Embed Size (px)
Citation preview

dr. Khomimah, [email protected]
RS Islam Pondok Kopi Jakarta Timur; RS Awal Bros Kalimalang; RS Antam Medica Jakarta Timur

Source: IDF Diabetes Atlas, 6th edn. Brussels, Belgium: International Diabetes Federation, 2013. http://www.idf.org/diabetesatlas

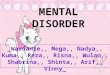
Pathophysiology of type 2 diabetes
Cernea S & Raz I. Diabetes Care 2011;34(suppl 2):S264–S271
CNS, central nervous system; GI, gastrointestinal; T2DM, type 2 diabetes mellitus
Adipocyte
CNS
Incretin deficiency
GI tract
Altered fat metabolism
INSULIN RESISTANCEINADEQUATE INSULIN
SECRETION↑ HEPATIC GLUCOSE
PRODUCTION
↑ BLOOD GLUCOSE
Hyperglucagonaemia↑ hepatic sensitivity
to glucagon
cellsα cells
SkeletalMuscle
Pancreas
Muscle
Kidney
Enhanced glucose reabsorption

Slide 7
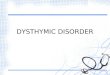
The goal of diabetes management is to secure optimal glycemic control to avoid complications
Diabetic
retinopathy
Leading cause
of blindness
in working-age
adults1
Diabetic
nephropathy
Leading cause of
end-stage renal disease2
Cardiovascular
disease
Stroke
1.2- to 1.8-fold increase in stroke3
Diabetic
neuropathy
Leading cause of non-
traumatic lower extremity
amputations5
75% diabetic patients
die from CV events4
1Fong DS, et al. Diabetes Care 2003;e 26 (Suppl.1):S99–S102. 2Molitch ME, et al. Diabetes Care 2003; 26 (Suppl.1):S94–S98. 3Kannel WB, et al. Am Heart J 1990; 120:672–676. 4Gray RP & Yudkin JS. Textbook of Diabetes 1997. 5Mayfield JA, et al. Diabetes Care 2003; 26 (Suppl.1):S78–S79.
Microvascular Macrovascular
Diabetic Foot
Erectile DysfunctionThe most secretive
Complication of DM

Can affect any part of the body, at any time
It is most common precursor to Coronary heart disease and heart attack
It also causes stroke by affecting the arteries in the neck
One of the most common form of vascular disease in PAD

Metabolic memory: A vascular perspective

Hyperglycemia and vascular outcome
Hyperglycemia activates multiple and complex pathogenetically relevant pathways.
• Inflammatory processes lead to a thickening ofthe basal membrane of microvessels andperivascular fibrosis resulting in micro vascularendpoints in the most susceptible organs, suchas renal insufficiency and retinopathy.
• The structural changes also result in functionalimpairment and a reduction in blood flowregulation, which in turn reduces macrovascularendothelial function.("Micro/Macro Interaction”).
• The loss of endothelial protection may lead tothe subsequent development of atherosclerosis.
• The structural changes within themicrocirculation may account for building up a
“metabolic memory”.
Jax Cardiovascular Diabetology 2010, 9:51

The Vascular Continuum. Conductance arteries mediate downstream effects to resistance arteries and capillaries. If
microcirculation is impaired by perivascular fibrosis as in diabetes, upstream effects influence conductance arteries.
Jax Cardiovascular Diabetology 2010, 9:51

Japanese Journal Of Physiology, 41, 1991A Novel Fibrinolytic Enzyme (Lumbrokinase)
Extracted From The EarthwormHisashi MIHARA, Et Al
Abtract• A Strong Fibrinolytic Enzyme Was Readily Obtained In Saline Extract Of The Earthworm• It Hydrolyzed Not Only Plasminogen-rich Fibrin Plate, But Also Plasminogen-free Fibrin
Plates
LumbrokinaseReseached And Developed ByThe Institute Of BiophysicsChinese Academy Of Sciences
Safe And Effective Supportive Measure In The Management Of Diabetes MellitusMicrovascular And Macrovascular Complications Prevention And Treatment

Activation of the coagulation cascade occurs through release of tissue factor (extrinsic pathway). This leads to the generation ofthrombin which activates fibrinogen by cleavage of fibrinopeptides A and B resulting in polymerisation to form the fibrin clot. FactorXIIIa catalyses the formation of covalent cross-links between fibrin molecules which enhances the stability of the clot. Fibrinolysis isinitiated by the activation of plasminogen to plasmin by tissue-plasminogen activator (t-PA) and urinary-type plasminogen activator (u-PA). The main inhibitors of fibrinolysis are plasminogen activator inhibitor-1 (PAI-1) and α2-antiplasmin.
Thromb Haemost 2011; 105 (Suppl 1): S43–S54

LUMBOKINASEMechanism of Action In The Management 0f Thrombotic Disorders
1. Directly dissolve fibrinogen and fibrin, convert plasminogen to plasmin, increase endogenous human t-PA activity (Fibrinolytic)
2. Inhibiting platelet activation and aggregation (Anti Platelet)3. Inhibiting of ICAM-1 expression (Anti Coagulation)Plus (+) Fibrinogenolytic
1. Biotechnology Research Institute, Chinese Academy of Agricultural Sciences, Beijing, China, 2. Department of Natural Sciences, Northeastern State University, Broken Arrow, Oklahoma, USA, and 3. harmaceutical School, Peking University, Beijing, China
3 in 1

Microcirculation were improved significantly after treatment in both groups (P <0.05).
Compared with the control group, the microcirculation improvement in the treatment group was significantly better
(P <0.05).
Conclusions
The Diamicron Plus Lumbrokinase Capsules Can Effectively Treat Microcirculatory Impairment In Diabetes Mellitus Without
Any Major Adverse Reactions.
Parameter
Table 1. Nailfold microcirculation indicators before and after treatment
* vs. Pre-Tx, p<0.05; ∆ vs.control, p<0.05

Evaluation : 1) Effective: abnormal sensations, decreased muscle tone & strength improved / disappeared; improvement in knee & achilles deep tendon reflex. 2) Ineffective: no improvement in abnormal sensations, decreased muscle tone and strength; no improvement in knee and achilles deep tendon reflex.
(X2=21.56, P<0.01). It explains that lumbrokinase is effective in treating diabetic peripheral neuropathy
Observation of the Effectiveness of
Treating Diabetic Peripheral Neuropathy by Lumbrokinase
Treatment Method: • Apply vitamin B1 20 mg 3 tid, muscle injection of vitamin B12 500μg once a day on top of diet control and
blood sugar lowering drugs• Treatment group has lumbrokinase 460 mg tid 30 minutes before meal. For 4 weeks.
XiuLan Gu, GuanYin Lee, Lian Lian Chinese Journal Of Primary Medicine and Pharmacy 2003; 10(7): 665.

Medical Management of Acute Limb Ischemia (PVD)The Role of Lumbrokinase
Kasim, M. et al The Journal of Alternative and Complementary Medicine; 2009; 15 (5): 539543
Diagnosis• 60 yrs man• Stage IIB Acute Limb Ischemia (PVD)• Atrial fibrilation with normoventricular response• Moderate mitral stenosis• Type-2 DM• Stage-1 hypertension
Treatment• Surgical Procedures (Surgical Thrombectomy) Refused• Tromboles (Lumbrokinase), 3 x 3 kalsul• Cilostazol, 2 x 100mg• Digoxin, 1 x 0,25mg• ISDN, 3 x 10mg• Metformin, 2 x 500mg• Irbesartan, 1 x 100mg

Day-4Pain and numbness of both legs disappearPatient only felt stiffness on dorsum pedis and toesPhysical examination: weak pulsation of tibialis anterior and dorsalis pedis arteries
Day-15CT angiography: better contrast flow on bothn legsAfter 2 weeks of treatment with Lumbrokinase discharged with good conditions
Day-50 CT angiography: normal contrast flow on both legs

• Tromboles (lumbrokinase) could be considered as an alternative medicaltreatment for acute limb ischemia, especially in patient who refused surgicaltreatment.
• The role of Tromboles (lumbrokinase) as a treatment option of acute limb ischemianeed further evaluation on large, well design, study.
Conclusion

Methods10 stable angina pectoris patients were randomly selected from proved CAD population innational cardiovascular center Harapan Kita.
Diagnosis of CAD determined by typical chest pain symptom and confirmed by MSCT orcoronary angiography examination.
They were given additional 2 capsules of Tromboles (containing 250 mg lumbrokinase for eachcapsul) three times daily for 30 days to a standard therapy including nitrate, ß blocker, statinand aspirin.
Perfusion imaging 99mTc-Sestimibi was used to evaluate the perfusion and viability ofmyocardium before and after treatment using DSX rectangular gamma Sophy camera.
One month treatment of oral Tromboles (lumbrokinase) resulted in an improvement myocardialperfusion in stable angina pectoris with metabolic syndrome without bleeding complication
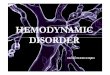
Improved Myocardial Perfusion in Stable Angina Pectoris by Oral Lumbrokinase (TROMBOLES)
A Pilot Study
Kasim, THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE 2009;15(5): 539-44

Figure 2.A case example of a patient's stress myocardial perfusion before and atthe end of 30 day treatment with Lumbrokinase (TROMBOLES).
Corresponding representativeapical (a), mid (b) and basal (c) short axis, and mid vertical long axis (d)tomographic perfusion images demonstrating significant reduction in theextent and degree of inducible ischemia in the anterior (arrows) andlateral (arrow heads) left ventricular wall.
Oral Lumbrokinase
TROMBOLESIMPROVES REGIONAL MYOCARDIAL PERFUSION
in Patients with Stable Angina

ObjectiveAssessment

Chin Med J 2013;126 (21)
• To assess the effect of one year therapy with oral lumbrokinase enteric-coated onsecondary ischemic stroke prevention.
• This is a multicenter, randomized, parallel group and controlled study that begantreatment in hospitalized patients with ischemic stroke and continued for 12 months.
• A total of 310 patients were enrolled:• 192 patients in the treatment group (standard stroke Tx plus enteric-coated
lumbrokinase capsul)• 118 patients in the control group (standard stroke Tx)
• Primary Outcome:All cause mortality; any event of reccurent IS/TIA, haemorrhagic stroke. MI/Angina,and other noncerebral ischemia or haemorrhage

Blood Indexes
(P < 0.05)
(P 0.013)
(p >0.05)
(p >0.05)

The Anti-thrombosis Action Prevention Of Pathologic Coagulation due toInhibiting 0f ICAM-1 Expression
European Journal Of Pharmacology 2008
12.12
12.3212.312.23
Before After
PT (seconds)Lumbrokinase Control
30.0430.3
30.45
30.73
BEFORE AFTER
APTT (seconds)Lumbrokinase Control
Unchanged, p >0.05
Unchanged, p >0.05
Lumbrokinase • Does Not Affect Physiological
Coagulation System• It May Reduce The Risk Of
HemorrhageChin Med J 2013;126 (21)
the content of PT and APTT were
unchanged (P >0.05)

1,38±0.52 1,40±0.79
1,62±0.561,59±0.69
1.2
1.3
1.4
1.5
1.6
1.7
LEFT RIGHTIM
T, m
m
Bilateral Carotid IMT
Control GroupBEFORE TX
AFTER TX
*P <0.001*P =0.055
CIMT – A Surrogate MarkerPerbaikan CIMT mengindikasikan
perbaikan atherosclerosis
diseluruh tubuh
1,26±0.49 1,25±0.51
1,09±0.40
1,06±0.35
0.9
1
1.1
1.2
1.3
LEFT RIGHT
IMT,
mm
Bilateral Carotid IMT
Treatment Group BEFORE TX
AFTER TX
*P <0.001
Intima-Media Thickness
(IMT)

Vascular endpoint (n(%))

Kaplan Meier survival
analysis showed a
significant reduction of
total vascular events,
falling by 4,7% in
treatment group

6,78 % 2,08 %
Vascular Endpoint
CONTROL; Standard Stroke TX
TREATMENT; Std Stroke TX + Tromboles

Summary• Diabetes is chronic progression disease, need to early intensification therapi to prevent
complications• Microvascular and macrovascular • The Role of Lumbrokinase in The Management of Thrombotic Disorder
Microvascular Disorders Diabetic Polyneuropathy
Improved Microcirculation and Nerve Conduction Diabetic Nephropathy
Markedly Reduced Albuminuria Improved the glomerulosclerosis and tubulointerstitial fibrosis
Micro/Macrovascular Disorders Stable Angina Pectoris: Improved Myaocardial Perfusion Acute Limb Ischemia (ALI): Improved Symptoms ang Signs at day-4Macrovascular Disorders as an Oral Fibrinogen Depleting Agent: Improved Carotid Atherosclerosis and
Improved Vascular Endpoints• Safe And Effective Supportive Measure In The Management Of Diabetes Mellitus Microvascular And
Macrovascular Complications Prevention And Treatment


After 6 mo Therapi:
NIHSS scores were signifivanly improve in both group (p<0.001)
After 1 year:
A further reduction in both group,significance reduction in treatment group (p,0.001)

Penderita angina pektoris diberikan tambahan Tromboles sehari 3 kali 2 kapsul,setelah penggunaan selama 30 hari, dievaluasi dengan Tc-Sestamibi didapatibahwa 70% dari penderita yang mengkonsumsi Tromboles perfusi myocardmembaik bermakna vs kelompok tanpa Tromboles, dan rasa nyeri dadamenghilang (p<0.001), tanpa efek samping.
One month treatment of oral Tromboles (lumbrokinase) resulted in an improvement myocardialperfusion in stable angina pectoris with metabolic syndrome without bleeding complication
MICRO AND MACROVASCULAR DISORDERS
The Role of TROMBOLES