1
INFLUENZA VIRUS
INFLUENZA VIRUS
CDC WEBSITE
http://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm

2
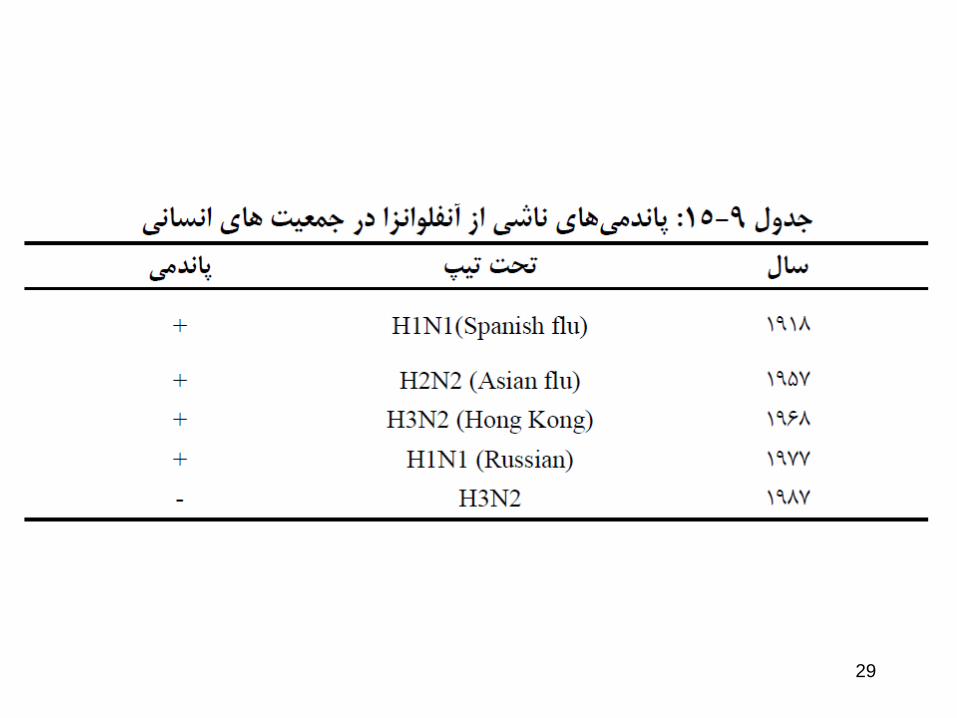
1 9 1 8 -1 9 S p a n is h f lu 5 0 0 ,0 0 0 U S
2 0 ,0 0 0 ,0 0 0 w o r ld
1 9 5 7 -5 8 A s ia n f lu 7 0 ,0 0 0 U S
THE IMPACT OF INFLUENZA
PANDEMICS
Deaths:
3
THE IMPACT OF INFLUENZA
• In the United States, on average:
• 36,000 deaths per year
• 114,000 hospitalizations per year
CDC: MMWR 53:8-11, 2004

4

5
ORTHOMYXOVIRUSES
M1 protein
helical nucleocapsid (RNA plus
NP protein)
HA - hemagglutinin
polymerase complex
lipid bilayer membrane
NA - neuraminidase
type A, B, C : NP, M1 protein
sub-types: HA or NA protein
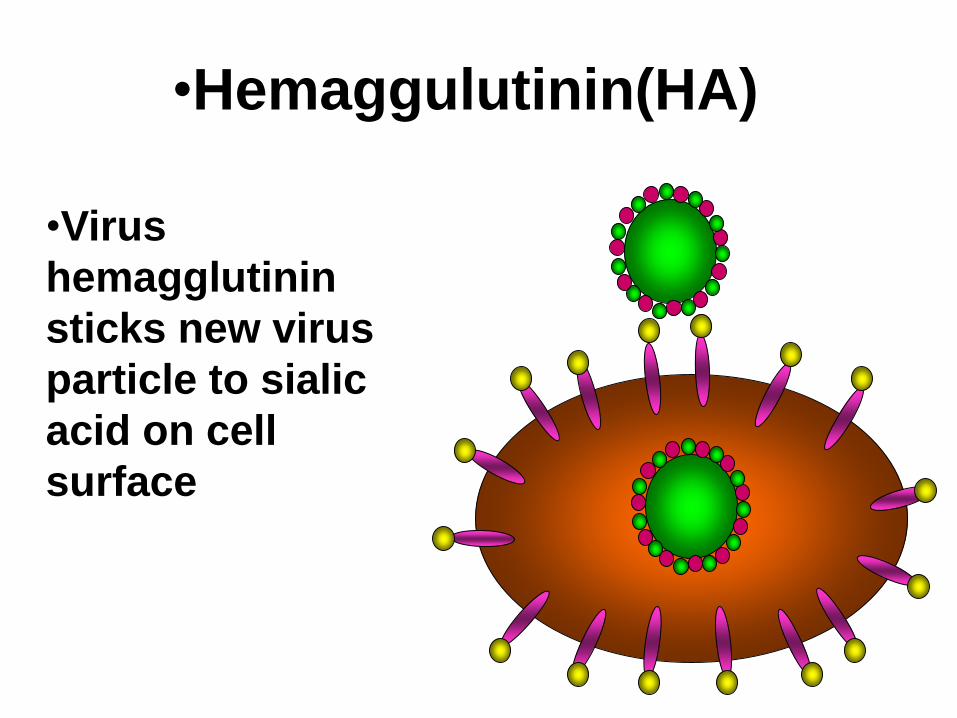
•Virus
hemagglutinin
sticks new virus
particle to sialic
acid on cell
surface
•Hemaggulutinin(HA)

7

Replication
8
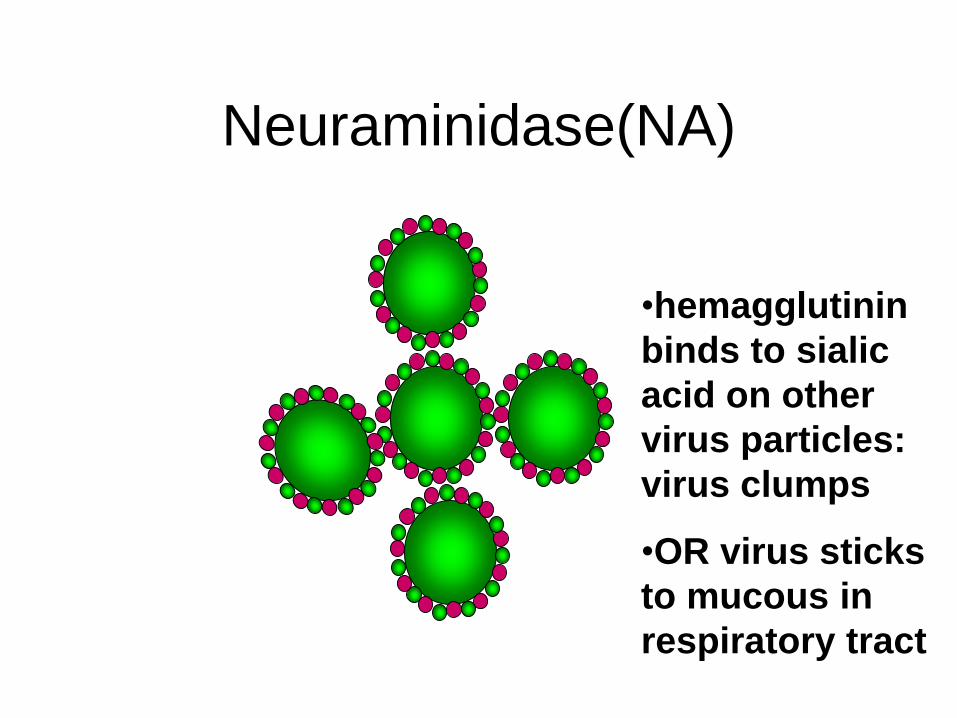
•hemagglutinin
binds to sialic
acid on other
virus particles:
virus clumps
•OR virus sticks
to mucous in
respiratory tract
Neuraminidase(NA)
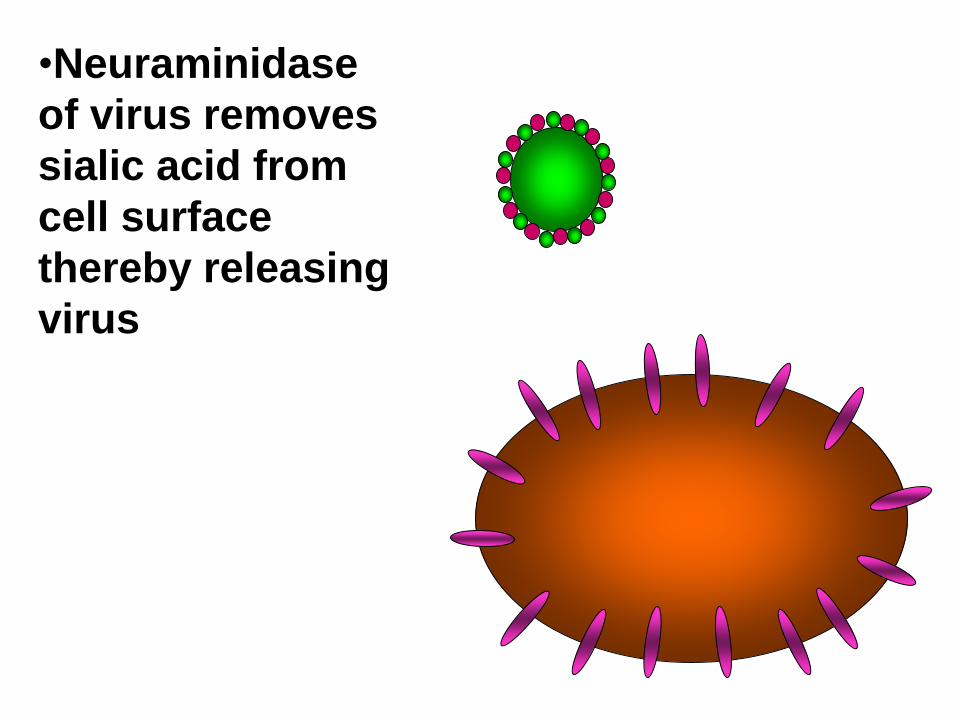
•Neuraminidase
of virus removes
sialic acid from
cell surface
thereby releasing
virus
11
TRANSMISSION
• AEROSOL
– 100,000 TO
1,000,000 VIRIONS
PER DROPLET
• 18-72 HR
INCUBATION
• SHEDDING
12
13
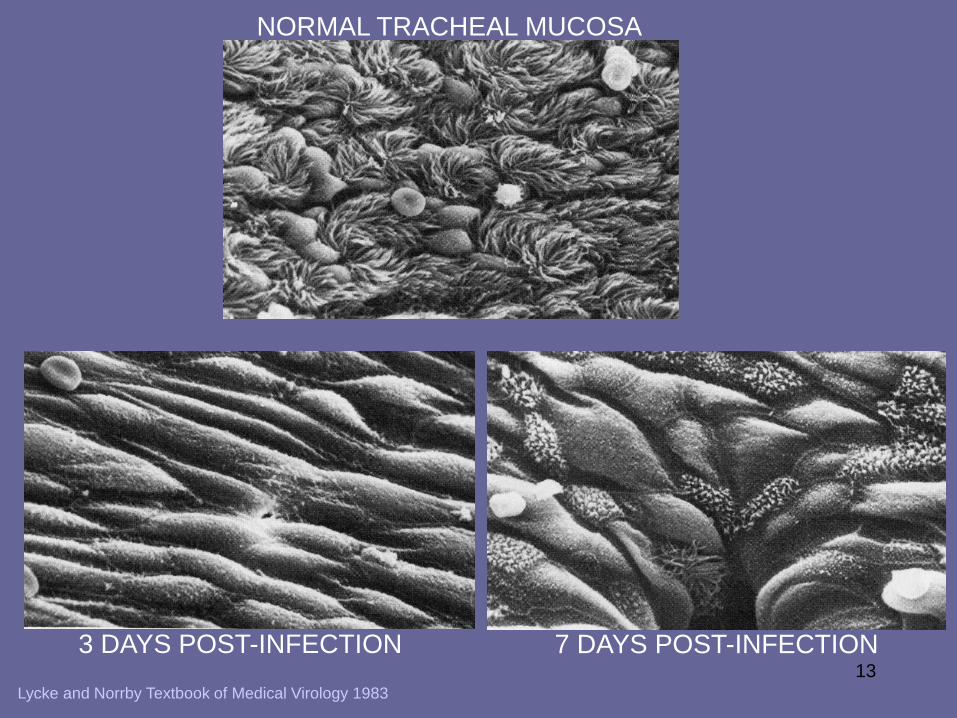
NORMAL TRACHEAL MUCOSA
3 DAYS POST-INFECTION 7 DAYS POST-INFECTION
Lycke and Norrby Textbook of Medical Virology 1983

14
• DECREASED
CLEARANCE
• RISK BACTERIAL
INFECTION
• VIREMIA RARE
Lycke and Norrby Textbook of Medical Virology 1983
15
RECOVERY
• INTERFERON - SIDE EFFECTS INCLUDE:
– FEVER, MYALGIA, FATIGUE, MALAISE
• CELL-MEDIATED IMMUNE RESPONSE
• TISSUE REPAIR
– CAN TAKE SOME TIME
16
SIDE EFFECTS OF
INTERFERONS
• FEVER
• MALAISE
• FATIGUE
• MUSCLE PAINS
17
PROTECTION AGAINST
RE-INFECTION
• IgG and IgA
– IgG less efficient but lasts longer
• antibodies to both HA and NA important
– antibody to HA more important (can
neutralize)
18
SYMPTOMS
• FEVER
• HEADACHE
• MYALGIA
• COUGH
• RHINITIS
• OCULAR SYMPTOMS
19
CLINICAL FINDINGS
• SEVERITY
– VERY YOUNG
– ELDERLY
– IMMUNO-
COMPROMISED
– HEART OR LUNG
DISEASE

20
PULMONARY
COMPLICATIONS• CROUP (YOUNG CHILDREN)
• PRIMARY INFLUENZA VIRUS PNEUMONIA
• SECONDARY BACTERIAL INFECTION
– Streptococcus pneumoniae
– Staphlyococcus aureus
– Hemophilus influenzae
21
NON-PULMONARY
COMPLICATIONS• myositis (rare, > in children, > with type B)
• cardiac complications
• recent studies report encephalopathy– 2002/2003 season studies of patients younger than
21 yrs in Michigan - 8 cases (2 deaths)
• liver and CNS– Reye’s syndrome
• peripheral nervous system– Guillian-Barré syndrome
22
Reye’s syndrome
• liver - fatty deposits
• brain - edema
• vomiting, lethargy, coma
• risk factors
– youth
– certain viral infections (influenza, chicken
pox)
– aspirin
23
Guillian-Barré syndrome
• 1976/77 swine flu vaccine
– 35,000,000 doses
• 354 cases of GBS
• 28 GBS-associated deaths
• recent vaccines much lower risk
24
MORTALITY
• MAJOR CAUSES OF INFLUENZA
VIRUS- ASSOCIATED DEATH
– BACTERIAL PNEUMONIA
– CARDIAC FAILURE
• 90% OF DEATHS IN THOSE OVER 65
YEARS OF AGE

25
DIAGNOSIS
• ISOLATION
– NOSE, THROAT SWAB
– TISSUE CULTURE OR EGGS
• SEROLOGY
• PCR
• RAPID TESTS
• provisional - clinical picture + outbreak
26
ANTIGENIC DRIFT
• HA and NA accumulate mutations
– RNA virus
• immune response no longer protects
fully
• sporadic outbreaks, limited epidemics
27
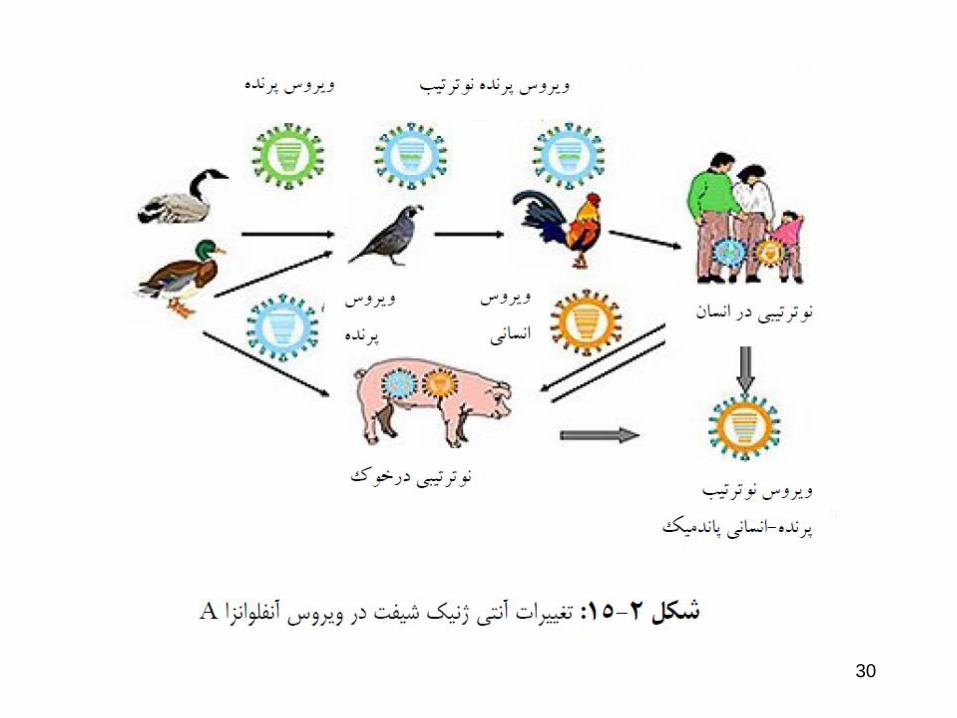
ANTIGENIC SHIFT
• “new” HA or NA proteins
• pre-existing antibodies do not protect
• may get pandemics
28
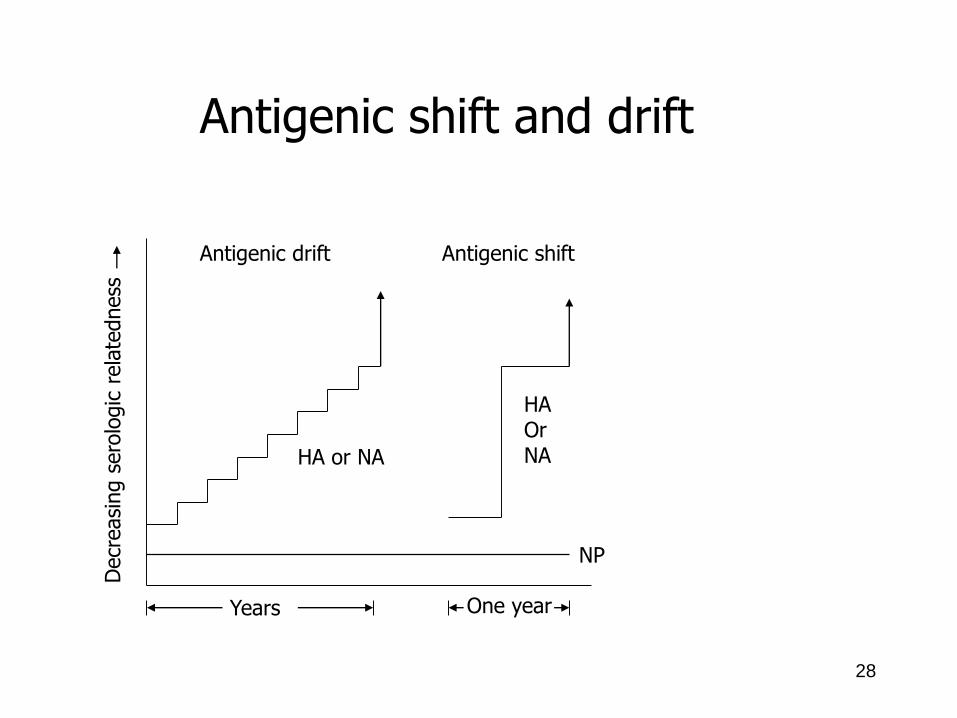
Years One year
HA or NA
HAOrNA
Antigenic drift Antigenic shift
Decr
easi
ng s
ero
logic
rela
tedness
NP
Antigenic shift and drift
29
30

31
Where do “new” HA and NA come from
- can ‘new’ bird flu directly infect humans?
Bird flu H5N1?
32
H5N1 – in birds
• Avian H5N1 has spread to humans
• So far human cases in Asia and Africa– 256 cases (12-1-03 through 10-16-06)
– 151 (59%) fatal
• Have been a few instances where may have spread human-to-human
• So far no sustained spread in humans
• Surveillance continues
33
why do we not have influenza
B pandemics?
• so far no shifts
have been
recorded
• no animal
reservoir
known
34
VACCINE
• ‘BEST GUESS’ OF MAIN ANTIGENIC
TYPES
– CURRENTLY
• type A - H1N1
• type A - H3N2
• type B
• each year choose which strain of each subtype
is the best to use for optimal protection
35
VACCINE
• inactivated
• egg grown
• some formulations licensed for children
• reassortant live vaccine approved 2003
– for healthy persons (those not at risk for complications from influenza infection) ages 5-49 years
36
PREVENTION - DRUGS
• RIMANTADINE (M2)• type A only
• AMANTADINE (M2)• type A only
• 2005-6 season• H3N2 virus - 92% isolates resistant to rimantadine and
amantadine in US, so these drugs not recommended until % resistance in major circulating type drops
• ZANAMIVIR (NA)• types A and B
• OSELTAMIVIR (NA)• types A and B
37
TREATMENT - DRUGS
• RIMANTADINE (M2)• type A only, needs to be given early
• AMANTADINE (M2)• type A only, needs to be given early
• ZANAMIVIR (NA)• types A and B, needs to be given early
• OSELTAMIVIR (NA)• types A and B, needs to be given early
38
OTHER TREATMENT
• REST, LIQUIDS, ANTI-FEBRILE
AGENTS (NO ASPIRIN FOR AGES
6MTHS-18YRS)
• BE AWARE OF COMPLICATIONS
AND TREAT APPROPRIATELY
39
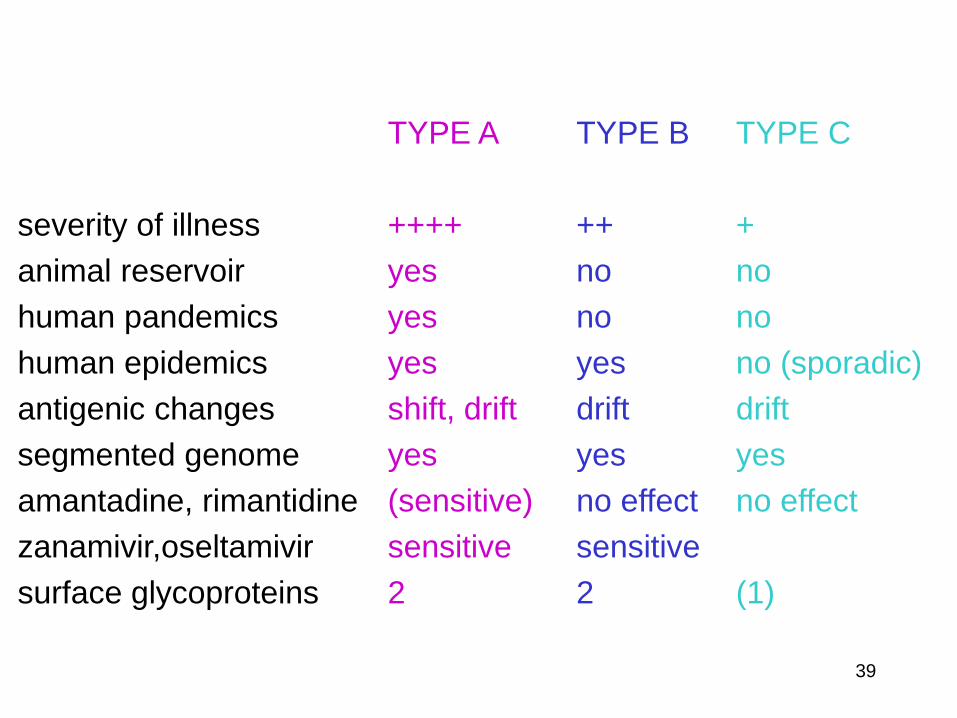
TYPE A
++++
yes
yes
yes
shift, drift
yes
(sensitive)
sensitive
2
severity of illness
animal reservoir
human pandemics
human epidemics
antigenic changes
segmented genome
amantadine, rimantidine
zanamivir,oseltamivir
surface glycoproteins
TYPE B
++
no
no
yes
drift
yes
no effect
sensitive
2
TYPE C
+
no
no
no (sporadic)
drift
yes
no effect
(1)
Recommended










![Dr. Ruby Kevala, DC, DACNB., Chiropractic Neurologist · Multiple Sclerosis Mumps Osteoporosis Pacemaker [2 Yes C] Yes C) Yes C] Yes C] Yes Parkinson's Disease C] Yes Pinched Nerve](https://img.pdfslide.tips/doc/110x75/5f437b6d8b35c93990049cb4/dr-ruby-kevala-dc-dacnb-chiropractic-neurologist-multiple-sclerosis-mumps-osteoporosis.jpg)





