Embed Size (px)
Citation preview

علیکم السلام

Dr Khesal AhmadPG Scholar, NIUM

CONTENTS
Prostate……..Anatomy
Surface , Lobes, RelationsSize, weight
PhysiologyFunctions, PSA
PathologyBPHProstatitis(Acute & Chronic)Prostatic AbscessBOOCA Prostate

Definition :Prostate is a fibromuculoglndular structure situated between the neck of
the bladder and external urethral sphincter and surround the prostatic urethra, it is conical in shape
SurfaceIt has 3 surfaces1. Anterior2. posterior3. Two inferio-lateral
Lobesit has 5 lobes1.Anterior2.Posterior3.Median4.Two Lateral
Anatomy

Size: About 3cm vertically , 4cm Transversally at base and about
2cm antero-posteriorly.
Weight:15-20 gm
NoteAdenoma usually occurs in medial and lateral lobes, it never occurs in ant & pos lobe because they are mainly of fibromuscular tissue & devoid of glandular structures

Parts of prostate




The prostate is related to the two capsules and one fascia behindCapsule:1. True Capsule
Formed by the condensation of the prostate at periphery
2. False CapsuleFormed by the visceral layer by the pelvic fascias(The prostatic venous plexus lies between these capsules)
3. Surgical CapsuleFormed by the non adenomatous tissue of the prostate which
is pushed by the hypertrophied gland to the periphery
Fascia Behind the Prostateit is also known as rectovesical, prostatoperitonial,denivillier’s fascia
Fascial Relations

inside and around the prostate
Urethra is divided into three parts1. Prostatic urethra(Widest and most dilatable part)
2. Membranous urethra (Shortest and least dilatable part)
3. Spongy Urethra
Sphincters A. Internal Sphincter(Sphincter Vesicae) at the neck of BladderB. External Sphincter or sphincter urethrae
Structures

Base Neck of BladderInferior External Urethral sphincterPosterior Danovillir’s fasciaLateral Levator ani
Blood SupplyInternal Iliac artery(Inferior Vesical and middle rectal arteries)
Venous drainage: Same as via posterior venous plexus but some drainage also occurs valve less vertebral plexus which is responsible for haematogenous spread of Ca of prostate to the bones of vertebra etc
Lymphatic DrainageInternal Iliac Lymph Node
Relations

1. The testicular hormone regulate the prostate, Testosterone is secreted by leydig cells of the testes, in the absence of the both testis (Testicular hormones) the prostate fails to develop.
2. The prostate secrete the specific fluid (Prostatic fluid( which provide 10-20% volume of ejaculation, it contains the prostaglandin enzymes and acid phosphates, it has anti bacterial property which helps to prevent UTI.
3. Prostate also secretes a glycoproteinous fluid which is known as PSA, The PSA actually liquefies the semen and allows the sperm to swim freely, and it is the best tumor marker for Ca prostate
Physiology of the Prostate

Normal Value of PSA
Less than 4 nmol/ml Normal4-8 nmol/ml BPH9-10 nmol/ml Diagnostic for BPH & suggestible for CA
More than 10 mol/ml Suggestive for CA Prostate

BPH

Benign prostatic hyperplasia is the histological pattern of the prostate, characterized by proliferation of smooth muscle and epithelial cells within the prostatic transition zone. This may lead to prostatic enlargement.
It is considered a normal part of aging in men and is hormonally dependent on testosterone and DHT production.
50% of men develop BPH by age 60 years and 90% by age 85 years.
Benign Prostatic Hyperplasia

It is involuntary hyperplasia due to disturbance of the ratio and quantity of circulating androgens and estrogens.
BPH is a benign neoplasm, also called as fibromyoadenoma.
With age TS level drops slowly. But fall of oestrogen level is not equal. So prostate enlarges through intermediate peptide growth factor.
BPH arises from submucosal glands of periurethral transitional zone with stromal proliferation and adenosis. It eventually compresses the peripheral zone and enlarges as lateral lobe.
BPH arising from subcervical glands of central zone enlarges as middle lobe projecting up into the bladder.
CAUSES


International prostate symptom score
1-7 = mild 8-19 = moderate 20-35 = severe

American Urological Association

Per rectal examination
1. Size- upper pole is easily reached/with difficulty/not reachable.2. Consistency- Rubber/soft/firm/hard.3. Rectal mucosa- Gliding/fixed4. Surface- Smooth/nodular.5. Tenderness- Absent/Present6. Median Sulcus- Prominent/palpable/obliterated

Grading of BPH
By P/R ExaminationGrade I---Upper pole easily reachableGrade II---Upper pole reachable with difficultyGrade III--- Can’t be reachable
By WeightNormal Weight --------18-20 gmGrade I up to --------upto 25gmGrade II upto --------upto 50gmGrade III upto --------upto 70gmGrade IVupto --------upto 80 gmGrade V upto -------->80 gm


Secondary changes due to prostate enlargement.
Changes in the urethra:Enlargement of the prostatic urethraExaggeration of the normal posterior curvature of the prostatic urethraUrethra compressed laterally reducing it to an A-P slit
Changes in the urinary Bladder: Compensatory hypertrophy of the vesical detrussor Trabeculation of bladder wall.Hypertrophy of the trigone.Formation of diverticulaFormation of pool of residual urine- cystitis,calculus
Changes in ureters and kidney:Hydroureter and HydronephrosisVesicoureteric reflux- Ac. & Chr. Pyelonephritis



PROSTATITISTypesAcute or chronic.
Causes: Due to instrumentation. Ascending infection from below. Haematogenous. Descending infection from above.
Bacteria involved: E. coli, Klebsiella, Proteus. Staphylococcus. Streptococcus faecalis. Gonococcus
Acute Prostatitis

Clinical features:
Pain, frequency, fever with chills and rigors. Retention of urine.
Perineal heaviness, pain on defaecation.
Tender prostate on per rectal examination. Initial fraction of urine is turbid which is sent for cultureand sensitivity.

Caused by E. coli, Staphylococcus, Streptococcus, Trichomonas,Chlamydia.
There is always associated posterior urethritis.Epididymitis. Pain in the perineum, rectum, low back pain, leg pain. Fever. Sexual dysfunction. Per rectal examination shows tender prostate. Prostatic fl uid obtained by prostatic massage shows 15 or more pus cells/HPF.
Chronic Prostatitis

It is infection, suppuration and pus formation in the prostate gland. Presentation is fever, rigors, perineal pain, urinary disturbances, and tender Soft fluctuant swelling in the prostate onrectal examination. Often presentation may be retention of urine. Total count will be increased. Urine will show pus cells. US is diagnostic. US is often done over perineum also. Treatment is antibiotics; US guided aspiration transperineally in lithotomy position or transperineal incision and drainage. Suprapubic cystostomy is better in case of retention of urine. After drainage antibiotics are needed for longer period of 6 weeks to prevent recurrent infection.
Prostatic Abscess

BLADDER OUTLET OBSTRUCTION (BOO)
It is low urinary flow rate with the presence of high voiding pressure. It is an urodynamically confirmed entity. It is diagnosed by urodynamic pressure flow study. Flow rate will be les than 10 ml/second with voiding pressure more than 80 cm of water. Eventually detrusor inefficiency occurs causing significant residual urine.

Causes of BOO—BPH; bladder neck hypertrophy or stenosis; carcinoma of prostate; urethral stricture; functional bladder neck obstruction.
Effects of BOO—acute retention of urine; chronic retention of urine; impaired bladder emptying; uraemia; infection; stone formation, haematuria.
US; renal function tests; IVU; PSA are the investigations.
Management is by treating the cause by cystoscopic bladderneck incision, urethrotomy; TURP, etc.

It is the most common malignant tumour in men over 65 years.
Carcinoma prostate occurs in peripheral zone in prostatic gland proper, i.e. commonly in posterior lobe. So prostatectomy for BPH does not confer protection against development of carcinoma prostate.
Incidence of prostate cancer in men over 80 years is 70%.
CARCINOMA PROSTATE

Microscopically latent Tumours incidentally found either by TURP or by PSA estimation Early localised carcinoma Advanced local prostatic carcinoma Metastatic carcinoma either into the bone commonly or other organs
Types of carcinoma prostate
Histology: It is an adenocarcinoma, wherein there is loss of myoepithelial cell layer which normally surrounds the prostatic glands (Gleason). Glands here appear in confluence. Grading of carcinoma is based on dedifferentiation as proposed by Gleason.

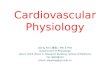
Staging of carcinoma prostateOccult—Diagnosed after investigation due to sus picionStage I—Tumour confi ned to prostate/local noduleStage II—Tumour involving capsule or diffuse typeStage III—Tumour involving seminal vesicleStage IV—Extension into adjacent tissue
Staging of Ca prostate (A) Occult, (B) Stage I, (C) Stage II, (D) Stage III, (E) Stage IV.
A
ED
CB

شکریہ




![A numerical simulation study of the dual role of 5α ... · BPH consists of the progressive enlargement of the prostate with ... [1–3]. This pathology only develops in the central](https://img.pdfslide.tips/doc/110x75/5f1cf29932fd7a79fb311813/a-numerical-simulation-study-of-the-dual-role-of-5-bph-consists-of-the-progressive.jpg)