Embed Size (px)
Citation preview
Acute PancreatitisKurdistan Board GEH/GIT Surgery J Club
2016Supervised by:
Professor Mohamed Alshekhani
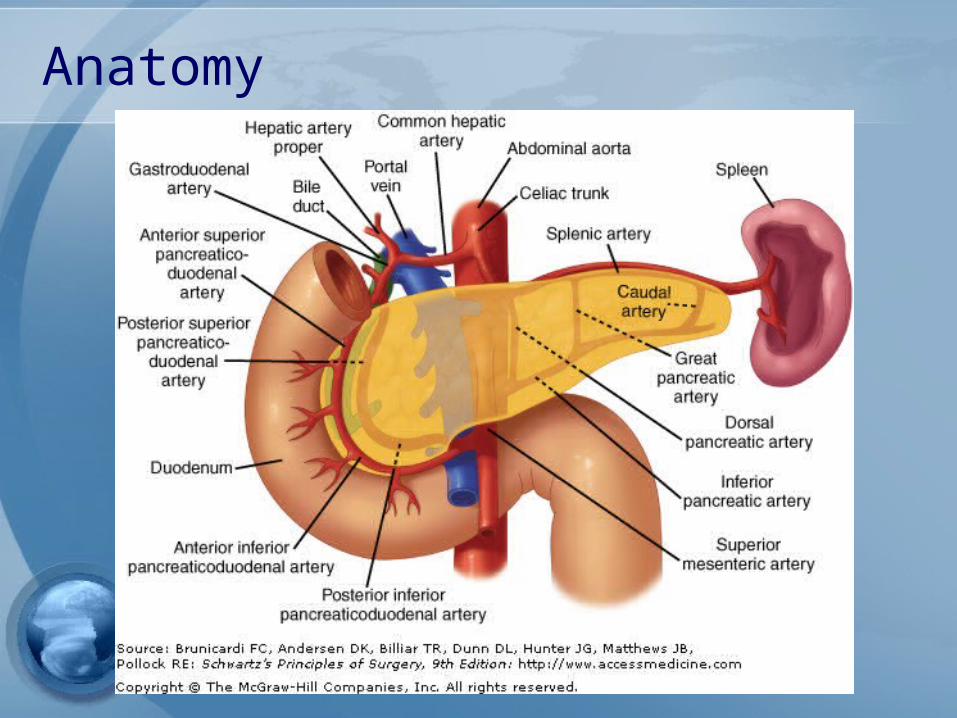
Anatomy
Introduction:
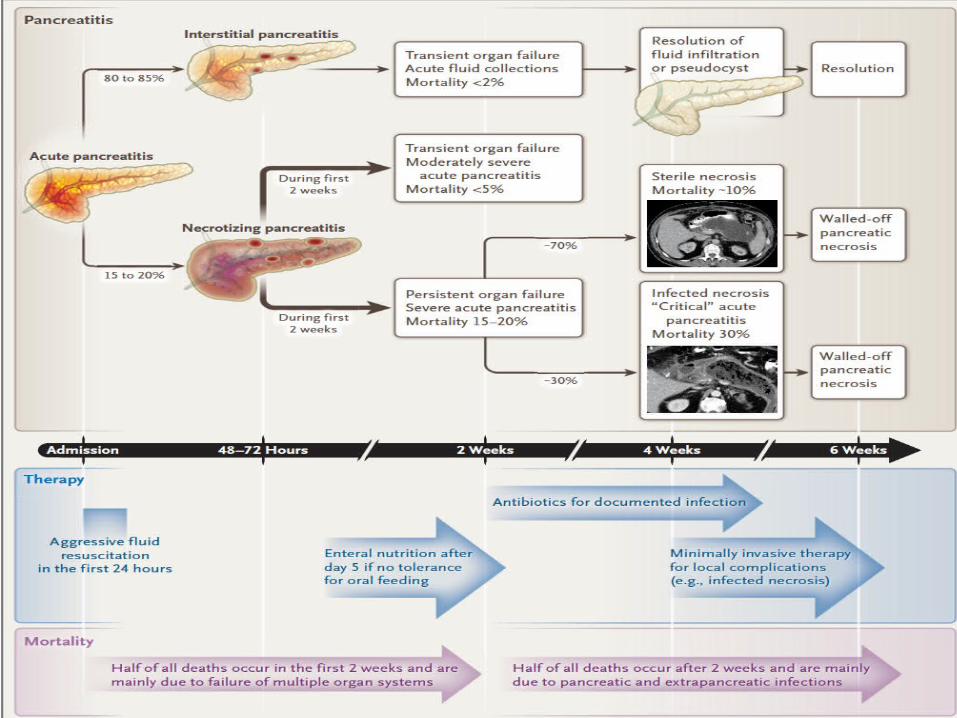
• The incidence is increasing • One of the most common reasons for hospitalization
with a GI condition. • 80% have mild, self-limited disease &discharged with several days.• Mortality has decreased over time&the overall
mortality is 2%.• Death is more likely in certain subgroups ; elderly,
those with more numerous &more severe coexisting conditions (obesity), hospitalacquired infections, severe episodes of acute pancreatitis (persistent failure of one or more organ systems or infected pancreatic necrosis).

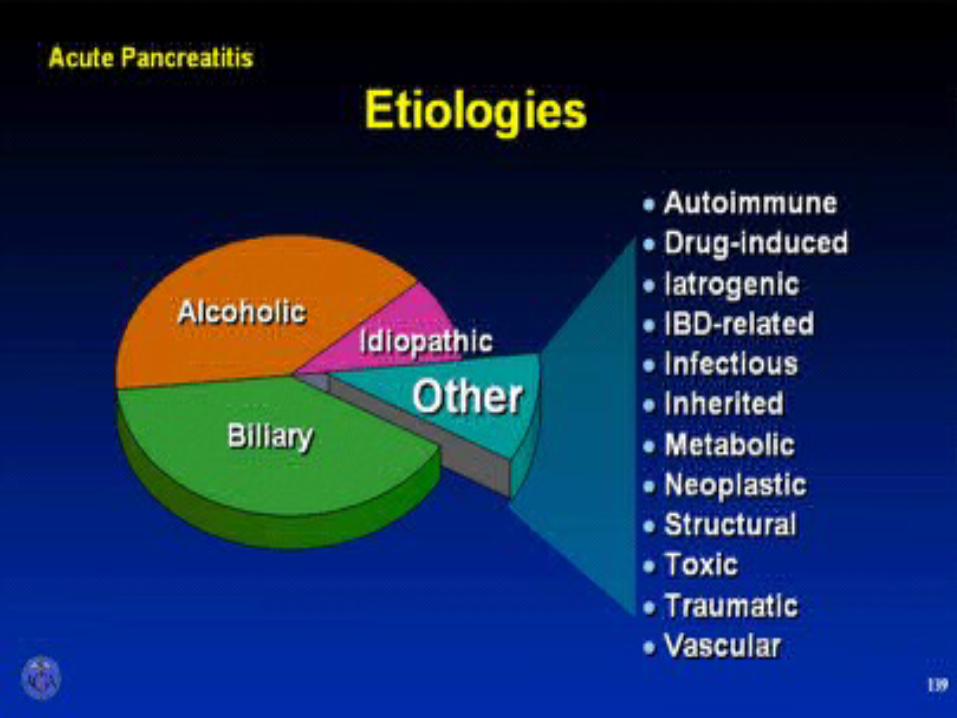
Etiology
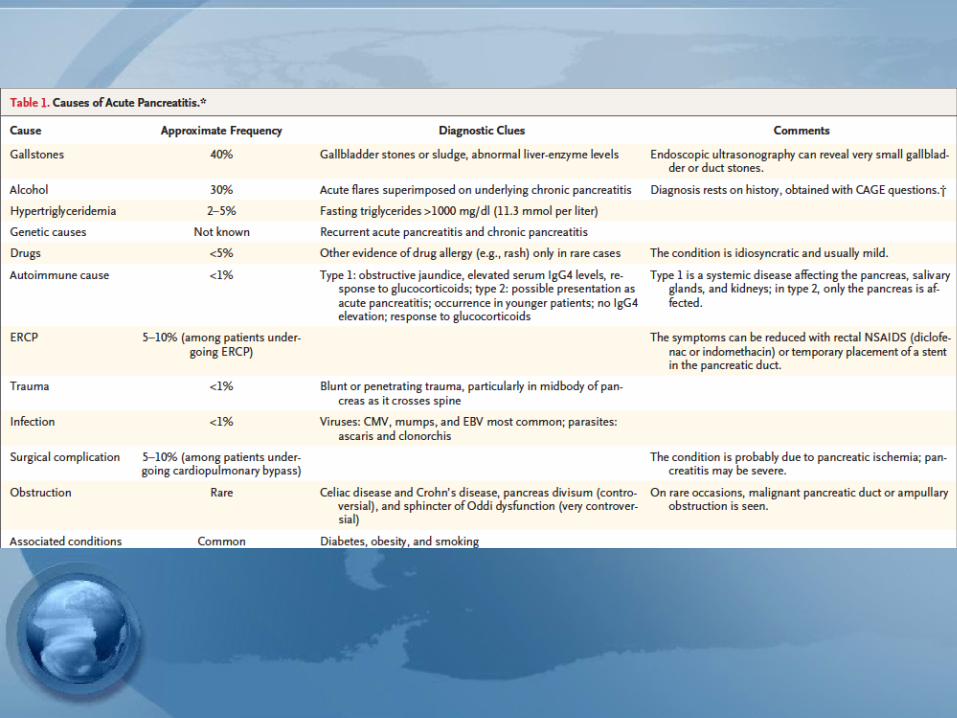
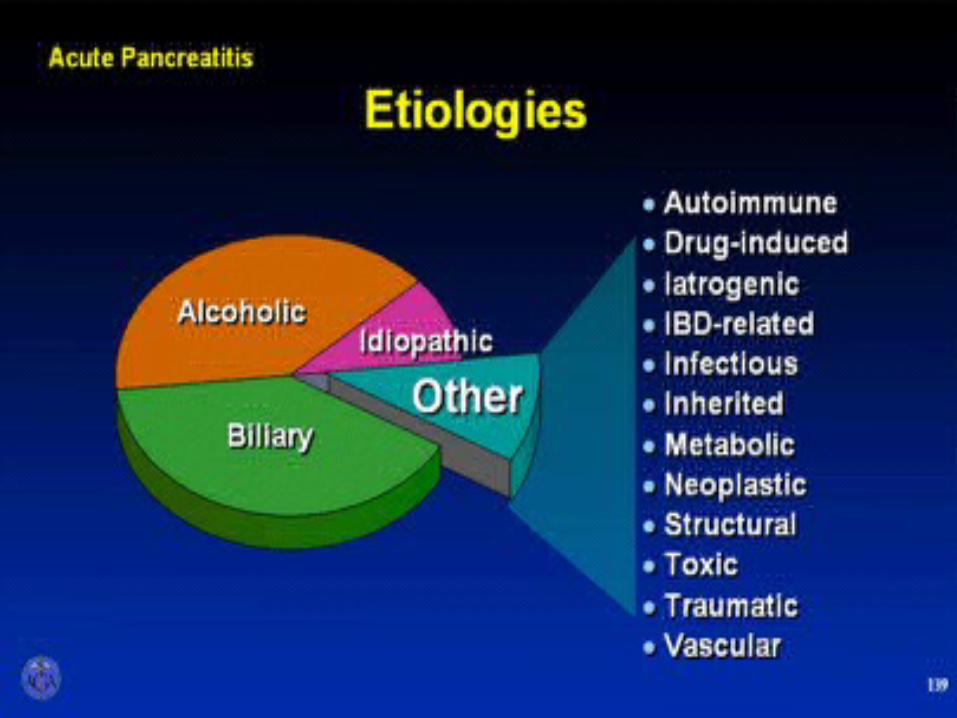
Gallstone pancreatitis:• Most common cause.• Migrating gallstones cause transient obstruction
of the pancreatic duct, a mechanism shared by other recognized causes (e.g., ERCP).
• SOD contributed to post-cholecystectomy biliary pain, but no convincing data that either pancreatic SOD or pancreas divisum plays a role in acute pancreatitis.
Alcoholic pancreatitis• Common in pt. alcohol drinking >
2yr. • Often much longer upto 10 yr.• Sphincter spasm• Decrease pancreatic blood flow
Alcoholic pancreatitis• The second most common cause. • Prolonged alcohol use (four to five drinks daily >5
years) is required for alcohol-associated pancreatitis; • The overall lifetime risk of pancreatitis among heavy
drinkers is 2 - 5%. • In most cases, chronic pancreatitis has already
developed&the acute clinical presentation represents a flare.
• The risk is higher for men than for women.• The mechanisms include both direct toxicity &
immunologic mechanisms.• Binge drinking in the absence of long-term, heavy
alcohol use does not appear to precipitate AP.
AGA Institute
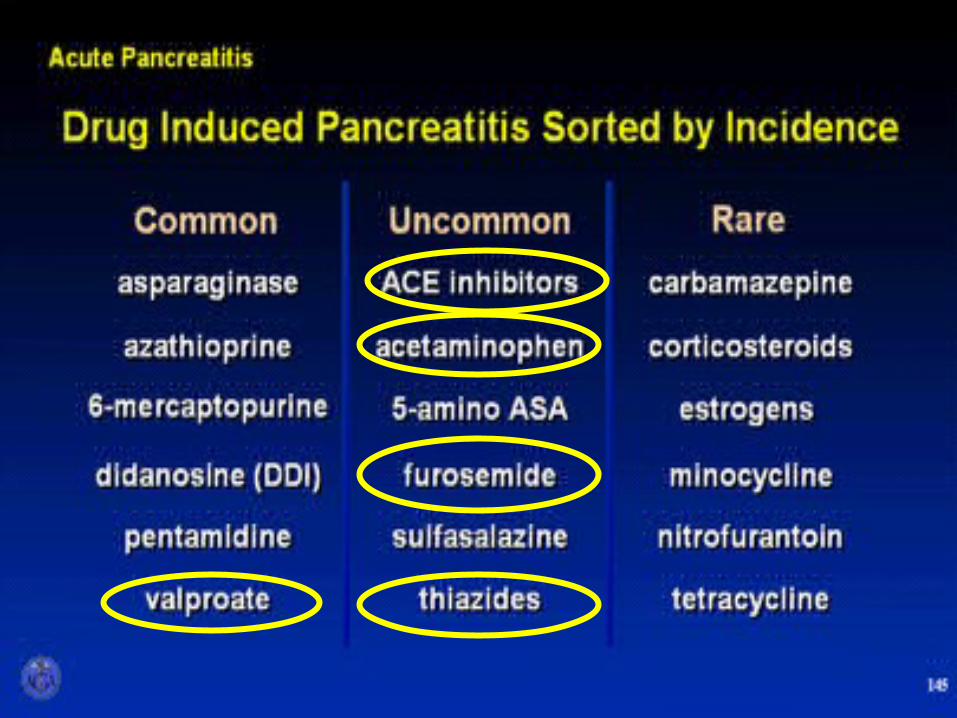
Drugs:• Cause <5% of all cases.• The drugs most strongly associated are
azathioprine, 6-mercaptopurine, didanosine, valproic acid, ACEIs, mesalamine.
• Usually mild. • GLP Not linked.
Genetics:• Genes are associated with acute (and chronic)
pancreatitis, including mutations in the genes encoding cationic trypsinogen (PRSS1 ), serine protease inhibitor Kazal type 1 (SPINK1 ), cystic fibrosis transmembrane conductance regulator (CFTR ), chymotrypsin C, calcium-sensing receptor& claudin-2.
• These mutations may serve as cofactors, interacting with other causes as claudin-2 mutations work synergistically with alcohol.
Obesity/DM:• Morbid obesity is a risk factor for acute
pancreatitis2&severe acute pancreatitis.• Type 2 diabetes increases the risk of acute
pancreatitis by a factor of 2 or 3. • Both obesity & diabetes are also risk factors for
chronic pancreatitis & pancreatic cancer.

Diagnosis
Diagnosis:• At least two of the following three : • Abdominal pain consistent with acute
pancreatitis, • serum lipase or amylase at least 3 times the
upper limit of the normal• Findings of on cross-sectional imaging ( CT or
MRI).
Diagnosis:• Cross-sectional imaging role:• Confirming an initial diagnostic impression.• Assessing patients for mimics.• Evaluating patients with atypical symptoms or
small elevations in serum pancreatic enzyme levels.
Classifications:• Classifications of moderately severe pancreatitis & severe
pancreatitis are defined by the presence of complications that are systemic, local, or both.
• Systemic complications include failure of an organ system (respiratory, cardiovascular, or renal) & exacerbation of a preexisting disorder (e.g.,COPD, HF, or CLD).
• Local complications comprise peripancreatic fluid collections or pseudocysts &pancreatic or peripancreatic necrosis, sterile or infected.
• Persistent organ failure(i.e.>48 hs) is the prime determinant of a poor outcome with mortality 30%.
• Both persistent organ failure & infected pancreatic necrosis is associated with the highest mortality.
Predicting severity:• Clinical factors increasing the risk of complications or
death include:• Advanced age (≥60 years),• Numerous / severe coexisting conditions (obesity
BMI>30 &long-term, heavy alcohol use.• Hemoconcentration&azotemia• Markers of inflammation (e.g., elevated CRP
interleukins 6, 8, 10). • The most useful predictors are elevated BUN
&creatinine &elevated hematocrit, particularly if they do not return to the normal with fluid resuscitation. The degree of elevation of the serum amylase or lipase level has no prognostic value.
Scoring systems:• All have a high false positive rate (i.e., in many patients
with high scores, severe pancreatitis does not develop.• The presence of SIRS is usually obvious.• SIRS can be diagnosed on the basis of four routine
clinical measurements, with findings of two or more of the following values:
• Temperature, <36C or >38 C• Pulse>90 /minute• RR>20 /minute (or Pa CO2, <32 mm Hg).• WBC<4000 or > 12,000. • SIRS that persists for 48 hours or more after the onset
of symptoms is indicative of a poor prognosis.
Scoring systems:• Recent guidelines uses demographic/clinical factors at
admission (advanced age, BMI,coexisting conditions),• Simple labvalues at admission&during the next 24 to
48 hours (hematocrit,>44%; BUN, >20 or creatinine >1.8 &* the presence of SIRS to identify patients who are at greatest risk for severe disease & most likely to benefit from a high-intensity nursing unit.
• During the first 48 to 72 hours, a rising hematocrit or blood urea nitrogen or creatinine level, persistent SIRS after adequate fluid resuscitation, or the presence of pancreatic or peripancreatic necrosis on cross-sectional imaging constitutes evidence of evolving severe pancreatitis
Physical exam
•Grey Turner’s Sign- ecchymosis in 1 or both flanks
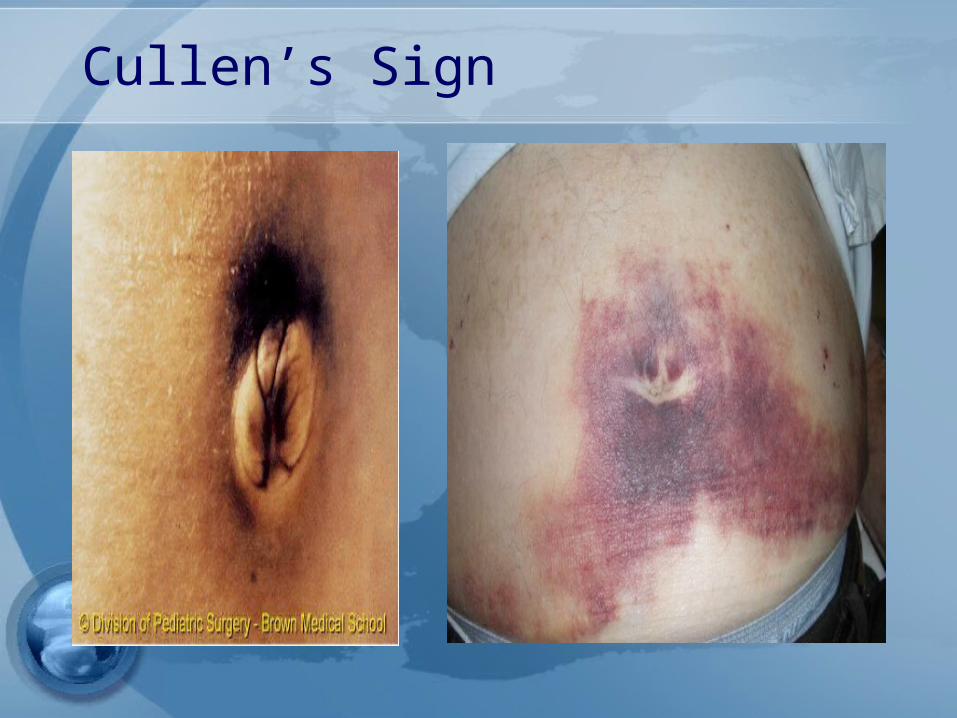
•Cullen’s sign- ecchymosis in periumbilical area
•Associated with Necrotizing pancreatitis• poor prognosis occurs in 1% of cases

Grey Turner’s Sign
Cullen’s Sign

Serum markers
Serum amylase• Elevates within HOURS and can
remain elevated for 3-5 days• High specificity when level >3x
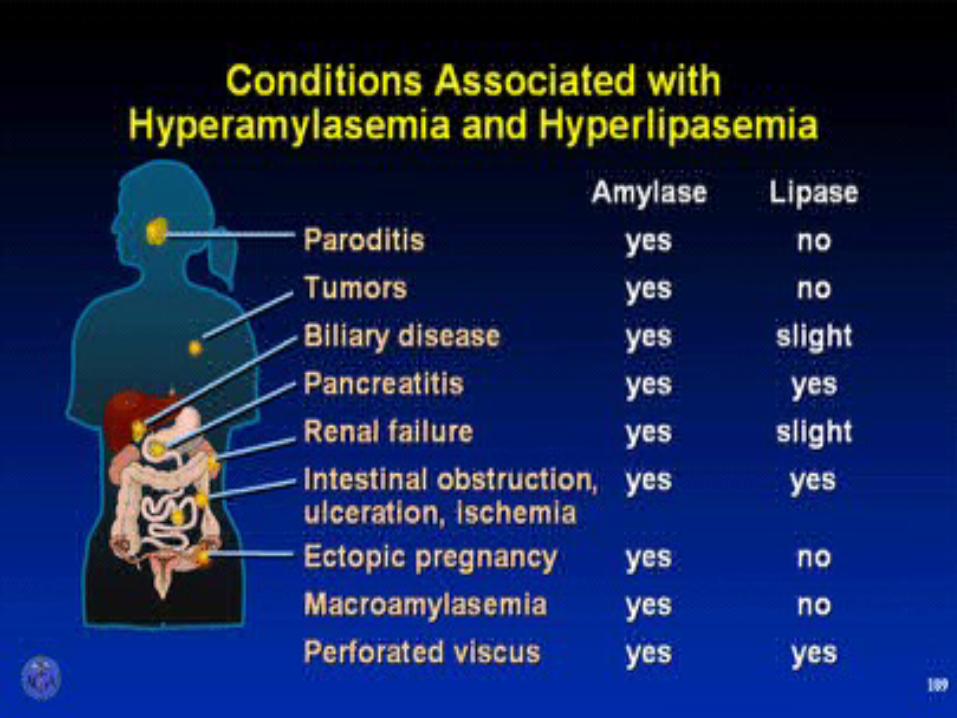
normal• Many false positives (see next
slide)• Most specific = pancreatic
isoamylase (fractionated amylase)
Urine amylase• urinary levels may be more
sensitive than serum levels.
• Urinary amylase levels usually remain elevated for several days after serum levels have returned to normal.
Serum lipase• The preferred test for diagnosis• Begins to increase 4-8H after
onset of symptoms and peaks at 24H
• Remains elevated for days• Sensitivity 86-100% and
Specificity 60-99%• >3X normal S&S ~100%
Slide 189

Plain Abdominal Radiograph
Plain Abdominal Radiograph• Bowel ileus• “Sentinel Loop” • “Colon cut off sign” • Loss of psoas shadow
• Helps exclude other causes of abdominal pain: bowel obstruction and perforation
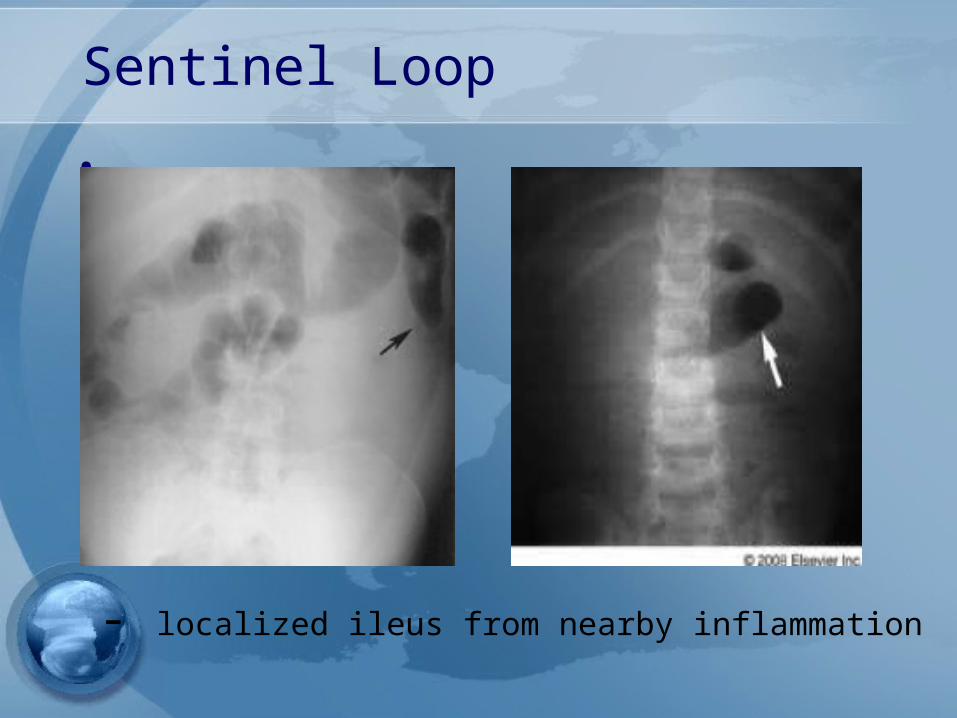
Sentinel Loop•
- localized ileus from nearby inflammation
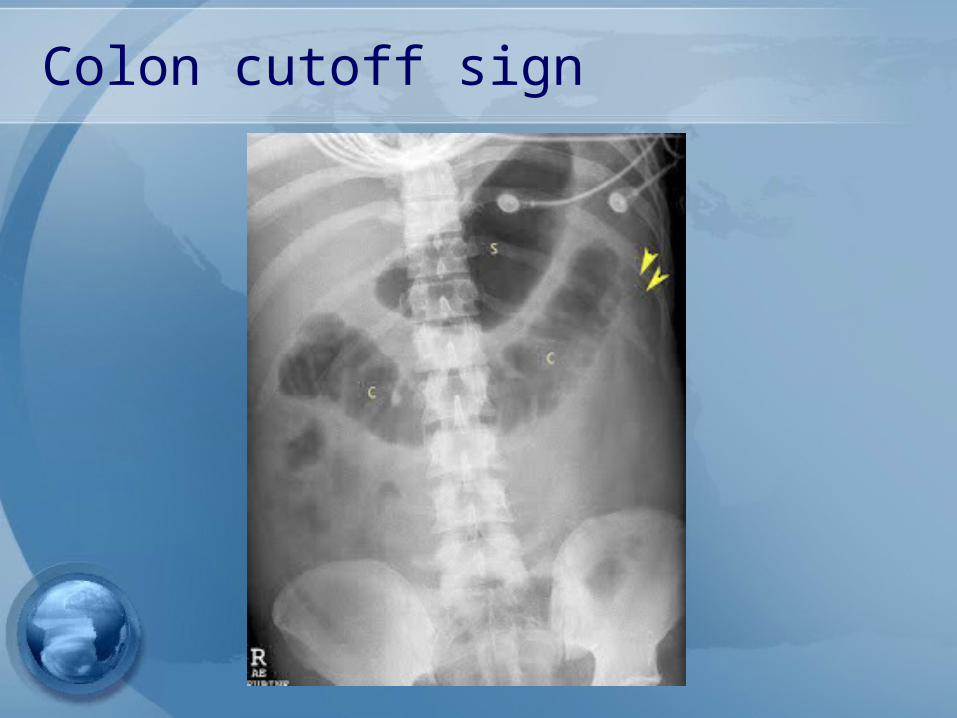
Colon cutoff sign
Radiologic Findings• Plain radiographs contribute little• Ultrasound may show the pancreas
in only 25-50%• CT scan provides better information
– Severity and prognosis– Exclusion of other diseases
• EUS & MRI with MRCP – cause of pancreatitis

Assessment of severity
Classification of severity
- Mild : lack of organ failure and complications
- Moderate : transient organ failure and/or complications < 48hr- Severe : persistent organ failure and complications
Reference : 2012 revision of atlanta classification of acute pancreatits
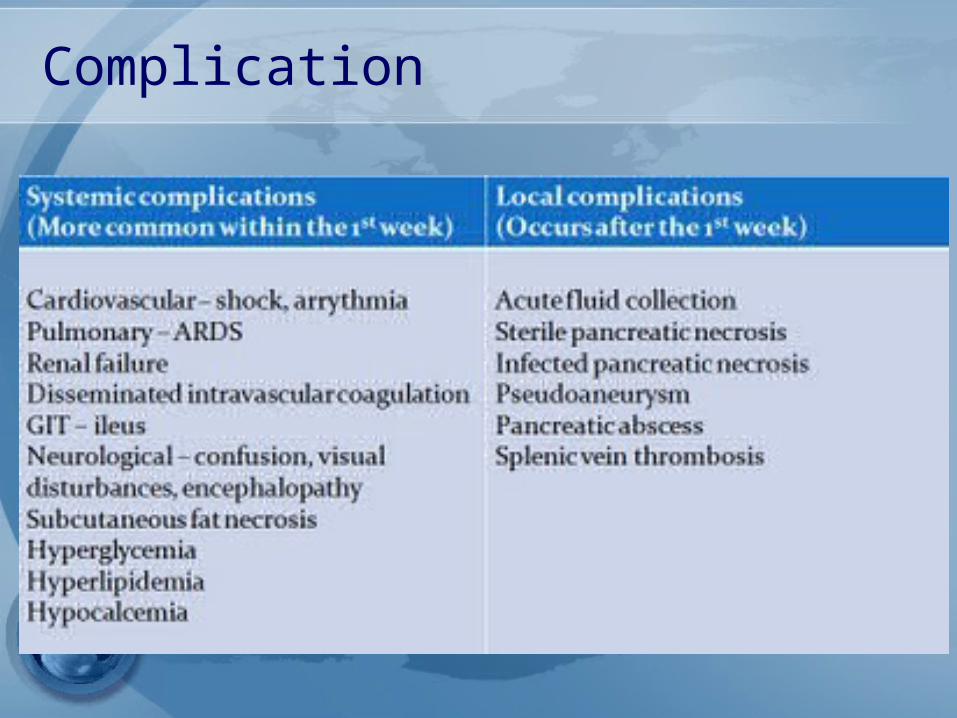
Complication
Early prognostic sign
•Ranson’s score•APACHE II
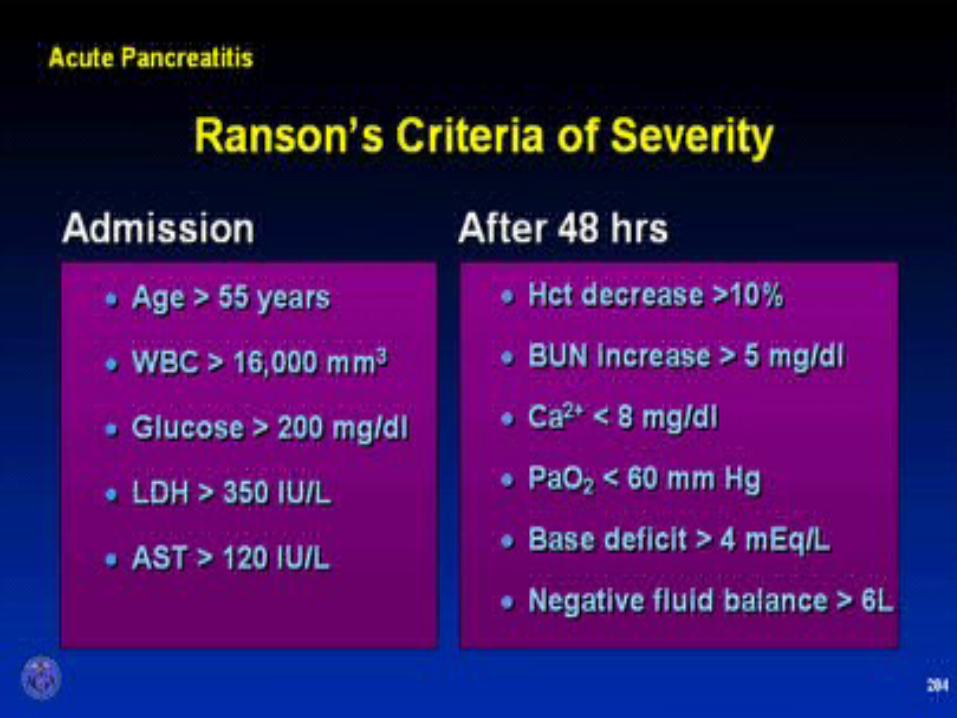
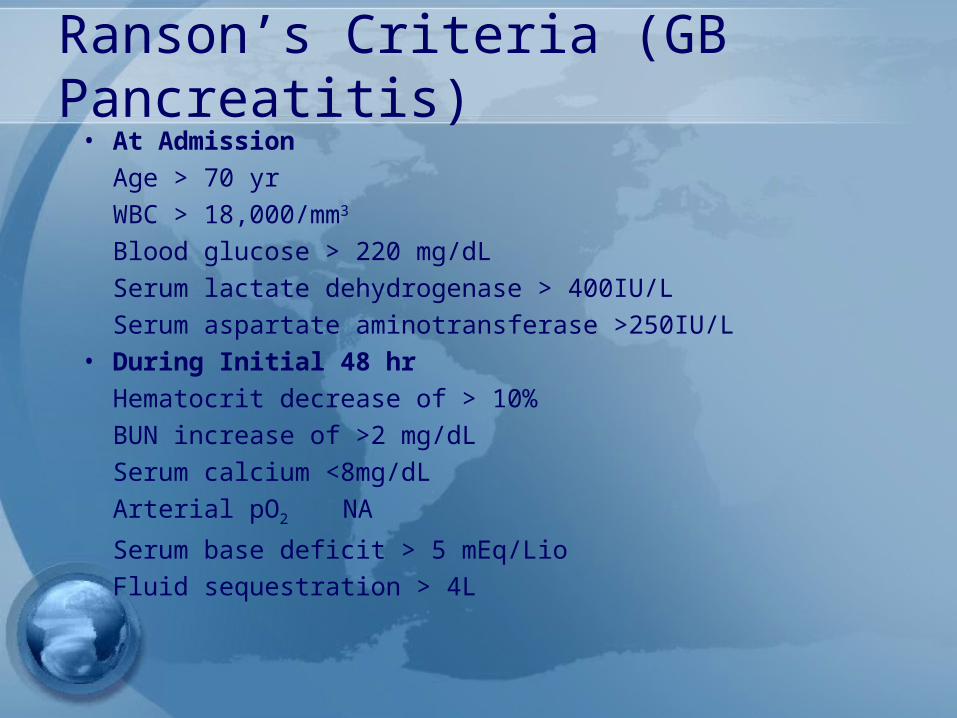
Ranson’s Criteria (GB Pancreatitis)
• At AdmissionAge > 70 yrWBC > 18,000/mm3
Blood glucose > 220 mg/dLSerum lactate dehydrogenase > 400IU/LSerum aspartate aminotransferase >250IU/L
• During Initial 48 hrHematocrit decrease of > 10%BUN increase of >2 mg/dLSerum calcium <8mg/dLArterial pO2 NASerum base deficit > 5 mEq/Lio Fluid sequestration > 4L
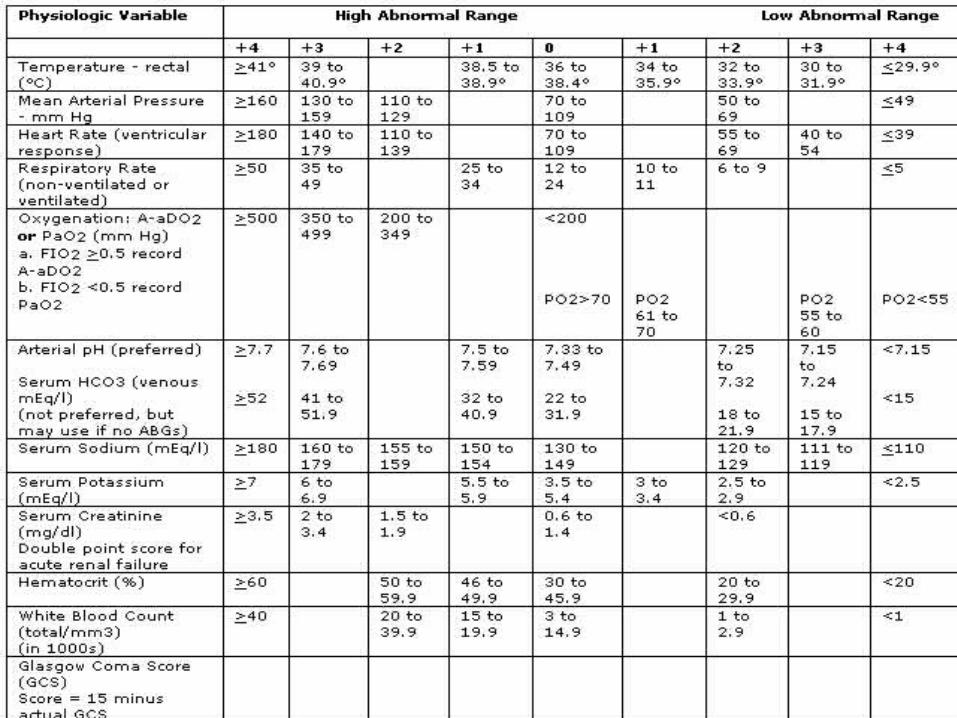
APACHE II• Measure at during the first 24
hours after admission• Using a cutoff of ≥8• The American Gastroenterological
Association (AGA) recommends: Prediction of severe disease by the APACHE II system
APACHE II
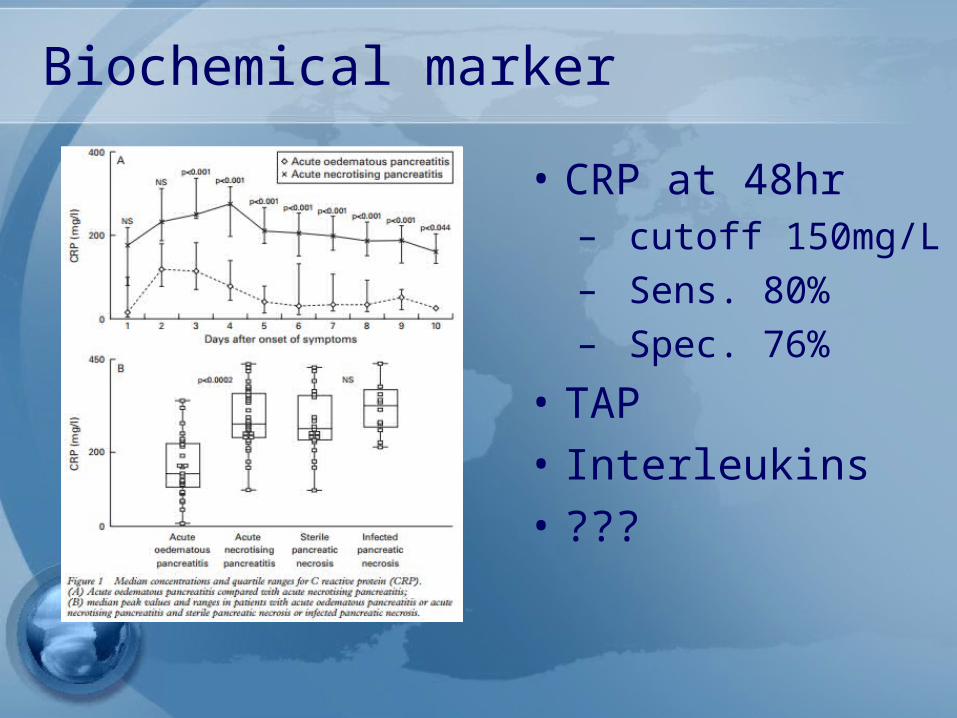
Biochemical marker• CRP at 48hr
– cutoff 150mg/L– Sens. 80%– Spec. 76%
• TAP• Interleukins• ???
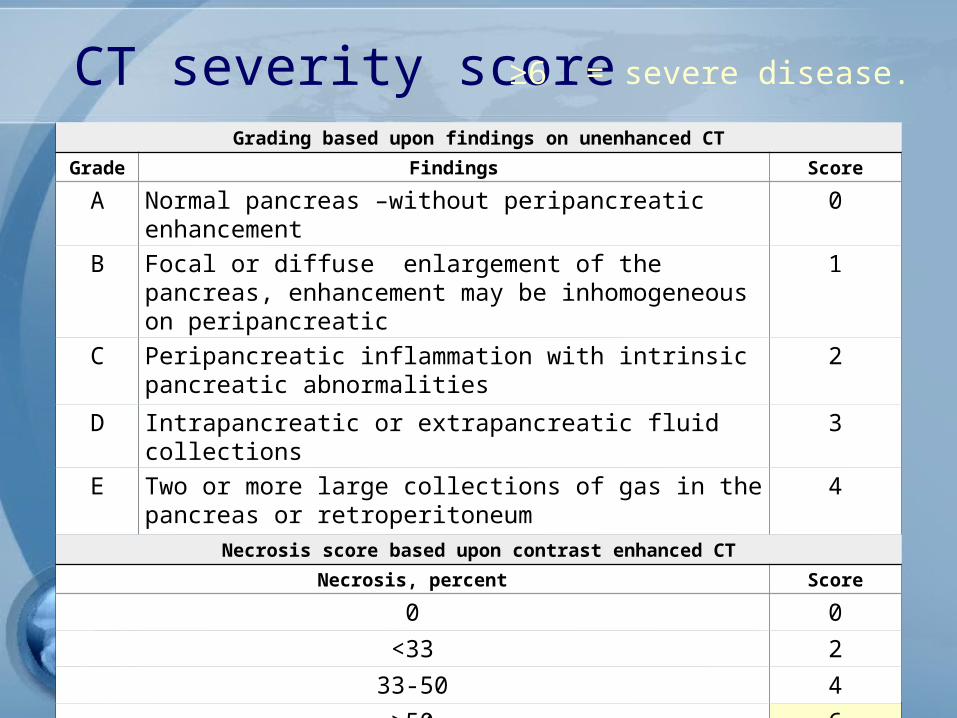
CT severity scoreGrading based upon findings on unenhanced CT
Grade Findings ScoreA Normal pancreas –without peripancreatic
enhancement0
B Focal or diffuse enlargement of the pancreas, enhancement may be inhomogeneous on peripancreatic
1
C Peripancreatic inflammation with intrinsic pancreatic abnormalities
2
D Intrapancreatic or extrapancreatic fluid collections
3
E Two or more large collections of gas in the pancreas or retroperitoneum
4
Necrosis score based upon contrast enhanced CTNecrosis, percent Score
0 033< 2-3350 4
≥50 6
≥6 = severe disease.

Treatment


Treatment• The essential requirements:• Accurate diagnosis• Appropriate triage• High-quality supportive care, • Monitoring for & treatment of
complications• Prevention of relapse
Fluids:• Aggressive fluid administration during first 24 hs
reduces morbidity & mortality.• Guidelines provide directions for early& vigorous fluid
administration.• Most important during the first 12 - 24 hours after the
onset of symptoms &of little value after 24 hours.• A balanced crystalloid solution at a rate of 200-500 ml /
hour, or 5 -10 ml / Kgm; 2500 - 4000 ml within the first 24 hours.
• Ringer’s lactate reduces inflammatory markers.• Clinical cardiopulmonary monitoring for fluid status,
hourly measurement of urine output&BUN/PCV are practical ways to gauge the adequacy of fluid therapy.
Fluids:• Excessive fluid administration results in
increased risks of the abdominal compartment syndrome, sepsis, need for intubation, & death.
Feeding:• Most patients with mild acute pancreatitis can be
started on a low-fat diet soon after admission, in the absence of severe pain, nausea, vomiting&ileus unusual in mild case.
• Total parenteral nutrition is now known to be more expensive, riskier&no more effective than enteral nutrition.
• Nasogastric or nasoduodenal feeding is clinically equivalent
• Total parenteral nutrition should be reserved for the rare cases in which enteral nutrition is not tolerated or nutritional goals are not met.
Antibiotics:• No benefit of prophylactic antibiotics. • Prophylaxis with antibiotic therapy is not
recommended for any type of acute pancreatitis unless infection is suspected or has been confirmed.
Endoscopic therapy:• ERCP is used primarily in patients with gallstone
pancreatitis &indicated in those who have evidence of cholangitis superimposed on gallstone pancreatitis.
• Also a reasonable treatment in patients with documented choledocholithiasis on imaging or findings strongly suggestive of a persistent bile duct stone (e.g., jaundice, a progressive rise in the results of liver biochemical studies, or a persistently dilated bile duct).
Pancreatic fluid & necrosis:• EUS is used as a platform for minimally invasive
treatment of a pancreatic pseudocyst or walled-off pancreatic necrosis.
• Acute peripancreatic fluid collections do not require therapy.
• Symptomatic pseudocysts are managed primarily with the use of endoscopic techniques, depending on local expertise.
• Necrotizing pancreatitis includes pan necrosis& peripancreatic fat necrosis.
• Over 4 wks or longer, becomes more liquid & becomes encapsulated by visible wall(WOPN)
• Sterile necrosis not require therapy except in rare case of collection that obstructs a nearby viscus.
Pancreatic fluid & necrosis:• The development of fever, leukocytosis, increasing
abdominal pain suggests infection of the necrotic tissue.
• A CT scan may reveal evidence of air bubbles in the necrotic cavity.
• Therapy begins with the initiation of broadspectrum antibiotics that penetrate the necrotic tissue.
• Aspiration / culture of the collection are not required.
• In current practice, efforts are made to delay any invasive intervention for at least 4 week.
• Nearly 60% of patients can be treated noninvasively and will have a low risk of death.
Pancreatic fluid & necrosis:• The step-up approach consists of antibiotic
administration, percutaneous drainage as needed& after a delay of several weeks, minimally invasive debridement, if required.
• A number of minimally invasive techniques (e.g., percutaneous, endoscopic, laparoscopic,retroperitoneal approaches) are available to debride infected necrotic tissue in patients with WOPN.
• Ssmall proportion of patients with infected necrosis can be treated with antibiotics alone.
Treatment• General Considerations
- adequate IV hydration and analgesia- NPO - NG tube: not routinely used * But may be used in patients with ileus or intractable N/V
• Nutrition• Early enteral feeding• Nasojejunal tube feeding• PPN,TPN
Treatment
• Metabolic Complications - Correction of electrolyte imbalance -
Ca,Mg- Cautiously for hyperglycemia
• Cardiovascular Care• Respiratory Care• Deep vein thrombosis prophylaxis
Prophylactic antibiotics– Although this is still an area of
debate– Not indicated for mild attack– suggest imipenem
or meropenem for 14 days for patients with proven necrosis
TREATMENT OF ASSOCIATED CONDITIONS
• Gallstone pancreatitis – ERCP should be performed within 72
hours in those with a high suspicion of persistent bile duct stones
– EUS & MRCP should be considered in case that clinical is not improving sufficiently
– Cholecystectomy +/- IOC

Complication
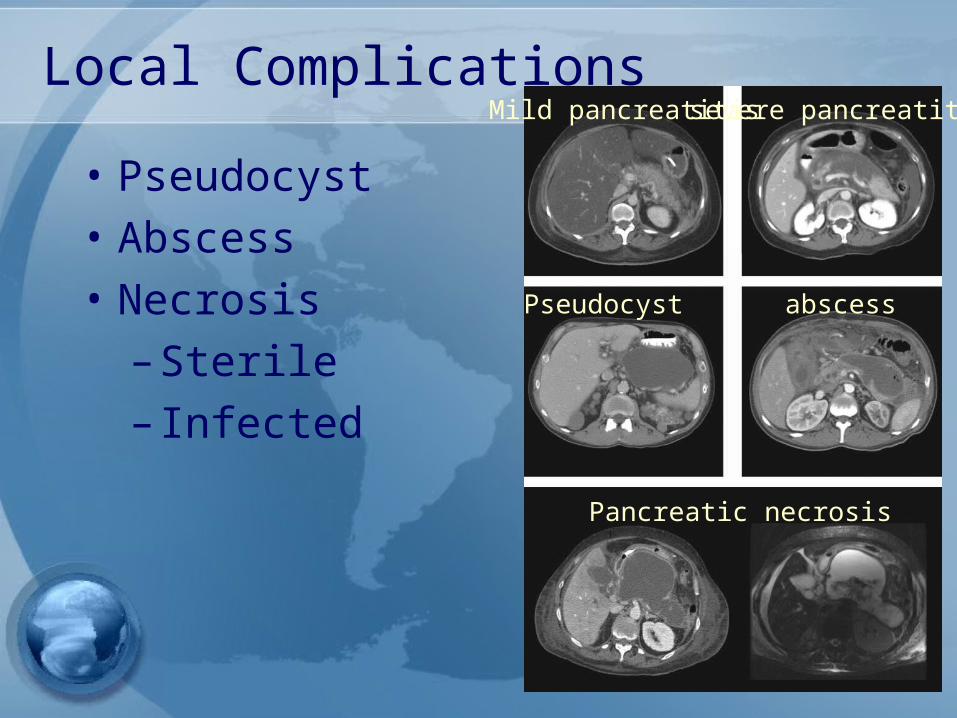
Local Complications• Pseudocyst• Abscess• Necrosis
– Sterile– Infected
Mild pancreatitis severe pancreatitis
Pseudocyst abscess
Pancreatic necrosis
New Classification Based onContrast-Enhanced CT (CECT)* • Interstitial Edematous Pancreatitis
– Acute Peripancreatic Fluid Collection
– Pancreatic Pseudocyst• Necrotizing Pancreatitis
– Acute Necrotic Collection– Walled-Off Necrosis
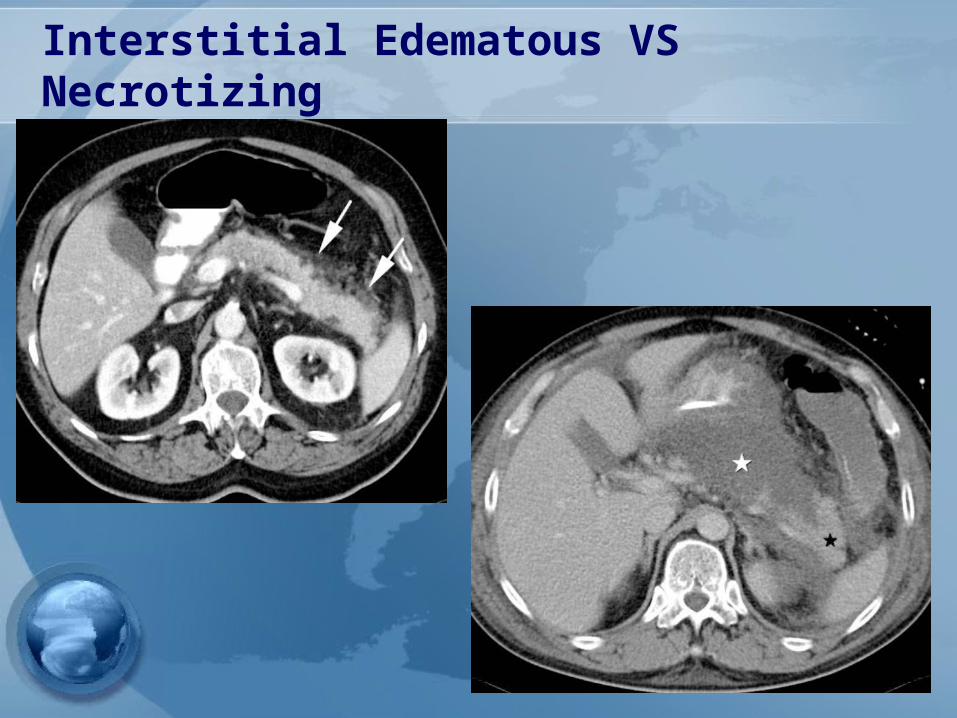
Interstitial Edematous VS Necrotizing
• Interstitial Edematous Pancreatitis – Pancreatic parenchyma enhances
with the contrast agent – Lack of peripancreatic necrosis
• Necrotizing Pancreatitis– Pancreatic parenchymal areas
without IV contrast enhancement +/- Peripancreatic necrosis (see below—ANC and WON)
Interstitial Edematous VS Necrotizing
Acute Peripancreatic Fluid Collection (APFC):
Occurring within the first 4 weeks in the setting of interstitial edematous pancreatitis.
• CECT Criteria –Homogeneous fluid adjacent to pancreas confined by peripancreatic fascial planes –No recognizable wall
Pancreatic Pseudocyst• An encapsulated, well-defined collection of
fluid but no or minimal solid components • Occurs >4 weeks after onset of in
interstitial edematous pancreatitis• CECT Criteria
– Well-defined wall , homogeneous, round or oval fluid collection
– No solid component – Only in interstitial edematous
pancreatitis
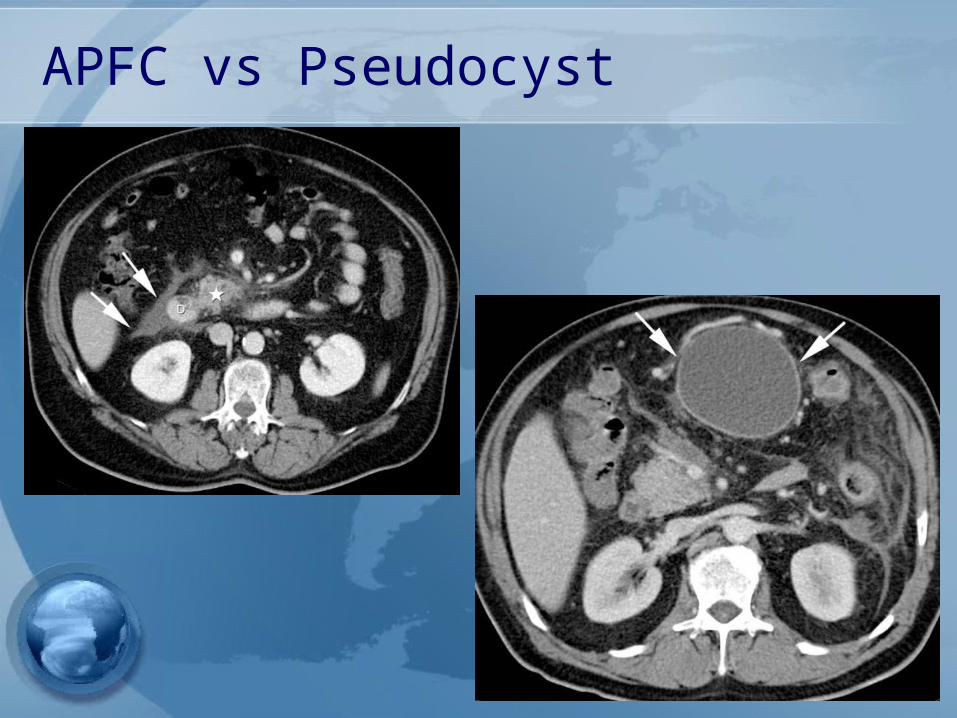
APFC vs Pseudocyst
Acute Necrotic Collection(ANC)
• A collection of both fluid and solid components (necrosis) occurring during necrotizing pancreatitis.
• This collection can involve the pancreatic and/or the peripancreatic tissues
• CECT Criteria – Heterogeneous– No encapsulating wall – Intrapancreatic and/or extrapancreatic
Walled-Off Necrosis(WON)• A mature, encapsulated ANC with a
well-defined inflammatory wall• these tend to mature >4 weeks after
onset of necrotizing pancreatitis.
• CECT Criteria – Heterogenous – Well-defined wall – Intrapancreatic and/or
extrapancreatic
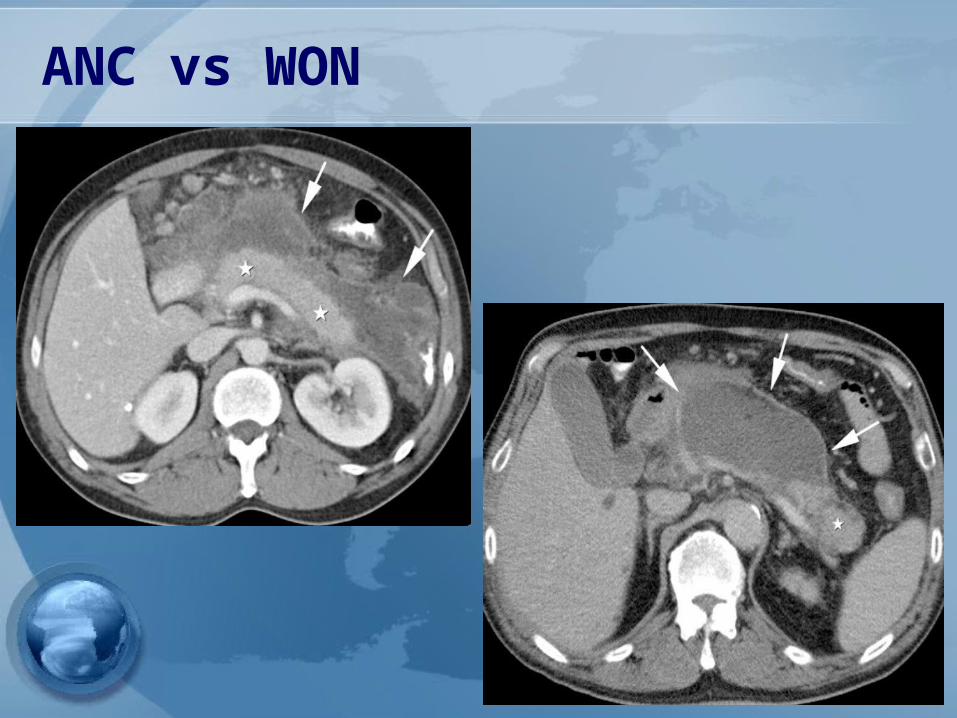
ANC vs WON
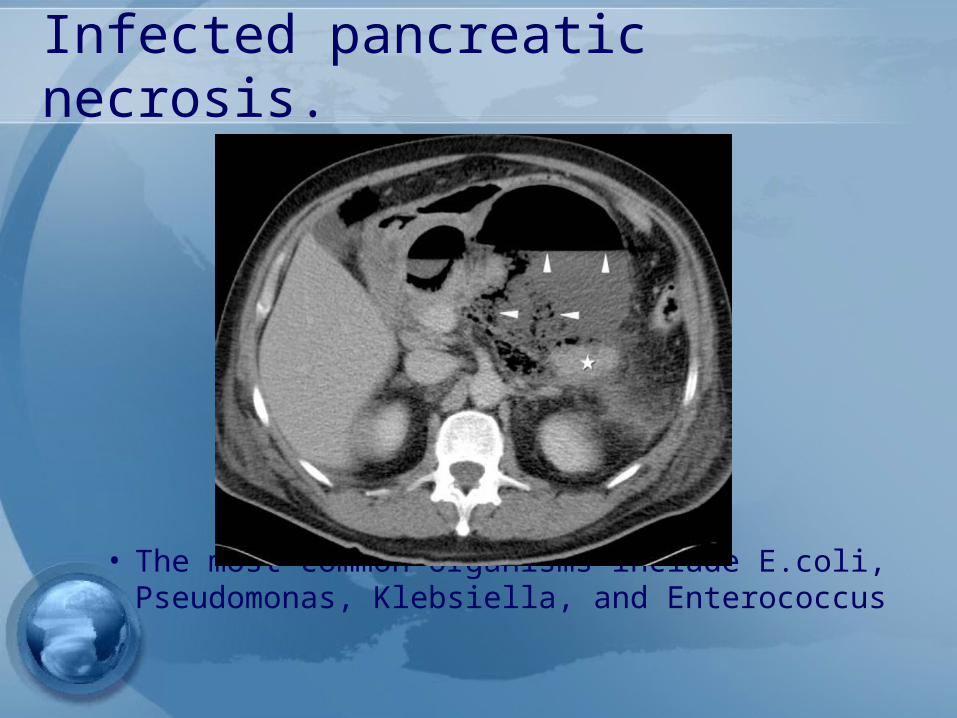
Infected pancreatic necrosis.
• The most common organisms include E.coli, Pseudomonas, Klebsiella, and Enterococcus

Guideline management of severe pancreatitis
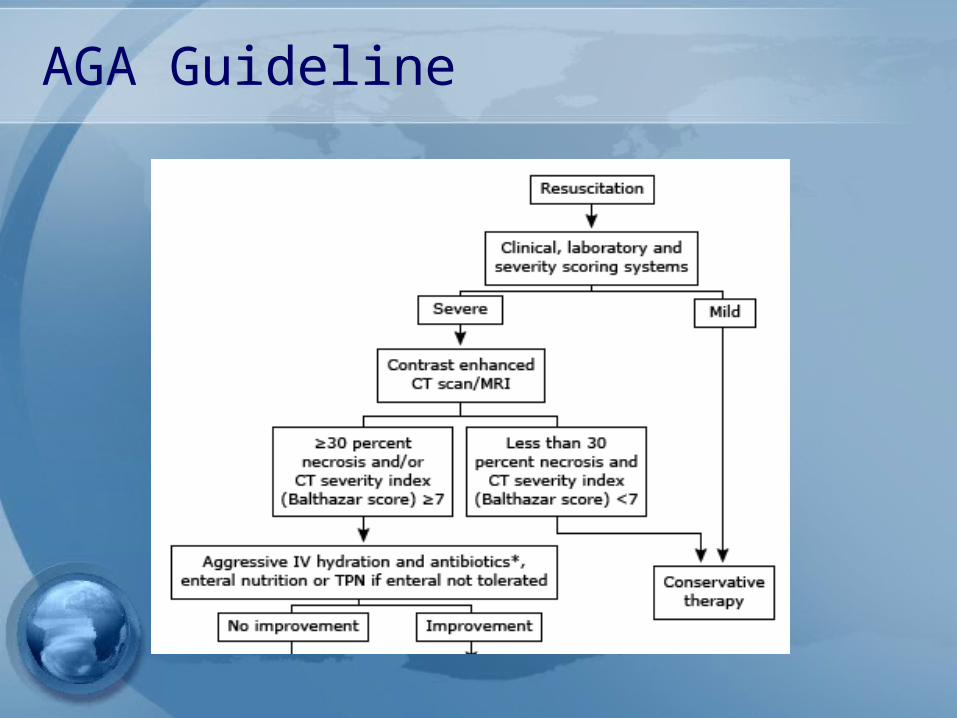
AGA Guideline
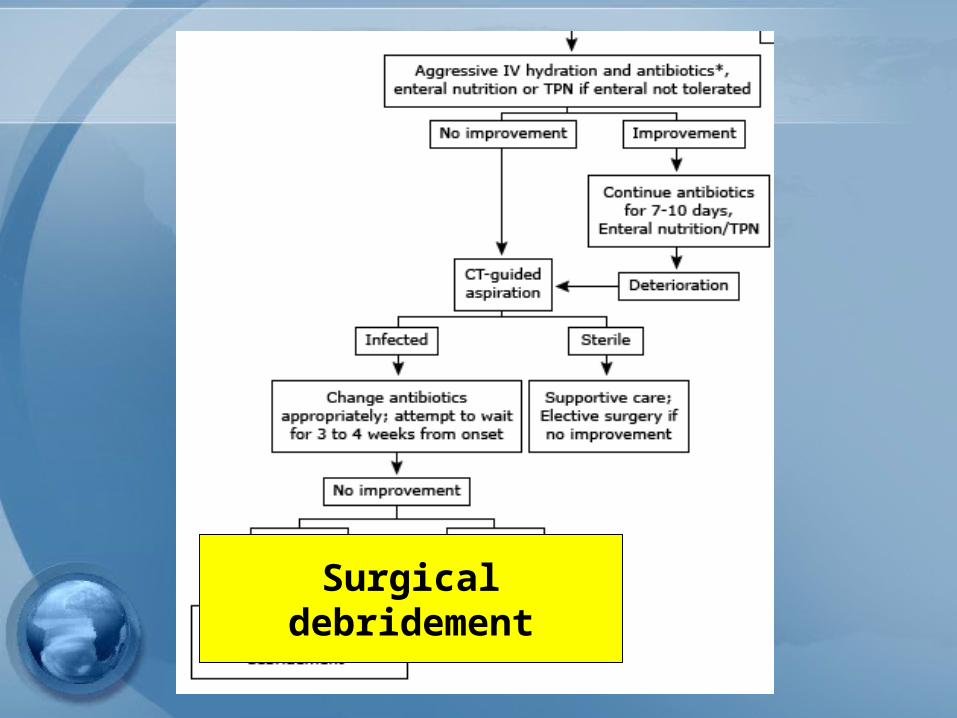
Surgical debridement

Management of pseudocyst
Management of pseudocyst• Watchful waiting:
- Operative intervention was recommended following an observation period of 6 wks
- However, there are some reports supportmore conservative approach
Management of pseudocyst• Surgical drainage – gold standard
Open vs endoscopic–cystgastrostomy–Cystenterostomy–Cystojejunostomy, Cystoduodenostomy–Ressection
Management of pseudocyst• Percutaneous catheter drainage
– As effective as surgery in draining and closing both sterile and infected pseudocysts
– Catheter drainage is continued until the flow rate falls to 5-10 mL/day
– If no reduction in flow, octreotide(50 -200 µg SC q 8hr) may be helpful.
– Should follow-up CT scan when the flow rate is reduced to ensure that the catheter is still in the pseudocyst cavity
– more likely to be successful in patients without duct-cyst communication
Management of local complication of pancreatitis
Indication forpancreatic debridement
• Infected pancreatic necrosis• Symptomatic sterile pancreatic
necrosis•chronic low grade fever•Nausea•Lethargy•Inability to eat•* Fail medical treatment
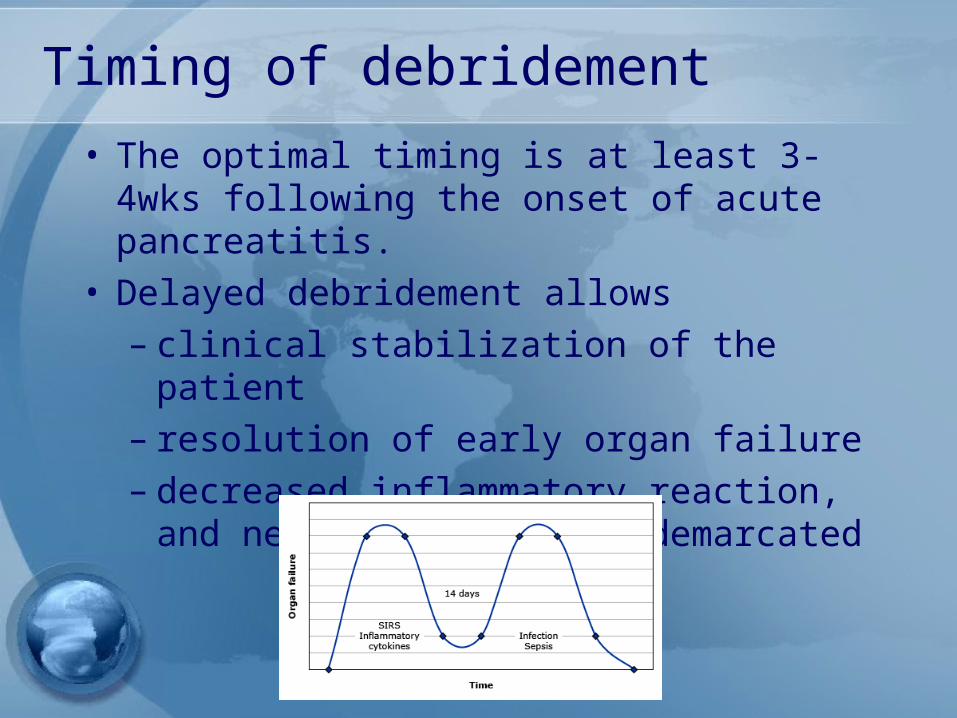
Timing of debridement• The optimal timing is at least 3-4wks
following the onset of acute pancreatitis.
• Delayed debridement allows – clinical stabilization of the patient– resolution of early organ failure– decreased inflammatory reaction,
and necrotic areas are demarcated
Surgical approach• Open debridement with external drainage
– gold standard• Open debridement with internal drainage and
cystgastrostomy - only appropriate for patients with WON
• Open packing — Open packing with planned reoperation every 48-72 hrs until the necrosis is adequately removed
• Laparoscopic debridement-Video-assisted retroperitoneal debridement-Laparoscopically-assisted transperitoneal debridement
Long-term complications:• Pancreatic exocrine/endocrine dysfunction
develops in 20- 30% &clear-cut chronic pancreatitis develops in one third to one half of those patients.
• Risk factors include:• The severity of the initial attack• The degree of pancreatic necrosis.• The cause of acute pancreatitis,Sp long-term,
heavy alcohol use as the cause & smoking as a cofactor dramatically increase the risk.
Prevention of relapse:• Cholecystectomy prevents recurrent gallstone
pancreatitis.• A delay of cholecystectomy for >few weeks places the
patient at a high (up to 30%) risk for relapse.• Cholecystectomy during the initial hospitalization
for mild pancreatitis due to gallstones reduces the rate of subsequent gallstone-related complications by almost 75%
• In severe or necrotizing pancreatitis endoscopic surgery can be delayed &biliary sphincterotomy will reduce (but not eliminate) the risk of recurrent biliary pancreatitis but may not reduce the risk of subsequent acute cholecystitis &biliary colic..
Prevention of relapse:• Alcohol & smoking quitting.• Withdrawing an implicated medication may prevent
relapse.• Tight control of hyperlipidemia can prevent a relapse.• Serum triglyceride levels will fall in the absence of
oral intake of food & fluids,so repeated measurements after dischargecan be informative.
• For PERCPP temporary placement of pancreatic duct stents& pharmacologic prophylaxis with NSAIDs.
• ERCP should be avoided in patients who are not likely to benefit from it (e.g., those with suspected SODD)
Conclusion:• Acute pancreatitis is an increasingly common
clinical problem. • New approaches to fluid resuscitation,antibiotic
use, nutritional support, treatment of necrosis have changed management but have not yet been widely adopted.
• More effective prevention of post-ERCP pancreatitis is possible, & gallstone pancreatitis can be prevented with timely cholecystectomy.