!Seminario de Fisiología Renal
MECANISMOS DE TRANSPORTE TUBULAR
Dr. Ernesto Castro Aguilar Julio 2014

TRANSPORTE EPITELIAL
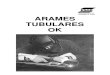
Filtrado glomerular sufre una serie de modificaciones antes de convertirse en orina
Reabsorción y secreción de solutos y fluidos

TRANSPORTE EPITELIAL

TRANSPORTE TUBULAR
Propiedades de membrana luminal deben ser diferentes a membrana basolateral.
Distribución asimétrica de proteínas transportadoras.
Transporte transcelular y paracelular (limitado por uniones estrechas)

TRANSPORTE PASIVO
Difusión simple: gradiente electroquímico. No requiere energía
Difusión facilitada: interacción de molécula o ión con transportador de membrana que favorece paso por membrana bilipídica.
Difusión por canal: favorece paso a una tasa mayor.

REABSORCIÓN
Movimiento de solutos o agua desde lúmen tubular hacia la sangre
Importante para manejo de Na+, Cl-, H2O, bicarbonato, glucosa, aminoácidos , proteínas, fosfatos, Ca2+, Mg2+, urea, ácido úrico y otras moléculas

SECRECIÓN
Movimiento de solutos desde la sangre o intersticio celular hacia el lúmen tubular.
Manejo de H+, K+, amonio (NH4+) y ácidos y bases orgánicas.

TRANSPORTE ACTIVO
Energía es requerida para transportar iones contra gradiente electroquímico.
Energía derivada de metabolismo celular
Mecanismo más importante es el de la bomba Na-K.
Confinada a membrana basolateral.
Energía de hidrólisis de ATP.


NA+-K+-ATPASA
Clave para el funcionamiento de mecanismos de transporte pasivo.
Mantiene concentración intracelular de sodio (10-20 mmol/L) y de potasio (150mmol/L)
Necesario para funcionamiento de cotransportadores, antiportadores.

TÚBULO PROXIMAL
Adaptado para reabsorción en “masa”.
Células con borde en cepillo en superficie apical
Membrana basolateral con pliegues que también aumentan superficie.
Ricas en mitocondrias y vacuolas lisosomales
Pocas uniones intercelulares


20 S E C T I O N I Essential Renal Anatomy and Physiology
Figure 2.7 Major transport mechanisms along the nephron. Major transport proteins for solutes in the apical and basolateral membranes of tubular cells in specific regions of the nephron. Stoichiometry is not indicated; it is not 1:1 in all cases. Red circles represent primary active transport; white circles represent carrier-mediated transport (secondary active); cylinders represent ion channels. In the proximal convoluted tubule (PCT), Na+ enters the cell through a Na+-H+ exchanger and a series of cotransporters; in the distal convoluted tubule (DCT), Na+ enters the cell through the thiazide-sensitive Na+-Cl− cotransporter; and in the principal cells of the cortical collecting duct (CCD), Na+ enters through a channel (ENaC). In all cases, Na+ is extruded from the cells through the basolateral Na+,K+-ATPase. Transporters in the thick ascending limb of Henle are dealt with separately (see Fig. 2.12).
!
Major Transport Mechanisms Along the Nephron
Na+
Lumen Interstitium
Cl−
Na+
Ca2+
Na+
K+
K+
Ca2+Ca2+
Lumen
Principal cells
Interstitium
Na+
K+
Glucose
Amino acids
Na+
Na+
HCO3−
K+
K+
Cl−
K+
Cl−
Lumen Interstitium
Intercalated cells
AlphaPCT
Beta
H+
H+
K+
HCO3−
Cl−
H+
HCO3−
Cl−
Cl−
Cl−
Na+
K+
K+
Na+
GlucoseNa+
Amino acidsNa+
PhosphateNa+
CitrateCl−
Formate/Oxalate
Na+
H+
Cl−
DCT
same property, so if the load to the loop of Henle or to the distal tubule is increased, some of the excess is mopped up. This is part of the reason that diuretics acting on the proximal tubule are relatively ineffective compared with those acting farther along the nephron; with the latter, there is less scope for buffering of their effects downstream. It is also the reason that combining two diuretics acting at different nephron sites causes a more striking diuresis and natriuresis.
The mechanism of glomerulotubular balance is not fully understood. As far as the proximal tubule is concerned, physical factors operating across peritubular capillary walls may be
involved. Glomerular filtration of essentially protein-free fluid means that the plasma leaving the glomeruli in efferent arterioles and supplying the peritubular capillaries has a relatively high oncotic pressure, which favors uptake of fluid reabsorbed from the proximal tubules. If GFR were reduced in the absence of a change in RPF, peritubular capillary oncotic pressure would also be reduced and the tendency to take up fluid reabsorbed from the proximal tubule diminished. It is thought that some of this fluid might leak back through the leaky tight junctions, reducing net reabsorption (Fig. 2.11). However, this mechanism could work only if GFR changed in the absence of a corresponding change in

TUBULO PROXIMAL
Responsable de reabsorción de Na+, K+, Cl- y HCO3-.
Reabsorción prácticamente completa de glucosa, aminoácidos y proteínas de bajo peso molecular (b-microglobulinas, proteína ligadora de retinol).
Reabsorción 60% calcio, 80% fosfato y 50% urea

TÚBULO PROXIMAL
Altamente permeable a agua (no hay generación de gradiente osmótico)
S2 y S3: secreción de ácidos y bases orgánicas débiles (diuréticos y PAH).

ASA DE HENLE
Conformada por:
Pars recta de TP (asa descendente gruesa)
Asas delgadas descendente y ascedente (presente en nefronas con asas largas)
Asa gruesa ascendente
Mácula densa
Responsable de reabsorción mayor de Mg2+ y concentración o dilución de orina.


C H A P T E R 2 Renal Physiology 23
descending limb of superficial nephrons is relatively impermeable to water.10) Both the thin ascending limb (found only in deep nephrons) and the TAL are essentially impermeable to water; however, Na+ is reabsorbed—passively in the thin ascending limb but actively in the TAL. Active Na+ reabsorption in the TAL is again driven by the basolateral sodium pump, which maintains a low intracellular Na+ concentration, allowing Na+ entry from the lumen through the Na+-2Cl−-K+ cotransporter (NKCC-2) and, to a much lesser extent, the Na+-H+ exchanger (Fig. 2.12). The apical NKCC-2 is unique to this nephron segment and is the site of action of loop diuretics like furosemide and bumetanide. Na+ exits the cell through the sodium pump, and Cl− and K+ exit through basolateral ion channels and a K+-Cl− cotransporter. K+ also re-enters the lumen (recycles) through apical membrane potassium channels. Re-entry of K+ into the tubular lumen is necessary for normal operation of the Na+-2Cl−-K+ cotransporter, presumably because the availability of K+ is a limiting factor for the transporter (the K+ concentration in tubular fluid being much lower than that of Na+ and Cl−). K+ recycling is also partly respon-sible for generating the lumen-positive potential difference found in this segment. This potential difference drives additional Na+ reabsorption through the paracellular pathway; for each Na+ reabsorbed transcellularly, another one is reabsorbed paracellu-larly (see Fig. 2.12).11 Other cations (K+, Ca2+, Mg2+) are also reabsorbed by this route. The reabsorption of NaCl along the TAL in the absence of significant water reabsorption means that the tubular fluid leaving this segment is hypotonic; hence the name diluting segment.
The U-shaped, countercurrent arrangement of the loop of Henle, the differences in permeability of the descending and ascending limbs to Na+ and water, and active Na+ reabsorption in the TAL are the basis of countercurrent multiplication and gen-eration of the medullary osmotic gradient (Fig. 2.13). Fluid
Figure 2.12 Transport mechanisms in the thick ascending limb of Henle. The major cellular entry mechanism is the Na+-K+-2Cl− cotrans-porter. The transepithelial potential difference drives paracellular trans-port of Na+, K+, Ca2+, and Mg2+.
Transport Mechanisms inthe Thick Ascending Limb
Lumen Cells of thick ascending limb Interstitial fluid
K+K+
K+
Na+
Na+
Na+
Na+
K+
Ca2+
Mg2+
H+
K+
K+
Cl−
Cl−
2Cl−
Paracellulardiffusion
Lumen-positivepotential difference
+
Figure 2.13 Countercurrent multiplication by the loop of Henle. The nephron drawn represents a deep (long-looped) nephron. Figures represent approximate osmolali-ties (mOsm/kg). Osmotic equilibration occurs in the thin descending limb, whereas NaCl is reabsorbed in the water-impermeable ascending limb; hypotonic fluid is delivered to the distal tubule. In the absence of vasopressin, this fluid remains hypotonic during its passage through the distal tubule and collecting duct, despite the large osmotic gradi-ent favoring water reabsorption. A large volume of dilute urine is therefore formed. During maximal vasopressin secretion, water is reabsorbed down the osmotic gradient, so that tubular fluid becomes isotonic in the cortical collect-ing duct and hypertonic in the medullary collecting duct. A small volume of concentrated urine is formed.
Countercurrent Multiplication
Cortex
Outermedulla
Innermedulla
Papilla 1200
900
600
290
1200
900
600
290
700
400
100
1200
900
600
290
NaCl NaCl NaCl
NaClNaCl
NaCl
H2O
H2O
H2O
NaCl
H2O
outer and inner medulla, whereas those of deep nephrons (long-looped nephrons) penetrate the inner medulla to varying degrees. The anatomic loops of Henle reabsorb approximately 40% of filtered Na+ (mostly in the pars recta and TAL) and approximately 25% of filtered water (in the pars recta and in the thin descending limbs of deep nephrons). (Recent evidence suggests that the thin

TÚBULO DISTAL
Conformado por: túbulo contorneado distal, túbulo conector y ducto colector
Conducto colector cortical: 2 células
Principales : reabsorción de Na+ y secreción de K+.
ENaC: genera gradiente eléctrico
Intercaladas: secreción de H+ (alfa) o bicarbonato (beta)


TÚBULO DISTAL
Ducto colector medular
Pérdida de células intercaladas
Modificación de células principales: no secretan K+ en esta porción.

20 S E C T I O N I Essential Renal Anatomy and Physiology
Figure 2.7 Major transport mechanisms along the nephron. Major transport proteins for solutes in the apical and basolateral membranes of tubular cells in specific regions of the nephron. Stoichiometry is not indicated; it is not 1:1 in all cases. Red circles represent primary active transport; white circles represent carrier-mediated transport (secondary active); cylinders represent ion channels. In the proximal convoluted tubule (PCT), Na+ enters the cell through a Na+-H+ exchanger and a series of cotransporters; in the distal convoluted tubule (DCT), Na+ enters the cell through the thiazide-sensitive Na+-Cl− cotransporter; and in the principal cells of the cortical collecting duct (CCD), Na+ enters through a channel (ENaC). In all cases, Na+ is extruded from the cells through the basolateral Na+,K+-ATPase. Transporters in the thick ascending limb of Henle are dealt with separately (see Fig. 2.12).
!
Major Transport Mechanisms Along the Nephron
Na+
Lumen Interstitium
Cl−
Na+
Ca2+
Na+
K+
K+
Ca2+Ca2+
Lumen
Principal cells
Interstitium
Na+
K+
Glucose
Amino acids
Na+
Na+
HCO3−
K+
K+
Cl−
K+
Cl−
Lumen Interstitium
Intercalated cells
AlphaPCT
Beta
H+
H+
K+
HCO3−
Cl−
H+
HCO3−
Cl−
Cl−
Cl−
Na+
K+
K+
Na+
GlucoseNa+
Amino acidsNa+
PhosphateNa+
CitrateCl−
Formate/Oxalate
Na+
H+
Cl−
DCT
same property, so if the load to the loop of Henle or to the distal tubule is increased, some of the excess is mopped up. This is part of the reason that diuretics acting on the proximal tubule are relatively ineffective compared with those acting farther along the nephron; with the latter, there is less scope for buffering of their effects downstream. It is also the reason that combining two diuretics acting at different nephron sites causes a more striking diuresis and natriuresis.
The mechanism of glomerulotubular balance is not fully understood. As far as the proximal tubule is concerned, physical factors operating across peritubular capillary walls may be
involved. Glomerular filtration of essentially protein-free fluid means that the plasma leaving the glomeruli in efferent arterioles and supplying the peritubular capillaries has a relatively high oncotic pressure, which favors uptake of fluid reabsorbed from the proximal tubules. If GFR were reduced in the absence of a change in RPF, peritubular capillary oncotic pressure would also be reduced and the tendency to take up fluid reabsorbed from the proximal tubule diminished. It is thought that some of this fluid might leak back through the leaky tight junctions, reducing net reabsorption (Fig. 2.11). However, this mechanism could work only if GFR changed in the absence of a corresponding change in


C H A P T E R 2 Renal Physiology 21
Figure 2.8 Renal sodium handling along the nephron. Figures outside the nephron rep-resent the approximate percentage of the fil-tered load reabsorbed in each region. Figures within the nephron represent the percentages remaining. Most filtered sodium is reabsorbed in the proximal tubule and loop of Henle; normal day-to-day control of sodium excretion is exerted in the distal nephron.
Distal convoluted tubule
Proximalconvoluted
tubule
Proximalstraighttubule
Cortex
Outermedulla
Innermedulla
Collecting ductConnectingtubule
Thindescending
limb
20%15%
50%
7%
Thickascendinglimb
Thinascendinglimb
3%
8%
5%
!1%
Renal Sodium Handling
35%
Figure 2.9 Renal potassium handling along the nephron. Figures are not given for percent-ages reabsorbed or remaining in every region because quantitative information is incomplete, but most filtered potassium is reabsorbed in the proximal convoluted tubule and thick ascending limb of Henle; approximately 10% of the filtered load reaches the early distal tubule. Secretion by connecting tubule cells and principal cells in the late distal tubule–cortical collecting duct is vari-able and is the major determinant of potassium excretion.
1%–100%
10%
Distal convoluted tubule
Proximalconvoluted
tubule
Proximalstraighttubule
Cortex
Outermedulla
Innermedulla
Collecting ductConnectingtubule
Thindescending
limb
45%
Thickascendinglimb
Thinascendinglimb
Renal Potassium Handling

C H A P T E R 2 Renal Physiology 21
Figure 2.8 Renal sodium handling along the nephron. Figures outside the nephron rep-resent the approximate percentage of the fil-tered load reabsorbed in each region. Figures within the nephron represent the percentages remaining. Most filtered sodium is reabsorbed in the proximal tubule and loop of Henle; normal day-to-day control of sodium excretion is exerted in the distal nephron.
Distal convoluted tubule
Proximalconvoluted
tubule
Proximalstraighttubule
Cortex
Outermedulla
Innermedulla
Collecting ductConnectingtubule
Thindescending
limb
20%15%
50%
7%
Thickascendinglimb
Thinascendinglimb
3%
8%
5%
!1%
Renal Sodium Handling
35%
Figure 2.9 Renal potassium handling along the nephron. Figures are not given for percent-ages reabsorbed or remaining in every region because quantitative information is incomplete, but most filtered potassium is reabsorbed in the proximal convoluted tubule and thick ascending limb of Henle; approximately 10% of the filtered load reaches the early distal tubule. Secretion by connecting tubule cells and principal cells in the late distal tubule–cortical collecting duct is vari-able and is the major determinant of potassium excretion.
1%–100%
10%
Distal convoluted tubule
Proximalconvoluted
tubule
Proximalstraighttubule
Cortex
Outermedulla
Innermedulla
Collecting ductConnectingtubule
Thindescending
limb
45%
Thickascendinglimb
Thinascendinglimb
Renal Potassium Handling

22 S E C T I O N I Essential Renal Anatomy and Physiology
regulatory protein serum- and glucocorticoid-inducible kinase (Sgk1), which increases the number of Na+ channels (ENaC) in the apical membrane (see Fig. 2.7). This stimulates Na+ uptake and further depolarizes the apical membrane, thereby facilitating K+ secretion in the late distal tubule and cortical collecting duct. Aldosterone also stimulates Na+ reabsorption and K+ secretion by upregulating the basolateral Na+,K+-ATPase.
The mineralocorticoid receptors have equal affinity in vitro for aldosterone and adrenal glucocorticoids. The circulating concentrations of adrenal glucocorticoids vastly exceed those of aldosterone, but in vivo, the mineralocorticoid receptors show specificity for aldosterone because of the presence along the distal nephron of the enzyme 11ß-hydroxysteroid dehydrogenase 2, which inactivates glucocorticoids in the vicinity of the receptor.9
COUNTERCURRENT SYSTEM
A major function of the loop of Henle is the generation and main-tenance of the interstitial osmotic gradient that increases from the renal cortex (~290 mOsm/kg) to the tip of the medulla (~1200 mOsm/kg). As indicated in Chapter 1, the loops of Henle of most superficial nephrons turn at the junction between the
RPF; if the two change in parallel (i.e., unchanged filtration frac-tion), there would be no change in oncotic pressure.
A second contributory factor to glomerulotubular balance in the proximal tubule could be the filtered loads of glucose and amino acids; if their loads increase (because of increased GFR), the rates of sodium-coupled glucose and amino acid reabsorption in the proximal tubule will also increase. Finally, it has been proposed that the proximal tubular brush border microvilli serve a mechanosensor function, transmitting changes in torque (caused by altered tubular flow rates) to the cells’ actin cytoskel-eton, which can modulate tubular transporter activity appropri-ately (although the mechanisms are unknown).7
Although the renal sympathetic nerves and certain hormones can influence reabsorption in the proximal tubule and loop of Henle, the combined effects of autoregulation and glomerulotu-bular balance ensure that a relatively constant load of glomerular filtrate is delivered to the distal tubule under normal circum-stances. It is in the final segments of the nephron that normal day-to-day control of sodium excretion is exerted. Evidence points toward important roles for the late DCT and the CNT, in addition to the collecting duct.8 Aldosterone, secreted from the adrenal cortex, stimulates mineralocorticoid receptors within principal cells and CNT cells, which leads to generation of the
Figure 2.10 Genetic defects in transport proteins resulting in renal disease. For more detailed coverage of these clinical conditions, see Chapter 47.
Transporter Consequence of Mutation
Proximal Tubule
Apical Na+-cystine cotransporter Cystinuria
Apical Na+-glucose cotransporter(SGLT2)
Renal glycosuria
Basolateral Na+-HCO3– cotransporter Proximal renal tubular acidosis
Intracellular H+-Cl– exchanger (CIC5) Dent disease
Thick Ascending Limb
Apical Na+-K+-2Cl– cotransporter
Apical K+ channel
Basolateral Cl– channel
Basolateral Cl– channel accessory protein
Bartter syndrome type 4
Bartter syndrome type 3
Bartter syndrome type 2
Bartter syndrome type 1
Distal Convoluted Tubule
Apical Na+-Cl– cotransporter
Collecting Duct
Apical Na+ channel (principal cells) Overexpression: Liddle’s syndromeUnderexpression: pseudohypoaldosteronism type 1b
Basolateral Cl–/HCO3– exchanger (intercalated cells)
Nephrogenic diabetes insipidus
Aquaporin-2 channel (principal cells)
Distal renal tubular acidosis
Apical H+-ATPase (intercalated cells)
Gitelman’s syndrome
Distal renal tubular acidosis (with or without deafness)
Defects in Transport Proteins Resultingin Renal Disease
Figure 2.11 Physical factors and proximal tubular reabsorption. Influence of peritubular capillary oncotic pressure on net reabsorption in proximal tubules. Uptake of reabsorbate into peritubular capillaries is determined by the balance of hydrostatic and oncotic pressures across the capillary wall. Compared with those in systemic capillaries, the peri-tubular capillary hydrostatic (Ppc) and oncotic (πpc) pressures are low and high, respectively, so that uptake of proximal tubular reabsorbate into the capillaries is favored. If peritubular capillary oncotic pressure decreases (or hydrostatic pressure increases), less fluid is taken up, interstitial pres-sure increases, and more fluid may leak back into the lumen paracellu-larly; net reabsorption in proximal tubules would therefore be reduced.
Normal
Peritubular Capillaries Modulate Fluid Reabsorption
Lumen Proximal tubule Interstitialfluid
Peritubularcapillary
Na+Na+
K+H2O
Reduced peritubular capillary oncotic pressure
Fluidreabsorbed
Paracellularbackflux
Ppc(low)
πpc(high)
Raisedinterstitialpressure
↓ πpc
Na+Na+
K+H2O
Less fluidreabsorbed
Increasedparacellular
backflux

20 S E C T I O N I Essential Renal Anatomy and Physiology
Figure 2.7 Major transport mechanisms along the nephron. Major transport proteins for solutes in the apical and basolateral membranes of tubular cells in specific regions of the nephron. Stoichiometry is not indicated; it is not 1:1 in all cases. Red circles represent primary active transport; white circles represent carrier-mediated transport (secondary active); cylinders represent ion channels. In the proximal convoluted tubule (PCT), Na+ enters the cell through a Na+-H+ exchanger and a series of cotransporters; in the distal convoluted tubule (DCT), Na+ enters the cell through the thiazide-sensitive Na+-Cl− cotransporter; and in the principal cells of the cortical collecting duct (CCD), Na+ enters through a channel (ENaC). In all cases, Na+ is extruded from the cells through the basolateral Na+,K+-ATPase. Transporters in the thick ascending limb of Henle are dealt with separately (see Fig. 2.12).
!
Major Transport Mechanisms Along the Nephron
Na+
Lumen Interstitium
Cl−
Na+
Ca2+
Na+
K+
K+
Ca2+Ca2+
Lumen
Principal cells
Interstitium
Na+
K+
Glucose
Amino acids
Na+
Na+
HCO3−
K+
K+
Cl−
K+
Cl−
Lumen Interstitium
Intercalated cells
AlphaPCT
Beta
H+
H+
K+
HCO3−
Cl−
H+
HCO3−
Cl−
Cl−
Cl−
Na+
K+
K+
Na+
GlucoseNa+
Amino acidsNa+
PhosphateNa+
CitrateCl−
Formate/Oxalate
Na+
H+
Cl−
DCT
same property, so if the load to the loop of Henle or to the distal tubule is increased, some of the excess is mopped up. This is part of the reason that diuretics acting on the proximal tubule are relatively ineffective compared with those acting farther along the nephron; with the latter, there is less scope for buffering of their effects downstream. It is also the reason that combining two diuretics acting at different nephron sites causes a more striking diuresis and natriuresis.
The mechanism of glomerulotubular balance is not fully understood. As far as the proximal tubule is concerned, physical factors operating across peritubular capillary walls may be
involved. Glomerular filtration of essentially protein-free fluid means that the plasma leaving the glomeruli in efferent arterioles and supplying the peritubular capillaries has a relatively high oncotic pressure, which favors uptake of fluid reabsorbed from the proximal tubules. If GFR were reduced in the absence of a change in RPF, peritubular capillary oncotic pressure would also be reduced and the tendency to take up fluid reabsorbed from the proximal tubule diminished. It is thought that some of this fluid might leak back through the leaky tight junctions, reducing net reabsorption (Fig. 2.11). However, this mechanism could work only if GFR changed in the absence of a corresponding change in

22 S E C T I O N I Essential Renal Anatomy and Physiology
regulatory protein serum- and glucocorticoid-inducible kinase (Sgk1), which increases the number of Na+ channels (ENaC) in the apical membrane (see Fig. 2.7). This stimulates Na+ uptake and further depolarizes the apical membrane, thereby facilitating K+ secretion in the late distal tubule and cortical collecting duct. Aldosterone also stimulates Na+ reabsorption and K+ secretion by upregulating the basolateral Na+,K+-ATPase.
The mineralocorticoid receptors have equal affinity in vitro for aldosterone and adrenal glucocorticoids. The circulating concentrations of adrenal glucocorticoids vastly exceed those of aldosterone, but in vivo, the mineralocorticoid receptors show specificity for aldosterone because of the presence along the distal nephron of the enzyme 11ß-hydroxysteroid dehydrogenase 2, which inactivates glucocorticoids in the vicinity of the receptor.9
COUNTERCURRENT SYSTEM
A major function of the loop of Henle is the generation and main-tenance of the interstitial osmotic gradient that increases from the renal cortex (~290 mOsm/kg) to the tip of the medulla (~1200 mOsm/kg). As indicated in Chapter 1, the loops of Henle of most superficial nephrons turn at the junction between the
RPF; if the two change in parallel (i.e., unchanged filtration frac-tion), there would be no change in oncotic pressure.
A second contributory factor to glomerulotubular balance in the proximal tubule could be the filtered loads of glucose and amino acids; if their loads increase (because of increased GFR), the rates of sodium-coupled glucose and amino acid reabsorption in the proximal tubule will also increase. Finally, it has been proposed that the proximal tubular brush border microvilli serve a mechanosensor function, transmitting changes in torque (caused by altered tubular flow rates) to the cells’ actin cytoskel-eton, which can modulate tubular transporter activity appropri-ately (although the mechanisms are unknown).7
Although the renal sympathetic nerves and certain hormones can influence reabsorption in the proximal tubule and loop of Henle, the combined effects of autoregulation and glomerulotu-bular balance ensure that a relatively constant load of glomerular filtrate is delivered to the distal tubule under normal circum-stances. It is in the final segments of the nephron that normal day-to-day control of sodium excretion is exerted. Evidence points toward important roles for the late DCT and the CNT, in addition to the collecting duct.8 Aldosterone, secreted from the adrenal cortex, stimulates mineralocorticoid receptors within principal cells and CNT cells, which leads to generation of the
Figure 2.10 Genetic defects in transport proteins resulting in renal disease. For more detailed coverage of these clinical conditions, see Chapter 47.
Transporter Consequence of Mutation
Proximal Tubule
Apical Na+-cystine cotransporter Cystinuria
Apical Na+-glucose cotransporter(SGLT2)
Renal glycosuria
Basolateral Na+-HCO3– cotransporter Proximal renal tubular acidosis
Intracellular H+-Cl– exchanger (CIC5) Dent disease
Thick Ascending Limb
Apical Na+-K+-2Cl– cotransporter
Apical K+ channel
Basolateral Cl– channel
Basolateral Cl– channel accessory protein
Bartter syndrome type 4
Bartter syndrome type 3
Bartter syndrome type 2
Bartter syndrome type 1
Distal Convoluted Tubule
Apical Na+-Cl– cotransporter
Collecting Duct
Apical Na+ channel (principal cells) Overexpression: Liddle’s syndromeUnderexpression: pseudohypoaldosteronism type 1b
Basolateral Cl–/HCO3– exchanger (intercalated cells)
Nephrogenic diabetes insipidus
Aquaporin-2 channel (principal cells)
Distal renal tubular acidosis
Apical H+-ATPase (intercalated cells)
Gitelman’s syndrome
Distal renal tubular acidosis (with or without deafness)
Defects in Transport Proteins Resultingin Renal Disease
Figure 2.11 Physical factors and proximal tubular reabsorption. Influence of peritubular capillary oncotic pressure on net reabsorption in proximal tubules. Uptake of reabsorbate into peritubular capillaries is determined by the balance of hydrostatic and oncotic pressures across the capillary wall. Compared with those in systemic capillaries, the peri-tubular capillary hydrostatic (Ppc) and oncotic (πpc) pressures are low and high, respectively, so that uptake of proximal tubular reabsorbate into the capillaries is favored. If peritubular capillary oncotic pressure decreases (or hydrostatic pressure increases), less fluid is taken up, interstitial pres-sure increases, and more fluid may leak back into the lumen paracellu-larly; net reabsorption in proximal tubules would therefore be reduced.
Normal
Peritubular Capillaries Modulate Fluid Reabsorption
Lumen Proximal tubule Interstitialfluid
Peritubularcapillary
Na+Na+
K+H2O
Reduced peritubular capillary oncotic pressure
Fluidreabsorbed
Paracellularbackflux
Ppc(low)
πpc(high)
Raisedinterstitialpressure
↓ πpc
Na+Na+
K+H2O
Less fluidreabsorbed
Increasedparacellular
backflux

FIN
Recommended