Viskoelastické metodyv doporučených postupech a
publikované literatuře

DIAGNOSTIKA A LÉČBA
ŽIVOT OHROŽUJÍCÍHO KRVÁCENÍ U
DOSPĚLÝCH PACIENTŮ V INTENZIVNÍ A
PERIOPERAČNÍ PÉČI
ČESKO-SLOVENSKÝ
MEZIOBOROVÝ DOPORUČENÝ POSTUP
II. Diagnostika a monitorace krvácení
Coagulation monitoring
Recommendation 12
We recommend that routine practice to detect post-traumatic coagulopathy include the early, repeated and combined measurement of prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen and platelets. (Grade 1C)
We recommend that viscoelastic methods also be performed to assist in characterising the coagulopathy and in guiding haemostatic therapy. (Grade 1C)
HYPERFIBRINOLÝZA
• Mimo ROTEM prakticky nediagnostikovatelná
• Proces který u je přítomen u těžkého krvácení vždy ! (pouze záleží na jeho míře)
• Pro TIC (Trauma Induced coagulopathy) charakteristická
• Není ale jen u TIC !!

V. Management krvácení a koagulace
Coagulation support
Recommendation 23
We recommend that monitoring and measures to support coagulation be initiated as early as possible. (Grade 1C)
V. Management krvácení a koagulace
Antifibrinolytic agentsRecommendation 24We recommend that tranexamic acid be administered as
early as possible to the trauma patient who is bleeding or at risk of significant hemorrhage at a loading dose of 1 g infused over 10 minutes, followed by an intravenous infusion of 1 g over 8 h. (Grade 1A)
We recommend that tranexamic acid be administered to the bleeding trauma patient within 3 h after injury. (Grade 1B)
We suggest that protocols for the management of bleeding patients consider administration of the first dose of tranexamic acid en route to the hospital. (Grade 2C)
tranexamová kyselina
dávka 20-25 mg/kg
dávka 1 g bolus a 1 g
kontinuálně
V. Management krvácení a koagulace
Calcium
Recommendation 25
We recommend that ionised calcium levels be monitored and maintained within the normal range during massive transfusion. (Grade 1C)
Volumoth - koloidy
V. Management krvácení a koagulace
Plasma
Recommendation 26
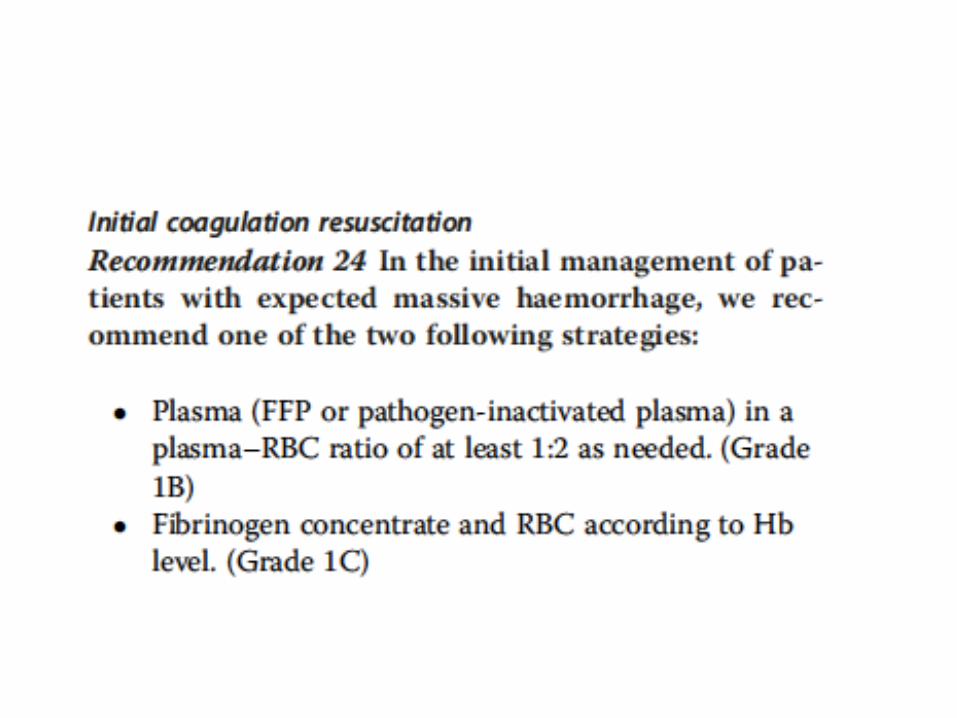
We recommend the initial administration of plasma (fresh frozen plasma (FFP) or pathogen-inactivated plasma) (Grade 1B) or fibrinogen (Grade 1C) in patients with massive bleeding.
If further plasma is administered, we suggest an optimal plasma:red blood cell ratio of at least 1:2. (Grade 2C)
We recommend that plasma transfusion be avoided in patients without substantial bleeding. (Grade 1B)
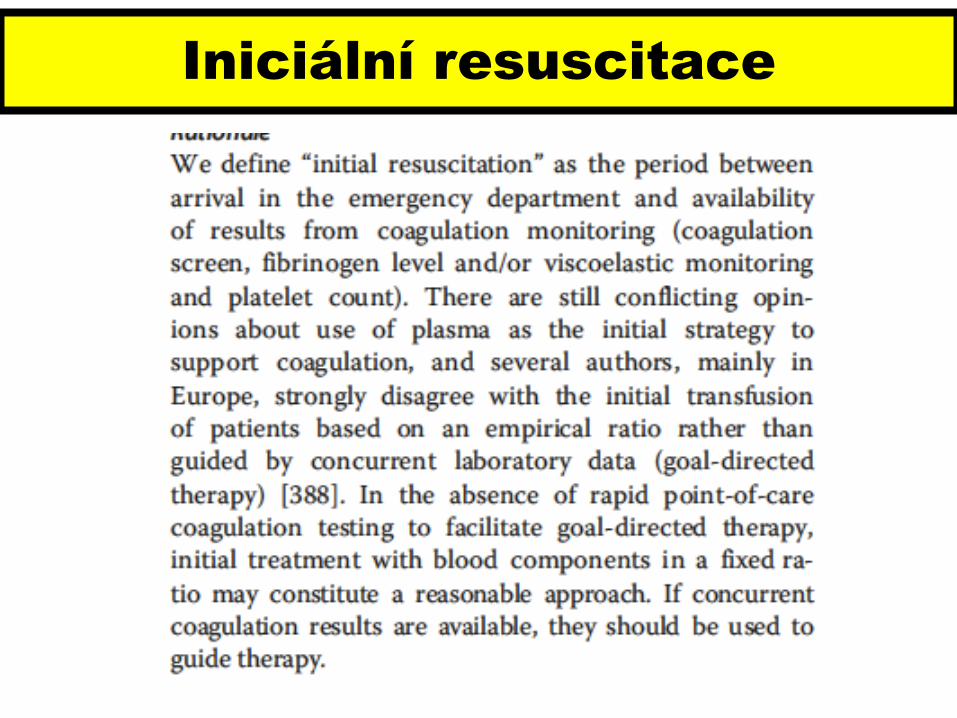
Iniciální resuscitace
o Trauma indukovanou koagulopatii rozvíjí ¼ až ½ všech pacientů s traumatem
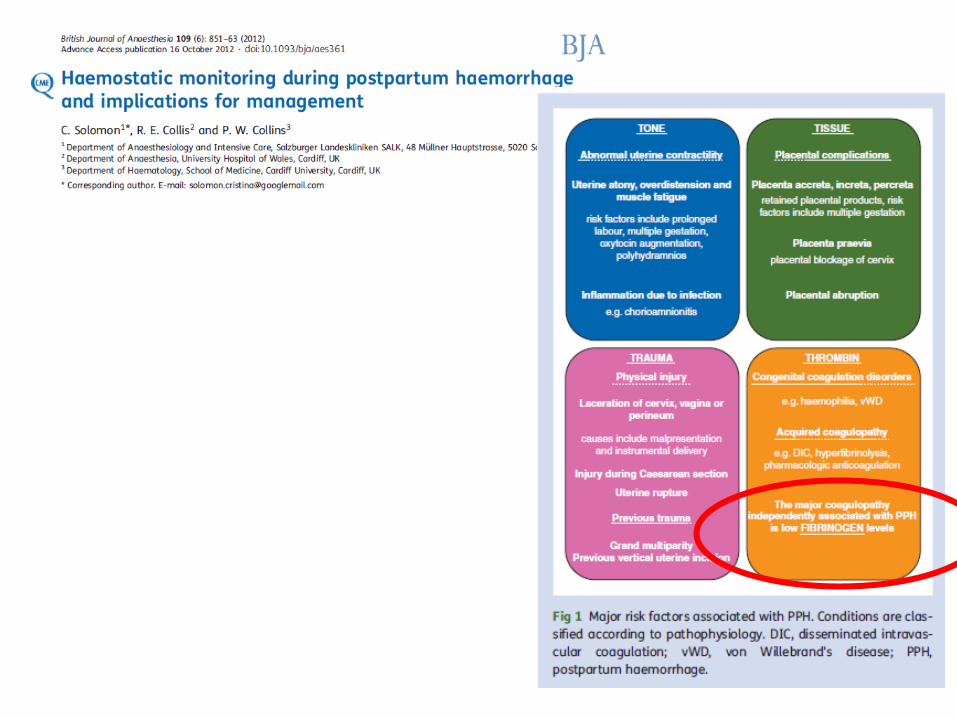
o V případě masivní krevní ztráty,dosahuje hladina fibrinogenukritických hodnot dříve než ostatníprokoagulační faktory nebotrombocyty.
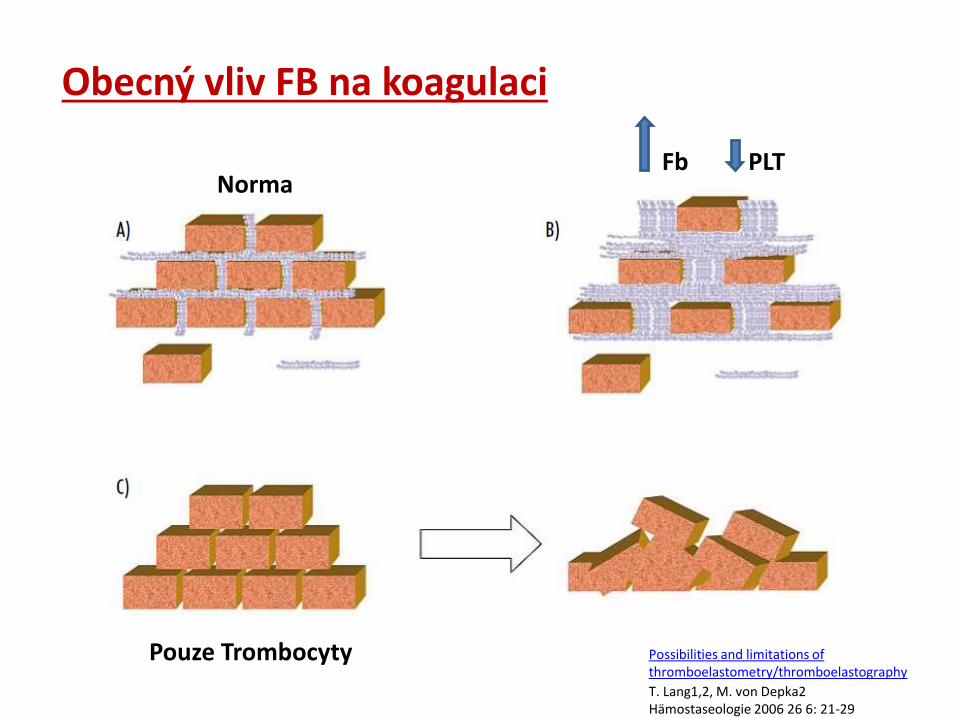
Obecný vliv FB na koagulaci
Possibilities and limitations of thromboelastometry/thromboelastography
T. Lang1,2, M. von Depka2Hämostaseologie 2006 26 6: 21-29
Pouze Trombocyty
NormaFb PLT
Podání již při podezření na
deficit fibrinogenu
Kritických hodnot
fibrinogenu může být
dosaženo dříve než je nutné
podávat PRBC
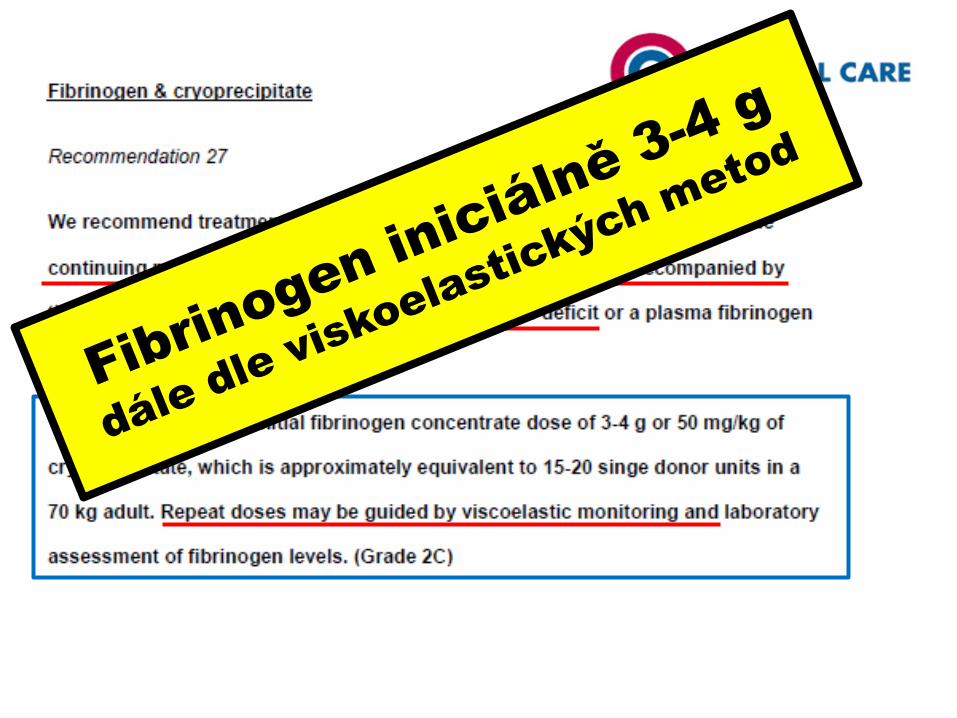
4 g fibrinogenu ...vzestup o
1g/l fibrinogenu
4 g fibrinogenu nebo 16 x FFP
Další resuscitace
BUĎ
ANEBO
agregometrie
PCC
Management koagulace
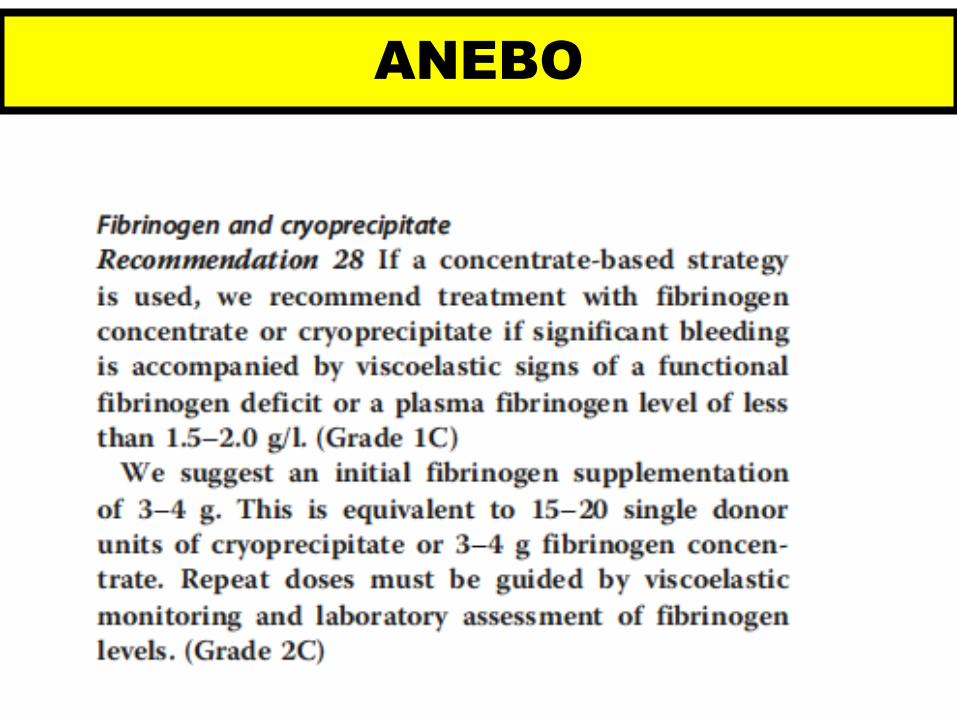
• We recommend treatment with fibrinogen concentrate if significant bleeding is accompanied by at least suspected low fibrinogen concentrations or function. 1C
• We recommend that a plasma fibrinogen concentration <1.5–2.0 g /l or ROTEM/TEG signs of functional fibrinogen deficit should be triggers for fibrinogen substitution. 1C
• We suggest an initial fibrinogen concentrate dose of 25–50 mg/ kg. 2C
• We suggest that the indication for cryoprecipitate is lack of available fibrinogen concentrate for the treatment of bleeding and hypofibrinogenaemia. 2C
Antifibrinolytika
• We recommend the consideration of tranexamic acid (20–25 mg kg). 1A
Management koagulace
• We recommend that patients on oral anticoagulant therapy should be given prothrombin complex concentrate (PCC) and vitamin K before any other coagulation management steps for severe perioperative bleeding. 1B
• We suggest that PCC (20–30 IU/kg) can also be admi-nistered to patients not on oral anticoagulant therapy in the presence of an elevated bleeding tendency and prolonged clotting time. Prolonged INR/PT alone is not an indication for PCC, especially in critically ill patients. 2C
Management koagulace – F XIII
• In cases of ongoing or diffuse bleeding and low clot strength despite adequate fibrinogen concentrations, it is likely that FXIII activity is critically reduced. In cases of significant FXIII deficiency (i.e. <60% activity), we suggest that FXIII concentrate (30 IU kg) can be administered. 2C
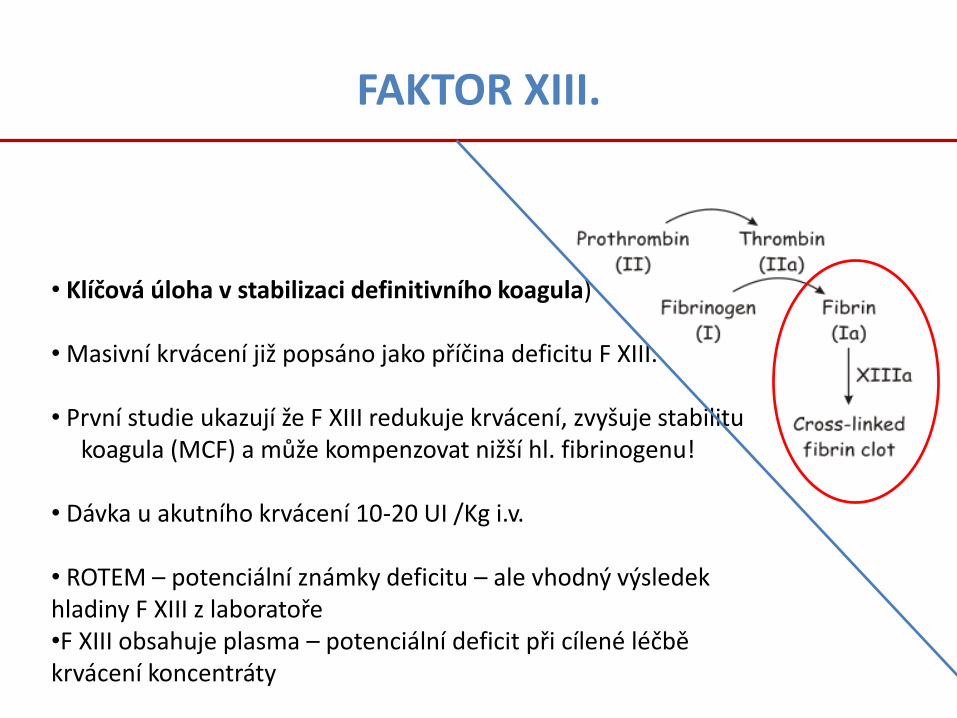
FAKTOR XIII.
• Klíčová úloha v stabilizaci definitivního koagula)
• Masivní krvácení již popsáno jako příčina deficitu F XIII.
• První studie ukazují že F XIII redukuje krvácení, zvyšuje stabilitukoagula (MCF) a může kompenzovat nižší hl. fibrinogenu!
• Dávka u akutního krvácení 10-20 UI /Kg i.v.
• ROTEM – potenciální známky deficitu – ale vhodný výsledek hladiny F XIII z laboratoře•F XIII obsahuje plasma – potenciální deficit při cílené léčbě krvácení koncentráty
Management koagulace
• We suggest that off-label administration of recombinant activated factor VII (rFVIIa) can be considered for bleeding which cannot be stopped by conventional, surgical or interventional radiological means and/or when comprehensive coagulation therapy fails. 2C

• Bleeding and transfusion of allogeneic blood products independently increase morbidity, mortality, length of stay in ICU and hospital, and costs. B
• Lysine analogues (tranexamic acid and e-aminocaproic acid; EACA) reduce perioperative blood loss and transfusion requirements; this can be highly cost-effective in several settings of major surgery and trauma. A
Outcome
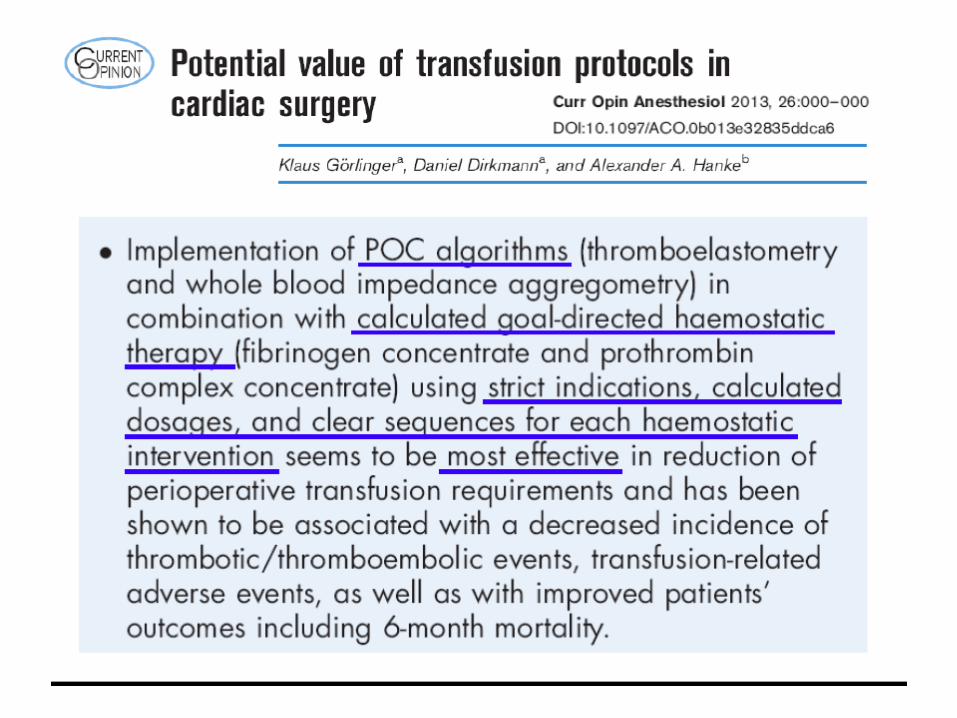
• Implementation of transfusion and coagulation management algorithms (based on ROTEM/TEG) can reduce transfusion-associated costs in trauma, cardiac surgery and liver transplantation. B
• Goal-directed therapy with coagulation factor concentrates (fibrinogen and/or PCC) may reduce transfusion- associated costs in trauma, cardiac surgery and liver transplantation. B
• Thromboembolic events are associated with increased in-hospital and post-hospital costs. B
• Targeted therapy with fibrinogen and/or PCC guided by ROTEM/TEG is not associated with an increased incidence of thromboembolic events. C
Cena, komplikace
Játra
• Despite PT, aPTT and INR indicating coagulopathy in chronic liver disease (CLD), global coagulation tests (thrombin generation and TEG/ROTEM) suggest that haemostasis is balanced in stable CLD. C
• Mild to moderate prolongation of the preoperative PT and INR do not predict bleeding in patients with CLD. C
• We recommend against the use of FFP for pre-procedural correction of mild to moderately elevated INR. 1C
Multiplate/Platelet
• To be useful in an emergency, a platelet function test needs to be applicable at the point-of-care and be capable of generating results quickly. A recent study used multiple electrode aggregometry (MEA, Multiplate) to assess platelet function of trauma patients on admission to the emergency room.
• ADPtest and TRAPtest values below the normal range were associated with increased mortality.
Detekce hyperfibrinolýzy

WHO – kyselina tranexamová
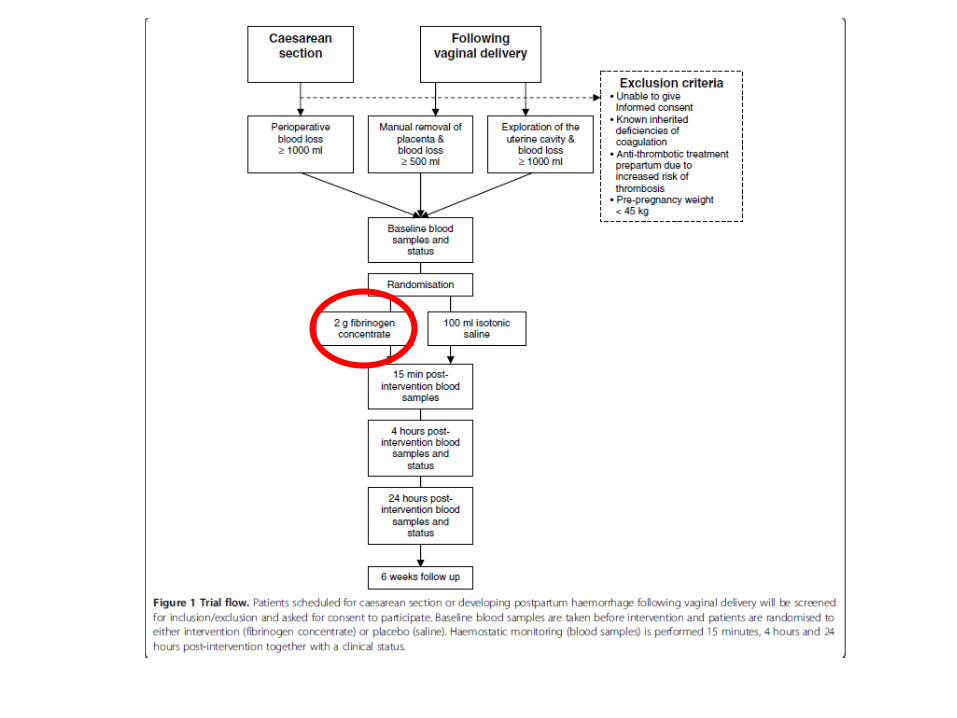
Peripartální krvácení
We suggest that using perioperative cell salvage during caesarean section may decrease postoperative homologous transfusion and reduce hospital stay. 2B
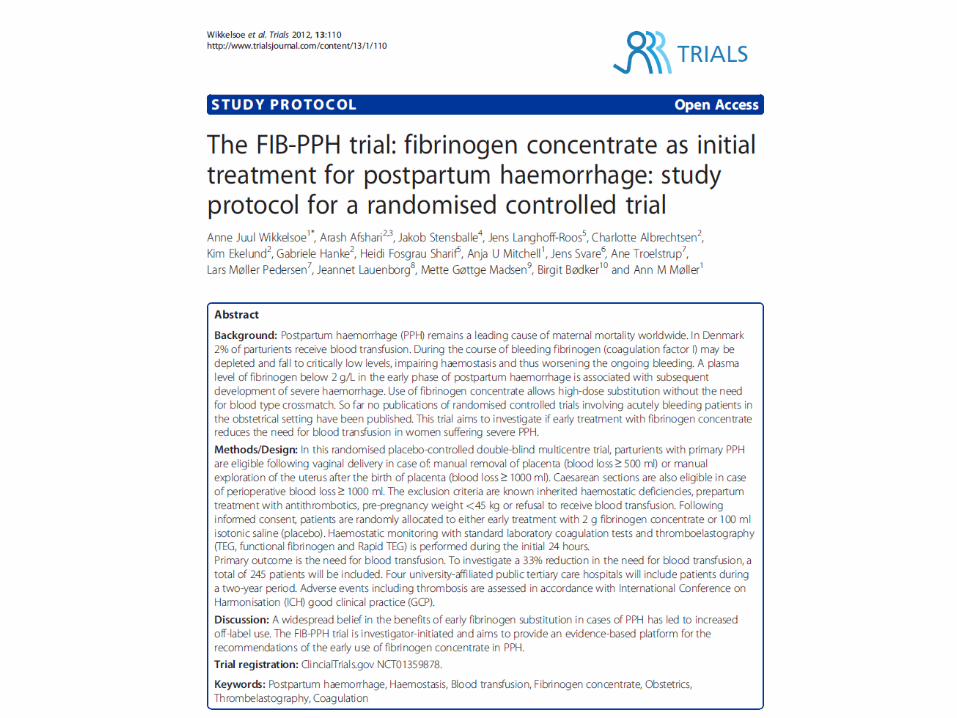
We suggest assessing fibrinogen concentration in parturients with bleeding, as concentrations < 2 g l-1 may identify those at risk of severe PPH. 2C
Platelet count < 100 x 109 l-1 at the onset of labour, particularly combined with plasma fibrinogen concentration < 2.9 g l-1, may indicate an increased risk of PPH. C
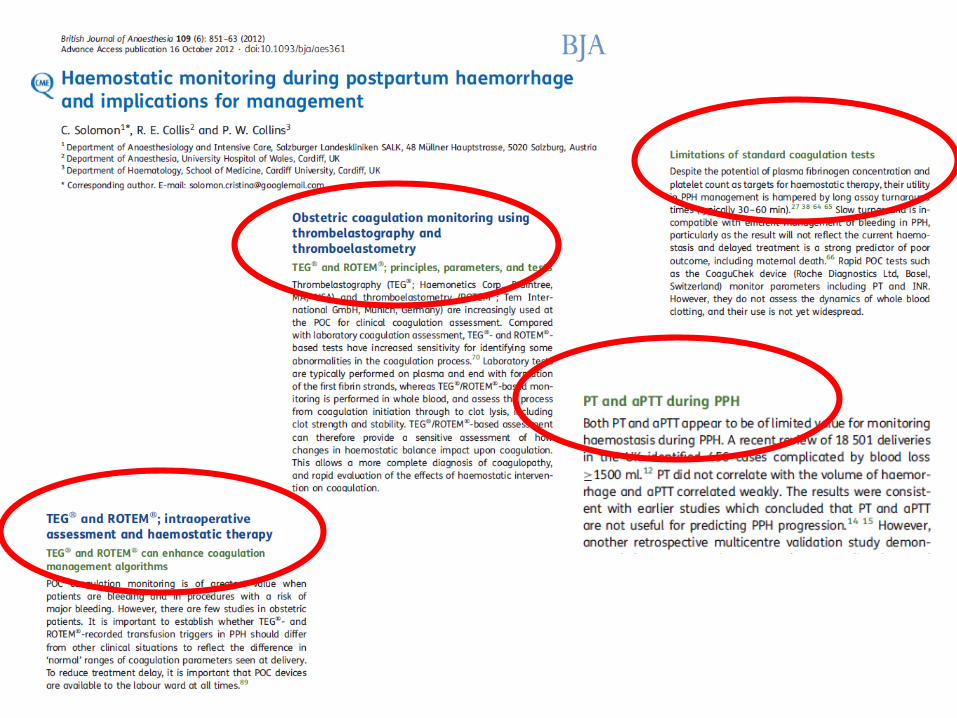
aPTT and PT are of little predictive value for PPH. C
Thromboelastometry can identify obstetric coagulopathy and hyperfibrinolysis and guide haemostatic therapy. C
In life-threatening PPH, we suggest a transfusion protocol with a fixed product ratio or individualised procoagulant intervention and factor substitution. 2C
Considering physiologically elevated fibrinogen concentrations in pregnancy, we suggest that a higher trigger value for treating hypofibrinogenaemia may be required. C
We recommend the administration of tranexamic acid in obstetric bleeding to reduce blood loss, bleeding duration and the number of units transfused. 1B
We suggest that tranexamic acid be considered before caesarean section. 2C
In antepartum bleeding, we suggest administration of tranexamic acid. 2B
Peripartální krvácení
“ROTEM-guided haemostatic therapy with fibrinogen concentrate as
first-line haemostatic therapy and additional use of PCC was
goaldirected, efficacious, and quick to administer.
Thromboelastometry allowed rapid and reliable diagnosis of the
underlying coagulopathy. A favourable survival rate was observed.”
Of 131 patients included, 128 received fibrinogen concentrate as first-line therapy, 98 additionally
received PCC, while 3 patients with recent coumarin intake received only PCC. Twelve patients
received FFP and 29 received platelet concentrate. The observed mortality was 24.4%, lower than
the TRISS mortality of 33.7% and the RISC mortality of 28.7%. After excluding 17 patients with
traumatic brain injury, the difference in mortality was 14% observed versus 27.8% predicted by
TRISS and 24.3% predicted by RISC.
PREDIKCE
ČAS
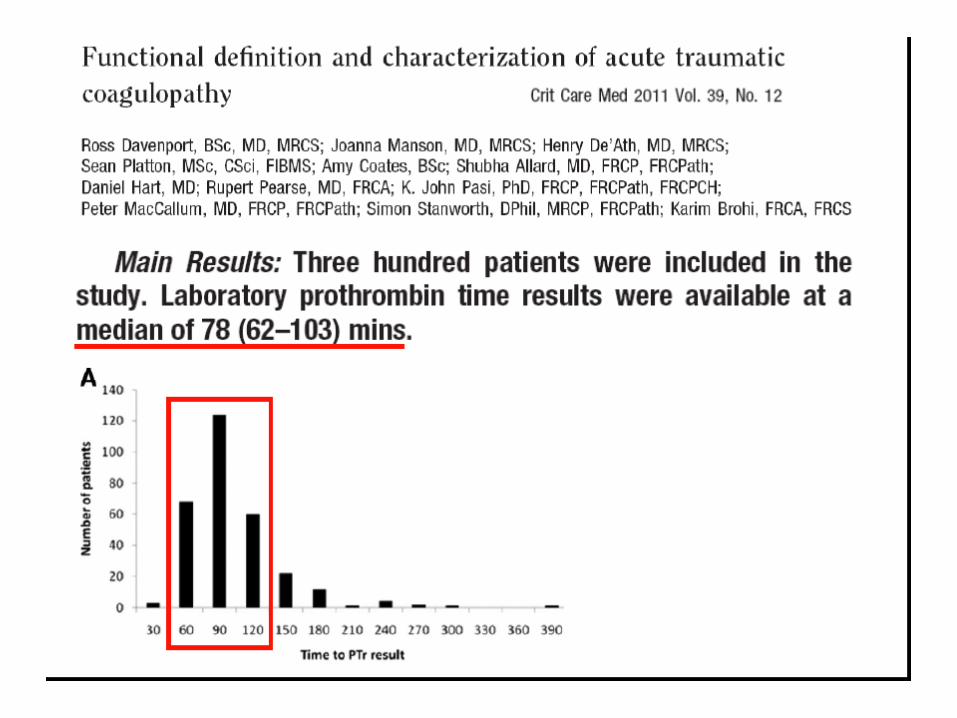
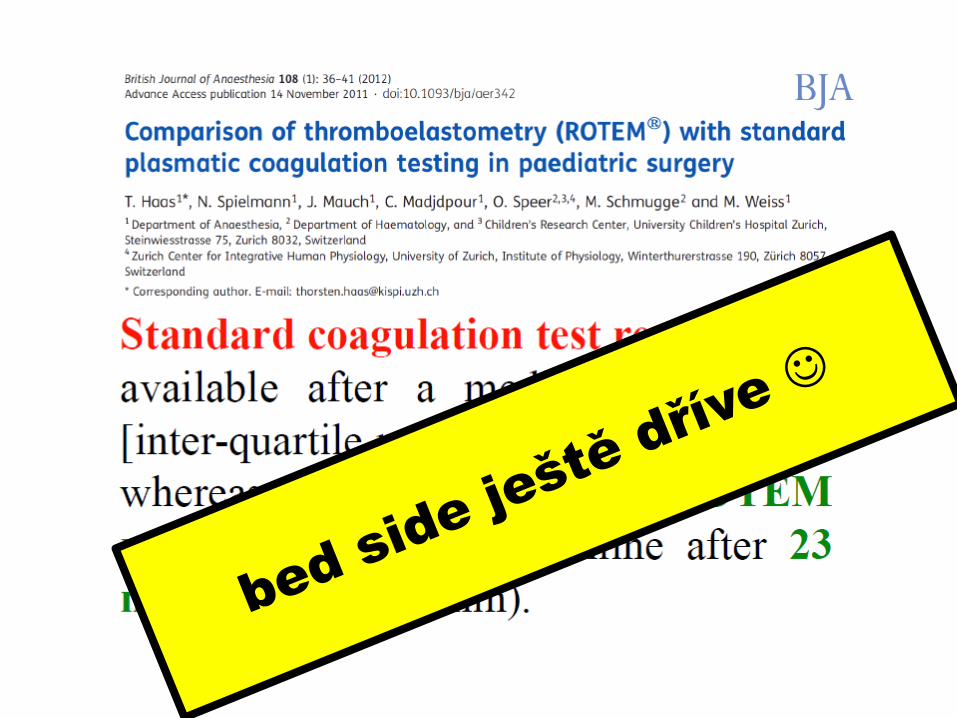
Kam umístit ROTEM ?
Laboratorní testy: APTT, Quick
kardiochirurgie
Recommended