1 Center for American Progress | Insurers’ Black Box
Insurers’ Black BoxNow-Secret Claims Denial Rates Could Tell Consumers a Lot About Their Insurance Company
Scot J. Paltrow October 21, 2009
Key points
• Therateatwhichinsurancecompaniesdenyclaimsiscriticalforconsumerstoknowwhenshoppingforinsurance—buttodayinsurancecompaniesarekeepingthoseratessecret.
• Claimsdenialrateshavebeenreleasedinonlyonestate—California—andthedatashowsdramaticvariationsindenialratesamongcompanies,whichoneexpertsaysshouldraiseanalarmforregulators.
• Whenitcomestoclaimdenials,insurersmaybeputtingprofitsaheadofpatients’bestinterests.Mostmajorinsurancecompanieshavereassignedtheirmedicaldirectors—thedoctorswhoapproveordenyclaimsformedicalreasons—toreporttotheirbusinessmanagers,whosemainresponsibilityistoboostprofits.
Introduction
ThehealthcarereformbillspendinginCongresswouldrequirenearlyeveryAmericantohavehealthinsurance.Millionsofpeoplewouldhavetoshopforcoverageforthefirsttime.Yetsomeofthemostusefulinformationforchoosingapolicyremainstopsecret—lockedawayinhealthinsurers’computers.
Consumershaveastronginterestinpickingacompanythatwillreliablypaytheirlegiti-mateclaimswhentheyneedmedicaltreatment.Buthealthinsurancecompaniesdon’tdisclosethepercentageofclaimstheyrejectanddeclinetopay.AndinquiriesbytheCenterforAmericanProgressshowthatthenation’sinsuranceregulatorshavenotaskedthemtodoso.

2 Center for American Progress | Insurers’ Black Box
CAPinrecentweekslaunchedaninvestigationtodeterminewhetherdataoncommercialhealthinsurers’claimdenialratesisavailablenationwideorinanystates.TheresearchincludedinterviewswithmultipleseniorofficialsoftheNationalAssociationofInsuranceCommissioners,othercurrentandformerinsuranceregulatorsandgovernmentofficialsinstatesaroundthecountry,officialsathealthinsurancecompanies,academicexperts,andothers.Allsaidthatnosuchdataisavailable.Nostateinsuranceregulatorsorfederalagen-ciesrequireinsurerstodisclosetheirclaimdenialrates,exceptinCalifornia.California’sDepartmentofManagedHealthCarerequiresinsurerstoincludeitinreportstheyfile.
CAPalsoaskedeachofthenation’ssevenlargestfor-profithealthinsurers—Aetna,AnthemBlueCrossBlueShield,Cigna,Coventry,HealthNet,Humana,andUnitedHealthcare—ifforthepurposesofthisreporttheywoulddisclosetheiroverallratesofclaimsdenialsandbreakdownsbyreasonforthedenials.Allofthecompaniesdeclinedordidnotgiveanydirectresponsetotherequest.Spokesmenforthecompaniesingeneralsaidthattheinsurerspaythevastmajorityofclaims,andthatdenialsarefair,withmostoccurringforroutinereasonssuchasapatienterroneouslysubmittingthesameclaimtwiceoraphysiciansendingaclaimtothewrongcompany.
ButthereportsfromCaliforniaindicatewhyhealthinsurancecompaniesmaybereluctanttodisclosetheirclaimdenialrates.Thatdatashowsthatthreeofthesixlargesthealthinsur-ancecompaniesinthestateeachdenied30percentormoreofallclaimsfiledinthefirstsixmonthsof2009.Italsoshowedwidevariationsindenialratesamongthecompanies.
TheCaliforniaNursesAssociation—whichdisclosedthedata—saysthatthehighpercent-ageofdenialsbysomeCaliforniahealthinsurersstronglysuggeststhattheinsurersaregoingbeyondreasonablestandardstorejectclaimsandmaybeimproperlyusingclaimstoboostprofits.CaliforniaAttorneyGeneralJerryBrownhaslaunchedaninvestigationintotheclaimsdenialsinresponsetothisnewdata,althoughtheCaliforniainsurersdenymak-ingimproperdenialsandsaytherawpercentagesofrejectionsaremisleading.
Otherevidencealsosuggeststhatinsurersmayberejectingsignificantnumbersofvalidclaimsduetoconstantpressuretoboostprofitsandsatisfyshareholders.Informationhasemergedrecentlyincongressionalhearingsonthehealthcaredebate,pressaccountsofindividuals’confrontationswithinsurersoverpaymentfortreatment,andfromscoresofinterviewsbytheCenterforAmericanProgress.
“Claimsdenialsareprobablythemosteffectivewaytheindustryhastomanagemedicalexpenses,”saysWendellPotter,whoin2008resignedasaseniorpublicrelationsexecutiveathealthinsurancecompanyCignaCorp.Potterisnowanoutspokencriticofhealthinsur-ersandsaidthecompaniesputpressureonemployeestohelpcontrollossesandmeetthecompanies’financialgoals,includingdoctorsandnurseswhomakedecisionsonwhethertoalloworrejectclaimsbasedonmedicalnecessity.

3 Center for American Progress | Insurers’ Black Box
QuestionsaboutreliableclaimspaymentwillbeparticularlyimportantifCongresspassesfederalhealthcarelegislation,becauseitwouldrequirethegovernmenttosubsidize,throughtaxcredits,insurancecoverageforlow-incomeindividuals.MembersofCongressandthepublicmaydemandtoknowifthegovernmentisgettingitsmoney’sworth.
Blurring the lines of ‘medical necessity’
Aclaimsdenialoccurswhenaninsurerdeclinestopayrequestedreimbursementforspe-cificservicesforapatient,suchasdoctorvisits,treatment,medicalprocedures,orhospitalstays.Denialsfallintothreecategories:Eligibilityissues,whichoccurswhenapatient’scoveragehasexpiredoratypeoftreatment,suchascosmeticsurgery,isexplicitlyexcludedinthehealthinsurancepolicy;administrativeissues,suchaswhenaclaimformisfilledoutimproperly;andappropriatenessissues,ordecisionsthatcertaintreatmentsaren’tmedi-callynecessary,orareexperimentalandnotyetprovedeffective.
Themostsensitiveandpotentiallycontroversialclaimsarethosebasedonmedicalcriteria—suchaswhetheratreatmentismedicallynecessaryorshouldnotbecoveredbecauseitisdeemedexperimental.CAPlearnedininterviewswithformerseniormedicalpersonnelatseveralofthelargestinsurersthatbiginsurers—includingAetna,Cigna,andUnitedHealthcare—madeinternalchangesinrecentyearsthatgavebusinessexecutivesmoredirectauthorityoverthecompanies’doctorswhoevaluateclaimsbasedonthesemedicalcriteria.
Insurancecompanieshadpreviouslymaintainedaseparationbetweenthemedicalevalua-tionstaffandtheexecutivesresponsibleforfinancialperformance.Thedoctorsandnursesreportedtothecompanies’chiefdoctor—knownasthechiefmedicalofficer—whohadfinalsayonwhethercoverageforaparticularindividual’streatmentshouldbegrantedordeniedbasedonmedicalcriteria.Butbeginningaboutadecadeago,inashakeupthatevidentlyreceivednopublicattention,companieschangedtheirpoliciessothatthemedicalstaffreportedtoregionalbusinessexecutives.Theseexecutivesweregiventheauthoritytodeter-minethedoctors’pay,bonuses,andpromotion,andconsequentlytheygainedthepowertoinfluencethedoctors’decisions.Thenewsystemsgenerallykept“dottedline”reportingtothechiefmedicaloffice,whowouldstillweighinonthemostdifficultclaimsdecisions.
Insurers likely deny millions of claims annually
KevinLembo,theConnecticutstategovernment’shealthcareadvocateforHMOandmanagedcarepatients,saiddisclosureofclaimsdenialrates,“Wouldbeincrediblyuseful.Asastraightconsumerchoiceissue,reallyattheendofthedaywhatdoconsumerswant?Theywanttheirinsurancecarrierstopaytheirbills.”

4 Center for American Progress | Insurers’ Black Box
FormerIndianaInsuranceCommissionerSallyMcCartysaidclaimsdatashowingwidevariationsbetweencompaniesinrejectionrates,orthataninsurergreatlyincreasedclaimsrejectionsfromoneyeartothenext,couldbeanalarmforregulatorstoinvestigate.
Theissueofrejectedclaimshasreceivedrelativelylittlepublicattentioninthehealthcaredebate,whilenewscoveragehasfocusedmoreondisclosuresincongressionalcommitteehearingsaboutotherpractices,suchasrescissions.Rescissionsaremuchlesscommonthanclaimrejectionsandoccurwhenhealthinsurerscancelanindividual’scoveragealto-gether,oftenwhenapolicyholderfilesaclaimforanexpensivetreatment.Thecompaniesinvolvedcommonlyjustifyrescissionsonthegroundsthatthepolicyholderhadimprop-erlyfailedtodiscloseapre-existingcondition,evenifthiswasminorandunrelatedtotheillnesspromptingtheclaim.
Thereisnoreliableestimateofthetotalnumberofhealthcareclaimsthatinsurersdenyannually.ButMarkRieger,chiefexecutiveofNationalHealthcareExchangeServices,whichcollectsclaimsdatafromphysicians,saysthenumbercertainlyisinthemillionsannually.Rescissionsareestimatedtobeonlyinthethousands.
Insurerssaythattheybasedecisionstoturndownclaimsonlyonobjective,clear-cutstandards,butindividualstorieshighlightthatcompaniesattimescantakewidelatitudeinapplyingthem.Forexample,recordsfromafederallawsuitinNorthCarolinashowthatCignaofNorthCarolinarefusedtopayforspecializedtreatmentforababybornwithaseverelydeformedskull.Thebaby’sdoctorswantedtouseanorthoticdevicetohelpmoldherheadintoamorenormalshapeasshegrew.Thedoctorssaidthatwithoutthetreatmentmoremedicalproblemscouldensue,suchasaworseningmalformationofherjaw.Cignadeclinedtopayonthegroundthatsuchtreatmentwasa“cosmeticprocedure.”A2002federalappealscourtdecisionnotedthatCignaneverprovidedanydefinitionof“cosmeticprocedure”initspolicyandorderedthecompanytopay.1
JohnPowell,aNewYorkStateinsurancedepartmentofficialwhomonitorshealthinsurers,sayssomeseizeontechnicalitiesorminorflawsinclaimstomakewhathecalls“gotchadenials”ofdoubtfulvalidity.These,hesaid,canincluderejectionsbecauseofminorerrorsinhowpatientsfilledoutclaimforms,orbecausetheinsurancecompanysaysaclaimwassubmittedtoolateaftertreatment.
Data from California shows high claim denial rates
TheCaliforniaNursesAssociationsoundedanalarmonclaimsdenialsinearlySeptemberthisyearafteritsresearchersfounddataonastateagencywebsitethathadnotreceivedpublicattention.TheinformationwasburiedinascheduleattachedtofinancialreportsfiledbyinsurerswithCalifornia’sDepartmentofManagedHealthCare.Datainthereportsshowedthatthreeofthesixlargesthealthinsurancecompaniesinthestateeach

5 Center for American Progress | Insurers’ Black Box
denied30percentormoreofallclaimsduringthefirstsixmonthsof2009.Thesixcom-paniescombinedhave67percentofCalifornia’smanagedcaremarket,whichbyfaristhelargestinthecountry.
CaliforniaNursesAssociationCo-PresidentDeborahBurgersaidthenumbersshowthattheinsurersoftendenyclaims“simplybecausetheydon’twanttopayforit.”
Theinsurancecompaniesstronglyreactedtothedisclosureandthenursesassociation’sconclusionthatthedataindicatehighratesofunfairdenials,eventhoughthedatacamefromtheirownreports.Theycorrectlynotedthatthepatientsreceivedtreatmentinmostinstanceseventhoughthecompanieslaterdeniedthereimbursementclaimsfromphysi-ciansandhospitals.
CaliforniaAssociationofHealthPlansCEOPatrickJohnstonsaidthenurses’disclosureofthedenialrates“wasacursoryandinaccurateportrayalofthepatternofhealthcareandpaymentstoproviderstypicalinCalifornia.”
QueriedbyCAPaboutthedata,UnitedHealthcareSpokeswomanCherylRandolphsaidthat80percentoftotaldenialsatthecompany’sPacifiCareHMOinCaliforniawerebecausephysiciangroupserroneouslysubmittedclaimsfortreatmenteventhoughPacifiCarepaysthegroupsaflatratebasedonthenumberofPacifiCare-coveredpatientstheytreatunderso-called“capitationagreements.”Randolphsaidtheflatrateissupposedtocoverallofpatient’streatmentcostsbythegroups,butthatthephysiciansoftenerroneouslysubmitclaimsforspecifictreatmentsorprocedures.Shesaidthatthepatientsdidreceivethemedicaltreatmenteventhoughthecompanydeclinedtoreimbursethephysicians.
Randolphsaidthatofthedenialsforotherreasons,“95percentofthoseweredeniedbecausetheindividualwasineligible,meaningtheywerenotinsuredunderaPacifiCareplan.”
CignaSpokesmanChristopherCurranalsocitedbillserroneouslysentforpatientscoveredundercapitationagreements,whichhesaidaccountedforabouthalfoftheCignadenials.Hesaidalargeportionoftherestwerefor“duplicatebillings”submittedfortreatmentsthattheinsureralreadyhadpaidfor.Curransaidthat,“OutofalleligiblerequestsforcoveragesubmittedtoCIGNAHealthcareofCaliforniainthefirsthalfof2009,morethan95.9percentwerecoveredandthepersonreceivedthecarerecommendedbythedoctor.”
Yetdenialsbecauseofcapitationagreementsaren’tnecessarilyblack-and-white.Physiciansmaybillforservicesthataren’tcoveredundertheircapitationagreements.AndJamesG.Kahn,presidentoftheCaliforniaPhysiciansAllianceandprofessoroftheUniversityofCaliforniaSanFrancisco’sInstituteforHealthPolicyStudies,saysconfusionoccursduetoanincreasingnumberof“carve-outs”fromcapitationagreements.Theseexemptcertainspecializedtreatments,ormayexcludeseriousdiseasessuchasAIDS.Dr.Kahnsaysthereareoftendisagreementsbetweenphysiciansandinsurersaboutwhetheraclaimfallsunderoneofthecarve-outs.
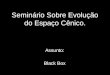
Percentage of claims denied
January – June 2009
CompanyPercent of
claims denied
UnitedHealth care’s PacifiCare 39.6
Cigna Health care of California 32.7
Health Net 30.0
Kaiser Permanente 28.3
Blue Cross 27.0
Aetna 6.4
Source: California Nurse’s Association and the individual company reports posted on California Department of Managed Health care web site, available at http://www.calnurses.org/media-center/press-releases/2009/september/california-s-real-death-panels-insurers-deny-21-of-claims.html and insurers’ reports filed with DMHC, available at http://wpso.dmhc.ca.gov/fe/search/#top

6 Center for American Progress | Insurers’ Black Box
Aetna’sdenialrateof6.4percentwassignificantlylowerthanitssixmaincompetitorsinCalifornia,butAetnaSpokesmanMohitGhosedeclinedtocommentonthepracticesoftheotherinsurers.HedidsayAetnaadheresstrictlytotherequiredtermsofitscoverage,andsaid,“Wetakeanyclaims’non-paymentveryseriouslyatAetna.”
Insurers pressure their doctors to deny claims
Officialsfromthebiggesthealthinsurershavesaidpubliclyatcongressionalhearingsandelsewherethattheybasedecisionsaboutmedicalnecessityand“experimental”treatmentssolelyonmedicalcriteria.Theyhavestatedthatthesedecisionsareinsulatedcompletelyfrompressuretoboostprofits.
YetformerseniordoctorsatbighealthinsurerssaidininterviewswithCAPthatCigna,Aetnaandmostoftheothertopcompaniesmadeanimportantchangeinwhotheirmedi-calstaffsreporttooverthepast10years.Companiesreassignedmedicaldirectors,thedoctorswhoapproveordenyclaimsformedicalreasons,toreporttoregionalbusinessexecutives.Theypreviouslyreportedonlytothecompanies’chiefmedicalofficer,whowasresponsibleforhiringandfiringdecisions,promotions,payraises,andbonusesformedicaldirectors.Aftertheswitch,thebusinessmanagers,whosemainresponsibilityistobolsterprofits,hadauthorityoverthesepayandincentivedecisionsforthemedicalstaff.
FormerCignaExecutiveWendellPottersaidthathavingmedicaldirectorsreporttobusi-nessmanagers“meanstheyarepartofateamthatisverymuchinvolvedinmakingsurethatthecompanyisprofitableatalllevels.”
Arthur“Abbie”Liebowitz,chiefmedicalofficeratAetnauntil2001,saidthatfinancialpressureswhenhewasthereledtothereassignmentofthecompany’sdoctors.Inaninterviewforthisreport,Liebowitzsaid,“TheconceptwasthatbusinessleadershadPandL[profitandloss]responsibilityfortheregion.ThebusinessguyssaidifIhaveresponsi-bilityforprofitsandlossesIhavetocontrolforthethingsthataccountformycosts.Thebiggestthingaffectingcostwasmedicaldeliverydecisions.”
Liebowitzsaidheopposedthechange.“Ifoughtuntiltheveryend,”hesaid.“Ididn’tthinkthatpeopleshouldbemakingmedicaldecisionsbasedonbusinessneeds.”
Companyspokesmendeniedthatthechangeaffectedmedicaldecisions.Aetnaspokes-manGhosesaidtherestructuringhashadnoeffectonthedecisionsthatdoctorsmake.“Medicalnecessitydecision[s]aremadeatAetnabasedonmedicalevidence,”hesaid.“Thereisnootherthingthatcomesintothatequation.”

7 Center for American Progress | Insurers’ Black Box
CignaspokesmanCurransaidthat,“allcliniciansareaccountabletothechiefmedicaloffi-cerfortheirclinicaldecisions.”Headdedthat“therearenofinancialincentivesforclini-cianstoapproveordeny”claims.AndaUnitedHealthcarespokesmansaidthecompany’smedicaldirectorsarefocusedonly“onsupportingourmembers’care.”
Rep.ElijahCummings(D-MD)pressedapanelofseniorexecutivesfromfiveofthebiggestfor-profithealthinsurersataHouseOversightandGovernmentReformSubcommitteeonDomesticPolicyhearingonSeptember17tosaywhethertheircom-paniesgavemedicaldirectorsandotheremployees’financialincentivestorejectclaims.Noneofthemmentionedthechangesinwhotheirmedicaldirectorsreportto,orthattheircompensationandpromotionisnowsetbybusinessexecutivesmainlyconcernedwithprofits,ratherthanthecompanies’chiefdoctors.
Alloftheexecutiveseitherflatlydeniedthatthereisanyfinancialincentiveforemployeestodenyclaims,orsaidthattothebestoftheirknowledgetheircompaniesgivenosuchinducements.CignaSeniorVicePresidentThomasRichardssaid,“AtCigna,therearenofinancialincentivesforourclinicianstodenycoverage.”AetnaSeniorVicePresidentPatriciaFarrellsaidthattoherknowledge,“wehaveabsolutelynoincentives,financialincentives,tiedtothatdecision-makingprocess.”
States do not require disclosure and face difficulties in regulation
CaliforniaandRhodeIslandaretheonlytwostatesthathaveanindependentdepart-ment—separatefromthestates’insurancedepartments—specificallytaskedwithregulatingmanagedcareorganizations.AndCaliforniaistheonlystatethatrequirescom-paniestofileclaimsdisclosuredata—RhodeIslanddoesnotcollectsuchdata,accordingtoastatespokeswoman.
Allotherstatesregulatehealthinsurersthroughtheirinsurancedepartments.KansasInsuranceCommissionerSandyPraeger,recentpastpresidentoftheNationalAssociationofInsuranceCommissionersandcurrentchairmanofitsHealthInsuranceandManagedCareCommittee,saidthattheissuehadn’tcomeupinrecentdecadesatNAIC’smeet-ingstodiscusspolicyissuesandproposemodellawsandstandardsforallstatestoadopt.Praegersaidshedoesn’tknowwhytheregulatorshaven’trequestedit,butsaidonefactormayberegulators’assumptionthatinsurerswouldputupafightratherthanturnovermoredata.“Theindustrydoesn’treadilygiveanythingup,”Praegersaid.
Giventhepotentialusefulnessofclaimsdenialdatainindicatingwhetherinsurersaretreatingcustomersfairly,itmayseemsurprisingthatregulatorshaven’taskedthecom-paniestoprovidethedata.Theapparentlackofinteresthighlightsalargerproblemwithinsuranceregulationthatwillbeofincreasingconcernifhealthreformlegislationgoesintoeffect:Nearlyallinsuranceindustryregulationislefttothestates.

8 Center for American Progress | Insurers’ Black Box
TheSupremeCourtruledin1869thatthesaleofinsurancepoliciesdidnotamounttointerstatecommerce,andthereforewasn’tsubjecttofederalauthority.2TheSupremeCourtreverseditsearlierdecisionin1944,aftertheriseofmanylargeinsurancecom-paniesthatsoldacrossstatelines,openingthedoortofederalregulation.3Butinsuranceexecutives,panickedthatthefederalgovernmentmightimposeharshercontrols,rushedtolobby,andin1945CongresspassedtheMcCarran-FergusonAct.Thislawbillpreservedstatecontrolofinsuranceregulationandisstillineffect.4
Moststateinsurancedepartmentsarechronicallyunderfundedandhobbledbythelocalinsurancelobby’sinfluenceoverstatelegislaturesandotherstateofficials.Andtheeco-nomicdownturnhasledtofurtherstaffreductionsatmanystateinsurancedepartments.What’smore,stateinsurancedepartmentshavetraditionallybeenconcernedalmostexclu-sivelywithsolvencyorensuringthatinsurersarefinanciallysoundanddon’tgobust.Onlyinrecentdecadeshaveregulatorsinmanystatesbegunfocusingonhowinsurers,includinghealthinsurers,treatcustomers.Buttheirregulatoryeffortstodatehavebeensmallandfitful,partlyduetostrongoppositionfromtheindustry.
Somesenators—angeredbyinsurers’tacticsinopposinghealthcarereformlegislation—arethreateningtorepealportionsoftheMcCarran-FergusonActthatexemptinsurersfromfederalantitrustlaws.Stateinsurancedepartmentsrelymainlyonperiodic“marketconductexaminations”ratherthanrequiringinsurerstoroutinelyturnoverdatarelatingtotheirpolicyholderobligations.Statessendexaminersintoacompanytoreviewrecordsandlookatcustomercomplaints,timelypaymentofclaims,marketing,andadvertising.
Yetstatesconductrelativelyfewsuchexams.Thereisnonationwidedataontheannualnumberofmarketconductexaminationsspecificallyofhealthinsurers.ButtheNationalAssociationofInsuranceCommissioner’s2008InsuranceDepartmentResourcesReportshowsthat25statesconducted10orfewermarketconductexamsofalltypesofinsurancecompaniesin2008.Severalstatesdidsay,however,thattheylookedatcertainconsumer-relatedissueswhenperformingregularfinancialexaminationsofinsurers.
Thefederalgovernmentdoesimposecertainrequirementsonhealthinsurersunderthe1996federalHealthInsurancePortabilityandAccountabilityAct,suchaslimitingtherestrictionsinsurerscanputoncoverageforpre-existingconditions.Butthefederalgovernmentleavesenforcementoftheserulesalmostentirelytothestates.AsGeorgetownUniversityHealthPolicyInstitute’sResearchProfessorKarenPollitztestifiedrecently,manystateinsurancedepartmentsoftenhavedifficultyenforcingHIPAArequirementsduetoother,conflictingstatelaws,suchaslawsthatallowforuptotwoyearsof“contest-ability”—thatis,enableinsurerstorescindapolicybasedonpre-existingconditions.5
HIPAAallowsthefederalgovernmenttoactifthestatesdon’tenforceitsrequirements.ButthedepartmentofHealthandHumanServices,whichhastheauthority,hassofarnotintervened.

9 Center for American Progress | Insurers’ Black Box
ThehealthreformmeasurescurrentlybeingconsideredbyCongresswouldimposesig-nificantnewresponsibilitiesonstateregulators.Itwillrequirethemtodrawupstandardsspellingoutmoredetailedguidelinesregardingwhatinformationinsurersarerequiredtogivetoconsumersabouttheircoverage.Regulatorswillhavetodraftandenforcenewlawsregulatinginsurancemarketingpractices.AndtheHousebillH.R.3200,America’sAffordableHealthChoicesActof2009,wouldrequirestepstodiscloseimportantnow-confidentialinformation,suchasinsurers’claimdenialrates.
Yetthependinglegislationdoesnotallocateanymoneytohelpcurrentlyunderfundedandunderstaffedinsurancedepartments.However,insurancedepartmentsinmanystatescontributelargeamountstostatesrevenuesbycollectinginsurerlicensingfeesandtaxes.Themoneygoesintothestates’generalcoffers,andstatelegislaturesappropriaterela-tivelysmallamountstoruntheinsurancedepartments.Federalandstatesgovernmentswillclearlyneedtodomoretoensurethatinsurancedepartmentshavetheresourcesandauthoritytheyneedtoproperlyoverseehealthinsurancecompanies.
Other data
Thereisnopubliclyavailablenationwidedatafromregulatorsorinsurersthemselvesontotalratesofclaimsdenials,butseveralinsurancecompanyspokesmenininterviewspointedtodatacontainedintheAmericanMedicalAssociation’s“NationalHealthInsurerReportCards”publishedin2008and2009.TheAMAreportcardsaremeanttorateinsur-ersandMedicare’sperformanceinseveralcategoriesimportanttodoctorsandconsum-ers.Thespokesmancontendedthatacolumnofnumbersinthereportsshowthatclaimsdenialratesactuallyareextremelysmall.
Acloselookatthereportedcardsshowsthatthecolumnofdatacitedbythecompanies—labeled“Percentageofclaimlinesdenied”—actuallyshowsonlyoneportionofthetotalclaimsdenied.Thefigureshows,forexample,thatUnitedHealthcare’sdenialratewas2.02percent,Cigna’s2.56percent,andAetna’s1.81percent.Thesepercentagesincludeonlyinstancesinwhichentireclaimsweredeniedforreasonssuchasthattheindividualwasn’tactuallycoveredbythecompany,orwhenaclaimformhadbeenfilledoutimproperly.Thesenumbersdonotincludeinstanceswherecompaniesdeniedselecttreatmentsandproceduresratherthantheentireclaim.
Interviewsandacloselookatexplanationsofthedatacontainedinappendicesshowedthatitisnecessarytoaddtogethertwoseparatesetsoffigurestocomeupwithanesti-mateofactualtotalclaimsdenials.TheAMAobtaineditsdataforthereportcardsfromSacramento,California-basedNationalHealthcareExchangeServices,aprivatecompanythatprovidessoftwaretodoctorsandhospitalstohelpthemcontestunderpaymentsandclaimsdenialsbyinsurers.Thecompanyuseditsowndatabasecontainingclaimspay-mentinformationprovidedtoitbydoctorsandhospitalsthatareitscustomers.Mark

10 Center for American Progress | Insurers’ Black Box
Rieger,thecompany’schiefexecutiveofficer,saidinaninterviewthattofindanestimateoftotaldenialratesitisnecessarytoaddthecolumncitedbythecompanyspokesmanwithanotherlabeled“claimsedits.”Thattechnicaltermreferstotheselectivedenialofreimbursementformultiplechargesonaclaim,suchasbyrefusingtoreimburseforonetreatmentbutpayingforothersperformedduringthesameofficevisit.
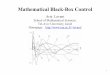
TotaldenialratesderivedbyaddingMetric11A,“disclosedandundisclosedclaimedits,”andMetric12,“Percentageofclaimlinesdenied.”
Thefiguresarestillsignificantlylowerthanthoseinthe30percentrangereportedbyseveraloftheCaliforniainsurers,butRiegersaidtheyshowrelativelyhighratesofdenialsandsignificantvariationsamongthecompanies—also,thedataisn’tcomprehensiveornationwide.ItisbasedonlyonasamplingofclaimssubmittedbydoctorsandhospitalstoinsurersduringFebruaryandMarch2009,anddoesnotincludeclaimssubmittedbypatients.Thedataincludesclaimsfrom29states,includingallofthemostpopulousstates.
Conclusion
Thereisnotacertainwaytotellwhetherthecommercialcompaniesaredenyingunfairlylargenumberofclaimstolimitlossesandboostprofitswithoutcomprehensivedataontheinsurers’ratesofclaimsdenials.Bigportionsofthedenialsareundoubtedlybeingkeptsecretforcompletelylegitimatereasonsasinsurersmaintain.Butthelimiteddatacurrentlyavailableraisesredflags,highlightingtheneedformuchwiderdisclosure.
ThedatareleasedinCaliforniashowswidevariationindenialratesfromcompanytocompany,andexposesthatsomecompaniesaredenying30percentormoreofallclaims.Thesefindingsshouldcausestatestobeginlookingcloselyatdenialrates,andexploringwhethercompaniesarecitingvalidreasonsfordenials.Evenifnationwidedenialpercent-agesturnouttobelowerthanthoseinCalifornia,suchastheroughly10percentdenialratesindicatedforsomebigcompaniesintheAMAdata,thatstillrepresentsmillionsofdeniedclaims.Stateswillalsoneedtolookatthecompanies’compensationstructurestoseeifthereisanyfinancialpressureonemployees,includingmedicaldirectors,toturndownclaims.
Ifthecurrentsystemofrelyingonstateregulationremainsineffect,thefederalgovern-mentorstatelegislatureswillhavetocomeupwithmoneytomakesurethattheinsurancedepartmentshaveadequateresources.Statelegislaturesinmanystatesalsowillhavetoshowmorewillingnesstopasslawsgivingtheinsurancedepartmentstheauthoritytheyneedtothoroughlyoverseetheinsurerstheyregulate.
American Medical Association claim denial estimates
Company Total denial rates (%)
Aetna 9.51
Anthem 9.34
CIGNA 9.06
Coventry 10.39
Humana 5.13
UHC 9.92
Medicare 5.4
Source: American Medical Association 2009 National Health Insurer Report Card, available at http://www.ama-assn.org/ama1/pub/upload/mm/368/2009-nhirc-long.pdf.

11 Center for American Progress | Insurers’ Black Box
Endnotes
1 Bynum v. Cigna Health care of N.C., Inc., 287 F.3d 305 (4th Cir. 2002).
2 Paul v. Virginia, 75 U.S. (8 Wall) 168 (1869).
3 United States v. South-Eastern Underwriters Association, 322 U.S. 533 (1944).
4 The McCarran-Ferguson Act, 15 U.S.C. § 1011.
5 Karen Pollitz, prepared statement for June 16, 2009 hearing before the House Energy and Commerce Committee’s Subcommittee on Oversight and Investigation, available at http://energycommerce.house.gov/Press_111/20090616/testimony_pollitz.pdf.

The Center for American Progress is a nonpartisan research and educational institute
dedicated to promoting a strong, just and free America that ensures opportunity
for all. We believe that Americans are bound together by a common commitment to
these values and we aspire to ensure that our national policies reflect these values.
We work to find progressive and pragmatic solutions to significant domestic and
international problems and develop policy proposals that foster a government that
is “of the people, by the people, and for the people.”
1333 H Street, NW, 10tH Floor, WaSHiNgtoN, DC 20005 • tel: 202-682-1611 • Fax: 202-682-1867 • WWW.ameriCaNprogreSS.org
Recommended