Embed Size (px)
Citation preview
DR. DAVIS KURIAN
TRACHEAL RESECTION
TRACHEAL LESIONS - ETIOLOGY
MC – post intubation injury (traumatic intubation – cricoid cartilage injury, subglottic injury, TE fistula).
Risk factors include – Prolonged hypotension Concurrent infections Prolonged intubation Persistently elevated cuff pressures
TRACHEAL LESIONS - ETIOLOGY
Second MC cause – tumours – squamous cell and adenoid cystic carcinomas.
Sq cell CA – discrete exophytic or ulcerating lesion.Adenoid cystic CA – slow growing – spreads either
locally (tracheal submucosa) or directly into the lung parenchyma or pleura.
Secondary tumours – thyroid (MC), esophagus, lung, breast, thymus, head and neck malignancies & lymphomas.
TRACHEAL LESIONS - ETIOLOGY
Other causes include Blunt injury – MC involves laryngotracheal junction Congenital causes – tracheal agenesis, congenital
stenosis, congenital chondromalacia. Infections – typhoid, diphtheria, syphilis, TB. Immunological – SLE, Wegener’s granulomatosis,
fibrosing mediastinitis, amyloidosis.
PREOP EVALUATION
Includes Detailed history Examination of the patient All routine blood investigations PFT – flow volume loops Radiological evaluation Diagnostic bronchoscopy
HISTORY AND PHYSICAL EXAMINATION
History of recent endotracheal intubation or tracheostomy.
Presence of coexisiting comorbidities – especially lung, CVS
Signs and symptoms of airway obstruction – dyspnea Wheeze Stridor (4mm or less narrowing) Persistent cough Hoarseness (involvement of recurrent laryngeal nerve & vocal
cords) Difficulty in clearing secretions Inabilility to tolerate supine position.
HISTORY AND PHYSICAL EXAMINATION
Mandatory to prove adequate laryngeal airway prior to tracheal resection and reconstruction.
Tracheal deviation or extra-thoracic compression – by palpation.
Stridor at rest/expiratory effort – elicited.Auscultation of the upper airway.Range of neck movements (should tolerate hyper
flexion and hyperextension comfortably) & C Spine stability.
Tracheostomy – should be examined for the patency of the tube and tracheal stoma.
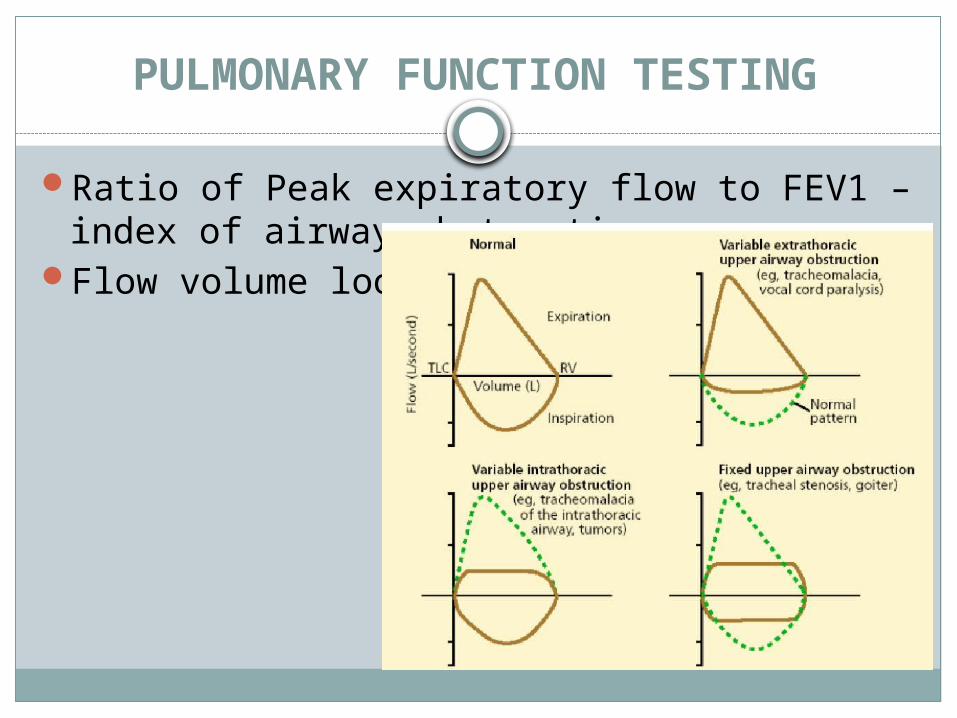
PULMONARY FUNCTION TESTING
Ratio of Peak expiratory flow to FEV1 – index of airway obstruction.
Flow volume loops
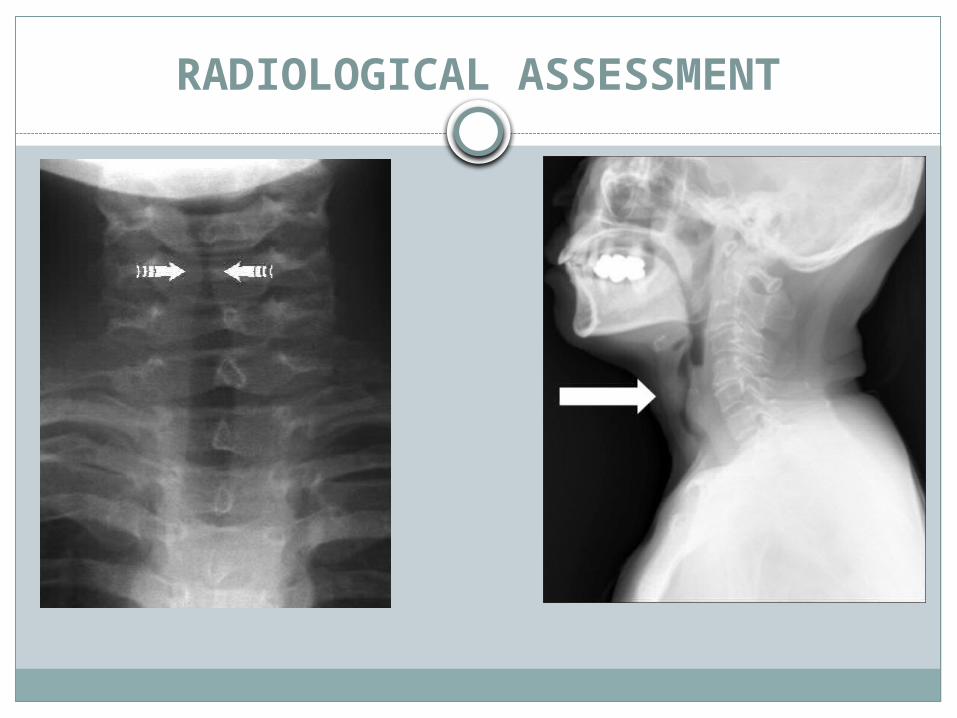
RADIOLOGICAL ASSESSMENT
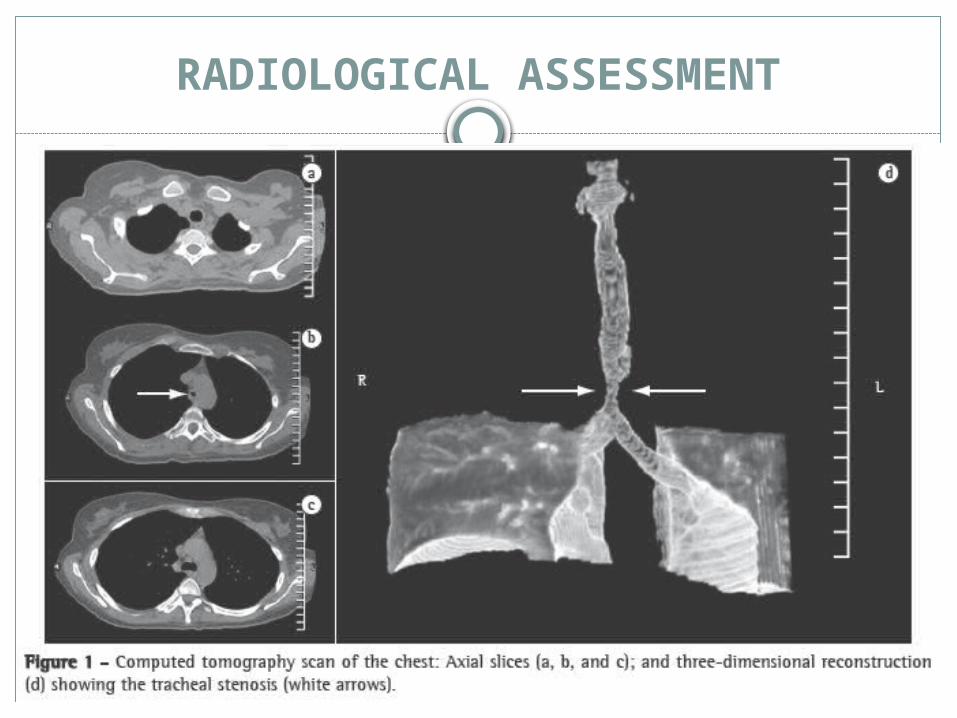
RADIOLOGICAL ASSESSMENT
RADIOLOGICAL ASSESSMENT
Fluoroscopic studies to demonstrate vocal cord movement, tracheomalacia.
CTMRI
Other investigations: Vocal cord mobility – by Laryngoscopy
ANAESTHETIC MANAGEMENT
Primary goal - to maintain the adequate airway – maintenance of ventilation and oxygenation and easy clearance of blood and secretions.
Intubation is mandatory.Airway management – challenging – reasons:
Distal airways become obstructed with blood or secretions
Rarely distal trachea may withdraw into the mediastinum.
Postoperative period – patient’s hyper flexed position or edema at the anastomotic site.
PREMEDICATION
Patients with significant tracheal narrowing – shouldn't receive premedication unless they are in the hands of a person skilled in airway management.
Over sedation and CNS depression should be avoided.
BZD – sedative and anxiolytic properties.Antisialagogues – atropine etc. can be
disastrous in patients with tracheal stenosis- tenacious secretions.
EQUIPMENT
Anaesthesia machine with high flow oxygenIndividualized masks and oral airwaysMask strapsLong bronchial sprayer with topical lidocaineEndotracheal tubesSterile tubings and connect0rsSingle leumen endobronchial tubesHigh frequency jet ventilatorJet cathetersVentilator capable of respiratory rate adjustments,
variable I:E ratio and pressure settings
MONITORING
ECGNIBPEsophageal stethoscope – breath sounds and
heart sounds.Pulse oximetryetCO2Left radial arterial catheter – for ABG and ABPCentral venous pressure – depending on the
patient’s cardiac history – best by antecubital approach or femoral vein.
INDUCTION & BRONCHOSCOPIC EXAMINATION
Patient with extrinsic compression of trachea or critical airway lesion – prefer to sit upright.
If supine – deflated thyroid bag under the shoulder to gain access.
All pressure points must be padded.Minor degree of airway obstruction – induced
with propofol or thiopentone.Significant airway obstruction – volatile
agents preferred for induction.
INDUCTION & BRONCHOSCOPIC EXAMINATION
Muscle relaxants must be avoided before securing the airway.
After adequate anaesthesia – DL scopy – topical anaesthesia to oropharynx and glottis – face mask reapplied – volatile agent+O2 continued – deepen the plane – DL scopy – topical anaesthesia below the vocal cord – bronchoscopy.
INDUCTION & BRONCHOSCOPIC EXAMINATION
Rigid bronchoscopy – To visualize the nature and extent of lesion Potential difficulty in ET tube placement Opportunity for tracheal dilation to provide airway of
adequate size – serial dilation with rigid pediatric bronchoscopes.
Tumor handling and dilation must be done with care – Dislodgement can cause further airway obstruction Bleeding can further compromise the airway.
INDUCTION & BRONCHOSCOPIC EXAMINATION
At the end of bronchoscopy – intubated with appropriate sized ET tube – generally in a sniffing position using DL scopy.
Tube position confirmed by chest movements, auscultation, etCO2 monitoring, FOB.
Tube secured, eyes protected, esophageal stethoscope positioned.
Orogastric tube – to empty the stomach of gas and fluid – orogastric tube is removed.
POSITIONING
Extra-thoracic and cervical tracheal lesions – anterior collar incision.
Positioned supine with inflated thyroid bag under the shoulder and head supported with head ring.
Back of the operating room table elevated to 10-15 degree to position the cervical and sternal areas parallel to the floor when the head is extended fully.
Arms tucked/left arm extended on arm board at 45 degree angle to the trunk.
POSITIONING
Lesions of distal trachea – explored through – right posterolateral thoracotomy in the fourth interspace or the bed of 4th rib.
Patient in left lateral decubitus position.Right arm – drapped and prepped into the
surgical field – for the surgeon to manipulate the arm to gain access to the neck.
CERVICAL TRACHEAL RECONSTRUCTION
Low cervical collar incision.Anterior dissection of trachea – careful dissection
around innominate artery and structures around the trachea.
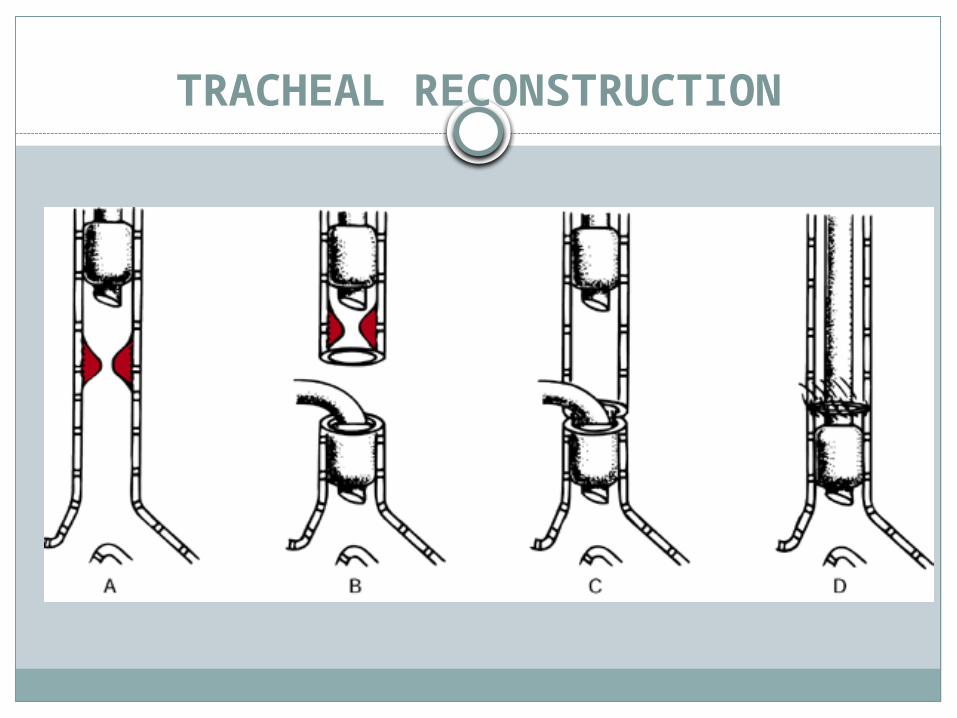
Anaesthesia maintained by oral ET tube – prior to tracheal division N2O eliminated from the gas mixture – maintained by O2+inhalational agent – surgical tape around the trachea below the lesion – ET tube cuff deflated prior placement of lateral sutures – trachea resected – distal part intubated across the field using flexible, sterile, reinforced tube – connected to circuit.
CERVICAL TRACHEAL RECONSTRUCTION
After resection – two free ends of trachea are anastomosed by traction sutures – patient’s neck flexed from above – once all the sutures have been put – reinforced tube is removed – the tube in the proximal trachea is readvanced into the distal trachea under supervision.
Prior to the final airway exchange – airway is suctioned of blood and secretions.
Anastomotic site is checked for leaks with sustained positive pressure breath 30 mm Hg.
Patient’s head is flexed and supported.
TRACHEAL RECONSTRUCTION
CERVICAL TRACHEAL RECONSTRUCTION
At the end – patient must be breathing spontaneously – awake extubation – head should be supported in a hyperflexed position to avoid undue traction at anastomotic site.
Equipments for re-intubation must be kept ready including a FOB.
Upper airway edema – MCC of respiratory distress in the immediate post operative period.
Patient must be transported with supplemental oxygen.
DISTAL TRACHEA AND CARINA RECONSTRUCTION
Preferred approach is right posterolateral thoracotomy.
General principles are the same for cervical tracheal reconstruction.
Thoracic epidural before induction of anaesthesia – then patient in left lateral position.
Positive pressure ventilation and ms relaxants of intermediate duration of action – with appropriate monitoring.
Ms relaxants must be promptly reversed at the end of the procedure.
DISTAL TRACHEA AND CARINA RECONSTRUCTION
Initial resection – performed with the tube proximal to the airway lesion – once trachea divided – too short to hold an ET tube – Left mainstem bronchus intubated from the operative field and one lung ventilation is employed.
Second endobronchial tube introduced into right mainstem bronchus and CPAP or HFPPV via jet ventilator.
SPO2 monitored with a pulse oximeter.HFPPV may also be used for left lung
ventilation.
DISTAL TRACHEA AND CARINA RECONSTRUCTION
End of procedure – ET tube is withdrawn into proximal trachea – ventilation proceeds through area of anastomosis – position of tube confirmed by FOB.
Routinely right mainstem bronchus is anastomosed to distal trachea.
Left mainstem bronchus is re-implanted in an end to side anastomosis to the bronchus intermedius or distal trachea.
Extubated similar to cervical approach and transported.
DISTAL TRACHEA AND CARINA RECONSTRUCTION
Most widely employed method – O2+/-N2O with volatile anasthetic.
Inhalational agents – bronchodilators.Isoflurane and sevoflurane – pleasant
induction, less arrythmogenic and less hepatotoxicity compared with halothane (less pungent than both iso and sevo).
POSTOPERATIVE CARE
ICU admissionChest XRay – to r/o pneumothoraxO2 via high flow, humidified system via face mask –
adequate oxygenation as well as thinning of secretions.
Head kept in a flexed position.Chest physiotherapy.Blind nasotracheal suction done with caution in
patient with inadequate cough reflex – take care not to cause perforation at the anastomotic site, airway edema, vomiting and aspiration.
Flexible FOB guided pulmonary toilet to clear off secretions.
POSTOPERATIVE CARE
Equipments for reintubation must be kept ready.
Laryngeal edema – another important complication can present as stridor or hoarseness – management includes placing the patient in a sitting position to promote venous drainage, controlled fluid administration and nebulisation with mixture of adrenaline and saline, IV steroids.
Pain contol – IV, epidural, intrapleural analgesia, intercostal blocks or PCA.