
CASE REPORT
Pyoderma gangrenosum occurring at the peri-ileal pouch-analanastomosis in a patient with ulcerative colitis: report of a case
Koji Tanaka • Toshimitsu Araki • Yoshiki Okita •
Hiroyuki Fujikawa • Mikio Kawamura •
Keiichi Uchida • Yasuhiko Mohri • Masato Kusunoki
Received: 25 April 2012 / Accepted: 3 October 2012
� Springer Japan 2012
Abstract Pyoderma gangrenosum (PG) is an idiopathic,
inflammatory, ulcerative skin disorder; the etiology and
pathogenesis of which are still poorly understood. It is one
of the most important extraintestinal manifestations that
can appear in the course of ulcerative colitis (UC).
Although skin ulcers with destructive and necrotizing
components are more commonly observed on the lower
extremities and trunk, PG at stomal sites (peri-stomal PG)
has been increasingly reported in patients with inflamma-
tory bowel diseases (IBDs), including UC. Although PG at
various surgical sites has been reported as an unusual
presentation of PG, postoperative PG developing at the
ileal pouch-anal anastomosis (IPAA) has not been reported
previously. We herein report the first published case of a
patient with UC who developed peri-anastomotic PG after
IPAA during the postoperative tapering of systemic
corticosteroids.
Keywords Pyoderma gangrenosum � Ulcerative
colitis � Ileal pouch-anal anastomosis
Case report
A 48-year-old female who had been diagnosed with ste-
roid-dependent chronic active UC 21 years prior was
referred to our department for surgical intervention. Med-
ical treatment had been initiated 21 years prior upon the
diagnosis of left-sided UC. Her past medical history
included corticosteroids, azathioprine and infliximab. She
had developed sepsis due to azathioprine-induced pancy-
topenia. The use of infliximab therapy to reduce the steroid
dose also failed. Corticosteroids were used not only to
control disease flare-ups but also to maintain remission.
She was being maintained on prednisolone (20 mg/day) at
the time of admission. She had steroid-dependent since her
diagnosis of UC, and the total steroid dosage was estimated
to be approximately 30,000 mg. However, she had no
apparent steroid-related complications before surgery.
She underwent a total proctocolectomy and ileal pouch-
anal anastomosis (IPAA) with loop ileostomy in June 2011.
Her postoperative course was uneventful. Intravenous
cortisol was administered at 200 mg/day perioperatively
for steroid coverage. Oral prednisolone was administered at
10 mg/day for weeks, and then tapered to 7.5 mg/day for
weeks.
Three months later, she visited our outpatient clinic
because of a rapidly increasing severe pain at her anus
which had begun a few days before her visit. She was on
oral prednisolone at 5 mg/day. On physical examination,
anal ulceration was found along the entire circumference of
the IPAA (Fig. 1a, b). Subsequent endoscopy revealed no
abnormality of the ileal mucosa in either the ileal pouch or
pre-pouch ileum (Fig. 1c). The ulcer was characterized by
an undermined border and a purulent necrotic base, which
was located at the anal skin without the involvement of the
ileal pouch mucosa. There was no anastomotic leakage
clinically or radiographically. There was no infectious or
neoplastic cause associated with this ulceration. She had no
skin disorders related to UC or steroid use prior to surgery.
Based on her history of associated systemic disease
(UC), her typical clinical presentation (a characteristic
painful skin ulcer) and the exclusion of other diseases, we
K. Tanaka (&) � T. Araki � Y. Okita � H. Fujikawa �M. Kawamura � K. Uchida � Y. Mohri � M. Kusunoki
Department of Gastrointestinal and Pediatric Surgery,
Mie University Graduate School of Medicine,
2-174 Edobashi, Tsu, Mie 514-8507, Japan
e-mail: [email protected]
123
Surg Today
DOI 10.1007/s00595-012-0463-7
considered this ulcerated lesion to be PG occurring at the
peri-IPAA. She had no ulcerated lesions at the peri-ileos-
tomy site or other surgical sites. Her lower extremities and
trunk, typical sites of PG, were also normal.
Both systemic (oral prednisolone at 40 mg/day) and
topical steroid therapy were initiated for her perianastomotic
PG. She responded rapidly to the steroid therapy. The anal
ulcer was completely healed weeks after the beginning of
steroid therapy. As a consequence, the anal ulcer and pain
disappeared (Fig. 1d). The dose of prednisolone was reduced
to 30 mg/day for week, and then tapered to 20 mg/day for an
additional week. The steroid dose was gradually reduced
thereafter. On oral prednisolone at 10 mg/day, the patient
had no recurrence of peri-IPAA PG at the month follow-up
examination. Radiological examination of the pouch using a
water-soluble contrast agent indicated no evidence of leaks
of the pouch or anastomosis, stricture of anastomosis or
abnormality of the evacuation status. Accordingly, we plan
to close the loop ileostomy.
Discussion
In 1930, Brunsting reported the first five patients with PG,
who presented with rapidly progressive and painful sup-
purative skin ulcers with necrotic and undermined borders
[1]. To date, the etiology and pathogenesis of PG are still
poorly understood [2, 3]. PG is also known to be one of the
most important extraintestinal manifestations of UC, the
frequency of which has been reported to vary between 1
and 10 % [4, 5].
Since the initial report, PG has been described at various
sites in the literature, although it classically occurs on the
lower legs, trunk and upper extremities and at peri-stomal
sites. PG can occur anywhere on the body. Unusual pre-
sentations of PG related to surgical sites have also been
reported in patients who have undergone splenectomy,
cesarean section, gastrectomy tube insertion, pacemaker
insertion and coronary artery bypass grafting [6].
In our series, a total of 246 consecutive UC patients with
total proctocolectomy and IPAA were identified between
September 2000 and December 2011. PG was observed in
12 (4.9 %) of these 246 patients. Four patients were
diagnosed with PG before surgery, and eight had peristo-
mal PG after surgery. This is the only case of peri-IPAA
PG in our experience. To the best of our knowledge, this is
also the first report of postoperative peri-IPAA PG in UC in
the literature.
The precise etiology and pathogenesis of PG remain
unclear. The association of PG with autoimmune disorders
and the successful response to immunosuppressant agents
suggest that immunological disturbances may play an
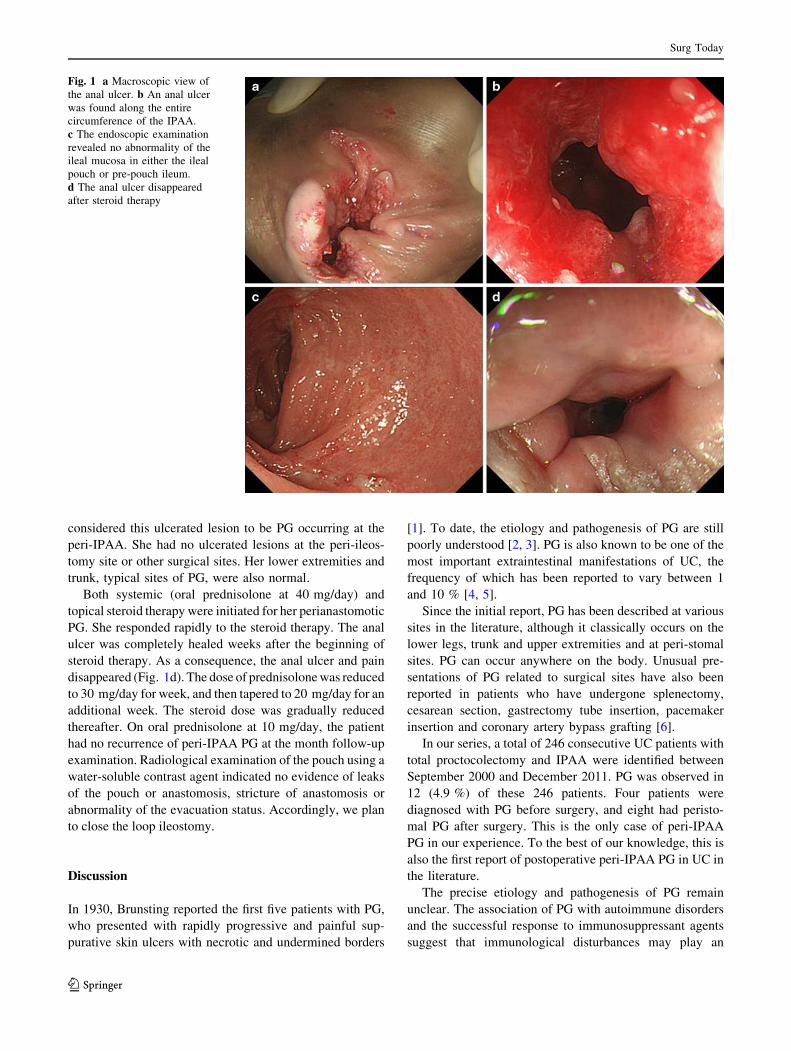
Fig. 1 a Macroscopic view of
the anal ulcer. b An anal ulcer
was found along the entire
circumference of the IPAA.
c The endoscopic examination
revealed no abnormality of the
ileal mucosa in either the ileal
pouch or pre-pouch ileum.
d The anal ulcer disappeared
after steroid therapy
Surg Today
123

important role in the pathogenesis of PG. Moreover, the
response to therapy (immunosuppressants) is one of the
important factors for the diagnosis of PG, in addition to the
clinical history, clinical features, ulcer features and asso-
ciated diseases [3].
Accordingly, the ulcerated lesion at the peri-IPAA site
presented in the present report was diagnosed as PG based
on its response to steroids, the patient’s clinical history,
the clinical features and the ulcer features, although its
anatomical location was extremely unusual. The pathergy
phenomenon after surgical trauma may be associated with
the pathogenesis of both peri-stomal PG and postoperative
peri-IPAA PG. In our case, the peri-IPAA PG appeared to
develop during the steroid tapering after total proctoco-
lectomy for steroid-dependent UC. PG can occur before,
during, or after the onset of UC. Whether the disease
activity of UC is related to PG is controversial. Poritz and
colleagues [7] reported that UC patients with residual
disease in the rectum after total colectomy experienced
peristomal PG just after the end of their steroid taper.
They also showed that the UC patients whose peristomal
PG resolved with infliximab had recurrence during the
drug withdrawal. These findings suggest that the devel-
opment or recurrence of PG may be associated with the
withdrawal or reduction of treatment, such as steroids or
infliximab.
The mainstay of the management of PG is immuno-
suppression. Currently, there is no standard treatment or
guideline for PG, since multiple therapeutic options, such
as corticosteroids, cyclosporine, azathioprine, cyclophos-
phamide and tacrolimus have been used without uniform
efficacy. Recently, several case reports and randomized
trials have demonstrated a favorable response of patients
to anti-TNF-a drugs, including infliximab [8, 9], etaner-
cept [10] and adalimumab [11, 12] or topical tacrolimus
[13, 14].
Although a causal relationship between the occurrence
of PG and the reduction of steroids after restorative proc-
tocolectomy has not been established, careful steroid
tapering for patients with steroid-dependent UC should be
considered [15]. An optimal steroid taper regimen might
prevent the occurrence of PG in such cases.
Conflict of interest The authors have no conflict of interest to
disclose.
References
1. Brunsting LA, Goeckerman WH, O’Leary PA. Pyoderma gan-
grenosum: clinical and experimental observations in five cases
occurring in adults. Arch Dermatol Syphilol. 1930;22:655–80.
2. Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G.
Pyoderma gangrenosum: an updated review. J Eur Acad Der-
matol Venereol. 2009;23:1008–17.
3. Hadi A, Lebwohl M. Clinical features of pyoderma gangrenosum
and current diagnostic trends. J Am Acad Dermatol. 2011;
64:950–4.
4. Lebwohl M, Lebwohl O. Cutaneous manifestations of inflam-
matory bowel disease. Inflamm Bowel Dis. 1998;4:142–8.
5. Yuksel I, Basar O, Ataseven H, Ertugrul I, Arhan M, Ibis M,
et al. Mucocutaneous manifestations in inflammatory bowel dis-
ease. Inflamm Bowel Dis. 2009;15:546–50.
6. Ahmadi S, Powell FC. Pyoderma gangrenosum: uncommon
presentations. Clin Dermatol. 2005;23:612–20.
7. Poritz LS, Lebo MA, Bobb AD, Ardell CM, Koltun WA. Man-
agement of peristomal pyoderma gangrenosum. J Am Coll Surg.
2008;206:311–5.
8. Brooklyn TN, Dunnill MG, Shetty A, Bowden JJ, Williams JD,
Griffiths CE, et al. Infliximab for the treatment of pyoderma
gangrenosum: a randomised, double blind, placebo controlled
trial. Gut. 2006;55:505–9.
9. Miller J, Yentzer BA, Clark A, Jorizzo JL, Feldman SR. Pyo-
derma gangrenosum: a review and update on new therapies. J Am
Acad Dermatol. 2010;62:646–54.
10. Kim FS, Pandya AG. The use of etanercept in the treatment of
peristomal pyoderma gangrenosum. Clin Exp Dermatol.
2012;37:442–3.
11. Hubbard VG, Friedmann AC, Goldsmith P. Systemic pyoderma
gangrenosum responding to infliximab and adalimumab. Br J
Dermatol. 2005;152:1059–61.
12. Carinanos I, Acosta MB, Domenech E. Adalimumab for pyo-
derma gangrenosum associated with inflammatory bowel disease.
Inflamm Bowel Dis. 2011;17:E153–4.
13. Marzano AV, Trevisan V, Lazzari R, Crosti C. Topical tacroli-
mus for the treatment of localized, idiopathic, newly diagnosed
pyoderma gangrenosum. J Dermatol Treat. 2010;21:140–3.
14. Altieri M, Vaziri K, Orkin BA. Topical tacrolimus for parastomal
pyoderma gangrenosum: a report of two cases. Ostomy Wound
Manag. 2010;56:56–9.
15. Okita Y, Miki C, Yoshiyama S, Otake K, Araki T, Uchida K,
et al. Neutrophil dysfunction in steroid-overdosed patients with
ulcerative colitis: potential relevance of macrophage migration
inhibitory factor to increased postoperative morbidity. Surg
Today. 2011;41:1504–11.
Surg Today
123
Recommended

















