Embed Size (px)
Citation preview

Surgical Removal of teethSurgical Removal of teeth
ByBy
Dr. Essam M. AshourDr. Essam M. AshourBDS 1992, Ms 2000, Alexandria UniversityBDS 1992, Ms 2000, Alexandria University
PHD 2007, Cairo UniversityPHD 2007, Cairo University
Lecturer of Oral & Maxillofacial Surgery,Lecturer of Oral & Maxillofacial Surgery,Oct. 6 UniversityOct. 6 University
Head of Oral & Maxillofacial Surgery Unit, Head of Oral & Maxillofacial Surgery Unit, Oct. 6 University HospitalOct. 6 University Hospital
Surgical ExodontiaSurgical Exodontia

Surgical extraction is the method by which a tooth is removed from its socket, after creating a flap and removing part of the bone that surrounds the tooth.
Indications:

1. Teeth of the maxilla or mandible that present unusual root morphology.

2. 2. Teeth with hypercementosis of root and root tips, presenting large bulbous roots

3. 3. Teeth with dilaceration of root tips

4. 4. Teeth with ankylosed roots or with abnormalities, e.g., dens in dente

5. 5. Impacted and semi-impacted teeth

6. 6. Teeth fused with an adjacent tooth

7. 7. Maxillary posterior teeth, whose roots are included in the maxillary sinus

88. . Roots with periapical lesions, whose entire removal through the tooth socket
would not be possible with curettage alone

9. 9. Roots of teeth found below the gum line, when their removal is impossible by any
other way

10. 10. Deciduous molars whose roots embrace the crown of the subjacent premolar.

Basic Principles of Basic Principles of Dentoalveolar SurgeryDentoalveolar Surgery
Radiographic examinationRadiographic examination Access to the field of operationAccess to the field of operation Reduction of resistanceReduction of resistance Removal of tooth structureRemoval of tooth structure Debridement of the fieldDebridement of the field ClosureClosure Post-operative carePost-operative care

I.Radiographic examinationI.Radiographic examination Root patternRoot pattern Relation to Relation to
important important structuresstructures• Max sinusMax sinus• TuberiosityTuberiosity• IANIAN• Mental N.Mental N.

II. Access to the field of II. Access to the field of operationoperation
Adequate visibility Adequate visibility during surgery is during surgery is very important.very important.
1.1. Adequate Light.Adequate Light. Continually reposition the Continually reposition the
source of light, modify your source of light, modify your position to avoid obstructing position to avoid obstructing the light, or use a headlight.the light, or use a headlight.

2. Adequate access2. Adequate access::
a)a) Ability to open the mouth widely.Ability to open the mouth widely.b)b) A surgical field free of excess blood A surgical field free of excess blood
& other fluids.& other fluids.c)c) Surgically created exposure.Surgically created exposure.d)d) Retraction of tissues away from the Retraction of tissues away from the
surgical field.surgical field.

Adequate accessAdequate access Ability to open the mouth widelyAbility to open the mouth widely
1.1. Mouth props:Mouth props: Rubber bite blocks Rubber bite blocks
used to hold the used to hold the mouth open.mouth open.
2.2.Mouth Gag:Mouth Gag: Used to open the Used to open the
mouth with mouth with uncooperative uncooperative patients.patients.

Adequate accessAdequate access A surgical field free of excess blood & other fluidsA surgical field free of excess blood & other fluids The typical suction is one that The typical suction is one that
has a small orifice so that has a small orifice so that the tooth socket or surgical the tooth socket or surgical cavity can be suctioned.cavity can be suctioned.
Fergusson suctionFergusson suction: Has a : Has a hole in the handle portion hole in the handle portion that can be covered to that can be covered to remove solutions rapidly as remove solutions rapidly as during cutting bone under during cutting bone under copious irrigation, and when copious irrigation, and when soft tissue is being soft tissue is being suctioned the hole is suctioned the hole is uncovered to prevent tissue uncovered to prevent tissue injury.injury.

Soft tissue flap:Soft tissue flap: The flap is a section of soft tissue that is The flap is a section of soft tissue that is
outlined by a surgical incision, carries its outlined by a surgical incision, carries its own blood supply, allows surgical access own blood supply, allows surgical access to underlying tissues, can be replaced into to underlying tissues, can be replaced into its original position to cover & protect the its original position to cover & protect the site of surgery and can be maintained with site of surgery and can be maintained with sutures & expected to heal & promote sutures & expected to heal & promote good healing to underlying tissues. good healing to underlying tissues.
II. Access to the field of operationII. Access to the field of operation Surgically created exposureSurgically created exposure

Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps
1. 1. The incision must be carried out with a firm, continuous stroke, not interrupted strokes.
. During the incision, the scalpel should be in constant contact With bone.
Repeated strokes at the same place, manytimes, impair wound healing.

2. 2. Flap design and incision should be carried out in such a way that injury of anatomic structures is avoided, such as:
The mental neurovascular bundle, palatal vessels emerging from the greater palatine foramen and incisive foramen, infraorbital nerve, lingual nerve, submandibular duct & parotid duct.
Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps

Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps
3. 3. The width of the flap must be adequate, so that the operative field is easily accessible, allowing easy instrumentation without creating tension and trauma during manipulation.
4. The base of the flap must be broader than the free gingival margin, to ensure adequate blood supply and to promote healing. Compromised blood supply can cause ischemic necrosis of the flap.

5. 5. The flap itself must be larger than the bone defect so that the flap margins, when sutured, are resting on intact, healthy bone and not over missing or unhealthy bone, thus preventing flap dehiscence and tearing.
Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps

6. 6. The flap should be a full-thickness mucoperiosteal flap including the surface mucosa, submucosa and periosteum which must be reflected together. This is achieved (after a deep incision) when the mucoperiosteal elevator is continuously kept and pressed firmly against the bone.
Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps

7. 7. Vertical releasing incisions should begin approximately at the buccal vestibule and end either mesial or distal to the interdental papillae of the gingiva in order not to damage the papilla or alter its contour.
Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps

Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps
8. Flaps performed in edentulous 8. Flaps performed in edentulous ridges in the process of alveoloplasty ridges in the process of alveoloplasty must be trimmed of their excess to must be trimmed of their excess to cover the alveolus without overlaping cover the alveolus without overlaping at their edges. To avoid the at their edges. To avoid the formation of flappy ridges.formation of flappy ridges.

Ideal requirements of Ideal requirements of mucoperiosteal flapsmucoperiosteal flaps
9. 9. During the surgical procedure, excessive pulling and crushing or folding of the flap must be avoided, because the blood supply is compromised and healing is delayed.

Types of FlapsTypes of FlapsFlaps may be described by:Flaps may be described by:
-Shape (pyramidal, semilunar)-Shape (pyramidal, semilunar)-Location (buccal, palatal)-Location (buccal, palatal)-Tissue included (skin, mucosal, -Tissue included (skin, mucosal,
mucoperiosteal)mucoperiosteal)-Number of incision lines (2 or 3 lines)-Number of incision lines (2 or 3 lines)-Number of corners (3 or 4 corners)-Number of corners (3 or 4 corners)-Microvascular.-Microvascular.

A. Triangular Flap (2 incision lines)
This flap is the result of an L-shaped incision with a horizontal incision made along the gingival sulcus and a vertical or oblique incision.
The vertical incision begins approximately at the vestibular fold and extends to the interdental papilla of the gingiva
. The triangular flap is performed labially or buccally on both jaws and is indicated in the
surgical removal of root tips, small cysts, and apicectomies.
1. Pyramidal flaps1. Pyramidal flaps


B. Trapezoidal Flap (3 incision lines)B. Trapezoidal Flap (3 incision lines)
The trapezoidal flap is created by a horizontal incision along the gingival sulcus, and two oblique vertical releasing incisions extending to the buccal vestibule.
The vertical releasing incisions always extend to the interdental papilla and never to the center of the labial or buccal surface of the tooth.
1. Pyramidal flaps1. Pyramidal flaps


1. Pyramidal flaps1. Pyramidal flaps(Triangular & Trapezoidal)(Triangular & Trapezoidal)
AdvantagesAdvantages• Adequate exposure & excellent access. Adequate exposure & excellent access. • Allow discovery of local pathosis.Allow discovery of local pathosis.• Allows resting on sound bone.Allows resting on sound bone.• Allows surgery to be performed on more than
one or two teeth.
DisadvantagesDisadvantages• Disturb gingival attachment Disturb gingival attachment (recession of
gingiva).

2. Semilunar flaps2. Semilunar flaps This flap is the result of a curved incision, which
begins just beneath the vestibular fold and has a bow-shaped course with the convex part towards the attached gingiva.
The lowest point of the Incision must be at least 0.5 cm from the gingival margin, so that the blood supply is not compromised.
The horizontal component should not cross major prominences such as the canine eminence.
.


• AdvantagesAdvantages Avoids disturbance to the gingiva Avoids disturbance to the gingiva
attachmentattachment
• DisadvantagesDisadvantages Limited exposureLimited exposure
• RequisitesRequisites 0.5 mm away from the gingival margin0.5 mm away from the gingival margin
2. Semilunar flaps2. Semilunar flaps

3. Gingival (Envelope) flaps 3. Gingival (Envelope) flaps Normally this flap is made by incising the Normally this flap is made by incising the
tissues in the gingival sulcus around the tissues in the gingival sulcus around the necks of several teeth and spreading the necks of several teeth and spreading the flap away from the bone.flap away from the bone.
The envelope flap is used for surgery of incisors, premolars and molars, on the labial or buccal and palatal or lingual surface and is usually indicated when the surgical procedure involves the cervical lines of the teeth


• AdvantagesAdvantages Avoids oblique incisions.Avoids oblique incisions. Avoids large area of periosteal detachment.Avoids large area of periosteal detachment. Minimize postoperative pain and edema.Minimize postoperative pain and edema.
• DisadvantagesDisadvantages Limited & shallow exposure.Limited & shallow exposure. Increased incidence of flap lacerations.Increased incidence of flap lacerations.
• RequirementsRequirements Adequate extensionAdequate extension..
3. Gingival (Envelope) flaps 3. Gingival (Envelope) flaps

4. Palatal flaps4. Palatal flaps Y-shaped Palatal FlapY-shaped Palatal Flap An incision is made along the midline of the
palate, as well as two anterolateral incisions, which are anterior to the canines to avoid severing of the nasopalatine artery to prevent bleeding.
This type of flap is indicated in surgical procedures involving the removal of small exostoses & small palatal tori.
.

Double Y-shaped Palatal FlapsDouble Y-shaped Palatal Flaps
This type of flap is used in larger palatal tori & bony exostoses, and is basically an extension of the Y-shaped incision. The difference is that two more posterolateral incisions are made, which are necessary for adequate access to the surgical field.
This flap is designed such that major branches of the greater palatine artery are not severed.
4. Palatal flaps4. Palatal flaps


5. Pedicle Flaps5. Pedicle Flaps The Pedicle flap is The Pedicle flap is
designed to be designed to be mobilized from one mobilized from one area and rotated to area and rotated to fill a soft tissue fill a soft tissue defect in another defect in another area like in closure area like in closure of oro-antral of oro-antral communications.communications.

The IncisionThe Incision Incisions are made Incisions are made
by means of sterile by means of sterile disposable disposable Bard Bard Parker Parker blades blades mounted on sterile mounted on sterile Bard Parker Bard Parker blade handles.blade handles.



Scalpel (Handle and Blade)
Handle: The most commonly used handle in oral surgery is the Bard Parker blade handle no. 3.
Its tip may receive different types of blades.
The IncisionThe Incision

Blade Blades are disposable and are of three different types (nos.
11, 12, and 15).
Blade is no. 15 The most common type used for flaps and incisions on edentulous alveolar ridges.
Blade no. 12 is indicated for incisions in inaccessible areas such as the maxillary tuberosity & retromolar areas.
Blade no. 11 is used for small incisions, such as those used for incising abscesses (stap incision)
.
The IncisionThe Incision


Basic principles of tissue Basic principles of tissue incisionincision
1.1. A sharp blade of proper size should A sharp blade of proper size should be used.be used.
2. One firm, smooth, continuous stroke 2. One firm, smooth, continuous stroke should be used keeping the blade in should be used keeping the blade in contact with bone through out the contact with bone through out the entire incision.entire incision.

Basic principles of tissue Basic principles of tissue incisionincision
3. The incisions through tissues should be 3. The incisions through tissues should be made with the blade held perpendicular to made with the blade held perpendicular to the epithelial surface in order to produce the epithelial surface in order to produce wound edges that can be easily reoriented wound edges that can be easily reoriented & re-approximated properly during & re-approximated properly during suturing, thus preventing necrosis of suturing, thus preventing necrosis of wound edges. wound edges.
For gingival incisions, the blade is held at For gingival incisions, the blade is held at a slight angle to the teeth.a slight angle to the teeth.

Basic principles of tissue Basic principles of tissue incisionincision
4.Avoid cutting through vital structures 4.Avoid cutting through vital structures as the mental, lingual, nasopalatine as the mental, lingual, nasopalatine & greater palatine neurovascular & greater palatine neurovascular bundles.bundles.
5.Incisions should be properly placed 5.Incisions should be properly placed through attached gingiva & over through attached gingiva & over healthy bone to provide support to healthy bone to provide support to the healing wound. the healing wound.

Mucoperiosteal elevators used Mucoperiosteal elevators used for reflection of the intra-oral for reflection of the intra-oral
mucoperiosteal flapsmucoperiosteal flaps

RetractorsRetractorsMinnesota retractors forretraction of the cheek and tongue

RetractorsRetractors

RetractorsRetractors

III Reduction of ResistanceIII Reduction of Resistance
AimAim• Allow removal of teeth with the least Allow removal of teeth with the least
amount of force.amount of force.
MethodsMethods• Bone removalBone removal• Tooth sectioningTooth sectioning

III Reduction of ResistanceIII Reduction of Resistance Bone removalBone removal PurposePurpose
• Gaining access to the tooth structure.Gaining access to the tooth structure.• Reduction of resistance around the tooth.Reduction of resistance around the tooth.• Provides point of application.Provides point of application.• Provides space into which the tooth may be Provides space into which the tooth may be
displayed.displayed. MethodsMethods
• Chisels.Chisels.• Rotary (surgical burs)Rotary (surgical burs)• Bone Rongeur.Bone Rongeur.

III Reduction of ResistanceIII Reduction of Resistance
1.1. Bone removal using chiselsBone removal using chisels Chisels shapeChisels shape
1.1. Unibeveled.Unibeveled.2.2. Bibeveled (Osteotome).Bibeveled (Osteotome).3.3. Grooved.Grooved.


Bone removal using chiselsBone removal using chisels
Methods of applicationMethods of application
1.1. Hand driven (copland chisel)Hand driven (copland chisel)2.2. Mallet drivenMallet driven3.3. Electric Pneumatic drivenElectric Pneumatic driven

Bone removal using chiselsBone removal using chisels• AdvantagesAdvantages
Clean and smooth cutClean and smooth cut Rapid bone removalRapid bone removal No heat generationNo heat generation
• DisadvantagesDisadvantages Needs skill and trainingNeeds skill and training Not comfortable for the patientNot comfortable for the patient Not practical in extremely dense boneNot practical in extremely dense bone Not indicated in the maxilla to avoid fracture Not indicated in the maxilla to avoid fracture
of max. sinus bone, max. tuberosity or large of max. sinus bone, max. tuberosity or large segment of alv. Bone.segment of alv. Bone.

2. Bone removal using surgical burs2. Bone removal using surgical burs
Different sizes & shapes are available.Different sizes & shapes are available.
They work on straight hand piece or They work on straight hand piece or contra-angles.contra-angles.
Round burs are used to drill holes in the Round burs are used to drill holes in the bones which are then connected by the bones which are then connected by the Fissure bur.Fissure bur.


2. Bone removal using surgical burs2. Bone removal using surgical burs
PrecautionsPrecautions• Needs copious irrigationNeeds copious irrigation• Needs frequent replacement and cleaningNeeds frequent replacement and cleaning• Sharp burs should be used to avoid using extra pressure Sharp burs should be used to avoid using extra pressure
and time during cutting bone & to prevent postop. Pain and time during cutting bone & to prevent postop. Pain & necrosis.& necrosis.
AdvantagesAdvantages• ControllableControllable• Practical especially in dense bonePractical especially in dense bone• Safe & accurate in maxillaSafe & accurate in maxilla• Comfortable to the patientComfortable to the patient
DisadvantagesDisadvantages• Heat generation which can cause bone necrosis.Heat generation which can cause bone necrosis.

3. Bone removal using Rongeurs3. Bone removal using Rongeurs
Types:Types:
1.1. Side-cuttingSide-cutting; suitable for trimming ; suitable for trimming sharp edges of the alv. Plates.sharp edges of the alv. Plates.
2.2. End-cuttingEnd-cutting; suitable for cutting ; suitable for cutting bone septum projecting in the bone septum projecting in the socket of extracted teeth.socket of extracted teeth.
3.3. Side and end cuttingSide and end cutting..


4. Bone removal using Bone files4. Bone removal using Bone files Bone files are usually double-ended Bone files are usually double-ended
instruments with a small & large ends.instruments with a small & large ends.
They cannot remove large amounts of bone.They cannot remove large amounts of bone.
They are used only for final smoothening of They are used only for final smoothening of sharp bone edges or spicules of bone before sharp bone edges or spicules of bone before closure of the flap.closure of the flap.
The teeth of the bone file are arranged so The teeth of the bone file are arranged so that they remove bone on pull stroke only.that they remove bone on pull stroke only.


Tooth Sectioning or divisionTooth Sectioning or division Alone or together with bone removalAlone or together with bone removal 2 or more segments2 or more segments MethodMethod
• Surgical bursSurgical burs• ChiselsChisels
AdvantagesAdvantages• Minimizes amount of bone removalMinimizes amount of bone removal• Decrease operating timeDecrease operating time• Minimizes trauma to bone, thus less postop. Minimizes trauma to bone, thus less postop.
pain & edema.pain & edema.• Saves more alv. Bone for better prosthetic Saves more alv. Bone for better prosthetic
options.options.


IV. Removal of tooth structureIV. Removal of tooth structure
ForcepsForceps
ElevatorsElevators

Dental ElevatorsDental Elevators Instruments used in extraction of teeth Instruments used in extraction of teeth
which cannot be grasped by forceps.which cannot be grasped by forceps. Indications:Indications:
1.1. To luxate teeth before application of To luxate teeth before application of forceps specially in difficult extractions forceps specially in difficult extractions (impacted, malposed, fragile & endo-(impacted, malposed, fragile & endo-treated teeth).treated teeth).
2. To remove broken or surgically sectioned 2. To remove broken or surgically sectioned roots from their sockets.roots from their sockets.

Dental ElevatorsDental Elevators ComponentsComponents
• HandleHandle• ShankShank• BladeBlade

Dental ElevatorsDental ElevatorsClassification of elevatorsClassification of elevators According to shapeAccording to shape
• StraightStraight• Cross barCross bar• CurvedCurved
According to useAccording to use• Luxation of teeth & roots.Luxation of teeth & roots.• Complete extraction (Miller for extraction of Complete extraction (Miller for extraction of
upper wisdom)upper wisdom)• Apical root fragmentsApical root fragments• Reflection of flaps (Periosteal elevators)Reflection of flaps (Periosteal elevators)

Dental ElevatorsDental Elevators

Dental ElevatorsDental Elevators

Dental ElevatorsDental Elevators

Dental ElevatorsDental Elevators

Dental ElevatorsDental Elevators

Dental ElevatorsDental Elevators Rules of elevator useRules of elevator use Never use adjacent teeth as fulcrum.Never use adjacent teeth as fulcrum.
Never use the buccal plate as a fulcrum Never use the buccal plate as a fulcrum except in the area of ext. oblique ridgeexcept in the area of ext. oblique ridge
Controled movement with the left hand Controled movement with the left hand used as a guard to avoid slippage of the used as a guard to avoid slippage of the elevator with possible injury to hard or elevator with possible injury to hard or soft tissues.soft tissues.

Dangers in elevator useDangers in elevator use Loosening or extraction of adjacent teethLoosening or extraction of adjacent teeth Fracturing alveolar process, tuberiosity, Fracturing alveolar process, tuberiosity,
maxilla or mandiblemaxilla or mandible Forcing teeth or roots into nearby vital Forcing teeth or roots into nearby vital
structuresstructures• Maxillary sinusMaxillary sinus• IACIAC• Tissue spacesTissue spaces
Slippage leading to tissue injurySlippage leading to tissue injury• Lingual nerveLingual nerve• Soft palateSoft palate• Oral mucosaOral mucosa• TongueTongue• Floor of the mouthFloor of the mouth• Pharynx and tonsilsPharynx and tonsils

Straight elevatorsStraight elevators Straight elevatorStraight elevator
• Luxation of mandibular 3rd molars with Luxation of mandibular 3rd molars with distally curved roots.distally curved roots.
• Mesial application of force.Mesial application of force.• Principal of actionPrincipal of action
Simple lever actionSimple lever action Rotational movementRotational movement
Straight apexo.Straight apexo.

Straight elevatorsStraight elevators
STRAIGHT APEXO

Straight elevatorsStraight elevators
COUPLAND CHISEL

Straight elevatorsStraight elevators
Straight Hospital elevatorStraight Hospital elevator

Curved elevatorsCurved elevators Curved ApexoCurved Apexo
• Removal of single Removal of single rootsroots
• Removal of apical Removal of apical fragmentsfragments
Principal of Principal of actionaction• wedgingwedging

Cryer elevatorCryer elevator

Curved Hospital patternCurved Hospital pattern

CROSS BAR ElevatorsCROSS BAR Elevators
SOCKET APPLICATORSOCKET APPLICATOR

CROSS BARCROSS BAR
BUCCAL APPLICATORBUCCAL APPLICATOR

V. Debridement of the fieldV. Debridement of the field Removing of any loose fragments or Removing of any loose fragments or
pathological tissues from the socket pathological tissues from the socket using bone curettes.using bone curettes.
Trimming of sharp bony edges.Trimming of sharp bony edges. Smoothening of the edges by bone Smoothening of the edges by bone
file.file. Irrigation of the surgical field to Irrigation of the surgical field to
remove any fine debris.remove any fine debris.

V. Debridement of the fieldV. Debridement of the field

V. Debridement of the fieldV. Debridement of the field

VI. Closure (Suturing)VI. Closure (Suturing) Approximation of the soft tissue Approximation of the soft tissue
edges to cover the surgical fieldedges to cover the surgical field
Advantages of suturing:Advantages of suturing:• Promotes healingPromotes healing• Prevents complications Prevents complications
InfectionInfection Haemorrhage Haemorrhage Tissue necrosis Tissue necrosis
• Restores the normal contour and shape Restores the normal contour and shape of tissuesof tissues

VI. Closure (Suturing)VI. Closure (Suturing) Sutures can be classified according Sutures can be classified according
to:to: A. size: 3/8 to ½ circle cutting edge.A. size: 3/8 to ½ circle cutting edge.
B. Performance:B. Performance: Resorbable or Non-resorbable.Resorbable or Non-resorbable.
C. Physical configuration:C. Physical configuration: Monofilament or multifilament.Monofilament or multifilament.

VI. Closure (Suturing)VI. Closure (Suturing) Suturing armamentariumSuturing armamentarium
1.1. Suture needles.Suture needles.2.2. Suture materials.Suture materials.3.3. Needle holders.Needle holders.4.4. Toothed tissue forceps.Toothed tissue forceps.5.5. Suture scissors.Suture scissors.

Suture NeedlesSuture Needles Patterns of the Patterns of the
suture needle suture needle according to according to accessibility:accessibility:
• Straight suture needlesStraight suture needles For skin closureFor skin closure
• Curved suture needlesCurved suture needles For intraoral suturingFor intraoral suturing For deep suturingFor deep suturing
• Half circle suture Half circle suture needlesneedles
For intraoral suturingFor intraoral suturing For deep suturingFor deep suturing

Suture NeedlesSuture Needles Patterns of suture needles according Patterns of suture needles according
to cross section:to cross section:
• Round suture needlesRound suture needles Round cross sectionRound cross section May be straight, curved or half circleMay be straight, curved or half circle Suturing of fragile and delicate tissues e.g. oral Suturing of fragile and delicate tissues e.g. oral
mucosa and mucous membranesmucosa and mucous membranes
• Cutting (Atraumatic) suture needlesCutting (Atraumatic) suture needles Triangular cross sectionTriangular cross section May be straight, curved or half circleMay be straight, curved or half circle Suturing of dense tissues e.g. oral mucoperiosteumSuturing of dense tissues e.g. oral mucoperiosteum

Suture NeedlesSuture Needles Patterns of suture needles Patterns of suture needles
according to attachment:according to attachment:
Frech eyed.Frech eyed.
Swaged (eyeless).Swaged (eyeless).

Suture NeedlesSuture Needles

Suture MaterialsSuture Materials Types of suture materialTypes of suture material
• Non-Absorbable suture materialsNon-Absorbable suture materials Skin closureSkin closure Routine intraoral closureRoutine intraoral closure Blood vessels ligationBlood vessels ligation
• Absorbable suture materialAbsorbable suture material Deep tissuesDeep tissues Fascial layersFascial layers Intraoral closure in cases of:Intraoral closure in cases of:
• Inability of the patient to return to remove the Inability of the patient to return to remove the suturessutures
• Mentally retarded patientsMentally retarded patients• Epileptic patients Epileptic patients • Sutures under surgical stentsSutures under surgical stents

Suture MaterialsSuture Materials Non-Absorbable suture materialsNon-Absorbable suture materials
• SilkSilk Black or whiteBlack or white Tough suture materialTough suture material Intraoral suturingIntraoral suturing
• CottonCotton Weak suture materialWeak suture material
• NylonNylon• PolypropylenePolypropylene
Very hard suture materialVery hard suture material Used for skin closureUsed for skin closure Cause mucosal irritation if used intraorallyCause mucosal irritation if used intraorally

Suture MaterialsSuture Materials Absorbable suture materialsAbsorbable suture materials
• Plain catgutPlain catgut Resorbed 5-10 daysResorbed 5-10 days Used for suturing of deep fascia and musclesUsed for suturing of deep fascia and muscles Occasionally tissue irritantOccasionally tissue irritant
• Chromic catgutChromic catgut Resorbed completely after 10-15 daysResorbed completely after 10-15 days Non irritant to the tissuesNon irritant to the tissues Sutures of ligaments, tendons and severed blood Sutures of ligaments, tendons and severed blood
vesselsvessels• Collagen suturesCollagen sutures• Polyglycolic acids sutures (Dexon)Polyglycolic acids sutures (Dexon)• Polyglactin-910 (Vicryl) suturesPolyglactin-910 (Vicryl) sutures

Suture MaterialsSuture Materials
• Collagen suturesCollagen sutures More uniform physical propertiesMore uniform physical properties Prepared from tendons of cattlePrepared from tendons of cattle
• Polyglycolic acids sutures (Dexon)Polyglycolic acids sutures (Dexon) Synthetic polymerSynthetic polymer Resorped by hydrolysis within 15-30 daysResorped by hydrolysis within 15-30 days
• Polyglactin-910 (Vicryl) suturesPolyglactin-910 (Vicryl) sutures Synthetic inert copolymerSynthetic inert copolymer The strongest absorbable suture materialThe strongest absorbable suture material Resorped 60 – 90 days Resorped 60 – 90 days

Suture MaterialsSuture Materials

Suture MaterialsSuture Materials

Needle holderNeedle holder

Needle holderNeedle holder

Tissue forcepsTissue forceps Used to hold soft Used to hold soft
tissue & stabilize it tissue & stabilize it for suturing or for suturing or dissection.dissection.

Suture scissorsSuture scissors They have long They have long
handles & short handles & short cutting edges.cutting edges.

Suturing techniquesSuturing techniques Simple interrupted sutures.Simple interrupted sutures. Continuous sutures.Continuous sutures. Continuous with lock (blanket)sutuesContinuous with lock (blanket)sutues Horizontal mattres sutures.Horizontal mattres sutures. Vertical mattress sutures.Vertical mattress sutures. Figure-of- 8 sutures.Figure-of- 8 sutures.


Simple Interrupted SuturesSimple Interrupted Sutures

Continuous SuturesContinuous Sutures

Continuous with Lock SuturesContinuous with Lock Sutures

Horizontal Mattress SuturesHorizontal Mattress Sutures

Vertical Mattress SuturesVertical Mattress Sutures

Principles of suturingPrinciples of suturing Use suture needle of suitable shape and Use suture needle of suitable shape and
size.size.
Use suture material that is of suitable type Use suture material that is of suitable type and size for the tissues being sutured.and size for the tissues being sutured.
Good bite (2:3 mm from the free edge of Good bite (2:3 mm from the free edge of the soft tissue). the soft tissue).
Sutures should not be placed under Sutures should not be placed under tension to avoid strangulation of blood tension to avoid strangulation of blood vessels leading to ischemia & tissue vessels leading to ischemia & tissue necrosis.necrosis.

Principles of suturingPrinciples of suturing Knots should be tied 2-3mm away Knots should be tied 2-3mm away
from the incision line.from the incision line.
Suture material is cut 4-5 mm away Suture material is cut 4-5 mm away from the knot.from the knot.
Superficial sutures must be removed Superficial sutures must be removed 5 days after surgery to prevent 5 days after surgery to prevent infection / forigen body reaction.infection / forigen body reaction.

TONGUE HOLDERTONGUE HOLDER

ARTERY FORCEPSARTERY FORCEPS

ARTERY FORCEPSARTERY FORCEPS

ALLIS FORCEPSALLIS FORCEPS

KOCHERKOCHER

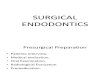
Extraction of Multi-Rooted Teethwith Destroyed Crown




Root Extraction After Removal of Part
of the Buccal Bone













THANK YouTHANK You for your attention for your attention