
Infection à Clostridium
Benoit Guery
Unité des Maladies Infectieuses CHRU - Faculté de Médecine
Lille
Remerciement à F Barbut pour quelques dias empruntées…..
ÉPIDÉMIOLOGIE
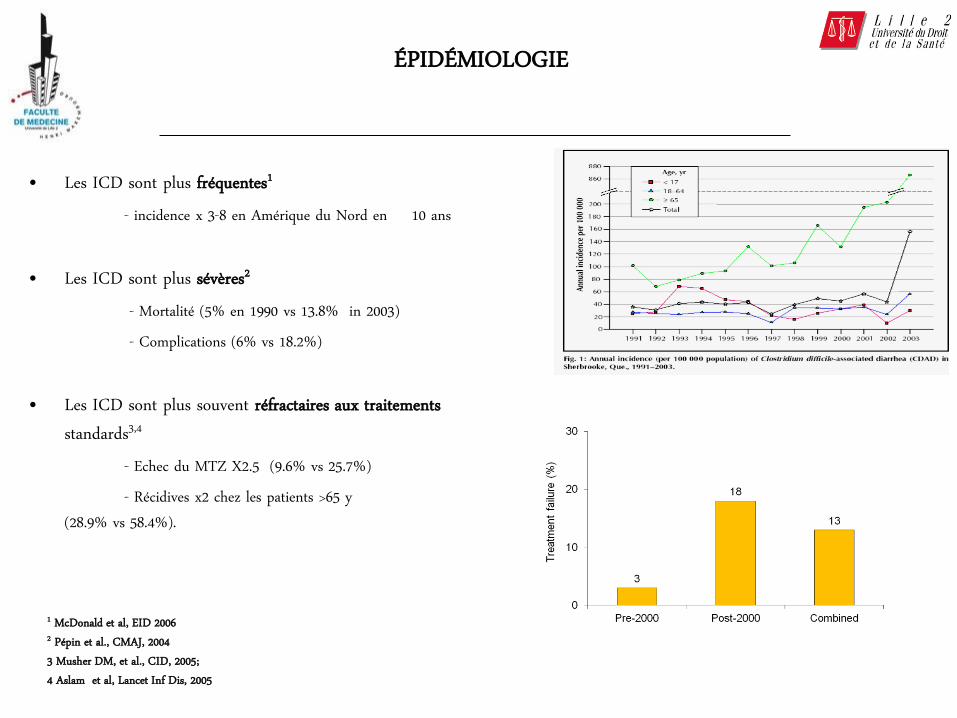
• Les ICD sont plus fréquentes1
- incidence x 3-8 en Amérique du Nord en 10 ans • Les ICD sont plus sévères2 - Mortalité (5% en 1990 vs 13.8% in 2003) - Complications (6% vs 18.2%) • Les ICD sont plus souvent réfractaires aux traitements
standards3,4 - Echec du MTZ X2.5 (9.6% vs 25.7%) - Récidives x2 chez les patients >65 y
(28.9% vs 58.4%).
1 McDonald et al, EID 2006 2 Pépin et al., CMAJ, 2004 3 Musher DM, et al., CID, 2005; 4 Aslam et al, Lancet Inf Dis, 2005

EMERGENCE D’UN CLONE EPIDEMIQUE
- Emergence d’un clone épidémique (NAP1/027/BI) - USA et Canada (2003) - Europe : 2004-2005 - Asie, Australie - Endémique aux US (50%), au Québec (80%) et UK (20%) mais rare avant 1990 (<0,3%) - Toujours présent et prédominant en 2015 (Europe :18.5%)
- Caractéristiques • Sensible au MTZ et à la VA/ Résistant aux FQ • Production accrue in vitro de toxines A et B (Warny M, Lancet 2005) • Toxine binaire + • Meilleure capacité à sporuler ? (Merrigan M., J. Bact 2010) • Meilleure translocation de la toxine B ? (Lanios JM, Plos Path 2010)

DISSÉMINATION MONDIALE DU CLONE 027/BI/NAP1
He, M., Nature Genetics 2013, 45, 109

INCIDENCE DES ICD
• L’incidence continue d’augmenter en Europe 1–4, 6-7 – Amélioration des techniques diagnostiques – Sensibilisation croissante des cliniciens – Diffusion du clone NAP1/027/BI en Europe de l’Est
6.4
7.3
1. Bauer et al Lancet 2011 2. Davies et al Lancet 2014 3. Barbut et al Presse med 2015
ECDIS EUCLID
106 ES
36 pays 482 ES
20 pays
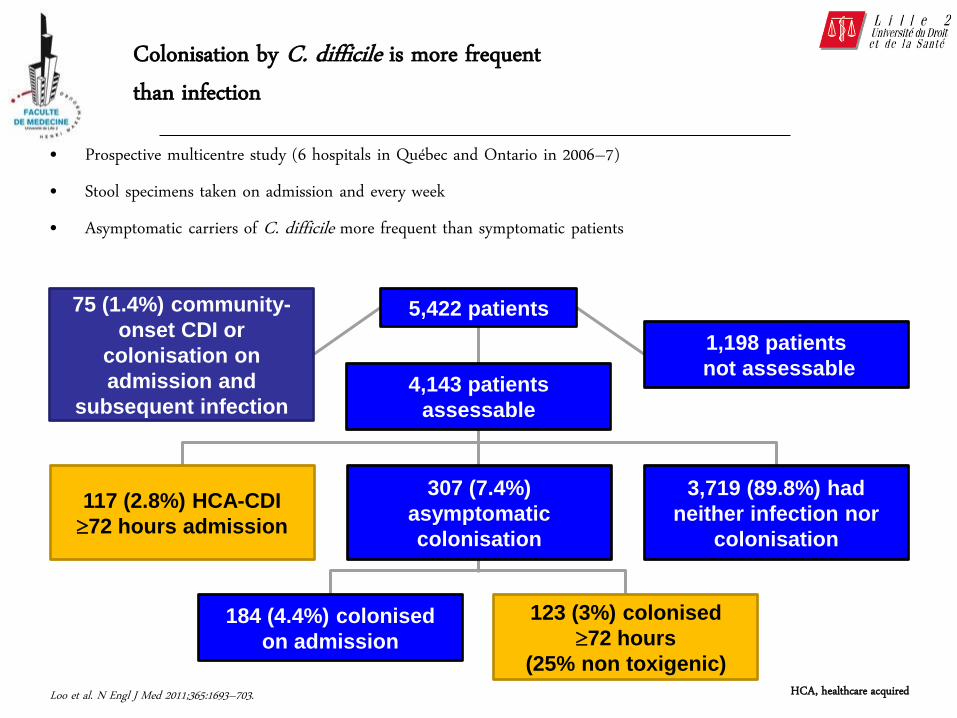
• Prospective multicentre study (6 hospitals in Québec and Ontario in 2006–7) • Stool specimens taken on admission and every week • Asymptomatic carriers of C. difficile more frequent than symptomatic patients
Loo et al. N Engl J Med 2011;365:1693–703.
307 (7.4%)
asymptomatic
colonisation
3,719 (89.8%) had
neither infection nor
colonisation
75 (1.4%) community-
onset CDI or
colonisation on
admission and
subsequent infection
117 (2.8%) HCA-CDI
72 hours admission
184 (4.4%) colonised
on admission
123 (3%) colonised
72 hours
(25% non toxigenic)
1,198 patients
not assessable 4,143 patients
assessable
5,422 patients
HCA, healthcare acquired
Colonisation by C. difficile is more frequent than infection

• Hôpital universitaire de 762 lits (Pittsburgh, US) • Juillet et novembre 2009
– Dépistage sélectif de 3006 patients vis-à-vis de C. difficile (314 patients positifs, 10.4 % positifs) – 124 ICD: 53 (43%) HA-CDI, 13 (10%) CO-CDI, 57 (46%) acquis dans d’autres établissements ou récidives
• Typage des souches par MLVA (méthode discriminante) • Origine des HA-CDI
– 22 avec génotype sans relation avec patient précédent – 16 avec génotype retrouvé chez porteurs asymptomatiques (29 % des cas) – 17 avec génotype de patients avec ICD ( 30% des cas)
• Une contamination environnementale des chambres de patients asymptomatiques ou symptomatiques peut expliquer la survenue d’ICD à distance (4/61)
• Résultats cohérents avec ceux de Walker et al. (Plos Med 2012) (MLST) et Eyre D. et al. (NEJM 2013) (WGS)
CID 2013, 57, 1094-102

TENDANCES ÉVOLUTIVES
• Emergence de nouveaux clones – 078/126 (formes sévères, communautaires, adultes jeunes)
• Profils de patients atypiques
– Patients jeunes sains (femmes en peripartum, enfants) – 24-54 % sans ATCD ATB
• Les ICD concernent le milieu vétérinaire
– Epidémies dans des élevages de porcelets, volailles, veaux … – Isolement de CD dans les viandes, légumes, coquillages…
• Plus fréquent aux US qu’en France • Recouvrement des génotypes humains/animaux/aliments
CDC, MMWR 2005
Gorrhuis at al., CID 2008
Gould , CID 2010
Songer, JG., EID 2009

• Durée de séjour1 : • Diagnostic principal : 5-13,6 jours (médiane 7 j) • Diagnostic associé : + 2,7-21,3 jours (médiane 7 j)
• Mortalité : • 0,6-1,5% pour les diarrhées simples2,3 • 30-50% si megacôlon ou perforation4
• Augmentation x2,5 taux de mortalité à J30 chez pts ICD vs contrôles sans diarrhée5
• Coût: • Surcoût : 9 024 € par séjour (étude ECODIFF6 )
1. Gabriel L., JHI 2014 2. Olson, ICHE, 1994 3. Miller, ICHE 2002 4. Morris, Am J Surgery, 1990 5. Hensgens et al CID 2013 6. Le Monnier et al., JHI 2015
IMPACT DES DIARRHÉES À C. DIFFICILE

Shen A. J Innate Immun 2012;4:149-58.
PATHOGÉNIE DES ICD
CDT : toxine binaire TcdA-TcdB : toxines A et B.

Two large toxins, toxin A and toxin B (TcdA and TcdB), are encoded on
the pathogenicity locus (PaLoc), which comprises five genes.
A third toxin, the binary toxin or CDT (Clostridium difficile transferase), is
encoded on a separate region of the chromosome (CdtLoc) and
comprises three genes.

Toxine binaire CDT
Activité actin ADP ribosyl transférase Désorganisation du cytosquelette
Redistribution des microtubules
Formation de protusions qui augmentent l’adhérence Schwan C et al. PlosPathogens, 2009
Produites par 0,5 à 5% des souches (027, 078 …)
Potentialiserait la toxicité de TcdA et TcdB Geric B et al.,J. Med. Microbiol. 2004 Barbut F et al. Inf Control Hosp epidemiol, 2007
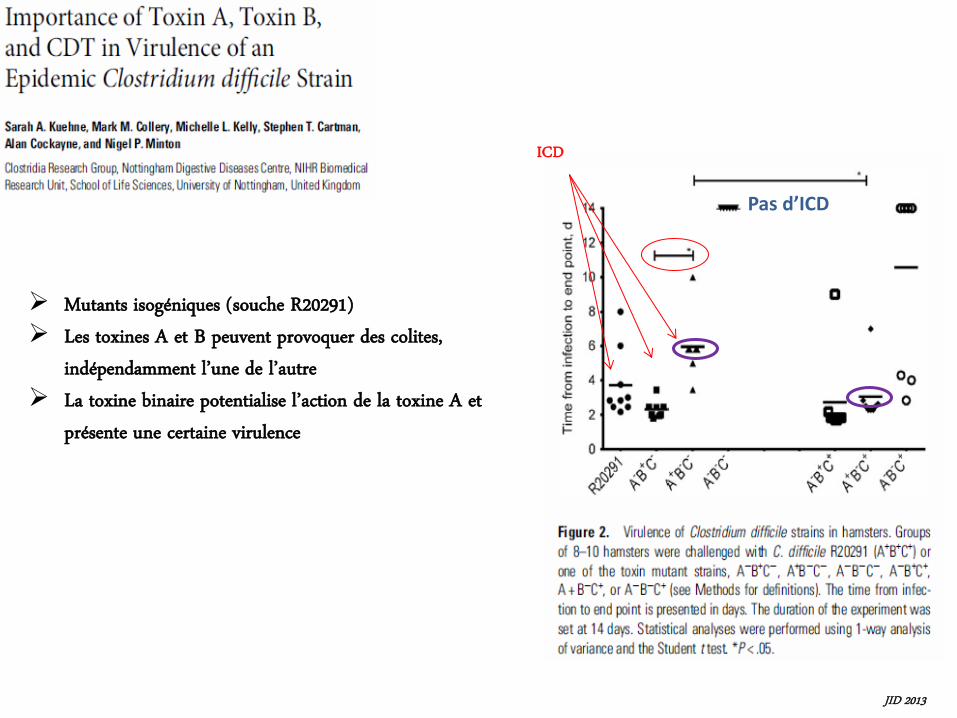
Mutants isogéniques (souche R20291) Les toxines A et B peuvent provoquer des colites,
indépendamment l’une de l’autre La toxine binaire potentialise l’action de la toxine A et
présente une certaine virulence
Pas d’ICD
ICD
JID 2013

PRÉSENTATIONS CLINIQUES
• Seules les souches toxinogènes sont pathogènes
• Formes cliniques
• > 95% CPM • 10-25% des diarrhées post ATB • 10 % diarrhées nosocomiales
• Complications – Mégacôlon toxique, perforation, choc septique (<10%) – Colectomies ~ 1% – Récidives (2 mois) : ~ 25%
Barbut F., et al. Hepato Gastro et Oncologie médicale 2013, 20, 111-122 Rupnik M, et al.. Nat Rev Microbiol. 2009 Jul;7(7):526-36

LES RÉCIDIVES d’ICD
• Nouvel épisode d’ICD dans les 8 semaines suivant un 1er épisode1
• 25% après un 1er épisode, 40% après une 1ère récidive
• Rechute ou réinfection2
• FDR récidives1,3,4 :
• Surcoût important5 : – Surcoût annuel des récidives 28,55 M €
1. Debast et al., CMI 2014 2. Barbut et al., JCM 2000 3. Denève et al. Int. J. Antimicrob. Agents 2009 4. Kyne et al, Lancet 2001 5. Le Monnier et al. JHI 2015
Kelly et al CMI
2012
Marqueurs Niveau de preuve Age> 65 ans A
Utilisation d’ATB pendant ou après le traitement de l’ICD
A
Comorbidités ou insuffisance rénale A
ATCD d’ICD A
Utilisation concomitante d’IPP B
Sévérité de l’infection initiale B
Niveau de preuve : A = fort B = modéré

FACTEURS DE RISQUE D’ICD
Patient
Exposition à C. difficile
Déséquilibre de flore
- Age > 65 ans - Co-morbidités (cancer, insuf. rénale, diabète..) - Immunodépression (hématologie, greffés..) - ATCD d’ICD - Faible taux d’Ac anti toxines
- Hospitalisations répétées, longs séjours - Voisin de chambre contaminé - Chambre précédemment occupée par un patient ICD+
- ATB < 3 mois - Chimiothérapie - IPP - Lavements, laxatifs…
McFarland et al, NEJM1999; Loo V., NEJM 2012

63 patients with nosocomial C difficile diarrhoea.
19 patients died (30%).
Of the 44 who survived, 22 had recurrent C difficile
diarrhoea
A serum antibody response to toxin A, during an initial episode of C difficile diarrhoea, is
associated with protection against recurrence.

DIAGNOSTIC DES ICD
• Le diagnostic doit être rapide et fiable – Prise en charge du patient
• Traiter rapidement les ICD • Éviter les traitements empiriques
– Prévention de la transmission nosocomiale • Isolement contact
– Précision des données épidémiologiques
• Critères de choix pour une méthode diagnostique: – Spécificité – Sensibilité – Rapide – Peu coûteux – Simple
Aucune des méthodes actuelles ne satisfait tous ces critères

DIAGNOSTIC MICROBIOLOGIQUE
• Une ICD est définie par “(i) un tableau clinique compatible avec une ICD et la mise en évidence microbiologique d’un C. difficile producteur de toxines dans les selles en l’absence d’autre cause évidente de diarrhée ou (ii) une colite pseudomembraneuse”
• Recommandations générales – Selles diarrhéiques (Echelle de Bristol : 5, 6, 7) – Recherche systématique en cas de diarrhée associée aux soins – Pas de répétition de tests – Coproculture de contrôle en fin de traitement non recommandée
CMI, 2009

LE SOUS-DIAGNOSTIC DES ICD EST MAJEUR EN FRANCE
• Etude EUCLID 2012/13 : prévalence de C. difficile dans toutes les selles diarrhéiques envoyées au laboratoire, indépendamment de la demande du clinicien
• Analyse de 651 selles (70 ES) par le CNR • 9.7% des échantillons positifs à C. difficile
toxinogène
• 55.6% des ICD NON diagnostiquées par l’ES
Barbut F. Presse médicale 2015 Apr;44(4 Pt 1):e75-83

MÉTHODES DIAGNOSTIQUES DES ICD
Test de cytotoxicité des selles (CTA)
Méthodes moléculaire (tcdA, tcdB)
EIA Toxines A+B
Sérologie
Mise en évidence des toxines libres
Culture Toxigénique
(CT)
EIA, enzyme immunoassay; GDH, glutamate dehydrogenase,,NAAT: nucleic acid amplification tests
Mise en évidence d’une souche toxinogène

Toxine libre Souche toxinogène
DIAGNOSTIC DES ICD
Très spécifique, moins sensible
signe la maladie
Très sensible, moins spécifique
Colonisation ou infection?
CTA + chez seulement 48% de 56 patients ayant une CPM
(Johal et al. Gut 2004;53:673–7)
Portage asymptomatique fréquent de C. difficile à l’hôpital (7.4%)
(Loo V., NEJM, N Engl J Med 2011;365:1693–703)
Diagnostic des ICD 2 cibles différentes

Recommendations de l’ESCMID, 2015
− +
Test de dépistage sensible NAAT (ou GDH EIA)
Test spécifique Toxines A/B
NAAT ou TC (si le test de dépistage est la GDH)
+ −
ICD Evaluation clinique
Une ICD ou un portage de souche tox. est possible
−/− +/− +/+
ICD
GDH-toxine A/B
+ −
NAAT Absence d’ICD
Evaluation clinique Une ICD ou un portage de souche tox.
est possible
Absence d’ICD
Crobach M., et al. , Manuscript in preparation, ECCMID 2015
Absence d’ICD
−/+
Refaire le test


Fidaxomicine
Les molécules disponibles

Traitement médical
Vancomycine per os
125 mgx4/j
Métronidazole per os (IV possible)
500 mgx3/j
Fidaxomicine (depuis fin 2012)
200 mgx2/j Spectre Moyen Large Etroit
Absorption Non Oui Non
Effets secondaires Rares Neuropathies périphériques, effet antabuse, goût métallique
Rares
Concentrations fécales (/g de selles)
3100 µg/g 0.4-14.9 µg/g 1433.3 µg/g
CMI90 0.75-2 µg/ml 0.2-2 µg/ml 0.125 µg/ml
Souches résistantes 3% souches espagnoles (CMI 4-16 µg/ml)
6.3% CMI >16 µg/ml (hétérorésistance)
Très rares
Impact clinique Non ??? -
Coût (10 jours) $ 61 $ 5 1300 €

• Métronidazole
– 6-15% d’excrétion dans les
selles
– Concentration proportionnelle
à la lésion
– Arrêt au dela du 14ème jour ou
si les selles sont formées
9.3 vs 1.2
n=10

Fidaxomicine
Nouvelle classe ATB : les macrocycliques Inhibition de la RNA polymérase
Absorption orale faible action topique Spectre étroit
C. difficile C. perfringens CG+ anaérobies
activité modérée sur CG+ aérobies
Activité bactéricide avec EPA de 10 h
Fréquence de mutation faible < 2. 108
Action sur la sporulation vs MTZ et vanco Tolérance : RAS de significatif
Sullivan KM Ann Pharmacother 2010; 44: 352

Thérapeutique
• ICD non grave
• Formes graves
• 1ere récidives
• Récidives multiples


Thérapeutique
• ICD non grave
• Formes graves
• 1ere récidives
• Récidives multiples

SÉVÉRITÉ DES ICD
IDSA/SHEA (Cohen et al., 2010)
ESCMID (traitement) (Debast et al., 2014)
ACG (Surawicz et al., 2013)
ICD de sévérité moyenne à modérée Leucocytes <15000/mm3 et Créatinine<1.5 x valeur de base ICD sévère Leucocytes >15000/mm3 ou Créatinine >1.5 x valeur de base ICD compliquée - hypotension, choc, ileus, ou mégacolon
Critères de sévérité (au moins un parmi les suivants): - Fièvre >38°5 C - Frissons - Instabilité hémodynamique (incluant le choc septique) - Signes de péritonite - Signes d’iléus - Leucocytose >15000/mm3 - Augmentation créatinine > 50% la valeur initiale -Lactate 5 mmole/L -Albuminémie < 30 g/l - Pseudomembranes à l’endoscopie - Distension colique >6 cm (radiologie) - Epaississement paroi colique (radiologie)
- Densité de la graisse péricolique - Ascite sans autre
explication
Critères de sévérité - Albuminémie<3g/dl + - Leucocytes> 15,000 mm3
ou - Douleurs abdominales

From October 1994 through June 2002, - 172 patients - oral metronidazole (250 mg 4 times per day) - oral vancomycin (125 mg 4 times per day) for 10 days


• 2 études multicentriques, prospectives randomisées double aveugle (2005-2007)
• 289 pts MTZ 375 mgx4/j • 266 pts Va 125 mgx4/j
• Suivi pendant 10 jours
• Guérison : résolution des symptômes
• Définition de la sévérité: nb de selles/j, GB, douleurs
abdominales
Johnson et al. CID 2014, 59(3):345-54
P=0.059

Thérapeutique
• ICD non grave
• Formes graves
• 1ere récidives
• Récidives multiples

Fidaxomicine (200 mg/12 h) vs vanco (125 mg/6 h) Traitement de 10 j Sujets > 16 ans
Exclusion : pronostic vital engagé leucocytes > 30 000/mm3
T > 40° C, choc septique, déshydratation +++
mégacolon toxique
Critères d’évaluation : principal : guérison en fin de traitement secondaire : récurrence et taux global de guérison à 25 j post traitement
Total de 629 patients inclus, 548 (87.1%) évalués en analyse per-protocole



Of 535 patients enrolled, 270 were assigned fidaxomicin and 265 vancomycin.
After 26 patients were excluded, 509 were included in the modified intention-to-treat (mITT)
population


Two phase 3 randomized, double-blind trials were conducted at 154 sites in the United
States, Canada, and Europe


Thérapeutique
• ICD non grave
• Formes graves
• 1ere récidives
• Récidives multiples

Récidive
• Récidive : survenue d’un épisode d’ICD au cours des 8 semaines suivant le début d’un précédent épisode. 25-30%.
• Les récidives sont dites multiples lorsque le patient développe plus d’une récidive.
Clin Microbiol Infect 2012; 18: 21–27
La récidive n’est pas en relation avec un problème de résistance aux ATB.

Marqueurs pronostiques pouvant être utilisés pour la détermination du risque de récidive d’une ICD
A : Recommandation FORTE en faveur de l’utilisation B : Recommandation MODEREE
Récidive



Traitement chirurgical
• Retrospective observational cohort study – 165 cases of CDAD that required ICU admission or
prolongation of ICU stay
– between January 2003 and June 2005 in 2 tertiary care hospitals of Quebec
• Eighty-seven (53%) cases resulted in death within 30 days of ICU admission
• Colectomy seemed more beneficial in patients – aged 65 years or more
– immunocompetent
– leukocytosis ≥20 × 109/L or lactate between 2.2 and 4.9 mmol/L
Lamontagne et al, Annals of Surgery, 2007


Alternative à la colectomie ?
Iléostomie sur baguette + vanco antérograde
Neal Ann Surg 2011

Alternative à la colectomie ?
Iléostomie sur baguette + lavages vanco antérograde
Neal Ann Surg 2011


Thérapeutique

TRAITEMENTS DES ICD : PERSPECTIVES (Essais enregistrés au niveau du US Institute of Health)
Laboratoires Nom Objectifs Phase de développement
MSD mAB anti A et B 2 Prévention récidive Phase III
Acambis, Sanofi Aventis
Vaccin Prévention primaire Phase III
Actelion Cadazolid Traitement ICD Phase III
Cubist Pharmaceuticals
CB183,315 surotomycine
Traitement ICD Phase III
ViroPharma VP20621 1 Prévention récidive Phase II
https://clinicaltrials.gov/ 1 Gerding DN, JAMA. 2015 May 5;313(17):1719-27. doi: 10.1001/jama.2015.3725. 2 Lowy et al., NEJM 2010, 362, 197

The antibodies were administered together as a single infusion, each at a dose
of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile
infection who were receiving either metronidazole or vancomycin.


The combined administration of CDA1 and CDB1 human monoclonal
antibodies in addition to antibiotics significantly reduced the recurrence of C.
difficile infection.

Monoclonal antibodies against toxins
• Humanized Mab anti-C. difficile toxins A et B de (MSD) – Anti toxin A (ACTO or MK3415), anti-toxin B (BEZLO MK 6072)
• Recognize the binding site (C-terminal) • 2 Phase 3 randomized double-blind clinical trials versus placebo (Modify I and II) • Inclusions : patient with CDI • Design
Primary endpoint : recurrent CDI in the following 3 months. Secondary endpoint : rate of global cure, sub-group analysis
Diagnosis of CDI SOC
Mab
Placebo
MODIFY II BEZ (MK 6072)
ACT+BEZ (MK 3415 A)
MODIFY I ACT (MK3415) BEZ (MK 6072)
ACT + BEZ
Wilcox M, ICAAC 2015; Gerding D., ICAAC 2015

MODIFY I (America) (M. Wilcox, Leeds, UK, ICAAC 2015)
1452 patients (median age 65 y., 57% female) from 19 pays Relapse rates: ACT+BEZ (15.9%, p<0.0001) BEZ alone (17.4%, p=0003) Global cure ACT + BEZ (58.7%, p=0.16) BEZ alone (60.1, p=0.09)

Non toxigenic C. difficile strain
• Strain VP20621;NTCD-M3 • Phase II randomised double blind clinical trial versus placebo • 173 patients with 1st episode or relapse of CDI and treated by VA or MZ • 4 arms
• 104 spores for 7 j • 107 spores for 7 j • 107 spores for 14 j • Placebo
• Primary endpoint : safety • Secondary endpoint : - colonisation rate after 6 weeks = 63-71% - rate of recurrences
0%
5%
10%
15%
20%
25%
30%
35%
NTCD Placebo colonized NTCD NTCDnon colonized
Recurrence Reccurences
Gerding D, JAMA.2015;313(17):1719-172
p<.001 p=0.06

Vaccine (toxoids A and B)
• Anatoxins A et B (Acambis, Sanofi Aventis): ACAM-CDIFF™
• Phase II clinical (US-UK)(NCT00772343 )
▫ Immunogenicity and safety
• Double blind randomized clinical study vs placebo ▫ Inclusion : 1er episode of CDI (in combination of a SOC)
▫ End-point : rate of recurrence • Phase III clinical trial on going • End point : CDI prevention in patients at high risk of CDI

La transplantation … vue par l’infectiologue…

4,788 specimens from 242 screened and phenotyped adults (129 males, 113 females)


Microbiota

Proc Natl Acad Sci USA 2011
Ampicillin (1 g/L), vancomycin (500 mg/L), neomycin sulfate (1 g/L), and
metronidazole (1 g/L) in drinking water for 4 wk before PR8 virus infection (10 pfu
per mouse).

• “Molasses flies” preferred to mate with other molasses flies and “starch flies” preferred to mate with other starch flies
• Antibiotic treatment abolished mating preference, suggesting that the fly microbiota was responsible for the phenomenon.
• Analytical data suggest that symbiotic bacteria can influence mating preference by changing the levels of cuticular hydrocarbon sex pheromones


Compared with those from control subjects and patients with an initial episode,
the fecal communities in patients with recurrent CDAD were highly variable in
bacterial composition and were characterized by markedly decreased
diversity.
The 16S sequences of all
patients in each group
were pooled
(4) (3) (3)

Almost poetry….
« Re-establish the balance of nature… »
Eiseman 1958




Debast SB, et al. Clin Microbiol Infect 2014;20(Suppl 2):1–26.

• Study Population
– >18 years of age
– Relapse of C. difficile infection after at least one course of
adequate antibiotic therapy
• C. difficile infection was defined as
– diarrhea (≥3 loose or watery stools per day for at least 2
consecutive days or ≥8 loose stools in 48 hours) and
– a positive stool test for C. difficile toxin.

• Groups
– Vancomycin followed by bowel lavage and the infusion of a
suspension of donor feces through a nasoduodenal tube
the next day
– Vancomycin regimen
– Vancomycin regimen with bowel lavage on day 4 or 5.
• Second infusion with feces from a different donor if
recurrence.
• Patients in whom antibiotic therapy failed were
offered treatment with donor feces off protocol.



Open-label, randomised clinical trial o FMT: short regimen of vancomycin (125 mg four times a
day for 3 days), followed by one or more infusions of faeces via colonoscopy
o Vancomycin: vancomycin 125 mg four times daily for 10 days, followed by 125–500 mg/day every 2–3 days for at least 3 weeks
The primary end point was the resolution of diarrhoea related to C. difficile infection 10 weeks after the end of treatments.

The study was stopped after a 1-year interim analysis
1st: 13/20 (65%) 2: 4 3: 1 4: 1

J Clin Gastroenterol. 2010 Sep 44(8):551-61.
• Fecal samples were collected from 10 patients undergoing fecal bacteriotherapy
• Bacterial populations in patient fecal samples were followed from pretreatment to 24 weeks post-initial infusion
• At intervals of 4, 8, and 24 weeks after the procedure, the bacterial populations in the patients' fecal samples consisted predominantly of bacteria derived from the healthy donor samples.
• This study demonstrates a durable beneficial change in the patients' bacterial populations of the colon to represent those of the healthy donor's microbiota.



• A multicenter long-term follow-up study was
performed on the use of FMT in hospitalized pts with
severe or complicated CDI.
• CDI was defined
– as severe in the presence of abdominal tenderness, albumin
< 3.0 g/dL or WBC >15,000 cells/μL and
– as complicated if there was admission to the intensive care
unit (as a consequence of CDI); hypotension with or without
the use of vasopressors; change in mental status;
WBC>35,000 cells/μL or <2,000 cells/μL; serum lactate
levels ≥ 2.2 mmol/L; end-organ failure; fever ≥ 38.5°C; ileus
or significant abdominal tenderness.
• 13 eligible pts identified.
Gastroenterology 2013;144: S-185.

• All pts were hospitalized at the time of FMT and diagnosed with severe (84%) or complicated CDI (92%).
• After FMT, diarrhea resolved in 9 pts (75%) within 1-7 days (mean: 4.5 days) and improved in the remaining 3 pts (25%).
• Primary cure rate was 84%.
• Secondary cure rate was 92%.
• Late CDI recurrence (≥ 90 days) after FMT was seen in 1 of 13 pts (8%) in association with antibiotic treatment of diverticulitis.
• FMT is a successful treatment option in pts with severe or complicated CDI.
Gastroenterology 2013;144: S-185.

A 74-year-old man with diabetes, coronary artery disease, and thyroid cancer was transferred from another hospital to our hospital.
3 FMT
Discharged on day 29
Initial Follow up

Case reports

75 adult and 5 pediatric patients treated with FMT for recurrent (55
%), refractory (11 %), and severe and/or overlap of
recurrent/refractory and severe CDI (34 %)
Reasons for IC included
o HIV/AIDS (3)
o solid organ transplant (19)
o oncologic condition (7)
o immunosuppressive therapy for inflammatory bowel disease
(36)
o other medical conditions/medications (15)
The overall cure rate was 89 %
Twelve (15 %) had any SAE within 12 weeks post FMT, of which 10
were hospitalizations and 2 death (1 related)

Adverse events
• Amsterdam 200 fecal transplantation procedures, Sydney more than 3000 without any serious adverse events – diarrhea on the day of infusion,
– a small percentage report belching and/or abdominal cramping or constipation.
• In another case report, nasoduodenal FMT for Crohn’s disease resulted in – transient adverse effects, including fever and
abdominal tenderness in 3 of 4 patients.
• Long-term follow-up studies have found that FMT is relatively free of adverse effects
Am J Gastroenterol 2012;107:1079–1087


OFID, 2015



Let’s do it!

Legal issues…
• Microbiota transplantation=Drug
– Under the pharmacist’s responsability
• Authorization for clinical trials
• Screening of the donors
March 2014

Perfect donor
• 18-65 yo
• BMI<30
• No chronic disease
• No current treatment
• No antibiotics within the last 3 months
• No foreign travel within the last 3 months
• No residency in tropical areas
• No admission in foreign hospitals within the last 12 months
• No diarrhea within the last 3 months
• No typhoid
• Normal aspect of the feces
• Negative tests for infectious pathogens
• ……

Screening
Blood Feces
Treponema pallidum C difficile
L monoctygenes
V cholerae/parahemolyticus
Salmonella
Shigella
MDR pathogens
HIV
HTLV
Hepatitis A B C E
CMV/EBV
Adenovirus
Astrovirus
Cacivirus
Picornavirus
Rotavirus
S stercoralis
T gondii
Trichinella sp
S stercoralis
Cryptosporidium sp
Cyclospora sp
E histolytica
G intestinalis
Isospora sp
Microsporidies
Bacte
ria
V
iru
s
Para
sit
es

« A good movie is better than 25 lousy slides » (And time is running and I’m probably already
late)

This movie will not candidate for the oscars
Oscar 2015 « meilleure transplanteuse » T Galpérine


Patients were randomly allocated to receive frozen (n = 114) or fresh (n = 118) FMT via enema.
The use of frozen compared with fresh FMT did not result in worse proportion of clinical resolution of diarrhea.
Given the potential advantages of providing frozen FMT, its use is a reasonable option in this setting.

Open-label, single-group, preliminary
feasibility study conducted at
Massachusetts General Hospital, Boston
Twenty patients with
o at least 3 episodes of mild to
moderate C difficile infection
o failure of a 6- to 8-week taper with
vancomycin or at least 2 episodes of
severe C difficile infection requiring
hospitalization
Patients received 15 capsules on 2
consecutive days and were followed up
for symptom resolution and adverse
events for up to 6 months



Bacteria were purified, concentrated, cryopreserved and
formulated into multi-layered capsules
Thirteen women and six men with recurrent CDI were provided
with microbiota transfer with orally
administered capsules
o Thirteen individuals responded to a single course
o Four patients were cured after a second course
o 2 failures.
The cumulative clinical cure rate of 89%

Stool substitute preparation, made from purified intestinal
bacterial cultures derived from a single healthy donor, to treat
recurrent C. difficile infection
Two patients who had failed at least three courses of
metronidazole or vancomycin underwent colonoscopy and the mixture
was infused throughout the right and mid colon.


Recommended

















