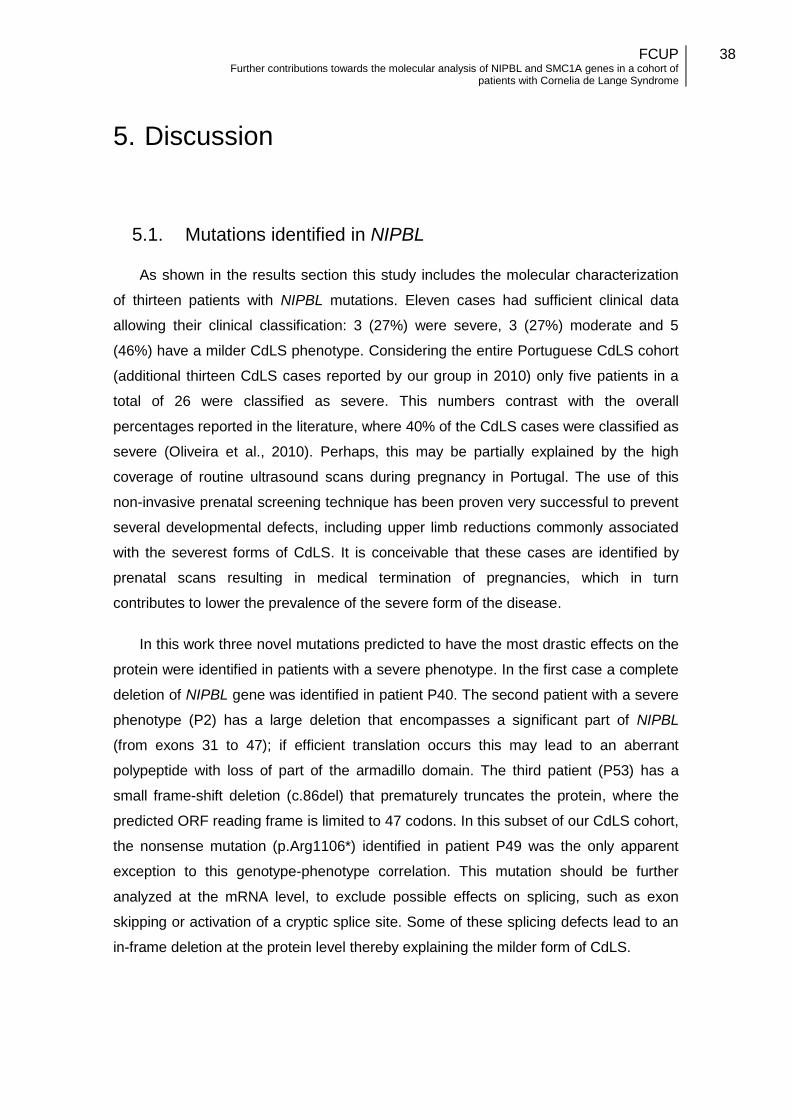
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
38
5. Discussion
5.1. Mutations identified in NIPBL
As shown in the results section this study includes the molecular characterization
of thirteen patients with NIPBL mutations. Eleven cases had sufficient clinical data
allowing their clinical classification: 3 (27%) were severe, 3 (27%) moderate and 5
(46%) have a milder CdLS phenotype. Considering the entire Portuguese CdLS cohort
(additional thirteen CdLS cases reported by our group in 2010) only five patients in a
total of 26 were classified as severe. This numbers contrast with the overall
percentages reported in the literature, where 40% of the CdLS cases were classified as
severe (Oliveira et al., 2010). Perhaps, this may be partially explained by the high
coverage of routine ultrasound scans during pregnancy in Portugal. The use of this
non-invasive prenatal screening technique has been proven very successful to prevent
several developmental defects, including upper limb reductions commonly associated
with the severest forms of CdLS. It is conceivable that these cases are identified by
prenatal scans resulting in medical termination of pregnancies, which in turn
contributes to lower the prevalence of the severe form of the disease.
In this work three novel mutations predicted to have the most drastic effects on the
protein were identified in patients with a severe phenotype. In the first case a complete
deletion of NIPBL gene was identified in patient P40. The second patient with a severe
phenotype (P2) has a large deletion that encompasses a significant part of NIPBL
(from exons 31 to 47); if efficient translation occurs this may lead to an aberrant
polypeptide with loss of part of the armadillo domain. The third patient (P53) has a
small frame-shift deletion (c.86del) that prematurely truncates the protein, where the
predicted ORF reading frame is limited to 47 codons. In this subset of our CdLS cohort,
the nonsense mutation (p.Arg1106*) identified in patient P49 was the only apparent
exception to this genotype-phenotype correlation. This mutation should be further
analyzed at the mRNA level, to exclude possible effects on splicing, such as exon
skipping or activation of a cryptic splice site. Some of these splicing defects lead to an
in-frame deletion at the protein level thereby explaining the milder form of CdLS.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
39
Figure 5.1 : Representat ion of the NIPBL gene with the distribut ion of al l known point and small del/ ins mutat ions throughout the gene. The
blue rectangles represent the exons, and the white rectangles represent the int rons, and the blue rectangles The i ntronic region is are not up to
scale, being much larger than represented especial ly intron one. The pale blue rectangles are the non-coding exonic areas of the gene. Numbers
under the exons indicate the odd exons. Each red bar marked above represents the mutat ion frequency along the gene.
5’ 3’
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
40
The eleven point mutations detected in the NIPBL seem to be spread along the
gene without an apparent mutational hotspot, although their distribution seems non-
random. The majority of the reported NIPBL mutations are located in regions of the
gene with a higher mutation frequency (Figure 5.1) (Oliveira et al., 2010). A probable
explanation to this is the presence of gene specific sequence context such as
hypermutable CpG dinucleotides that might be affected by methylation-mediated
deamination (Cooper and Youssoufian, 1988), regions of repetitive sequences (like
short tandem repeats) and/or homopolymeric nucleotide stretches that are susceptible
to replication errors. In fact, the mutation detected on patient P14
(c.6653_6655delATA) is one of the most frequent recurrent mutations of the NIPBL
gene, being also an example of a mutation occurring in a repetitive sequences stretch
(deletion of one of three ATA repeats). In addition, five single substitutions c.64+1G>A
(patient P46), c.1885C>T (patient P10), c.3316C>T (patient P49), c.5471C>T (patient
P34), c.7168G>A (patient P09) are located in CpG dinucleotides. Seven mutations
including five missense mutations, an in-frame deletion and a change affecting splicing
were found inside the armadillo domain of delangin. This protein domain occupies a
considerable part of the gene (exons 13 to 37) and it is located in a highly conserved
region (Jahnke et al., 2008).
5.1.1. Detection of large NIPBL deletions by MLPA
Two large deletions in the NIPBL gene were found in our patients:
c.(?_-481)_(*927_?)del and c.(5710-?)_(*927_?)del. Although, CdLS diagnosis has
been confirmed, further molecular characterization should be made to determine the
breakpoints of these mutations. In the case of the patient with a complete deletion of
NIPBL (P40), this delineation would be of clinical importance to confirm or exclude the
involvement of neighboring genes. However, the patient has decease and there are no
additional biological samples available for analysis. The detection of two NIPBL gross
deletions in 3.8% of our patients (2/53) is quite relevant as compare to other CdLS
genes detection rates (please see section 5.3). It shows the importance of using MLPA
technique after exclusion of point mutations by genomic sequencing in order to
increase the overall NIPBL mutation detection rate. These numbers are very similar to
those reported in a recent study, where the same strategy detected mutations in 3.5%
of patients (7/200) (Russo et al., 2012). Overall, these results confirm the
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
41
recommendation for the use of MLPA technique on NIPBL in a routine molecular
diagnostic setting.
5.1.2. Somatic mosaicism
As it was shown in the results section, the c.1885C>T mutation (p.Arg629*) in exon
10 of patient P31 was suspected of somatic mosaicism. Compared to the wild type (wt)
the mutated allele is under-represented, <25% of the fluorescence intensity of the wt
allele, estimated by comparing both signals in the sequence electropherogram. This
mutation if not carefully looked-up could have been missed during analysis using
default settings. Myake et al. (2005) reported a Japanese patient having this nonsense
mutation associated to a severe phenotype; while patient P31 was classified as
moderate. This discrepancy is also in favor of mosaicism, since patients with mosaic
mutations tend to express an attenuated phenotype than non-mosaic patients with the
same mutation (Kluwe et al., 2003). For further characterization of this case
quantitative methods such as real-time PCR should be applied to quantify the
percentage of cells with the mutation as compared to wt, ideally this quantification
should be perform on DNA obtained from different tissues (from distinct germ layers).
Mendelian disorders with a high frequency of de novo mutations (as is the case of
CdLS) have a relatively frequent occurrence of somatic mosaicism (Castronovo et al.,
2010). However very few of such cases have been reported in NIPBL so far
(http://www.lovd.nl/NIPBL, last accessed September 2012). It is possible that some
somatic mutations with low-level mutant alleles could escape detection by routine
sequencing methods. Somatic mosaicism in NIPBL gene could help to explain the
phenotypic variability of patients, and is another source of clinical and genetic
heterogeneity of this syndrome (Castronovo et al., 2010). These observations raise the
possibility that mutation rates of genes involved in CdLS are currently underestimated.
In addition, as demonstrated by the use of hrMCA technique it is important to combine
different techniques for diagnosis purposes. In molecularly unresolved cases next
generation sequencing (NGS) would be a powerful tool to detect pathogenic mosaic
mutations since this approach, specially using a high coverage strategy, is sensible
enough to detect low allele frequencies (Pagnamenta et al., 2012). Furthermore, Next
generation sequencing (NGS) allows the screening of several genes simultaneously
which is another advantage for its use in this field.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
42
5.1.3. Novel silent polymorphism
The apparently silent substitution c.2727T>C sequence variant in NIPBL detected
in patient P44 was further studied at the mRNA level. We have shown that this change,
although it was not detected in control samples, does not have an impact on splicing
(inclusion of exon 10). Very recently this variant was reported in the Single Nucleotide
Polymorphism database of NCBI (dbSNP, rs148394805), as a rare variant with an
allelic frequency of only 0.2%. Due to its very low frequency it was not detected during
our population screening.
5.2. Implementation of hrMCA for SMC1A
One of the goals of this work was to set up a molecular diagnostic for mutation
screening in SMC1A gene. The fast, efficiency and low-cost of the hrMCA technique,
combined with the gene characteristics (small easily amplifiable exons and limited
number of polymorphisms) made this technique an ideal choice for the mutation
screening of SMC1A. This is the first known study to apply hrMCA technique for
mutation screening on SMC1A gene. While there are no references in the literature for
the use of the technique in this gene, studies in other genes stated the robustness,
high-throughput, high sensitivity and low false positive ratio of this technique (Millat et
al., 2009; Santos et al., 2012). Because of its high sensitivity the melting curve profile
can be altered by several secondary factors like the presence of primer-dimers,
amplification of non specific products, or using DNA templates with different
concentrations or quality/purity. These might cause false positives results but it can be
easily avoided by a good PCR optimization. The use of at least three replicas for each
sample and the inclusion of previously genotyped controls may avoid problems with
individual samples. Amplicons that present a shifted melting curve have to be
sequenced. Although, this technique is extremely sensitive to detect a variation, it
cannot determine what the precise sequence change is unless positive controls are
added to the same run. DNA sequencing after hrMCA is also useful to exclude false
positives. hrMCA scanning accuracy depends on high quality PCR (Santos et al., 2012),
but as long as optimal PCR conditions can be assured, and if combined with genome
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
43
sequencing to validate results, this technique can provide an fast and effective way of
screening SMC1A gene for mutations.
The proof-of-principle of the successful deployment of this technique for mutation
scanning in SMC1A was the identification of a sequence variant (c.1487G>A) in patient
P17, initially detected by hrMCA and later confirmed by genomic sequencing. This
missense mutation (p.Arg496His) identified in exon 9 of SMC1A, was previously
reported in six other CdLS patients (Deardorff et al., 2007). The mutation occurs in the
SMC flexible hinge domain. A previous study reported that mutations in this domain
increase the affinity for DNA binding, comparing with the wild type proteins (Revenkova
et al., 2009).
5.3. Mutation detection rate
The Portuguese CdLS patient cohort studied by our group includes a total of fifty-
three individuals studied by different techniques applied to SMC1A and NIPBL genes.
Overall results have allowed the successful molecular characterization of twenty-seven
patients, the majority with mutations in NIPBL gene and only one case with a
pathogenic variant in SMC1A (Table 5.1).
The mutation detection rate for NIPBL gene is 49.1% (26/53) which is within the
range of values (40-60%) indicated in the literature for this locus (Russo et al., 2012).
Although some research groups report mutation detection rates for NIPBL gene up to
60%. This might be attributed to different inclusion or exclusion criteria for selection of
patients that could lead for the mildest phenotypes to be excluded from NIPBL gene
analysis.
Concerning SMC1A gene, the mutation detection rate was 1.9% below the 5%
detection rate reported in the literature by other groups (Russo et al., 2012). One
possible explanation may be attributed to the fact that SMC1A gene was not completed
sequenced in all NIPBL-negative cases. It is conceivable that some mutations may
have not been detected by hrMCA that was used as a prospective scanning method.
SMC1A sequencing analysis should be performed in all molecularly unresolved cases
to exclude the involvement of this locus.
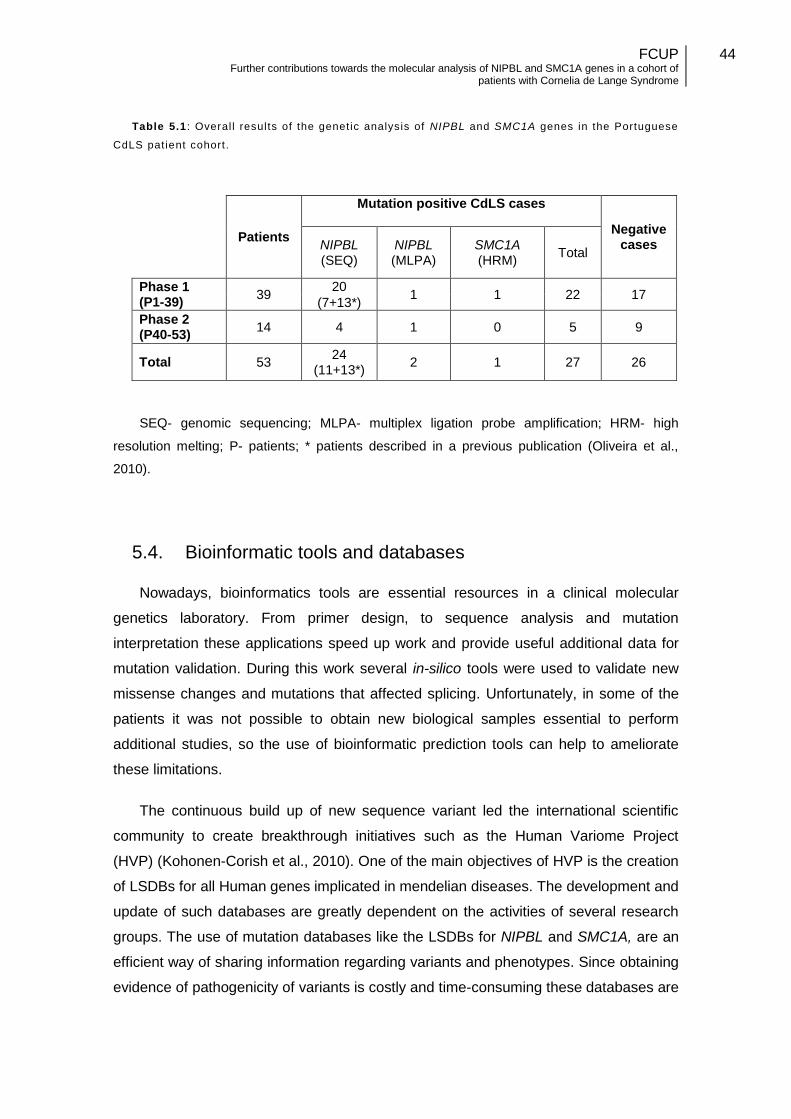
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
44
Table 5.1 : Overal l results of the genetic analysis of NIPBL and SMC1A genes in the Portuguese
CdLS pat ient cohort.
SEQ- genomic sequencing; MLPA- multiplex ligation probe amplification; HRM- high
resolution melting; P- patients; * patients described in a previous publication (Oliveira et al.,
2010).
5.4. Bioinformatic tools and databases
Nowadays, bioinformatics tools are essential resources in a clinical molecular
genetics laboratory. From primer design, to sequence analysis and mutation
interpretation these applications speed up work and provide useful additional data for
mutation validation. During this work several in-silico tools were used to validate new
missense changes and mutations that affected splicing. Unfortunately, in some of the
patients it was not possible to obtain new biological samples essential to perform
additional studies, so the use of bioinformatic prediction tools can help to ameliorate
these limitations.
The continuous build up of new sequence variant led the international scientific
community to create breakthrough initiatives such as the Human Variome Project
(HVP) (Kohonen-Corish et al., 2010). One of the main objectives of HVP is the creation
of LSDBs for all Human genes implicated in mendelian diseases. The development and
update of such databases are greatly dependent on the activities of several research
groups. The use of mutation databases like the LSDBs for NIPBL and SMC1A, are an
efficient way of sharing information regarding variants and phenotypes. Since obtaining
evidence of pathogenicity of variants is costly and time-consuming these databases are
Patients
Mutation positive CdLS cases
Negative cases NIPBL
(SEQ) NIPBL (MLPA)
SMC1A (HRM)
Total
Phase 1 (P1-39)
39 20
1 1 22 17 (7+13*)
Phase 2 (P40-53)
14 4 1 0 5 9
Total 53 24
(11+13*) 2 1 27 26
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
45
also important resources for diagnostic laboratories, which can rapidly cross-check if a
sequence changes in one of the CdLS genes have been already reported.
5.5. Procedure for the molecular diagnostic of CdLS patients
Due to the genetic complexity of CdLS which concerns different mutation types and
multiple genes, a procedure flowchart for the genetic molecular diagnostic of CdLS is
proposed (Figure 5.2). The sequential order of the different techniques was established
considering their sensitivity to optimize time and economical resources. The first gene
that should be considered for analysis is NIPBL since the majority of mutations
described up to now are related to this locus. Direct genomic sequence should be the
first technique to be applied, considering that the most frequent variants are point
mutations or small deletions/insertions. Although it was not included in the flowchart, it
is of importance to emphasize that approximately 80% of NIPBL mutations described to
date are located on 21 exons (out of a total of 47) (Oliveira et al., 2010). Therefore,
NIPBL sequencing step may be sub-divided in two steps, starting by exons with higher
mutation frequency and afterwards sequencing the remaining 26 exons of NIPBL with
less mutations reported. Theoretically, this partial NIPBL gene sequencing would allow
detection of mutations in about one third of the CdLS patients. After NIPBL genomic
sequencing, cases still unresolved should be submitted to MLPA technique to detected
large deletions or duplication involving one or more exons of NIPBL. As discussed
above, this technique has a greater mutation detection rate than sequencing SMC1A
itself. Results have shown that hrMCA enables a fast and cost-effective scanning of
SMC1A. However, hrMCA technique must always be validated by genomic sequencing
to exclude false positives and polymorphisms.
As mentioned in the Introduction, besides NIPBL and SMC1A other genes, to be
precise SMC3, RAD21, and HDAC8, have been associated with milder CdLS (or
Cornelia-like) phenotypes in a limited number of cases (Revenkova et al., 2009;
Deardorff et al., 2012a). In spite of the low mutation detection rate, these genes should
be considered for genetic analysis, especially if there is a specific clinical request
based upon characteristic phenotypic traits or suggestive patterns of inheritance (such
as X-linked).
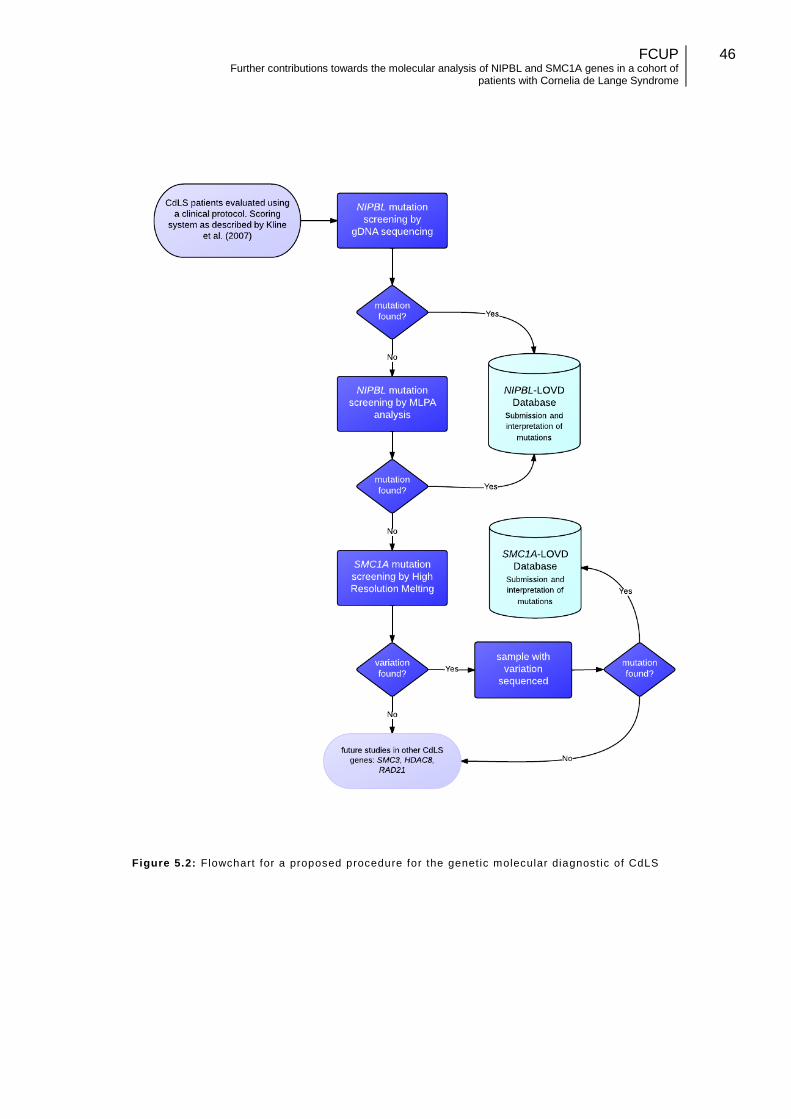
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
46
Figure 5.2: Flowchart for a proposed procedure for the genetic molecular diagnost ic of CdLS

FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
47
5.6. Future perspectives
All the available data within public domain suggests that at least 30% of CdLS
patients are still molecularly unsolved. This prompts to new lines of research dedicated
to the identification of new genetic causes for CdLS. The obvious candidates can be
found among the genes involved with the cohesion complex and their regulators. A
new technological paradigm is currently changing the face of Human Genetics, next
generation sequencing (NGS), which consist in extremely high-throughput genetic
analyzers. NGS technology can be used for CdLS research by at least two different
approaches. The first is based on the development of custom genomic libraries for
targeted resequencing where a number of candidate genes (such as those involved in
the cohesin complex) are selected and analyzed simultaneously in several patients. An
alternative strategy is in well selected CdLS patients perform a whole exome
sequencing, meaning that all the coding regions of all known Human genes are
sequenced to identify variants responsible for CdLS.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
48
6. Bibliography
Adzhubei IA, Schmidt S, Peshkin L, Ramensky VE, Gerasimova A, Bork P,
Kondrashov AS, Sunyaev SR. (2010). A method and server for predicting damaging
missense mutations. Nature Methods. 7(4):248-249.
Bhuiyan ZA, Stewart H, Redeker EJ, Mannens MM, Hennekam RC. (2007). Large
genomic rearrangements in NIPBL are infrequent in Cornelia de Lange syndrome.
European Journal of Human Genetics. 15(4):505-508.
Borck G, Redon R, Sanlaville D, Rio M, Prieur M, Lyonnet S, Vekemans M, Carter
NP, Munnich A, Colleaux L, Cormier-Daire V. (2004). NIPBL mutations and genetic
heterogeneity in Cornelia de Lange syndrome. Journal of Medical Genetics.
41(12):e128.
Borck G, Zarhrate M, Bonnefont JP, Munnich A, Cormier-Daire V, Colleaux L.
(2007). Incidence and clinical features of X-linked Cornelia de Lange syndrome due to
SMC1L1 mutations. Human Mutation. 28(2):205-206.
Braunholz D, Hullings M, Gil-Rodríguez MC, Fincher CT, Mallozzi MB, Loy E,
Albrecht M, Kaur M, Limon J, Rampuria A, Clark D, Kline A, Dalski A, Eckhold J,
Tzschach A, Hennekam R, Gillessen-Kaesbach G, Wierzba J, Krantz ID, Deardorff MA,
Kaiser FJ. (2012). Isolated NIBPL missense mutations that cause Cornelia de Lange
syndrome alter MAU2 interaction. European Journal of Human Genetics. 20(3):271-
276.
Buggy JJ, Sideris ML, Mak P, Lorimer DD, McIntosh B, Clark JM. (2000). Cloning
and characterization of a novel human histone deacetylase, HDAC8. Biochemical
Journal. 350 Pt 1:199-205.
Burpo FJ. (2001). A critical review of pcr primer design algorithms and cross-
hybridization case study. Biochemistry 2001:218-233
Carramolino L, Lee BC, Zaballos A, Peled A, Barthelemy I, Shav-Tal Y, Prieto I,
Carmi P, Gothelf Y, González de Buitrago G, Aracil M, Márquez G, Barbero JL, Zipori
D. (1997). SA-1, a nuclear protein encoded by one member of a novel gene family:
molecular cloning and detection in hemopoietic organs. Gene. 195(2):151-159.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
49
Castronovo P, Delahaye-Duriez A, Gervasini C, Azzollini J, Minier F, Russo S,
Masciadri M, Selicorni A, Verloes A, Larizza L. (2010). Somatic mosaicism in Cornelia
de Lange syndrome: a further contributor to the wide clinical expressivity? Clinical
Genetics. 78(6):560-564.
de Lange, C. (1933). Sur un type nouveau de dégénération (Typus
Amstelodamensis). Médecine des Enfants. XXXVI-12:714-719.
Deardorff MA, Kaur M, Yaeger D, Rampuria A, Korolev S, Pie J, Gil-Rodríguez C,
Arnedo M, Loeys B, Kline AD, Wilson M, Lillquist K, Siu V, Ramos FJ, Musio A,
Jackson LS, Dorsett D, Krantz ID. (2007). Mutations in cohesin complex members
SMC3 and SMC1A cause a mild variant of cornelia de Lange syndrome with
predominant mental retardation. American Journal of Human Genetics. 80(3):485-494.
Deardorff MA, Clark DM, Krantz ID. (2011). Cornelia de Lange Syndrome. Gene
Review. University of Washington, Seattle. Last accessed online on 27 September
2012 on: http://www.ncbi.nlm.nih.gov/books/NBK1104/.
Deardorff MA, Bando M, Nakato R, Watrin E, Itoh T, Minamino M, Saitoh K,
Komata M, Katou Y, Clark D, Cole KE, De Baere E, Decroos C, Di Donato N, Ernst S,
Francey LJ, Gyftodimou Y, Hirashima K, Hullings M, Ishikawa Y, Jaulin C, Kaur M,
Kiyono T, Lombardi PM, Magnaghi-Jaulin L, Mortier GR, Nozaki N, Petersen MB,
Seimiya H, Siu VM, Suzuki Y, Takagaki K, Wilde JJ, Willems PJ, Prigent C, Gillessen-
Kaesbach G, Christianson DW, Kaiser FJ, Jackson LG, Hirota T, Krantz ID, Shirahige
K. (2012a). HDAC8 mutations in Cornelia de Lange syndrome affect the cohesin
acetylation cycle. Nature. 489(7415):313-317.
Deardorff MA, Wilde JJ, Albrecht M, Dickinson E, Tennstedt S, Braunholz D,
Mönnich M, Yan Y, Xu W, Gil-Rodríguez MC, Clark D, Hakonarson H, Halbach S,
Michelis LD, Rampuria A, Rossier E, Spranger S, Van Maldergem L, Lynch SA,
Gillessen-Kaesbach G, Lüdecke HJ, Ramsay RG, McKay MJ, Krantz ID, Xu H,
Horsfield JA, Kaiser FJ. (2012b). RAD21 mutations cause a human cohesinopathy.
American Journal of Medical Genetics. 90(6):1014-1027.
Desmet FO, Hamroun D, Lalande M, Collod-Beroud G, Claustres M, Beroud C.
(2009) Human Splicing Finder: an online bioinformatics tool to predict splicing signals.
Nucleic Acid Research, 37(9):e67.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
50
Dias C., Costa E., Oliveira J., Silva J., Martins M., Fortuna A. M., Sousa A. B.,
Basto J. P., Soares-Silva I., Kay T., Santos H., Medeira A., Cordeiro I., Lourenço T.,
Nunes L., Santos R., Reis-Lima M. (2008). Clinical characterization and NIPBL
mutation analysis of 42 Portuguese patients with Cornelia de Lange Syndrome.
Barcelona, May 2008. European Society of Human Genetics. 16-2:97
Dorsett D. (2007). Cohesin, gene expression and development: lessons from
Drosophila. Chromosome Research. 17(2):185-200.
Dorsett D, Krantz ID. (2009). On the molecular etiology of Cornelia de Lange
syndrome. Annals of the New York Academy of Sciences. 1151:22-37.
Fay A, Misulovin Z, Li J, Schaaf CA, Gause M, Gilmour DS, Dorsett D. (2011).
Cohesin selectively binds and regulates genes with paused RNA polymerase. Current
Biology. 11;21(19):1624-1634.
Galehdari H, Monajemzadeh R, Nazem H, Mohamadian G, Pedram M. (2011).
dentification of a novel de novo mutation in the NIPBL gene in an Iranian patient with
Cornelia de Lange syndrome: A case report. Journal of Medical Case Reports. 5:242.
Geck P, Maffini MV, Szelei J, Sonnenschein C, Soto AM. (2000). Androgen-
induced proliferative quiescence in prostate cancer cells: the role of AS3 as its
mediator. Proceedings of the National Academy of Sciences USA. 97(18):10185-10190.
Glasel, JA. (1995). Validity of Nucleic Acid Purities Monitored by A260/A280
Absorbance Ratios. Biotechniques 18-1:62-63.
Gordillo M, Vega H, Trainer AH, Hou F, Sakai N, Luque R, Kayserili H, Basaran S,
Skovby F, Hennekam RC, Uzielli ML, Schnur RE, Manouvrier S, Chang S, Blair E,
Hurst JA, Forzano F, Meins M, Simola KO, Raas-Rothschild A, Schultz RA, McDaniel
LD, Ozono K, Inui K, Zou H, Jabs EW. (2008). The molecular mechanism underlying
Roberts syndrome involves loss of ESCO2 acetyltransferase activity. Human Molecular
Genetics. 17(14):2172-2180.
Hoppman-Chaney N, Jang JS, Jen J, Babovic-Vuksanovic D, Hodge JC., (2011).
In-frame multi-exon deletion of SMC1A in a severely affected female with Cornelia de
Lange Syndrome. American Journal of Medical Genetics. Part A 158A:193-198.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
51
Horsfield JA, Print CG, Mönnich M. (2012). Diverse developmental disorders from
the one ring: distinct molecular pathways underlie the cohesinopathies. Frontiers in
Genetics. 3:171-186.
Hou F, Zou H. (2005). Two human orthologues of Eco1/Ctf7 acetyltransferases are
both required for proper sister-chromatid cohesion. Molecular Biology of the Cell.
16(8):3908-3918.
Jahnke P, Xu W, Wülling M, Albrecht M, Gabriel H, Gillessen-Kaesbach G, Kaiser
FJ. (2008). The Cohesin loading factor NIPBL recruits histone deacetylases to mediate
local chromatin modifications. Nucleic Acids Research. 36(20):6450-6458.
Johns DA, Bhonsale DL, Shivashanker VY, Johns M. (2012). Aesthetic and
functional management of a patient with Cornelia de Lange syndrome. Contemporary
Clinical Dentistry. 3(Suppl 1):S86-S91.
Kalendar R, Lee D, Schulman AH (2011). Java web tools for PCR, in silico PCR,
and oligonucleotide assembly and analysis. Genomics, 98(2): 137-144.
Kline AD, Krantz ID, Sommer A, Kliewer M, Jackson LG, FitzPatrick DR, Levin AV,
Selicorni A. (2007). Cornelia de Lange syndrome: clinical review, diagnostic and
scoring systems, and anticipatory guidance. American Journal of medical genetics
143A(12):1287-1296.
Kluwe L, Mautner V, Heinrich B, Dezube R, Jacoby LB, Friedrich RE, MacCollin M.
(2003). Molecular study of frequency of mosaicism in neurofibromatosis 2 patients with
bilateral vestibular schwannomas. Journal of Medical Genetics. 40(2):109-114.
Kohonen-Corish MR, Al-Aama JY, Auerbach AD, Axton M, Barash CI, Bernstein I,
Béroud C, Burn J, Cunningham F, Cutting GR, den Dunnen JT, Greenblatt MS, Kaput J,
Katz M, Lindblom A, Macrae F, Maglott D, Möslein G, Povey S, Ramesar R, Richards
S, Seminara D, Sobrido MJ, Tavtigian S, Taylor G, Vihinen M, Winship I, Cotton RG;
Human Variome Project Meeting. (2010). How to catch all those mutations--the report
of the third Human Variome Project Meeting, UNESCO Paris, May 2010. Human
Mutation 31(12):1374-1381.
Krantz ID, McCallum J, DeScipio C, Kaur M, Gillis LA, Yaeger D, Jukofsky L,
Wasserman N, Bottani A, Morris CA, Nowaczyk MJ, Toriello H, Bamshad MJ, Carey JC,
Rappaport E, Kawauchi S, Lander AD, Calof AL, Li HH, Devoto M, Jackson LG. (2004).
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
52
Cornelia de Lange syndrome is caused by mutations in NIPBL, the human homolog of
Drosophila melanogaster Nipped-B. Nature Genetics. 36(6):631-635.
Kueng S, Hegemann B, Peters BH, Lipp JJ, Schleiffer A, Mechtler K, Peters JM.
(2006). Wapl controls the dynamic association of cohesin with chromatin. Cell.
127(5):955-967
Kumar D, Blank CE, Griffiths BL. (1985). Cornelia de Lange syndrome in several
members of the same family. Journal of Medical Genetics, 22, 296-300.
Kumar D, Sakabe I, Patel S, Zhang Y, Ahmad I, Gehan EA, Whiteside TL, Kasid U.
(2004). SCC-112, a novel cell cycle-regulated molecule, exhibits reduced expression in
human renal carcinomas. Gene. 328:187-196.
Lalatta F, Russo S, Gentilin B, Spaccini L, Boschetto C, Cavalleri F, Masciadri M,
Gervasini C, Bentivegna A, Castronovo P, Larizza L. (2007). Prenatal/neonatal
pathology in two cases of Cornelia de Lange syndrome harboring novel mutations of
NIPBL. Genetics in Medicine. 9(3):188-194.
Liu J, Krantz ID. (2009). Cornelia de Lange syndrome, cohesin, and beyond.
Clinical Genetics. 76(4):303–314.
Maniatis T, Fritsch EF, and Sambrook J. (1982) Molecular Cloning A Laboratory
Manual, Cold Spring Harbor Laboratory, Cold Springs Harbor, NY.
Mannini L, Liu J, Krantz ID, Musio A. (2010). Spectrum and consequences of
SMC1A mutations: the unexpected involvement of a core component of cohesin in
human disease. Human Mutation. 31(1):5-10.
Millat G, Chanavat V, Julia S, Crehalet H, Bouvagnet P, Rousson R. (2009).
Validation of high-resolution DNA melting analysis for mutation scanning of the LMNA
gene. Clinical Biochemistry. 42(9):892-898
Miller SA, Dykes DD, and Polesky HF. (1998). A simple salting out procedure for
extracting DNA from human nucleated cells. Nucleic Acids Research. 16(3): 1215.
Musio A, Selicorni A, Focarelli ML, Gervasini C, Milani D, Russo S, Vezzoni P,
Larizza L. (2006). X-linked Cornelia de Lange syndrome owing to SMC1L1 mutations.
Nature Genetics. 8(5):528-530.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
53
Miyake N, Visser R, Kinoshita A, Yoshiura K, Niikawa N, Kondoh T, Matsumoto N,
Harada N, Okamoto N, Sonoda T, Naritomi K, Kaname T, Chinen Y, Tonoki H,
Kurosawa K. (2005). Four novel NIPBL mutations in Japanese patients with Cornelia
de Lange syndrome. American Journal of Medical Genetics. 135(1):103-105.
Nishiyama T, Ladurner R, Schmitz J, Kreidl E, Schleiffer A, Bhaskara V, Bando M,
Shirahige K, Hyman AA, Mechtler K, Peters JM. (2010). Sororin mediates sister
chromatid cohesion by antagonizing Wapl. Cell. 143(5):737-749.
Oliveira J, Dias C, Redeker E, Costa E, Silva J, Reis Lima M, den Dunnen JT,
Santos R. (2010). Development of NIPBL locus-specific database using LOVD: from
novel mutations to further genotype-phenotype correlations in Cornelia de Lange
Syndrome. Human Mutation. 31(11):1216-1222.
Oostra RJ, Baljet B, Hennekam RC. Brachmann-de Lange syndrome "avant la
lettre". (1994). American Journal of Medical Genetics. 1994 Sep 1;52(3):267-268.
Pagnamenta AT, Lise S, Harrison V, Stewart H, Jayawant S, Quaghebeur G, Deng
AT, Murphy VE, Sadighi Akha E, Rimmer A, Mathieson I, Knight SJ, Kini U, Taylor JC,
Keays DA. (2012). Exome sequencing can detect pathogenic mosaic mutations
present at low allele frequencies. Journal of Human Genetics. 57(1):70-72
Parisi S, McKay MJ, Molnar M, Thompson MA, van der Spek PJ, van Drunen-
Schoenmaker E, Kanaar R, Lehmann E, Hoeijmakers JH, Kohli J. (1999). Molecular
and Cellular Biology. 19(5):3515-3528.
Pauline C. and Henikoff S, (2003) SIFT: predicting amino acid changes that affect
protein function. Nucleic Acid research. 31(13): 3812–3814.
Pezzi N, Prieto I, Kremer L, Pérez Jurado LA, Valero C, Del Mazo J, Martínez-A C,
Barbero JL. (2000). STAG3, a novel gene encoding a protein involved in meiotic
chromosome pairing and location of STAG3-related genes flanking the Williams-
Beuren syndrome deletion. Journal of the Federation of American Society for
Experimental Biology. 14(3):581-592.
Pertea M, Lin X, Salzberg SL. GeneSplicer: a new computational method for splice
site prediction. Nucleic Acid Research. 29(5):1185-1190.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
54
Reese MG, Eeckman FH, Kulp D, Haussler D. (1997) Improved splice site
detection in Genie. 4(3):311-323.
Rankin S, Ayad NG, Kirschner MW. (2005). Sororin, a substrate of the anaphase-
promoting complex, is required for sister chromatid cohesion in vertebrates. Molecular
Cell. 18(2):185-200.
Revenkova E, Eijpe M, Heyting C, Gross B, Jessberger R. (2001). Novel meiosis-
specific isoform of mammalian SMC1. Molecular Cell Biology. 21(20):6984-6998.
Revenkova E, Eijpe M, Heyting C, Hodges CA, Hunt PA, Liebe B, Scherthan H,
Jessberger R. (2004). Cohesin SMC1 beta is required for meiotic chromosome
dynamics, sister chromatid cohesion and DNA recombination. Nature Cell Biology.
6(6):555-562.
Revenkova E, Focarelli ML, Susani L, Paulis M, Bassi MT, Mannini L, Frattini A,
Delia D, Krantz I, Vezzoni P, Jessberger R, Musio A. (2009). Cornelia de Lange
syndrome mutations in SMC1A or SMC3 affect binding to DNA. Human Molecular
Genetics. 18(3):418-427.
Russo S, Masciadri M, Gervasini C, Azzollini J, Cereda A, Zampino G, Haas O,
Scarano G, Di Rocco M, Finelli P, Tenconi R, Selicorni A, Larizza L. (2012). Intragenic
and large NIPBL rearrangements revealed by MLPA in Cornelia de Lange patients.
European Journal of Human Genetics. 20(7):734-741.
Sadano H, Sugimoto H, Sakai F, Nomura N, Osumi T. (2000) NXP-1, a human
protein related to Rad21/Scc1/Mcd1, is a component of the nuclear matrix. Biochemical
and Biophysical Research Communications. 267(1):418-422.
Santos S, Marques V, Pires M, Silveira L, Oliveira H, Lança V, Brito D, Madeira H,
Esteves JF, Freitas A, Carreira IM, Gaspar IM, Monteiro C, Fernandes AR. (2012) High
resolution melting: improvements in the genetic diagnosis of hypertrophic
cardiomyopathy in a Portuguese cohort. BMC Medical Genetics. 13:17.
Selicorni A, Russo S, Gervasini C, Castronovo P, Milani D, Cavalleri F, Bentivegna
A, Masciadri M, Domi A, Divizia MT, Sforzini C, Tarantino E, Memo L, Scarano G,
Larizza L. (2008). Clinical score of 62 Italian patients with Cornelia de Lange syndrome
and correlations with the presence and type of NIPBL mutation. Clinical Genetics.
72(2):98-108.
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
55
Sumara I, Vorlaufer E, Gieffers C, Peters BH, Peters JM. (2000). Characterization
of vertebrate cohesin complexes and their regulation in prophase. 151(4):749-762.
Tonkin ET, Wang TJ, Lisgo S, Bamshad MJ, Strachan T. (2004). NIPBL, encoding
a homolog of fungal Scc2-type sister chromatid cohesion proteins and fly Nipped-B, is
mutated in Cornelia de Lange syndrome, Nature Genetics. 36(6):636-641.
Vega H, Waisfisz Q, Gordillo M, Sakai N, Yanagihara I, Yamada M, van Gosliga D,
Kayserili H, Xu C, Ozono K, Jabs EW, Inui K, Joenje H. (2005). Roberts syndrome is
caused by mutations in ESCO2, a human homolog of yeast ECO1 that is essential for
the establishment of sister chromatid cohesion. 37(5):468-470.
Van den Wyngaert I, de Vries W, Kremer A, Neefs J, Verhasselt P, Luyten WH,
Kass SU. (2000). Cloning and characterization of human histone deacetylase 8. FEBS
Letters. 478(1-2):77-83.
Watrin E, Peters JM. (2006). Cohesin and DNA damage repair. Experimental Cell
Research. 312(14):2687-2693.
Watrin E, Schleiffer A, Tanaka K, Eisenhaber F, Nasmyth K, Peters JM. (2006).
Human Scc4 is required for cohesin binding to chromatin, sister-chromatid cohesion,
and mitotic progression. Current Biology. 16(9):863-874.
Yan J, Saifi GM, Wierzba TH, Withers M, Bien-Willner GA, Limon J, Stankiewicz P,
Lupski JR, Wierzba J. (2006). Mutational and genotype-phenotype correlation analyses
in 28 Polish patients with Cornelia de Lange syndrome. American Journal of Human
Genetics. 140(14):1531-1541.
Ye J, Coulouris G, Zaretskaya I, Cutcutache I, Rozen S, and Madden TL (2012).
Primer-BLAST: A tool to design target-specific primers for polymerase chain reaction.
Bioinformatics. 13:134.
Yeo G, Burge CB. (2004). Maximum entropy modeling of short sequence motifs
with applications to RNA splicing signals. Journal of Computational Biology. 11(2-
3):377-94.
Zhang B, Chang J, Fu M, Huang J, Kashyap R, Salavaggione E, Jain S, Kulkarni S,
Deardorff MA, Uzielli ML, Dorsett D, Beebe DC, Jay PY, Heuckeroth RO, Krantz I,

FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
56
Milbrandt J. (2009). Dosage effects of cohesin regulatory factor PDS5 on mammalian
development: implications for cohesinopathies. PLoS One. 4(5):e5232.
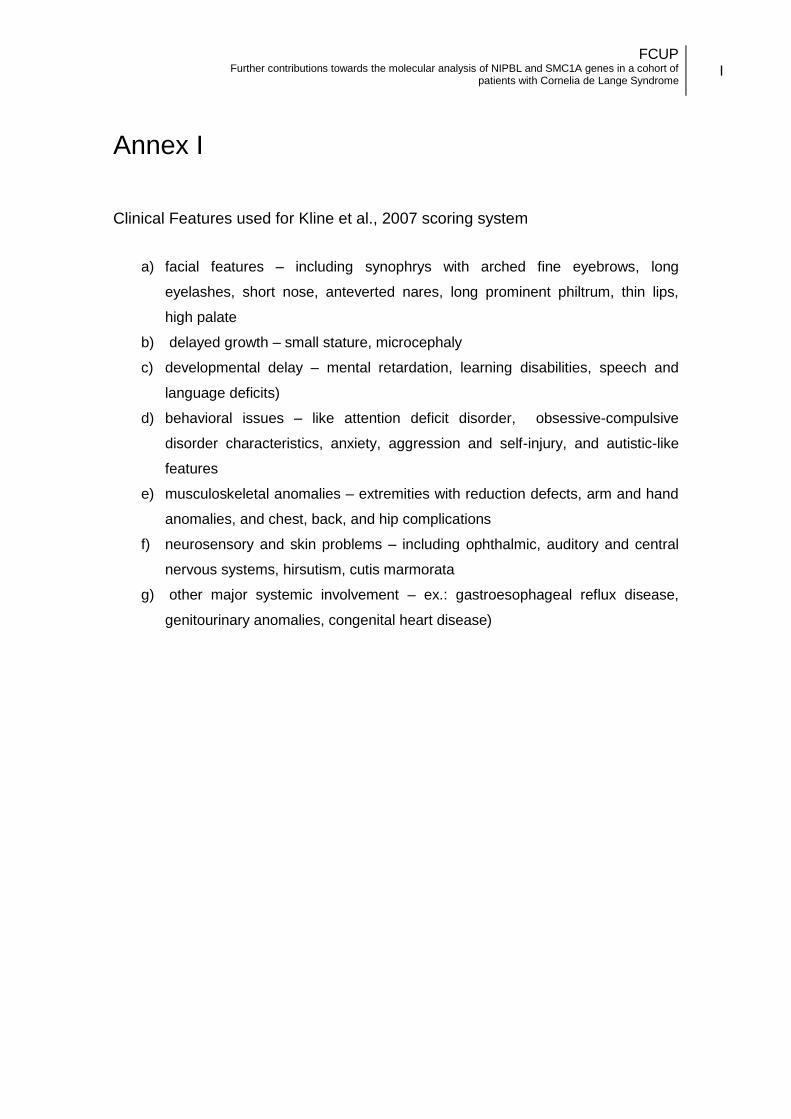
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
I
Annex I Clinical Features used for Kline et al., 2007 scoring system
a) facial features – including synophrys with arched fine eyebrows, long
eyelashes, short nose, anteverted nares, long prominent philtrum, thin lips,
high palate
b) delayed growth – small stature, microcephaly
c) developmental delay – mental retardation, learning disabilities, speech and
language deficits)
d) behavioral issues – like attention deficit disorder, obsessive-compulsive
disorder characteristics, anxiety, aggression and self-injury, and autistic-like
features
e) musculoskeletal anomalies – extremities with reduction defects, arm and hand
anomalies, and chest, back, and hip complications
f) neurosensory and skin problems – including ophthalmic, auditory and central
nervous systems, hirsutism, cutis marmorata
g) other major systemic involvement – ex.: gastroesophageal reflux disease,
genitourinary anomalies, congenital heart disease)
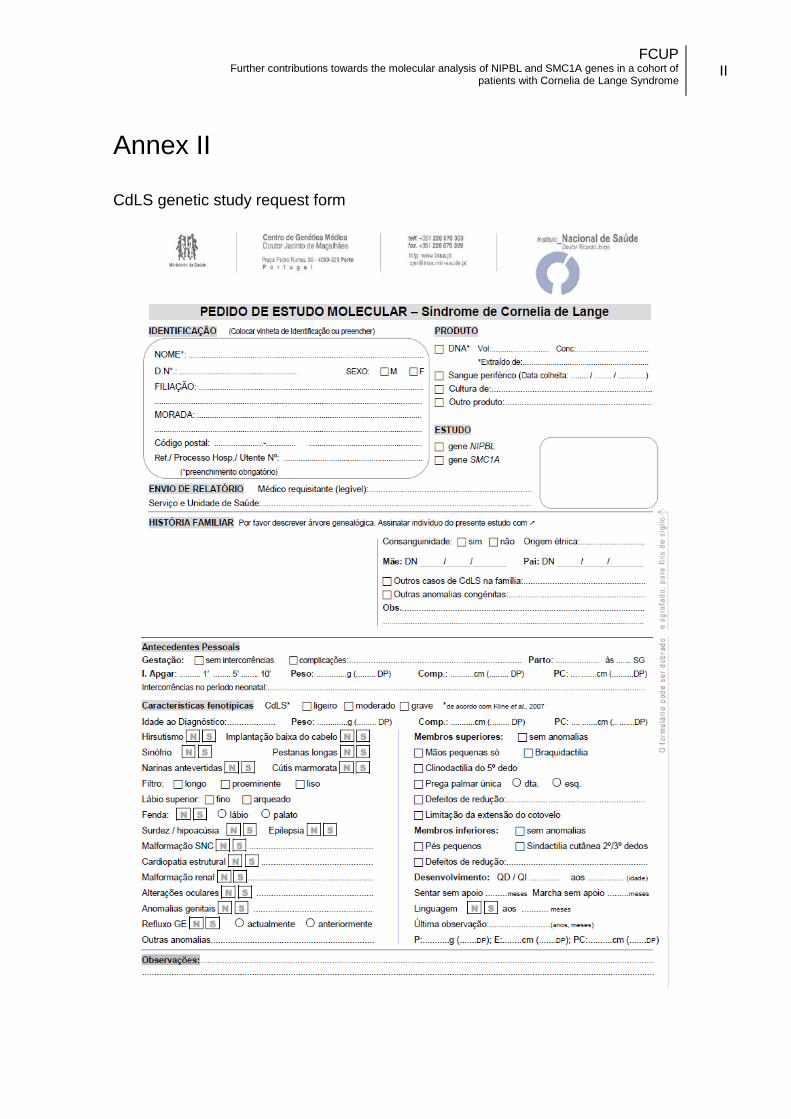
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
II
Annex II CdLS genetic study request form
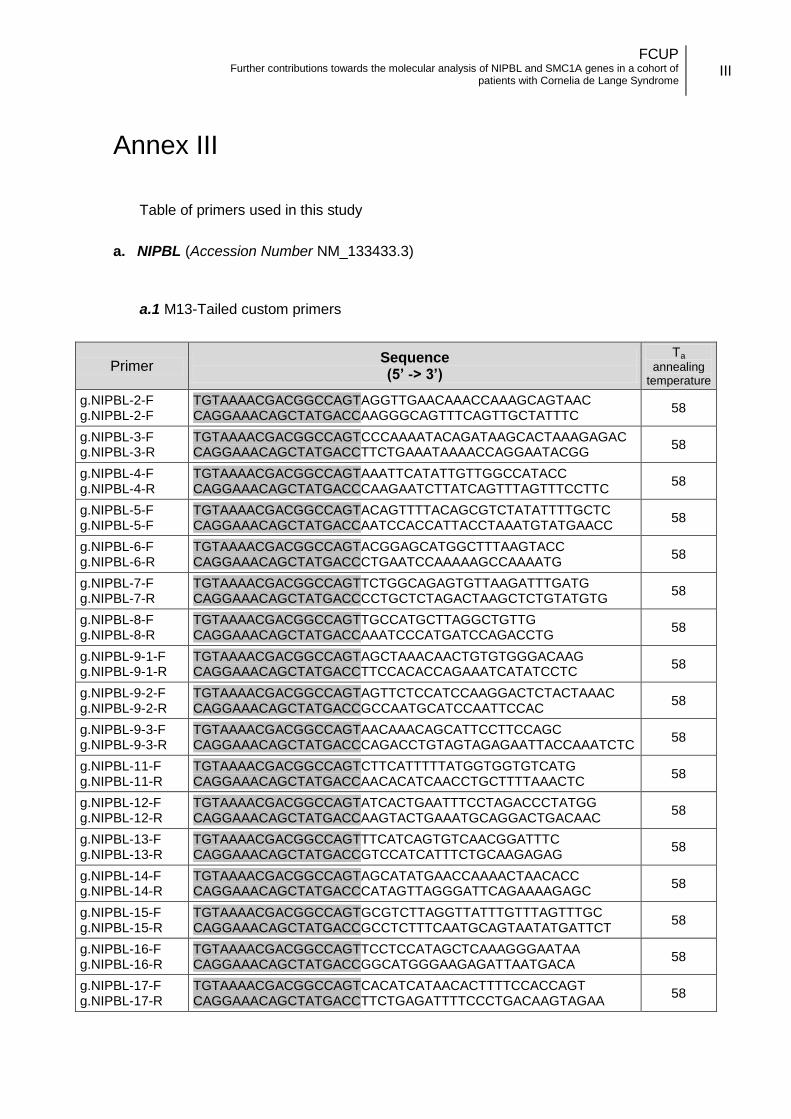
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
III
Annex III
Table of primers used in this study
a. NIPBL (Accession Number NM_133433.3)
a.1 M13-Tailed custom primers
Primer Sequence (5’ -> 3’)
Ta
annealing temperature
g.NIPBL-2-F g.NIPBL-2-F
TGTAAAACGACGGCCAGTAGGTTGAACAAACCAAAGCAGTAAC CAGGAAACAGCTATGACCAAGGGCAGTTTCAGTTGCTATTTC
58
g.NIPBL-3-F g.NIPBL-3-R
TGTAAAACGACGGCCAGTCCCAAAATACAGATAAGCACTAAAGAGAC CAGGAAACAGCTATGACCTTCTGAAATAAAACCAGGAATACGG
58
g.NIPBL-4-F g.NIPBL-4-R
TGTAAAACGACGGCCAGTAAATTCATATTGTTGGCCATACC CAGGAAACAGCTATGACCCAAGAATCTTATCAGTTTAGTTTCCTTC
58
g.NIPBL-5-F g.NIPBL-5-F
TGTAAAACGACGGCCAGTACAGTTTTACAGCGTCTATATTTTGCTC CAGGAAACAGCTATGACCAATCCACCATTACCTAAATGTATGAACC
58
g.NIPBL-6-F g.NIPBL-6-R
TGTAAAACGACGGCCAGTACGGAGCATGGCTTTAAGTACC CAGGAAACAGCTATGACCCTGAATCCAAAAAGCCAAAATG
58
g.NIPBL-7-F g.NIPBL-7-R
TGTAAAACGACGGCCAGTTCTGGCAGAGTGTTAAGATTTGATG CAGGAAACAGCTATGACCCCTGCTCTAGACTAAGCTCTGTATGTG
58
g.NIPBL-8-F g.NIPBL-8-R
TGTAAAACGACGGCCAGTTGCCATGCTTAGGCTGTTG CAGGAAACAGCTATGACCAAATCCCATGATCCAGACCTG
58
g.NIPBL-9-1-F g.NIPBL-9-1-R
TGTAAAACGACGGCCAGTAGCTAAACAACTGTGTGGGACAAG CAGGAAACAGCTATGACCTTCCACACCAGAAATCATATCCTC
58
g.NIPBL-9-2-F g.NIPBL-9-2-R
TGTAAAACGACGGCCAGTAGTTCTCCATCCAAGGACTCTACTAAAC CAGGAAACAGCTATGACCGCCAATGCATCCAATTCCAC
58
g.NIPBL-9-3-F g.NIPBL-9-3-R
TGTAAAACGACGGCCAGTAACAAACAGCATTCCTTCCAGC CAGGAAACAGCTATGACCCAGACCTGTAGTAGAGAATTACCAAATCTC
58
g.NIPBL-11-F g.NIPBL-11-R
TGTAAAACGACGGCCAGTCTTCATTTTTATGGTGGTGTCATG CAGGAAACAGCTATGACCAACACATCAACCTGCTTTTAAACTC
58
g.NIPBL-12-F g.NIPBL-12-R
TGTAAAACGACGGCCAGTATCACTGAATTTCCTAGACCCTATGG CAGGAAACAGCTATGACCAAGTACTGAAATGCAGGACTGACAAC
58
g.NIPBL-13-F g.NIPBL-13-R
TGTAAAACGACGGCCAGTTTCATCAGTGTCAACGGATTTC CAGGAAACAGCTATGACCGTCCATCATTTCTGCAAGAGAG
58
g.NIPBL-14-F g.NIPBL-14-R
TGTAAAACGACGGCCAGTAGCATATGAACCAAAACTAACACC CAGGAAACAGCTATGACCCATAGTTAGGGATTCAGAAAAGAGC
58
g.NIPBL-15-F g.NIPBL-15-R
TGTAAAACGACGGCCAGTGCGTCTTAGGTTATTTGTTTAGTTTGC CAGGAAACAGCTATGACCGCCTCTTTCAATGCAGTAATATGATTCT
58
g.NIPBL-16-F g.NIPBL-16-R
TGTAAAACGACGGCCAGTTCCTCCATAGCTCAAAGGGAATAA CAGGAAACAGCTATGACCGGCATGGGAAGAGATTAATGACA
58
g.NIPBL-17-F g.NIPBL-17-R
TGTAAAACGACGGCCAGTCACATCATAACACTTTTCCACCAGT CAGGAAACAGCTATGACCTTCTGAGATTTTCCCTGACAAGTAGAA
58
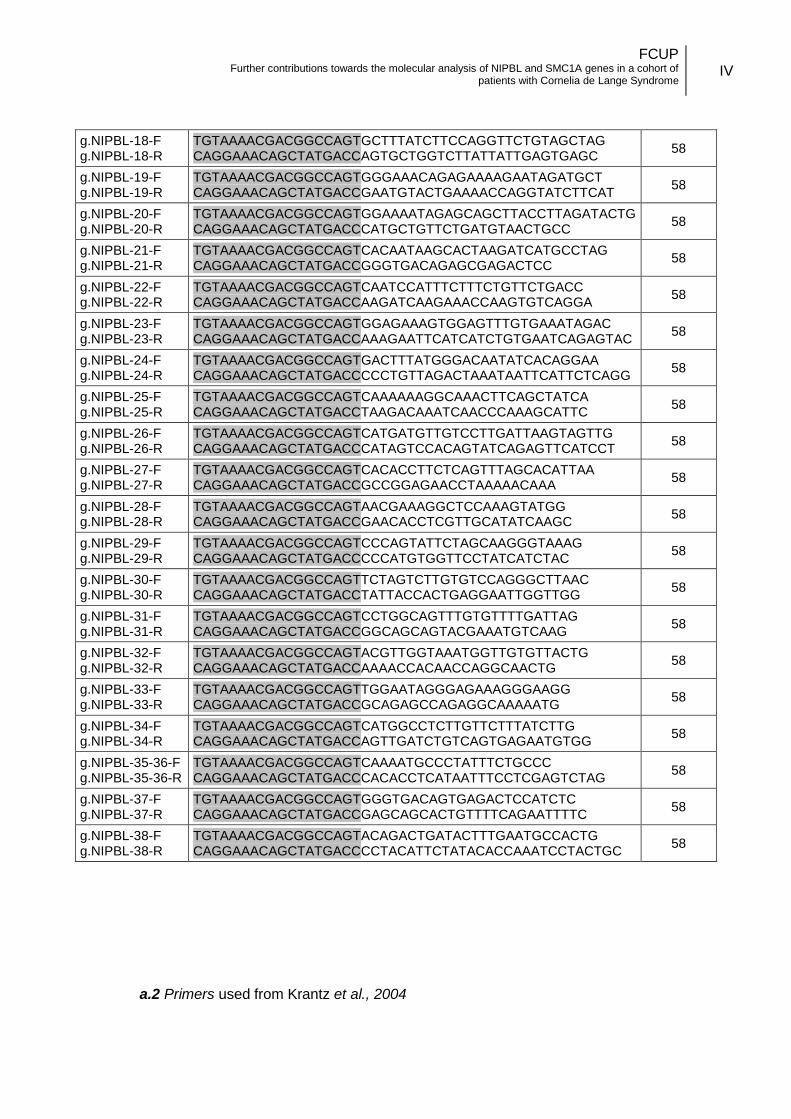
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
IV
g.NIPBL-18-F g.NIPBL-18-R
TGTAAAACGACGGCCAGTGCTTTATCTTCCAGGTTCTGTAGCTAG CAGGAAACAGCTATGACCAGTGCTGGTCTTATTATTGAGTGAGC
58
g.NIPBL-19-F g.NIPBL-19-R
TGTAAAACGACGGCCAGTGGGAAACAGAGAAAAGAATAGATGCT CAGGAAACAGCTATGACCGAATGTACTGAAAACCAGGTATCTTCAT
58
g.NIPBL-20-F g.NIPBL-20-R
TGTAAAACGACGGCCAGTGGAAAATAGAGCAGCTTACCTTAGATACTG CAGGAAACAGCTATGACCCATGCTGTTCTGATGTAACTGCC
58
g.NIPBL-21-F g.NIPBL-21-R
TGTAAAACGACGGCCAGTCACAATAAGCACTAAGATCATGCCTAG CAGGAAACAGCTATGACCGGGTGACAGAGCGAGACTCC
58
g.NIPBL-22-F g.NIPBL-22-R
TGTAAAACGACGGCCAGTCAATCCATTTCTTTCTGTTCTGACC CAGGAAACAGCTATGACCAAGATCAAGAAACCAAGTGTCAGGA
58
g.NIPBL-23-F g.NIPBL-23-R
TGTAAAACGACGGCCAGTGGAGAAAGTGGAGTTTGTGAAATAGAC CAGGAAACAGCTATGACCAAAGAATTCATCATCTGTGAATCAGAGTAC
58
g.NIPBL-24-F g.NIPBL-24-R
TGTAAAACGACGGCCAGTGACTTTATGGGACAATATCACAGGAA CAGGAAACAGCTATGACCCCCTGTTAGACTAAATAATTCATTCTCAGG
58
g.NIPBL-25-F g.NIPBL-25-R
TGTAAAACGACGGCCAGTCAAAAAAGGCAAACTTCAGCTATCA CAGGAAACAGCTATGACCTAAGACAAATCAACCCAAAGCATTC
58
g.NIPBL-26-F g.NIPBL-26-R
TGTAAAACGACGGCCAGTCATGATGTTGTCCTTGATTAAGTAGTTG CAGGAAACAGCTATGACCCATAGTCCACAGTATCAGAGTTCATCCT
58
g.NIPBL-27-F g.NIPBL-27-R
TGTAAAACGACGGCCAGTCACACCTTCTCAGTTTAGCACATTAA CAGGAAACAGCTATGACCGCCGGAGAACCTAAAAACAAA
58
g.NIPBL-28-F g.NIPBL-28-R
TGTAAAACGACGGCCAGTAACGAAAGGCTCCAAAGTATGG CAGGAAACAGCTATGACCGAACACCTCGTTGCATATCAAGC
58
g.NIPBL-29-F g.NIPBL-29-R
TGTAAAACGACGGCCAGTCCCAGTATTCTAGCAAGGGTAAAG CAGGAAACAGCTATGACCCCCATGTGGTTCCTATCATCTAC
58
g.NIPBL-30-F g.NIPBL-30-R
TGTAAAACGACGGCCAGTTCTAGTCTTGTGTCCAGGGCTTAAC CAGGAAACAGCTATGACCTATTACCACTGAGGAATTGGTTGG
58
g.NIPBL-31-F g.NIPBL-31-R
TGTAAAACGACGGCCAGTCCTGGCAGTTTGTGTTTTGATTAG CAGGAAACAGCTATGACCGGCAGCAGTACGAAATGTCAAG
58
g.NIPBL-32-F g.NIPBL-32-R
TGTAAAACGACGGCCAGTACGTTGGTAAATGGTTGTGTTACTG CAGGAAACAGCTATGACCAAAACCACAACCAGGCAACTG
58
g.NIPBL-33-F g.NIPBL-33-R
TGTAAAACGACGGCCAGTTGGAATAGGGAGAAAGGGAAGG CAGGAAACAGCTATGACCGCAGAGCCAGAGGCAAAAATG
58
g.NIPBL-34-F g.NIPBL-34-R
TGTAAAACGACGGCCAGTCATGGCCTCTTGTTCTTTATCTTG CAGGAAACAGCTATGACCAGTTGATCTGTCAGTGAGAATGTGG
58
g.NIPBL-35-36-F g.NIPBL-35-36-R
TGTAAAACGACGGCCAGTCAAAATGCCCTATTTCTGCCC CAGGAAACAGCTATGACCCACACCTCATAATTTCCTCGAGTCTAG
58
g.NIPBL-37-F g.NIPBL-37-R
TGTAAAACGACGGCCAGTGGGTGACAGTGAGACTCCATCTC CAGGAAACAGCTATGACCGAGCAGCACTGTTTTCAGAATTTTC
58
g.NIPBL-38-F g.NIPBL-38-R
TGTAAAACGACGGCCAGTACAGACTGATACTTTGAATGCCACTG CAGGAAACAGCTATGACCCCTACATTCTATACACCAAATCCTACTGC
58
a.2 Primers used from Krantz et al., 2004
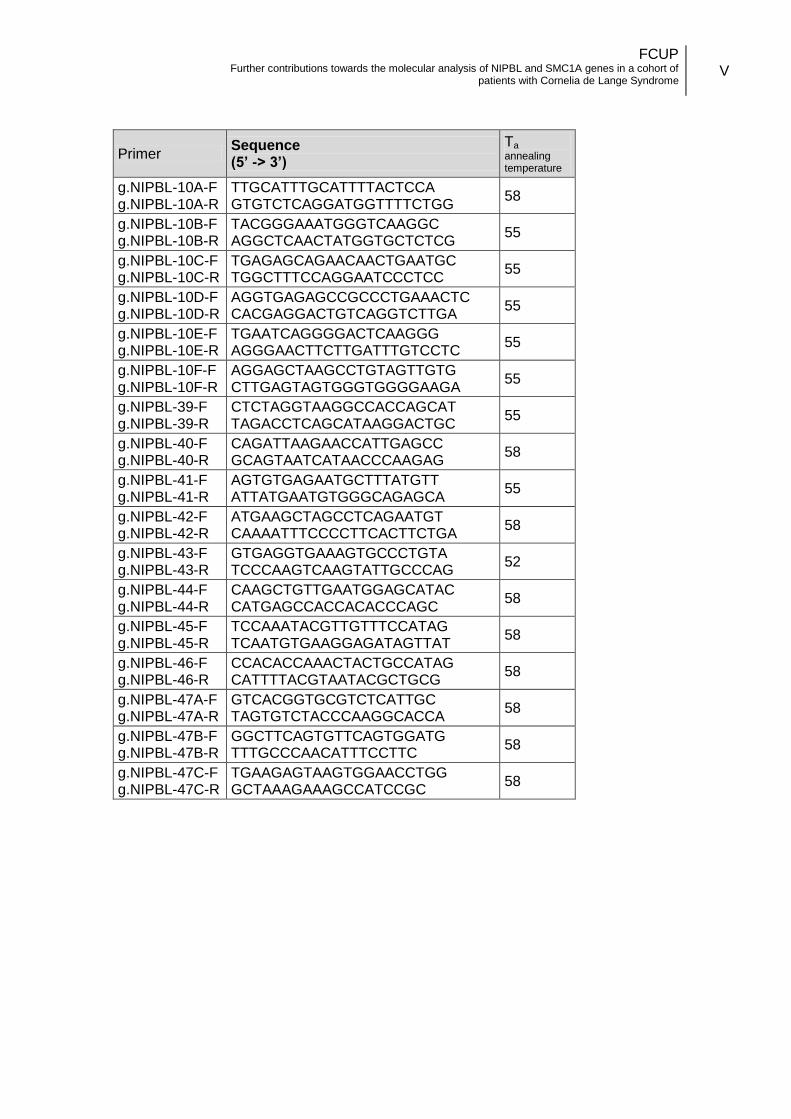
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
V
Primer Sequence (5’ -> 3’)
Ta
annealing temperature
g.NIPBL-10A-F g.NIPBL-10A-R
TTGCATTTGCATTTTACTCCA GTGTCTCAGGATGGTTTTCTGG
58
g.NIPBL-10B-F g.NIPBL-10B-R
TACGGGAAATGGGTCAAGGC AGGCTCAACTATGGTGCTCTCG
55
g.NIPBL-10C-F g.NIPBL-10C-R
TGAGAGCAGAACAACTGAATGC TGGCTTTCCAGGAATCCCTCC
55
g.NIPBL-10D-F g.NIPBL-10D-R
AGGTGAGAGCCGCCCTGAAACTC CACGAGGACTGTCAGGTCTTGA
55
g.NIPBL-10E-F g.NIPBL-10E-R
TGAATCAGGGGACTCAAGGG AGGGAACTTCTTGATTTGTCCTC
55
g.NIPBL-10F-F g.NIPBL-10F-R
AGGAGCTAAGCCTGTAGTTGTG CTTGAGTAGTGGGTGGGGAAGA
55
g.NIPBL-39-F g.NIPBL-39-R
CTCTAGGTAAGGCCACCAGCAT TAGACCTCAGCATAAGGACTGC
55
g.NIPBL-40-F g.NIPBL-40-R
CAGATTAAGAACCATTGAGCC GCAGTAATCATAACCCAAGAG
58
g.NIPBL-41-F g.NIPBL-41-R
AGTGTGAGAATGCTTTATGTT ATTATGAATGTGGGCAGAGCA
55
g.NIPBL-42-F g.NIPBL-42-R
ATGAAGCTAGCCTCAGAATGT CAAAATTTCCCCTTCACTTCTGA
58
g.NIPBL-43-F g.NIPBL-43-R
GTGAGGTGAAAGTGCCCTGTA TCCCAAGTCAAGTATTGCCCAG
52
g.NIPBL-44-F g.NIPBL-44-R
CAAGCTGTTGAATGGAGCATAC CATGAGCCACCACACCCAGC
58
g.NIPBL-45-F g.NIPBL-45-R
TCCAAATACGTTGTTTCCATAG TCAATGTGAAGGAGATAGTTAT
58
g.NIPBL-46-F g.NIPBL-46-R
CCACACCAAACTACTGCCATAG CATTTTACGTAATACGCTGCG
58
g.NIPBL-47A-F g.NIPBL-47A-R
GTCACGGTGCGTCTCATTGC TAGTGTCTACCCAAGGCACCA
58
g.NIPBL-47B-F g.NIPBL-47B-R
GGCTTCAGTGTTCAGTGGATG TTTGCCCAACATTTCCTTC
58
g.NIPBL-47C-F g.NIPBL-47C-R
TGAAGAGTAAGTGGAACCTGG GCTAAAGAAAGCCATCCGC
58
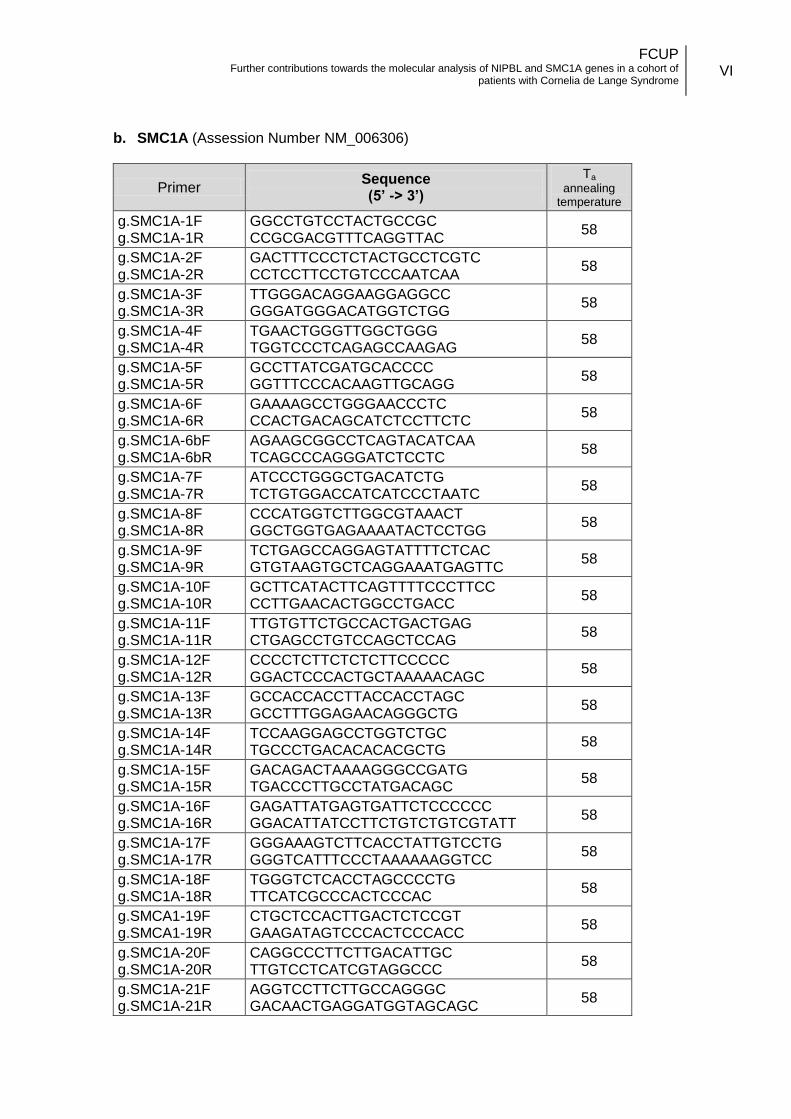
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
VI
b. SMC1A (Assession Number NM_006306)
Primer Sequence (5’ -> 3’)
Ta
annealing temperature
g.SMC1A-1F g.SMC1A-1R
GGCCTGTCCTACTGCCGC CCGCGACGTTTCAGGTTAC
58
g.SMC1A-2F g.SMC1A-2R
GACTTTCCCTCTACTGCCTCGTC
CCTCCTTCCTGTCCCAATCAA 58
g.SMC1A-3F g.SMC1A-3R
TTGGGACAGGAAGGAGGCC GGGATGGGACATGGTCTGG
58
g.SMC1A-4F g.SMC1A-4R
TGAACTGGGTTGGCTGGG TGGTCCCTCAGAGCCAAGAG
58
g.SMC1A-5F g.SMC1A-5R
GCCTTATCGATGCACCCC GGTTTCCCACAAGTTGCAGG
58
g.SMC1A-6F g.SMC1A-6R
GAAAAGCCTGGGAACCCTC CCACTGACAGCATCTCCTTCTC
58
g.SMC1A-6bF g.SMC1A-6bR
AGAAGCGGCCTCAGTACATCAA TCAGCCCAGGGATCTCCTC
58
g.SMC1A-7F g.SMC1A-7R
ATCCCTGGGCTGACATCTG TCTGTGGACCATCATCCCTAATC
58
g.SMC1A-8F g.SMC1A-8R
CCCATGGTCTTGGCGTAAACT GGCTGGTGAGAAAATACTCCTGG
58
g.SMC1A-9F g.SMC1A-9R
TCTGAGCCAGGAGTATTTTCTCAC GTGTAAGTGCTCAGGAAATGAGTTC
58
g.SMC1A-10F g.SMC1A-10R
GCTTCATACTTCAGTTTTCCCTTCC CCTTGAACACTGGCCTGACC
58
g.SMC1A-11F g.SMC1A-11R
TTGTGTTCTGCCACTGACTGAG CTGAGCCTGTCCAGCTCCAG
58
g.SMC1A-12F g.SMC1A-12R
CCCCTCTTCTCTCTTCCCCC GGACTCCCACTGCTAAAAACAGC
58
g.SMC1A-13F g.SMC1A-13R
GCCACCACCTTACCACCTAGC GCCTTTGGAGAACAGGGCTG
58
g.SMC1A-14F g.SMC1A-14R
TCCAAGGAGCCTGGTCTGC TGCCCTGACACACACGCTG
58
g.SMC1A-15F g.SMC1A-15R
GACAGACTAAAAGGGCCGATG TGACCCTTGCCTATGACAGC
58
g.SMC1A-16F g.SMC1A-16R
GAGATTATGAGTGATTCTCCCCCC GGACATTATCCTTCTGTCTGTCGTATT
58
g.SMC1A-17F g.SMC1A-17R
GGGAAAGTCTTCACCTATTGTCCTG GGGTCATTTCCCTAAAAAAGGTCC
58
g.SMC1A-18F g.SMC1A-18R
TGGGTCTCACCTAGCCCCTG TTCATCGCCCACTCCCAC
58
g.SMCA1-19F g.SMCA1-19R
CTGCTCCACTTGACTCTCCGT GAAGATAGTCCCACTCCCACC
58
g.SMC1A-20F g.SMC1A-20R
CAGGCCCTTCTTGACATTGC TTGTCCTCATCGTAGGCCC
58
g.SMC1A-21F g.SMC1A-21R
AGGTCCTTCTTGCCAGGGC GACAACTGAGGATGGTAGCAGC
58
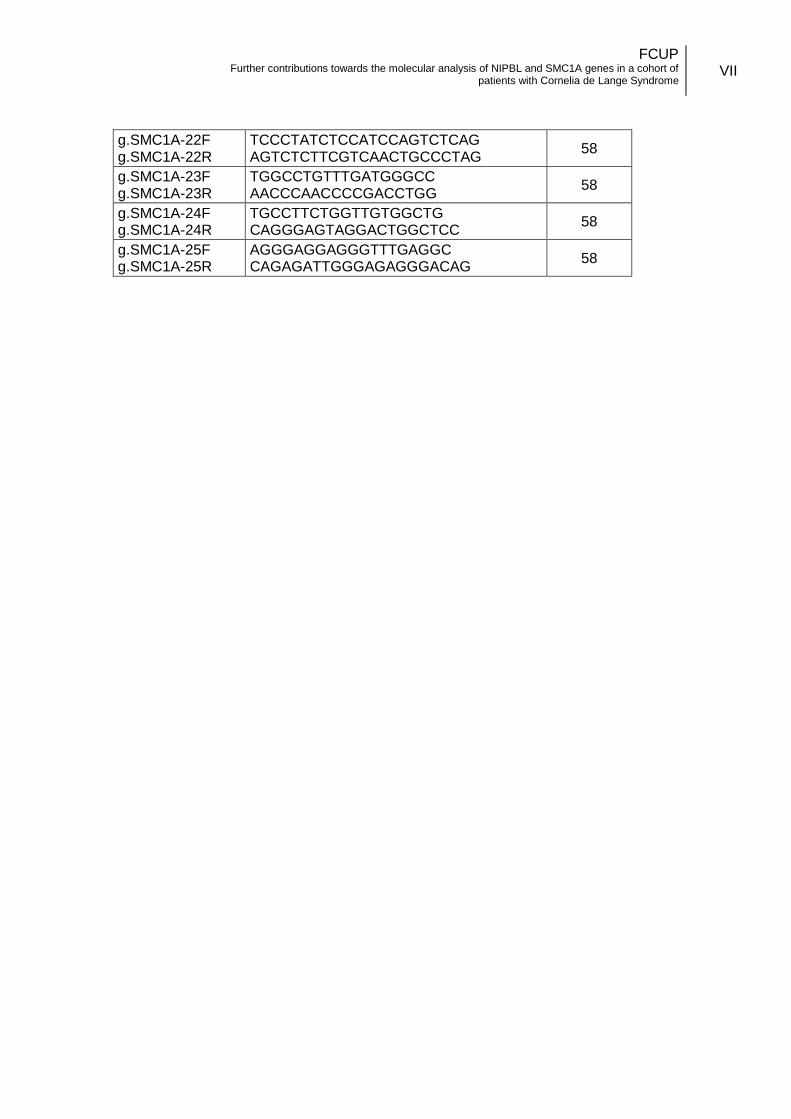
FCUP Further contributions towards the molecular analysis of NIPBL and SMC1A genes in a cohort of
patients with Cornelia de Lange Syndrome
VII
g.SMC1A-22F g.SMC1A-22R
TCCCTATCTCCATCCAGTCTCAG AGTCTCTTCGTCAACTGCCCTAG
58
g.SMC1A-23F g.SMC1A-23R
TGGCCTGTTTGATGGGCC AACCCAACCCCGACCTGG
58
g.SMC1A-24F g.SMC1A-24R
TGCCTTCTGGTTGTGGCTG CAGGGAGTAGGACTGGCTCC
58
g.SMC1A-25F g.SMC1A-25R
AGGGAGGAGGGTTTGAGGC CAGAGATTGGGAGAGGGACAG
58
Recommended

















