Embed Size (px)
Citation preview
BY ASLAM MATANIA
GROUP-3FACULTY OF MEDICINE
TSMU
MYCOBACERIUM LEPRAE
INTRODUCTION IT IS A GRAM POSITIVE ORGANISM
CAUSING LEPROSY OR HANSEN’S DISEASE.
IT IS NON-MOTILE, NON-SPORING, ACID FAST BACILLI WHICH IS MAINLY RESPONSIBLE FOR CAUSING DAMAGE TO NERVES.
– this organism was described by Hansen in 1873– it has not been
cultivated on nonliving bacteriologic media– There are more than
10 million cases of leprosy, mainly in Asia
Armauer Hansen in 1873
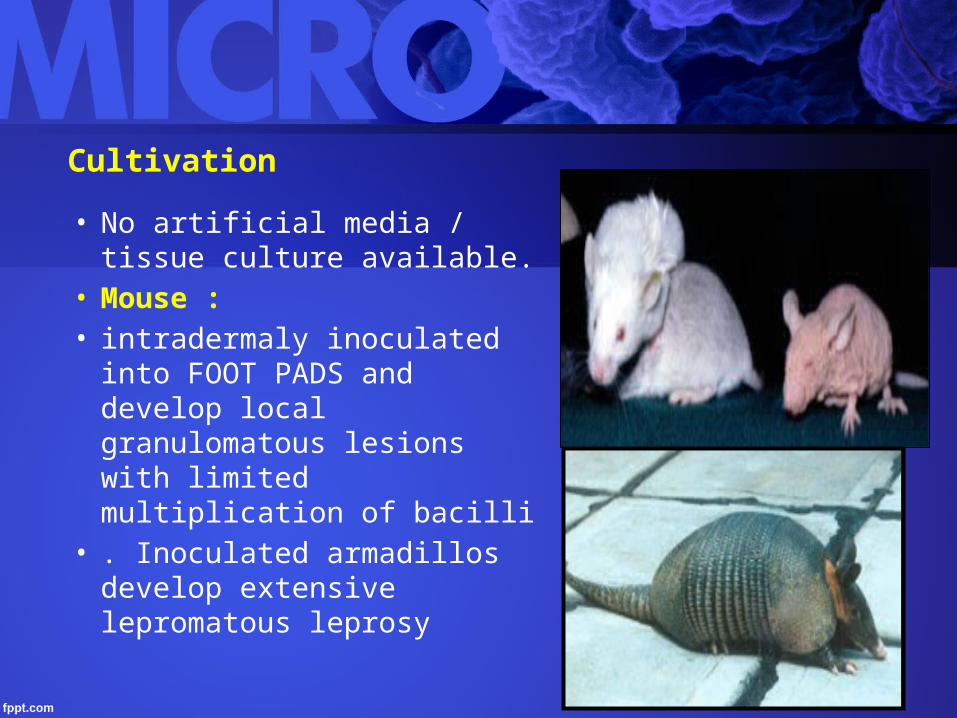
Cultivation
• No artificial media / tissue culture available.
• Mouse :• intradermaly inoculated into
FOOT PADS and develop local granulomatous lesions with limited multiplication of bacilli
• . Inoculated armadillos develop extensive lepromatous leprosy
Epidemiology
• Without prophylaxis, about 10% of exposed children may acquire the disease
• The incubation period is probably 2–10 years.• The naturally infected armadillos found in Texas and
Mexico probably play no role in transmission of leprosy to humans.
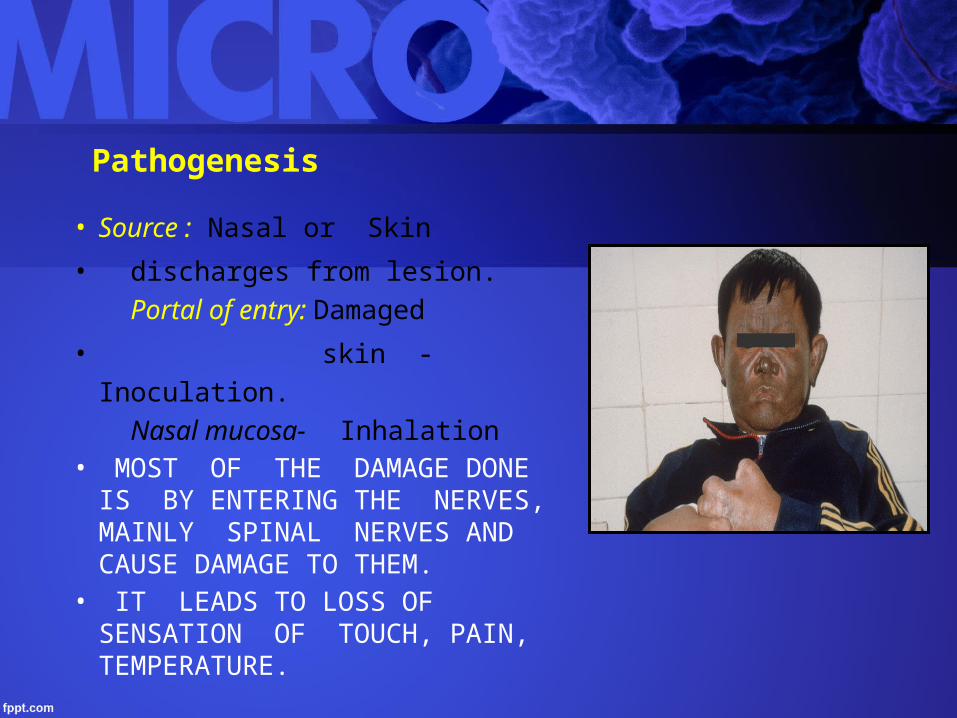
Pathogenesis
• Source : Nasal or Skin
• discharges from lesion. Portal of entry: Damaged
• skin -Inoculation. Nasal mucosa- Inhalation
• MOST OF THE DAMAGE DONE IS BY ENTERING THE NERVES, MAINLY SPINAL NERVES AND CAUSE DAMAGE TO THEM.
• IT LEADS TO LOSS OF SENSATION OF TOUCH, PAIN, TEMPERATURE.
• IT LEADS TO WHITE PATCHES ON THE SKIN WHICH ARISE DUE TO LOSS OF PIGMENTATION FROM SKIN.
• IF THIS DISEASE STARTS DETERIORATING , NODES APPEAR ON THE SKIN WHICH CONTAINS BUNDLES OF BACTERIA, SLOWLY IT DISSESEMINATES INTO THE COMPLETE BODY AND CAUSES FORMATION OF “ GRANULOMA”
• THIS GRANULOMA IS DIFFERENT FROM TUBERCLE GRANULOMA DUE TO ABSENCE OF CENTRAL CASEIATING NECROSIS.
STAGES OF LEPROSY
• The disease is divided into two major types, lepromatous and tuberculoid, with several intermediate stages
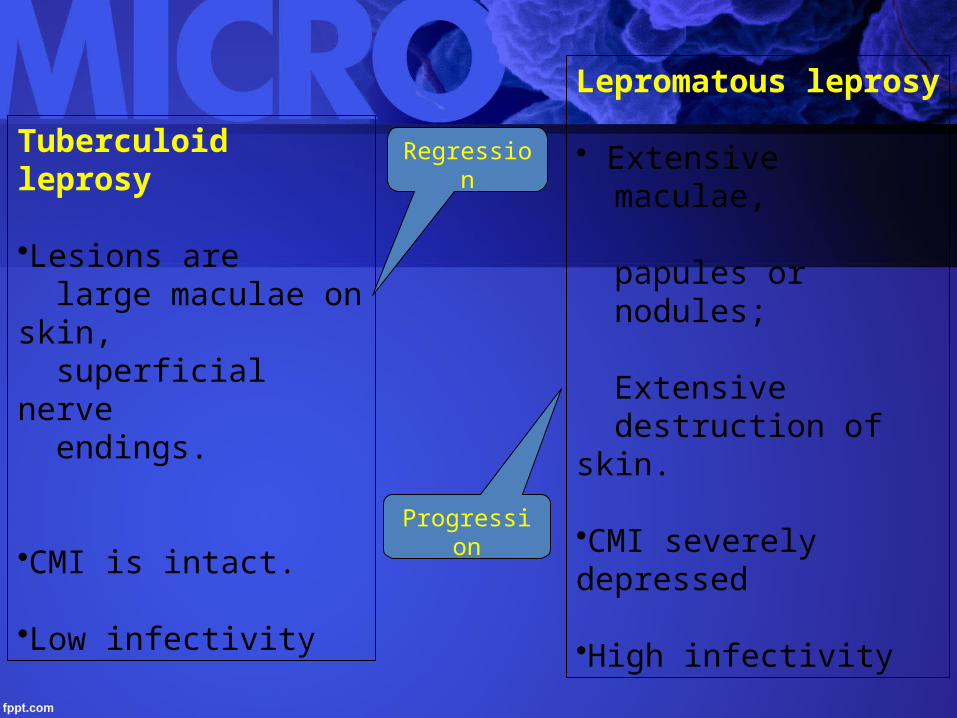
Tuberculoid leprosy
•Lesions are large maculae on skin, superficial nerve endings.
•CMI is intact.
•Low infectivity
Lepromatous leprosy
• Extensive maculae,
papules or nodules;
Extensive destruction of skin.
•CMI severely depressed
•High infectivity
Regression
Progression
Generalized form with decreased CMI.
“Lepromata” : Granulation tissue with plenty of vacuolated cells
Ulceration
Secondary infection &Mutilation of limbs.
Skin lesions are extensive and bilaterally symmetrical.
Lepromatous leprosy
Face,ear lobules,hands and feet.
Symmetrical thickening of peripheral nerves
& anesthesia.
Bacilli invade mucosa of Nose , Mouth and
Respiratory tract → shed in secretions.
Bacteremia present.
Auto antibodies are produced.
Lateral part of eyebrows are lost.

Lepromatous leprosy Lepromatous leprosy
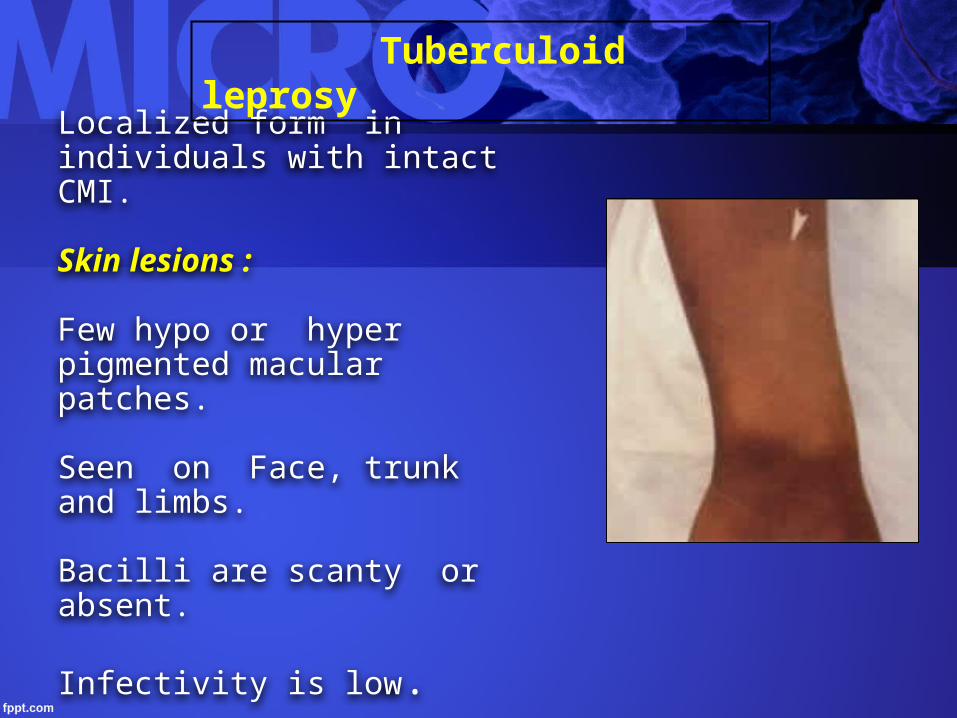
Localized form in individuals with intact CMI.
Skin lesions :
Few hypo or hyper pigmented macular patches.
Seen on Face, trunk and limbs.
Bacilli are scanty or absent.
Infectivity is low.
Tuberculoid leprosy
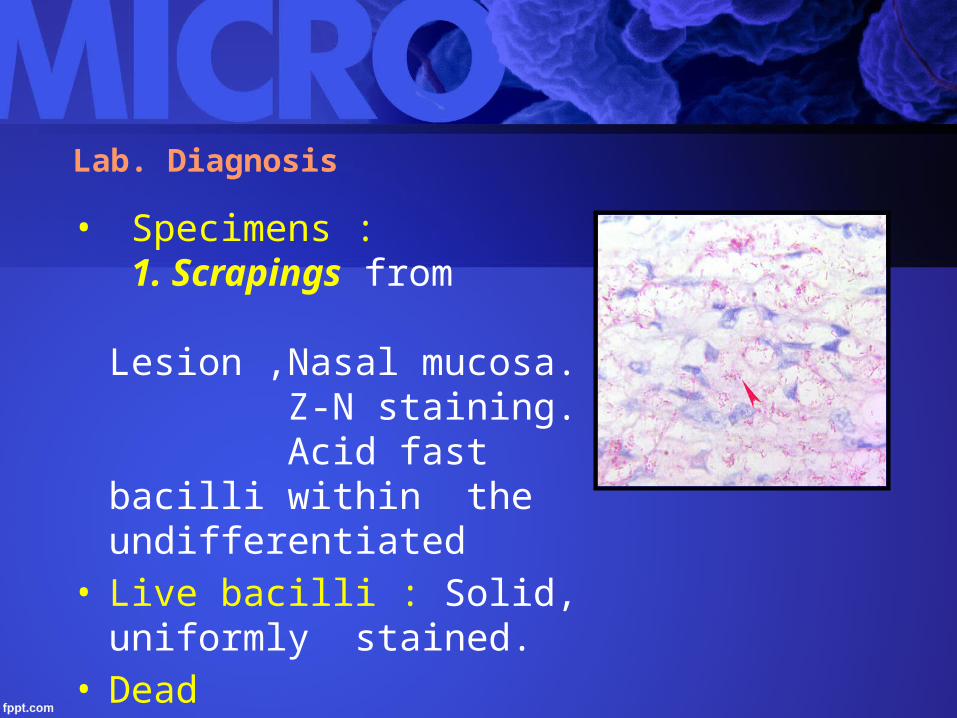
Lab. Diagnosis
• Specimens : 1. Scrapings from Lesion ,Nasal mucosa. Z-N staining. Acid fast bacilli within the undifferentiated
• Live bacilli : Solid, uniformly stained.
• Dead bacilli :Fragmented and granular.
• 2. Skin & Nerve biopsy.
• 3.Ear lobules ( Slit skin smear ).
• 5. Lepromin test : To know prognosis. • Not for diagnosis.• 6.Molecular diagnosis: Identifying DNA
codes for • 65 & 18-kDa M.leprae proteins.
Treatment :
• Sulfones such as dapsone are first-line therapy for both tuberculoid and lepromatous leprosy
• RMP or clofazimine generally is included in the initial treatment regimens
• Other drugs active against M leprae include minocycline, clarithromycin, and some fluoroquinolones.