712 CASE REPORT WESTABY ET AL Ann Thorac Surg TRAUMATIC CORONARY ANEURYSM 1995;60:712-3
R e f e r e n c e s
1. Warter A, Satge D, Roeslin N. Angioinvasive plasma cell granulornas of the lung. Cancer 1987;59:435-43.
2. Maier HC, Sommers SC. Recurrent and metastatic pulmo- nary fibrous histiocytoma/plasma cell granuloma in a child. Cancer 1987;60:1073- 6.
3. Janigan DT, Marrie TJ. An inflammatory pseudotumor of the lung in Q fever pneumonia. N Engl J Med 1983;308:86-8.
4. Bates T, Hull OH. Histiocytoma of the bronchus. Am J Dis Child 1958;95:53-6.
5. Grossman DE, Bemis EL, Pemberton AH, Narodick BG. Fibrous histiocytoma or xanthoma of the lung with bronchial involvement. J Thorac Cardiovasc Surg 1973;65:653-7.
6. Duncan JD, Greenberg SD, Mattox KL, Madewell JE. Benign fibrous histiocytoma: a rare endobronchial neoplasm. Int Surg 1986;71:110-1.
7. Armstrong P, Elston C, Sanderson M. Endobronchial histio- cytoma. Br J Radiol 1975;48:221-2.
8. Bates HR, Buis LJ, Johns TNP. Endobronchial histiocytoma. Chest 1976;69:705-6.
Posttraumatic Coronary Artery Aneurysm Stephen Westaby, FRCS, George Drossos, MD, and
Nicholas Giannopoulos, MD
Oxford Heart Centre, Oxford, England
A 31-year-old man sustained blunt deceleration trauma with dissection of the left anterior descending coronary artery. We repaired a posttraumatic coronary aneurysm to prevent late occlusion of the recanalized vessel . An internal mammary artery graft was applied as a precau- tion against postoperative thrombosis. Follow-up at 12 months showed improved left ventricular function.
(Ann Thorac Surg 1995;60:712-3)
D espite the frequency of deceleration b lunt chest trauma, coronary artery injuries are rare. Posttrau-
matic left anterior descending coronary aneurysm has been described previously in association with acute myo- cardial infarction and left ventricular aneurysm [1-3]. Traumatic coronary artery occlusion and rupture also occur without aneurysm formation [4, 5]. Because of the unusua l nature of this injury there is little consensus as to opt imum management . Some authors suggest a wait and watch option, whereas others have advocated operation [2, 3]. In 1 case a left ventricular aneurysm was resected and coronary aneurysm left in situ due to "'inaccessibil- ity" [3]. In this report we describe a patient who sus- tained b lunt cardiac trauma with acute dissection of the left anterior descending coronary artery and myocardial infarction. We elected to repair the aneurysm to avoid the
possibility of secondary thrombosis of the recanalized artery.
A 31-year-old man sustained multiple injuries dur ing a motorcycle accident. Skeletal t rauma included bilateral fractures of the humerus and fracture of the right tibia and fibula. In addition he sustained a head injury with cerebral contusion and subarachnoid hemorrhage, which resulted in unconsciousness for 24 hours. On the 12th postoperative day he complained of retrosternal chest pain and became dyspneic with chest roentgenographic findings of pulmonary edema. The electrocardiogram suggested acute anterior myocardial infarction. Two- dimensional echocardiography showed apical and ventric- ular septal dyskinesia. He required intermittent positive- pressure ventilation and intravenous nitrate therapy for 4 days, after which he made an uneventful recovery.
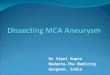
Four weeks later and 2 months after the accident he underwent coronary angiography. This showed a dis- crete proximal left anterior descending coronary artery aneurysm with a patent distal artery (Fig 1). Left ven- triculography showed dyskinesia of the interventricular septum and left ventricular apex, but a substantial area of left anterior descending territory remained viable. He was referred for operation.
Median sternotorny was performed and the left inter- nal mammary artery harvested. Inspection of the heart showed thickening and fibrosis of the traumatized right ventricle and scarring in the area of anterior myocardial infarction. The left anterior descending coronary artery was patent, and there was no mitral or tricuspid regur- gitation. Palpation of the proximal left anterior descend- ing coronary artery behind the pu lmonary artery re- vealed the site of the coronary aneurysm. We decided to approach this directly by transection and anterior retrac- tion of the main pulmonary artery.
The heart was arrested with anterograde St. Thomas"
Accepted for publication March 21, 1995
Address reprint requests to Mr Westaby, Oxford Heart Centre, Oxford Radcliffe Hospital, The John Radcliffe, Oxford, England OX3 9DU.
Fig 1. Coronary angiogram showing the left coronary artery with a traumatic aneurysm at the origin of the left anterior descending cor- onary artery.
© 1995 by The Society of Thoracic Surgeons 0003-4975]95/$9.50 0003-4975(95)00342-I

Ann Thorac Surg CASE REPORT WESTABY ET AL 713 1995;60:712-3 TRAUMATIC CORONARY ANEURYSM
cardioplegia, and the pu lmonary artery was transected, providing direct access to the left main and proximal left anter ior descending coronary arteries. The aneurysm was opened longitudinally; the morphology of this was compat ible with acute localized dissection of the vessel wall. The aneurysm was obl i terated by cont inuous su- ture, and the left internal m a m m a r y artery was anasto- mosed to the middle third of the left anterior descending artery. The procedure was per formed with normothermic perfusion and ca rd iopu lmonary bypass, which was dis- cont inued without difficulty. He was extubated immedi - ately and discharged from the hospital on the sixth postoperat ive day. At follow-up 12 months later he is asyrnptomatic (New York Heart Association functional class I) with a normal exercise e lect rocardiogram and improvement in echocardiographic contractile function of the interventr icular septum. We could not justify repeat angiograms.
Comment
Saccular aneurysms occur in both Kawasaki 's disease and a theromatous coronary disease and may thrombose with embolizat ion or occlusion of the parent vessel. Aneurysms also occur after percutaneous t ransluminal coronary angioplasty, and the incidence of this p rob lem may increase in the future. Coronary aneurysms are extremely rare after blunt chest t rauma and are usually associated with acute myocardia l infarction through tem- porary occlusion of the injured vessel. Bjorn-Hansen and colleagues I2] documented the natural history of one post t raumat ic aneurysm with angiography 1, 5, and 11 mon ths after the accident . Their pa t ien t r e m a i n e d asymptomat ic and the aneurysm disappeared , p resum- ably by thrombosis of the lumen. Stone and Fleming I3l descr ibed a 17-year-old pat ient with a proximal left anterior descending coronary artery aneurysm almost identical to that in our own pat ient but with a well- es tabl ished left ventr icular aneurysm. The left anterior descending vessel was widely patent. In their pat ient left ventr icular aneurysmec tomy was per formed but the cor- onary aneurysm was left in situ because of inaccessibility. In the presence of an es tabl ished aneurysm further left anter ior descending coronary artery occlusion did not pose a threat, but the pat ient suffered a stroke pos toper- atively.
Our pat ient had viable muscle in the left anter ior descending coronary ar tery terr i tory and, a l though there is nothing in the l i terature to suggest that this aneurysm was likely to rupture, the possibi l i ty of thrombosis with propagat ion into the left anter ior descending coronary ar tery lumen remained. We made a direct surgical ap- proach to the distal left main coronary ar tery and proxi- mal left anter ior descending coronary ar tery and opened the aneurysm directly. Access to the left main and prox- imal left anterior descending coronary arteries is straight- forward when the pu lmonary ar tery is transected. Al- though the left main coronary ar tery can be approached by retraction on the pu lmonary artery in the empty heart, there were inf lammatory adhes ions a round the aneu- rysm, and transect ion of the pu lmonary ar tery facili tated access. The morphology in our pat ient was clearly dis- section of the vessel wall with di latat ion of the false lumen. There may well have been a risk of aneurysm rupture in this patient. Al though the left anter ior de- scending coronary ar tery r emained pa tent after the re- pair, we dec ided to implant the left internal m a m m a r y artery on the distal vessel as an insurance policy. An al ternative approach would have been to excise the aneurysm and close the vessel with a vein patch, but we did not consider this to be as rel iable as an internal m a m m a r y graft.
Despi te advocates of conservative t rea tment we advise direct surgical repai r of post t raumat ic coronary aneu- rysm to prevent the potent ial for late thrombosis with occlusion of the distal vessels.
References
1. Westaby S. The injured heart. Clin Intensive Care 1990;1: 210-9.
2. gjorn-Hansen LS, Thomassen AR, Nielsen TT. Aneurysm of the left anterior descending coronary artery after chest trauma. Eur Heart J 1989;10:177-9.
3. Stone DL, Fleming HA. Aneurysm of left ventricle and left coronary artery after non-penetrating chest trauma. Br Heart J 1983;50:495-7.
4. Pifarr6 R, Grieco J, Garibaldi A, Sullivan H, Montoya A, Bakhos M. Acute coronary artery occlusion secondary to blunt chest trauma. J Thorac Cardiovasc Surg 1982;83:122-5.
5. Heyndrick XG, Vermeire P, Goffin Y, Van den Bogest P. Rupture of the right coronary artery due to nonpenetrating chest trauma. Chest 1974;65:577-9.
Recommended






![[症例報告]Aneurysm of the gastroduodenal artery with 琉球 ...okinawa-repo.lib.u-ryukyu.ac.jp/bitstream/20.500.12001/...emboh can result in dangerous consequences of small or](https://img.pdfslide.tips/doc/110x75/60d001b4b68fcf06f50ac7dc/caneurysm-of-the-gastroduodenal-artery-with-ccf-okinawa-repolibu-.jpg)