Embed Size (px)
Citation preview

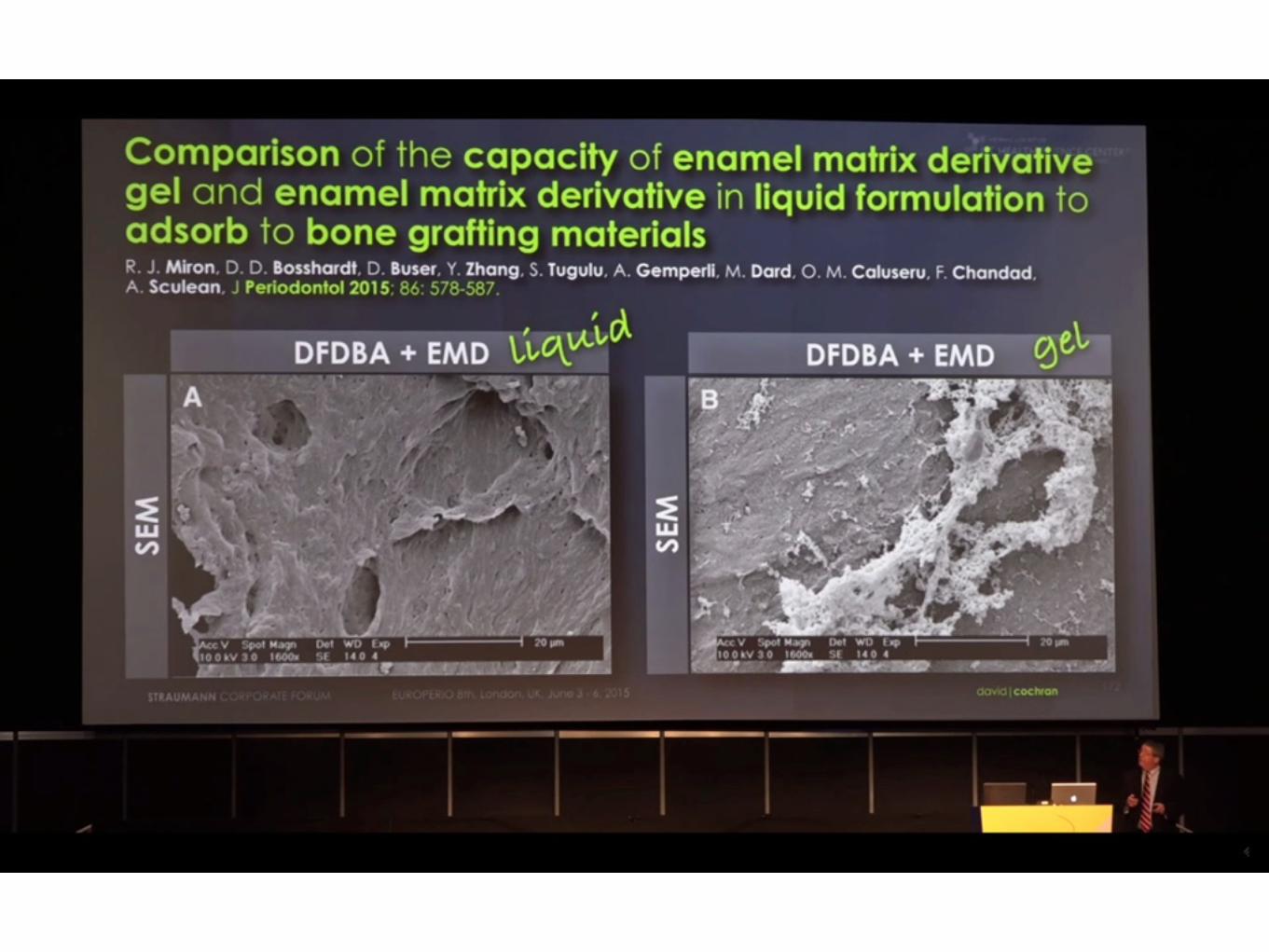
Comparison of the Capacity of Enamel Matrix Derivative Gel and Enamel
Matrix Derivative in Liquid Formulation to Adsorb to Bone Grafting Materials Richard J. Miron, Dieter D. Bosshardt, Daniel Buser, Yufeng Zhang, Stefano Tugulu, Anja Gemperli, Michel Dard, Oana M. Caluseru, Fatiha
Chandad, and Anton Sculean
担当:篠田純


INTRODUCTION• 過去20年間、歯周病学と口腔外科の分野で著しい革新がもたらされた。
• 骨欠損の治療に対する骨移植材と人工骨の使用もそれにあたる。
• 口腔外科において骨欠損の充填、骨増大、骨修復、再生膜の機械的支持、血餅の安定化のために、通常骨移植材が用いられる。
• 自家骨移植は未だ骨移植術のgold standardであるが、ドナーサイトの侵襲や手術時間・コストなど自家骨の欠点や制限を回避するため、他家骨移植(ヒトドナーのフリーズドライ)、異種移植(動物、植物)、無生物材料移植(ハイドロキシアパタイト、β-TCP、リン酸カルシウム、ポリマー、生体活性ガラスのような人工的に合成されたもの)を含む多くの代替材料が、広範囲に渡り研究されている。

INTRODUCTION• 血小板由来成長因子、骨形成タンパクなどの成長因子の併用は、自家骨採取を避けつつ臨床的成功を得るために行われてきた。
• ブタ歯胚から抽出したenamel matrix derivative (EMD) は、歯周外科分野において重要である。
• EMDは当初、歯根膜とセメント質の再生のために開発され、骨縁下欠損、歯肉退縮、分岐部欠損など様々な歯周外科において用いられてきた。

INTRODUCTION• 歯周組織再生を誘導する能力に加え、EMDは骨形成と創傷治癒を促進することがわかっている。
• 市場で入手可能な多くの異なった骨移植材と骨形成促進材を用いて、どの材料の組み合わせがより予知性を高めるのかが研究されてきた。
• 過去10年間、EMDと様々な移植材の組み合わせが様々な結果を生み出した。
• 多くの臨床研究、動物実験が併用法の利点を明らかにしているが、そのような結果が得られなかった研究もある。

INTRODUCTION• 最近著者らの研究室において、液状のEMD (EMD liquid) と EMD gel が様々な移植材との併用で骨芽細胞と歯根膜細胞の増殖と分化に影響を与える能力を試験した。
• これらの in vitro 研究は様々な骨移植材がEMDと併用された時に、細胞の付着、増殖と分化における多様性を示した。
• 生体材料の表面に対するタンパク質の吸着はその後の細胞の反応に影響する主要な要因であるため、EMD liquid と EMD gel が骨移植材に塗布後細胞の反応において様々な影響を引き起こすという所見から、移植材の表面へのEMDの吸着にも大きな幅があるという仮説が導き出される。
INTRODUCTION• それゆえ、今回の研究の目的は EMD liquid と EMD gel の下記の3種類の骨移植材に対する吸着の影響を調べることである。1) ウシ由来の天然骨無機成分 (NBM) ; 2) DFDBA; 3) リン酸カルシウム (CaP)
• EMDタンパクの骨移植材顆粒表面に吸着する能力は、EMD抗体を用いた高解像度免疫染色と同様に、弱拡大、強拡大の走査電子顕微鏡によっても調査された。
• それぞれの移植材の表面に吸着されたアメロジェニンタンパクの総量を定量するために、ELISA法を用いてさらなる実験が行われた。
• さらに、エナメルマトリックスタンパクが周囲に放出される割合を測定するため、8時間後、1、3、5、10日後のアメロジェニンタンパクの放出動態が定量された。
MATERIALS AND METHODS
MATERIALS AND METHODS
Coating of Grafting Materials With EMD Liquid and EMD Gel
• NBM, DFDBA, CaP の3種類の骨移植材が実験に用いられた。
• 30mg EMD を 0.1%酢酸溶液3mlに溶解させた。
• さらに100 mg/mLの作業溶液を作るため、4℃でEMD溶液を0.1M炭酸緩衝液を用いて100倍に希釈した。
• EMD liquid 群作成のため、1mlのEMD溶液を24-well培養皿上の100mgの移植材に注ぎ、4℃で一晩放置した。
• EMD gel 群は100 mg/mL の濃度に希釈、骨移植材にコーティングするため4℃で一晩放置された。
MATERIALS AND METHODSSEM
• コントロールのEMDコーティングされていない CaP, DFDBA, NBM 顆粒とEMD liquid と EMD gel でコーティングした移植材はSEMのために1%グルタールアルデヒドと1%フォルムアルデヒドで固定された。
• エタノールによる脱水の後、試料を臨界点乾燥した。
• 翌日、試料を10nmの金でコーティングしてSEMで表面のタンパクの吸着を分析した。

MATERIALS AND METHODSHistologic Processing for Transmission Electron Microscopy (TEM/透過電子顕微鏡)
• EMD liquid と EMD gel が CaP, DFDBA, NBM 顆粒に浸透し吸着する能力を検査するため、試料は0.08Mカコジル酸ナトリウム緩衝液 (pH 7.4) で処理された1%グルタールアルデヒドと1%ホルムアルデヒド溶液で固定された。
• 4℃で4.13% 二ナトリウム EDTA により脱灰された後、試料は 5% ショ糖を含む 0.1 M カコジル酸ナトリウム緩衝液 (pH 7.3) により洗浄され、樹脂包埋された。

MATERIALS AND METHODSHistologic Processing for Transmission Electron Microscopy (TEM)
• 樹脂包埋試料はガラスナイフとダイヤモンドナイフを用いてミクロトームで「Semi-thin」に切りだされた。

MATERIALS AND METHODS
Histologic Processing for Transmission Electron Microscopy (TEM)
• EMD liquid/EMD gel の免疫化学的確認には、高解像度 protein A‒gold technique※ が用いられた。
• ※金の粒子を結合したタンパク質と抗体との特異的結合を利用し、電子顕微鏡下で抗原タンパク質の存在部位を観察する実験手法。

MATERIALS AND METHODSHistologic Processing for Transmission Electron Microscopy (TEM)
• 樹脂包埋試料の薄切 (80 to 100 nm) はダイヤモンドナイフで行われ、熱可塑性レジンコーティング、カーボンコーティングのニッケルグリッド上に載せ、1% 卵白アルブミンを含む 0.01 M リン酸塩緩衝生理食塩水 (PBS) (pH 7.3) 上に浮かべた。
• 切片はPBSで希釈し親和性精製されたウサギ抗EMDポリクローナル抗体上に移され、1時間放置された。

MATERIALS AND METHODSHistologic Processing for Transmission Electron Microscopy (TEM)
• 1次抗体による処理の後、グリッドをPBSで洗浄し、PBSと1% 卵白アルブミン上に10分間浮遊させ、10-14nmの金粉の入ったprotein A‒gold complexで30分間処理した。
• ネガティブ・コントロールとして、切片はprotein A‒goldのみ、または関係のない抗IgG抗体により処理した。
• 未成熟ヒトおよびブタエナメルマトリクスをポジティブ・コントロールとして用いた。

MATERIALS AND METHODSHistologic Processing for Transmission Electron Microscopy (TEM)
• その後、グリッドをPBSと蒸留水で洗浄し、酢酸ウラニルとクエン酸鉛で染色し、加速電圧60 kVのTEMで観察した。
• データの記録には顕微鏡に接続したデジタルカメラを用いた。
• 試料の定量化のため、イメージング・ソフトウェアを用いてそれぞれの試料の10枚の画像からgold labelingを測定し平均値を算出した。
• gold labelingから移植材の表面までの距離もそれぞれの試料について10枚の画像から定量した。

MATERIALS AND METHODSELISA Protein Quantification of EMD Liquid/EMD Gel Adsorption to Grafting Material
• CaP, DFDBA, NBM骨移植材の表面へ吸着したEMD liquidまたはEMD gelの定量化のため、ELISA定量分析を用いて2つ目の試験を行った。
• 簡単に言うと、コーティングの後、吸着しなかったエナメルマトリックスタンパクを含む残留PBS溶液を集め、ELISAを用いて移植材に吸着しなかったアメロジェニンタンパクを定量した。
• タンパクの総量から吸着しなかったタンパクの量を引くことにより、それぞれの移植材表面に吸着した量を求めた。
• すべての試料は3回定量され、3つの独立した実験が行われた。

MATERIALS AND METHODSAnalysis of EMD Liquid/EMD Gel Protein Release Kinetics From Grafting Materials With Time
• EMD liquidまたはEMD gelによりコーティングされたそれぞれの移植材から放出されたアメロジェニンタンパクの定量のために、コーティングされた顆粒を1mL PBSに浸漬し、8時間、1、3、5、10日の時間経過後、試料を回収した。
• そして試料はアメロジェニンタンパクの定量のため、ELISAを用いて分析された。
• それぞれの試料群について3回の独立した実験が行われた。

MATERIALS AND METHODS
Statistical Analysis
• すべてのデータは平均ー標準誤差として示した。
• 金でコーティングした顆粒を用いた実験の統計学的分析には一元配置分散分析を行った。
• さらに、ELISA法による定量の統計学的分析にも一元配置分散分析が用いられた。
RESULTS

RESULTSSEM and TEM
• まず、骨移植材の顆粒の大きさと表面形態の両方をSEMで観察した (Fig. 1)。
• NBM顆粒は他の2つの移植材よりも大きく(Fig. 1A)、 多くのmicro, nano サイズの表面性状を持つことがわかった(Fig. 1B)。
• 対照的に、DFDBA 顆粒は著しく小さく (Fig. 1C) おそらく脱灰と滅菌の結果、表面はなめらかになっている (Fig. 1D)。
• CaP は大きなスケールとnano スケールの表面粗さの特徴を示す (Figs. 1E and 1F)。
demonstrating the effects of the polyglycol alginate(PGA) carrier responsible for transporting enamelmatrix proteins in EMD gel (Fig. 2B). The TEM im-ages revealed that the combination of NBM + EMDliquid demonstrated gold-labeled particles of EMDprincipally directly at the surface of NBM scaffolds(Fig. 2C). It was also noted that some gold particleswere observed in the interior of scaffolds, demon-strating that EMD liquid was able to penetrate thesurface of NBM particles when delivered in a liquidformat and adsorb to the interior region of NBMparticles (Fig. 2C). Interestingly, scaffolds coatedwith EMD gel showed a much thicker pattern of goldlabeling, found extended from the surface of graftingparticles (Fig. 2D). Very little gold-labeling particleswere observed on the interior of grafting particlescoated with EMD gel when compared to coating withEMD liquid.
The coating of DFDBA par-ticles followed a similar pattern(Fig. 3). The surface topogra-phy of DFDBA particles was onlyslightly modified after coatingwith EMD liquid and did not affectthe surface characteristics ofDFDBA particles (Fig. 3A). Sim-ilarly to NBM particles, whenDFDBA particles were coatedwith EMD gel, the coating changedthe surface topography and sur-face properties of bone graftingparticles by demonstrating re-gions of thicker coating, likelya result of the PGA carrier used inEMD gel (Fig. 3B). Analysis ofTEM images revealed once againthat DFDBA particles coatedwith EMD liquid demonstratedsurface coating of gold-labeledanti-EMD antibody at the surfaceof grafting particles (Fig. 3C,arrows). In contrast, DFDBAparticles precoated with EMD geldemonstrated surface coatingwith a wide range of gold labelingextended from the surface asa result of the thickness of coatingvia EMD gel (Fig. 3D, arrows).
When CaP particles were coat-ed with EMD liquid, the surfacecharacteristics of particles dem-onstrated slightly modified sur-face topographies (Fig. 4A). Itwas again noted that when CaPparticles were coated with EMDgel, a thick gel-like pattern was
observed on the surface of grafting materials, likelycaused by the PGA carrier (Fig. 4B). Interestingly, theanalysis by TEM demonstrated that the gold labelingshowed staining at variable distances from the surfacein EMD liquid–coated CaP particles (Fig. 4C, arrows).Similarly, the coating of particles with EMD gel furtherincreased the range and distance from the surface ofthe CaP scaffolds (Fig. 4D, arrows).
TEM samples were then quantified for the numberof gold-labeling particles per image, and the averagedistance was calculated from the surface of bonegrafting materials (Fig. 5) (see supplementary Table 1in online Journal of Periodontology). A highernumber of gold labeling was observed on NBMand DFDBA scaffolds coated with EMD liquid whencompared to EMD gel (see supplementary Table 1 inonline Journal of Periodontology). Interestingly, onCaP scaffolds, only a small, non-significant increase
Figure 1.SEM of the bone grafting materials used for this study. Low (·70) (A) and high (·1,200) (B)magnification of a NBM bone graft derived from bovine origin displays bone chips resembling humanbone with visible large and small nanotopographies present on the surface. C) DFDBA demonstratessmaller-sized bone particles that lack mineralized tissues. (·25.) D) The surface properties showa smooth surface at highmagnification (·1,600). E and F) The CaP bone graft demonstrates a surfacewith many large and small nanotopographies. (·25 and ·1,600, respectively.) Scale bars = A) 500mm;B), D), and F) 20 mm; C) and E) 1 mm.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
581

RESULTSSEM and TEM
• さらにすべての骨移植材は EMD liquid または EMD gel でコーティングされ、SEM と TEM で表面状態を分析された (see Figs. 2 through 4)。
• NBM顆粒はその表面が EMD liquid と最も密接に境を接している (Fig. 2)。
• SEMの結果から、コントロールのNBMとEMD liquidでコーティングされたもので、表面性状は大きく変わらないことがわかった (Fig. 2A)。
• しかし、NBMがEMD gelでコーティングされた場合、EMD gelにおいてenamel matrix proteinのキャリアとなるPGAの効果を示す、大きなコーティングが顆粒表面に形成されている (Fig. 2B)。
was observed. The most notable difference was thedistance from which the labeling was observed fromthe scaffold surface. On NBM + EMD liquid andDFDBA + EMD liquid, most adsorption of proteinswas done either within the scaffold or directly on thescaffold surface. Results from the TEM analysis re-vealed values of 8.45 and 44.85 nm from the scaffoldsurface, respectively (Fig. 5) (see supplementaryTable 1 in online Journal of Periodontology). Whenthese scaffolds were coated with EMD gel, this distanceincreased to 906.45 and 1,133.65 nm, respectively.This same trend was also observed on CaP scaffolds,although to a lesser extent (Fig. 5) (supplementaryTable 1 in online Journal of Periodontology).
Quantification of Amelogenin Protein to theScaffold Surface by ELISATo provide a second method to quantify the adsorp-tion of amelogenin proteins to the surface of scaffoldscoated with either EMD liquid or EMD gel, ELISAprotein quantification was performed (Fig. 6). It wasshown that the coating of bone grafts with EMD liquidwas again superior for all bone grafts, but because ofthe variability in coating, a non-significant increasewas observed (Fig. 6A). Interestingly, when the
bone grafts were compared fortheir release of amelogenin pro-file with time, significant differ-ences were observed betweenEMD liquid and EMD gel (Figs.6B through 6D). For NBM parti-cles coated with either EMD liq-uid or EMD gel, it was observedthat 82.34 – 8.24 and 58.23 –13.25 ng, respectively, werecoated on the surface materials(Fig. 6B). After PBS rinsing, theresults demonstrated that, al-though NBM particles coatedwith EMD liquid decreasedslightly to 78.52 – 9.15 ng (from82.34 ng), surfaces coated withEMD gel decreased to 22.53 –14.54 ng (from 58.23 ng). Thus,one simple PBS rinse signifi-cantly reduced surface coatingof enamel matrix proteins frombone grafts coated with EMD gelbut had little effect on graftscoated with EMD liquid. There-after, only slight amounts ofamelogenin proteins were re-leased to the surrounding solu-tion during the time from 8 hoursto 10 days. This observation wasalso observed for DFDBA par-
ticles coated with either EMD liquid or EMD gel(Fig. 6C) and CaP particles (Fig. 6D). The resultsreveal that a single rinse with PBS is able to de-crease surface coating of amelogenin proteinscoated to bone grafting materials with EMD gel by>50% in all three bone grafting materials used in thisstudy (Fig. 6).
DISCUSSION
The aim of the current study is to investigate therelation between protein adsorption of enamel matrixproteins to grafting materials coated with either EMDin a liquid formulation or the commercially availableEMD gel. The use of EMD gel with a bone graft ina clinical setting has generated an array of mixedresults from clinical trials.22,23 Although a number ofstudies confirm an additional benefit, others havespeculated that only certain types of graftingmaterialsare advantageously mixed with EMD gel, whereasother grafts fail to provide additional benefits.22,23 Forthese reasons, the purpose of the present study is toinvestigate the patterns of enamel matrix proteinadsorption to the surface of grafting materials anddetermine what variability may exist between carriersystems for EMD.
Figure 2.SEM and TEM images of a NBM after coating with either EMD liquid or EMD gel. A) SEM image(·1,120) of NBM particles coated with EMD liquid demonstrates very similar surface characteristics asnative uncoatedparticles. The results from the TEM images, whichwere stained for EMDvia gold-labelingnanoparticles, demonstrate that all surface staining was either near the surface or penetrated withthe surface of the grafting material (C, arrows). B) In contrast, NBM particles coated with EMD geldemonstrated the presence of a much thicker coating by its PGA carrier.D) The surface coating with ananti-EMD antibody also revealed the presence of most of its coating far from the surface of graftingparticles (arrows). (·1,200.) Scale bars A and B) = 20 mm
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
582

RESULTSSEM and TEM
• TEM画像からは、NBMとEMD liquidの組み合わせでは金が付着したEMDの顆粒がNBMの足場の表面に主に直接存在することがわかる (Fig. 2C)。
• また、いくらかの金の粒子は足場の内側でも観察された。これは、EMD liquidはNBMの表面を貫通し、NBM顆粒の内部に吸着できることを示している (Fig. 2C)。
• 興味深いことに、EMD gelでコーティングされた足場では移植材表面から広がる、著しく厚いgold labelingが観察された (Fig. 2D)。
• EMD liquidと比較して、EMD gelでコーティングされた移植材の内部にはgold labeling顆粒はほとんど存在しなかった。
was observed. The most notable difference was thedistance from which the labeling was observed fromthe scaffold surface. On NBM + EMD liquid andDFDBA + EMD liquid, most adsorption of proteinswas done either within the scaffold or directly on thescaffold surface. Results from the TEM analysis re-vealed values of 8.45 and 44.85 nm from the scaffoldsurface, respectively (Fig. 5) (see supplementaryTable 1 in online Journal of Periodontology). Whenthese scaffolds were coated with EMD gel, this distanceincreased to 906.45 and 1,133.65 nm, respectively.This same trend was also observed on CaP scaffolds,although to a lesser extent (Fig. 5) (supplementaryTable 1 in online Journal of Periodontology).
Quantification of Amelogenin Protein to theScaffold Surface by ELISATo provide a second method to quantify the adsorp-tion of amelogenin proteins to the surface of scaffoldscoated with either EMD liquid or EMD gel, ELISAprotein quantification was performed (Fig. 6). It wasshown that the coating of bone grafts with EMD liquidwas again superior for all bone grafts, but because ofthe variability in coating, a non-significant increasewas observed (Fig. 6A). Interestingly, when the
bone grafts were compared fortheir release of amelogenin pro-file with time, significant differ-ences were observed betweenEMD liquid and EMD gel (Figs.6B through 6D). For NBM parti-cles coated with either EMD liq-uid or EMD gel, it was observedthat 82.34 – 8.24 and 58.23 –13.25 ng, respectively, werecoated on the surface materials(Fig. 6B). After PBS rinsing, theresults demonstrated that, al-though NBM particles coatedwith EMD liquid decreasedslightly to 78.52 – 9.15 ng (from82.34 ng), surfaces coated withEMD gel decreased to 22.53 –14.54 ng (from 58.23 ng). Thus,one simple PBS rinse signifi-cantly reduced surface coatingof enamel matrix proteins frombone grafts coated with EMD gelbut had little effect on graftscoated with EMD liquid. There-after, only slight amounts ofamelogenin proteins were re-leased to the surrounding solu-tion during the time from 8 hoursto 10 days. This observation wasalso observed for DFDBA par-
ticles coated with either EMD liquid or EMD gel(Fig. 6C) and CaP particles (Fig. 6D). The resultsreveal that a single rinse with PBS is able to de-crease surface coating of amelogenin proteinscoated to bone grafting materials with EMD gel by>50% in all three bone grafting materials used in thisstudy (Fig. 6).
DISCUSSION
The aim of the current study is to investigate therelation between protein adsorption of enamel matrixproteins to grafting materials coated with either EMDin a liquid formulation or the commercially availableEMD gel. The use of EMD gel with a bone graft ina clinical setting has generated an array of mixedresults from clinical trials.22,23 Although a number ofstudies confirm an additional benefit, others havespeculated that only certain types of graftingmaterialsare advantageously mixed with EMD gel, whereasother grafts fail to provide additional benefits.22,23 Forthese reasons, the purpose of the present study is toinvestigate the patterns of enamel matrix proteinadsorption to the surface of grafting materials anddetermine what variability may exist between carriersystems for EMD.
Figure 2.SEM and TEM images of a NBM after coating with either EMD liquid or EMD gel. A) SEM image(·1,120) of NBM particles coated with EMD liquid demonstrates very similar surface characteristics asnative uncoatedparticles. The results from the TEM images, whichwere stained for EMDvia gold-labelingnanoparticles, demonstrate that all surface staining was either near the surface or penetrated withthe surface of the grafting material (C, arrows). B) In contrast, NBM particles coated with EMD geldemonstrated the presence of a much thicker coating by its PGA carrier.D) The surface coating with ananti-EMD antibody also revealed the presence of most of its coating far from the surface of graftingparticles (arrows). (·1,200.) Scale bars A and B) = 20 mm
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
582

RESULTSSEM and TEM
• DFDBA顆粒のコーティングは同様の所見を示した (Fig. 3)。
• DFDBA顆粒の表面性状はEMD liquidによるコーティング後、ごくわずかに変化したのみで、DFDBA顆粒の表面の特徴には影響しなかった (Fig. 3A)。
• NBM顆粒と同様に、DFDBA顆粒がEMD gelでコーティングされた場合には、骨移植材顆粒表面の形態と特性は変わり、EMD gelに用いられるPGA carrierのためにコーティング層は厚くなった (Fig. 3B)。
In the present study, the choice was made toinvestigate three grafting materials commonly usedin dentistry. NBM was used as the xenograft of choicebecause it is studied extensively and the presentauthors have previous experience handling it. TheDFDBA used in this study was selected because ofits widespread use and osteoinductive advantagescompared to other DFDBA grafts.48-50 An alloplastbone graft fabricated from hydroxyapatite and b-TCPwas chosen as the synthetic material. To the best ofthe authors’ knowledge, in the present study, it is thefirst time observed by both SEM and TEM that largevariability existed with respect to the ability of enamelmatrix proteins to adsorb to these various bone grafts(Figs. 2 through 5). Interestingly, although the NBMparticles were able to adsorb the highest quantity ofprotein, the more interesting finding was the inabilityfor EMD gel to efficiently adsorb enamel matrix pro-teins to the surface of grafting materials at the presentsettings (Fig. 5). It was noted that the average distancein which amelogenin proteins were found from thesurface of bone grafting particles was >20 timesgreater in samples coated with EMD gel when com-pared to EMD liquid (see supplementary Table 1 inonline Journal of Periodontology).
The present study reveals thatthe adsorption of enamel matrixproteins may be attributed tothe material composition. BothDFDBA and NBM are derivedfrom natural bone, and their na-tive composition naturally con-tains specific sites for proteinadsorption. Because NBM parti-cles are completely devoid ofcells and proteins (deproteinizedmatrix), their ability to providespecific sites for new proteinadsorption make it an ideal graftchoice as a carrier for bioactivemolecules. A similar observationfor DFDBA was also observedwith a surprisingly high ability forenamel matrix proteins coatedwithin the interior surface ofgrafting material (Fig. 3A). Con-trary to this, no ability of EMDgel to penetrate the surface ofCaP molecules was observed.Because the surface containsno discernible pores able toallow any form of protein ad-sorption within the grafting ma-terial, it signifies that proteinadsorption is limited strictly tothe material surface, thus pro-
viding much less ability for the graft to carry ahigher load of bioactive molecules.
Although the SEM and TEM analyses were ableto provide much qualitative analysis, the use of anELISA kit greatly enhanced the ability to accuratelyquantify the amount of amelogenin bound to thematerial surface. Although each of the bone graftswas able to adsorb either EMD liquid or EMD gel tothe surface of the bone grafting material, the no-ticeable difference was evident after rinsing with PBSat neutral pH. Because this solution is used in vitro torepresent physiologic pH, the finding that a simplerinse was able to wash >50% of amelogenin bound tothe surface of grafting materials coated with EMD gelwas quite surprising (Fig. 6). Although it is verydifficult to speculate what effect this might have ina clinical setting, the finding that such a large per-centage of protein is flushed so easily raises theclinical concern that after the placement of EMD gel +bone graft in a bone defect, a similar effect might beimagined whereby bodily fluids are able to dissociatethe adsorbed enamel matrix proteins from the scaf-fold surface. Noteworthy also is the fact that bone ap-position should be directly adjacent to the bone graftingmaterial surface. In the present study, it is found that
Figure 3.SEM and TEM images of DFDBA after coating with either EMD liquid or EMD gel. A) SEM imageof DFDBA particles coated with EMD liquid demonstrates its smooth surface properties with littleaccumulation of a thick surface coatingwith amelogenin proteins. The results fromTEM further confirmedthat most of the staining was present on the surface or slightly penetrated within the surface of thegrafting material (C, arrows). B) In contrast, DFDBA particles coated with EMD gel demonstrated thepresence of a much thicker coating caused by its PGA carrier. The surface coating with an anti-EMDantibody also revealed the presence of most of its coating far from the surface of grafting particles(D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
583

RESULTSSEM and TEM
• TEM画像の分析からNBMと同様に、EMD liquidでコーティングされたDFDBA顆粒の表面にはgold-labelされた抗EMD抗体によるコーティングが見られた (Fig. 3C, arrows)。
• 対照的に、EMD gelでコーティングされたDFDBA顆粒では表面から広い幅のgold-labelが観察された (Fig. 3D, arrows)。
In the present study, the choice was made toinvestigate three grafting materials commonly usedin dentistry. NBM was used as the xenograft of choicebecause it is studied extensively and the presentauthors have previous experience handling it. TheDFDBA used in this study was selected because ofits widespread use and osteoinductive advantagescompared to other DFDBA grafts.48-50 An alloplastbone graft fabricated from hydroxyapatite and b-TCPwas chosen as the synthetic material. To the best ofthe authors’ knowledge, in the present study, it is thefirst time observed by both SEM and TEM that largevariability existed with respect to the ability of enamelmatrix proteins to adsorb to these various bone grafts(Figs. 2 through 5). Interestingly, although the NBMparticles were able to adsorb the highest quantity ofprotein, the more interesting finding was the inabilityfor EMD gel to efficiently adsorb enamel matrix pro-teins to the surface of grafting materials at the presentsettings (Fig. 5). It was noted that the average distancein which amelogenin proteins were found from thesurface of bone grafting particles was >20 timesgreater in samples coated with EMD gel when com-pared to EMD liquid (see supplementary Table 1 inonline Journal of Periodontology).
The present study reveals thatthe adsorption of enamel matrixproteins may be attributed tothe material composition. BothDFDBA and NBM are derivedfrom natural bone, and their na-tive composition naturally con-tains specific sites for proteinadsorption. Because NBM parti-cles are completely devoid ofcells and proteins (deproteinizedmatrix), their ability to providespecific sites for new proteinadsorption make it an ideal graftchoice as a carrier for bioactivemolecules. A similar observationfor DFDBA was also observedwith a surprisingly high ability forenamel matrix proteins coatedwithin the interior surface ofgrafting material (Fig. 3A). Con-trary to this, no ability of EMDgel to penetrate the surface ofCaP molecules was observed.Because the surface containsno discernible pores able toallow any form of protein ad-sorption within the grafting ma-terial, it signifies that proteinadsorption is limited strictly tothe material surface, thus pro-
viding much less ability for the graft to carry ahigher load of bioactive molecules.
Although the SEM and TEM analyses were ableto provide much qualitative analysis, the use of anELISA kit greatly enhanced the ability to accuratelyquantify the amount of amelogenin bound to thematerial surface. Although each of the bone graftswas able to adsorb either EMD liquid or EMD gel tothe surface of the bone grafting material, the no-ticeable difference was evident after rinsing with PBSat neutral pH. Because this solution is used in vitro torepresent physiologic pH, the finding that a simplerinse was able to wash >50% of amelogenin bound tothe surface of grafting materials coated with EMD gelwas quite surprising (Fig. 6). Although it is verydifficult to speculate what effect this might have ina clinical setting, the finding that such a large per-centage of protein is flushed so easily raises theclinical concern that after the placement of EMD gel +bone graft in a bone defect, a similar effect might beimagined whereby bodily fluids are able to dissociatethe adsorbed enamel matrix proteins from the scaf-fold surface. Noteworthy also is the fact that bone ap-position should be directly adjacent to the bone graftingmaterial surface. In the present study, it is found that
Figure 3.SEM and TEM images of DFDBA after coating with either EMD liquid or EMD gel. A) SEM imageof DFDBA particles coated with EMD liquid demonstrates its smooth surface properties with littleaccumulation of a thick surface coatingwith amelogenin proteins. The results fromTEM further confirmedthat most of the staining was present on the surface or slightly penetrated within the surface of thegrafting material (C, arrows). B) In contrast, DFDBA particles coated with EMD gel demonstrated thepresence of a much thicker coating caused by its PGA carrier. The surface coating with an anti-EMDantibody also revealed the presence of most of its coating far from the surface of grafting particles(D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
583

RESULTSSEM and TEM
• CaP顆粒がEMD liquidでコーティングされた場合、顆粒表面の特徴は表面状態がわずかに変化していることを示した (Fig. 4A)。
• CaP顆粒がEMD gelでコーティングされた場合、PGAキャリアによるものと思われる分厚いジェルのようなパターンが移植材の表面に観察された (Fig. 4B)。
the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584

RESULTSSEM and TEM
• 興味深いことにTEMによる分析から、EMD liquidでコーティングされたCaP顆粒の表面から様々な距離にgold labelingによるステインが見られることがわかった (Fig. 4C, arrows)。
• 同様に、EMD gelによる顆粒のコーティングではCaPの表面からの範囲と距離が著しく増加した (Fig. 4D, arrows)。
the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584

RESULTS
the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584
SEM and TEM
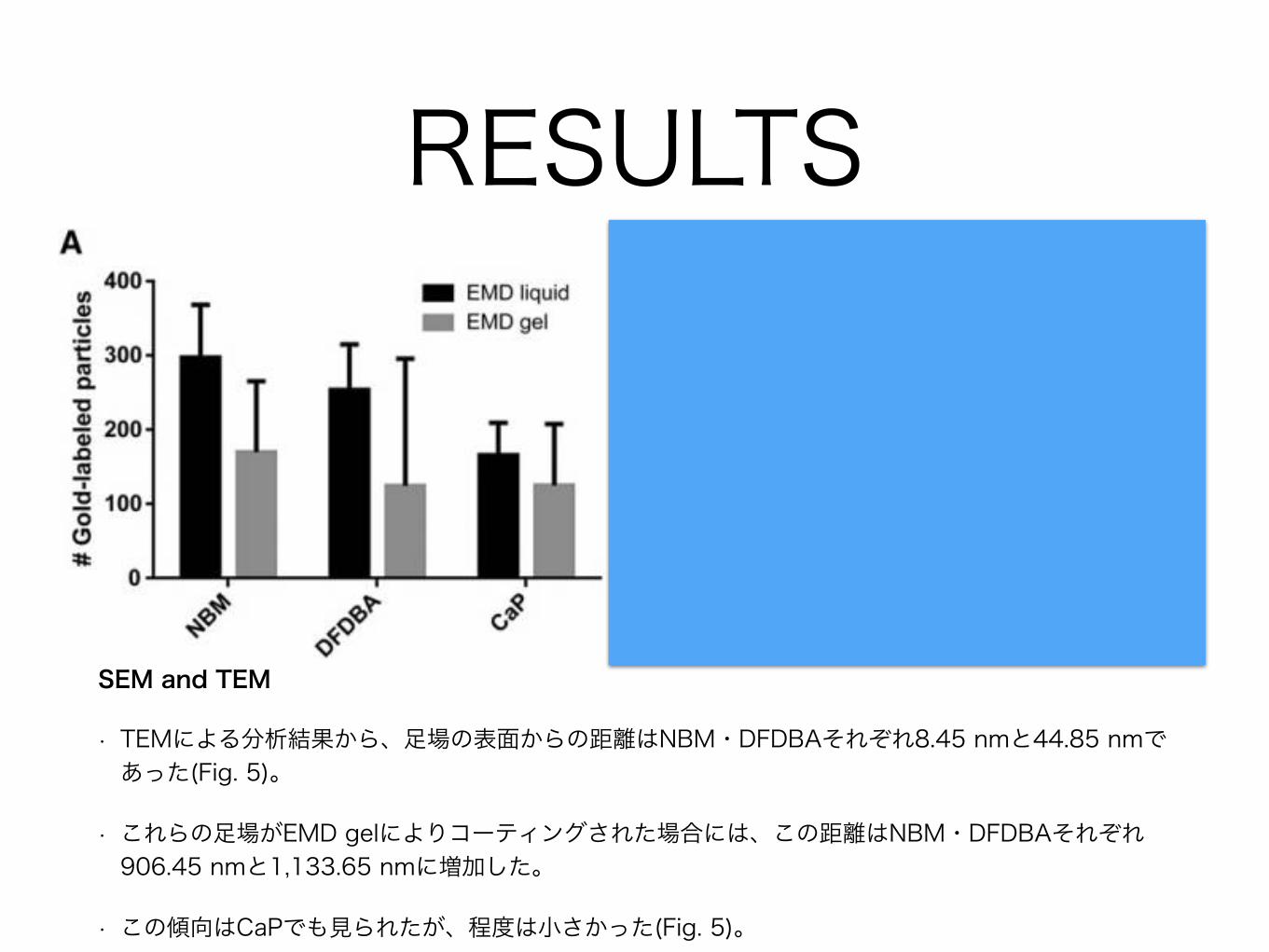
• さらにTEM標本において画像ごとのgold-labeling粒子の数を測定し、骨移植材の表面からの平均距離を計算した (Fig. 5)。
• NBMとDFDBAではEMD gelに比べてEMD liquidでgold labelingがより多く観察された。
• 興味深いことに、CaPではごくわずかな、有意差のない増加が認められるのみであった。

RESULTS
SEM and TEM
• 最も顕著な違いは足場の表面からlabelingが観察された位置までの距離であった。
• NBM + EMD liquidとDFDBA + EMD liquidでは、タンパクの吸着のほとんどは足場の内側か表面であった。
the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584
RESULTS
SEM and TEM
• TEMによる分析結果から、足場の表面からの距離はNBM・DFDBAそれぞれ8.45 nmと44.85 nmであった(Fig. 5)。
• これらの足場がEMD gelによりコーティングされた場合には、この距離はNBM・DFDBAそれぞれ906.45 nmと1,133.65 nmに増加した。
• この傾向はCaPでも見られたが、程度は小さかった(Fig. 5)。the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584

RESULTSQuantification of Amelogenin Protein to the Scaffold Surface by ELISA
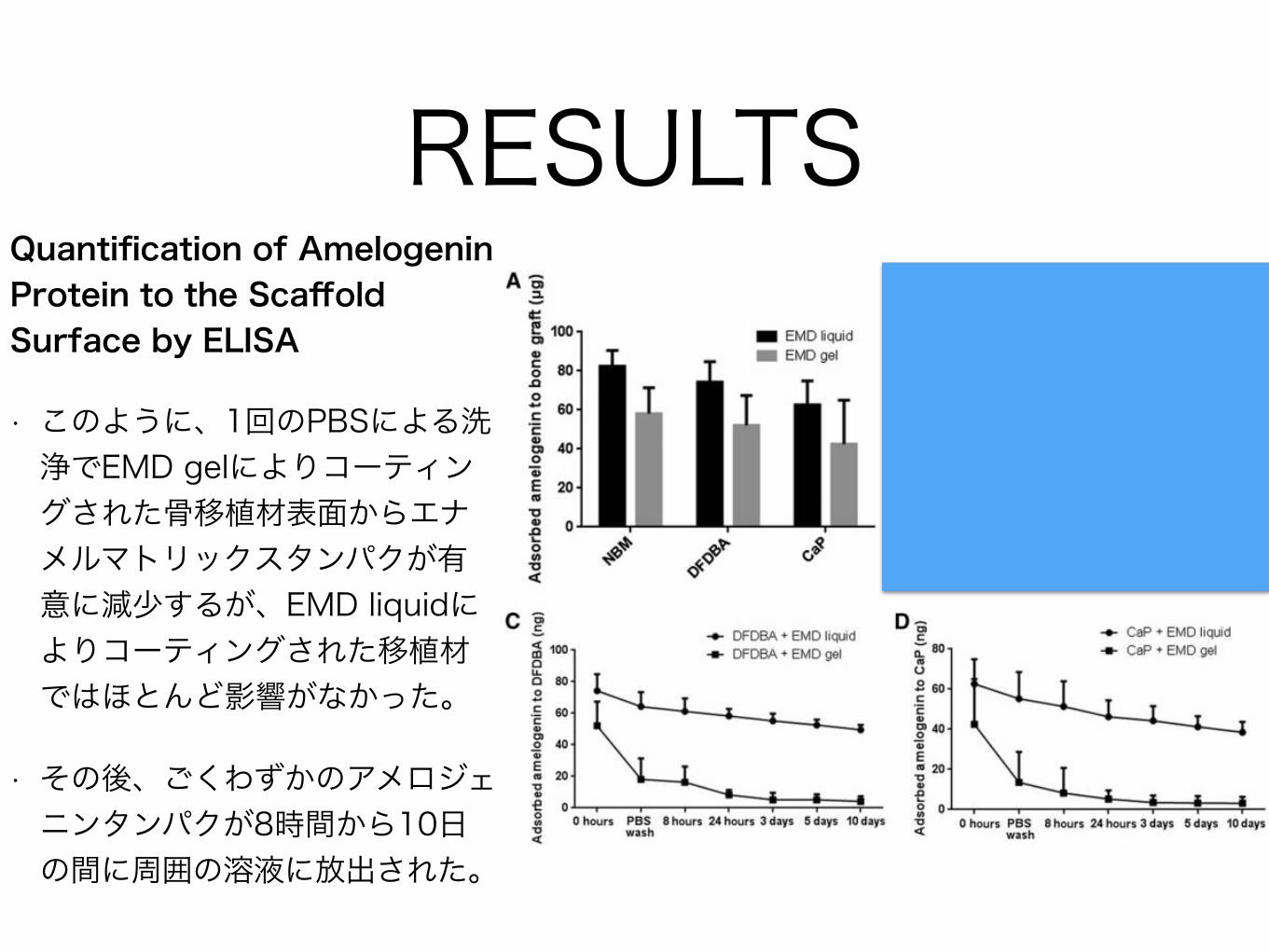
• EMD liquidまたはEMD gelによりコーティングされた足場の表面へのアメロジェニンタンパクの吸着を定量するための2番目の手法として、ELISAが用いられた(Fig. 6)。
• EMD liquidによる骨移植材のコーティングはすべての骨移植材に対してより優れていることが再度示されたが、コーティングの多様性のために、有意差に届かない増加が観察された(Fig. 6A)。
Dr. Sculean has received lecture fees from InstituteStraumann. Institute Straumannmanufactured the bonegraft, EMD, and EMD gel used in this study. Drs. Miron,Bosshardt, Buser, Zhang, Caluseru, and Chandad re-port no conflicts of interest related to this study.
REFERENCES1. Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized
ridge augmentation using guided bone regeneration. 1.Surgical procedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13:29-45.
2. Jung RE, Fenner N, Hammerle CH, Zitzmann NU. Long-term outcome of implants placed with guided boneregeneration (GBR)using resorbable andnon-resorbablemembranes after 12-14 years. Clin Oral Implants Res2013;24:1065-1073.
3. Lorenzoni M, Pertl C, Keil C, Wegscheider WA. Treat-ment of peri-implant defects with guided bone regener-ation:A comparative clinical studywith variousmembranesand bone grafts. Int J Oral Maxillofac Implants 1998;13:639-646.
4. Wiltfang J, Schultze-Mosgau S, Merten HA, Kessler P,LudwigA,EngelkeW.Endoscopic andultrasonographicevaluation of the maxillary sinus after combined sinusfloor augmentation and implant insertion.Oral SurgOralMed Oral Pathol Oral Radiol Endod 2000;89:288-291.
5. Calori GM,Mazza E, ColomboM, Ripamonti C. The use ofbone-graft substitutes in large bone defects: Any specificneeds? Injury 2011;42(Suppl. 2):S56-S63.
6. Dragoo MR, Sullivan HC. Aclinical and histological evalu-ation of autogenous iliac bonegrafts in humans. I. Woundhealing 2 to 8 months. J Peri-odontol 1973;44:599-613.
7. Gross JS. Bone grafting mate-rials for dental applications: Apractical guide. Compend Con-tin Educ Dent 1997;18:1013-1018,1020-1022,1024,passim;quiz.
8. Hiatt WH, Schallhorn RG,Aaronian AJ. The induction ofnew bone and cementum for-mation. IV. Microscopic exam-ination of the periodontiumfollowing human bone andmarrow allograft, autograftand nongraft periodontal re-generative procedures. J Peri-odontol 1978;49:495-512.
9. Misch CE, Dietsh F. Bone-grafting materials in implantdentistry. Implant Dent1993;2:158-167.
10. Froum SJ, Wallace SS, ChoSC, Elian N, Tarnow DP. His-tomorphometric comparison ofa biphasic bone ceramic toanorganic bovine bone for si-nus augmentation: 6- to 8-month postsurgical assessmentof vital bone formation. A pilotstudy. Int J Periodontics Restor-ative Dent 2008;28:273-281.
11. Schwartz Z, Weesner T, van Dijk S, et al. Ability ofdeproteinized cancellous bovine bone to induce newboneformation. J Periodontol 2000;71:1258-1269.
12. Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- andgene-based therapeutic strategies for periodontal regen-erative medicine. J Periodontol 2011;82:1223-1237.
13. Jepsen S, Heinz B, Jepsen K, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal Class II furcation in-volvement in mandibular molars. Part I: Study designand results for primary outcomes. J Periodontol 2004;75:1150-1160.
14. Meyle J, Gonzales JR, Bodeker RH, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal class II furcation in-volvement in mandibular molars. Part II: Secondaryoutcomes. J Periodontol 2004;75:1188-1195.
15. Modica F, Del Pizzo M, Roccuzzo M, Romagnoli R.Coronally advanced flap for the treatment of buccalgingival recessions with and without enamel matrixderivative. A split-mouth study. J Periodontol 2000;71:1693-1698.
16. Nemcovsky CE, Artzi Z, Tal H, Kozlovsky A, Moses O.A multicenter comparative study of two root coverageprocedures: Coronally advanced flap with addition ofenamel matrix proteins and subpedicle connectivetissue graft. J Periodontol 2004;75:600-607.
17. Sculean A, Donos N, Windisch P, et al. Healing ofhuman intrabony defects following treatment withenamel matrix proteins or guided tissue regeneration.J Periodontal Res 1999;34:310-322.
Figure 6.A)Quantitative analysis by ELISA to determine the quantity of adsorbed amelogenin proteins demonstratesa slight, non-significantpreference for grafting particles coatedwith EMD liquid.BthroughD) Interestingly,the surfaces coated with EMD gel demonstrated a much faster release profile of amelogeninproteins with time, demonstrating a more preferential binding of amelogenin to bone grafting particleswhen particles were coated with EMD liquid compared to EMD gel.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
585

RESULTSQuantification of Amelogenin Protein to the Scaffold Surface by ELISA
• 興味深いことに、骨移植材を経時的なアメロジェニンタンパクの放出について比較したところ、EMD liquidとEMD gelの間に有意差が見られた(Figs. 6B through 6D)。
Dr. Sculean has received lecture fees from InstituteStraumann. Institute Straumannmanufactured the bonegraft, EMD, and EMD gel used in this study. Drs. Miron,Bosshardt, Buser, Zhang, Caluseru, and Chandad re-port no conflicts of interest related to this study.
REFERENCES1. Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized
ridge augmentation using guided bone regeneration. 1.Surgical procedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13:29-45.
2. Jung RE, Fenner N, Hammerle CH, Zitzmann NU. Long-term outcome of implants placed with guided boneregeneration (GBR)using resorbable andnon-resorbablemembranes after 12-14 years. Clin Oral Implants Res2013;24:1065-1073.
3. Lorenzoni M, Pertl C, Keil C, Wegscheider WA. Treat-ment of peri-implant defects with guided bone regener-ation:A comparative clinical studywith variousmembranesand bone grafts. Int J Oral Maxillofac Implants 1998;13:639-646.
4. Wiltfang J, Schultze-Mosgau S, Merten HA, Kessler P,LudwigA,EngelkeW.Endoscopic andultrasonographicevaluation of the maxillary sinus after combined sinusfloor augmentation and implant insertion.Oral SurgOralMed Oral Pathol Oral Radiol Endod 2000;89:288-291.
5. Calori GM,Mazza E, ColomboM, Ripamonti C. The use ofbone-graft substitutes in large bone defects: Any specificneeds? Injury 2011;42(Suppl. 2):S56-S63.
6. Dragoo MR, Sullivan HC. Aclinical and histological evalu-ation of autogenous iliac bonegrafts in humans. I. Woundhealing 2 to 8 months. J Peri-odontol 1973;44:599-613.
7. Gross JS. Bone grafting mate-rials for dental applications: Apractical guide. Compend Con-tin Educ Dent 1997;18:1013-1018,1020-1022,1024,passim;quiz.
8. Hiatt WH, Schallhorn RG,Aaronian AJ. The induction ofnew bone and cementum for-mation. IV. Microscopic exam-ination of the periodontiumfollowing human bone andmarrow allograft, autograftand nongraft periodontal re-generative procedures. J Peri-odontol 1978;49:495-512.
9. Misch CE, Dietsh F. Bone-grafting materials in implantdentistry. Implant Dent1993;2:158-167.
10. Froum SJ, Wallace SS, ChoSC, Elian N, Tarnow DP. His-tomorphometric comparison ofa biphasic bone ceramic toanorganic bovine bone for si-nus augmentation: 6- to 8-month postsurgical assessmentof vital bone formation. A pilotstudy. Int J Periodontics Restor-ative Dent 2008;28:273-281.
11. Schwartz Z, Weesner T, van Dijk S, et al. Ability ofdeproteinized cancellous bovine bone to induce newboneformation. J Periodontol 2000;71:1258-1269.
12. Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- andgene-based therapeutic strategies for periodontal regen-erative medicine. J Periodontol 2011;82:1223-1237.
13. Jepsen S, Heinz B, Jepsen K, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal Class II furcation in-volvement in mandibular molars. Part I: Study designand results for primary outcomes. J Periodontol 2004;75:1150-1160.
14. Meyle J, Gonzales JR, Bodeker RH, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal class II furcation in-volvement in mandibular molars. Part II: Secondaryoutcomes. J Periodontol 2004;75:1188-1195.
15. Modica F, Del Pizzo M, Roccuzzo M, Romagnoli R.Coronally advanced flap for the treatment of buccalgingival recessions with and without enamel matrixderivative. A split-mouth study. J Periodontol 2000;71:1693-1698.
16. Nemcovsky CE, Artzi Z, Tal H, Kozlovsky A, Moses O.A multicenter comparative study of two root coverageprocedures: Coronally advanced flap with addition ofenamel matrix proteins and subpedicle connectivetissue graft. J Periodontol 2004;75:600-607.
17. Sculean A, Donos N, Windisch P, et al. Healing ofhuman intrabony defects following treatment withenamel matrix proteins or guided tissue regeneration.J Periodontal Res 1999;34:310-322.
Figure 6.A)Quantitative analysis by ELISA to determine the quantity of adsorbed amelogenin proteins demonstratesa slight, non-significantpreference for grafting particles coatedwith EMD liquid.BthroughD) Interestingly,the surfaces coated with EMD gel demonstrated a much faster release profile of amelogeninproteins with time, demonstrating a more preferential binding of amelogenin to bone grafting particleswhen particles were coated with EMD liquid compared to EMD gel.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
585

RESULTSQuantification of Amelogenin Protein to the Scaffold Surface by ELISA
• EMD liquidまたはEMD gelでコーティングされたNBM顆粒では、表面がそれぞれ82.34 ± 8.24 ngと58.23 ± 13.25 ngのアメロジェニンタンパクにコーティングされていた(Fig. 6B)
• PBSによる洗浄後、EMD liquidによりコーティングされたNBM顆粒は82.34 ngから78.52 ± 9.15 ngにわずかに減少した一方、EMD gelでコーティングされたものは58.23 ngから22.53 ± 14.54 ngに減少した。
Dr. Sculean has received lecture fees from InstituteStraumann. Institute Straumannmanufactured the bonegraft, EMD, and EMD gel used in this study. Drs. Miron,Bosshardt, Buser, Zhang, Caluseru, and Chandad re-port no conflicts of interest related to this study.
REFERENCES1. Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized
ridge augmentation using guided bone regeneration. 1.Surgical procedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13:29-45.
2. Jung RE, Fenner N, Hammerle CH, Zitzmann NU. Long-term outcome of implants placed with guided boneregeneration (GBR)using resorbable andnon-resorbablemembranes after 12-14 years. Clin Oral Implants Res2013;24:1065-1073.
3. Lorenzoni M, Pertl C, Keil C, Wegscheider WA. Treat-ment of peri-implant defects with guided bone regener-ation:A comparative clinical studywith variousmembranesand bone grafts. Int J Oral Maxillofac Implants 1998;13:639-646.
4. Wiltfang J, Schultze-Mosgau S, Merten HA, Kessler P,LudwigA,EngelkeW.Endoscopic andultrasonographicevaluation of the maxillary sinus after combined sinusfloor augmentation and implant insertion.Oral SurgOralMed Oral Pathol Oral Radiol Endod 2000;89:288-291.
5. Calori GM,Mazza E, ColomboM, Ripamonti C. The use ofbone-graft substitutes in large bone defects: Any specificneeds? Injury 2011;42(Suppl. 2):S56-S63.
6. Dragoo MR, Sullivan HC. Aclinical and histological evalu-ation of autogenous iliac bonegrafts in humans. I. Woundhealing 2 to 8 months. J Peri-odontol 1973;44:599-613.
7. Gross JS. Bone grafting mate-rials for dental applications: Apractical guide. Compend Con-tin Educ Dent 1997;18:1013-1018,1020-1022,1024,passim;quiz.
8. Hiatt WH, Schallhorn RG,Aaronian AJ. The induction ofnew bone and cementum for-mation. IV. Microscopic exam-ination of the periodontiumfollowing human bone andmarrow allograft, autograftand nongraft periodontal re-generative procedures. J Peri-odontol 1978;49:495-512.
9. Misch CE, Dietsh F. Bone-grafting materials in implantdentistry. Implant Dent1993;2:158-167.
10. Froum SJ, Wallace SS, ChoSC, Elian N, Tarnow DP. His-tomorphometric comparison ofa biphasic bone ceramic toanorganic bovine bone for si-nus augmentation: 6- to 8-month postsurgical assessmentof vital bone formation. A pilotstudy. Int J Periodontics Restor-ative Dent 2008;28:273-281.
11. Schwartz Z, Weesner T, van Dijk S, et al. Ability ofdeproteinized cancellous bovine bone to induce newboneformation. J Periodontol 2000;71:1258-1269.
12. Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- andgene-based therapeutic strategies for periodontal regen-erative medicine. J Periodontol 2011;82:1223-1237.
13. Jepsen S, Heinz B, Jepsen K, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal Class II furcation in-volvement in mandibular molars. Part I: Study designand results for primary outcomes. J Periodontol 2004;75:1150-1160.
14. Meyle J, Gonzales JR, Bodeker RH, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal class II furcation in-volvement in mandibular molars. Part II: Secondaryoutcomes. J Periodontol 2004;75:1188-1195.
15. Modica F, Del Pizzo M, Roccuzzo M, Romagnoli R.Coronally advanced flap for the treatment of buccalgingival recessions with and without enamel matrixderivative. A split-mouth study. J Periodontol 2000;71:1693-1698.
16. Nemcovsky CE, Artzi Z, Tal H, Kozlovsky A, Moses O.A multicenter comparative study of two root coverageprocedures: Coronally advanced flap with addition ofenamel matrix proteins and subpedicle connectivetissue graft. J Periodontol 2004;75:600-607.
17. Sculean A, Donos N, Windisch P, et al. Healing ofhuman intrabony defects following treatment withenamel matrix proteins or guided tissue regeneration.J Periodontal Res 1999;34:310-322.
Figure 6.A)Quantitative analysis by ELISA to determine the quantity of adsorbed amelogenin proteins demonstratesa slight, non-significantpreference for grafting particles coatedwith EMD liquid.BthroughD) Interestingly,the surfaces coated with EMD gel demonstrated a much faster release profile of amelogeninproteins with time, demonstrating a more preferential binding of amelogenin to bone grafting particleswhen particles were coated with EMD liquid compared to EMD gel.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
585
RESULTSQuantification of Amelogenin Protein to the Scaffold Surface by ELISA
• このように、1回のPBSによる洗浄でEMD gelによりコーティングされた骨移植材表面からエナメルマトリックスタンパクが有意に減少するが、EMD liquidによりコーティングされた移植材ではほとんど影響がなかった。
• その後、ごくわずかのアメロジェニンタンパクが8時間から10日の間に周囲の溶液に放出された。
Dr. Sculean has received lecture fees from InstituteStraumann. Institute Straumannmanufactured the bonegraft, EMD, and EMD gel used in this study. Drs. Miron,Bosshardt, Buser, Zhang, Caluseru, and Chandad re-port no conflicts of interest related to this study.
REFERENCES1. Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized
ridge augmentation using guided bone regeneration. 1.Surgical procedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13:29-45.
2. Jung RE, Fenner N, Hammerle CH, Zitzmann NU. Long-term outcome of implants placed with guided boneregeneration (GBR)using resorbable andnon-resorbablemembranes after 12-14 years. Clin Oral Implants Res2013;24:1065-1073.
3. Lorenzoni M, Pertl C, Keil C, Wegscheider WA. Treat-ment of peri-implant defects with guided bone regener-ation:A comparative clinical studywith variousmembranesand bone grafts. Int J Oral Maxillofac Implants 1998;13:639-646.
4. Wiltfang J, Schultze-Mosgau S, Merten HA, Kessler P,LudwigA,EngelkeW.Endoscopic andultrasonographicevaluation of the maxillary sinus after combined sinusfloor augmentation and implant insertion.Oral SurgOralMed Oral Pathol Oral Radiol Endod 2000;89:288-291.
5. Calori GM,Mazza E, ColomboM, Ripamonti C. The use ofbone-graft substitutes in large bone defects: Any specificneeds? Injury 2011;42(Suppl. 2):S56-S63.
6. Dragoo MR, Sullivan HC. Aclinical and histological evalu-ation of autogenous iliac bonegrafts in humans. I. Woundhealing 2 to 8 months. J Peri-odontol 1973;44:599-613.
7. Gross JS. Bone grafting mate-rials for dental applications: Apractical guide. Compend Con-tin Educ Dent 1997;18:1013-1018,1020-1022,1024,passim;quiz.
8. Hiatt WH, Schallhorn RG,Aaronian AJ. The induction ofnew bone and cementum for-mation. IV. Microscopic exam-ination of the periodontiumfollowing human bone andmarrow allograft, autograftand nongraft periodontal re-generative procedures. J Peri-odontol 1978;49:495-512.
9. Misch CE, Dietsh F. Bone-grafting materials in implantdentistry. Implant Dent1993;2:158-167.
10. Froum SJ, Wallace SS, ChoSC, Elian N, Tarnow DP. His-tomorphometric comparison ofa biphasic bone ceramic toanorganic bovine bone for si-nus augmentation: 6- to 8-month postsurgical assessmentof vital bone formation. A pilotstudy. Int J Periodontics Restor-ative Dent 2008;28:273-281.
11. Schwartz Z, Weesner T, van Dijk S, et al. Ability ofdeproteinized cancellous bovine bone to induce newboneformation. J Periodontol 2000;71:1258-1269.
12. Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- andgene-based therapeutic strategies for periodontal regen-erative medicine. J Periodontol 2011;82:1223-1237.
13. Jepsen S, Heinz B, Jepsen K, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal Class II furcation in-volvement in mandibular molars. Part I: Study designand results for primary outcomes. J Periodontol 2004;75:1150-1160.
14. Meyle J, Gonzales JR, Bodeker RH, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal class II furcation in-volvement in mandibular molars. Part II: Secondaryoutcomes. J Periodontol 2004;75:1188-1195.
15. Modica F, Del Pizzo M, Roccuzzo M, Romagnoli R.Coronally advanced flap for the treatment of buccalgingival recessions with and without enamel matrixderivative. A split-mouth study. J Periodontol 2000;71:1693-1698.
16. Nemcovsky CE, Artzi Z, Tal H, Kozlovsky A, Moses O.A multicenter comparative study of two root coverageprocedures: Coronally advanced flap with addition ofenamel matrix proteins and subpedicle connectivetissue graft. J Periodontol 2004;75:600-607.
17. Sculean A, Donos N, Windisch P, et al. Healing ofhuman intrabony defects following treatment withenamel matrix proteins or guided tissue regeneration.J Periodontal Res 1999;34:310-322.
Figure 6.A)Quantitative analysis by ELISA to determine the quantity of adsorbed amelogenin proteins demonstratesa slight, non-significantpreference for grafting particles coatedwith EMD liquid.BthroughD) Interestingly,the surfaces coated with EMD gel demonstrated a much faster release profile of amelogeninproteins with time, demonstrating a more preferential binding of amelogenin to bone grafting particleswhen particles were coated with EMD liquid compared to EMD gel.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
585

RESULTSQuantification of Amelogenin Protein to the Scaffold Surface by ELISA
• この所見はEMD liquidまたはEMD gelでコーティングされたDFDBA顆粒(Fig. 6C)とCaP顆粒(Fig. 6D)でも観察された
• 結果から今回の研究で用いた3種類の骨移植材において、PBSによる1回の洗浄でEMD gelによりコーティングされた骨移植材表面のアメロジェニンタンパクを50%以上減少させることができることがわかった(Fig. 6)。
Dr. Sculean has received lecture fees from InstituteStraumann. Institute Straumannmanufactured the bonegraft, EMD, and EMD gel used in this study. Drs. Miron,Bosshardt, Buser, Zhang, Caluseru, and Chandad re-port no conflicts of interest related to this study.
REFERENCES1. Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized
ridge augmentation using guided bone regeneration. 1.Surgical procedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13:29-45.
2. Jung RE, Fenner N, Hammerle CH, Zitzmann NU. Long-term outcome of implants placed with guided boneregeneration (GBR)using resorbable andnon-resorbablemembranes after 12-14 years. Clin Oral Implants Res2013;24:1065-1073.
3. Lorenzoni M, Pertl C, Keil C, Wegscheider WA. Treat-ment of peri-implant defects with guided bone regener-ation:A comparative clinical studywith variousmembranesand bone grafts. Int J Oral Maxillofac Implants 1998;13:639-646.
4. Wiltfang J, Schultze-Mosgau S, Merten HA, Kessler P,LudwigA,EngelkeW.Endoscopic andultrasonographicevaluation of the maxillary sinus after combined sinusfloor augmentation and implant insertion.Oral SurgOralMed Oral Pathol Oral Radiol Endod 2000;89:288-291.
5. Calori GM,Mazza E, ColomboM, Ripamonti C. The use ofbone-graft substitutes in large bone defects: Any specificneeds? Injury 2011;42(Suppl. 2):S56-S63.
6. Dragoo MR, Sullivan HC. Aclinical and histological evalu-ation of autogenous iliac bonegrafts in humans. I. Woundhealing 2 to 8 months. J Peri-odontol 1973;44:599-613.
7. Gross JS. Bone grafting mate-rials for dental applications: Apractical guide. Compend Con-tin Educ Dent 1997;18:1013-1018,1020-1022,1024,passim;quiz.
8. Hiatt WH, Schallhorn RG,Aaronian AJ. The induction ofnew bone and cementum for-mation. IV. Microscopic exam-ination of the periodontiumfollowing human bone andmarrow allograft, autograftand nongraft periodontal re-generative procedures. J Peri-odontol 1978;49:495-512.
9. Misch CE, Dietsh F. Bone-grafting materials in implantdentistry. Implant Dent1993;2:158-167.
10. Froum SJ, Wallace SS, ChoSC, Elian N, Tarnow DP. His-tomorphometric comparison ofa biphasic bone ceramic toanorganic bovine bone for si-nus augmentation: 6- to 8-month postsurgical assessmentof vital bone formation. A pilotstudy. Int J Periodontics Restor-ative Dent 2008;28:273-281.
11. Schwartz Z, Weesner T, van Dijk S, et al. Ability ofdeproteinized cancellous bovine bone to induce newboneformation. J Periodontol 2000;71:1258-1269.
12. Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- andgene-based therapeutic strategies for periodontal regen-erative medicine. J Periodontol 2011;82:1223-1237.
13. Jepsen S, Heinz B, Jepsen K, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal Class II furcation in-volvement in mandibular molars. Part I: Study designand results for primary outcomes. J Periodontol 2004;75:1150-1160.
14. Meyle J, Gonzales JR, Bodeker RH, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal class II furcation in-volvement in mandibular molars. Part II: Secondaryoutcomes. J Periodontol 2004;75:1188-1195.
15. Modica F, Del Pizzo M, Roccuzzo M, Romagnoli R.Coronally advanced flap for the treatment of buccalgingival recessions with and without enamel matrixderivative. A split-mouth study. J Periodontol 2000;71:1693-1698.
16. Nemcovsky CE, Artzi Z, Tal H, Kozlovsky A, Moses O.A multicenter comparative study of two root coverageprocedures: Coronally advanced flap with addition ofenamel matrix proteins and subpedicle connectivetissue graft. J Periodontol 2004;75:600-607.
17. Sculean A, Donos N, Windisch P, et al. Healing ofhuman intrabony defects following treatment withenamel matrix proteins or guided tissue regeneration.J Periodontal Res 1999;34:310-322.
Figure 6.A)Quantitative analysis by ELISA to determine the quantity of adsorbed amelogenin proteins demonstratesa slight, non-significantpreference for grafting particles coatedwith EMD liquid.BthroughD) Interestingly,the surfaces coated with EMD gel demonstrated a much faster release profile of amelogeninproteins with time, demonstrating a more preferential binding of amelogenin to bone grafting particleswhen particles were coated with EMD liquid compared to EMD gel.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
585

DISCUSSION
DISCUSSION• 今回の研究の目的は液状のEMDまたは市場で入手可能なEMD gelによりコーティングされた骨移植材におけるエナメルマトリックスタンパクの吸着を調べることである。
• 臨床研究において、EMD gelと骨移植材の併用の結果は様々である。
• 多くの研究で付加的な効果が確認されているが、一方では特定の種類の骨移植材のみがEMD gelとの併用で付加的な効果をもたらし、それ以外の移植材に付加的な効果はないと推測されている。
• これらの理由で、今回の研究の目的は移植材の表面に対するエナメルマトリックスタンパクの吸着のパターンの調査とEMDのキャリアシステム間にどのような違いがあるかを調べることである。
DISCUSSION• 今回の研究では歯科臨床で一般的に用いられる3種類の移植材を調査することとした。
• NBMは多くの研究で用いられており、本研究の著者らも以前に扱った経験があるため、異種骨移植材として選択した。
• 今回の研究で用いたDFDBAは広く用いられていることと、他のDFDBAと比較して骨誘導能が高いために選択した。
• ハイドロキシアパタイトとβ-TCPから作られた無機移植材は合成材料として選択した。
• 今回の研究は様々な骨移植材に対するエナメルマトリックスタンパクの吸着の能力に多様性が存在することを、SEMとTEMの両方で観察した著者の知る限り最初の研究である(Figs. 2 through 5)。

• 興味深いことに、NBM顆粒が最も大量にタンパクを吸着することができたが、さらに面白い所見は今回の設定では移植材の表面に対するエナメルマトリックスタンパクの効果的な吸着がEMD gelでは起こらないということである(Fig. 5)。
the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584
DISCUSSION

• アメロジェニンタンパクが観察された骨移植材表面からの平均距離は、EMD liquidでコーティングされた試料と比べてEMD gelでは20倍以上であった。
the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584
DISCUSSION
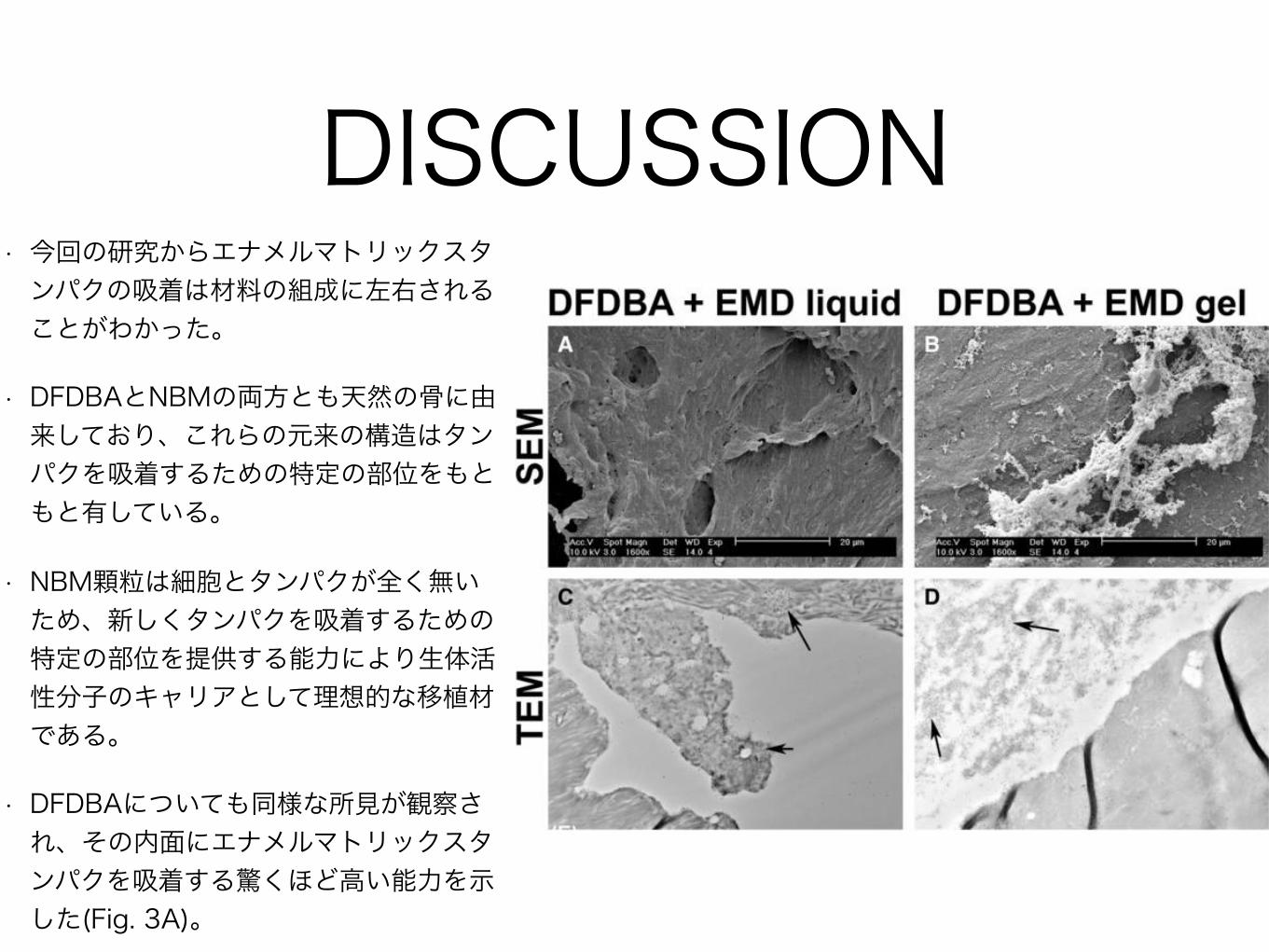
• 今回の研究からエナメルマトリックスタンパクの吸着は材料の組成に左右されることがわかった。
• DFDBAとNBMの両方とも天然の骨に由来しており、これらの元来の構造はタンパクを吸着するための特定の部位をもともと有している。
• NBM顆粒は細胞とタンパクが全く無いため、新しくタンパクを吸着するための特定の部位を提供する能力により生体活性分子のキャリアとして理想的な移植材である。
• DFDBAについても同様な所見が観察され、その内面にエナメルマトリックスタンパクを吸着する驚くほど高い能力を示した(Fig. 3A)。
In the present study, the choice was made toinvestigate three grafting materials commonly usedin dentistry. NBM was used as the xenograft of choicebecause it is studied extensively and the presentauthors have previous experience handling it. TheDFDBA used in this study was selected because ofits widespread use and osteoinductive advantagescompared to other DFDBA grafts.48-50 An alloplastbone graft fabricated from hydroxyapatite and b-TCPwas chosen as the synthetic material. To the best ofthe authors’ knowledge, in the present study, it is thefirst time observed by both SEM and TEM that largevariability existed with respect to the ability of enamelmatrix proteins to adsorb to these various bone grafts(Figs. 2 through 5). Interestingly, although the NBMparticles were able to adsorb the highest quantity ofprotein, the more interesting finding was the inabilityfor EMD gel to efficiently adsorb enamel matrix pro-teins to the surface of grafting materials at the presentsettings (Fig. 5). It was noted that the average distancein which amelogenin proteins were found from thesurface of bone grafting particles was >20 timesgreater in samples coated with EMD gel when com-pared to EMD liquid (see supplementary Table 1 inonline Journal of Periodontology).
The present study reveals thatthe adsorption of enamel matrixproteins may be attributed tothe material composition. BothDFDBA and NBM are derivedfrom natural bone, and their na-tive composition naturally con-tains specific sites for proteinadsorption. Because NBM parti-cles are completely devoid ofcells and proteins (deproteinizedmatrix), their ability to providespecific sites for new proteinadsorption make it an ideal graftchoice as a carrier for bioactivemolecules. A similar observationfor DFDBA was also observedwith a surprisingly high ability forenamel matrix proteins coatedwithin the interior surface ofgrafting material (Fig. 3A). Con-trary to this, no ability of EMDgel to penetrate the surface ofCaP molecules was observed.Because the surface containsno discernible pores able toallow any form of protein ad-sorption within the grafting ma-terial, it signifies that proteinadsorption is limited strictly tothe material surface, thus pro-
viding much less ability for the graft to carry ahigher load of bioactive molecules.
Although the SEM and TEM analyses were ableto provide much qualitative analysis, the use of anELISA kit greatly enhanced the ability to accuratelyquantify the amount of amelogenin bound to thematerial surface. Although each of the bone graftswas able to adsorb either EMD liquid or EMD gel tothe surface of the bone grafting material, the no-ticeable difference was evident after rinsing with PBSat neutral pH. Because this solution is used in vitro torepresent physiologic pH, the finding that a simplerinse was able to wash >50% of amelogenin bound tothe surface of grafting materials coated with EMD gelwas quite surprising (Fig. 6). Although it is verydifficult to speculate what effect this might have ina clinical setting, the finding that such a large per-centage of protein is flushed so easily raises theclinical concern that after the placement of EMD gel +bone graft in a bone defect, a similar effect might beimagined whereby bodily fluids are able to dissociatethe adsorbed enamel matrix proteins from the scaf-fold surface. Noteworthy also is the fact that bone ap-position should be directly adjacent to the bone graftingmaterial surface. In the present study, it is found that
Figure 3.SEM and TEM images of DFDBA after coating with either EMD liquid or EMD gel. A) SEM imageof DFDBA particles coated with EMD liquid demonstrates its smooth surface properties with littleaccumulation of a thick surface coatingwith amelogenin proteins. The results fromTEM further confirmedthat most of the staining was present on the surface or slightly penetrated within the surface of thegrafting material (C, arrows). B) In contrast, DFDBA particles coated with EMD gel demonstrated thepresence of a much thicker coating caused by its PGA carrier. The surface coating with an anti-EMDantibody also revealed the presence of most of its coating far from the surface of grafting particles(D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
583
DISCUSSION

• これとは対照的に、EMD gelにはCaPの表面を貫通する能力がないことが観察された。
• 移植材の中にタンパクを吸着することができる穴が表面に無いため、タンパクの吸着は材料表面だけに限られ、生体活性分子を大量に運ぶキャリアとしての能力に欠けている。
the use of EMD gel provided a much thicker surfacecoating, one that extends several micrometers, asviewed by SEM and TEM images. Although in someclinical studies the use of EMD gel has demonstratedpositive outcomes when combined with bone graftingmaterials, the present findings provide conclusiveevidence that a large variability exists betweenamelogenin adsorption to the various bone grafting
materials used in reconstructiveperiodontal surgery. Moreover,the present data provide therationale for the development ofan optimized delivery systemusing a liquid solution of EMDfor future combination with bonegrafting materials.
CONCLUSIONS
The results from the presentstudy demonstrate that surfacecoatings with enamel matrixproteins vary depending onthe coating of bone graftingmaterials with either EMD liquidor EMD gel. Surface coatingwith EMD gel increased drasti-cally the thickness of coating ofenamel matrix proteins to bonegrafting surfaces, which wereeasily dissolved after a simplePBS rinse. The use of EMD ina liquid formulation was able toprovide better surface coatingdirectly adjacent to scaffoldsurface, whereas protein adsorp-tion was also observed within theinterior of the bone grafting par-ticles when coated on NBM andDFDBA. When bone grafts werecoated with EMD in a liquid for-mulation, they demonstratedbetter long-term delivery ofenamel matrix proteins duringa 10-day period compared toEMD in a gel formulation. Thus,the liquid formulation of EMDallows for the following: 1) in-creased and more completesurface loading of porous graftmaterials; and 2) tighter andmore stable surface coating withenamel matrix proteins.
ACKNOWLEDGMENTS
The authors gratefully acknowl-edge the Robert K. Schenk Lab-
oratory of Oral Histology, Dental School at theUniversity of Bern, most notably Thuy Tran Nguyen,Monika Aeberhard, and David Reist for their consid-erable time and valuable insights into the histologicperformance of experiments. This work was fundedby the Department of Periodontology at the Univer-sity of Bern and Institute Straumann, for whichDrs. Tugulu, Gemperli, and Dard are employees.
Figure 4.SEM and TEM images of CaP bone grafting after coating with either EMD liquid or EMD gel. A) SEMimage of CaP particles coated with EMD liquid demonstrates accumulation of EMD on the surface ofgrafting particles. The results from TEM further confirmed that most of the staining was present at a slightdistance from the surface, with no presence of penetration within the bone grafting scaffold (C, arrows).B)Similarly, CaP particles coated with EMD gel demonstrated the presence of a thicker coating caused by itsPGA carrier. The surface coating with an anti-EMD antibody also revealed the presence of its coating ata distance from the surface of grafting particles (D, arrows). (A) and B) ·1,600; scale bars = 20 mm.)
Figure 5.A) Quantitative analysis of the number of gold-labeled particles that appear from TEM images revealeda slight increase in number on grafting particles coated with EMD liquid and EMD gel. B) The particleswere then quantified for their average distance from the scaffold surface, and results demonstrate a muchcloser binding affinity to scaffolds when grafts were coated with EMD liquid instead of EMD gel. * denotessignificant differences of P <0.05.
Enamel Matrix Derivative Adsorption to Bone Grafts Volume 86 • Number 4
584
DISCUSSION

• SEMとTEMにより定量分析を行うことができるが、ELISAを用いることにより材料表面のアメロジェニンの量をより正確に測定することができる。
• どの骨移植材もEMD liquidまたはEMD gelを表面に吸着することができるが、中性のPBSによる洗浄後顕著な違いが現れた。
• この溶液はin vitroで生理的pHを再現するために用いられるため、EMD gelによりコーティングされた移植材表面のアメロジェニンを簡単な洗浄で50%以上洗い流すという所見は非常に驚くべきものである(Fig. 6)。
Dr. Sculean has received lecture fees from InstituteStraumann. Institute Straumannmanufactured the bonegraft, EMD, and EMD gel used in this study. Drs. Miron,Bosshardt, Buser, Zhang, Caluseru, and Chandad re-port no conflicts of interest related to this study.
REFERENCES1. Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized
ridge augmentation using guided bone regeneration. 1.Surgical procedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13:29-45.
2. Jung RE, Fenner N, Hammerle CH, Zitzmann NU. Long-term outcome of implants placed with guided boneregeneration (GBR)using resorbable andnon-resorbablemembranes after 12-14 years. Clin Oral Implants Res2013;24:1065-1073.
3. Lorenzoni M, Pertl C, Keil C, Wegscheider WA. Treat-ment of peri-implant defects with guided bone regener-ation:A comparative clinical studywith variousmembranesand bone grafts. Int J Oral Maxillofac Implants 1998;13:639-646.
4. Wiltfang J, Schultze-Mosgau S, Merten HA, Kessler P,LudwigA,EngelkeW.Endoscopic andultrasonographicevaluation of the maxillary sinus after combined sinusfloor augmentation and implant insertion.Oral SurgOralMed Oral Pathol Oral Radiol Endod 2000;89:288-291.
5. Calori GM,Mazza E, ColomboM, Ripamonti C. The use ofbone-graft substitutes in large bone defects: Any specificneeds? Injury 2011;42(Suppl. 2):S56-S63.
6. Dragoo MR, Sullivan HC. Aclinical and histological evalu-ation of autogenous iliac bonegrafts in humans. I. Woundhealing 2 to 8 months. J Peri-odontol 1973;44:599-613.
7. Gross JS. Bone grafting mate-rials for dental applications: Apractical guide. Compend Con-tin Educ Dent 1997;18:1013-1018,1020-1022,1024,passim;quiz.
8. Hiatt WH, Schallhorn RG,Aaronian AJ. The induction ofnew bone and cementum for-mation. IV. Microscopic exam-ination of the periodontiumfollowing human bone andmarrow allograft, autograftand nongraft periodontal re-generative procedures. J Peri-odontol 1978;49:495-512.
9. Misch CE, Dietsh F. Bone-grafting materials in implantdentistry. Implant Dent1993;2:158-167.
10. Froum SJ, Wallace SS, ChoSC, Elian N, Tarnow DP. His-tomorphometric comparison ofa biphasic bone ceramic toanorganic bovine bone for si-nus augmentation: 6- to 8-month postsurgical assessmentof vital bone formation. A pilotstudy. Int J Periodontics Restor-ative Dent 2008;28:273-281.
11. Schwartz Z, Weesner T, van Dijk S, et al. Ability ofdeproteinized cancellous bovine bone to induce newboneformation. J Periodontol 2000;71:1258-1269.
12. Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- andgene-based therapeutic strategies for periodontal regen-erative medicine. J Periodontol 2011;82:1223-1237.
13. Jepsen S, Heinz B, Jepsen K, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal Class II furcation in-volvement in mandibular molars. Part I: Study designand results for primary outcomes. J Periodontol 2004;75:1150-1160.
14. Meyle J, Gonzales JR, Bodeker RH, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal class II furcation in-volvement in mandibular molars. Part II: Secondaryoutcomes. J Periodontol 2004;75:1188-1195.
15. Modica F, Del Pizzo M, Roccuzzo M, Romagnoli R.Coronally advanced flap for the treatment of buccalgingival recessions with and without enamel matrixderivative. A split-mouth study. J Periodontol 2000;71:1693-1698.
16. Nemcovsky CE, Artzi Z, Tal H, Kozlovsky A, Moses O.A multicenter comparative study of two root coverageprocedures: Coronally advanced flap with addition ofenamel matrix proteins and subpedicle connectivetissue graft. J Periodontol 2004;75:600-607.
17. Sculean A, Donos N, Windisch P, et al. Healing ofhuman intrabony defects following treatment withenamel matrix proteins or guided tissue regeneration.J Periodontal Res 1999;34:310-322.
Figure 6.A)Quantitative analysis by ELISA to determine the quantity of adsorbed amelogenin proteins demonstratesa slight, non-significantpreference for grafting particles coatedwith EMD liquid.BthroughD) Interestingly,the surfaces coated with EMD gel demonstrated a much faster release profile of amelogeninproteins with time, demonstrating a more preferential binding of amelogenin to bone grafting particleswhen particles were coated with EMD liquid compared to EMD gel.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
585
DISCUSSION

• これが臨床においてどんな効果を持っているのかを推測するのは非常に難しいが、このように大きな割合のタンパクが簡単に流されてしまうという所見から、骨欠損へのEMD gelと骨移植材の設置後、体液が移植材表面から吸着したエナメルマトリックスタンパクを引き離すということが想像される。
• 骨添加は直接骨移植材表面から起こるという事実は注目に値する。
Dr. Sculean has received lecture fees from InstituteStraumann. Institute Straumannmanufactured the bonegraft, EMD, and EMD gel used in this study. Drs. Miron,Bosshardt, Buser, Zhang, Caluseru, and Chandad re-port no conflicts of interest related to this study.
REFERENCES1. Buser D, Dula K, Belser U, Hirt HP, Berthold H. Localized
ridge augmentation using guided bone regeneration. 1.Surgical procedure in the maxilla. Int J PeriodonticsRestorative Dent 1993;13:29-45.
2. Jung RE, Fenner N, Hammerle CH, Zitzmann NU. Long-term outcome of implants placed with guided boneregeneration (GBR)using resorbable andnon-resorbablemembranes after 12-14 years. Clin Oral Implants Res2013;24:1065-1073.
3. Lorenzoni M, Pertl C, Keil C, Wegscheider WA. Treat-ment of peri-implant defects with guided bone regener-ation:A comparative clinical studywith variousmembranesand bone grafts. Int J Oral Maxillofac Implants 1998;13:639-646.
4. Wiltfang J, Schultze-Mosgau S, Merten HA, Kessler P,LudwigA,EngelkeW.Endoscopic andultrasonographicevaluation of the maxillary sinus after combined sinusfloor augmentation and implant insertion.Oral SurgOralMed Oral Pathol Oral Radiol Endod 2000;89:288-291.
5. Calori GM,Mazza E, ColomboM, Ripamonti C. The use ofbone-graft substitutes in large bone defects: Any specificneeds? Injury 2011;42(Suppl. 2):S56-S63.
6. Dragoo MR, Sullivan HC. Aclinical and histological evalu-ation of autogenous iliac bonegrafts in humans. I. Woundhealing 2 to 8 months. J Peri-odontol 1973;44:599-613.
7. Gross JS. Bone grafting mate-rials for dental applications: Apractical guide. Compend Con-tin Educ Dent 1997;18:1013-1018,1020-1022,1024,passim;quiz.
8. Hiatt WH, Schallhorn RG,Aaronian AJ. The induction ofnew bone and cementum for-mation. IV. Microscopic exam-ination of the periodontiumfollowing human bone andmarrow allograft, autograftand nongraft periodontal re-generative procedures. J Peri-odontol 1978;49:495-512.
9. Misch CE, Dietsh F. Bone-grafting materials in implantdentistry. Implant Dent1993;2:158-167.
10. Froum SJ, Wallace SS, ChoSC, Elian N, Tarnow DP. His-tomorphometric comparison ofa biphasic bone ceramic toanorganic bovine bone for si-nus augmentation: 6- to 8-month postsurgical assessmentof vital bone formation. A pilotstudy. Int J Periodontics Restor-ative Dent 2008;28:273-281.
11. Schwartz Z, Weesner T, van Dijk S, et al. Ability ofdeproteinized cancellous bovine bone to induce newboneformation. J Periodontol 2000;71:1258-1269.
12. Rios HF, Lin Z, Oh B, Park CH, Giannobile WV. Cell- andgene-based therapeutic strategies for periodontal regen-erative medicine. J Periodontol 2011;82:1223-1237.
13. Jepsen S, Heinz B, Jepsen K, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal Class II furcation in-volvement in mandibular molars. Part I: Study designand results for primary outcomes. J Periodontol 2004;75:1150-1160.
14. Meyle J, Gonzales JR, Bodeker RH, et al. A randomizedclinical trial comparing enamel matrix derivative andmembrane treatment of buccal class II furcation in-volvement in mandibular molars. Part II: Secondaryoutcomes. J Periodontol 2004;75:1188-1195.
15. Modica F, Del Pizzo M, Roccuzzo M, Romagnoli R.Coronally advanced flap for the treatment of buccalgingival recessions with and without enamel matrixderivative. A split-mouth study. J Periodontol 2000;71:1693-1698.
16. Nemcovsky CE, Artzi Z, Tal H, Kozlovsky A, Moses O.A multicenter comparative study of two root coverageprocedures: Coronally advanced flap with addition ofenamel matrix proteins and subpedicle connectivetissue graft. J Periodontol 2004;75:600-607.
17. Sculean A, Donos N, Windisch P, et al. Healing ofhuman intrabony defects following treatment withenamel matrix proteins or guided tissue regeneration.J Periodontal Res 1999;34:310-322.
Figure 6.A)Quantitative analysis by ELISA to determine the quantity of adsorbed amelogenin proteins demonstratesa slight, non-significantpreference for grafting particles coatedwith EMD liquid.BthroughD) Interestingly,the surfaces coated with EMD gel demonstrated a much faster release profile of amelogeninproteins with time, demonstrating a more preferential binding of amelogenin to bone grafting particleswhen particles were coated with EMD liquid compared to EMD gel.
J Periodontol • April 2015 Miron, Bosshardt, Buser, et al.
585
DISCUSSION

DISCUSSION• 今回の研究ではSEMとTEM画像から、EMD gelの使用によりはるかに厚いコーティングが得られるがわかった。
• いくつかの臨床研究ではEMD gelの使用と骨移植材の併用により良い結果が得られたが、今回の所見から歯周外科において用いられる様々な骨移植材に対するアメロジェニンの吸着には大きなばらつきがあるという決定的な証拠が得られた。
• さらに今回のデータは、骨移植材とEMD liquidを併用した最適化されたdelivery systemの発展のための原理を提供する。

CONCLUSIONS
CONCLUSIONS• 本研究の結果により、エナメルマトリックスタンパクによるコーティングはEMD liquidまたはEMD gelによる骨移植材のコーティングにより多様性があることが示された。
• EMD gelによる表面のコーティングによりエナメルマトリックスタンパクの厚みが著しく増加し、それはPBSによる洗浄後簡単に溶かされた。
• EMD liquidの使用により移植材表面を直接コーティングすることができ、NBMとDFDBAにおいては移植材内部までタンパクの吸着が観察された。
• 骨移植材がEMD liquidによりコーティングされた場合、EMD gelに比べて10日の期間中エナメルマトリックスタンパクの長期にわたるより良い供給を示した。
• このようにEMD liquidには以下の様な利点がある:1) 多孔性移植材の表面により大量により完璧な吸着が得られる;2) エナメルマトリックスタンパクによるより強固でより安定したコーティングが得られる

COMMENTSEMD gel群は100 mg/mL の濃度に希釈、骨移植材にコーティングするため4℃で一晩放置された。(本文)
• 実際の臨床では、EMD gelを骨移植材と混ぜてからほとんど時間を置かず移植するため、今回の実験結果よりもさらにエナメルマトリックスタンパクが吸着しにくく、流されやすいことが予想される。

COMMENTSEMD gelによる表面のコーティングによりエナメルマトリックスタンパクの厚みが著しく増加し、それはPBSによる洗浄後簡単に溶かされた。
骨移植材がEMD liquidによりコーティングされた場合、EMD gelに比べて10日の期間中エナメルマトリックスタンパクの長期にわたるより良い供給を示した。(本文)
• エナメルマトリックスタンパクの吸着が実際に歯周組織再生に影響を与えるのか、臨床試験の結果を見てみたい。




![Sensitivity analyses of turbulence ... - ife.uni-hannover.de fileFigure 3: Example correlation matrix (Cn = 1.0e-7 [m-1/3], wind velocity = 4.0 [m/s]) Figure 4: Partial derivative](https://img.pdfslide.tips/doc/110x75/5d542d9d88c99355178b9656/sensitivity-analyses-of-turbulence-ifeuni-3-example-correlation-matrix.jpg)
























