Embed Size (px)
Citation preview
Adrenal Antagonist By Dr. Sara Sami
Yuzuncu Yil University
2015
Adrenoceptor Antagonist Drugs
Classification
– Alpha Antagonists
• Non Selective
• α1 Selective
• α2 Selective
– Beta Antagonists
• Non Selective
• β1 Selective
• β2 Selective
• Toxicity
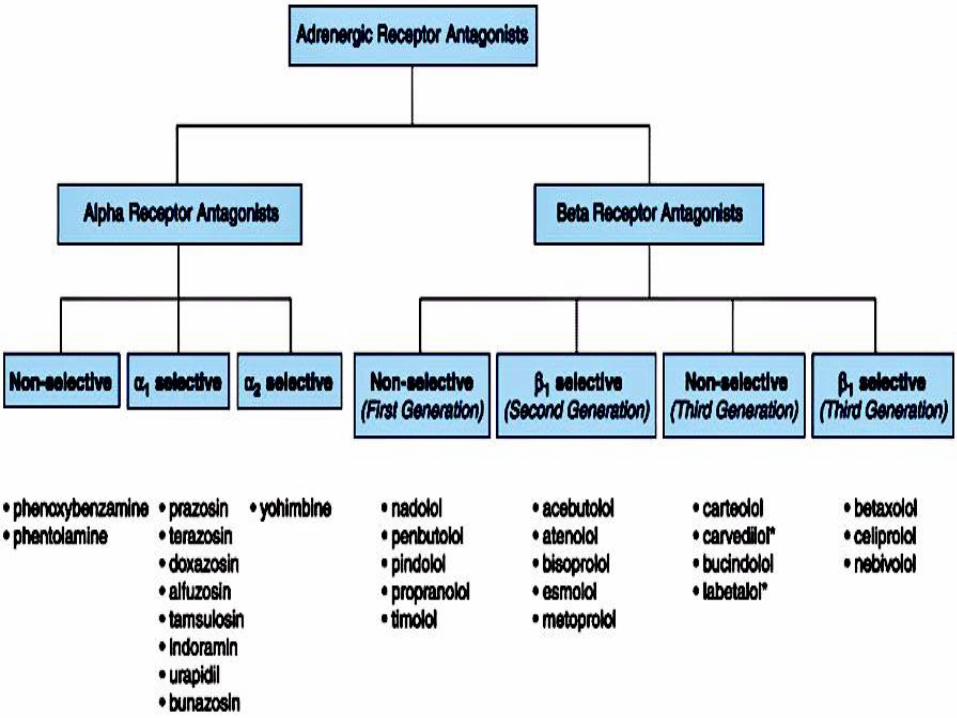
Classification of adrenergic receptor antagonist.
Wording
• Adrenoceptor Blocker
• Adrenergic Antagonist
• Subgroups in Sympathoplegic drugs
• Alpha Blocker, Alpha Antagonist
• Beta Blocker, Beta Antagonist
General effects of α blockers
Blood vessels
• α1-blockade→reduces peripheral resistance
Fall in BP
Postural hypotension
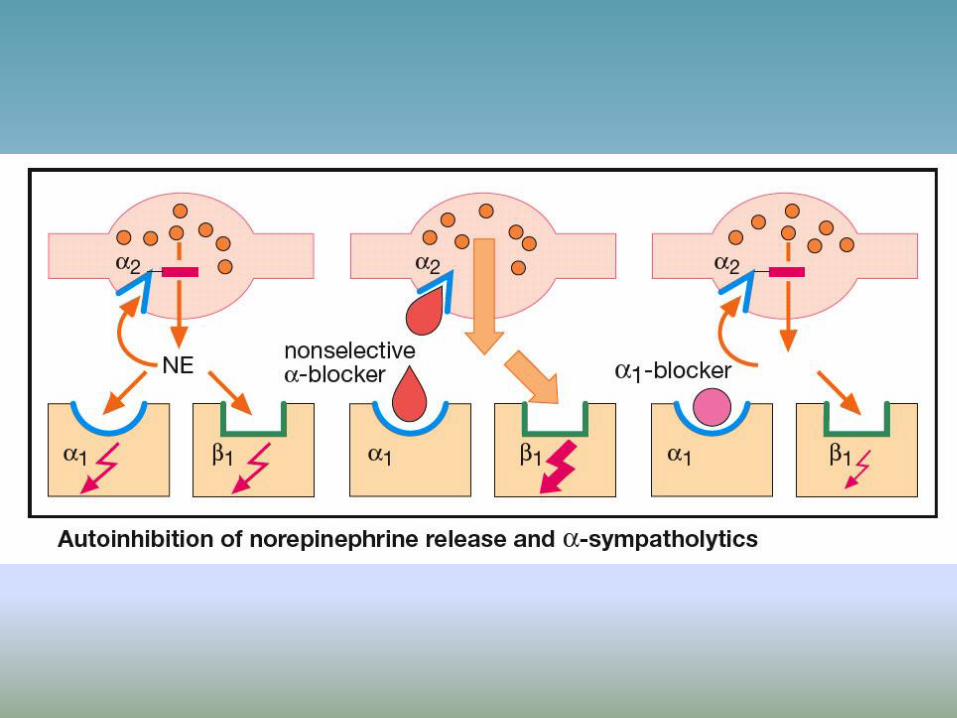
• α2-blockade in brain ↑se vasomotor tone.
• Block pressor action of adrenaline, fall in BP due
toβ2.
action- “vasomotor reversal of Dale”
• Actions of selective α-agonists supressed.
Heart
• Reflex tachycardia due to:-
fall in mean arterial pressure
Blockade of presynaptic α2 receptors- ↑ NA release.
Nose: nasal stuffiness
Eye: miosis
GIT: intestinal motility ↑se
Kidney: Hypotension
↓se GFR
NA+ & H2O reabsorption
Urinary bladder
• α1A blockade- ↓se tone of smooth muscle in trigone,
sphincter & prostrate.
• Improved urine flow, used in BPH.
Reproductive system
• Contraction of vas deferens result in ejaculation
through α receptors.
• Blockade results in impotence.
Alpha-Blocking Drugs
A. Classification
–based on: selective affinity for alpha receptors, reversibility
1. Irreversible, long-acting alpha blockers
2. Reversible, short-acting alpha blockers
3. a1-selective blockers
4. a2-selective blockers
Classification
1. Irreversible alpha blockers : Phenoxybenzamine
–slightly a 1 -selective, long-acting
2. Reversible alpha blockers: Phentolamine (nonselective), tolazoline (slightly a 2 -selective)
3. a 1 blockers: Prazosin, Doxazosin, Terazosin
4. a 2 blockers: Yohimbine
used primarily in researches
Pharmacokinetics
• All active orally as well as parenterally
• Phenoxybenzamine: short t1/2 but long duration-48 hr (covalent bond)
• Phentolamine, tolazoline: parenteral,
duration 20-40 min by parenteral route
• Prazosin: oral, duration 8-10 hr
Irreversible non-selective α- blockers
Phenoxybenzamine
• Cyclizes spontaneously to highly reactive
ethyleniminium intermediate.
• Binds covalently to α-receptors- irreversible or non-
equilibrium competitive block.
• Blockade is slow onset & longer duration (3-4 days).
• Also inhibits reuptake of NE.
• Shifts blood from pulmonary to systemic circuit.
• Shift fluid from extravascular to vascular compartment-
relaxation of postcapillary vessels.
Reversible alpha blockers
Yohimbine
• Natural alkaloid from Pausinystalia yohimbe.
• No established clinical role.
Idazoxan
• Has membrane stabilizing action.
Ergot alkaloids
• Ergotamine & Dihydroergotamine
• Competitive α-receptor blockers.
• Principal use is migraine.
Reversible, selective α1- blockers
Prazosin
• Highly selective α1-blocker , α1: α2 selectivity 1000:1
• Fall in BP with only mild tachycardia.
• Dilates arterioles more than veins
• Postural hypotension occurs as 1st dose effect,
minimized by starting with low doses at bed time.
• Also inhibits PDE- ↑se cAMP in smooth muscle.
PK
• Effective orally, BA- 60%.
• Highly bound to plasma proteins (α1 acid
glycoprotein).
• Metabolized in liver, 1o excreted in bile.
• t1/2 – 2-3hrs, effect lasts for 6-8hrs.
Uses
• Primarily as antihypertensive.
• LVF not controlled by diuretics & digitalis.
• Raynaud’s disease
• BPH
• Scorpion sting
PK
• Preferred ROA- i.v.
• Lipid soluble penetrates brain.
• Mainly excreted through urine in 24 hrs.
• Accumulates in adipose tissue on ch. Administration.
Dose
20-60 mg/d oral
1mg/kg/1hr slow i.v infusion.
Uses
Pheochromocytoma, occasionally 2oshock, PVD.
Reversible non-selective α-blockers
Tolazoline
• Block is modest & short lasting.
• Direct vasodilator & stimulates the heart.
• Also blocks 5-HT receptors, histamine like gastric secretagouge & Ach like motor action on intestine.
SE
• N, V, cramps, diarrhoea, nervousness, chills
• Tachycardia, Exacerbation of MI, peptic ulcer.
Use
• PVD
• Pulmonary HT of newborn.
• Cause reflex tachycardia (due to decreasedMAP)
• Tachycardia may be exaggerated because a 2receptors are also blocked.
• e.g. phenoxybenzamine, phentolamine, tolazoline
Effects of Alpha Blockers
1. Nonselective alpha blockers (cont)
Clinical Uses
1. Nonselective alpha-blockers
Presurgery of pheochromocytoma: phenoxybenzamine
During surgery: phentolamine (sometimes)
Carcinoid tumor: phenoxybenzamine (5-HT blocking)
Mastocytosis: phenoxybenzamine (H1 antihistamine)
Accidental local infiltration of alpha agonist: phentolamine
Overdose of sympathomimetics (amphetamine, cocaine, phenylpropranolamine)
Raynaud’ s phenomenon, erectile dysfunction (phentolamine)
2. Selective a 1 blockers
• The same effects as nonselective alpha blockers
• But cause much less tachycardia than nonselective blocker
• e.g. Prazosin, Doxazosin, Terazosin
Effects of Alpha Blockers
Clinical Uses
2. Selective a 1 -blockers
Prazosin and others
Essential Hypertension
Urinary hesitancy
Prevention of urinary retention in
benign prostatic hyperplasia (BPH)
Terazosin &Doxazosin
• Long acting( t1/212 & 18hr) congener of prazosin.
• Used in HTN & BPH as single daily dose.
Tamsulosin & Silodosin
• Uroselective α1A blocker
• α1A –bladder base, prostrate. α1B- blood vessels.
• Don't cause significant changes in BP & HR.
• t1/2- 6-9hr, MR cap(0.2-0.4 mg) can be taken OD.
• Efficacious in Rx of BPH.
• SE: retrograde ejaculation, dizziness,, floppy iris syd.
• Silodosin weaker(4-8mg/d) but longer acting.
Phentolamine
• More potent α-blocker than tolazoline.
• Other actions are less marked.
• Duration of action is shorter (min).
• Equally blocks α1 & α2 receptors- NA release ↑sed.
Uses
• ∆sis & intraop.management of pheochromocytoma. 5mg
i.v- B.P falls by 25(D)or35(S)mmHg.
• HTN due to clonidine withdrawl, cheese reaction.
• Dermal necrosis due to extravasated i.v NA/DA. Given S.C as local infiltration.
Bunazosin & Alfuzosin
• Orally effective α1 blockers similar to prazosin.
• Alfuzosin t1/2 4hrs (2.5mgTDS or 10mg SR OD).
• CI in hepatic impairment, metabolized in liver.
• Bunazosin slightly longer t1/2.
• Primarily used in BPH.
F Adverse effects of Alpha blockers
Orthostatic hypotension (venodilatation)
Reflex tachycardia (nonselective > selective)
First dose hypotension (take before going to bed)
Nausea/vomiting
Caution in patients with coronary artery disease (CAD or CHD): angina
Side effects of α-blockers
• Palpitation
• Postural hypotension
• Nasal blockade
• Diarrhea
• Fluid retention
• Inhibition of ejaculation & impotence.
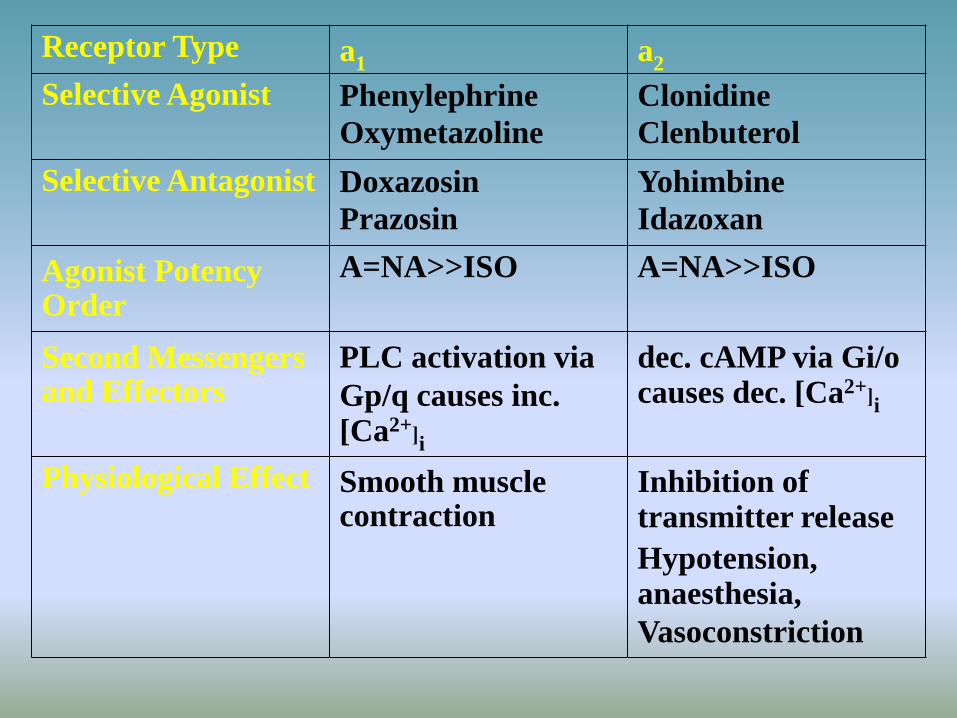
Receptor Type a1 a2
Selective Agonist Phenylephrine
Oxymetazoline
Clonidine
Clenbuterol
Selective Antagonist Doxazosin
Prazosin
Yohimbine
Idazoxan
Agonist Potency Order
A=NA>>ISO A=NA>>ISO
Second Messengers and Effectors
PLC activation via
Gp/q causes inc. [Ca2+]i
dec. cAMP via Gi/o causes dec. [Ca2+]i
Physiological Effect Smooth muscle contraction
Inhibition of transmitter release
Hypotension, anaesthesia,
Vasoconstriction
Beta-Blocking Drugs
A. Classification and Mechanisms
All are competitive antagonists
Propranolol is prototype
Classification is based on
Beta subtypes selectivity
Partial agonist activity
Lipid solubility
Local anesthetic action
3. Propranolol is contraindicated in
one of the following diseases:
a) Hypertension
b) Tachycardia
c) Hyperthyroidism
d) Angina pectoris
e) Bronchial asthma
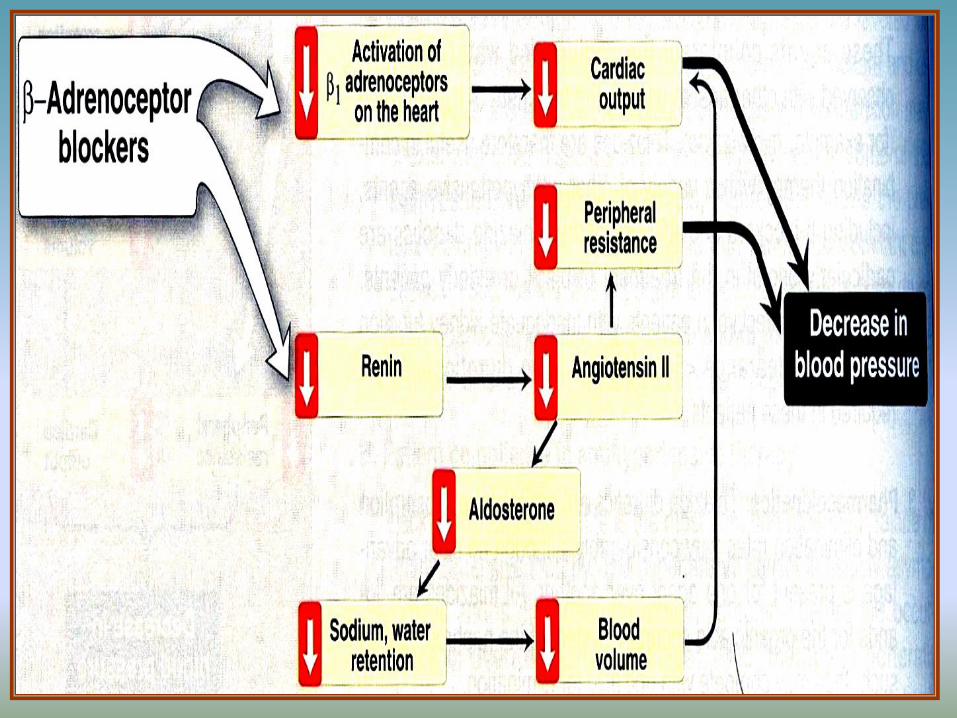
4. Propranolol produces its
antihypertensive action by:
a) Vasodilatation
b) Ganglionic blockade
c) Decreased cardiac output
d) A diuretic action
e) Blockade of 1 receptors
Classification and Mechanisms
1. Receptor selectivity
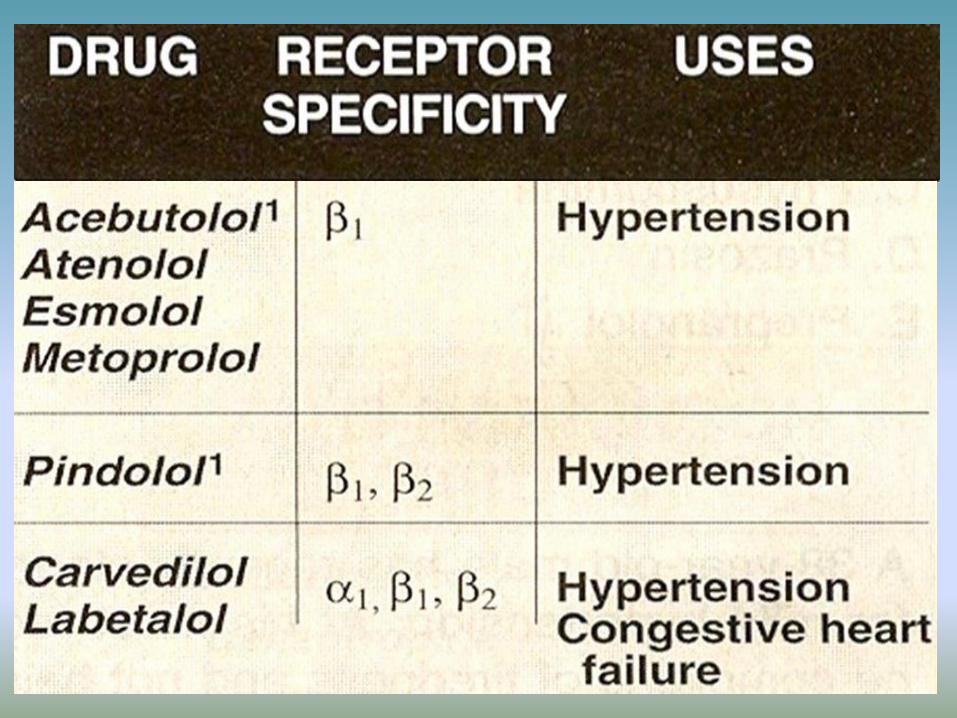
– b 1 -selective: metoprolol, atenolol
– b 2 -selective: butoxamine (research
only)
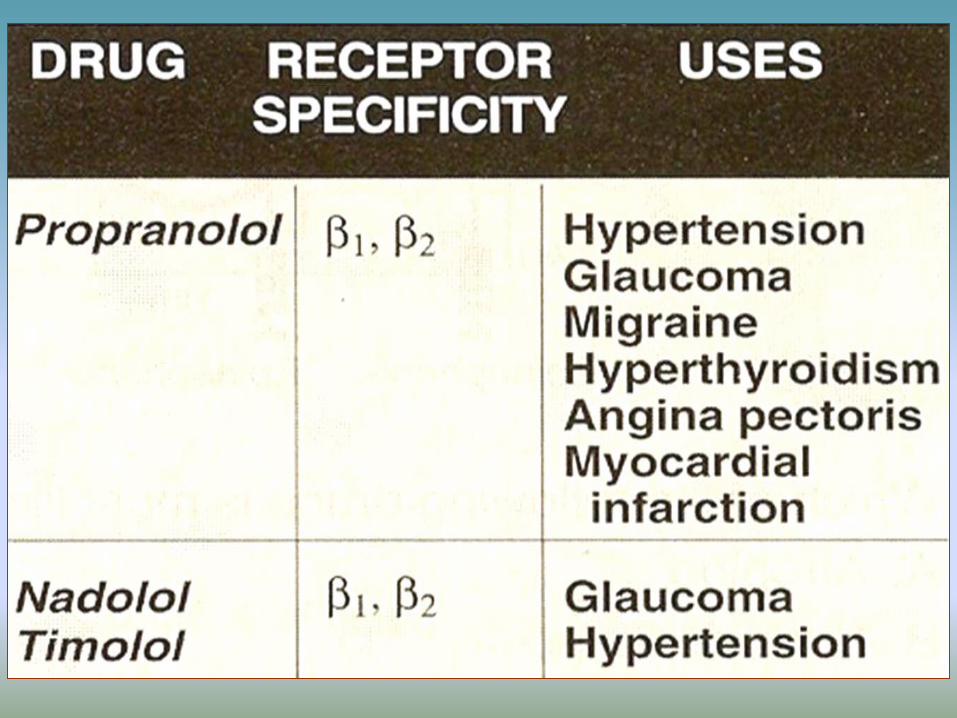
– Nonselective: propranolol
–Combined beta- and alpha-blocking: labetalol
A. Classification and Mechanisms
Partial agonist activity
–Intrinsic sympathomimetic
activity, ISA
–eg, pindolol, acebutolol
–may be useful in patients
with asthma
Classification and Mechanisms
3. Local anesthetic activity (membrane-stabilizing activity):
–disadvantage when used topically in the eye
–timolol: no this activity
4. Lipid solubility
–responsible for CNS adverse effects: propranolol
Pharmacokinetics of Beta blockers
• For systemic effects, developed for chronic oral use
• Esmolol: short-acting--only used parenterally
• Nadolol: longest-acting
• Atenolol, acebutolol are less lipid-soluble
Effects and Clinical Uses
• Predict from beta blockade
–decreased HR, force of contraction
–decreased A-V conduction
–slow firing rate of SA node
• Cardiovascular and ophthalmicapplications are extremly important
Clinical Uses
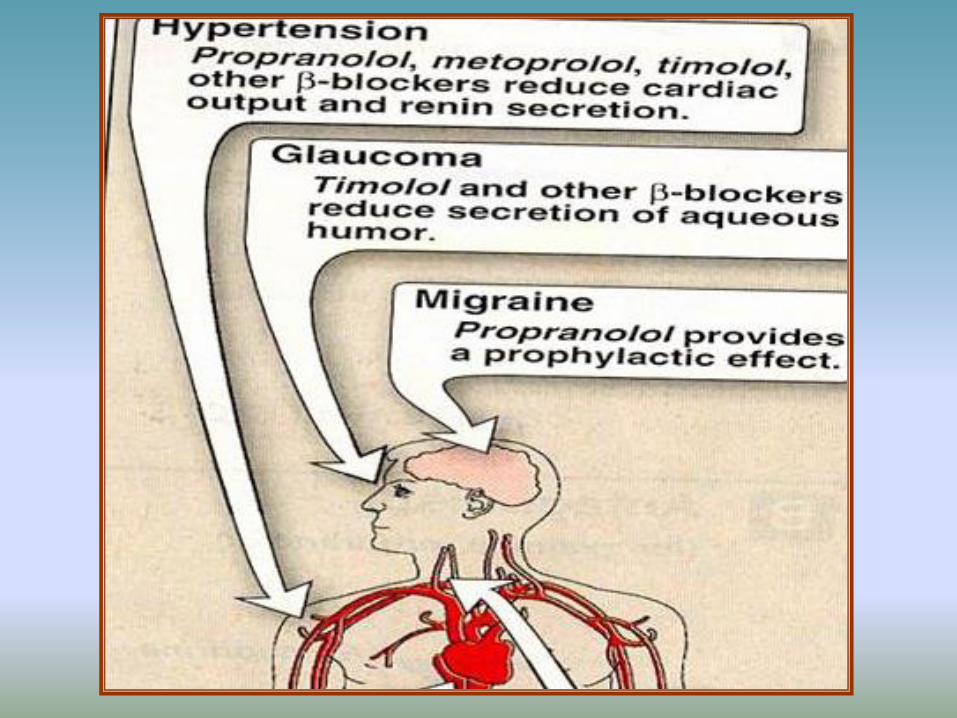
• CVS: hypertension, angina pectoris, arrhythmia prophylaxis after MI, supraventricular tachycardias, hypertrophic cardiomyopathy, congestive heart failure*
• Glaucoma: reduce aqueous humor secretion (timolol)
Clinical Uses
• Migraine: propranolol
• Thyroid storm, thyrotoxicosis: propranolol
• Famillial tremor, other types of
tremor, “stage fright” : propranolol
Adverse effects
• CVS: bradycardia, A-V blockade, congestive heart failure
• Patients with airway disease: asthmatic attack
• Mask sign of hypoglycemia in diabetic patients: tachycardia, tremor, anxiety
• CNS effects: sedation, fatigue, sleep alterations
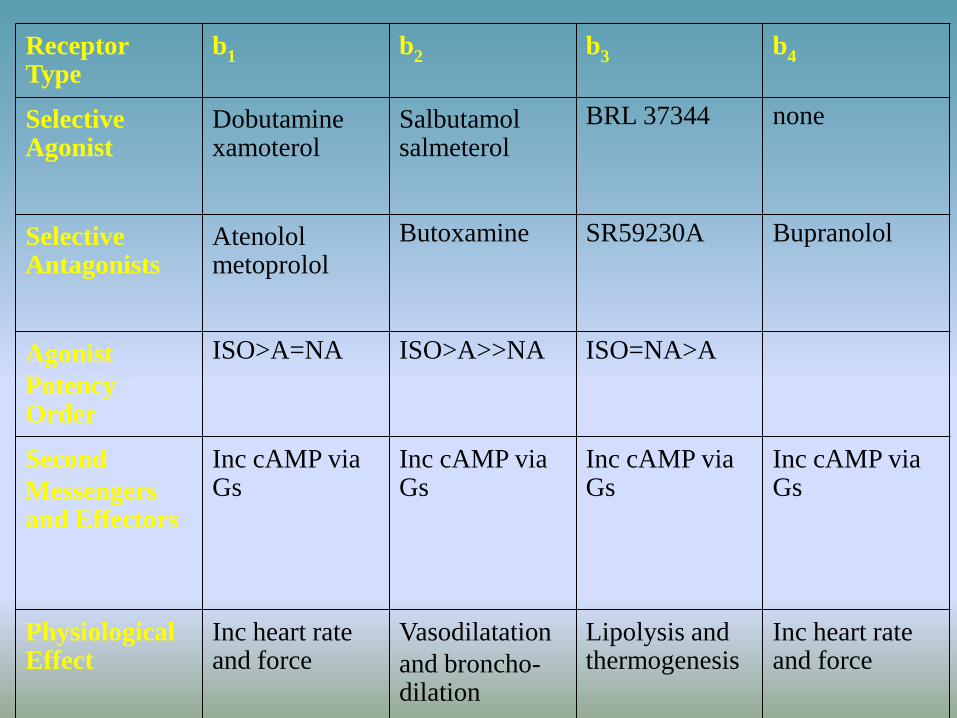
Receptor Type
b1 b2 b3 b4
Selective Agonist
Dobutamine xamoterol
Salbutamol salmeterol
BRL 37344 none
Selective Antagonists
Atenolol metoprolol
Butoxamine SR59230A Bupranolol
Agonist
Potency Order
ISO>A=NA ISO>A>>NA ISO=NA>A
Second
Messengers and Effectors
Inc cAMP via Gs
Inc cAMP via Gs
Inc cAMP via Gs
Inc cAMP via Gs
Physiological Effect
Inc heart rate and force
Vasodilatation
and broncho-dilation
Lipolysis and thermogenesis
Inc heart rate and force

SUMMARY
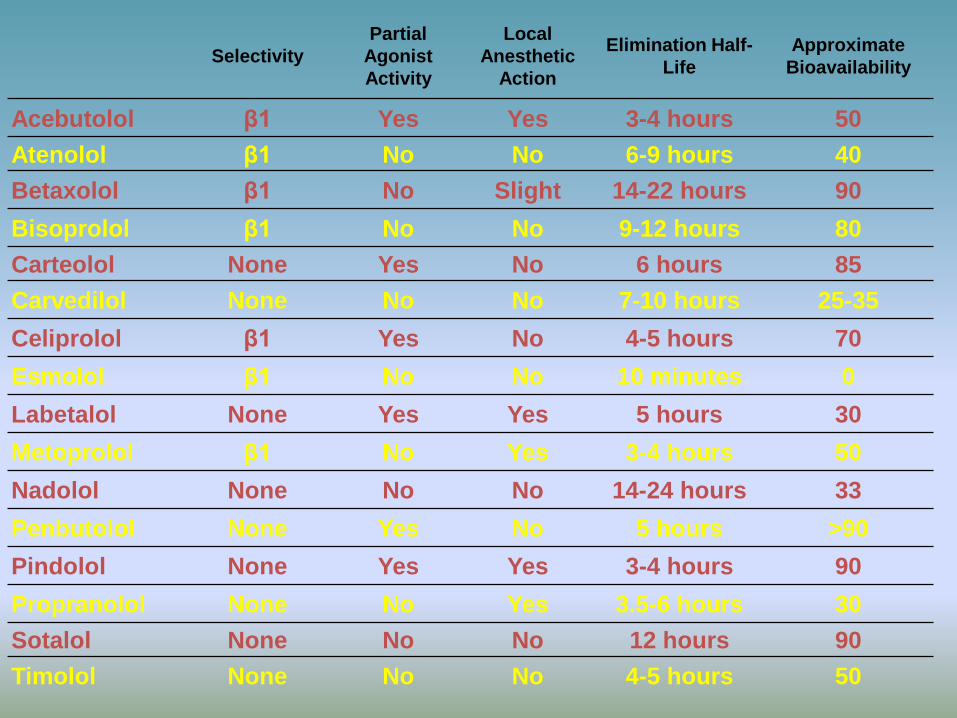
Selectivity
Partial
Agonist
Activity
Local
Anesthetic
Action
Elimination Half-
Life
Approximate
Bioavailability
Acebutolol β1 Yes Yes 3-4 hours 50
Atenolol β1 No No 6-9 hours 40
Betaxolol β1 No Slight 14-22 hours 90
Bisoprolol β1 No No 9-12 hours 80
Carteolol None Yes No 6 hours 85
Carvedilol None No No 7-10 hours 25-35
Celiprolol β1 Yes No 4-5 hours 70
Esmolol β1 No No 10 minutes 0
Labetalol None Yes Yes 5 hours 30
Metoprolol β1 No Yes 3-4 hours 50
Nadolol None No No 14-24 hours 33
Penbutolol None Yes No 5 hours >90
Pindolol None Yes Yes 3-4 hours 90
Propranolol None No Yes 3.5-6 hours 30
Sotalol None No No 12 hours 90
Timolol None No No 4-5 hours 50