Embed Size (px)
Citation preview
Endocrine emergencies
By Dr. Mohammed Al Ameen
Hypoglycemia
• <60mg/dl, <4mmol/L• Protection against hypoglycemia is
normally provided by cessation of insulin release and mobilization of counter-regulatory hormones
Causes
• Overdose of insulin or oral hypoglycaemic agents
• Alcohol-induced hypoglycaemia• Addison’s disease • Insulinomas. • Liver failure. • Extra-pancreatic tumors.• Pituitary insufficiency.
Signs and symptoms
• Signs and symptoms of hypoglycemia are caused by excessive secretion of epinephrine and CNS dysfunction
• sweating, nervousness, tremor, tachycardia, hunger, and neurologic symptoms ranging from bizarre behavior and confusion to seizures and coma.
• hypoglycemia unawareness.• Somogyi phenomenon
Investigations
• Blood glucose• LFT• Electrolytes• ECG• C-peptide
Management
• C A B• 50% dextrose in water (D50W) is administered
intravenously• Alcohol-thiamine• <8yrs-25% (D25W) or even 10% (D10W) dextrose• Glucagon 1mg • Discharge- cause for the episode and fully recovered
Diabetic Ketoacidosis
• An acute metabolic complication of diabetes characterized by• hyperglycemia• hyperketonemia• metabolic acidosis
Causes
• Infection• Infraction• Insufficient insulin
Symptoms and signs
• Signs of dehydration• GI symptoms• Kussmaul respiration, fruity breath • Neurological symptoms :altered level of conciousness
,confusion, coma and death – if not treated timely
Investigations
• Blood glucose• ABG• Serum ketones• Infective screen• Blood tests— urea and electrolytes, FBC, and
bicarbonate• ECG and cardiac monitoring
Treatment• A B C• Fluid management -resuscitation -replacement • Insuline 0.1 unit/kg/hour, ketones do not fall by at least 0.5
mmol/L/hour the infusion rate should be increased by 1 unit/hour• Change IV solution to D5W when glucose concentration is ≤300
mg/dL• Potassium replacement Over 5.5mmol/l Nil 3.5–5.5mmol/l 20 mmol/LBelow 3.5mmol/l 40–60 mmol/L (HDU support required)
• Sodium, Phosphorus & magnesium• Bicarbonates• Monitoring: Fluid balance should be monitored,
aiming for a urine output > 0.5 ml/kg/hr. Blood ketones and capillary glucose should be measured hourly . ABG every 2 hrs.
Hyperosmolar hyperglycemic nonketotic syndrome
• Pathophysiology: there is enough circulating insulin to prevent ketogenesis , and therefore acidosis
• Clinical features similar to DKA• Investigation: blood glucose >30mmol/l, serum
osmolality• Management: similar to DKA
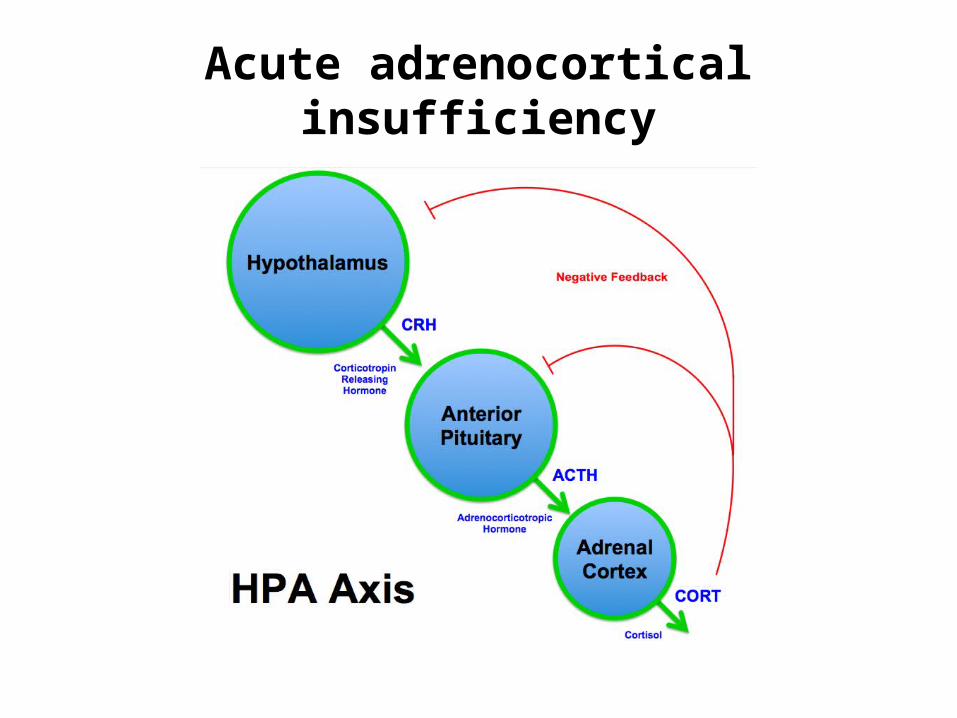
Acute adrenocortical insufficiency
• Precipitants of an adrenal crisis include: Infection.Trauma.Myocardial infarction.Stroke. Asthma.Hypothermia. Alcohol.• Exogenous steroid withdrawal/reduction.
Clinical features
• Onset is usually insidious with features including weight loss, lethargy, weakness, vague abdominal pain, nausea
• Adrenal crisis the patient can be profoundly shocked (tachycardic, hypotensive, vasoconstricted,oligouric) and hypoglycaemic
Investigation
Serum cortisol and plasma ACTHRFT:Hyponatraemia. Hyperkalaemia. Elevated urea and creatinine.Blood glucose: Hypoglycaemia.ABG: Metabolic acidosis.To identify the precipitant : ECG, CT, CBC, blood culture, CXR, urine routine .
Treatment
• A B C• Hydrocortisone 100 mg IV should be given as soon as
an adrenal crisis is suspected.• Fluid resuscitation• Patients should be monitored for hypoglycemia.• Treat the precipitant
Phaeochromocytoma
• functional tumors that arise from chromaffin cells in the adrenal medulla
• Catecholamines α –receptors and β -receptors
Clinical features
• Hypertension.• Palpitations.• Sweating.• Pallor.• Headache.• Anxiety.• Pulmonary oedema.• Nausea and vomiting.• Altered level of consciousness (hypertensive
encephalopathy)
Diagnosis
• 24-hour urinary free catecholamines level• CT/MRI
Treatment
• Phenoxybenzamine ( α -blocker) is the drug of choice.
• Propranolol
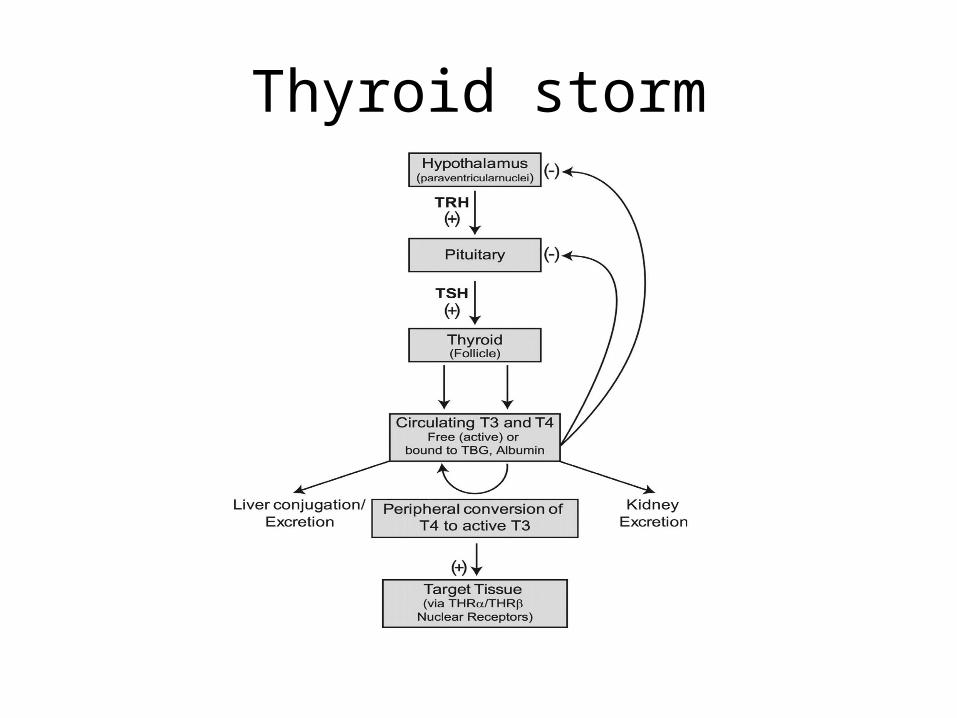
Thyroid storm
Precipitating factors of a thyroid storm
• Infection• Non-thyroidal trauma or surgery• Parturition, pre-eclampsia• Major acute medical conditions,
e.g.myocardial infarction, DKA, HONK,hypoglycaemia.
• Radioiodine or high-doses of iodine-containingcompounds, e.g. contrast media, amiodarone.• Discontinuation of anti-thyroid medication.• Thyroid hormone overdose• Thyroid injury (infarction of an adenoma, neck
trauma)
Clinical Feature
• Cardiovascular — severe tachycardia, atrial fibrillation, congestive heart failure, hypertension.
• Neurological — agitation, confusion, delirium, coma.• Gastrointestinal dysfunction — vomiting, diarrhoea,
acute abdomen.• Fever.
Investigation
• Bloods — renal function, glucose, calcium, FBC, thyroid function tests.
• Infective screen• ECG
Treatment
• Inhibition of thyroid hormone synthesis and release - propylthiouracil and carbimazole
- Iodide• Inhibition of peripheral effects of thyroid hormone
-propranolol 80 mg PO - hydrocortisone 100 mg IV or
dexamethasone 4 mg PO• Treat underlying cause• Supportive management
Myxoedema coma
• Myxoedema coma is a rare condition typically found in elderly patients with undiagnosed or undertreated hypothyroidism.
• Precipitants : infections or infractions • Clinical features :- Altered mental state ranging from
poor cognitive function to coma. -Hypothermia or the absence of fever despite severe infection• Management – Thyroid profile, Thyroid hormones,
Hydrocortisone, Rx precipitant
Thank you