Embed Size (px)
Citation preview

ACUTE OSTEOMYELITIS
NUR HANISAH ZAINOREN

OSTEOMYELITIS
ACUTE CHRONIC
PRIMARY SECONDARY
HEMATOGENOUS FOLLOWING AN OPEN FRACTURE/BONE OPERATION
Infection of the bone by pyogenic micro-organisms

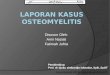
• Highly vascularized zone
• Venous system begins in this area and drains towards the diaphysis
• Vessel are arranged in the form of hair-pin arrangement blood stasis responsible for the metaphysis being the favourite site for bacteria osteomyelitis
METAPHYSIS OF LONG BONE

TYPES OF METAPHYSIS

AETIOPATHOGENESIS• Staph. aureus commonest causative organisms
• Others: Streptococcus & Pneumococcus
• Reach the bone via blood circulation
• Lodged in the metaphysis – Lower femoral metaphysis *commonest– Upper femoral metaphysis– Upper tibial metaphysis– Upper humeral metaphysis





• Disease of CHILDHOOD, more common in BOYS, probably because they are more prone to injury
• Diagnosis is clinical
• Presenting complaints: – Pain– Swelling – Fever– Chills and rigor
• Examination:– Febrile and dehydrated– Red, hot, tender, swelling, edema– Abscess in the muscle or subcutaneous plane (later stages)– There may be swelling of the adjacent joint

• Investigations:– Blood:
• PMN leucocytosis• Elevated ESR• Blood culture at the peak of the fever
may yield the causative organism
– X-rays:• Earliest sign (7-10 days):
periosteal new bone deposition at the metaphysis (periosteal reaction)
– Bone scan (Technetium-99):• May show increased uptake by the
bone in the metaphysis (positive before changes appear in x-ray)

• Differential diagnosis:a) Acute septic arthritisb) Acute rheumatic arthritisc) Scurvyd) Acute poliomyelitis
*Any acute inflammatory disease at the end of a bone, in a child, should be taken as acute osteomyelitis unless proved otherwise.
*Any history of trauma, must be thoroughly questioned

• Treatment:Within 48 hours of the onset of symptoms
• Pus not yet formed and the inflammatory process can be halted by systemic antibiotics
• Consists of rest, antibiotics and general building-up of the patient Rest - Limb is put to rest in a splint or by traction
Antibiotics - choices varies depend on the age of the child & choice of the doctor
General – rehydration with IV fluids, weight bearing restriction for 6-8 weeks

• Treatment:After 48 hours of the onset of symptoms
• Child is brought late or does not respond to conservative treament Collection of pus within or outside the bone
• Detection of pus by ultrasound examination (because it may lie deep to the periosteum)
• Surgical exploration and drainage
• Antibiotics are continued for 6 weeks

• Complications:– General complications:• Septicaemia• Pyemia
– Local complications:• Chronic osteomyelitis• Acute pyogenic arthritis• Pathological fracture• Growth plate disturbances

SECONDARY OSTEOMYELITIS • Arises from a wound infection in an open
fractures or after operations on the bone
• Less severe than hematogenous osteomyelitis (as wound provide some drainage)
• Prevention: – adequate initial treatment of open fractures– adherence to sterile operating conditions

THANK YOU :)