Programma Scientifico Preliminare
LUNEDI’ 27 NOVEMBRE 2017
9.00 – 9.30 Apertura Segreteria e Registrazione dei Partecipanti
9.30 -10.00 Saluto delle Autorità e Apertura dei Lavori Giovannella Baggio (Padova) Rosario Rizzuto - Rettore, Università di Padova Mario Plebani - Presidente Scuola di Medicina (Padova) Cristina Parolin - Direttore Dipartimento di Medicina Molecolare (Padova) Paolo Simioni – Presidente Ordine dei Medici (Padova)
10.00 – 11.00 LETTURE MAGISTRALI Moderatore: Sergio Pecorelli (Brescia)
10.00 - 10.30 Ruolo della Medicina di Genere nella Economia Sanitaria
Francesco Saverio Mennini (Roma)
10.30 - 11.00 Epigenetica e Genere Giuseppe Novelli (Roma)
11.00 – 13.00 UPDATE LECTURES Cardiologia e oncologia genere-specifiche Moderatori: Cecilia Politi (Isernia) Annamaria Moretti (Bari)
11.00 - 11.30 Lo Scompenso Cardiaco
Gianfranco Sinagra (Trieste)
11.30 - 12.00 Le Aritmie Cardiache Loira Leoni (Padova)
12.00 – 12.30 Differenze di genere in oncologia toraco-polmonare Giulia Pasello (Padova)
Programma Scientifico Preliminare
LUNEDI’ 27 NOVEMBRE 2017
9.00 – 9.30 Apertura Segreteria e Registrazione dei Partecipanti
9.30 -10.00 Saluto delle Autorità e Apertura dei Lavori Giovannella Baggio (Padova) Rosario Rizzuto - Rettore, Università di Padova Mario Plebani - Presidente Scuola di Medicina (Padova) Cristina Parolin - Direttore Dipartimento di Medicina Molecolare (Padova) Paolo Simioni – Presidente Ordine dei Medici (Padova)
10.00 – 11.00 LETTURE MAGISTRALI Moderatore: Sergio Pecorelli (Brescia)
10.00 - 10.30 Ruolo della Medicina di Genere nella Economia Sanitaria
Francesco Saverio Mennini (Roma)
10.30 - 11.00 Epigenetica e Genere Giuseppe Novelli (Roma)
11.00 – 13.00 UPDATE LECTURES Cardiologia e oncologia genere-specifiche Moderatori: Cecilia Politi (Isernia) Annamaria Moretti (Bari)
11.00 - 11.30 Lo Scompenso Cardiaco
Gianfranco Sinagra (Trieste)
11.30 - 12.00 Le Aritmie Cardiache Loira Leoni (Padova)
12.00 – 12.30 Differenze di genere in oncologia toraco-polmonare Giulia Pasello (Padova)
LO SCOMPENSO CARDIACO
Dr. Marco MERLOS.C. Cardiologia, ASUITs, Trieste
DISCLOSURE: None


SCOMPENSO CARDIACO
VIA FINALE COMUNE DI MOLTELICI PATOLOGIE


Scardovi et al. G Ital Cardiol 2012

SCOMPENSO CARDIACO CRONICO –FISIOPATOLOGIA

?






ALLA RICERCA DI NUOVI TARGET

DEFINIZIONE EZIOLOGICAHFpEF - HFrEF

ESC-HF guidelines. Ponikowski P. Eur Heart J 2016
COMORBIDITA’

PROGNOSI


Chioncel O et al. EJHF 2017


DONNE E SCOMPENSO CARDIACO

Cardiovascular disease in women
• Coronary artery disease• Heart attacks, angina
• Congestive heart failure• Preserved systolic function/Hypertensive• Peri-partum cardiomyopathy• Chemotherapy induced cardiomyopathy• Autoimmune related cardiomyopathy
• Arrhythmia• Atrial fibrillation
• Valvular heart disease• Aortic stenosis• Mitral regurgitation
• Stroke
• Pericardial disease

Precision Medicine in Heart Failure
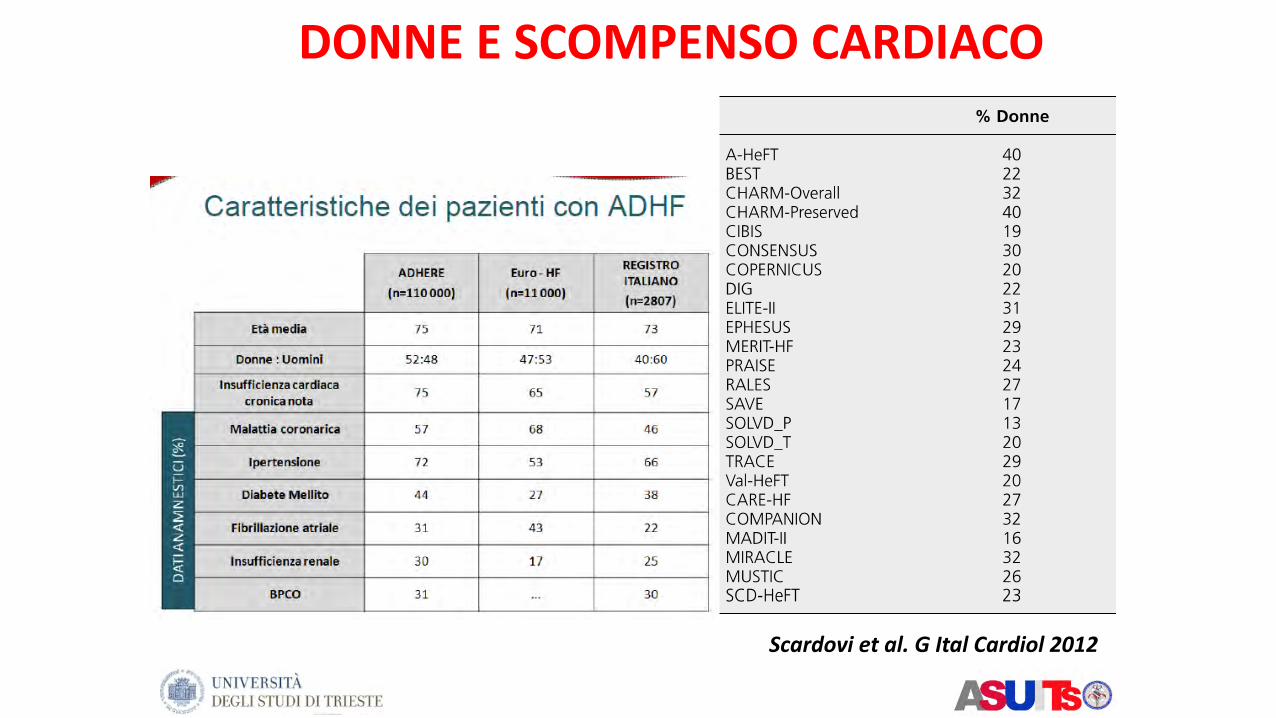
Scardovi et al. G Ital Cardiol 2012
DONNE E SCOMPENSO CARDIACO

Sex differences: Physiology
• Compared to Men, Women have:• Lower LV mass
• Greater contractility
• Preserved mass with aging
• Lower rate of apoptosis
• Small coronary vessels
• Lower blood pressure
• Faster resting HR
• Less catecholamine mediated vasoconstriction

Sex Hormones
• Estrogen• Receptors on cardiac cells
• Estrogen affects hepatic gene expression
• Improved lipids
• Vascular effects: vasodilation
• Stimluates immune system• Affects cytokine/inflammatory pathways
• Testosterone• Increases inflammation/cholesterol

CHD and menopausal status
0
0,5
1
1,5
2
2,5
3
3,5
4
40-44 45-49 50-54
Pre-menopausal
Post-menopausal
An
nu
al in
cid
ence
per
10
00

Women vs. Men
• More non-ischemic etiology of HF
• More HTN, diabetes
• Older age at presentation
• Lower QOL, more depression
• More frequent LBBB
• Similar hospitalization/readmission rates
• Lower mortality/transplant rate in DCM
• Lower representation in HF trials (17-23%)
• Less procedures, including ICDs, CRT

ESC-HF guidelines. Ponikowski P. Eur Heart J 2016
HEART FAILURE SPECTRUM

HFrEF
ACE inhibitors
Beta-blockers Spironolactone/Eplerenone
ICD/CRT
Structured Follow-up Early diagnosis
Best management in HFrEF
Ivabradine
LCZ696

Simon et al. Circulation 2001

HFrEF
Shore S et al. JACC HF, 2015

Shore S et al. JACC HF, 2015

CVD –leading cause of death in women
0
50
100
150
200
250
300
350
400
450
500
CVD Stroke Breast CA
Death/100,000
AHA 2003

Coronary Heart Disease Mortality in Younger Women Higher than in Men
Vaccarino NEJM 1999;341:217
2,9
4,1
5,7
8,2
10,7
14,4
18,4
21,8
25,3
6,1
7,4
9,5
11,1
13,4
16,6
19,1
21,5
24,2
0
5
10
15
20
25
30
< 50 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89
Dea
th d
urin
g H
ospi
taliz
atio
n (%
)
Men Women
Figure 1. Rates of death during hospitalization for Myocardial Infarction among women and men, according to age. The interaction between sex and age was significant (P<0.001).

Cardiovascular disease (CVD) mortality trends for men and women in the United States from 1979 to 2011

Women and CAD
Compared to men…..
Less classical symptoms
More related to diabetes, inactivity, obesity, depression
2/3 women who die suddenly had no previous heart attack
2x more likely to die soon after heart attack
Worse outcome after bypass surgery

Women’s Symptoms
• Prodromal• Unusual fatigue 70%
• Sleep disturbance 48%
• Shortness of breath 42%
• Indigestion 39%
• Anxiety 35%
• Acute• Shortness of breath 58%
• Weakness 55%
• Unusual fatigue 43%
• Cold sweat 39%
• Dizziness 39%
• 43% did NOT have chest pain



Total 775 patients 593 men + 182 women182 matched men
Archives of Cardiovascular Disease (2015)

Totale (N=1289) mediana, IQR
Maschi (N=952) mediana, IQR
Femmine (N=337) mediana, IQR
p
Età 66 (57 – 75) 64 (55 – 72) 74 (65 – 81) <0.001
Glicemia ingr (mg/dl)
145 (121 – 184) 142 (119 – 176) 154 (131 – 195) 0.001
GFR ingr(ml/min)
69 (50 – 85) 72 (54 – 87) 60 (43 – 76) <0.001
Tempo ischemia (ore)
3.38 (2.35 – 5.29) 3.26 (2.30 – 5.12) 4.05 (3.00 – 5.57) <0.001
FEVS (%) 52 (43 – 57) 52 (44 – 57) 52 (42 – 57) N.S.
Troponina(mcg/ml)
57 (24 – 112) 57 (25 – 119) 58 (26 – 94) N.S.
Tabella descrittiva variabili continue
Dati registro STEMI Trieste 12.2003 – 12.2012Analisi di Genere

Totale (N=1289) Maschi (N=952) Femmine (N=337) p
Età > 75 27.3% 19.1% 49.8% <0.001
Diabete 22.6% 22.0% 24.4% N.S.
Killip 3 - 4 11.7% 10.5% 14.8% 0.035
Tempo isch > 6 h 14.6% 13.1% 18.8% 0.026
SCC 23.2% 21.3% 28.6% 0.007
FEVS < 35% 8.9% 8.4% 10.6% N.S.
ACR 6.5% 7.1% 5.0% N.S.
Tabella descrittiva variabili discrete
Dati registro STEMI Trieste Dicembre 2003 - Dicembre 2012Analisi di genere

Totale (N=1289) Maschi (N=952) Femmine (N=337) p
Mortalità intraospedaliera
6.8% 5.5% 10.4% 0.002
Mortalità a 30 giorni 7.5% 6.1% 11.6% 0.001
Mortalità totale(f-up mediano 48 mesi)
13.3% 11.6% 18.4% 0.001
Mortalità in base al sesso
Dati registro STEMI Trieste Dicembre 2003 - Dicembre 2012Analisi di genere

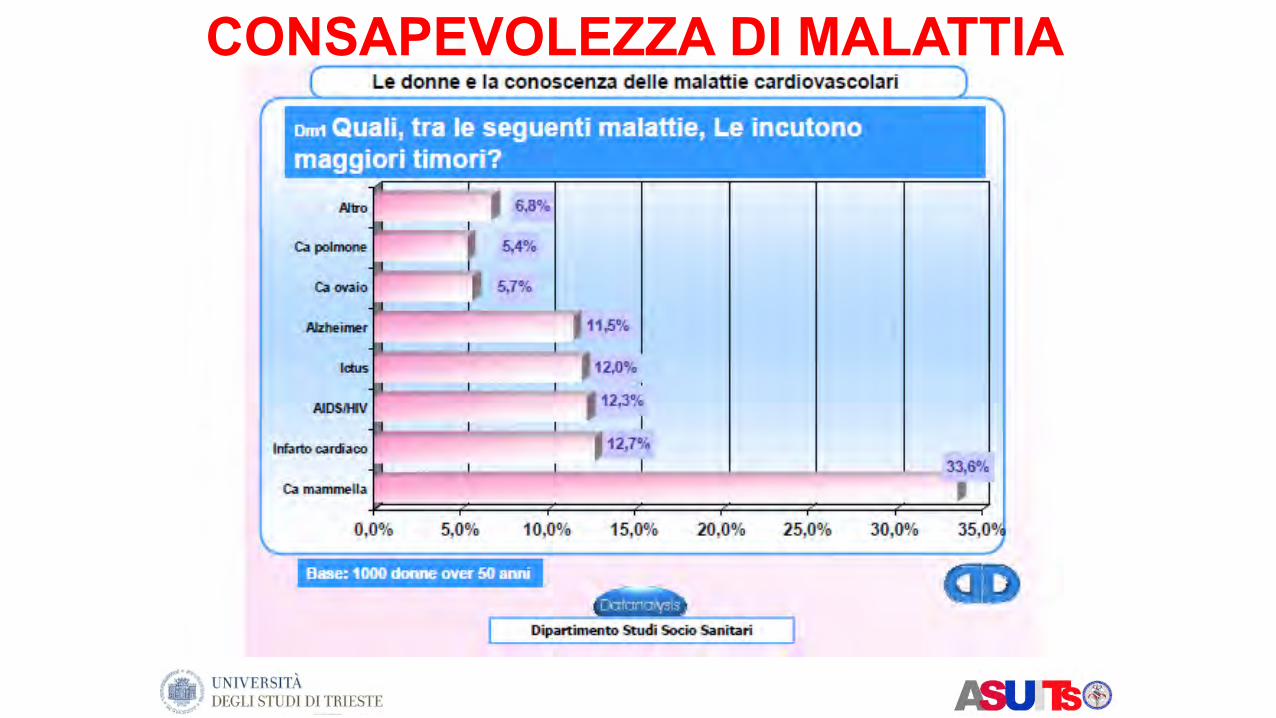
CONSAPEVOLEZZA DI MALATTIA

Non tutte le DCM sono geneticamente determinate
Merlo M. et al. Eur J Heart Fail. In press

Shore S et al. JACC HF 2015
ETIOLOGICAL CLASSIFICATION

Takotsubo Cardiomyopathy• Reported by Japanese in 1990
• “Broken heart”, apical ballooning, stress CM
• Octopus trap appearance
• Up to 90% women, age > 60
• 70% with Severe emotional stress
• Troponin moderately elevated
• Echo resolution within ~ 30 days
Rivera et al. Med Sci Monit, 2011;17(6):RA135-147

Post-partum Cardiomyopathy
• 1/4000 live US births
• 1 month pre or 5 months post-partum
• Increased maternal age, multiparity, multiple gestations, preeclampsia/HTN
• 2.9x more likely in AA women
• ?viral, immune, stress, prolactin, tocolysis, hereditary
• Usual HF therapy, until resolved
• 4% need transplant
• Future pregnancies NOT recommended

Heart Failure and Chemotherapy
• Breast cancer most common malignancy
• Adriamycin• Dose dependent cardiotoxicity (>450 mg/m2)
• Clinical HF in 2-7% of pts; increases over time
• Herceptin• Reduces recurrence rate up to 50%
• CHF in 2-4%; up to 3-27% after combination
• Esp in pts with elevated troponin/BNP
• Cyclophosphamide, XRT

FIGURE 3. Cardiovascular death free survival.
FIGURE 1. Longitudinal trends during follow-up. Red lines are for females and black lines are for males. NYHA: New York Heart Association class; LVEF: Left ventricular ejection fraction; LVEDD: Left ventricular end-diastolic diameter; LVEDV: left ventricular end-diastolic volume; MR: mitral regurgitation; RFP: restrictive filling pattern.
TABLE 2. Events
All( N = 803 )
Males( N= 576, 72 % )
Females( N=227, 28% )
P value(Kaplan- Meier)
Mean follow-up (months)
All cause mortality/ heart transplant n(%)
Heart transplant n (%)
Cardiovascular death n (%)
Pump failure death n (%)
Unexpected sudden death n (%)
Unknown cause death n ( % )
Appropriate intervention of ICD N=40N (% of implanted patients 132: 102 men, 30 women)
FIGURE 2. Total death/ heart transplantation free survival.

FIGURE 3. Cardiovascular death free survival.
FIGURE 1. Longitudinal trends during follow-up. Red lines are for females and black lines are for males. NYHA: New York Heart Association class; LVEF: Left ventricular ejection fraction; LVEDD: Left ventricular end-diastolic diameter; LVEDV: left ventricular end-diastolic volume; MR: mitral regurgitation; RFP: restrictive filling pattern.
TABLE 2. Events
All( N = 803 )
Males( N= 576, 72 % )
Females( N=227, 28% )
P value(Kaplan- Meier)
Mean follow-up (months)
All cause mortality/ heart transplant n(%)
Heart transplant n (%)
Cardiovascular death n (%)
Pump failure death n (%)
Unexpected sudden death n (%)
Unknown cause death n ( % )
Appropriate intervention of ICD N=40N (% of implanted patients 132: 102 men, 30 women)
FIGURE 2. Total death/ heart transplantation free survival.

LVRR after OPT
Aimo et al. JACC HF 2017

Fa-Hui Yin et al. Plos One 2017
Han et al. Plos One 2017
LVRR after CRT

32,3 ‰
8,6 ‰
102,2 ‰
38,4 ‰


In an analysis of the Medicare Claims database:women were 3 times less likely than men to receive an ICD for primary preventionand 2,5 times less likely tha men to receive an ICD for secondary prevention !!!
No longer racial disparities… sex differences persisted

Likelihood of receiving evidence-based treatment

Keller et al Can J Cardiol 2016
HFpEF: HF of ELDERLY

Gori M et al. Eur J Heart Fail 2014
HFpEF: HF of WOMEN

HFpEF

HFpEF

HFpEF

Characteristic Women (n=2491) Men (n=1637) P Value
Age, y 72±7 71±7 <0.001Obesity*, % 46 35 <0.001Heart failure cause, % ischemic 19 34 <0.001Hypertension, % 91 85 <0.001Atrial fibrillation, % 27 33 <0.001Diabetes mellitus, % 28 27 0.74
Chronic obstructive pulmonary disease, %
8 13 <0.001
Smoking, % 9 32 <0.001NYHA class II/III/IV, % 20/77/2 22/75/3 0.006
Hospitalization in the last 6 mo, % 44 45 0.49
Ejection fraction, % 61±9 58±9 <0.001Minnesota living with heart failure
score45±21 39±21 <0.001
Median (Q1–Q3) NT-pro-BNP, pg/mL 301 (126–897) 413 (155–1051) <0.001Hemoglobin, g/dL 13.5±1.8 14.5±1.9 <0.001Anemia†, % 11 16 <0.001Chronic kidney disease‡, % 34 26 <0.001
Medications
Loop diuretic, % 51 53 0.08
Thiazide diuretic, % 41 34 <0.001Spironolactone, % 15 17 0.08
Angiotensin-converting enzymeinhibitor, %
23 29 <0.001
Digoxin, % 12 16 0.006
β-Blocker, % 59 59 0.93
Antiarrythmic, % 8 11 0.003
Calcium channel blocker, % 42 37 <0.001Nitrate, % 25 30 <0.001Oral anticoagulant, % 55 64 <0.001Aspirin, % 52 59 <0.001Lipid lowering, % 28 35 <0.001
Lam C et al. Circulation Heart Fail 2012
WOMEN vs. MEN in HFpEF

Outcome
Event Rate Per 100 Patient-Years Multivariable Analysis*
Women Men HR (95% CI), Women vs Men PValue
All-cause death 4.32 6.72 0.70 (0.59–0.83) <0.001All-cause hospitalization or death 19.42 25.05 0.80 (0.72–0.89) <0.001
Cardiovascular hospitalization or death 11.76 15.97 0.81 (0.72–0.92) 0.001
Noncardiovascular hospitalization or death 9.89 12.40 0.78 (0.69–0.90) <0.001
Heart failure hospitalization or death 4.43 5.02 0.94 (0.77–1.14) 0.51
First all-cause hospitalization 18.43 23.14 0.77 (0.66–0.89) <0.001
Lam C et al. Circulation Heart Fail 2012
WOMEN vs. MEN in HFpEF

Ziaeian and Fonarow, Nat Cardiol Rev. 2016
WOMEN vs. MEN in HFpEF

Summary• Compared to men, women have several differences in HF:
• Physiology• Psychological• Social• Etiology of heart failure• Response to therapy
• HFeRF: typical of man; reduced mortality --> mostly in women (except ACS)
• HFpEF: typical of women and elderly; women have better survival than men but global survival has been unchanged (complex syndrome)
• HFpEF: increasing incidence
• Heart failure types more common in women• Diastolic HF, Takotsubo CM, pregnancy
• Women in HF: • understudied gap of knowledge• Precision medicine• Social changes

GRAZIE
Recommended

















