Embed Size (px)
Citation preview

HYPERTENSION IN PATIENTS
ON REGULAR HEMODIALYSIS
Prepared by
Dr/ Ehab Ashoor M.B.B.Ch. Alex. University
M.Sc. Internal Medicine, Cairo University

TALK OUTLINE
General view
Pathogenesis
Blood pressure measurement in dialysis patients
Management of high blood pressure in hemodialysis patients:
Target blood pressure of hypertensive dialysis patients
Algorithm for blood pressure control in dialysis patients
Intradialytic hypertension
Hemodialysis patients admitted with hypertensive urgency

General view Hypertension is common in dialysed patients
- at pre-dialysis state >80%,
- in patients with haemodialysis >60%,
- in those with peritoneal dialysis >30 %
The leading cause of death in dialysed patients
is cardiovascular!
Rahman M, Smith MC. Hypertension in hemodialysis patients. Current Hypertension Reports 2001; 3: 496-502.

General view But:
in dialysed patients the relationship between
hypertension and cardiovascular mortality/morbidity
is controversial because of
- the high prevalence of co-morbid conditions,
- by the underlying vascular pathology and
- by the effects of
- dialysis on blood pressure
- age
- left ventricular hypertrophy/dysfunction (also
more prevalent in patients with hypertension)
- poor nutrition .

General view In patients on hemodialysis, hypertension has been
associated with:
- stroke,
- MI,
- CHF,
- ventricular arrhythmias and
- progression of atherosclerosis

General view Characteristics of cardiovascular
complications in patients on dialysis
Hypertension present in 60-90%
LVH: 90%
Total mortality: 12-25% - CV mortality: 60-70%
CHD: 17x mortality
Risk factors 1 mm Hg icrease in MAP = 35% increase in CV morbidity
5 mm Hg increase in MAP = 3% increase in the risk of LVH

PATHOGENESIS
Putative Pathogenetic Mechanisms of Hypertension in ESRD Patients
Expanded extracellular fluid volume
Renin angiotension aldosterone stimulation
Increased sympathetic activity
Endogenous digitalis-like factors
Prostaglandins/bradykinins
Altered function of endothelium-derived factors
Erythropoietin administration
Nephron number
Parathyroid hormone secretion
Calcified arterial tree
Worsening of pre-existing essential hypertension
Renal vascular disease

EXPANDED EXTRACELLULAR FLUID VOLUME
Volume expansion is perhaps the most important factor in the development and maintenance of hypertension in dialyzed patients
It leads to an elevation in BP through the combination of an increased in cardiac output and an inappropriately high systemic resistance

INCREASED SYMPATHETIC ACTIVITY
Sympathetic overactivity is a common finding in ESRD
The afferent signal may arise within the kidney because sympathetic activation is not seen in aphrenic patients
Chemoreceptors within the kidney by uremic metabolites may be important in generation of these signals

ENDOGENOUS DIGITALIS-LIKE SUBSTANCE
It is believed to be produced in either the hypothalamus or adrenal cortex
Because it inhibits Na+-K+ ATPase activity, cytosolic sodium increases, inhibiting calcium outflux, and causing increased smooth muscle calcium content leading to increased smooth muscle tone

ENDOTHELIUM-DERIVED FACTORS
The abnormal endothelial release of hemodynamically active compounds
Elevated plasma levels of endothelin-1, the potent vasoconstrictor, had been found in uremic patients
Uremic plasma contains a higher level of an endogenous compound, asymmetrical dimethylarginine, that is an inhibitor of NO synthesis

ERYTHROPOIETIN
An increase in BP of 10mmHg or more occurs in approximately one third of the patients with renal failure who are treated with erythropoietin
Through increased total peripheral resistance related to increased viscosity and decreased hypoxic vasodilatation

HYPERPARATHYROIDISM
Increase in intracellular calcium induced by parathyroid hormone excess cause vasoconstriction and hypertension
Either vitamin D administration or parathyroidectomy has been shown to lower blood pressure

Blood pressure measurement
in dialysis patients
Pre- or post-dialysis blood pressure measurements
in patients with hemodialysis may be misleading for
the diagnosis of hypertension:
- the pre-dialysis systolic blood pressure may
overestimate by an average of 10 mmHg
- the post-dialysis systolic blood pressure may
underestimate by an average of 7 mmHg
Blood pressure readings over a period of 1 to 2 weeks rather than
isolated readings should be used
Luik AJ, Kooman JP, Leunissen ML. Hypertension in hemodialysis patients: Is it only hypervolaemia?
Nephrol Dial Transplant 1997; 12: 1557-60.

Blood pressure measurement
in dialysis patients
Ambulatory blood pressure monitoring (ABPM)
appears to be reproducible in pts. on hemodialysis.
Blood pressure is frequently
- high in pre-dialysis state,
- it falls immediately after dialysis, and then
- it gradually increases during the inter-dialytic period.
ABPM may be useful in determining “systolic blood pressure
load”(the amount of time that the patient′s systolic Bp exceeds normal values) which
is an important factor in the development of left ventricular hypertrophy.

- Pre-dialysis blood pressure correlates better with
LVH than post-dialysis blood pressure.
- The dialyzed patients usually lose the diurnal variation
in blood pressure and consequently these patients develop
nocturnal hypertension.
- Home blood pressure measurement, an increasingly popular
method, may be useful to estimate the blood pressure control
also in dialysed patients
Conion PJ, Walshe JJ, Heinle SK et al. Predialysis systolic blood pressure correlates strongly with mean 24-hour systolic blood pressure
and left ventricular mass in stable hemodialysis patients. J Am Soc Nephrol 1996; 7: 2658-63.
Agarwal R. Role of home blood pressure monitoring in hemodialysis patients. Am J Kidney Dis 1999; 33: 682-7.

Management of high blood pressure in
hemodialysis patients
Improved survival due to adequate blood pressure
control of dialysed patients has been clearly demonstrated,
stressing the importance of adequate antihypertensive treatment.
Salem MM, Bower J. Hypertension int he hemodialysis population: any relation to one-year survival? Am J Kidney Dis 1996; 28: 737-40.

Target blood pressure of hypertensive
dialysed patients
The pre-dialysis & post-dialysis Bp goals should be <140/90
mmHg & <130/80 mmHg respectively (C). In some younger
patients the target Bp may even be set as low as 120/80
mmHg. In patients with reduced vascular & cardiac
compliance, Bp goals need to be higher.
The reasonable target goal of a mean ABPM value
- during the day < 135/85 mmHg
- by night < 120/80 mmHg.
CAUTION! Very low systolic blood pressure (<110 mm Hg)
may be associated with enhanced cardiovascular mortality
Henrich WL, Mailloux LU. Hypertension in dialysis patients. Rose B. UpToDate online 11.3, 2004, http://www.uptodate.com

Algorithm for blood pressure control
in dialysis patients
1. Estimate dry weight
2. Initiate non-pharmacological treatment
3. Attain dry weight
4. Start or increase the dose of antihypertensives
to maintain BP below 140/90 mmHg
Fishbane S, Maseka JK, Goreja MA et al. Hypertension in Dialysis Patients . In Cardiovascular Disease in End-stage Renal Failure.
Loscalzo J, London GM. Oxford University Press, New York, USA, 2000. pp 471-484.

Clinical definitions of stable “dry weight”
- either the blood pressure has normalized or
- symptoms of hypervolemia disappear (not merely the absence
of edema);
- after dialysis seated blood pressure is optimal, and
- symptomatic orthostatic hypotension and clinical signs of
fluid overload are not present;
- at the end of dialysis patients remain normotensive until the
next dialysis without antihypertensive medication.
- No HTN (pre-dialysis Bp at the beginning of the week < 140/90 mmHg)
- No peripheral edema
- CXR; no pulmonary congestion & cardiothoracic ratio ≤ 50% (≤ 53% in females)
- Absence of edema does not exclude the hypervolemia

DRY WEIGHT
Not merely the absence of edema, but the body sodium content and volume of body water below which further reduction results in hypotension
Volume removal to correct clinical fluid overload and optimized seated BP without symptomatic orthostatic hypotension after dialysis
Body weight at the end of dialysis at which the patient can remain normotensive until the next dialysis without antihypertensive medication
Salt & water balance: Patient compliance is often suboptimal & so, heavy reliance is placed on dialysis UF capacity to remove this excess fluid

LAG PHENOMENON
In new patients starting dialysis, some period of time passes before volume is controlled, dry weight is achieved, and BP is controlled; this period has been called the lag phenomenon
This is the time required to convert the patient from a catabolic to an anabolic state while the extracellular fluid space slowly stabilized

Algorithm for blood pressure control
in dialysis patients
5. If BP is not controlled or dry weight not attained in 30 days,
consider:
- 24-48 hours ABPM
- increasing the duration of dialysis to facilitate removal
of fluid and attainment of dry weight
- increasing the dose or number of antihypertensives
6. If BP remains uncontrolled, consider:
- evaluating for secondary forms of hypertension
- peritoneal dialysis
- bilateral nephrectomy (exceptional)
Fishbane S, Maseka JK, Goreja MA et al. Hypertension in Dialysis Patients . In Cardiovascular Disease in End-stage Renal Failure.
Loscalzo J, London GM. Oxford University Press, New York, USA, 2000. pp 471-484.

COMMON CAUSES OF SECONDARY HYPERTENSION
Primary aldosternism
Pheochromocytoma
Cushing‘s syndrome
RAS & renal diseases
Obstructive sleep apnea
Obesity (metabolic syndrome)

Non-pharmacological treatment of
hypertension in dialysed patients
Important remarks:
-Control of plasma volume can either normalize or help to
normalize blood pressure in dialysed patients.
- Fluid removal predisposes to episodes of hypotension during
hemodialysis treatment.
-Hypotension is one of the important cardiovascular
risk factors.

Non-pharmacological treatment of
hypertension in dialysed patients
- Aerobic exercise
- Control of salt and fluid intake
- Cessation of smoking
- Weight reduction
- Avoidance of alcohol
- Long, slow and more frequent hemodialysis treatment
- Bilateral nephrectomy

Non-pharmacological treatment of
hypertension in dialysed patients
- Aerobic exercise
- Control of salt and fluid intake - Cessation of smoking
- Weight reduction
- Avoidance of alcohol
- Long, slow and more frequent hemodialysis treatment
- Bilateral nephrectomy

To avoid large inter-dialytic weight gains, patients should
restrict salt intake (750 to 1000 mg of sodium/day). This also
decreases thirst and improves patient’s compliance.
A fixed or a programmed decrease in the concentration of
sodium in the dialysate (from 155 to 135 mEq/L) with
combination of dietary salt restriction, may result in smaller
doses of antihypertensive drugs to control blood pressure.

Non-pharmacological treatment of
hypertension in dialysed patients
- Aerobic exercise
- Control of salt and fluid intake
- Cessation of smoking
- Weight reduction
- Avoidance of alcohol
- Long, slow and more frequent hemodialysis
treatment - Bilateral nephrectomy

The long, slow hemodialysis treatment (eight hours, and
three times a week) is associated with the maintenance of
normotension without medications in almost all patients,
as this decreases afferent renal nerve activity and efferent
sympathetic activation.
Nocturnal hemodialysis treatment (six or seven nights a
week during sleep hours) can also normalize blood pressure
without medications in most of the patients.
More frequent hemodialysis treatment (two hours six times
per week) may also be associated with normotension without
medications and with regression of left ventricular hypertrophy.

Non-pharmacological treatment of
hypertension in dialysed patients
- Aerobic exercise
- Control of salt and fluid intake
- Cessation of smoking
- Weight reduction
- Avoidance of alcohol
- Long, slow and more frequent hemodialysis treatment
- Bilateral nephrectomy

Bilateral nephrectomy may be considered in:
- noncompliant individuals
- with life-threatening hypertension
- blood pressure cannot be controlled with any of the
above detailed dialysis modality.

Pharmacological treatment of hypertension
in dialyzed patients
Suggested use of antihypertensive drugs in hemodialysis patients
(which drug - when)
Drugs Compelling indication Specific side-effects Special precautions
ACE inhibitors LVH, CHF, DM, Anaphylactoid reactions with
AN69 dialyzer
DHP-CCB CHD
Non-DHP-CCB CHD No comb. with BBL
BBL CHD Excessive bradycardia No comb with
with liposoluble compounds non-DHP-CCB
Centrally act. none Post-dialysis rebound Avoid
agents with methyldopa
ABL Dyslipidemia Severe hypotension
Insulin resistance
Direct Hypertensive In hospital use
vasodilators crisis

Some remarks for antihypertensive drug classes
ACE-inhibitors: -effective and well tolerated
- reduce mortality also of dialysed patients (age < 65 yrs) independently
from the antihypertensive effect
- can reduce the synthesis/secretion of erythropoietin (anemia !)
- can trigger an anaphylactoid reaction in patients dialyzed with
AN69 dialyzer

PHARMACOKINETIC PROPERTIES OF ACE
INHIBITORS IN ESRD
T1/2(h)
normal
T1/2(h)
ESRD
Initial
dose in
HD
Maintenance
dose in HD
Removal
during HD
Captopril 2-3 20-30 12.5 q24h 25-50 q24h Yes
Enalapril 11 prolonged 2.5 q24h
or q48h
2.5-10 q24h
or q48h
Yes
Fosinopril 12 prolonged 10 q24h 10-20 q24h No
Lisinopril 13
54 2.5 q24h
or q48h
2.5-10 q24h
or q48h
Yes
Ramipril 11 prolonged 2.5-5q24h 2.5-10 q24h yes
Henrich W. Principles and Practice of Dialysis

Some remarks for antihypertensive drug classes
ARB: - limited experience
- losartan does not enhance the risk of anaphylactoid dialyzer-reactions
- no dose adjustment is necessary in renal failure in the absence of
volume depletion.

PHARMACOKINETIC PROPERTIES OF ARB’S IN ESRD
T1/2(h)
normal
T1/2(h)
ESRD
Initial dose
in HD
Maintenance
dose in HD
Removal
during HD
Candesartan 9 ? 4 q24h 8-32 q24h No
Irbesartan 11-15 11-15 75-150 q24h 150-300 q24h No
Losartan 2 4 50 q24h 50-100 q24h No
Telmisartan 24 ? 40 q24h 20-80 q24h No
Valsartan 6 ? 80 q24h 80-160 q24h No
Henrich W. Principles and Practice of Dialysis

Some remarks for antihypertensive drug classes
CCB: - effective and well tolerated
- do not require supplementary post dialysis dosing
-26 % (significant) reduction in cardiovascular mortality
in USRDS Study
BBL: - side effects include CNS depression (mainly lipid-soluble drugs),
bradycardia, and heart failure
- preferable beta-blocker may be atenolol, labetalol, carvedilol

PHARMACOLOGIC PROPERTIES OF Β-BLOCKERS IN
CHRONIC DIALYSIS PATIENTS
T1/2(h)
normal
T1/2(h)
ESRD
Initial dose
in HD
Maintenance
dose in HD
Removal
during HD
Bisoprolol 9-12 18-24 5 q24h
1.25 in HF
5-10 q24h
1.25-10 in HF
No
Atenolol 6-9 <120 25 q24h 25-50 q24h Yes
Carvedilol 4-7 4-7 12.5 od, b.i.d 12.5-50 od,
b.i.d
No
Metoprolol 3-4 3-4 50 b.i.d. 50-100 b.i.d. No
Propranolol 2-4 2-4 40 b.i.d. 40-80 b.i.d. No
Labetalol 4-8 4-8 50 bid 50-800 bid,
t.d.s, q.i.d
No
Henrich W. Principles and Practice of Dialysis

Some remarks for antihypertensive drug classes
ABL: - Prazocin, Doxazocin
- help counteract the increase in sympathetic nerve activity.
- on long-term treatment the favourable metabolic effects
on lipids and insulin resistance might be advantageous.
- preferred mostly in antihypertensive combinations.
Centrally acting drugs: - methyldopa, clonidine, guanfacine have more side effects,
- moxonidine, rilmenidine (imidazoline I1 receptor agonists are safe
and effective, but only limited experience is available).

Special situations
Erythropoietin (EP)-induced hypertension - decrease the actual dry weight
- decrease the dose (if possible)of EP or interrupt treatment
- reintroduce treatment later at lower dose
- introduce or increase antihypertensive medication with preference
of CCB
Ribstein J, Mourad G, Argiles A et al. Hypertension in end-stage renal failure. In Complications of Dialysis.
Ed. by Lameire N, Mehta RL. Marcel Dekker, Inc. New York, USA, 2000. pp 274-287.

Special situations
Diabetic dialysis patients Characteristics
- the number of T2DM is rapidly increasing
- patients are generally hypertensive
- exchangeable sodium is increased
- frequent:
- orthostatic hypotension due to autonomic neuropathy with
severe symptoms
- coronary artery disease
- peripheral atherosclerosis

Special situations
Diabetic dialysis patients cont.
Treatment
To avoid the risk of severe hypotension:
- longer dialysis
- slow ultrafiltration rate
- hemofiltration
- glucose-containing dialysate can be used.
- ACE inhibitors and/or ARBs may prevent end-organ vascular
diseases
- CCBs are very effectively reduce blood pressure but may result in
severe hypotensive episodes
- BBL-benefit is particularly significant in patients with CHD

• Blood pressure remaining above goal in spite
of concurrent use of 3 antihypertensive agents of
different classes.
Resistant Hypertension

CLINICAL MARKERS FOR RESISTANT HYPERTENSION:
Advancing age
High base line blood pressure
Obesity and over weight
Excessive dietary salt intake, alcoholism
Chronic kidney disease
Diabetes mellitus type 2
Left ventricular hypertrophy
Black race
Female gender

RESISTANT HTN IN ESRD TREATMENT
Transdermal clonidine at weekly intervals.
Minoxidil, a potent vasodilator,
used with beta blockers
Spironolactone in Hemodialysis Patients
25-50 mg post dialysis
Risk of hyperkalemia
Improve EF and Improve BP control
Large studies are done

RESISTANT HYPERTENSION
The use of non steroidal anti-inflammatory drugs
Renovascular hypertension
Increasing cysts in polysystic kidney disease
Compliance

PSEUDORESISTANCE
Pseudo hypertension
Non-adherence may account for up to 50% of resistant cases
Inadequate Regimen
Especially inadequate diuretic component (pre-dialysis state)
Interfering medicines and substances also need to be considered
NSAIDs
Excessive Alcohol, Caffeine, or Tobacco
Excessive Salt Intake
Drugs of Abuse
Oral contraceptives

PSEUDOHYPERTENSION
Calcification of the arteries resulting in failure of the BP cuff to compress and occlude flow
Suspect if:
severe hypertension by cuff but no end organ injury
Antihypertensive excess results in symptoms/signs of Hypoperfusion/hypotension without measurable hypotension
Pipe stem calcification on x-ray

PSEUDOHYPERTENSION
Osler’s Maneuver (the radial artery remains palpable due to calcification and thickening despite inflation of cuff above systolic pressure) Poorly reproducible
“Dynamap”-like devices may be more accurate in this setting
Direct Intra-arterial measurement is the only definitive way to establish the diagnosis, but this is uncommonly done

RESISTANT HTN IN ESRD
Renal sympathetic nerve ablation
Hyperactivation of the sympathetic nervous system
J Clin Hypertens (Greenwich). 2012 Nov;14
The Future?
Device-Based Therapy for Resistant Hypertension
Baroreflex Activation Therapy
Renal Denervation Therapy

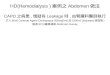
BAROREFLEX ACTIVATION THERAPY (BAT) CONTINUOUSLY MODULATES THE AUTONOMIC NERVOUS SYSTEM
Carotid Baroreceptor Stimulation
Heart Vessels Kidney
Inhibit sympathetic & Enhance Parasymp
HR Vasodilation Natriuresis
Renin
secretion

ANATOMICAL LOCATION OF RENAL SYMPATHETIC NERVES
Arise from T10-L1
Follow the renal artery to the kidney
Primarily lie within the adventitia
The Journal of Clinical Hypertension. 14, pages 799–801,2012
Circulation. 2002;106:1974–1979

Special features of frequently used
antihypertensive drugs in hemodialysis patients
Diuretics -avoid thiazide-type drugs, K-sparing drugs (amiloride, spironolactone)
acetazolamide
- furosemide is useful but it has ototoxicity and augment
aminoglycoside-toxicity
BBL - no change in the dose of carvedilol, labetalol, metoprolol, pindolol,
propranolol (active metabolites!), tertatolol, timolol
ACEi - fosinopril has dual excretion (50% kidney, 50% liver), therefore no
need to reduce the dose

Special features of frequently used
antihypertensive drugs in hemodialysis patients
ARBs - no need to change the dose of irbesartan, losartan, olmesartan,
telmisartan and valsartan
CCB - DHP-CCB: no need to change the dose
- verapamil: the dose should be reduced by 50 % (active metabolites!)
Direct vasodilators - no need to change the dose of diazoxide, hydralazine, minoxidil
- nitroprusside-Na: thiocyanate is dialysable

Antihypertensive drugs in dialysis patients Summary (when – which drug)
Cliniucal situation Drugs of choice Not recommended
CHF ACEi, ARB, BBL -
Post-MI ACEi, BBL Dir. vasodil.
LVH diast.dysf. BBL, dilti., verap. Dir. vasodil., α1BL
COPD ACEi, ARB, CCB BBL
CHD BBL, ACEi, CCB
ARB
Locatelli F. et al. Nephrol. Dial. Transoléant. 2004; 19:1058-1068

INTRADIALYTIC HYPERTENSION:
DEFINITIONS An increase in mean arterial blood pressure (MAP) ≥ 15 mmHg during or immediately after hemodialysis
An increase in systolic BP (SBP) >10 mmHg from pre
to postdialysis
sustained increase of BP during the dialysis session with BP values during and at the end of the dialysis session exceeding BP values at dialysis onset
Hypertension during the second or third hour of
hemodialysis after significant ultrafiltration has taken
place
An increase in BP that is resistant to ultrafiltration
Inrig JK. Intradialytic hypertension: a less-recognized cardiovascular complication of hemodialysis. Am
J Kidney Dis. 2010 March ; 55(3): 580–589 Chazot C and Jean G. Intradialytic hypertension: It is time to act. Nephron Clin Pract 2010;115:c182–c188

INTRADIALYTIC HYPERTENSION
5-15%
Mechanism
Extracellular volume overload
Increased cardiac output
Changes in sodium levels
Activation of the renin–angiotensin–aldosterone system
Overactivity of the sympathetic nervous system
Endothelial cell dysfunction.
Removal of anti HTN during dialysis

INTRADIALYTIC HYPERTENSION
The most important treatment is adequate sodium and water removal and reducing sympathetic hyperactivity.
Changing to non-dialyzable antihypertensive medications
Altering the dialysis prescription.



THANK YOU FOR YOUR ATTENION