Embed Size (px)
Citation preview

ANS
Planos Acessiacuteveis
(Etapa Participaccedilatildeo Social) 29 de junho de 2017
Ligia Bahia
Roteiro
bullBreve Histoacuterico
bullOrigem da Proposta Atual
bullDefiniccedilatildeo de Acessiacutevel (preccedilo)
bullO Grupo de Trabalho do MS
bullParticipantes
bullO Grupo de Trabalho do MS
bullProposiccedilotildees
bullProacuteximos Passos
Preacute-1998
ausecircncia de regulamentaccedilatildeo
Planos com segmentaccedilatildeo
assistencial limites de internaccedilatildeo
exclusatildeo de doentes e de
procedimentosldquomoacutedulosrdquo opcionais (onco diaacutelise cardio etc)
Lei 965698 MUITAS LACUNAS
mas cobertura miacutenima obrigatoacuteria
Rol de Procedimentos e Eventos em Sauacutede
Mobilizaccedilatildeo ndash 19931998
Pela regulamentaccedilatildeo
EFEITOS denuacutencias desembolso das
famiacutelias desassistecircncia ldquoestouravardquo no
prestador
Breve Histoacuterico
2001 MP 217743(FHCSerra)
Planos com segmentaccedilotildees subsegmentaccedilotildees e exigecircncias miacutenimas diferenciadas
ldquoplano de rederdquo e ldquoplano de acessordquo
Cobertura condicionada a serviccedilos na aacuterea de abrangecircncia
Breve Histoacuterico
SimpoacutesioRegulamentaccedilatildeo dos Planos de Sauacutede 28
e 29 de agosto de 2001 Auditoacuterio
Petrocircnio Portella ndash Senado
CPI dos Planos de Sauacutede (2003)
Breve Histoacuterico
2013 pacote de estiacutemulos ao setor
(Dilma)
Planos ldquopopularesrsquo
com subsiacutedio puacuteblico
Reduccedilatildeo de impostos e
tributos
Financiamento puacuteblico
para ampliaccedilatildeo da rede
credenciada
Antecedentes da Proposta Atual
2015 PEC 451(Dep Eduardo Cunha)
Plano obrigatoacuterio para todos os empregados
Antecedentes da Proposta Atual
6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Roteiro
bullBreve Histoacuterico
bullOrigem da Proposta Atual
bullDefiniccedilatildeo de Acessiacutevel (preccedilo)
bullO Grupo de Trabalho do MS
bullParticipantes
bullO Grupo de Trabalho do MS
bullProposiccedilotildees
bullProacuteximos Passos
Preacute-1998
ausecircncia de regulamentaccedilatildeo
Planos com segmentaccedilatildeo
assistencial limites de internaccedilatildeo
exclusatildeo de doentes e de
procedimentosldquomoacutedulosrdquo opcionais (onco diaacutelise cardio etc)
Lei 965698 MUITAS LACUNAS
mas cobertura miacutenima obrigatoacuteria
Rol de Procedimentos e Eventos em Sauacutede
Mobilizaccedilatildeo ndash 19931998
Pela regulamentaccedilatildeo
EFEITOS denuacutencias desembolso das
famiacutelias desassistecircncia ldquoestouravardquo no
prestador
Breve Histoacuterico
2001 MP 217743(FHCSerra)
Planos com segmentaccedilotildees subsegmentaccedilotildees e exigecircncias miacutenimas diferenciadas
ldquoplano de rederdquo e ldquoplano de acessordquo
Cobertura condicionada a serviccedilos na aacuterea de abrangecircncia
Breve Histoacuterico
SimpoacutesioRegulamentaccedilatildeo dos Planos de Sauacutede 28
e 29 de agosto de 2001 Auditoacuterio
Petrocircnio Portella ndash Senado
CPI dos Planos de Sauacutede (2003)
Breve Histoacuterico
2013 pacote de estiacutemulos ao setor
(Dilma)
Planos ldquopopularesrsquo
com subsiacutedio puacuteblico
Reduccedilatildeo de impostos e
tributos
Financiamento puacuteblico
para ampliaccedilatildeo da rede
credenciada
Antecedentes da Proposta Atual
2015 PEC 451(Dep Eduardo Cunha)
Plano obrigatoacuterio para todos os empregados
Antecedentes da Proposta Atual
6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Preacute-1998
ausecircncia de regulamentaccedilatildeo
Planos com segmentaccedilatildeo
assistencial limites de internaccedilatildeo
exclusatildeo de doentes e de
procedimentosldquomoacutedulosrdquo opcionais (onco diaacutelise cardio etc)
Lei 965698 MUITAS LACUNAS
mas cobertura miacutenima obrigatoacuteria
Rol de Procedimentos e Eventos em Sauacutede
Mobilizaccedilatildeo ndash 19931998
Pela regulamentaccedilatildeo
EFEITOS denuacutencias desembolso das
famiacutelias desassistecircncia ldquoestouravardquo no
prestador
Breve Histoacuterico
2001 MP 217743(FHCSerra)
Planos com segmentaccedilotildees subsegmentaccedilotildees e exigecircncias miacutenimas diferenciadas
ldquoplano de rederdquo e ldquoplano de acessordquo
Cobertura condicionada a serviccedilos na aacuterea de abrangecircncia
Breve Histoacuterico
SimpoacutesioRegulamentaccedilatildeo dos Planos de Sauacutede 28
e 29 de agosto de 2001 Auditoacuterio
Petrocircnio Portella ndash Senado
CPI dos Planos de Sauacutede (2003)
Breve Histoacuterico
2013 pacote de estiacutemulos ao setor
(Dilma)
Planos ldquopopularesrsquo
com subsiacutedio puacuteblico
Reduccedilatildeo de impostos e
tributos
Financiamento puacuteblico
para ampliaccedilatildeo da rede
credenciada
Antecedentes da Proposta Atual
2015 PEC 451(Dep Eduardo Cunha)
Plano obrigatoacuterio para todos os empregados
Antecedentes da Proposta Atual
6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

2001 MP 217743(FHCSerra)
Planos com segmentaccedilotildees subsegmentaccedilotildees e exigecircncias miacutenimas diferenciadas
ldquoplano de rederdquo e ldquoplano de acessordquo
Cobertura condicionada a serviccedilos na aacuterea de abrangecircncia
Breve Histoacuterico
SimpoacutesioRegulamentaccedilatildeo dos Planos de Sauacutede 28
e 29 de agosto de 2001 Auditoacuterio
Petrocircnio Portella ndash Senado
CPI dos Planos de Sauacutede (2003)
Breve Histoacuterico
2013 pacote de estiacutemulos ao setor
(Dilma)
Planos ldquopopularesrsquo
com subsiacutedio puacuteblico
Reduccedilatildeo de impostos e
tributos
Financiamento puacuteblico
para ampliaccedilatildeo da rede
credenciada
Antecedentes da Proposta Atual
2015 PEC 451(Dep Eduardo Cunha)
Plano obrigatoacuterio para todos os empregados
Antecedentes da Proposta Atual
6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

CPI dos Planos de Sauacutede (2003)
Breve Histoacuterico
2013 pacote de estiacutemulos ao setor
(Dilma)
Planos ldquopopularesrsquo
com subsiacutedio puacuteblico
Reduccedilatildeo de impostos e
tributos
Financiamento puacuteblico
para ampliaccedilatildeo da rede
credenciada
Antecedentes da Proposta Atual
2015 PEC 451(Dep Eduardo Cunha)
Plano obrigatoacuterio para todos os empregados
Antecedentes da Proposta Atual
6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

2013 pacote de estiacutemulos ao setor
(Dilma)
Planos ldquopopularesrsquo
com subsiacutedio puacuteblico
Reduccedilatildeo de impostos e
tributos
Financiamento puacuteblico
para ampliaccedilatildeo da rede
credenciada
Antecedentes da Proposta Atual
2015 PEC 451(Dep Eduardo Cunha)
Plano obrigatoacuterio para todos os empregados
Antecedentes da Proposta Atual
6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

2015 PEC 451(Dep Eduardo Cunha)
Plano obrigatoacuterio para todos os empregados
Antecedentes da Proposta Atual
6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

6 de julho de 2016
8 de marccedilo de 2017
24032017
Portaria nordm 8851
Grupo Interno da ANS para avaliar
proposta
04082016
Portaria nordm 1482
MS cria GT dos Planos Acessiacuteveis
Origem da Atual Proposta
Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Criacuteticas
Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Fonte IBGE 2015 Pesquisa Nacional de Sauacutede Elaboraccedilatildeo proacutepria (Bahia L Scheffer M)
Os planos atuais satildeo caros
38
196
134
141
102
47
Proporccedilatildeo de Titulares de Planos Privados por Faixa de Valor da Mensalidade Brasil 2013
lt R$ 10000
gt R$ 10000 lt R$ 20000
gt R$ 20000 lt R$ 30000
gt R$ 30000 lt R$ 50000
gt R$50000 lt R$ 100000
gt R$ 100000
Em 2013
Aproximadamente 60 eram
mensalidades para os clientes de
MENOS que R$ 20000
Aproximadamente 30 custavam
MAIS que R$ 30000
Ano IPCA Reajuste ANS
2013 591 9042014 641 965
2015 1067 1355
Mesmo com reajustes natildeo haveria mudanccedilas
significativas entre as faixas de preccedilos
Acessiacutevel=Menor Preccedilo
20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

20000valor meacutedio do plano familiar
Ateacute R$ 5000
+ de R$ 50 a R$ 10000
+ de R$ 100 a R$ 20000
+ de R$ 200 a R$ 30000
+ de R$ 30000
Natildeo paga nada (dependente)
Natildeo sabe
18
11
20
10
24
6
10
Fonte P15 (PARA TODOS) Vocecirc possui algum plano ou seguro sauacutede atualmente seja como titular ou dependente Veja que eu estou
perguntando sobre plano de sauacutede de empresas particulares e natildeo do SUS ou de atendimento puacuteblico municipal ou estadual gratuito (SE
SIM) Como titular ou dependente - Base Total da amostra
Fonte Pesquisa DatafolhaInterfarma - 2014
Os planos atuais satildeo caros Acessiacutevel=Menor Preccedilo
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo
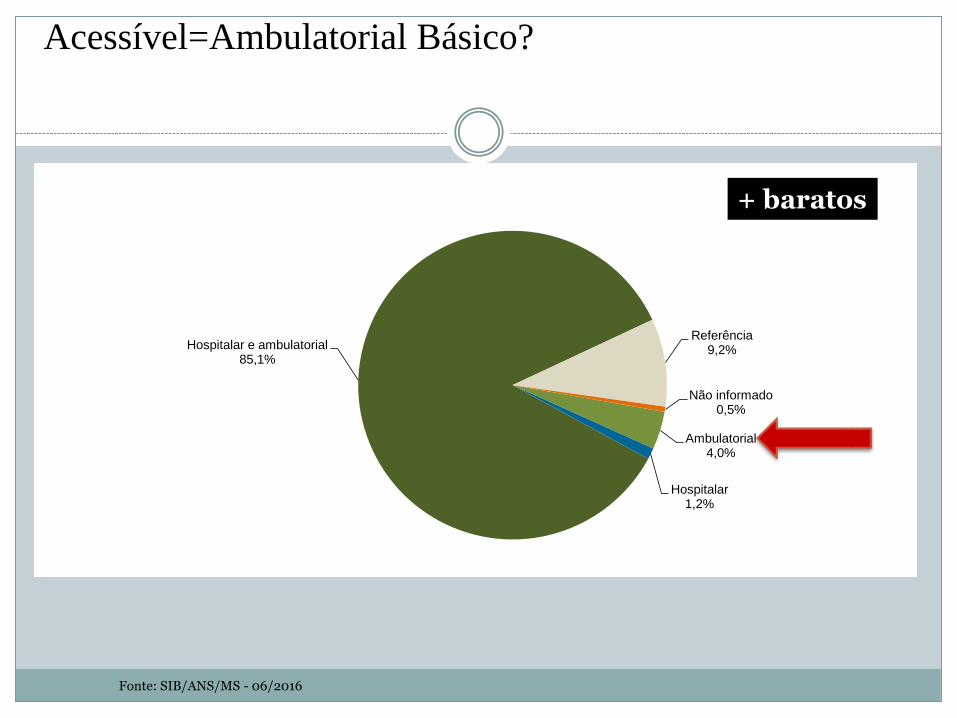
Fonte SIBANSMS - 062016
Ambulatorial40
Hospitalar12
Hospitalar e ambulatorial851
Referecircncia92
Natildeo informado05
Acessiacutevel=Ambulatorial Baacutesico
+ baratos
Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Os ldquopejotinhasrdquoAcessiacuteveis = IndividualColetivo
Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Acessiacuteveis = IndividualColetivo
Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Acessivel=Poacutes Pagamento
previstos desde 1998 (Artigos 2ordm e 3ordm da Resoluccedilatildeo CONSU 08)33 dos planos jaacute praticam (Fonte ANS)Sem regras Sem limite de percentuais e procedimentosem debate desde 2010
O QUE PROPOtildeE A ANS
Percentual maacuteximo (40)
Natildeo cobranccedila em alguns procedimentos preventivos
Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Cliacutenicas populares ndash Poacutes Pagamento (natildeo satildeo planos)
Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Decisotildees judiciais contra planos de sauacutede jaacute superam decisotildees contra o SUS ( Segunda Instacircncia ndash TJSP)
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
SUS em SP atende toda a populaccedilatildeo Planos
atendem 40 Extensatildeo de cobertura SUS eacute
maior (medicamentos alta complexidade )
Accedilotildees - Planos de Sauacutede Accedilotildees - SUS
2016 11406 10152
2015 11476 7355
2014 9499 6325
2013 9935 6354
2012 11405 6955
2011 4819 7683
Total 63238 49959
Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Cresce nuacutemero de Accedilotildees Judiciais contra Planos de Sauacutede -SP
Fonte TJSP Observatoacuterio da Judicializaccedilatildeo da Sauacutede Suplementar (DMPFMUSP)
Primeiros cinco meses
(0101 a 3105)
Primeira instacircncia (N) Segunda Instacircncia (N)
2011 821 1768
2012 1246 3583
2013 2995 3881
2014 5948 3902
2015 6775 4692
2016 6885 4870
2017 7015 4698
Em 2017 mais de 110 decisotildees por dia uacutetil
Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Integrantes do Grupo de Trabalho do MS
Participantes
Fenasauacutede
Abramge
ANAB
Unimed Brasil
CBM
MS
Proteste
ANAHP
Associaccedilatildeo Emergecircncias
SINOG
Entre outros
Natildeo Participantes
AMB
APM
IDEC
Entre outros
Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Proposiccedilotildees
CMB
Unimed
Abramge
1 Plano ambulatorial (meacutedicos
generalistas sem emergecircncia sem
urgecircncia (exames RX ECG
Ultrassografia e Mamografia)
2 Plano Regionalizado
Acesso de acordo com a oferta local
3 Plano Poacutes-Pagamento
Ambulatorial e Preacute-Pagamento
(hospitalar)
Tabela remuneraccedilatildeo menor
Sem urgecircnciaemergencia
Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Proposiccedilotildees
Fenasauacutede
Incluir o plano acessiacutevel na lei
9656
Franquias Co-Participaccedilatildeo
Protocolos
Segunda Opiniatildeo
Plano Regionalizado
Prazos de Atendimento Dilatados
Pondera que o plano
simplificado eacute
comercialmente
inviaacutevel e passiacutevel de
judicializaccedilatildeo
ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

ANAB
Planos Acessiacuteveis apenas para os contratos
coletivos contra comercializaccedilatildeo para contratos
individuais
Diferenccedila de preccedilo entre a primeira faixa
etaacuteria e a uacuteltima 10 vezes
Proposiccedilotildees
Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Proposiccedilotildees (documentos)
Conjur
Recomendaccedilotildees Cautela
Recomendaccedilotildees Ampliaccedilatildeo do Grupo de Trabalho
(inclusatildeo consumidores sanitaristas juristas etc)
APM Contra
Proteste Contra
ANAPH Preocupaccedilatildeo com a Qualidade da
Atenccedilatildeo
Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Proacuteximos Passos
Analise do Material Disponiacutevel
Anaacutelise dos PLacutes Congresso Nacional
Acompanhamento Comissatildeo Especial
E a ANS
Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo

Cochrane Database Syst Rev 2015 May 8(5)CD007017 doi 10100214651858CD007017pub2
Pharmaceutical policies effects of cap and co-payment on rational use of medicines
Luiza VL1 Chaves LA Silva RM Emmerick IC Chaves GC Fonseca de Arauacutejo SC Moraes EL Oxman AD
MAIN RESULTS
We included 32 full-text articles (17 new) reporting evaluations of 39 different interventions (one study -
Newhouse 1993 - comprises five papers) We excluded from this update eight controlled before-after
studies included in the previous version of this review because they included only one site in their
intervention or control groups Five papers evaluated caps and six evaluated a cap with co-insurance and
a ceiling Six evaluated fixed co-payment two evaluated tiered fixed co-payment 10 evaluated a ceiling
with fixed co-payment and 10 evaluated a ceiling with co-insurance Only one evaluation was a
randomised trial The certainty of the evidence was found to be generally low to very low Increasing
the amount of money that people pay for medicines may reduce insurers medicine expenditures and
may reduce patients medicine use This may include reductions in the use of life-sustaining
medicines as well as medicines that are important in treating chronic conditions and medicines for
asymptomatic conditions These types of interventions may lead to small decreases in or uncertain
effects on healthcare utilisation We found no studies that reliably reported the effects of these types of
interventions on health outcomes
AUTHORS CONCLUSIONS
The diversity of interventions and outcomes addressed across studies and differences in settings
populations and comparisons made it difficult to summarise results across studies Cap and co-
payment polices may reduce the use of medicines and reduce medicine expenditures for health
insurers However they may also reduce the use of life-sustaining medicines or medicines that are
important in treating chronic including symptomatic conditions and consequently could increase
the use of healthcare services Fixed co-payment with a ceiling and tiered fixed co-payment may be less
likely to reduce the use of essential medicines or to increase the use of healthcare services
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo
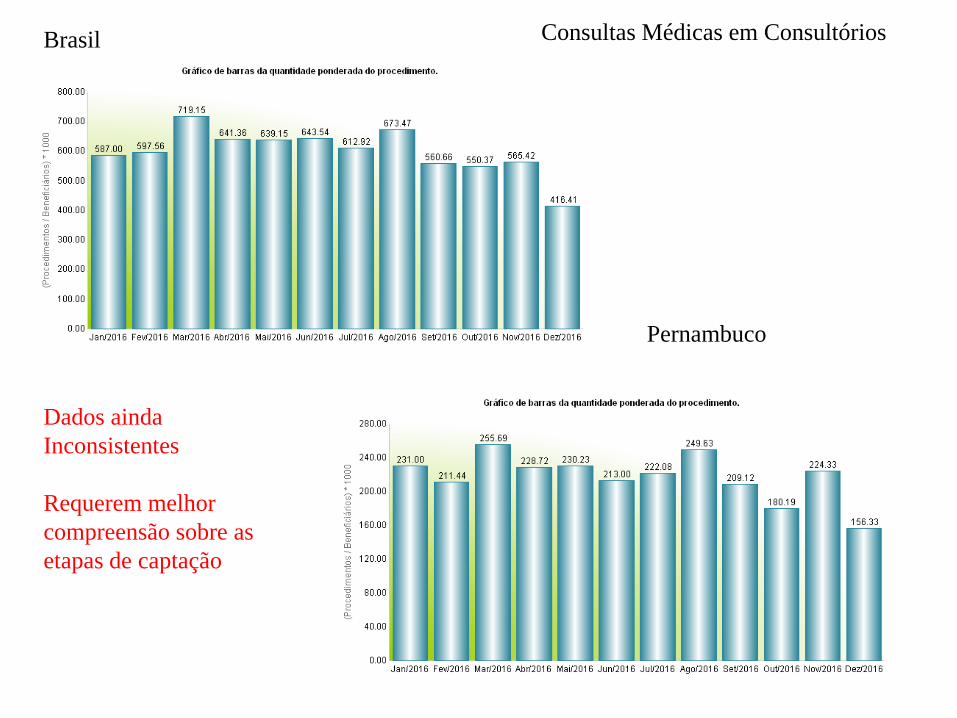
Brasil
Pernambuco
Consultas Meacutedicas em Consultoacuterios
Dados ainda
Inconsistentes
Requerem melhor
compreensatildeo sobre as
etapas de captaccedilatildeo





























