1. NOOR MUHAMMAD WAZIR 08-143 BATCH: I FINAL YEAR MBBS
GYNAE:C
2. ENDOMETRIAL CARCINOMA
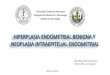
3. ANATOMY OF UTERUS GROSS HISTOLOGIC
4. ENDOMETRIAL HYPERPLASIA A spectrum of proliferative
abnormalities of endometrium are subdivided into: CYSTIC
HYPERPLASIA: increase in the number of glands. ADENOMATOUS
HYPERPLASIA: back to back crowding of glands with little
intervening stroma. ATYPICAL HYPERPLASIA: glands show nuclear
5. CAUSES AND RISK FACTORS OF ENDOMETRIAL CARCINOMA
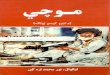
6. EFFECTS OF ESTROGEN ON ENDOMETRIUM
7. M Other causes : Myomas Senile endometritis Dietary
factors
8. PATHOLOGY GROSS FEATURES: DIFFUSE TYPE: Involves most of
endometrium. May reach the myometrium and serous surface. PYOMETRA:
uterus is enlarged due to the formation of pyometra which is formed
following an infection of the tumor with accumulation of pus due to
stenosis of internal cervical os LOCALIZED TYPE: It is limited to
small area where it forms a polypoidal growth. polyp is friable,
ulcerated and necrosed.
9. MICROSCOPIC FEATURES: 1.Adenocarcinoma(ca. arising from
glandular tissue) 2.adenocanthoma. 3.Adenosquamous carcinoma
Histological grading of adenocarcinoma depends upon degre of
differentiation. GRADE 1: 50% non squamous undifferentiated
10. SPREAD DIRECT: Cervical canal: here the tumor may get
infected and blocks the Cervix leading to pyometra formation
Myometrium Ovaries LYMPHATIC SPREAD: inguinal lymph nodes para
aortic lymph nodes. BLOOD BORNE: Lungs, Liver, Bone etc
IMPLANTATION: During hysterectomy malignant cells may get implanted
in the vaginal vault causing recurrence.
11. CLINICAL FEATURES SYMPTOMS BLEEDING: due to ulceration and
sloughing off of the carcinoma. Irregular vaginal bleeding. Post
menopausal bleeding. MENORHAGIA in premenopausal patients. VAGINAL
DISCHARGE: Brownish or blood stained, offensive or purulent due to
pyometra.
12. PAIN: late symptom. Indicates advanced growth with
metastasis. Dull, colicky lower abdominal pain. Occurs due to
strong contractions of uterus to expel the polypoid growth or
pyometra. ASYMPTOMATIC
13. PHYSICAL EXAMINATION Palpation of supraclavicular and groin
nodes. Breast is examined for a co-existent primary or secondary
lesion. Speculum examination: done for metastatic invasion of
vagina.in case of pyometra a pyogenic or blood stained discharge
pours from the cervix.
14. BIMANUAL PELVIC EXAMINATION: To assess the size,consistency
and mobility of uterus. Findings: large size, soft consistency in
case of pyometra Reduced mobility if the tumor has extended
beyond
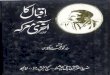
15. CLINICAL STAGING
16. DIAGNOSTIC TECHNIQUES ENDOMETRIAL SAMPLING: Fractional
curettage: The endometrial curetting are bulky and necrotic.
17. HYSTEROSCOP Y: Extent of the disease and site of invasion
can be biopsied easily
18. TRANSVAGINAL ULTRASOUND(TVS): Uterine enlargement Thick
hyper echoic endometrial lining. Loss of subendometrial halo in
case of myometrial
20. TUMOUR MARKERS: CA-125 is a non specific tumor marker.
Patients with clinical stage 4 disease show raised levels. OTHER
TESTS: CBC Blood group Blood sugar level Serum creatinine Urea
Electrolytes ECG
21. GENERAL MEASURES SURGERY SURGERY AND RADIOTHERAPY
CHEMOTHERAPY According to the stage of the disease TREATMENT
22. GENERAL MEASURES General health should be improved LFTs
RFTs Blood glucose
23. STAGE TREATMENT PLAN STAGE 1a grade 1 TAH/BSO OTHER STAGE 1
TAH/BSO,radiotherapy STAGE 2 radical hysterectomy/BSO ,pelvic
lymphadenectomy radiotherapy STAGE 3 Radiotherapy:if only pelvis is
involved Laparotomy;if disease spreads beyond
pelvis(omentectomy,lymphadenecto my) STAGE 4
radiotherapy,chemotherapy,debulki ng surgery,hormonal therapy
24. FIVE YEAR SURVIVAL RATES STAGE RATES 1 82-86% 2 70% 3 40% 4
16-27%
25. SURGICAL OPTIONS
26. RADIOTHERAPY OPTIONS COMBINED WITH SURGERY: Treatment of
choice for stage 1C or stage 2 in which more than half of the
myometrium and cervical glands and stroma are involved.
RADIOTHERAPY ALONE: If the growth is wide spread in the
pelvis(stage 3,4) or if the patient is too weak to undergo surgery.
ROUTES: BRACHYTHERAPY:intracavitary TELETHERAPY:by external
routes
27. CHEMOTHERAPY OPTIONS PROGESTOGEN: For relief of pain in
advanced cases. 2-3 injections are given before or after surgery or
radiotherapy. Minimum duration of treatment is more than 3 months.
PREPARATIONS: Inj.medroxyprogesterone acetate 200 mg im
weekly(depoProvera) Inj.hydroxyprogesterone caproate 250 mg im
weekly(proluton Depot) Tab.norethisterone10 mg tid.(primolute
28. FOLLOW UP TO DETECT THE RECURRENCE: Vaginal recurrence is
common so it should be examined at every visit. TO DETECT
COMPLICATIONS OF THERAPY: Hematuria, Cystitis, Diarrhea, Melena
Rectal spasm, Ilietus, Vaginal stenosis, Lymphedema etc












![Hu-wal-Kazzab - Writer: Maulana Qari Ahmadullah - Afada: Maulana Noor Muhammad Qadri Tonswi [DB]](https://img.pdfslide.tips/doc/110x75/577d229f1a28ab4e1e97daee/hu-wal-kazzab-writer-maulana-qari-ahmadullah-afada-maulana-noor-muhammad.jpg)