10/4/2013
1
C e c e l i a E . S c h m a l b a c h , M D , M S , FA C S
A s s o c i a t e P r o f e s s o r
P r o g r a m D i r e c t o r
H e a d & N e c k - M i c r o v a s c u l a r S u r g e r y
T h e U n i v . o f A l a b a m a i n B i r m i n g h a m
ORAL CANCER
Sisson 2013
GOALS
• Oral Cavity Anatomy
• Staging• Elective ND
• Sentinel Lymph Node Biopsy
• Treatment• Surgery vs. XRT +/- Chemotherapy
• Managing the Neck
• Adjuvant therapy
• Tx of Lip Cancer
• Reconstruction
• Pearls
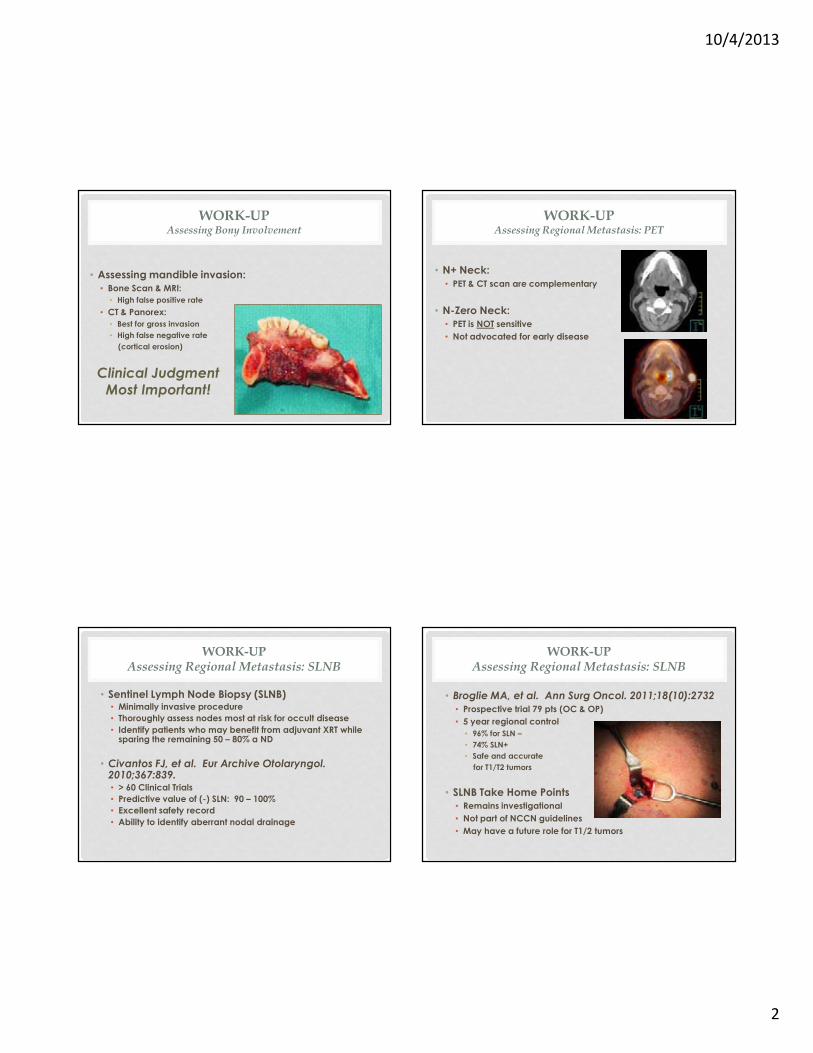
ORAL CAVITY SUBSITES
• Mucosal Lip
• Buccal Mucosa
• Lower Alveolar Ridge
• Upper Alveolar Ridge
• Retromolar Trigone (RMT)
• Floor of Mouth (FOM)
• Hard Palate (HP)
• Oral Tongue
• LIP CANCER ACCOUNTS FOR 25-30% OF ALL ORAL CAVITY MALIGNANCIES
WORK-UP
• History & Physical
• Biopsy
• HPV NOT routine (<5%)
• Neck CT or MRI as indicated
• Chest Imaging
• Consider PET for Stage III/IV
• EUA & endoscopy as clinically indicated
• Preanesthesia work-up
• Dental evaluation
• Speech & nutrition evaluation
NCCN Practice Guidelines in Oncology v.2.2013
10/4/2013
2
WORK-UPAssessing Bony Involvement
• Assessing mandible invasion:
• Bone Scan & MRI:
• High false positive rate
• CT & Panorex:
• Best for gross invasion
• High false negative rate
(cortical erosion)
Clinical Judgment
Most Important!
WORK-UPAssessing Regional Metastasis: PET
• N+ Neck:
• PET & CT scan are complementary
• N-Zero Neck:
• PET is NOT sensitive
• Not advocated for early disease
WORK-UPAssessing Regional Metastasis: SLNB
• Sentinel Lymph Node Biopsy (SLNB)• Minimally invasive procedure
• Thoroughly assess nodes most at risk for occult disease
• Identify patients who may benefit from adjuvant XRT while sparing the remaining 50 – 80% a ND
• Civantos FJ, et al. Eur Archive Otolaryngol. 2010;367:839.• > 60 Clinical Trials
• Predictive value of (-) SLN: 90 – 100%
• Excellent safety record
• Ability to identify aberrant nodal drainage
WORK-UPAssessing Regional Metastasis: SLNB
• Broglie MA, et al. Ann Surg Oncol. 2011;18(10):2732
• Prospective trial 79 pts (OC & OP)
• 5 year regional control
• 96% for SLN –
• 74% SLN+
• Safe and accurate
for T1/T2 tumors
• SLNB Take Home Points
• Remains investigational
• Not part of NCCN guidelines
• May have a future role for T1/2 tumors
10/4/2013
3
WORK-UPAssessing Regional Metastasis
• Low risk patients
• < 2cm (T1)
• Minimal depth of invasion (< 4mm)
• Favorable histology
• High risk patients
• Retrospective studies demonstrate decreased regional &
distant recurrence with ND • Yuen. Head Neck 1997;19:583
• Oreste. Head Neck 1996;18:566
• 1/3 N-zero H&N patients had occult disease (1/3 with ECS)• Pitman. Arch Otolaryngol. 1997;123:917.
• “Watchful waiting” leads to increased regional recurrence (33% vs 12%) and were often unresectable (76%)
• Kligerman. Am J Surg. 1994;168:391.
WHEN DO YOU PERFORM AN END?
• High incidence of occult nodal disease
• >20% risk
• Depth of invasion > 4mm
• Need for surgical violation of the neck
• Poor patient compliance
• Obese or muscular neck (difficult to follow clinically)
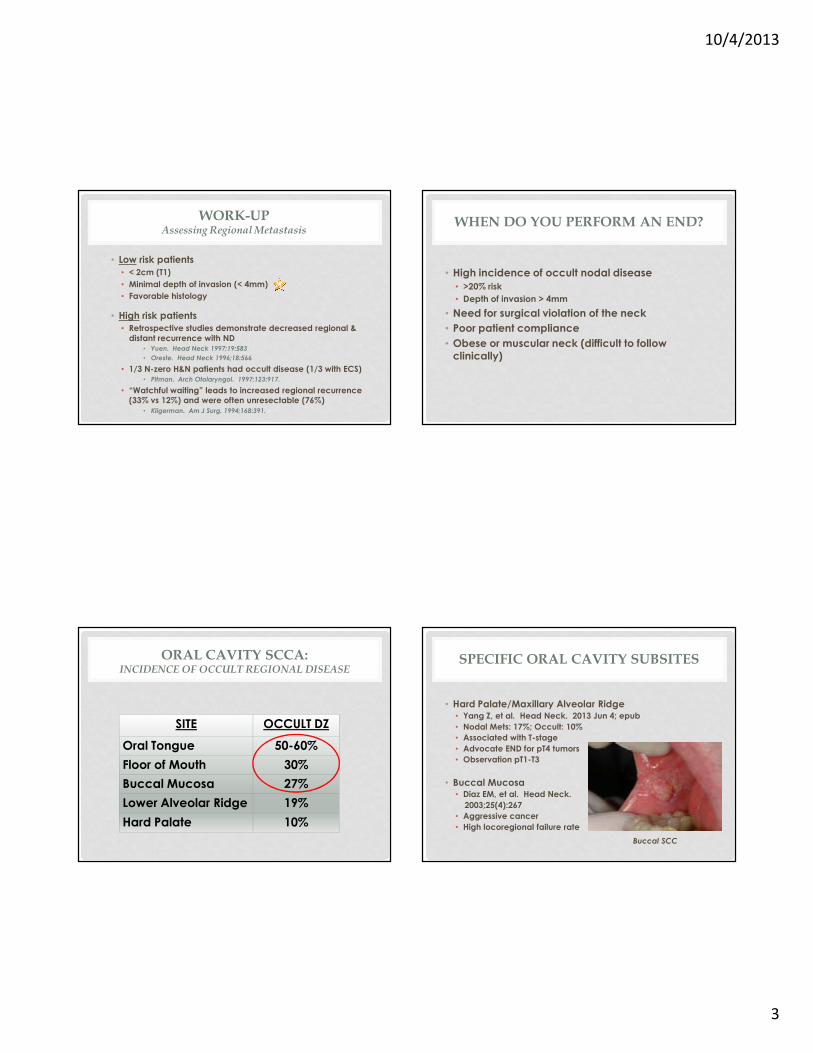
ORAL CAVITY SCCA:INCIDENCE OF OCCULT REGIONAL DISEASE
SITE OCCULT DZ
Oral Tongue 50-60%
Floor of Mouth 30%
Buccal Mucosa 27%
Lower Alveolar Ridge 19%
Hard Palate 10%
SPECIFIC ORAL CAVITY SUBSITES
• Hard Palate/Maxillary Alveolar Ridge• Yang Z, et al. Head Neck. 2013 Jun 4; epub
• Nodal Mets: 17%; Occult: 10%
• Associated with T-stage
• Advocate END for pT4 tumors
• Observation pT1-T3
• Buccal Mucosa• Diaz EM, et al. Head Neck.
2003;25(4):267
• Aggressive cancer
• High locoregional failure rate
Buccal SCC
10/4/2013
4
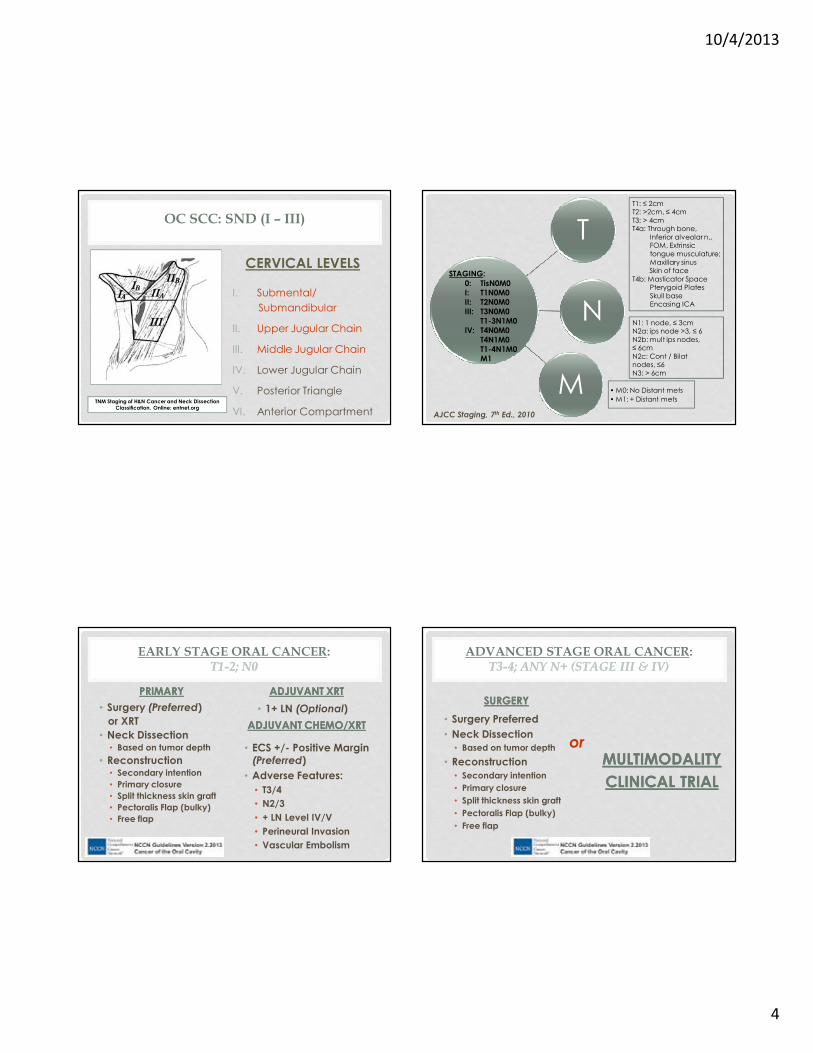
OC SCC: SND (I – III)
CERVICAL LEVELS
I. Submental/
Submandibular
II. Upper Jugular Chain
III. Middle Jugular Chain
IV. Lower Jugular Chain
V. Posterior Triangle
VI. Anterior CompartmentTNM Staging of H&N Cancer and Neck Dissection
Classification. Online: entnet.org
T
N
M • M0: No Distant mets
• M1: + Distant mets
STAGING:
0: TisN0M0
I: T1N0M0
II: T2N0M0
III: T3N0M0
T1-3N1M0
IV: T4N0M0
T4N1M0
T1-4N1M0
M1
AJCC Staging, 7th Ed., 2010
T1: ≤ 2cm T2: >2cm, ≤ 4cm
T3: > 4cm T4a: Through bone,
Inferior alveolar n., FOM, Extrinsic
tongue musculature;
Maxillary sinusSkin of face
T4b: Masticator SpacePterygoid Plates
Skull baseEncasing ICA
N1: 1 node, ≤ 3cmN2a: ips node >3, ≤ 6
N2b: mult ips nodes, ≤ 6cm
N2c: Cont / Bilatnodes, ≤6
N3: > 6cm
EARLY STAGE ORAL CANCER: T1T1--2; N02; N0
PRIMARYPRIMARY
• Surgery (Preferred)
or XRT
• Neck Dissection• Based on tumor depth
• Reconstruction• Secondary intention
• Primary closure
• Split thickness skin graft
• Pectoralis Flap (bulky)
• Free flap
ADJUVANT XRTADJUVANT XRT
• 1+ LN (Optional)
ADJUVANT CHEMO/XRTADJUVANT CHEMO/XRT
• ECS +/- Positive Margin (Preferred)
• Adverse Features:
• T3/4
• N2/3
• + LN Level IV/V
• Perineural Invasion
• Vascular Embolism
ADVANCED STAGE ORAL CANCER: T3T3--4; ANY N+ (STAGE III & IV) 4; ANY N+ (STAGE III & IV)
SURGERYSURGERY
• Surgery Preferred
• Neck Dissection
• Based on tumor depth
• Reconstruction
• Secondary intention
• Primary closure
• Split thickness skin graft
• Pectoralis Flap (bulky)
• Free flap
MULTIMODALITY MULTIMODALITY
CLINICAL TRIALCLINICAL TRIAL
or
10/4/2013
5
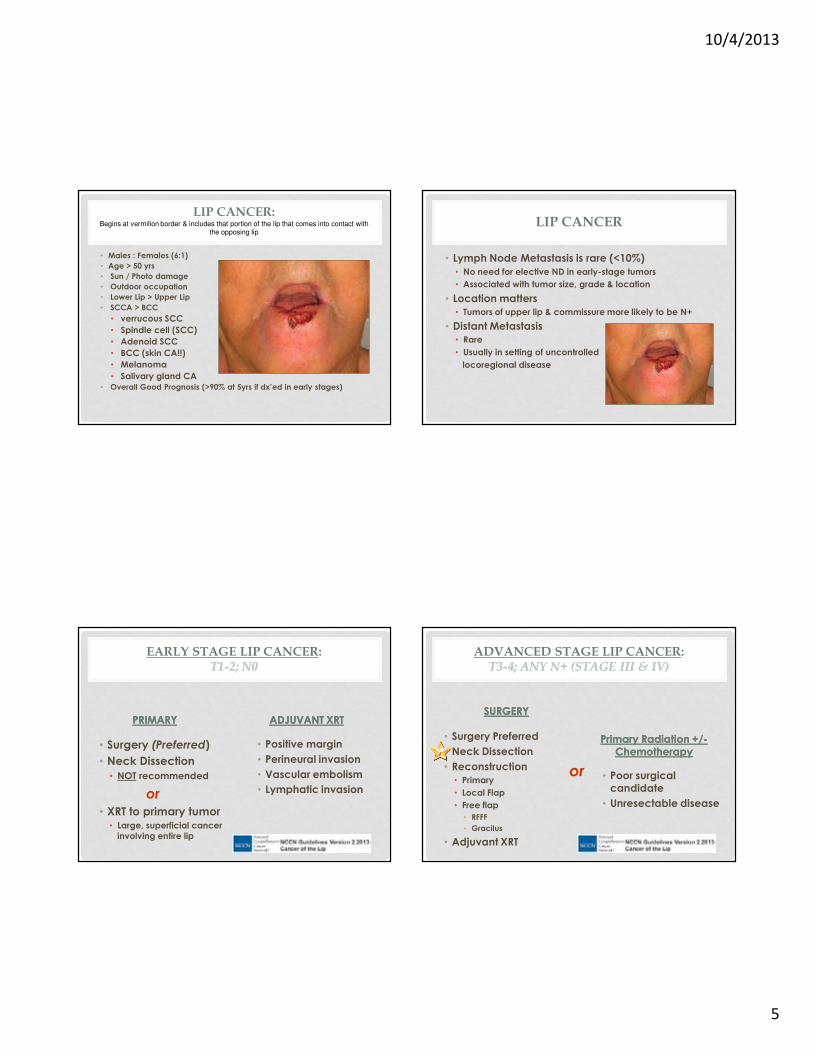
LIP CANCER:Begins at vermilion border & includes that portion of the lip that comes into contact with
the opposing lip
• Males : Females (6:1)
• Age > 50 yrs
• Sun / Photo damage
• Outdoor occupation
• Lower Lip > Upper Lip
• SCCA > BCC
• verrucous SCC
• Spindle cell (SCC)
• Adenoid SCC
• BCC (skin CA!!)
• Melanoma
• Salivary gland CA
• Overall Good Prognosis (>90% at 5yrs if dx’ed in early stages)
LIP CANCER
• Lymph Node Metastasis is rare (<10%)
• No need for elective ND in early-stage tumors
• Associated with tumor size, grade & location
• Location matters
• Tumors of upper lip & commissure more likely to be N+
• Distant Metastasis
• Rare
• Usually in setting of uncontrolled
locoregional disease
EARLY STAGE LIP CANCER: T1T1--2; N02; N0
PRIMARYPRIMARY
• Surgery (Preferred)
• Neck Dissection
• NOT recommended
or
• XRT to primary tumor• Large, superficial cancer
involving entire lip
ADJUVANT XRTADJUVANT XRT
• Positive margin
• Perineural invasion
• Vascular embolism
• Lymphatic invasion
ADVANCED STAGE LIP CANCER: T3T3--4; ANY N+ (STAGE III & IV) 4; ANY N+ (STAGE III & IV)
SURGERYSURGERY
• Surgery Preferred
• Neck Dissection
• Reconstruction
• Primary
• Local Flap
• Free flap
• RFFF
• Gracilus
• Adjuvant XRT
Primary Radiation +/Primary Radiation +/--ChemotherapyChemotherapy
or • Poor surgical candidate
• Unresectable disease
10/4/2013
6
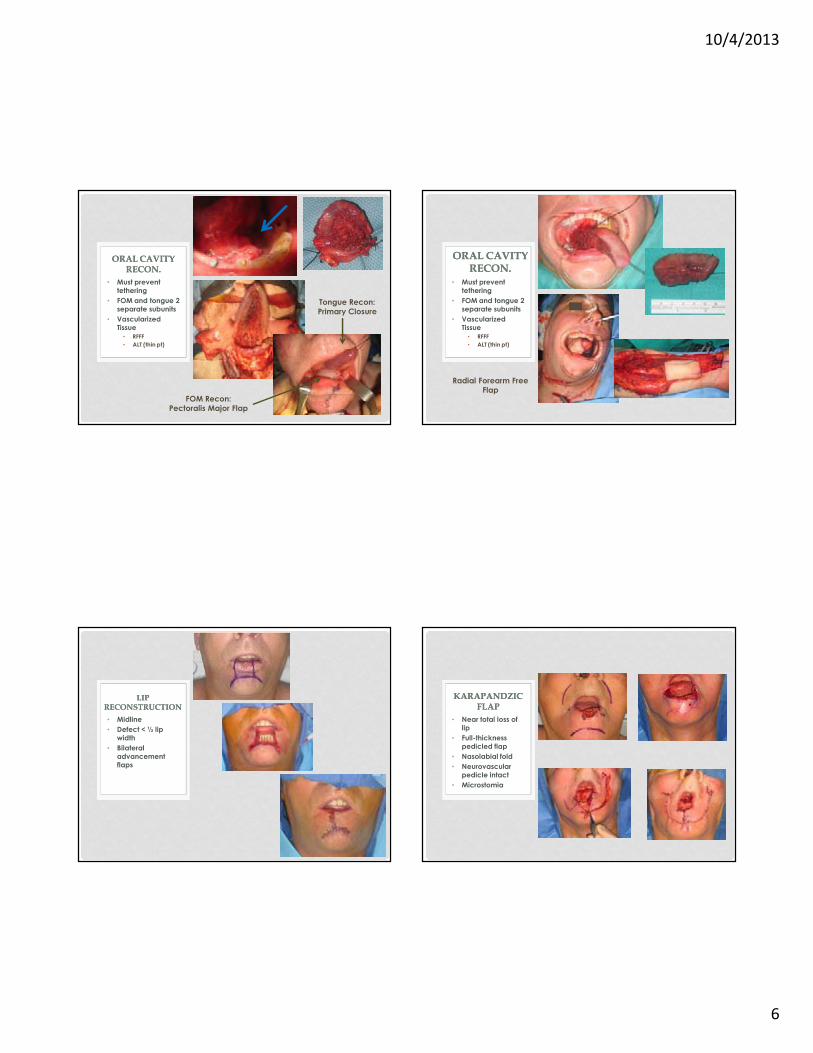
FOM Recon:
Pectoralis Major Flap
• Must prevent
tethering
• FOM and tongue 2
separate subunits
• Vascularized
Tissue
• RFFF
• ALT (thin pt)
ORAL CAVITY ORAL CAVITY
RECON.RECON.
Tongue Recon:
Primary Closure
Radial Forearm Free
Flap
• Must prevent
tethering
• FOM and tongue 2
separate subunits
• Vascularized
Tissue
• RFFF
• ALT (thin pt)
ORAL CAVITY ORAL CAVITY RECON.RECON.
• Midline
• Defect < ½ lip
width
• Bilateral
advancement
flaps
LIP LIP
RECONSTRUCTIONRECONSTRUCTION
• Near total loss of
lip
• Full-thickness
pedicled flap
• Nasolabial fold
• Neurovascular
pedicle intact
• Microstomia
KARAPANDZICKARAPANDZIC
FLAPFLAP
10/4/2013
7
ORAL CAVITY SCC PEARLS
1. Surgery is preferred primary choice
2. Depth of invasion (4mm) dictates and 20% risk of nodal metastasis = need for prophylactic neck treatment• Selective ND (I – III)
• XRT to the neck
3. Oral tongue with floor of mouth defects require vascularized tissue for reconstruction.
LIP CANCER PEARLS
• Lower lip
• Presents early
• Excellent prognosis; high cure rate
• Upper lip & commissure
• More aggressive disease
• Lymph node metastasis rare: END only for advanced stage disease
• Surgery and XRT have comparable cure rates for early stage disease
QUESTIONS ???
Recommended