T1 colonic carcinoma – Is endoscopic resection sufficient?
HC Yip
JHGR 21/7/2012
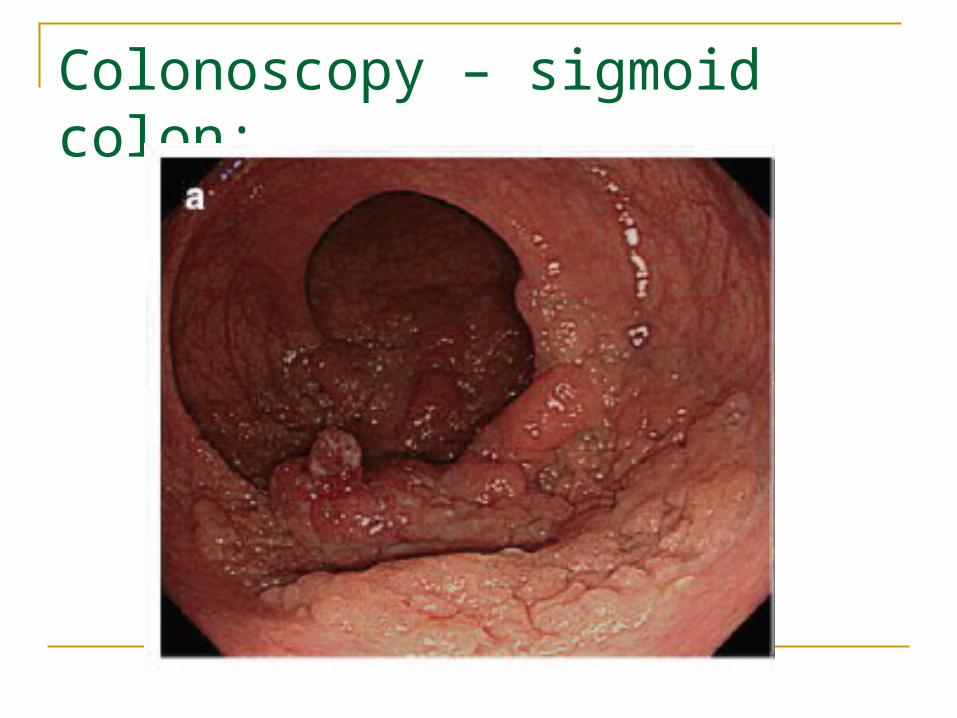
Colonoscopy – sigmoid colon:
Questions
1. Can we remove this lesion completely with endoscope?
2. If pathology confirms invasive carcinoma, is endoscopic resection sufficient? Do we need formal surgical resection?
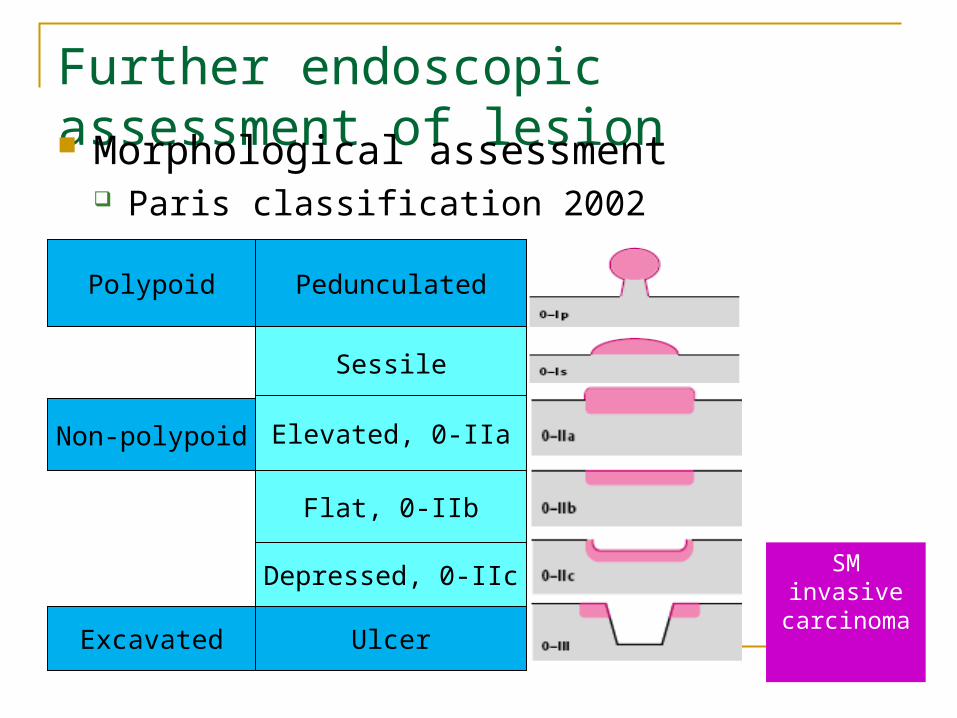
Further endoscopic assessment of lesion Morphological assessment
Paris classification 2002
Pedunculated
Sessile
Polypoid
Elevated, 0-IIa
Flat, 0-IIb
Depressed, 0-IIc
Ulcer
Non-polypoid
Excavated
SM invasive carcinoma
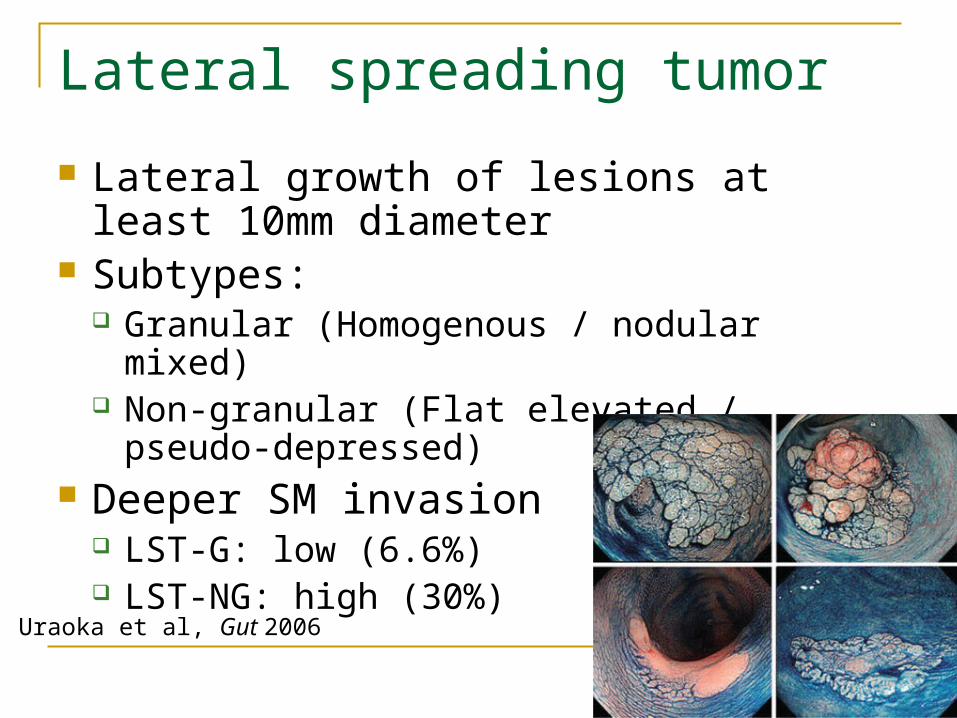
Lateral spreading tumor
Lateral growth of lesions at least 10mm diameter
Subtypes: Granular (Homogenous / nodular mixed) Non-granular (Flat elevated / pseudo-
depressed) Deeper SM invasion
LST-G: low (6.6%) LST-NG: high (30%)
Uraoka et al, Gut 2006
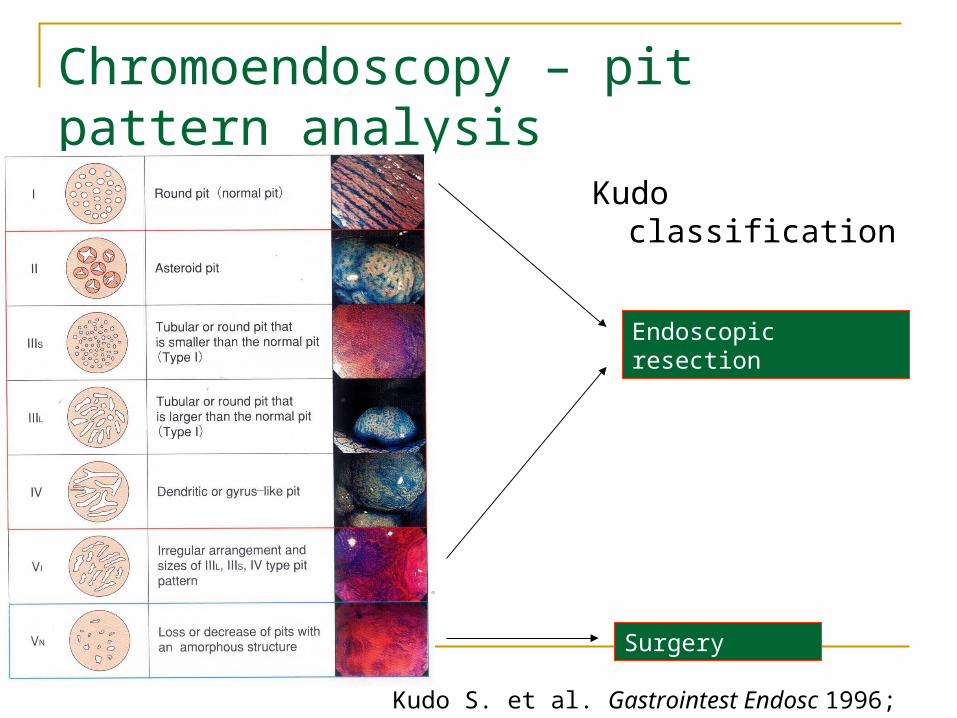
Chromoendoscopy – pit pattern analysis
Kudo classification
Endoscopic resection
Surgery
Kudo S. et al. Gastrointest Endosc 1996; 44: 8-14
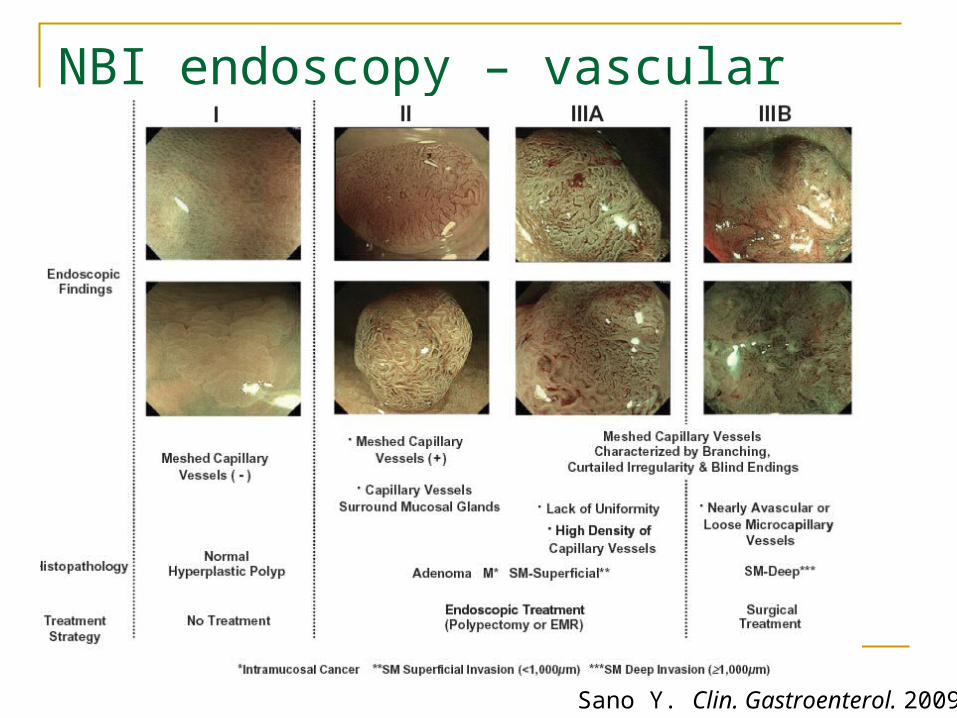
NBI endoscopy – vascular pattern analysis
Sano Y. Clin. Gastroenterol. 2009
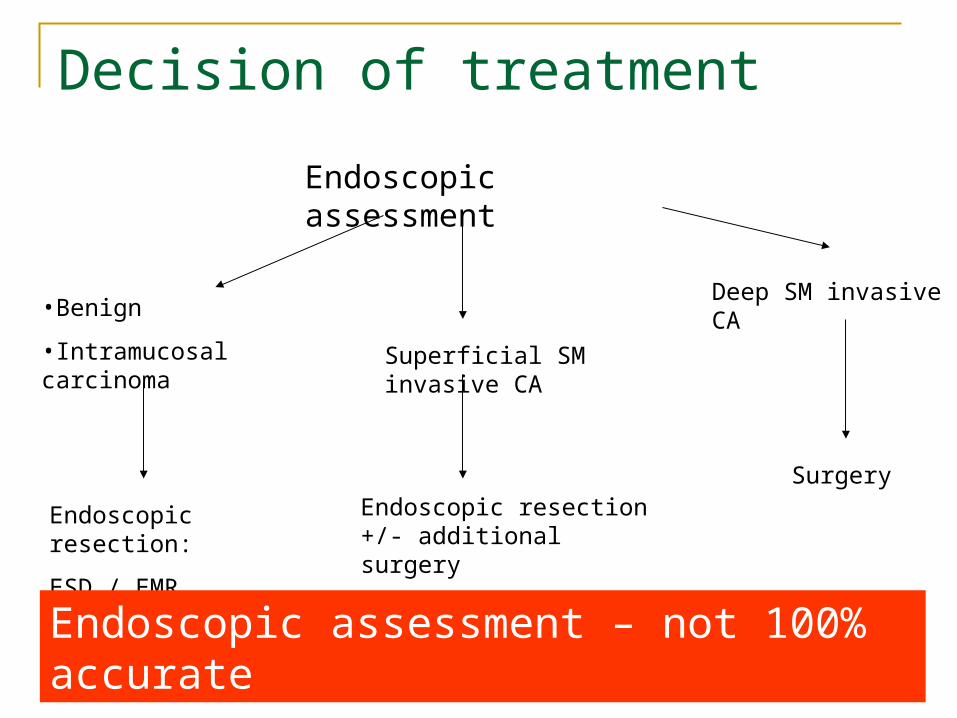
Decision of treatment
Endoscopic assessment
•Benign
•Intramucosal carcinoma
Endoscopic resection:
ESD / EMR
Superficial SM invasive CA
Endoscopic resection +/- additional surgery
Deep SM invasive CA
Surgery
Endoscopic assessment – not 100% accurate
Endoscopic resection
Endoscopic mucosal resection (EMR)
Endoscopic submucosal dissection (ESD)
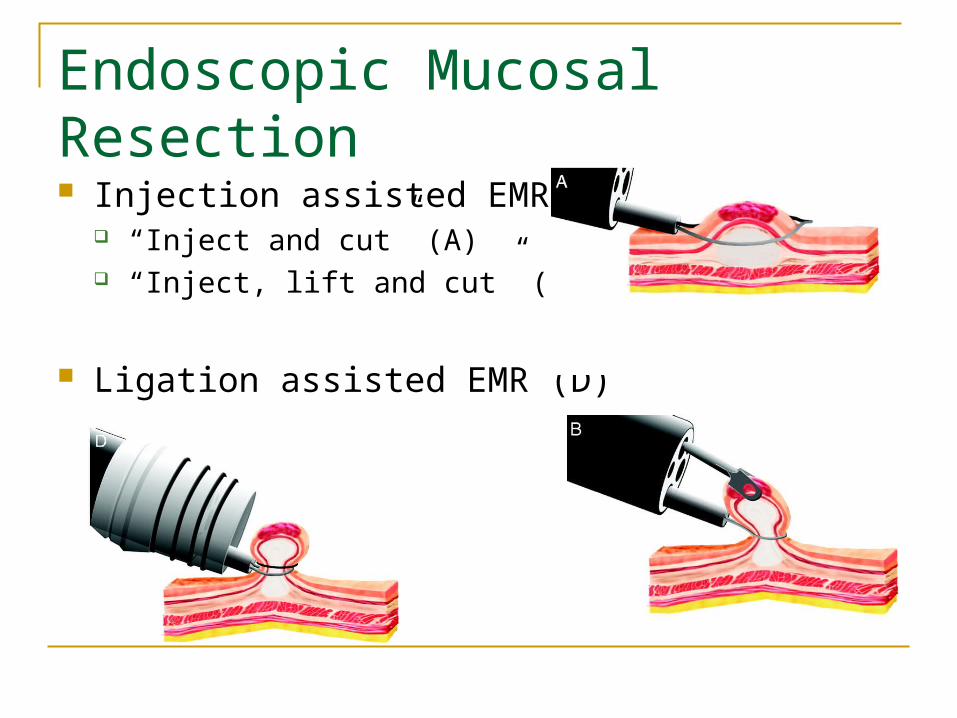
Endoscopic Mucosal Resection Injection assisted EMR
“Inject and cut” (A) “Inject, lift and cut” (B)
Ligation assisted EMR (D)
Limitation of EMR
Difficult for en-bloc resection for lesions > 20mm in size
Piecemeal resection of large lesions Possible local recurrence due to residual lesion
Published rate of recurrence up to 27.2% Inability to obtain complete specimen for detail
pathological assessment
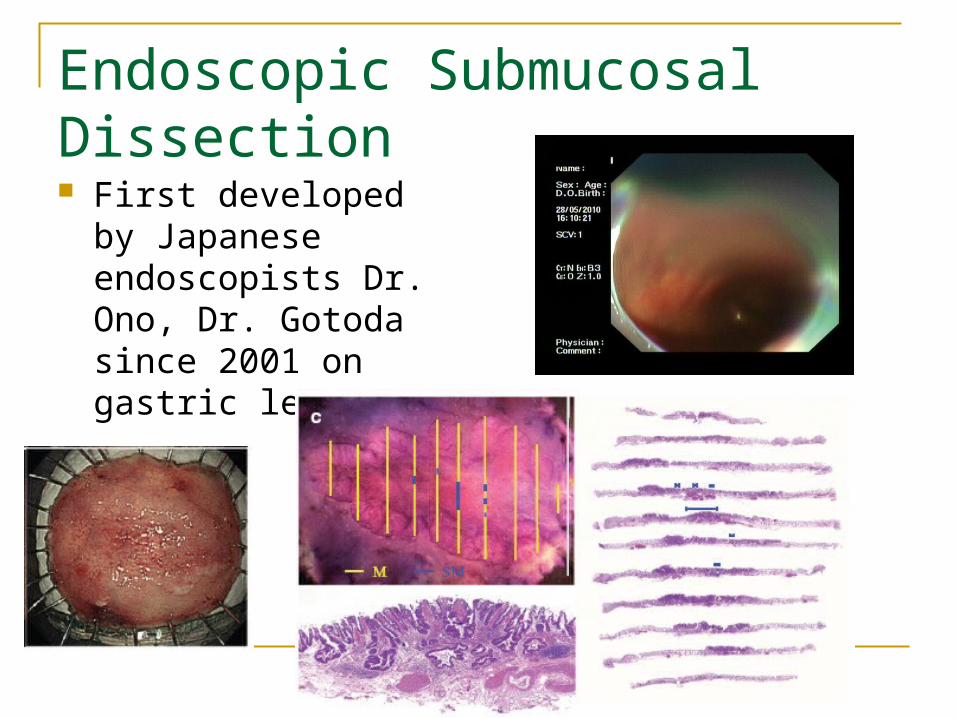
Endoscopic Submucosal Dissection First developed by
Japanese endoscopists Dr. Ono, Dr. Gotoda since 2001 on gastric lesion
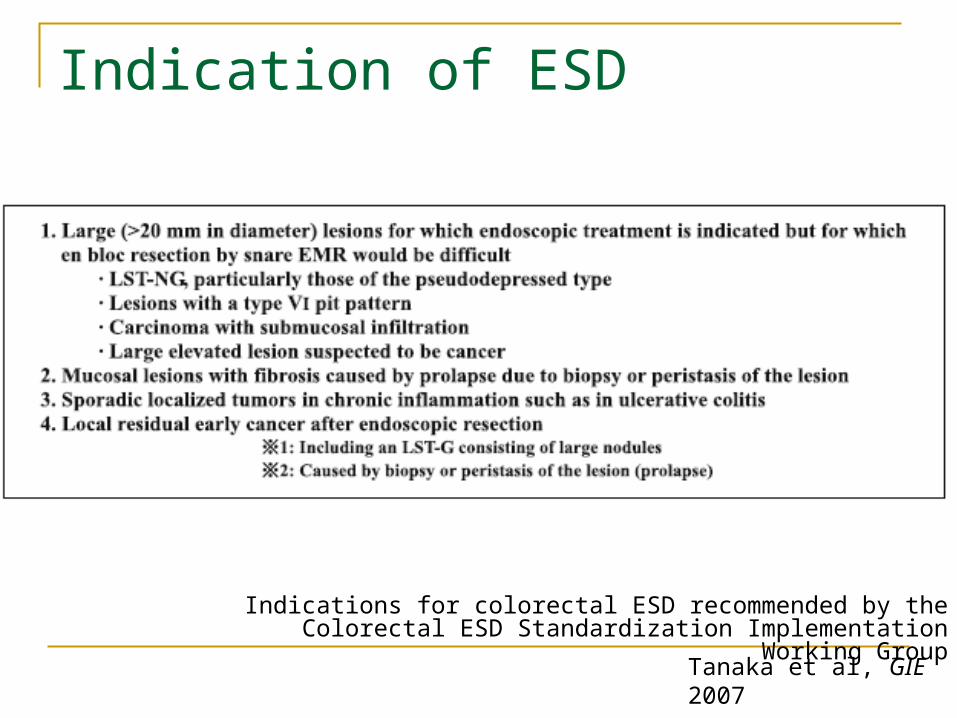
Indication of ESD
Tanaka et al, GIE 2007
Indications for colorectal ESD recommended by the Colorectal ESD Standardization Implementation Working Group
Short term outcomes of ESD – Systemic review 2841 ESD treated lesions R0 resection rate: 88% Bleeding rate: 2% Perforation rate: 4%
ESD is safe and effective, at least in expert hands
Repici A et al. Endoscopy 2012
Long term outcomes of ESD for colorectal neoplasms 146 adenomas, 164 carcinomas Local recurrence rate: 2.0% Median FU 38.7 months 3 year overall survival: 97.1% 5 year overall survival: 95.3%
Niimi K, Fujishiro M, Endoscopy 2010
Potential pitfalls for ESD
Technically demanding Tortuous structures – difficulty in maintaining
scope position Narrow lumen – difficulty in controlling the knife Thin colonic wall – Increase risk of perforation
Overall risk of perforation higher than EMR or EPMR
Questions
1. Can we remove this lesion completely with endoscope?
2. If pathology confirms invasive carcinoma, is endoscopic resection adequate? Do we need formal surgical resection?
Risk of recurrence after endoscopic resection alone Adequacy of local tumor control
Margin positivity
Adequacy of regional tumor control Lymphatic involvement Need for further lymphatic clearance, i.e. formal
colonic resection?
Adequacy of local tumor control Resection margin involved or less than 1mm Relapse rate 21–33%
Most authors believe a resection margin of ≥ 2 mm is safe and the probability of residual disease or recurrent carcinoma is low
Cooper HS et al, Gastroenterology 1995
L Bujanda et al, W. J. Gastroenterology 2010
Predictive factor of recurrence after endoscopic resection
Multiple studies addressing the issue since 1980s
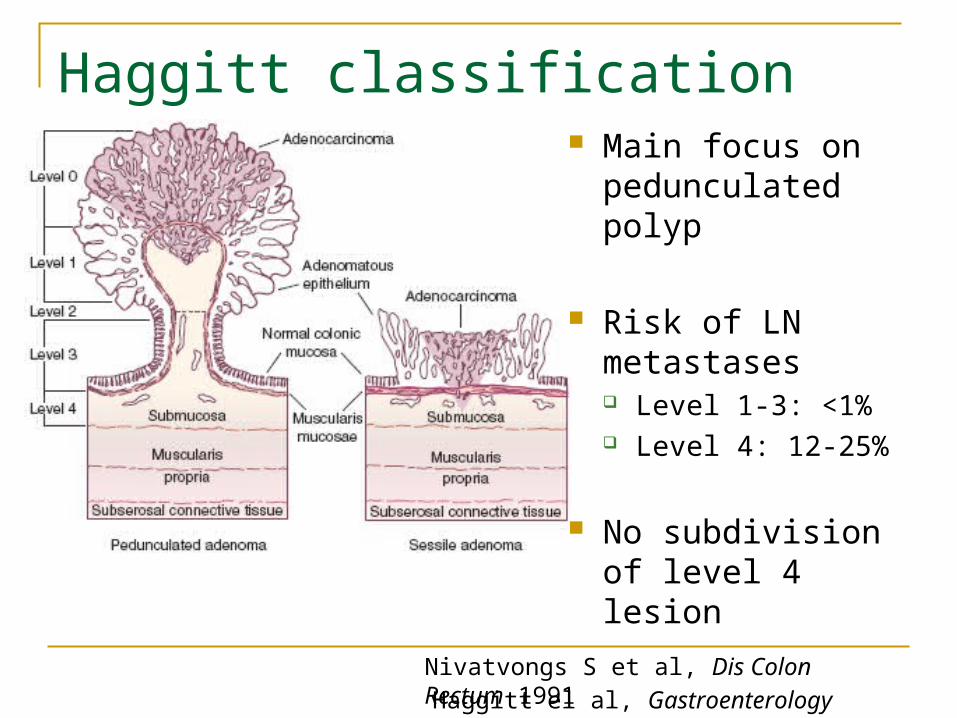
Haggitt classification
Haggitt el al, Gastroenterology 1985
Main focus on pedunculated polyp
Risk of LN metastases Level 1-3: <1% Level 4: 12-25%
No subdivision of level 4 lesion
Nivatvongs S et al, Dis Colon Rectum 1991
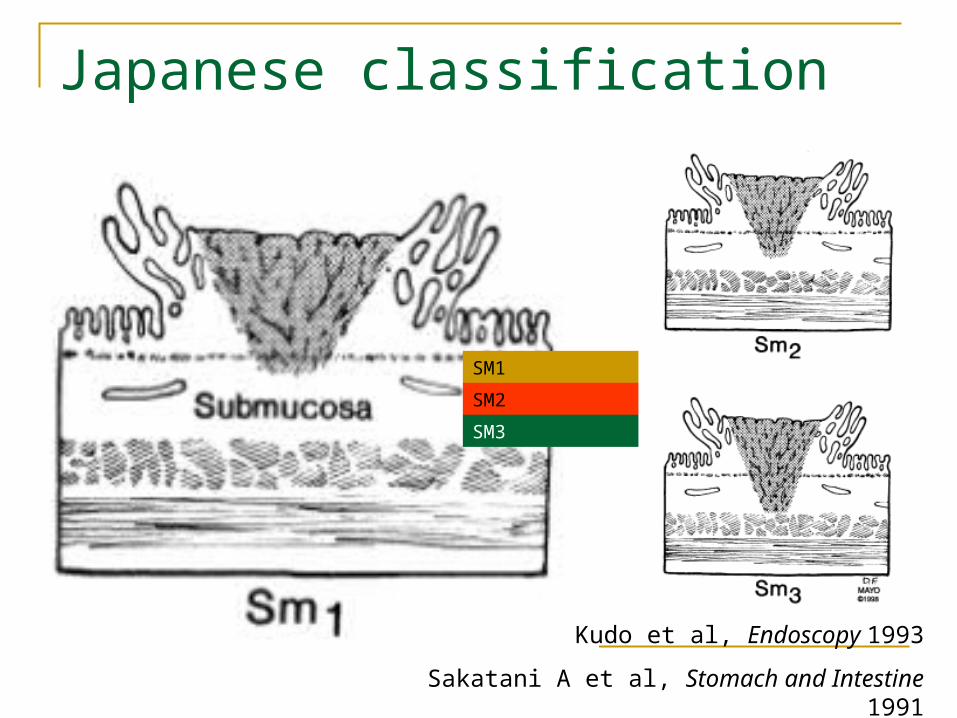
Japanese classification
SM1
SM2
SM3
Kudo et al, Endoscopy 1993
Sakatani A et al, Stomach and Intestine 1991
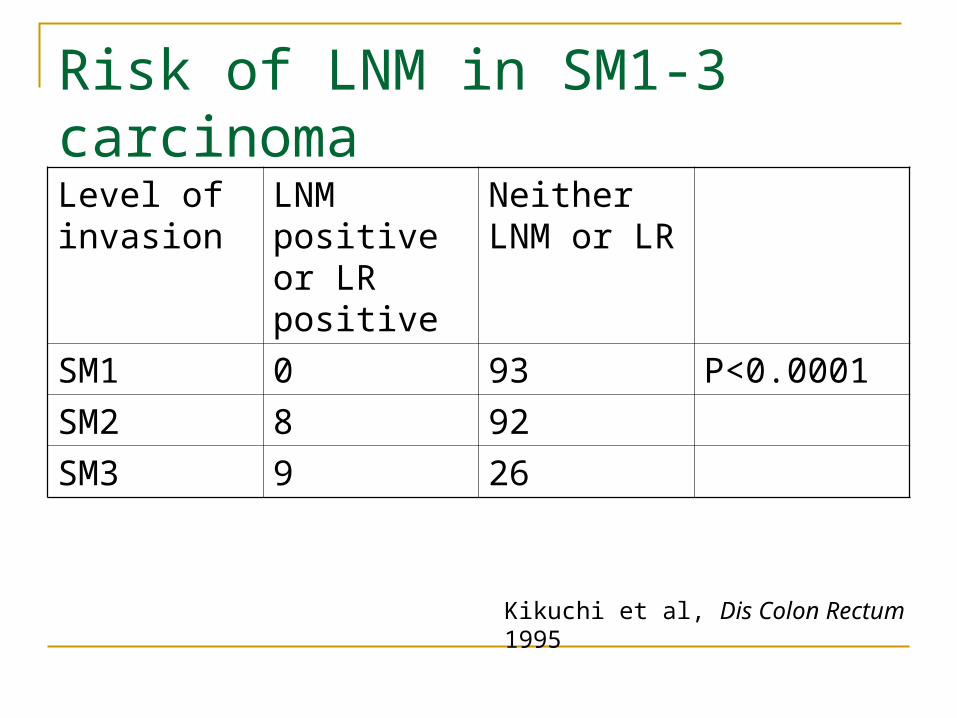
Risk of LNM in SM1-3 carcinomaLevel of invasion
LNM positive or LR positive
Neither LNM or LR
SM1 0 93 P<0.0001
SM2 8 92
SM3 9 26
Kikuchi et al, Dis Colon Rectum 1995
Journal of Gastrointestinal Surgery 2012
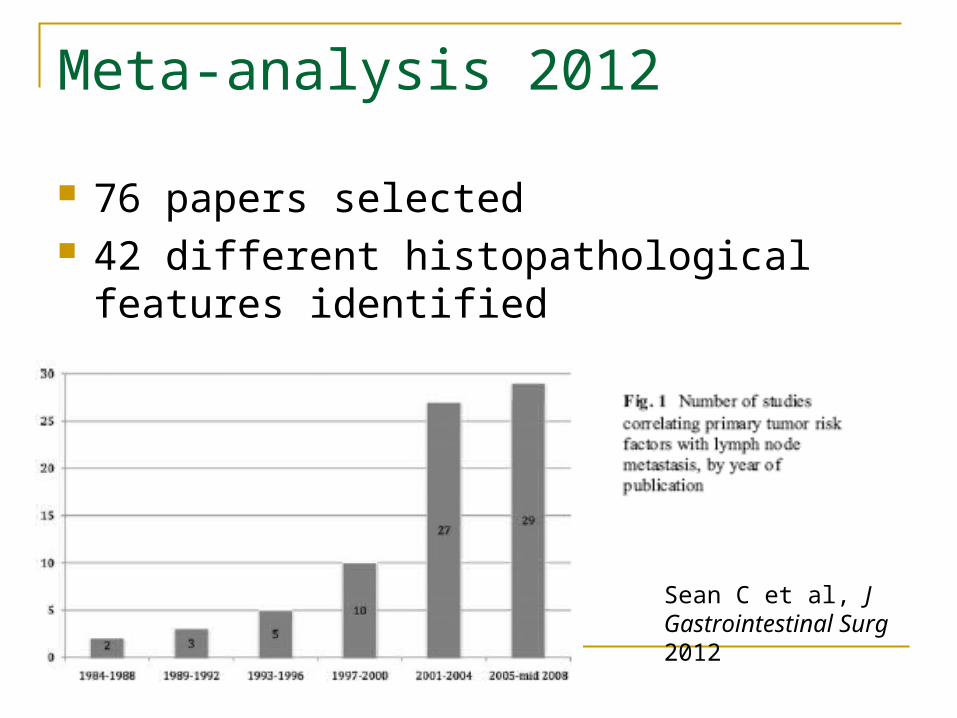
Meta-analysis 2012
76 papers selected 42 different histopathological features
identified
Sean C et al, J Gastrointestinal Surg 2012
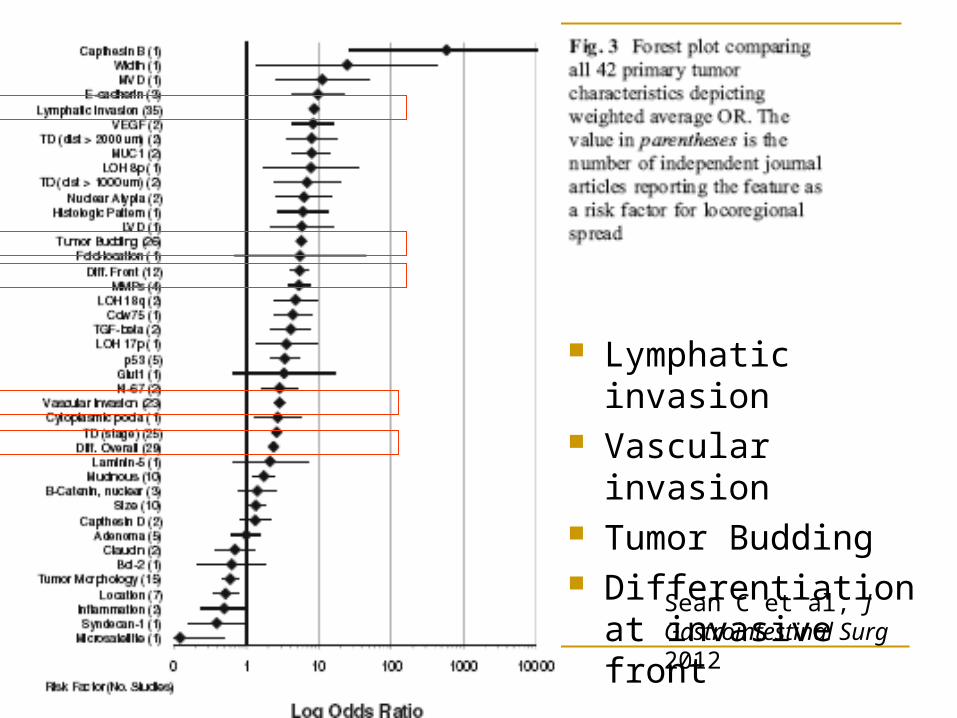
Lymphatic invasion Vascular invasion Tumor Budding Differentiation at
invasive front
Sean C et al, J Gastrointestinal Surg 2012
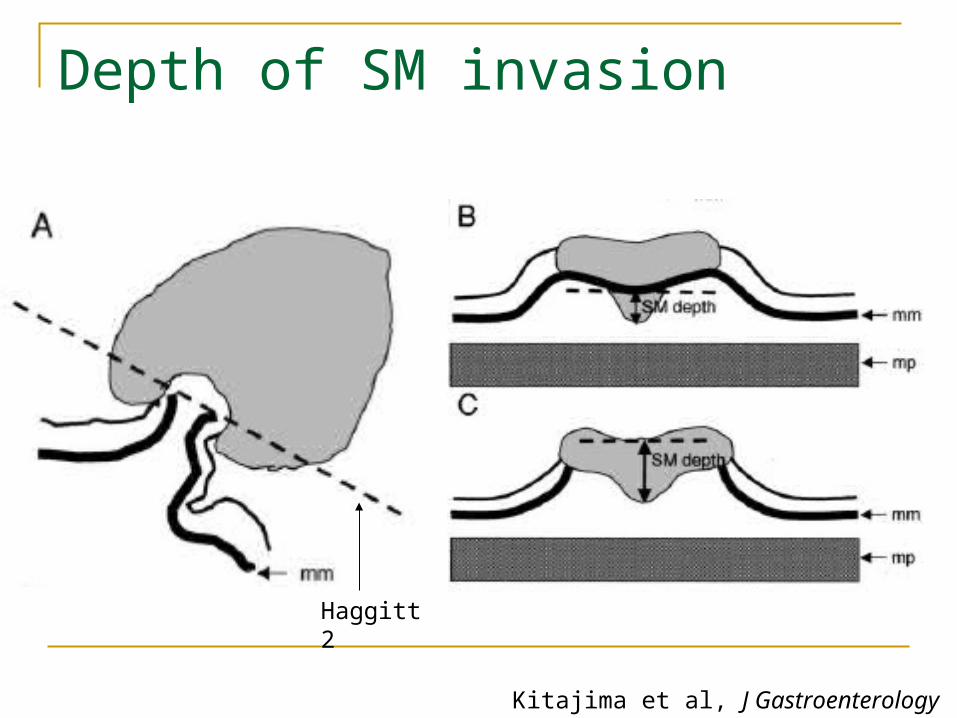
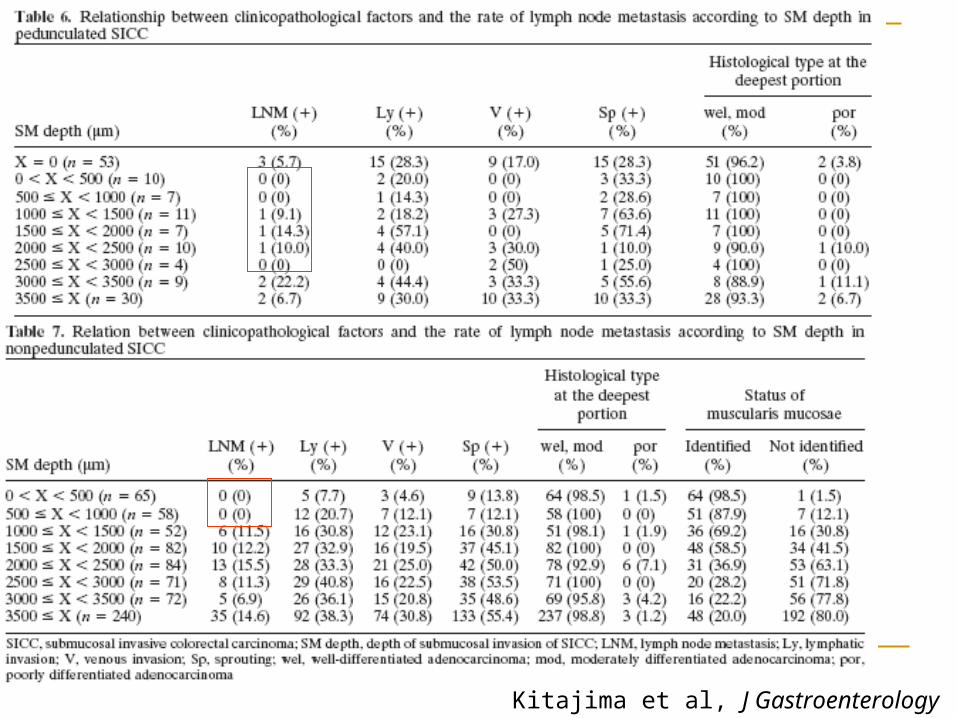
Depth of SM invasion
Kitajima et al, J Gastroenterology 2004
Haggitt 2
Kitajima et al, J Gastroenterology 2004
Conclusion
Endoscopic resection adequate if SM invasion <1000μm for non-pedunculated
polyp SM invasion <3000μm for pedunculated polyp in
the absence of lymphatic invasion
Kitajima et al, J Gastroenterology 2004
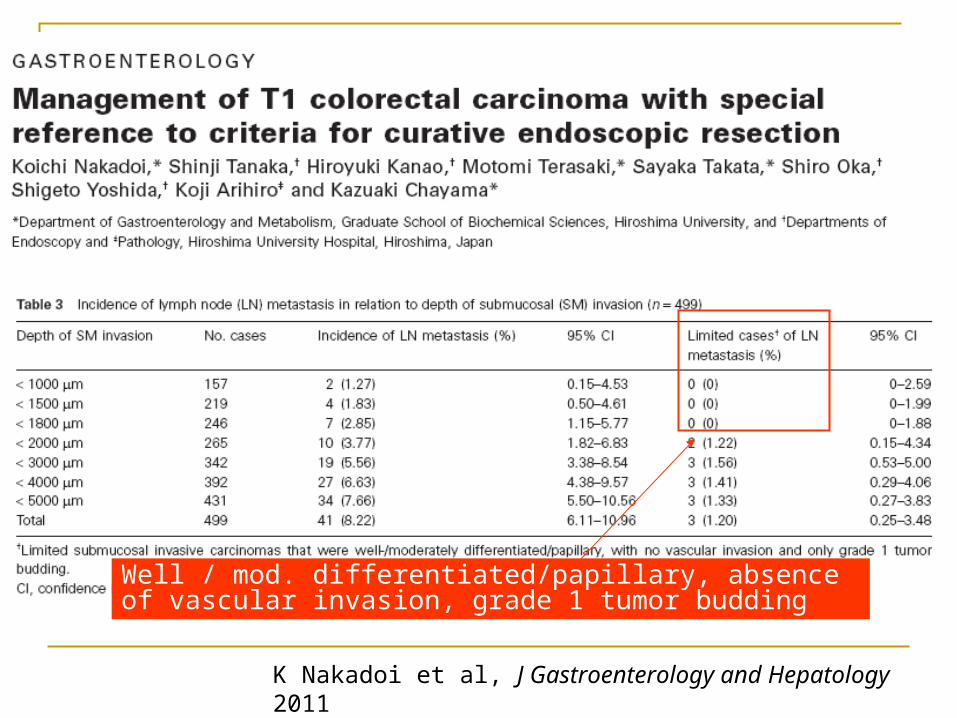
K Nakadoi et al, J Gastroenterology and Hepatology 2011
Well / mod. differentiated/papillary, absence of vascular invasion, grade 1 tumor budding
Japanese guidelines
Submucosal carcinomas can be followed up: Tumor-negative horizontal margin Differentiated adenocarcinoma Submucosal invasion of < 1000 μm Absence of vascular invasion Grade 1 (low grade) tumor budding
Otherwise additional surgery with lymph node dissection recommended
Japanese Society for Cancer of the Colon and Rectum. 2010
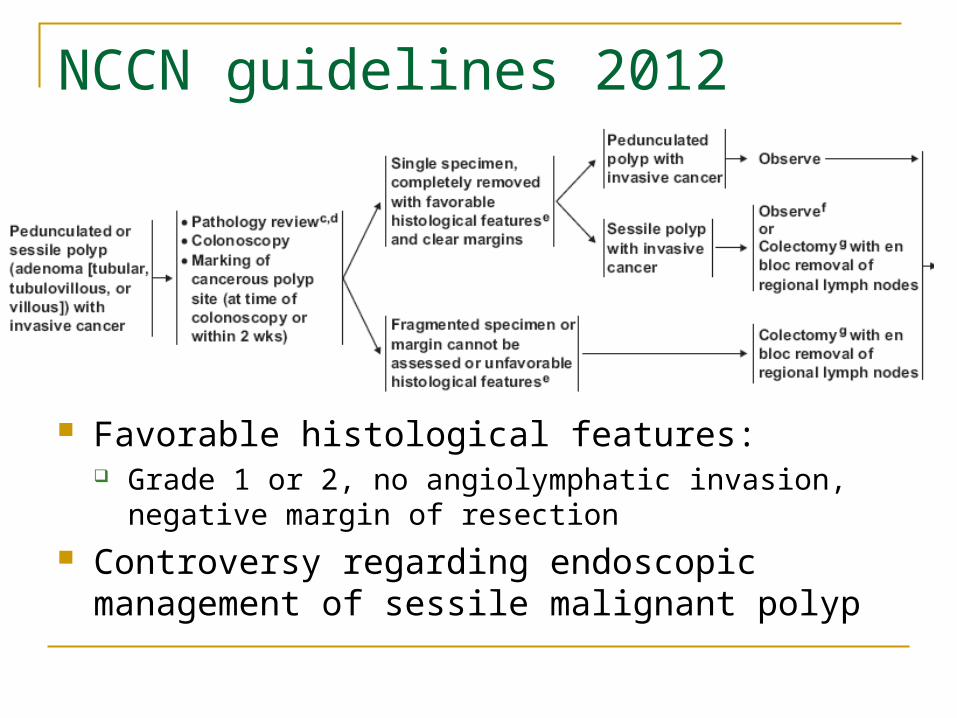
NCCN guidelines 2012
Favorable histological features: Grade 1 or 2, no angiolymphatic invasion, negative margin
of resection Controversy regarding endoscopic management of
sessile malignant polyp
T1 colonic carcinoma – Is endoscopic resection sufficient? No direct comparison between endoscopic resection alone
with formal surgical resection in prospective manner Practically difficult to conduct
Endoscopic resection alone should be safe in selected subgroup of patients with favorable histology and limited SM invasion
Endoscopic resection also useful in accurate staging to predict need for additional surgery in marginal cases
Need good liaison with dedicated pathologist to accurately identify the histological features that predict risk of lymph node metastases
Questions?
Thank you
Acknowledgement:
Dr. SF Hon, PWH
Recommended