Embed Size (px)
Citation preview

Diving accidentDiving accident
นตนต. . คมสนั วฒุิประเสริฐ รนคมสนั วฒุิประเสริฐ รน..
กองเวชศาสตร์ใต้นำำาและการบิน กองเวชศาสตร์ใต้นำำาและการบิน กรมแพทย์ทหารเรือกรมแพทย์ทหารเรือ

Classification of Diving InjuriesClassification of Diving Injuries
Increase in atmospheric pressure (during Increase in atmospheric pressure (during descent)descent)
Middle ear/ sinus barortauma of descent.Middle ear/ sinus barortauma of descent.barotrauma to inner ear.barotrauma to inner ear.
At depthAt depthSalt water aspirationSalt water aspirationNitrogen NarcosisNitrogen NarcosisUnconsciousnessUnconsciousness

Classification of DivingClassification of Diving InjuriesInjuries
Decrease in atmospheric pressure (during Decrease in atmospheric pressure (during ascent)ascent)
barotrauma of ascentbarotrauma of ascentDecompression illnessDecompression illnessArterial EmbolismArterial Embolism
On surfaceOn surfaceSalt water aspirationSalt water aspirationDrowningDrowningPhysical injury (environment/water craft)Physical injury (environment/water craft)

BarotraumaBarotrauma
Middle & inner ear barotraumaMiddle & inner ear barotrauma Sinus barotraumaSinus barotrauma Pulmonary barotraumaPulmonary barotrauma Equipment BarotraumaEquipment Barotrauma
““mask squeeze”/ facial barotraumamask squeeze”/ facial barotrauma
“ “suit squeeze”/ skin barotraumasuit squeeze”/ skin barotrauma Dental BarotraumaDental Barotrauma

Boyle’s lawBoyle’s law
- If the temperature remain constant , - If the temperature remain constant , the volume of the given mass of gas is the volume of the given mass of gas is inversely proportional to the absolute pressureinversely proportional to the absolute pressure
PP11VV11 = P = P22VV22

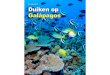
Boyle’s LawBoyle’s Law
If mass and temperature remain constant, the volume of a If mass and temperature remain constant, the volume of a given mass of gas is inversely proportional to the absolute given mass of gas is inversely proportional to the absolute
pressurepressure
PP11VV11 = P = P22VV22
Surface
10 m10 m
20 m20 m
30 m30 m
2 ATA2 ATA
3 ATA3 ATA
4 ATA4 ATA
1 ATA
1/21/2
1/31/3
1/41/4
6 L
3 L3 L
2 L2 L
1.5 L1.5 L 3 L3 L
6 L6 L
4 L4 L
{12 L}

Middle ear barotrauma



Middle Ear Barotrauma of Middle Ear Barotrauma of DescentDescent
Causes of Blockage of Eustachian TubeCauses of Blockage of Eustachian Tube URI and allergies (anything that can cause URI and allergies (anything that can cause
mucosal congestion)mucosal congestion) alcohol ingestionalcohol ingestion cigarette smokingcigarette smoking mucosal polypsmucosal polyps head down positionhead down position

Middle Ear Barotrauma of Middle Ear Barotrauma of DescentDescent
ManagementManagement Stop Diving Stop Diving (( temporary ) temporary ) avoid Valsalva manoeuvre/ strainingavoid Valsalva manoeuvre/ straining decongestantsdecongestants serial audiometry (compare to last medical)serial audiometry (compare to last medical) advice on ear clearing techniquesadvice on ear clearing techniques preventionprevention

Middle Ear Barotrauma of Middle Ear Barotrauma of AscentAscent
less common - usually equalises passivelyless common - usually equalises passively damage from distension by enclosed gases damage from distension by enclosed gases
within the middle ear that continues to expand within the middle ear that continues to expand with ascentwith ascent
more serious as it restricts more serious as it restricts ASCENTASCENT discomfort to pain discomfort to pain alternobaric vertigoalternobaric vertigo avoid decongestants, diving with a coldavoid decongestants, diving with a cold


Grade 0 - Symptoms without signs Grade 1 - Injection of the TM (especially along the handle of the malleus)

Grade 2 - Injection plus slight haemorrhage within TM
Grade 3 - Gross haemorrhage within the TM

Grade 4 - Free blood in the middle earGrade 5 - Perforation/Rupture of the TM

Inner Ear BarotraumaInner Ear Barotrauma(Perilymph Fistula)(Perilymph Fistula)

Inner Ear BarotraumaInner Ear Barotrauma
Symptoms and SignsSymptoms and Signs1.1. TinnitusTinnitus
2.2. High frequency hearing lossHigh frequency hearing loss
3.3. Vestibular disturbanceVestibular disturbance nausea, vomiting, vertigo, ataxianausea, vomiting, vertigo, ataxia
Sensation of blockage in affected earSensation of blockage in affected ear +/- features of middle ear barotrauma+/- features of middle ear barotrauma

Inner Ear BarotraumaInner Ear BarotraumaManagementManagement Avoid increase in CSF pressureAvoid increase in CSF pressure
Immediate bed rest with head elevated 30Immediate bed rest with head elevated 30°°
Consider operative interventionConsider operative intervention
avoid diving and flyingavoid diving and flying

Sinus BarotraumaSinus Barotrauma

Sinus BarotraumaSinus Barotrauma
pain over sinus during descentpain over sinus during descent may continue as dull persistent ache for may continue as dull persistent ache for
several hoursseveral hours usually frontal, less frequently retro-orbital,usually frontal, less frequently retro-orbital,
maxillary pain uncommon but may refer to maxillary pain uncommon but may refer to upper teethupper teeth
numbness over maxillary division of the numbness over maxillary division of the trigeminal nerve is possibletrigeminal nerve is possible
Symptoms and Signs:

Sinus BarotraumaSinus Barotrauma
PreventionPrevention refrain from diving with URTI/sinus infectionsrefrain from diving with URTI/sinus infections discourage use of decongestants while divingdiscourage use of decongestants while diving appropriate treatment of allergic rhinitis with appropriate treatment of allergic rhinitis with
topical steroidstopical steroids cease smokingcease smoking

Sinus BarotraumaSinus Barotrauma
ManagementManagement decongestantsdecongestants analgesicsanalgesics antibioticsantibiotics stop diving and flying until resolvedstop diving and flying until resolved

mask squeeze/ facial barotraumamask squeeze/ facial barotrauma

Facial Barotrauma of DescentFacial Barotrauma of Descent
puffy, oedematous facial tissue, especially under puffy, oedematous facial tissue, especially under the eyesthe eyes
purpuric haemorrhagespurpuric haemorrhages conjunctival haemorrhagesconjunctival haemorrhages generalised bruising of skin underlying the maskgeneralised bruising of skin underlying the mask


Pulmonary barotraumaPulmonary barotrauma

Pulmonary Barotrauma of AscentPulmonary Barotrauma of Ascent
burst lung or pulmonary overinflation syndromeburst lung or pulmonary overinflation syndrome
result of overdistension and rupture of the lungs result of overdistension and rupture of the lungs by expanding gases during ascentby expanding gases during ascent

Pulmonary Barotrauma of AscentPulmonary Barotrauma of Ascent
Precipitating factorsPrecipitating factors inadequate exhalationinadequate exhalation caused by panic, faulty caused by panic, faulty
apparatus, inexperienceapparatus, inexperience
Predisposing factorsPredisposing factors asthmaasthma, intrapulmonary fibrosis, cysts, infection, , intrapulmonary fibrosis, cysts, infection,
pleural adhesions, sarcoidosis, pleural adhesions, sarcoidosis, previous previous pneumothoraxpneumothorax


Decompression sickness.Decompression sickness.
The liberation of gas bubbles from solution, into tissues or blood, in an individual exposed to a reduction of environmental pressure.

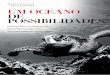
Henry’s lawHenry’s law
- At a constant temperature - At a constant temperature
the amount of a gas that will dissolve in a liquid the amount of a gas that will dissolve in a liquid is proportion to the partial pressure of the gas is proportion to the partial pressure of the gas over the liquidover the liquid

1 atm 2 atm 3 atm

PathologyPathology
-BubbleBubble form first inform first in tissuetissue and thenand then inin venous bloodvenous blood
--TheThe lunglung are usually an effective filterare usually an effective filter for bubblefor bubble ( ( pulmonary arteriolespulmonary arterioles ) )

PathologyPathology
--The ability of lung to filter the bubbleThe ability of lung to filter the bubble which thenwhich then resolve by gas resolve by gas diffusion todiffusion to the alveolithe alveoli
--Bubble can also be bypassed through Bubble can also be bypassed through anatomical defectanatomical defect patent foramenpatent foramen ovale ( PFO)ovale ( PFO)

Effects of Tissue BubblesEffects of Tissue Bubbles..
Obstruction of vascular flow Obstruction of vascular flow
External compression to vascular , nerveExternal compression to vascular , nerve
lymphatics and sensory cell lymphatics and sensory cell
Mechanical damage to tissues and Mechanical damage to tissues and structuresstructures
Activation of inflammatory responseActivation of inflammatory response..

Extravasations of fluid
Increased hemoglobin concentration
Progressive worsening of blood flow

Decompression sicknessDecompression sickness
Type 1Type 1 - - limb or joint pain ( bends )limb or joint pain ( bends ) Type 2Type 2 - - sign or symptom ,cause bysign or symptom ,cause by involvement of CNS , cardiopulmonary systeminvolvement of CNS , cardiopulmonary system Type 3Type 3 - - DCS + AGE DCS + AGE

Traditional Signs & Symptoms.Traditional Signs & Symptoms.
PainPain Pins and needlesPins and needles Paresthesia/ paralysisParesthesia/ paralysis

More commonly experienced More commonly experienced Signs & Symptoms.Signs & Symptoms.
painpainparaesthesiaparaesthesiaheadacheheadachetinglingtinglingdizzinessdizzinessnumbnessnumbnesslethargylethargyNauseaNauseaDifficulty concentratingDifficulty concentratingFatigueFatigue
Difficulty walking Difficulty walking acheache
tiredtiredvisual distvisual distweaknessweaknessvertigovertigochest painchest paindizzydizzyitchingitchinglight headedlight headed

DCS type 1 DCS type 1
Bend
Limb and joint pain only
Skin rash

DCS type 2DCS type 2
- - Cardiopulmonary systemCardiopulmonary system
- “- “chokechoke””
- Nervous systemNervous system
- numbness - numbness
- “- “spinal cord hitspinal cord hit””
- spinal cord DCS - spinal cord DCS

Spinal cord DCSSpinal cord DCS
Venous infarction of cordVenous infarction of cord - Venous gas embolism block the pulmonary arterioles- Venous gas embolism block the pulmonary arterioles - Rise in intra-thoracic pressure- Rise in intra-thoracic pressure ( ( pulmonary hypertensionpulmonary hypertension ) ) - Interferes drainage of venous system - Interferes drainage of venous system ( ( spinovertebral-azygos systemspinovertebral-azygos system ) )
Autochthonous bubbleAutochthonous bubble EmbolismEmbolism - Spinal cord is - Spinal cord is relativelyrelatively poor perfusionpoor perfusion when compare to the when compare to the
brainbrain

First Aid.First Aid.
Remove from waterRemove from waterLie FlatLie Flat100% O2100% O2
oral /IV fluidoral /IV fluidEmergency Service Emergency Service
AmbulanceAmbulanceAir (Helo/ Air Ambulance)Air (Helo/ Air Ambulance)

First Aid.First Aid.

First Aid.First Aid.

First Aid.First Aid.

First Aid.First Aid.

First Aid.First Aid.

First Aid.First Aid.

First Aid.First Aid.

First Aid.First Aid.

Patient Assessment.Patient Assessment.
Dive details.Dive details.
- ascent, at depth and descent.- ascent, at depth and descent.
- contributing factors- contributing factors
- exclusion of alternate potential causes- exclusion of alternate potential causes
- onset of symptoms- onset of symptoms
Physical assessment.Physical assessment.
- neurological assessment- neurological assessment

TreatmentTreatment..
Hyperbaric Oxygen Therapy.Hyperbaric Oxygen Therapy.
Mechanical compression of bubbles.Mechanical compression of bubbles.
Washout of inert gas (N2).Washout of inert gas (N2).
IV fluids.IV fluids.
Rehydration.Rehydration.
IV Lignocaine.IV Lignocaine.
Stabilization of cell membranes.Stabilization of cell membranes.
NSAIDS.NSAIDS.
Combats inflammatory response. Combats inflammatory response.



Decompression IllnessDecompression Illness
PrognosisPrognosis avoid dive - 4 weeksavoid dive - 4 weeks avoid fly 2-4 weeksavoid fly 2-4 weeks Review 4 weeksReview 4 weeks ? Further ? Further
investigationsinvestigations

Flying after divingFlying after diving

New guideline New guideline
> > Flying after a single no-decompression Flying after a single no-decompression
divedive:: A minimum preflight surface interval of A minimum preflight surface interval of 1122 hours is suggested. hours is suggested.

New guidelineNew guideline
> > Flying after multiple no-decompression Flying after multiple no-decompression dives in a single day or multiple days of no-ddives in a single day or multiple days of no-decompression divingecompression diving:: A minimum preflight su A minimum preflight su
rface interval of rface interval of 1818 hours is suggested. hours is suggested.

New guidelineNew guideline
> > Flying after dives requiring Flying after dives requiring decompression stopsdecompression stops:: There is little experimen There is little experimental or published evidence on which to base a rectal or published evidence on which to base a recommendation for decompression dives. A prefliommendation for decompression dives. A prefli
ght surface interval substantially ght surface interval substantially longer thanlonger than 1188 hours appears prudent. hours appears prudent.

cabin altitudes of cabin altitudes of 2,0002,000 to to 8,0008,000 feet for feet for divers who do not have symptoms of decompresdivers who do not have symptoms of decompression sickness (DCS). sion sickness (DCS).

The recommended preflight surface intervals The recommended preflight surface intervals do do not guaranteenot guarantee avoidance of DCS. avoidance of DCS.
Longer surface intervals will reduce DCS Longer surface intervals will reduce DCS risk furtherrisk further. .

Emergency air evacuationEmergency air evacuation
-Aircraft pressurized 1 ATA ( if possible)-Aircraft pressurized 1 ATA ( if possible)-Un-pressurized aircraft-Un-pressurized aircraft - - no more than 1000 feetno more than 1000 feet
-Have the patient breath 100% oxygen -Have the patient breath 100% oxygen during transportduring transport

Emergency air evacuationEmergency air evacuation
Aircraft pressurized 1 ATA ( if possible)Aircraft pressurized 1 ATA ( if possible)
Un-pressurized aircraft Un-pressurized aircraft
- - no more than 1000 feetno more than 1000 feet Have the patient breath 100% oxygen Have the patient breath 100% oxygen
during transportduring transport

THANK YOU