대 한 방 사 선 의 학 회 지 1993 ; 29 (5) : 923~929
Journal of Korean Radiological Society, September, 1993
Percutaneous Catheter Drainage of Lung Abscess *
Young Shin Kim, M.D., Kyung Ah Chun, M.D., Hyo Sun Choi, M.D. Hyun Kown Ha, M.D., Kyung Sub Shinn, M.D.
Dφa1τment 0/ Radiology, Catholic University Medical College
- Abstract-
From March 1987 to July 1989, six patients (five dadults and one child) with lung abscess (size, 5- 13cm in
diameter) were treated with percutaneous aspiration and drainage. In each case , the puncture was made where
the wall of the abscess was in contact with the pleura1 surface. An 8 to 10 Fr catheter was inserted for drain
age. Five of 6 had a dramatic clinica1 response within 24 hours of the drainage. Percutaneous drainage was
successful with complete abscess resolution in four and partial res이ution in one patient. No response was seen
in the rest one. The duration of drainage ranged from 7 to 18 days (average , 15.5days) in successful cases.
One case of the fai lure in drainage was due to persistent aspiration of the neurologically impaired patient. In
one patient, the abscess resolved after drainage but recurred after inadvertent removal of the catheter 7 days
after insertion. In two patients, concurrent pleura1 empyema was resolved completely by the drainage. Comput
ed tomography provided anatomic details necessaη for choosing the puncture site and avoiding a puncture of
the lung parenchyma. Percutaneous catheter drainage is a safe and effective method for treating patient with
lung abscess.
Index Words: Lung, Abscess 60.216
Abscess, Percutaneous drainage
INTRODUCTION
Despite the wide availability of antibiotics
and advances in medical technology, lung
abscess continues to be a serious medical prob
lem, particularly in the debilitated patients
such as those with alcoholism, diabetes mellitus, and medical conditions requiring steroid thera
py. The mortality rates for lung abscess ranged
from 17 to 75% (1, 2). Although the admini
stration of appropriate antibiotics has proved to
be an effective treatment for most of acute
lung abscesses , medical therapy could fail in
chronic cases that formed a thick fibrotic wall
or bronchial stenosis. Because delay in the
treatment of a lung abscess may result in irre
versible parenchymal damage , surgical interven
tion was used in the management of patients
with chronic lung abscesses unresponsive to
medical therapy. Surgical intervention is also
warranted when the abscess is associated with
hemoptysis, empyema, or bronchopleural fistu
la. Percutaneous drainage of lung abscess is an
effective alternative to open surgery. Percutane
ous aspiration and drainage were reported to
be safe and effective in management of patients
with intra-abdominal, pulmonary, and mediasti-
* 이 논문은 1992년 가톨릭중앙의료원 연구보조비로 이루어진것임 이 논문은 1992년 6월 22일 접수하여 1993년 4월 20일에 채택되었음.
Received June 22, 1992, Accepted April 20 , 1993
- 923-

Journal of Korean Radi이 ogical Society 1993; 29 (5) : 923~929
nal abscesses (3-5). The purpose of this report
is to present our experience of percutaneous
catheter drainage in six patients with lung
abscess.
MATERIALS AND METHODS
Six patients (3 women and 3 men, aged 6-
66) underwent percutaneous aspiration and
drainage of lung abscesses at St. Maη’ s Hospi
tal of Catholoic University Medical college in
Seoul, Korea between March 1987 and June
1989. The predisposing causes of the abscesses
were diabetes mellitus (n = 2) , complicated
bronchoscopic biopsy (n = 1) , aspiration pneu
monia (n = 1), and unknown etiology (n = 2).
Clinically, all patients presented with productive
cough, chest pain, and feve r. One patient with
whom the abscess was in the right middle lobe
presented with dyspnea, tachycardia, and cardi
ac arrythmia additionally. The locations of the
abscesses were the superior segment of the
right lower lobe (n = 2) and left lower lobe (n =
2) , the right middle lobe (n = 1) , and the pos
terior segment of thr right upper lobe (n = 1).
The size of abscess ranged from 5 to 13cm in
diameter.
In each patient, the chest radiographs and
computed tomographic scans or ultrasonograms
were reviewed before the drainage procedure
to localize the nearest skin puncture site from
the wall of the abscess. An 18 gauge needle was
inserted into the abscess cavity under a fluoro
scopic (five patients) or CT (one patient) guid
ance while respiration was suspended. Once the
needle tip was located within the abscess cavity,
fluid was withdrawn and then an O.035-inch, J
shaped guide wire was introduced into the cavi
ty. After aspiration of pus, the abscess cavity
was irrigated with small aliquots of normal sa
line solution until they became clear of pus . We
used 8 .3Fr catheters with a "pigtail " configura
tion in three , 8Fr polyethylene catheters with a
"cobra head" configuration in two and a 10Fr
924
Malecot catheter in one patient. The choice of
catheter was made on the availability of cathe
ter at the time of drainage.
In each patient, culture and antibiotic sensi
tivity studies for the aspirated fluid were per
formed. An appropriate antibiotic regimen was
administered according to the results of the
bacteriologic study.
In all patients irrigation was performed
twice a day. Body temperature was recorded
and white blood cell (WBC) counts were mea
sured before and selially after the placement of
a catheter. The size of abscess was measured on
the chest radiographs . Volume of the drained
material was recorded daily. The catheter was
removed when the abscess resolved and drain
age stopped. Abscess drainage was not attempt
ed when the abscess wall did not touch the
pleura because of possibility of inducing pyo
thorax or pneumothorax.
RESULTS
Five of the six patients had dramatic clinical
response after drainage. In these patients fever
dropped rapidly and their WBC counts de
creased to normal or near normal value within
two days of drainage. The size of the abscesses
decreased gradually during the first week of
drainage , remained unchanged afterward in
four patients, and continued to decrease in one
patient by the time of catheter removal. The
duration of drainage in four patients showed
complete resolution of abscesses rangd from 11
to 18 days (caverage, 15.5 days) in two patients
it took 11 days , and in the other two patients
12 days and 18 days were required, respec
tively.
In four of the six patients, the abscess
resolved completely without recurrence of any
pulmonary infection. In one patient who initial
ly responded favorably after drainage (.vith an
8Fr polyethylene catheter with a "cobra head "
configuration) , the abscess recurred after an in-

a
b
c
Young Shin Kim , et al : Percutaneous Catheter Drainage of Lung Abscess
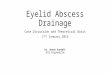
Fig. 1. Lung abscess associated with right pleural empyema in a 6-year-old girl who had staphylococal pneumoma a. Adrrússion chest radiograph shows a 10cm abscess 씨th an air- f1 uid in the right rrúddle lobe (arrow) and pleural effusion (smaller arrow). b. Follow-up chest radiograph 1 day after drainage shows a decrease in the size of the abscess and the drainage catheter (arrow) c. Chest radiograph obtained after 12 days of drainage shows complete resolution of the abscess end empyema
advertent removal of the catheter 7 days after
the insertion. The patient refused the reinser
tion of the catheter and drainage catheter sub
sequently withdrew form the patient who left
the hospital 4 days Jater against medical advice.
1n the rest one patien t who was in comatous
state for six months due to traumatic brain con
tusion and right putaminal hematoma, an
abscess with a thick wall, measuring 10cm in di
ameter, was developed in the right upper lobe
Ultrasonograhy confirmed the thick wall of the
abscess at the time of drainage. The amount of
drained pus was scanty throughout the entire
drainage period revealing only a minimal de
crease in size of the absess inspite of several at
tempts of catheter repositioning. Therefore; the
catheter was removed 9 days after the inser
tion. The failure of the drainage was thought to
be attributed to the thick abscess wall and re
current aspiration pneumonia due to dimin
ished cough reflex. The bacteriologic study
showed Proteus , Klebsiella and Peptostrepto
coccus . The patient eventually succumbed to
respiratory failure 3 months later.
1n all patients chest radiographs were
checked after removal of the catheters: one pa
tient had complete resolution of the abscess
(Fig. 1), three had small residual cavities with
out any air-fluid level (Fig. 2) , one had
reaccumulation of f1uid after an inadvertent re
moval of the catheter, and in the rest one pa
tient, the residual cavities that were noted at
the time of catheter removal were completely
- 925 -

Journal of Korean Radiological Society 1993; 29 (5) : 923~929
a b
c
resolved. In the second patient, a chest rad io
graph taken 2 months later showed coJlapse of
the cavity to be col1apsed with focaJ fibrosis. In
the third patient, the residual cystic cavity re
mained unchanged, however, a recurrent pneu
monia was developed around the thin wal1ed
cystic residua 3 years later. This reinfection
might have been related to the underlying
chronic paranasal sinus disease
Before the drainage , al1 patients received
antibiotic therapy for 1 to 14 days. Cefazolin
and a combination of cefazolin and gentamicin
were common types of initial drug therapy.
These regimens were changed later according
to bacte rial susceptibiJity during drainage and
d
Fig. 2. Lung abscess in a 62-year-old womaen who had streptococcal pneumonia. a. admission chest radiograph shows a 8cm diameter, thick walled abscess in the right middle lobe (arrow). b. Chest radiograph after placement of a Malecot catheter within the abscess cavity shows the proper position of the catheter tip in the cavity (arrow) c. CT scan of chest sh。、vs the entJγ of the catheter into the cavity ‘vhich is in contact with the pleural surface (arrow) d. Upright chest radiograph obtained after removal of the catheter shows residual cavity
continued for average of 5 days after removal
of catheters. In two patient concurrent pleural
empyema (proved by pleurocentesis) resolved
after percutaneous drainage of the abscess (Fgi.
1). There were no complications related to the
proceudre.
The causative organismjorganisms on the
bacteriolo멍c studies of the abscess fluid wasj
were Staphylococcus (n = 1), Streptococcus (n =
1), Streptococcus and Citrobacter (n = 1),
Streptococcus, Staphylococcus and Veillone l1a
(n= 1), Proteus , Klebsiella, and Peptostrepto
coccus (n = 1).
In one patient showed recurrent abscess , no
microorganism was isolated from aspirated pus.
Therefore appropriate antibiotics could not be
selected and this was considered to be the rea-
926

Young Shin Kim , et al : Percutaneous Catheter Drainage of Lung Abscess
son that the abscess recurred in spite of contin
ued antibiotic therapy after inadvertent removal
of catheter.
DISCUSSION
The initial therapy of lung abscess has been
medical with the administration of appropriate
antimicrobial agents and supportive measures
with cure rates of 40 to 90 percent (6). It was
considered that medical therapy was often inef
fective in the treatment of abscesses with a
thick wall or bronchial obstruction (7) . Thus ,
surgical intervention (lobectomy, wedged lung
resection , or external drainage through thora
cotomy) is required to avoid the development
of bronchiectasis and pulmonary fibrosis . Sur
gery is also indicated for patients with lung
abscess associated with empyema, broncho
pleural fistula, or suspected malignancy (8).
The mortality rate of surgery for lung abscess
was low but the incidence of empyema after
pulmonary resection for abscess ranged from
10 to 28.8 percent (6 , 9).
Surgeη of the lung abscesses necessitates
sacrifice of lung volume and creates a resultant
contamination of the pleural space, which if not
obliterated, may develop and empyema. Percu
taneous drainage of lung abscesses may avoid
some shortcomings. However, the major draw
back is that a bronchial deforrnity persists after
drainage and the the patient will experience a
recurrence. Secondly, the tube or packing may
erode pulmonaη vessels and cause exsanguina
ting hemorrhage.
A1though the procedure of the percutane
ous drainage of lung abscess was not described
in the 1940 s, it was not used clinically. Recent
ly, to overcome the long duration of medial
treatment and the risk of surgery, intervention
al technique within the thorax was designed
and applied. The majority of reports describe
their use in the drainage of pleural effusion or
empyema in adults (1 이 . Several authors also
reported good results with mediastinal, chest
wall , and intraparenchymal abscess (1, 6 , 11).
A1though our series is small, our results indi
cate that percutaneous aspiration and drainage
are safe and effective in managing patients with
lund abscess except chronic lung abscess with
thick fibrotic wall. The drainage technique that
was used in our patients is the smae as used for
drainage of intra-abdominal and mediastinal
abscesses.
The indications of the percutaneous drain
age method include persistent unremitting sep
sis and toxicity from and abscess over 4cm in
diameter while receving an antibiotics , lack of
adequate cough mechanism, radiologic e、rid
neces of developing contralateral lung pneumo
nia, and increasing size or fluid content of the
abscess (1 2, 13).
Computed tomography will provide infor
mations about the site and the distance be
tween the skin and the wall of the abscess con
tacting the pleural surface. A1 though we did
not encounter any complication in this series , the pU l1cture should be made where the wall of
abscess was in contact with the pleural surface
to avoid spillage of pus into the pleural cavity
and the development of pneumothorax. Until
more experiences are gained , those abscesses
that are surrounded by the lung parenchyma
and fail to respond to a medical therapy should
be subjected to a surgical intervention.
We used 8 or 10Fr catheters for drainage
of the abscesses in our patients. A larger bore
catheter may be necessaη for drainage of the
abscess with thick fluid. Replacement of the
drainage catheter with a larger bore-catheter
after the tract was matured is a safe and simple
procedure and dose not cause pneumothorax
and bleeding. Continuous negative pressure
suction with catheter irrigation should be used
to facilitate drainage and reduce spillage of
abscess fluid into the pleural cavity.
It is important to check the patient clinically
with the amount of drainage, catheter position,
- 927-

Journal of Korean Radi이ogical Society 1993; 29 (5) : 923~929
and the size of the abscess by chest radiogra
phy. We recomrnend administration of appro
priate antibiotics before , during, and after
drainage. The optimal duration of catheter
drainage for lung abscess has not determined.
The average duration of drainage in our four
cured patients was 15.5 days (range , 11-18
days) , which were much shorter period than
those of the cases included in the report of Ball
(1 이. We removed the catheter when the size of
abscess decreased significantly and there was no
evidence of drainage for at least 3days. It is
possible to monitor recurrence of the abscess
by withdraqing the catheter gradually over a
period of a few days or replacing the catheter
with a smaller end-hole catheter and clamping
it. 1t was demonstrated that the residual abscess
cavity might continue to resolve after removal
of the catheter after drainage. We also ob
served that the drainage catheter might be re
moved before the abscess cavity completely
resolved radiographically. There is a concern
that infection is related to the persistence of
the predisposing cause of the original lung
abscess as in our case (1 4). 1n addition, imrne
diate reinfection in the area of thin walled
residue of the lung absess could be easily
controled with antimicrobial drugs obtained
from bacteriologic study.
1n sumrnaη, percutaneous drainage is a safe
and effective method for management of pa
tients with s이itary large lung abscess unrespon
sive to medical therapy. 1t can be carried out
with minimal stress and risk to the patient and
results in a dramatic clinical response and rapid
resolution of the abscess. Further study is
reguired to determine whether the percutane
ous method can be safely used to treat the lung
abscess surrounded by the lung parenchyma.
Until then, the method described heretofore
should be reserved for treatment of patients
with lung abscess unresponsive to medical ther
apy.
REFERENCES
1. VanSonnenberg EM, Muller pr, Ferrucci JT J r.
Percutaneous drainage of 250 abdominal abs
cesses and fluid collection. 1. Results, failure , and complications. Radiology 1984; 151:267-
277
2. VanSonnengerg E, Nakamoto SK, Muller PR, Casola G, Neff CC, FPJ , Ferruci JT Jr, Simeone
JF. CT and Ultrasound-guide catheter drainage
of empyemas after chest tube failure. Radiology
1984; 151:349-353
3. Vainrub B, Musher D, Guinn GA, Young EJ , Septimus EJ, Travis LL. Percutaneous drainage
of lung abscess. Am Rev of Respir Dis 1978;
117:153- 159
4. Aronberg DJ , Sagel SS, Jost RG , Lee J 1. Percu
taneous drainage of lung abscess. AJR 1979; 132:282-288
5. Gobien RP , Stanley JH , Gobien BS , Vl~ic 1, Pass
HF. Percutaneous catheter aspiration and drain
age of suspected mediastinal abscesses. Radiology1984;151 ’ 69-71
6. Estrera AS , Platt MR, Mills LJ , Shaw RR. Pri
maη lung abscess. J Thorac Cardiovascular sur
gerγ 1980; 79:275-282
7. Fisher WR, Husebye K, Chedister C, Miller M.
Primaη lung abscess. Arch Intern Med 1961; 107-100-112
8. Delarue NC, Pearson FG , Nelems JM , Cooper
JD. Lung abscess: Surgical implications. Can J
Surg 1980; 23:297-302
9. Shaw RR, Pauson D1. Pulmonary resection for
chronic abscess of the lung. J Thoracic Surg 1948; 17:514
10. Ball WS , Bisset III GS Jr, Towbin RB. Percuta
neous drainage of chest abscesses in children Radiology 1989; 171 :431 -434
11. Neff C, Lowson DW ‘ Boerhaave syndrom: inter
ventional radiologic management. AJR 1985; 145:819-820
12. Eric VS , Horacio BD, Giovanna C, et al. Lung
abscess: CT -guided drainage. Radiology 1991;
178:347-351
13. Ricε πN, Ginsberg l\J, Todd TRJ. Tube drain-
- 928 -

Yo ung Shin Kim , et al : Percutaneous Catheter Drainage of Lung Abscess
age of lung abscesses . Ann Thorac Surg 1987;
44:356-359
c1assfication and analysis of 97 cases‘ ung
abscess. Am Rev of Respir Dis 1969; 99:390-
398 14. Perlman LV, Lerner E , D ’esopo N. Clinical
〈국문 요약〉
폐 농양의 경피적 도관 배액술
가톨릭대학 의학부 방사선과학교실
김영신·천경아·최효선·하현권·신경섭
저자들은 6예의 폐 농양 환자를 대상으로 경피적 홉인과 도관 배액술을 시행하였다. 각예에서 늑막표면과 접촉하
고 있는 폐농양 벽에서 천자하여 8-10Fr 도관을 삽입하였다. 6명중 5명이 배액 24시간 내에 현저한 임상적 호전을
보였다. 농양은 배액술후 4명에서 완전히 농양이 없어졌고 한명은 부분적인 크기의 감소를 보였고 나머지 한명에서
는 농양의 변화가 없었다. 성공한 배액술의 기간은 7- 18일 이었고 평균 15. 5일 이었다. 신경학적 장애를 가진 한명
의 환자에서 배액이 실패한 이유는 계속적인 홉-인 때문이었다. 배액술후 초기에는 농양이 호전되었으나 부주의로 도
관이 빠진후 농양이 다시 커진 환자가 일례 있었다. 두맹의 환자에서 폐농양과 공존하던 늑막농흉이 배액후 완전히
없어졌다. 천자 위치를 결정하고 정상폐에 천자하는 것을 피하기 위하여, 정확한 해부학적 구조를 아는데 전산화단
층촬영이 유용하였다. 경피적 도관 배액술을 폐농양을 치료하는데 안전하고 효과적인 방법이다.
- 929-
Recommended