
ICU における PPI・H2B の副作用
2015年10月20日(火)東京慈恵会医科大学付属病院
薬剤部鮎川 英明
1

目次• PPI vs. H2B
• 院内肺炎
• Clostridium difficile感染症
• 経腸栄養とH2B
• 低Mg血症
• まとめ
ü ストレス潰瘍予防の適応(参考) ü クロピドグレルとオメプラゾール(参考)
2

PPI vs. H2B
ICU患者におけるメタ解析と副作用
3

ICU患者において上部消化管出血予防としてのPPIとH2Bを比較したメタアナリシスMethods:MEDLINE、EMBASEなどで検索した1200以上
の文献から14のRCTを選択Pa=ents:成人のICU入室患者1720例Outcome: ・PrimaryoutcomeClinicallyimportantuppergastrointes=nalbleedingOvertuppergastrointes=nalbleeding・Secondaryoutcome 院内肺炎、CD感染、ICU死亡率、ICU滞在期間
2014.7.22勉強会 「H2B vs. PPI」参照
ProtonPumpInhibitorsVersusHistamine2ReceptorAntagonistsforStressUlcerProphylaxisinCriDcallyIllPaDents:ASystemaDcReviewandMeta-Analysis. CritCareMed2013;41:693–705
4

• Clinicallyimportantuppergastrointes=nalbleeding →PPIがbeSer(RR:0.36(95%CI:0.19–0.68),p=0.002,I2=0%)• Overtuppergastrointes=nalbleeding →PPIがbeSer(RR:0.35(95%CI0.21–0.59),p<0.0001,I2=15%)
2014.7.22勉強会 「H2B vs. PPI」参照
Alhazzani et al
700 www.ccmjournal.org
Sensitivity AnalysisSensitivity analysis was conducted examining the effect of using risk difference as an estimate of effect for clinically im-portant bleeding (risk difference −0.03; 95% CI −0.05 to 0.00, p = 0.06, I 2 = 52%) and overt bleeding (risk difference −0.06; 95% CI −0.11 to −0.02, p = 0.009, I 2 = 80%), although signifi-cant heterogeneity was present. The second sensitivity analysis excluded trials pub lished in abstract form (22–25). Clinically important bleed ing (RR 0.42; 95% CI 0.21–0.84; p = 0.01;
I 2 = 0%) and overt bleeding (RR 0.40; 95% CI 0.25–0.67; p = 0.0004; I 2 = 12%) were significantly reduced, consistent with the main analysis.
DISCUSSIONIn this meta-analysis, we found that PPIs were more effective than H2RAs at preventing clinically important bleeding and overt gastrointestinal bleeding. The main reservation about using PPIs
Figure 4. Forrest plot for clinically important gastrointestinal bleeding outcome. Data from 12 trials were included in the analysis using random effects model. The use of proton pump inhibitor (PPI) was associated with a significantly lower risk of clinically important bleeding compared with histamine 2 receptor antagonist (H2RA) (risk ratio [the same as relative risk] [RR] 0.36; 95% confidence interval [CI] 0.19–0.68). M-H = Mantel Haenszel.
TABLE 3. Evidence Profile Using GRADE Approach
Quality Assessment No. of Patients Effect
QualityImpor-tance
No. of Stud-ies Design Risk of Bias Inconsistency Indirectness Imprecision
Proton Pump Inhibitor
Histamine 2 Receptor Antagonist
Relative (95% Confidence Interval) Absolute
Clinically important bleeding
12 Randomized trials
Seriousa No serious inconsistency
No serious indirectness
Serious imprecisionb
12/1019 (1.2%) 38/595 (6.4%) RR 0.36 (0.19–0.68) 46 fewer per 1000 (from 23 fewer to 58 fewer)
Low Critical
Overt upper gastrointestinal bleeding
14 Randomized trials
Seriousa No serious inconsistency
No serious indirectness
No serious imprecision
41/1077 (3.8%) 101/643 (15.7%) RR 0.35 (0.21–0.59) 113 fewer per 1000 (from 72 fewer to 138 fewer)
Moderate Important
Mortality
8 Randomized trials
Serious No serious inconsistency
No serious indirectness
No serious imprecision
127/726 (17.5%) 100/470 (21.2%) RR 1.01 (0.83–1.24) 0 fewer per 1000 (from 42 fewer to 51 more)
Moderate Critical
Nosocomial pneumonia
8
Randomized trials
Seriousa
No serious inconsistency
No serious indirectness
No serious imprecision
66/626 (10.5%) 50/474 (10.5%) RR 1.06 (0.73–1.52) 6 more per 1000 (from 28 fewer to 55 more)
Moderate Critical
This table is generated using the GRADEprofiler software that summarizes the quality of evidence for individual outcomes based on five main domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. For each outcome, the quality of evidence is presented along with the clinical importance of the outcome.aDowngraded for risk of bias mainly due to lack of or incomplete blinding.bDowngraded for low number of events rather than confidence interval. Feature Article
Critical Care Medicine www.ccmjournal.org 701
in the critical care setting rather than H2RAs is the potential to increase the incidence of nosocomial pneumonia (38, 39); how-ever, trials do not suggest such a difference. Mortality and length of ICU stay were not affected. None of the trials reported C. dif-ficile infection, although a systematic review of 12 observational studies evaluating 2,948 patients with C. difficile found an asso-ciation with antisecretory therapy (OR 1.94; 95% CI 1.37–2.75).
The association was present for PPI use (OR 2.05; 95% CI 1.47–2.85) and for H2RA use (OR 1.47; 95% CI 1.06–2.05), with no difference between PPIs and H2RAs (p = 0.17) (40).
There was no heterogeneity of results in this meta-analysis. Subgroup analyses examining dosing and frequency of PPI administration, and specific populations (medical vs. surgical ICU patients, and Asian vs. non-Asian patients) showed no sig-
Figure 5. Forrest plot for overt upper gastrointestinal bleeding outcome. Data from 14 trials were included in the analysis using random effects model. The use of proton pump inhibitor (PPI) was associated with a significantly lower risk of overt bleeding compared with histamine 2 receptor antagonist (H2RA) (risk ratio [the same as relative risk] [RR] 0.35; 95% confidence interval [CI] 0.21–0.59). M-H = Mantel Haenszel.
TABLE 3. Evidence Profile Using GRADE Approach
Quality Assessment No. of Patients Effect
QualityImpor-tance
No. of Stud-ies Design Risk of Bias Inconsistency Indirectness Imprecision
Proton Pump Inhibitor
Histamine 2 Receptor Antagonist
Relative (95% Confidence Interval) Absolute
Clinically important bleeding
12 Randomized trials
Seriousa No serious inconsistency
No serious indirectness
Serious imprecisionb
12/1019 (1.2%) 38/595 (6.4%) RR 0.36 (0.19–0.68) 46 fewer per 1000 (from 23 fewer to 58 fewer)
Low Critical
Overt upper gastrointestinal bleeding
14 Randomized trials
Seriousa No serious inconsistency
No serious indirectness
No serious imprecision
41/1077 (3.8%) 101/643 (15.7%) RR 0.35 (0.21–0.59) 113 fewer per 1000 (from 72 fewer to 138 fewer)
Moderate Important
Mortality
8 Randomized trials
Serious No serious inconsistency
No serious indirectness
No serious imprecision
127/726 (17.5%) 100/470 (21.2%) RR 1.01 (0.83–1.24) 0 fewer per 1000 (from 42 fewer to 51 more)
Moderate Critical
Nosocomial pneumonia
8
Randomized trials
Seriousa
No serious inconsistency
No serious indirectness
No serious imprecision
66/626 (10.5%) 50/474 (10.5%) RR 1.06 (0.73–1.52) 6 more per 1000 (from 28 fewer to 55 more)
Moderate Critical
This table is generated using the GRADEprofiler software that summarizes the quality of evidence for individual outcomes based on five main domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. For each outcome, the quality of evidence is presented along with the clinical importance of the outcome.aDowngraded for risk of bias mainly due to lack of or incomplete blinding.bDowngraded for low number of events rather than confidence interval.
5

• CD感染について検討した研究は、選択したRCTに含まれなかった
・院内肺炎・ICU死亡率・ICU滞在期間 に差は見られなかった院内肺炎 相対リスク1.06;95%信頼区間0.73–1.52;p=0.76;I2=0%ICU死亡率 相対リスク1.01;95%信頼区間0.83–1.24;p=0.91;I2=0%ICU滞在期間 相対リスク-0.54;95%信頼区間-2.20–1.13;p=0.53;I2=0%
2014.7.22勉強会 「H2B vs. PPI」参照
Alhazzani et al
702 www.ccmjournal.org
Figure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.
Alhazzani et al
702 www.ccmjournal.org
Figure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.
Alhazzani et al
702 www.ccmjournal.org
Figure 6. Forrest plot for nosocomial pneumonia outcome. Data from eight trials were included in the analysis using random effects model. The risk of nosocomial pneumonia was similar in both groups risk ratio [the same as relative risk] [RR] 1.06; 95% confidence interval [CI] 0.73–1.52). H2RA = hista-mine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 7. Forrest plot for ICU mortality outcome. Data from eight trials were included in the analysis using random effects model. The risk of death dur-ing the ICU stay was similar in both groups (risk ratio [the same as relative risk] [RR] 1.01; 95% confidence interval [CI] 0.83–1.24). H2RA = histamine 2 receptor antagonist; M-H = Mantel Haenszel; PPI = proton pump inhibitor.
Figure 8. Forrest plot for ICU length of stay outcome. Data from five trials were included in the analysis using random effects model. There was no statistically significant difference between groups (weighted mean difference −0.54; 95% confidence interval [CI] −2.20 to 1.13). H2RA = histamine 2 receptor antagonist; PPI = proton pump inhibitor.
6

Histamine-2ReceptorAntagonistsvsProtonPumpInhibitorsonGastrointesDnalTractHemorrhageandInfecDousComplicaDonsintheIntensiveCareUnit.
JAMAInternMed.2014;174(4):564-574
2014.7.22勉強会 「H2B vs. PPI」参照
【目的】
ストレス潰瘍予防薬としてのH2BとPPIを評価肺炎、CD感染症の発生率についても検討【方法】
後ろ向きコホート研究【対象】2003年1月1日〜2008年12月31日
アメリカの71の病院、24時間以上人工呼吸管理が行われ、ストレス潰瘍予防にH2BorPPIが投与された35312例【Primaryoutcome】二次診断(=入院中の病名)としての消化管出血、肺炎、CD感染症【Secondaryoutcome】ICU滞在期間、ICU死亡率、入院期間、コスト
7

Primaryoutcome、Secondaryoutcome• 単純比較
消化管出血:2.1%vs.5.9%院内肺炎:27%vs.38.6%CD感染症:2.2%vs.3.8%
ICU滞在期間(day)、ICU死亡率(%)、コスト($)も同様の結果。• プロペンシティスコアで修正→単純比較と同様の結果
消化管出血: 2.4%vs.4.7%(P<0.01)院内肺炎:30.7%vs.34%(P<0.01)CD感染症:2.6%vs.3.4%(P=0.02)
ICU死亡率のみPPI群で高かった。
2014.7.22勉強会 「H2B vs. PPI」より改変
H2BorPPIの投与をうけた35312例→H2B投与群13439人(38.1%)vs.PPI投与群21873人(61.9%)
いずれの発症率もPPI群で有意に高かった(p<0.001)
プロペンシティスコアで修正後→消化管出血のOR:2.24(1.81-2.76)と PPI群で有意に高い。
PPIはH2Bと比べ、消化管出血の増加、肺炎やCDIの増加と関連していた。
8
院内肺炎
ICU患者においてRCTのメタ解析ではPPIとH2Bに
院内肺炎について有意差はないが
9

JAMA. 2009;301(20):2120-2128
Acid-Suppressive Medication Use and the Risk for Hospital-Acquired Pneumonia.
【目的】
制酸剤と院内肺炎の関連を検討
【方法】
Prospective pharmacoepidemiologic cohort study
【対象】
3日間以上入院した18歳以上の患者
非人工呼吸器管理患者に制限するためICU患者は除外
【評価項目】
Primary:院内肺炎全て
(誤嚥性肺炎+非誤嚥性肺炎,ICD-9-CM codeに従って診断)
Secondary:誤嚥性肺炎,非誤嚥性肺炎 10

制酸剤全体の結果
PPI,H2Bの比較
PPIでは、有意に院内肺炎が多く発症するH2Bでは、調整済みオッズ比では有意差がなくなった 11

【目的】
重症患者において、 Pantoprazoleがranitidineと比べ、
肺炎リスクを上昇させるかを検討
【方法】
Retrospective cohort study
【対象】
Wake Forest University Baptist Medical Center(WFUBMC)
、Society of Thoracic Surgeons(STS)データベースに登録さ
れた18歳以上の心臓外科患者 1682例
【評価項目】
Pantoprazole群(377人)およびranitidine群(457人)に分割
Propensity scoreを用いて調節し肺炎の発生率を比較検討
Nosocomial Pneumonia Risk and Stress Ulcer Prophylaxis : A Comparison of Pantoprazole vs. Ranitidine in Cardiothoracic Surgery Patient.
2009年9月29日勉強会「 PPI vs. H2-blocker」改変
CHEST 2009; 136: 440-447
12

患者背景年齢,GERDの有無,心不全,人工呼吸の期間,輸血・輸血製剤の使用→有意差ありPropensity scoreにて調整後,有意差はなくなった消化管出血Pantoprazole : 3/337 (0.8%), Ranitidine : 1/457 (0.2%) p=0.33 有意差なし
2009年9月29日勉強会「 PPI vs. H2-blocker」参照13

2009年9月29日勉強会「 PPI vs. H2-blocker」参照
肺炎発生率 Pantoprazole: 35/377(9.3%) Ranitidine: 7/457(1.5%) OR:6.6 (95%CI:2.9-14.9)
Pantoprazoleが用いられる可能性で患者群を分割 Medium群,High群で 肺炎の発生が多かった
14

Acid-Suppressive Medication Use in Acute Stroke and Hospital-Acquired Pneumonia.
【目的】
急性脳卒中後の制酸剤使用と肺炎リスクを検討
【方法】
Retrospective cohort study
【対象】
18歳以上で急性の虚血性脳卒中もしくは出血性脳卒中
で入院した患者(入院2日以上の患者が対象)
1676人(2000年1月~2010年1月)
【評価項目】
院内肺炎発症
ANNNEUROL2014;76:712–718
15
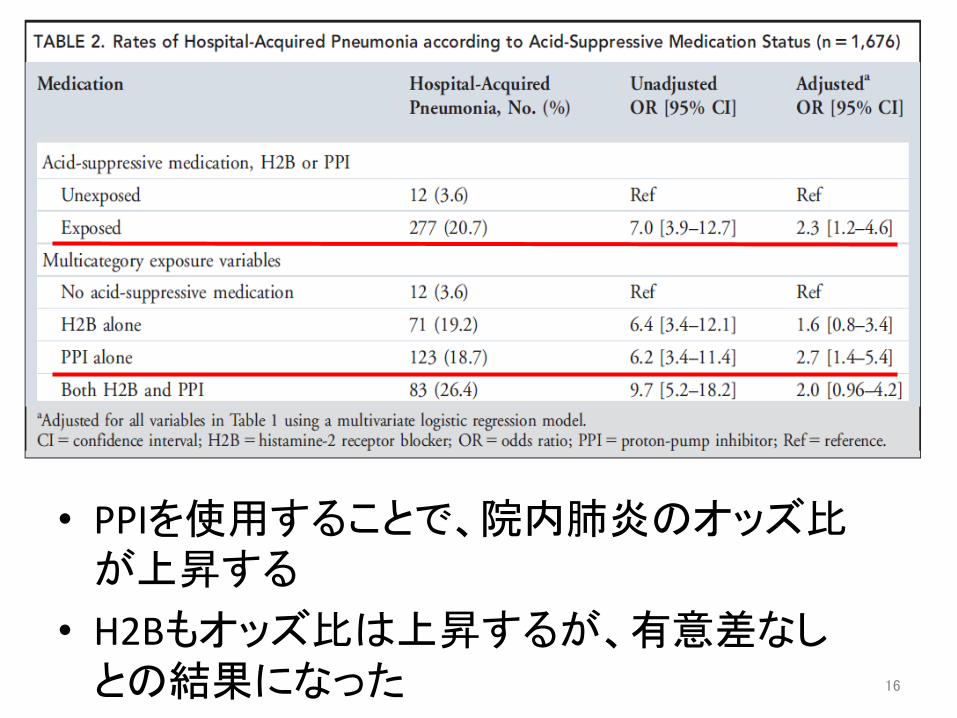
• PPIを使用することで、院内肺炎のオッズ比が上昇する
• H2Bもオッズ比は上昇するが、有意差なしとの結果になった 16

Clostridiumdifficile感染症
17

HostandPathogenFactorsforClostridiumdifficileInfecDonandColonizaDon NEnglJMed2011;365:1693.• カナダの6病院,15か月の前向き観察研究• Healthcare関連CDIとcoloniza=onの危険因子
2013.10.8勉強会 「重症CDI」参照
18

ProtonPumpInhibitorsandtheRiskforHospital-AcquiredClostridiumdifficileInfec=on.
MayoClinProc.2013;88(10):1085-1090
【目的】PPIと院内発症CDIとの関連を検討
【方法】Retrospective case-control study
【対象】入院3日以降にCDIを発症した67症例と、対照群としてマッチさせた134症例を比較
19

投与期間が長くなるほどCDIのリスクが上昇する
20
抗生剤の使用数によらず、PPIの使用期間が長いほどCD感染症率も上がる
Fig.1PPI使用期間と抗菌薬投与数からみたCDI発生率

【目的】 PPIとC.difficile再感染との関連をretrospec=veに解析【方法】Retrospec=vecohortstudy【対象】NewEnglandVeteransHealthSystem(VISN1)からデータを抽出(2003.10-2008.9)C.difficile(+)1549人 → CD(+)診断3日前後でメトロニダゾール,バンコマイシンで治療された1166例(PPI527名,non-PPI639名)
2010.9.14勉強会 「PPIとクロストリジウム」参照
ProtonPumpInhibitorsandRiskforRecurrentClostridiumdifficileInfecDon. ArchInternMed2010;170(9):772-778
21
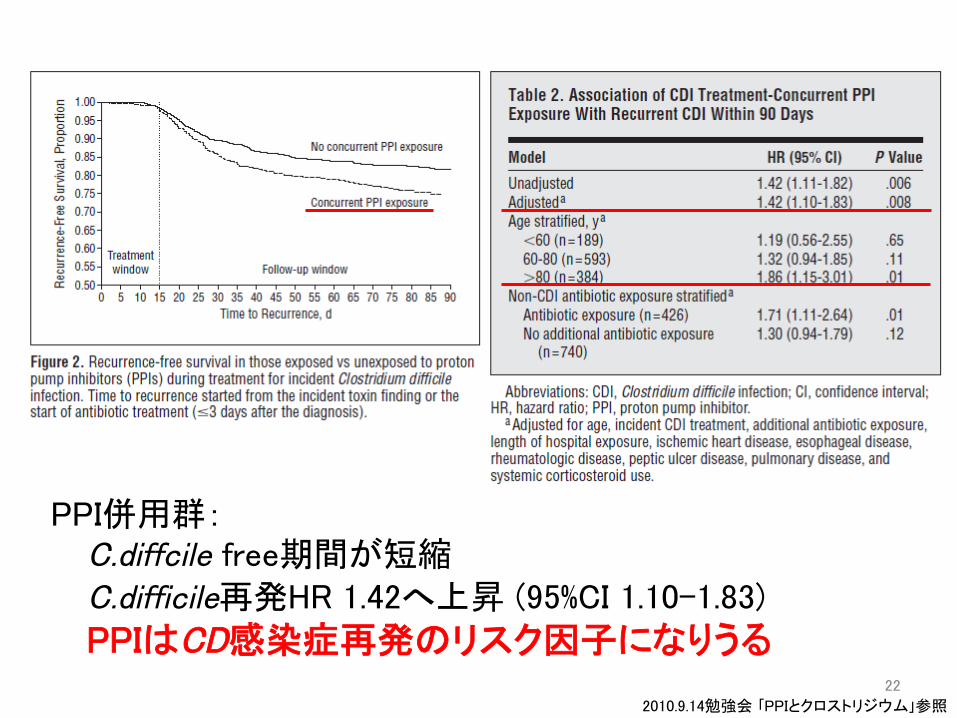
PPI併用群:C.diffcile free期間が短縮C.difficile再発HR 1.42へ上昇 (95%CI 1.10-1.83)
PPIはCD感染症再発のリスク因子になりうる
2010.9.14勉強会 「PPIとクロストリジウム」参照 22

経腸栄養とH2B
23

経腸栄養(EN)の普及
• 1990年代に入り”NilPerOs(NPO)”から”経腸栄養(EN)”が普及するようになってきた。• Enteralalimenta=onandgastrointes=nalbleedinginmechanicallyven=latedpa=entsCritCareMed1983;11:13-16• OUTCOMES:ICU入室した43名の患者について検討。21名に上部消化管出血が発生。制酸剤投与群では20人中14人、シメチジン投与群は9人中7人で上部消化管 出血を認めた。ENは合併症も少なく、上部消化管出血は1例も認めなかった。(14人中0人)→ENが上部消化管出血予防に有効?
2011.1.18 勉強会 「新世紀のストレス潰瘍予防」参照 24

【目的】SUPにおけるH2Bと経腸栄養の有益性と危険性をメタ解析にて検証【対象】SUPとUGBの関連性に関するRCT(H2B vs. プラセボのみ)【評価項目】Primaryoutcome臨床的に重要な上部消化管出血の発生SecondaryoutcomeHospital-acquiredpneumonia(HAP)の発生
Stressulcerprophylaxisinthenewmillennium:AsystemaDcreviewandmeta-analysis
2011.1.18 勉強会 「新世紀のストレス潰瘍予防」参照
CritCareMed2010;38(11):2222-8
25

消化管出血率 EN(-): H2B投与群で低い EN(+): 有意差なし
院内肺炎 EN(-): 有意差なし EN(+): H2B投与群で高い
死亡率 EN(-): 有意差なし, EN(+): H2B投与群で高い
消化管出血率 院内発生肺炎(HAP)
死亡率
2011.1.18 勉強会 「新世紀のストレス潰瘍予防」参照
H2B+EN→ストレス潰瘍出血のリスクを減少しない
26

Weighing risks and benefits of stress ulcer prophylaxis in
critically ill patients.
Stress ulcer prophylaxis in the new millennium: A systematic
review and meta-analysis. に対するコメント
Crit Care 2012; 16: 322-323
H2BはEN投与患者には、+ストレス潰瘍予防効果がなったとの結論を受
けEN投与の試験のみに着目。
Outcome 母集団全体 EN群 非EN群
消化管出血OR 0.47[0.29-0.76] 1.26[0.43-3.70] 0.37[0.23-0.61]
院内肺炎OR 1.53[0.89-2.61] 2.81[1.20-6.56] 1.26[0.68-2.32]
死亡率OR 1.03[0.78-1.37] 1.89[1.04-3.44] 0.87[0.36-1.19]
経腸栄養施行患者へのH2B投与は、院内肺炎や死亡率のリスクが増加する可能性がある。と論じられている。27

低マグネシウム血症
28

PPI長期服用による低マグネシウム血症との関連 (米国FDA2011.3.2通知)
• 副作用報告システムに寄せられた事例や文献報告などの 51事例を検討
• PPI長期服用(1年以上)が低Mg血症を引き起こす可能性がある
• Mg補充のみでは低Mg血症が改善せず、PPIの服用中止が必要となったものが、検討症例の1/4あった
• 発生機序は不明であるが、長期服用はMg腸管吸収の変化と関連する可能性がある
医薬品安全性情報 Vol.9No.07より抜粋29

Systematic review: hypomagnesaemia induced by proton pump inhibition.
【目的】PPIと血清Mg値の変動を検討【対象】2011年11月までにMEDLINE、PubMedに投稿された36症例(女性24例(66.7%)、平均67.4±1.9歳(30〜83歳))【評価項目】PPI投与中止、再開における血清Mg値低マグネシウム血症誘発までのPPIの投与期間
Aliment Pharmacol Ther 2012; 36: 405–413
30

PPI中断後の血中Mg濃度変化 PPI再開後の血中Mg濃度変化
• 発症までの投与期間は中央値で5.5年(14日から13年)• 低Mg血症は中止後4日程度で回復、再開後4日程度で再発につながる可能性あり• H2Bは代替薬剤として考慮すべき 31

【目的】PPI、H2Bが血清Mg濃度に与える影響を調査【対象】ベスイスラエルメディカルセンターICUに2001-2008年までに入院した成人患者。H2B、PPIが入院時処方に記載されている場合、暴露ありとした。 内訳→PPI:2632人、H2B:657人【評価項目】入院後36時間以内の血清Mg濃度
32

• PPI使用者は血清Mg低下と関連あり• 利尿剤併用で、低下の度合、オッズ比が増
強した
単位:mg/dL
33

まとめ
• 消化管出血予防効果は、エビデンスレベルに違いはあるが PPIが優れている というわけではない
• 院内肺炎は、コホート研究ではPPI使用によるリスクの上昇が示唆されており考慮が必要
• Clostridiumdifficile 感染症は、ICU患者に限定した報告はないが PPIによるリスク上昇が報告されている
• Clostridiumdifficile 感染症再発時は、PPIの使用は要検討
34

まとめ
• ENはストレス潰瘍予防効果を有する可能性があるが、H2Bとの併用では副作用のリスクを上昇させてしまう
• ENが開始できない場合、ストレス潰瘍予防を考慮すべき
• PPIは短期使用でも低Mg血症は起きるとされるが、適切にモニタリングしていれば重篤にはならない
• 種々の合併症を防ぐためにも、ストレス潰瘍予防薬は病態が改善すれば終了すべきである
35

参考
36

ストレス潰瘍予防の適応
37

成人ICU患者でのストレス潰瘍予防の適応(エビデンスの強さ)
絶対適応(1つでも該当すれば適応) 凝固障害(血小板<50000/mm3、PT-INR>1.5、APTTが正常時の2倍以上)(B) 48時間以上の人工呼吸器管理(B) 1年以内の上部消化管潰瘍または出血(D) GCS≦10(または簡単な指示に従えない)(B) 体表面積>35%の熱傷(B) 肝部分切除後(C) 多発外傷(InjurySeverityScore≧16など),移植患者周術期, 肝不全,脊椎外傷に該当(D)相対適応(2つ以上該当すれば適応) 敗血症(D) 1週間以上のICU在室(D) 6日間以上の便潜血(D) 高用量コルチコステロイド治療(ヒドロコルチゾン250mg/日相当量以上)(D)
INTENSIVISTVol.6No.22014 より転載38

SSCG(SurvivingSepsisCampaignGuidelines)におけるストレス潰瘍予防
• 出血リスクを有する重症敗血症/敗血症性ショックの患者に対して,ストレス潰瘍の予防としてH2BやPPIの投与を推奨する(1B)
• ストレス潰瘍の予防には,H2RAよりもPPIのほうが望ましい(2C)
• 危険因子のない患者には予防を行うべきではない(2B)
39
クロピドグレルとオメプラゾール
プラセボ対象RCTの報告
40

ClopidogrelwithorwithoutOmeprazoleinCoronaryArteryDisease.(COGNETtrial) NEnglJMed2010;363:1909-17
【目的】
DAPT(clopidogrel+aspirin)併用療法を受けている冠動脈疾患患者において、omeprazole併用の有効性・安全性を検討
【方法】
多施設(15か国393施設)、プラセボ対照、RCT【対象】
omeprazole群(1,876例):clopidogrel(75mg)/omeprazole(20mg)配合剤を投与プラセボ群(1,885例):clopidogrel(75mg)のみを投与 全例にaspirinを75~325mg/日投与
21歳以上,ACSor冠動脈ステント植込み予定の患者で、12か月以上のclopidogrel+aspirin併用療法が予想されるもの。
大追跡期間は2年であったが、スポンサーの資金調達が不能となり早期に中止されている。(追跡期間106日(中央値))
【評価項目】
有効性:上部消化管イベントの初発までの期間安全性:心血管死+非致死性心筋梗塞+再血行再建術+脳梗塞(複合エンドポイント)41

Ome:4.9%Pla:5.7%
有効性1次エンドポイント消化管イベントはomeprazole群で有意に低下安全性1次エンドポイント心血管イベントは群間差なし
DAPT中冠動脈疾患患者において• PPIの予防的投与により上部消化管出血の発生率は有意に減少• Omeprazole併用による心血管系イベントリスクはなかった
この結果が、PPIの使用により心血管イベントに臨床的に意味のある差異が生じることを否定するものではない。としている。 42
Recommended

















