Embed Size (px)
Citation preview
Quinolone Hypersensitivity
Sirinoot Palapinyo,RPh
Case• ผู้ป่วยหญิงไทย อายุ 43 ปี
• CC: เหนื่อย อ่อนแรงด้านซ้าย 7 วันก่อนมาโรงพยาบาล
• Underlying disease
• SLE with secondary APS with Hx of DVT Lt.leg
• Suspected renal vasculitis
• Moderate pulmonary hypertension
• OA knee
• Hypertension
• Allergy :
• Cotrimoxazole : MP rash
• Ceftriaxone : anaphylaxis
• Cefditoren : ไม่ทราบอาการ
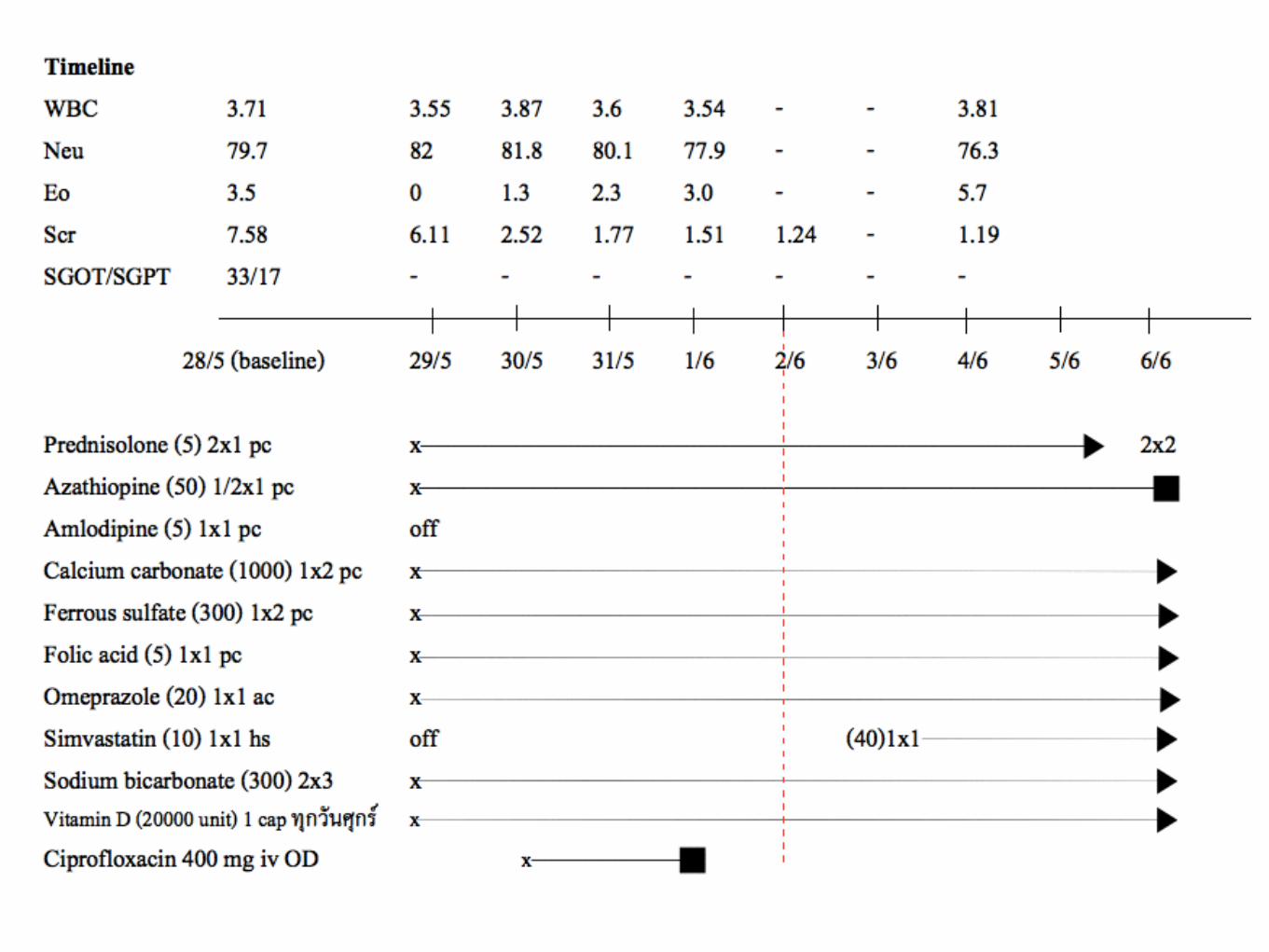
Case• Septic work up -> UTIs
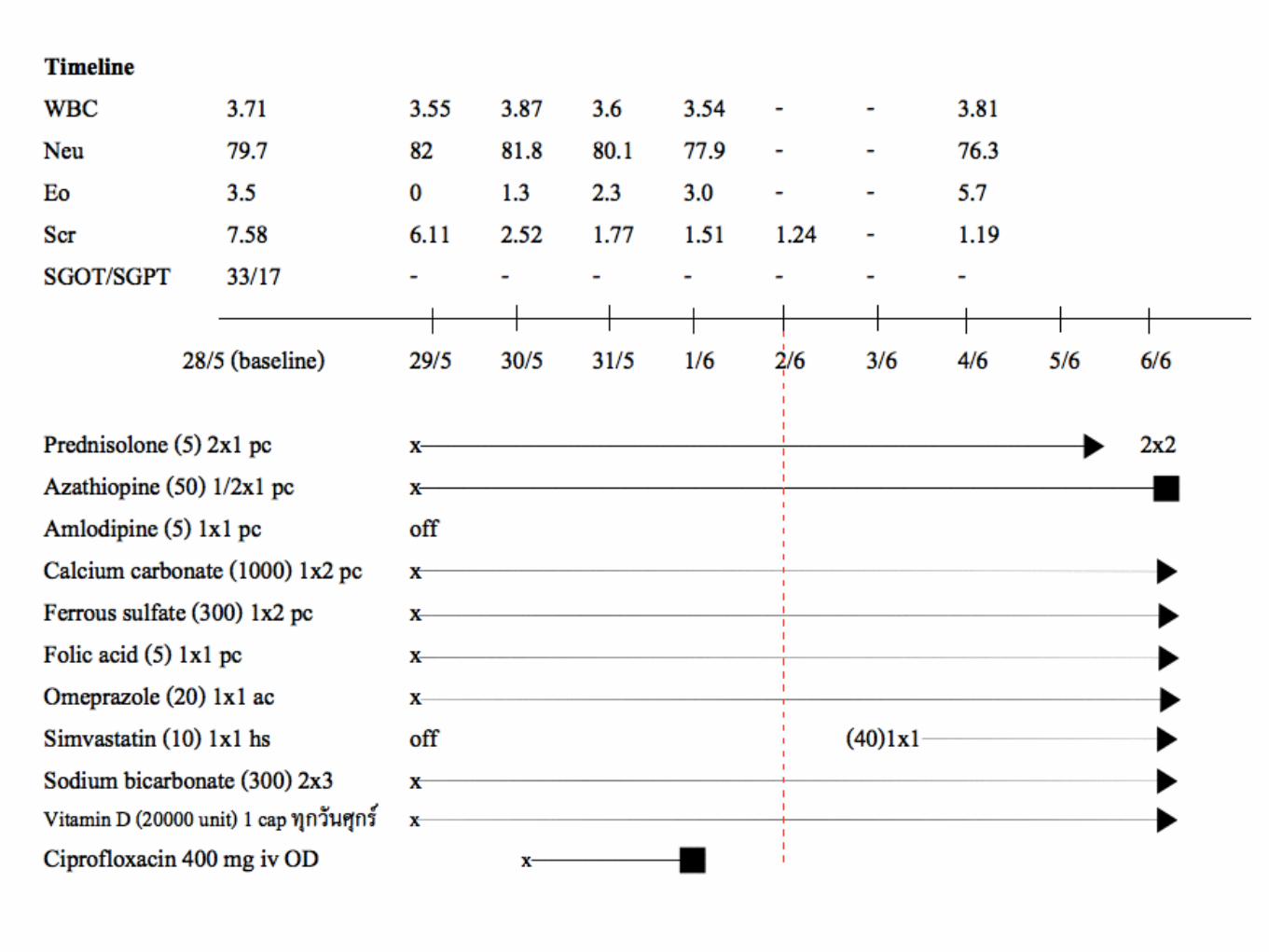
• Med : Ciprofloxacin 400 mg IV once daily
• หลังจากได้รับยาไป 3 วัน เริ่มมีผื่น generalized MP rash ขึ้นบริเวณแขน ฝ่ามือ ขา หน้าท้อง และหลัง (2/6/58)
• No mucosal involvement, No internal organ involvement
• Culprit drug : Ciprofloxacin
Case• จากประวัติการรักษาพบว่าผู้ป่วยเคยได้รับยา Ciprofloxacin 4 ครั้ง
• 5/1/55 : Ciprofloxacin (500) 1x2 pc นาน 15 วัน
• 29/3/55 : Ciprofloxacin (500) 1x2 pc นาน 10 วัน
• 1/8/56 : Ciprofloxacin (500) 1x2 pc นาน 7 วัน
• เคยได้รับยา Levofloxacin ทั้งรูปแบบฉีดและรับประทานรวมกัน 11 ครั้ง โดยไม่พบอาการไม่พึงประสงค์จากยา
Introduction
Introduction• History of ADR to antibiotics -> receive alternative
antibiotics which are sometimes less effective, often more toxic, and usually more expensive.
• Beta lactams & sulfa are most common -> lots of study
• Quinolones are the third most common class of drugs associated with hypersensitivity syndrome reactions (HSRs)
Neuman MG, et al, Quinolones-induced hypersensitivity reactions, Clin Biochem (2015)
Quinolone
• One of the largest classes of antimicrobial agents used worldwide
• The development of the quinolones
• 1962 with the discovery of nalidixic acid, the prototype 4-quinolone antibiotic
Neuman MG, et al, Quinolones-induced hypersensitivity reactions, Clin Biochem (2015)
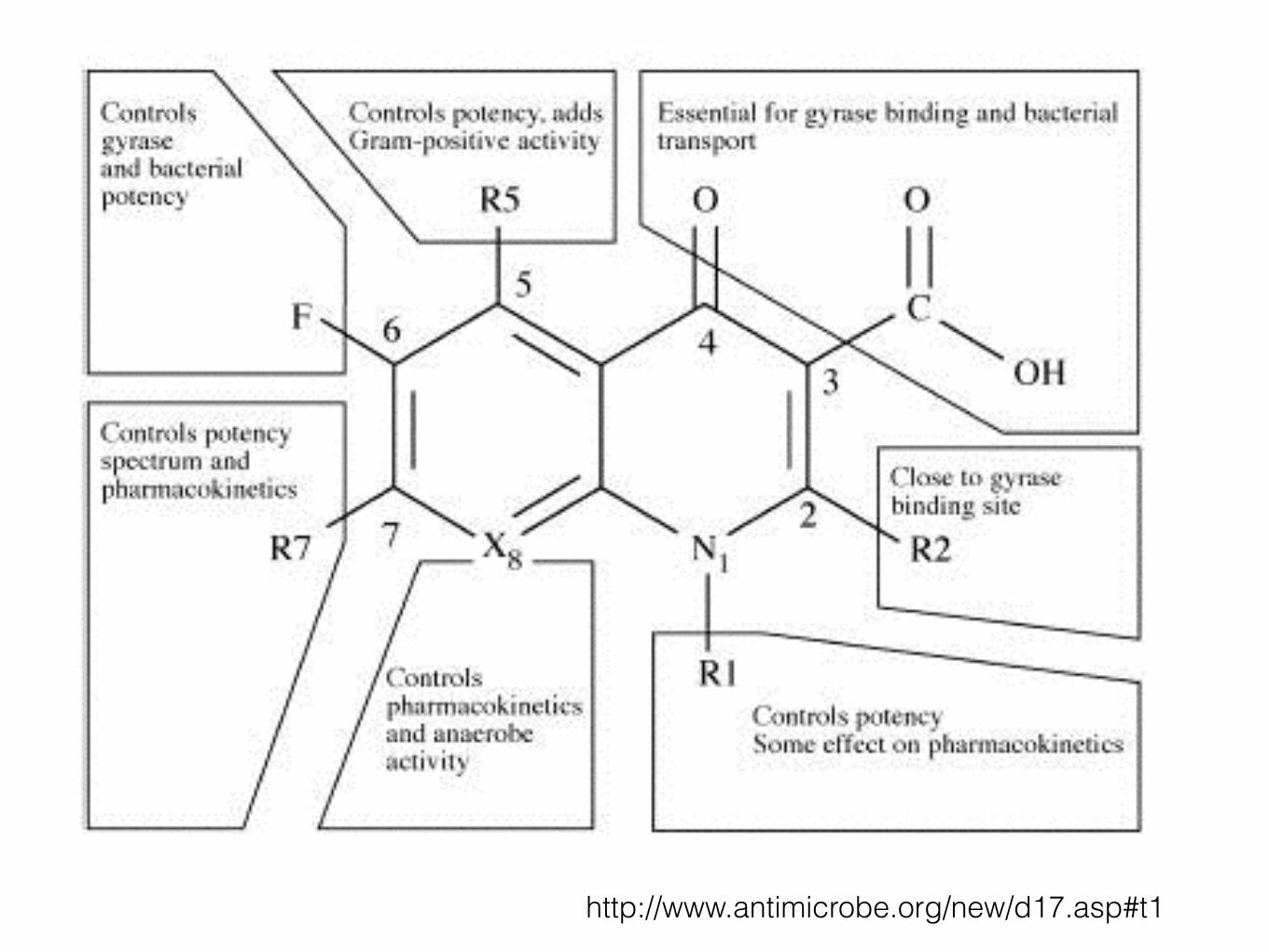
http://www.antimicrobe.org/new/d17.asp#t1
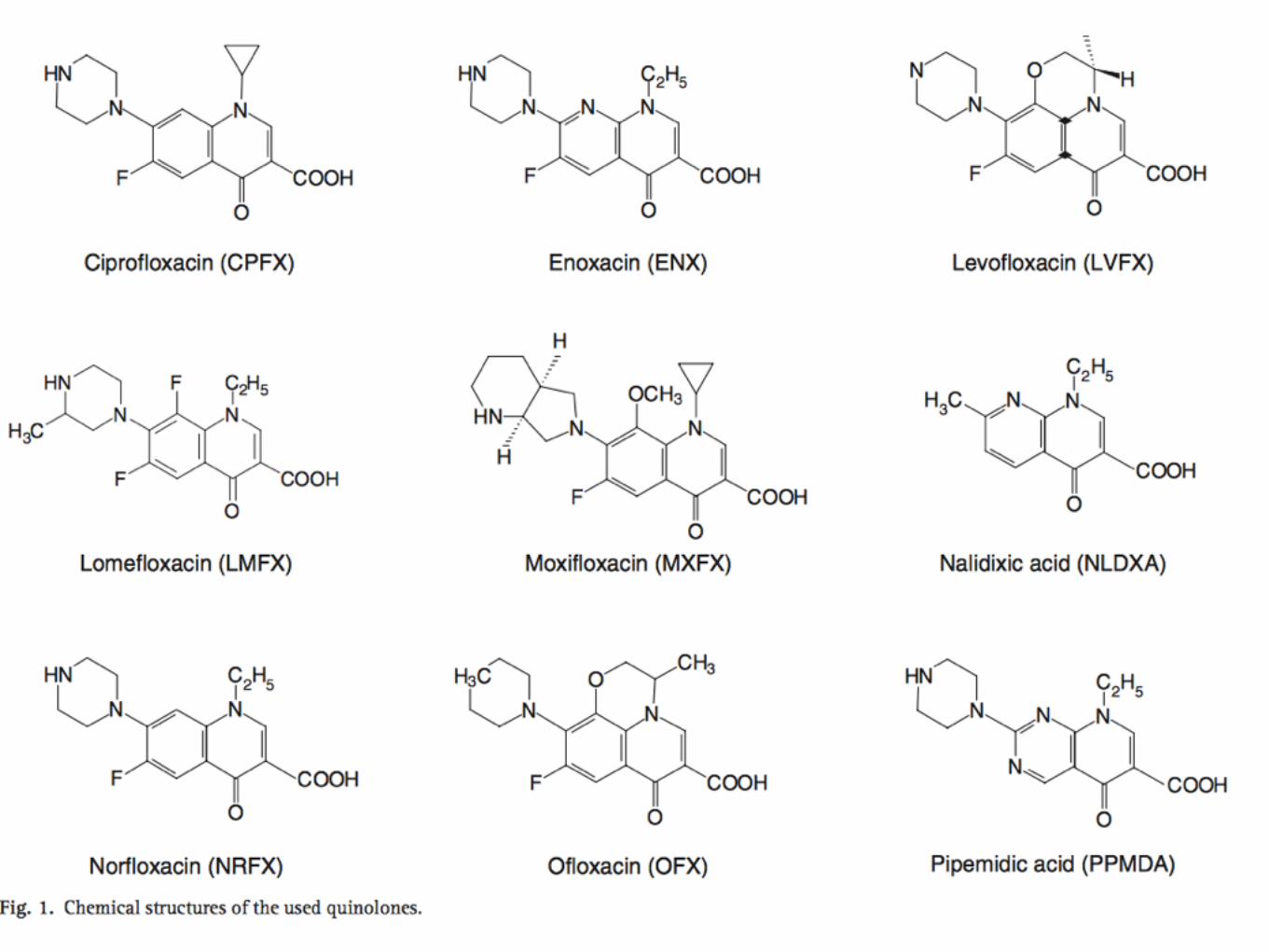
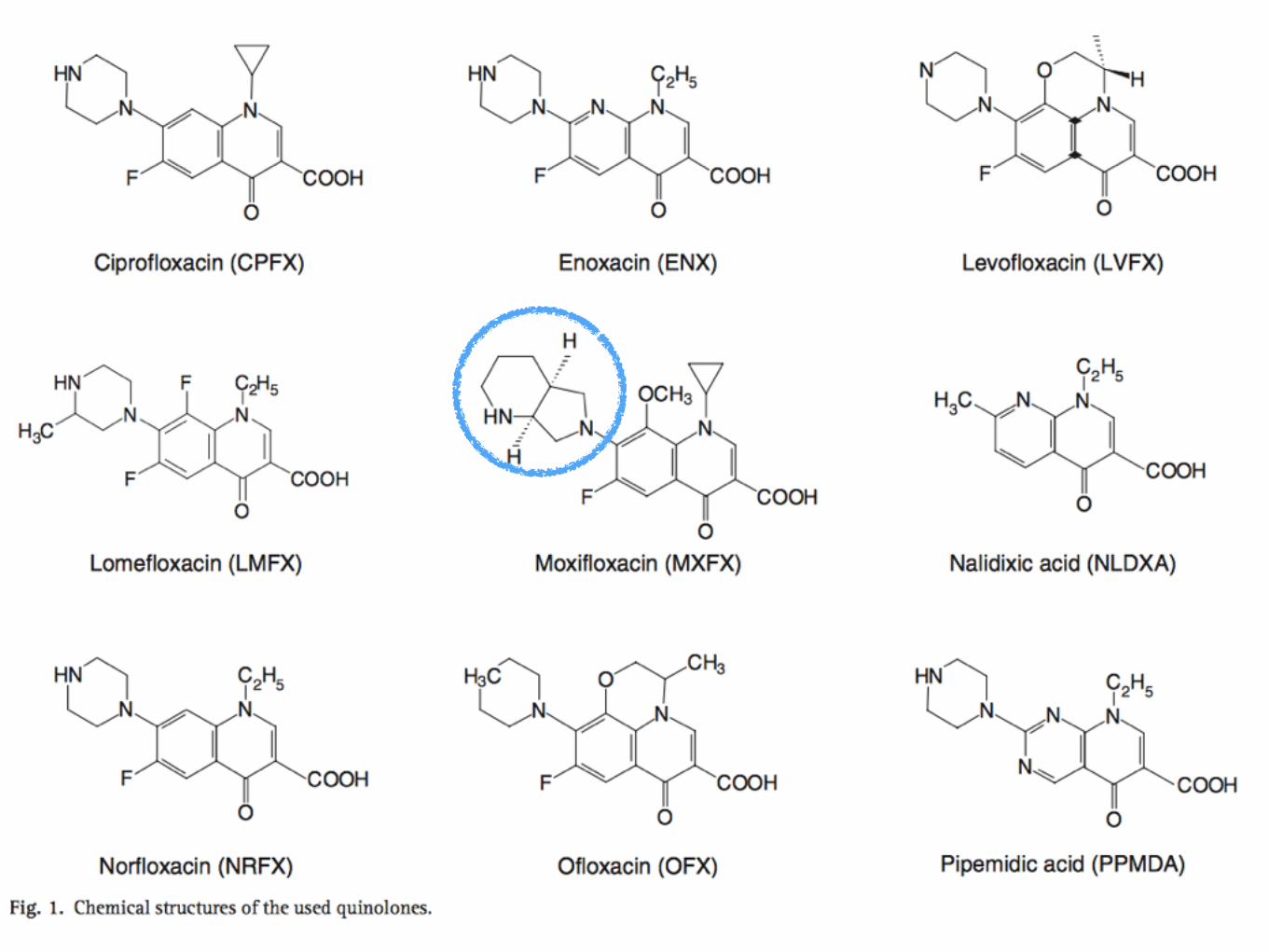
Quinolone• 4 groups, based on chemical structure and
antibacterial activity.
• First generation : Pipemidic acid
• Second generation : Ciprofloxacin, Norfloxacin and Ofloxain.
• Third generation : Levofloxacin
• Fourth generation : MoxifloxacinFluoroquinolone Safety and Tolerability, CID 2005:41 (Suppl 2)
Anaphylaxis and anaphylactoid (Type 1 hypersensitivity reactions)
• Urticaria, angioedema and anaphylactic shock were the most common immediate ADRs associated with quinolone
• Incidence of serious allergic reactions (Per 10,000 ; Siriraj)
• Moxifloxacin [4.3, 95% confidence interval (CI) 3.5–5.3]
• Ciprofloxacin (5.4, 95% CI 4.4–6.5)
• Levofloxacin (8.7, 95% CI 7.4–10.0)
Neuman MG, et al, Quinolones-induced hypersensitivity reactions, Clin Biochem (2015)
Anaphylaxis and anaphylactoid (Type 1 hypersensitivity reactions)
• In Europe
• Moxifloxacin was associated with the highest incidence of anaphylactic shock (57.1%),
• Levofloxacin (35.7%)
• Ciprofloxacin (7.1%)
Anaphylaxis and anaphylactoid (Type 1 hypersensitivity reactions)
• Incidence of anaphylaxis reactions to quinolones is on the rise
• Estimated at 1.8–2.3 per 10,000,000 days of treatment
• Mechanism is not well understood
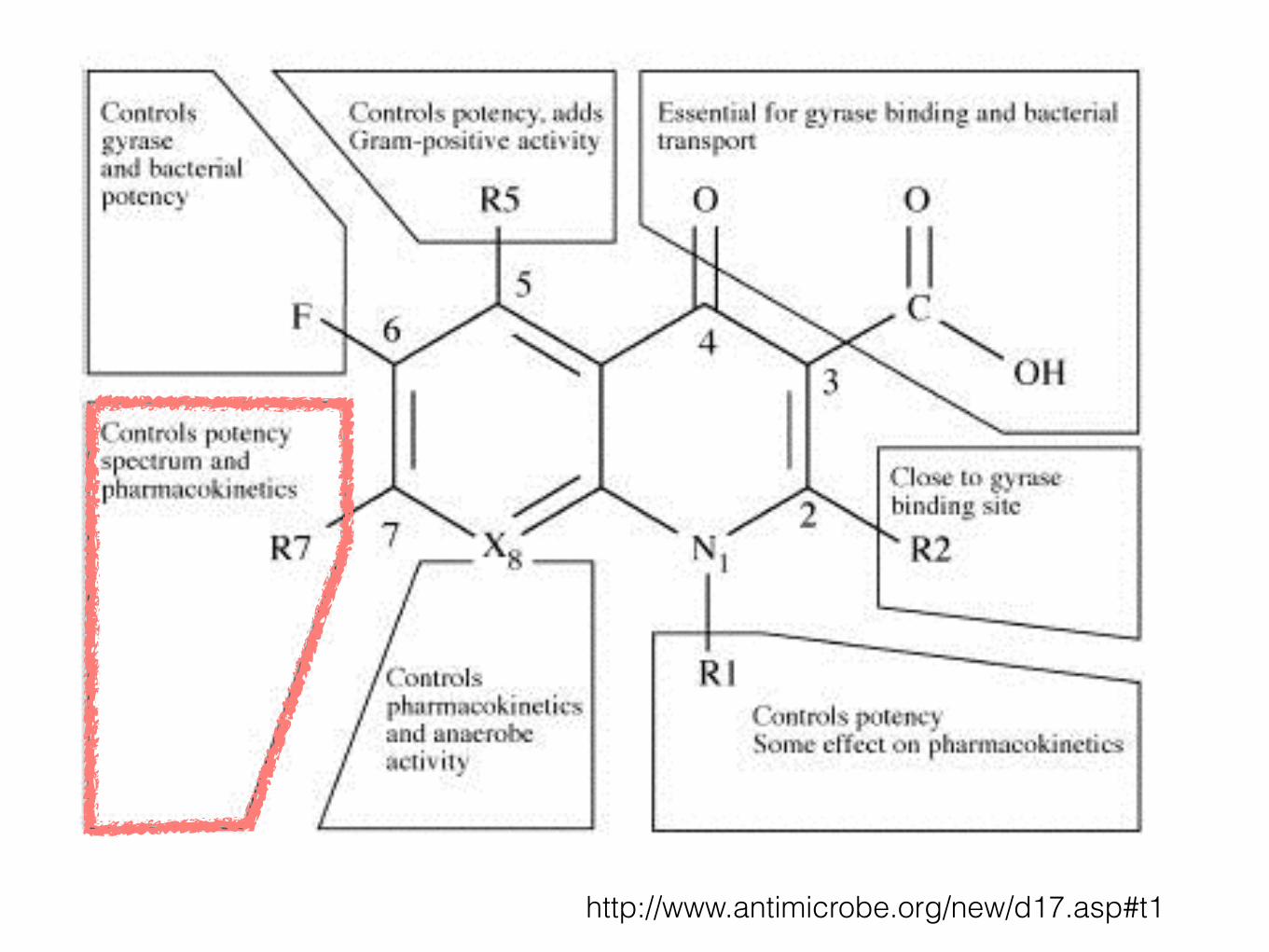
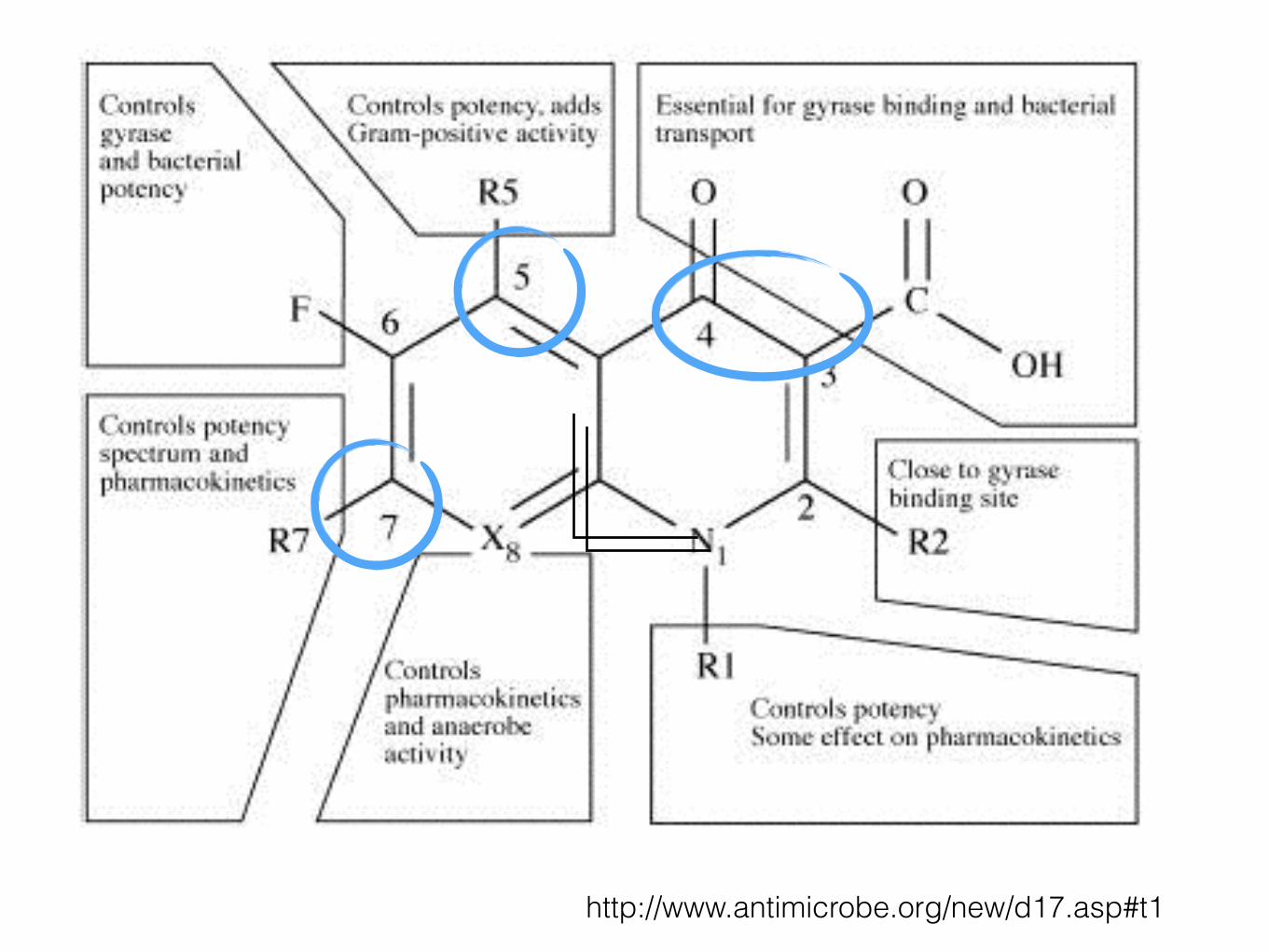
• IgE-molecule seems to induce a covalent binding between the substitute at position 7 of the quinolone-molecule and a unknown soluble protein
Neuman MG, et al, Quinolones-induced hypersensitivity reactions, Clin Biochem (2015)
http://www.antimicrobe.org/new/d17.asp#t1
Anaphylaxis and anaphylactoid (Type 1 hypersensitivity reactions) • The diagnosis of immediate hypersensitivity
reactions is often difficult
• Skin testing is not reliable Vs some authors consider skin testing useful
• A high number of false-positive results
• FQs induce direct histamine release
• Sensitivity for skin test : ~50%
Neuman MG, et al, Quinolones-induced hypersensitivity reactions, Clin Biochem (2015)
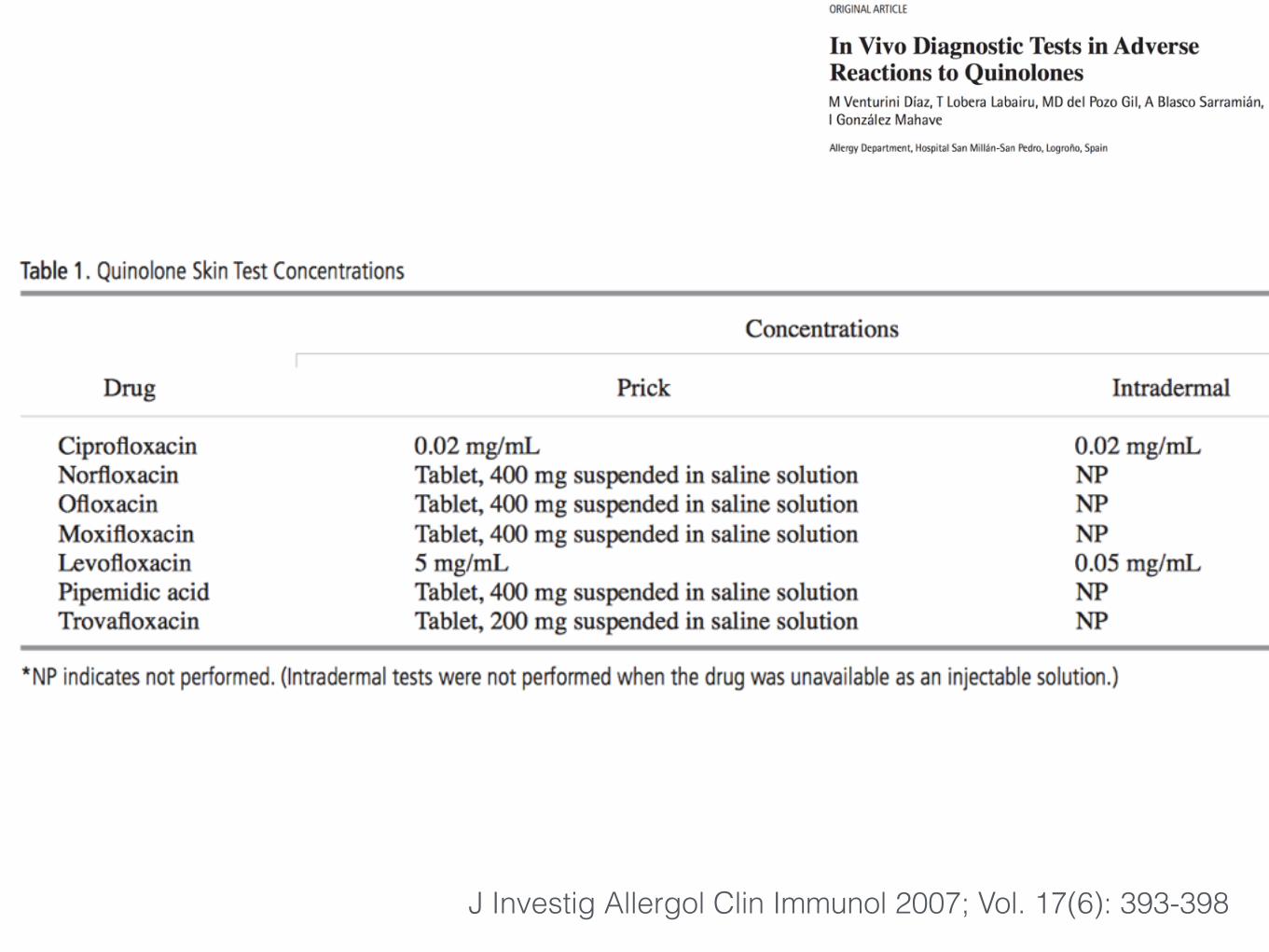
• Retrospective analysis of clinic cases
• 71 patients with reactions to a quinolone over a period of 5 years
• 12 with no history of allergy
• Skin prick test -> ID -> DPT
J Investig Allergol Clin Immunol 2007; Vol. 17(6): 393-398
J Investig Allergol Clin Immunol 2007; Vol. 17(6): 393-398
Results
• 34 patients were diagnosed with quinolone hypersensitivity:
• 21 diagnosed by means of positive skin tests
• 7 diagnosed by means of challenge tests (5 with positive skin tests and 2 with negative skin tests)
• 6 patients by means of a suggestive clinical history despite having negative skin tests
• 94% negative skin prick test -> negative DPT
• 50% positive skin prick test -> positive DPT
J Investig Allergol Clin Immunol 2007; Vol. 17(6): 393-398
Discussion
• Skin prick test useful before DPT
• Size of wheal : diameter of 4 mm in the prick test and 6 mm in the ID test was the usual size in false positive patients
• Wheal sizes were usually greater in true positives
J Investig Allergol Clin Immunol 2007; Vol. 17(6): 393-398
Anaphylaxis and anaphylactoid (Type 1 hypersensitivity reactions)
• The European Network for Drug Allergy of the European Academy of Allergology and Clinical Immunology recommends the use of drug provocation test (DPT) to confirm drug hypersensitivity
• Drug provocation test (DPT), which is not free of risk
J Investig Allergol Clin Immunol 2007; Vol. 17(6): 393-398
Anaphylaxis and anaphylactoid (Type 1 hypersensitivity reactions) • In vitro specific IgE to quinolones
• Sepharose radioimmunoassay (Sepharose-RIA)
• Sensitivity of 54.5%
• In vitro tests detecting only free serum IgE but not cell-bound
• Level of the specific serum IgE does not correlate with the severity
• Considering only the patients tested within 8 months of the ADRs
• Cross-reactivity: common core structure of quinolones predisposes
• Basophil activation test (BAT)
Detection of specific IgE to quinolones, JACI 2004
• “In vitro evaluation of IgE-mediated hypersensitivity reactions to quinolones” in Allergy 2011
• Evaluated 38 patients with confirmed immediate allergic reactions to quinolones.
• Those with anaphylaxis were considered allergic by clinical history, once other possible causes were ruled out
• Those with urticaria by drug provocation.
• Sepharose-radioimmunoassay (RIA) and basophil activation test (BAT)
• Culprit drug : Ciprofloxacin, Moxifloxacin & Levofloxacin
- J Investig Allergol Clin Immunol. 2010;20(7):607-11. - Allergy 2011; 66: 247–254.
• “In vitro evaluation of IgE-mediated hypersensitivity reactions to quinolones” in Allergy 2011
• Results:
• Sepharose-RIA was positive in 12 cases (31.57%)
• 8 (21%) were positive to ciprofloxacin
• 7 (18.4%) were positive to moxifloxacin
• 7 (18.4%) were positive to levofloxacin.
• BAT was positive in 27 (71.05%).
• Sepharose-RIA and BAT were repeated in positive cases 1 year later, detecting a decrease in all cases, with four becoming negative.
• Conclusion:
• BAT is a useful method for diagnosing patients.
• Specific IgE was demonstrated by Sepharose-RIA and inhibition assay.
- J Investig Allergol Clin Immunol. 2010;20(7):607-11. - Allergy 2011; 66: 247–254.
Immune-mediated severe cutaneous hypersensitivity
reactions
Immune-mediated severe cutaneous hypersensitivity reactions
• Immune-mediated ADRs : Rare
• Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), fixed drug eruption (FDE), cutaneous vasculitis, maculopapular exanthema, serum sickness-like disease, and acute generalized exanthematous pustulosis (AGEP)
• Hemolytic uremic syndrome, hemolytic anemia, thrombocytopenia, leukopenia or pancytopenia, acute interstitial nephritis, pacute pancreatitis, hotosensitization, acute hepatitis and acute cholestatic jaundice and eosinophilic meningitis
Neuman MG, et al, Quinolones-induced hypersensitivity reactions, Clin Biochem (2015)
Immune-mediated severe cutaneous hypersensitivity reactions
• Study in Europe
• HSR to fluoroquinolone (OR 3.09, 95% CI 1.16–8.24, p = 0.024)
• Common HSR manifestations were cutaneous (urticarial or exanthema)
• Moxifloxacin was the most commonly incriminated drug
• Moxifloxacin carries a higher risk of HSRs compared to levofloxacin and ciprofloxacin :141.3 vs. 40.8 and 26.3 emergency department visits/100,000 prescriptions
Curr Opin Allergy Clin Immunol 2011;11:285–91.
Immune-mediated severe cutaneous hypersensitivity reactions
• Cutaneous ADRs were the predominant type of ADRs (0.5-3.0%)
• Ciprofloxacin : 34.9% of all reported ADRs
• Moxifloxacin : 13.5%
• Levofloxacin : 19.9%
Curr Opin Allergy Clin Immunol 2011;11:285–91.
Immune-mediated severe cutaneous hypersensitivity reactions
• Retrospective study
• Voluntary reports (≥18 years of age) of any adverse events associated with fluoroquinolone
• Reported from January 2004 to December 2008
• From the Adverse Drug Reaction Center, Siriraj Hospital, Thailand
• Among 166,736 patients treated with FQ -> 155 enrolled
Dermatitis, Vol 22, No 3 (May/June), 2011: pp 155–160
Immune-mediated severe cutaneous hypersensitivity reactions
• Prevalence of ADRs from FQ was 0.13%
• Rate of cutaneous ADRs was 0.09% [0.04-0.37]
• Maculopapular rash (39.7%)
• Cutaneous ADRs
• Ciprofloxacinwas 0.37%
• Moxifloxacin 0.1%
• Levofloxacin 0.06% Dermatitis, Vol 22, No 3 (May/June), 2011: pp 155–160
Immune-mediated severe cutaneous hypersensitivity reactions
• SJS/TEN developed during 1–19 days after oral FQ
• 8.6% involved a previous history of FQ hypersensitivity
• 15.4% had cross-reactivity potential
Dermatitis, Vol 22, No 3 (May/June), 2011: pp 155–160
Immune-mediated severe cutaneous hypersensitivity reactions
• FQs were associated with a high risk of SJS/TEN in the EuroSCAR study (OR 6.9, 95% CI 1.8–27)
• FQs were identified as one of classes of drugs associated with SJS/TEN in a large sample of patients in a multinational cohort.
• SJS/TEN associated with FQs was found to occur exclusively in the first 2 months of treatment
Neuman MG, et al, Quinolones-induced hypersensitivity reactions, Clin Biochem (2015)
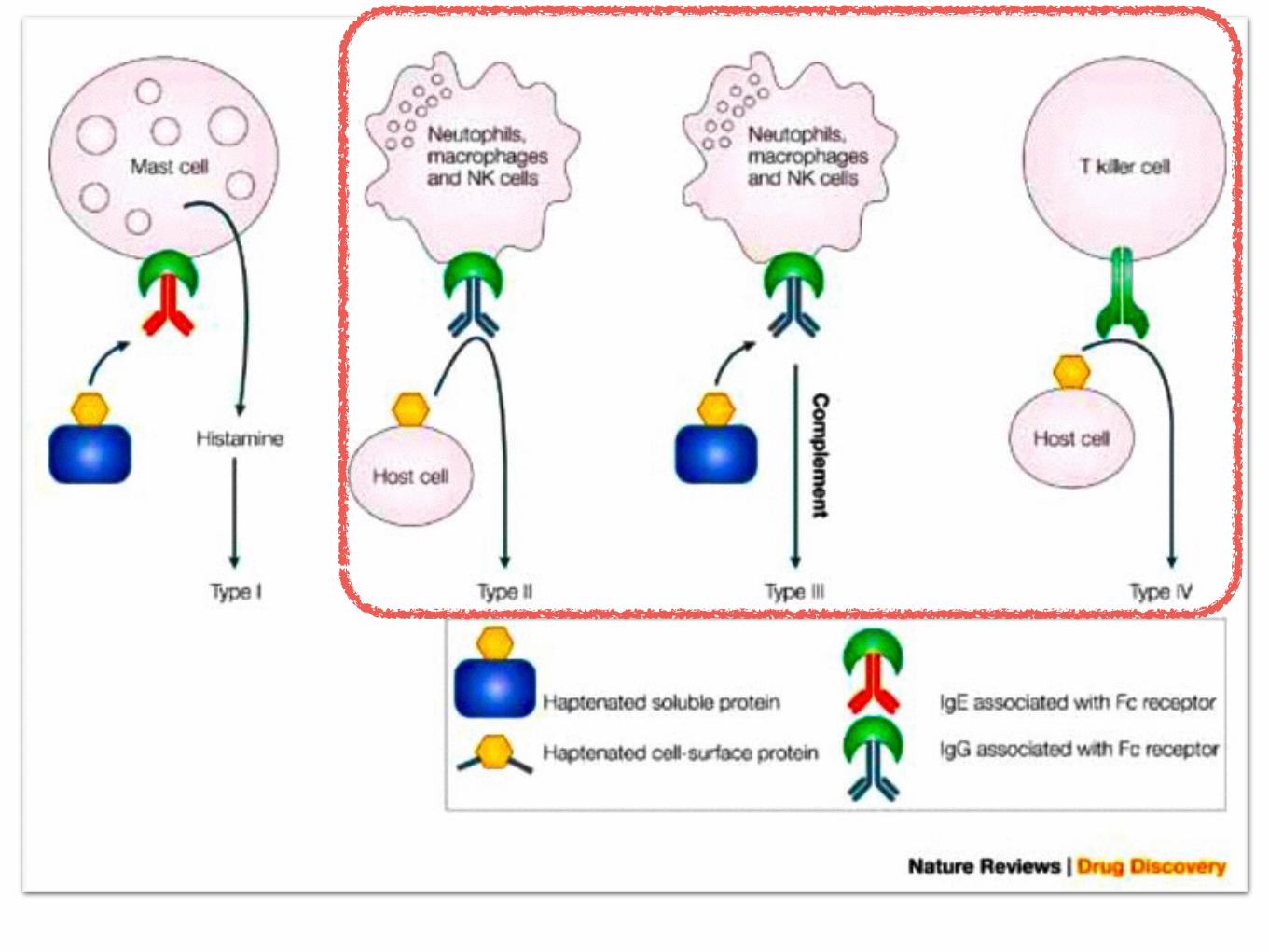
Immune-mediated severe cutaneous hypersensitivity reactions
• Immune-mediated ADRs
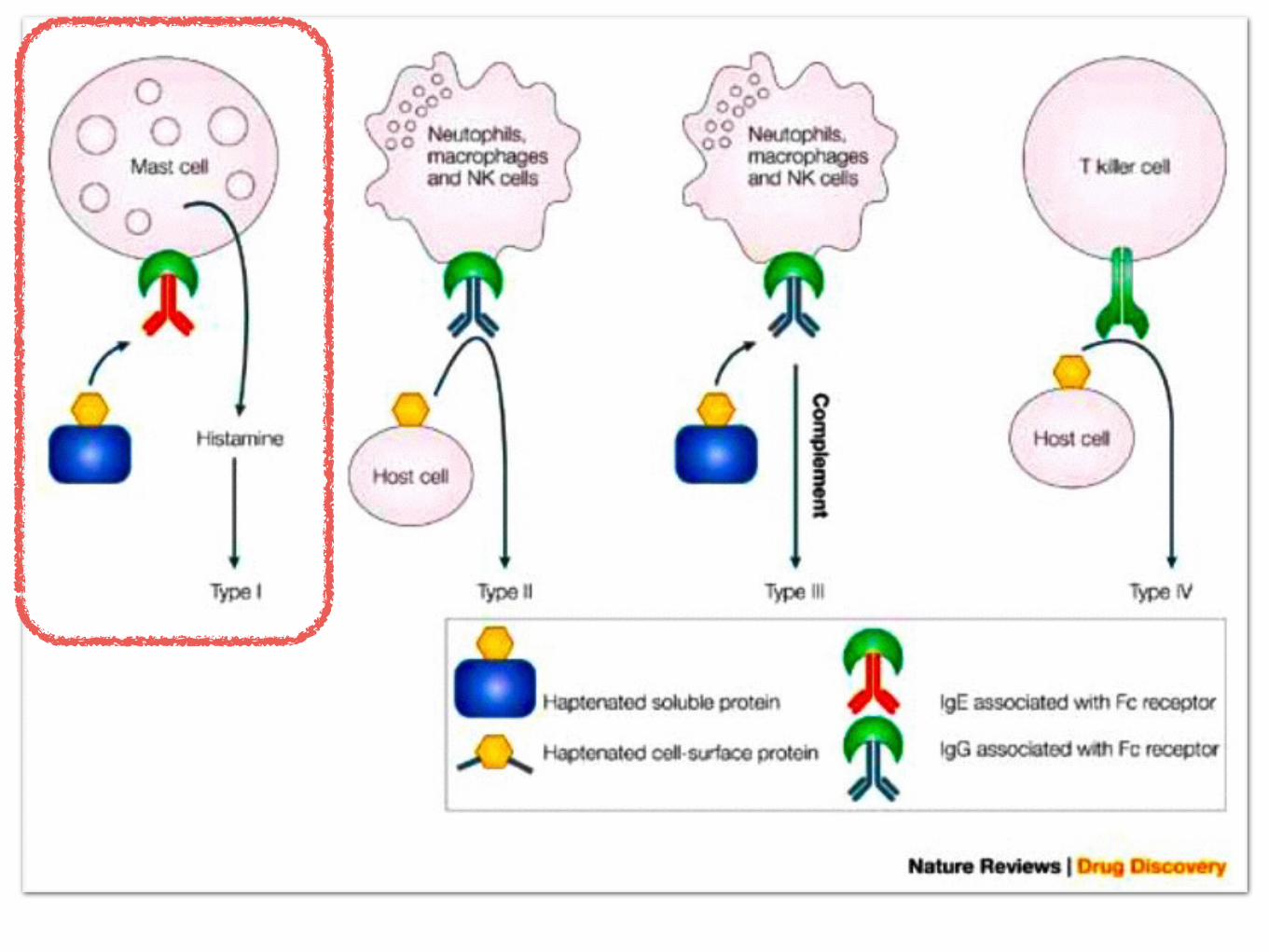
• Suspected mechanism
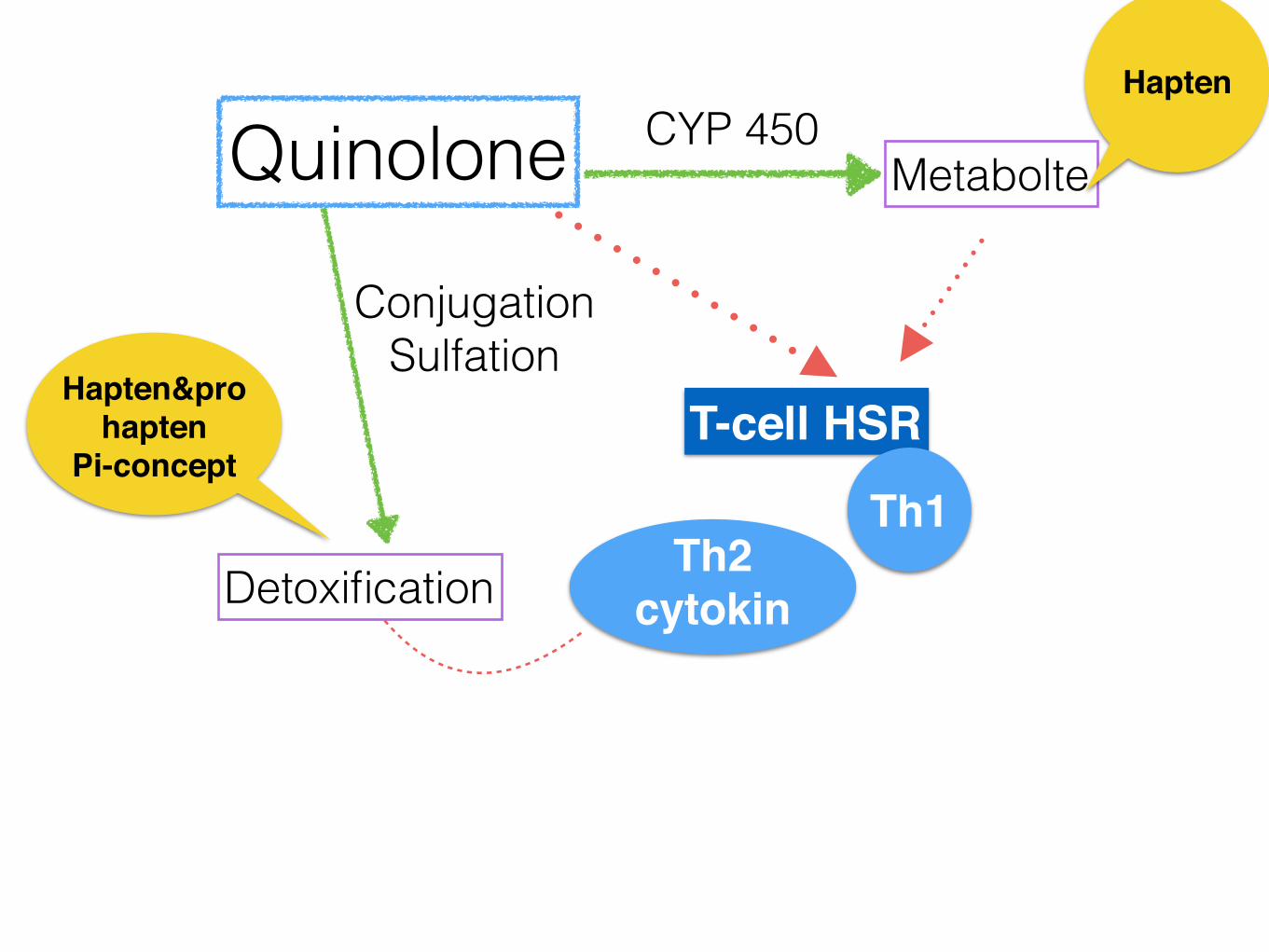
• Quinolones are suspected of causing HSR by both the hapten and the p–i concepts
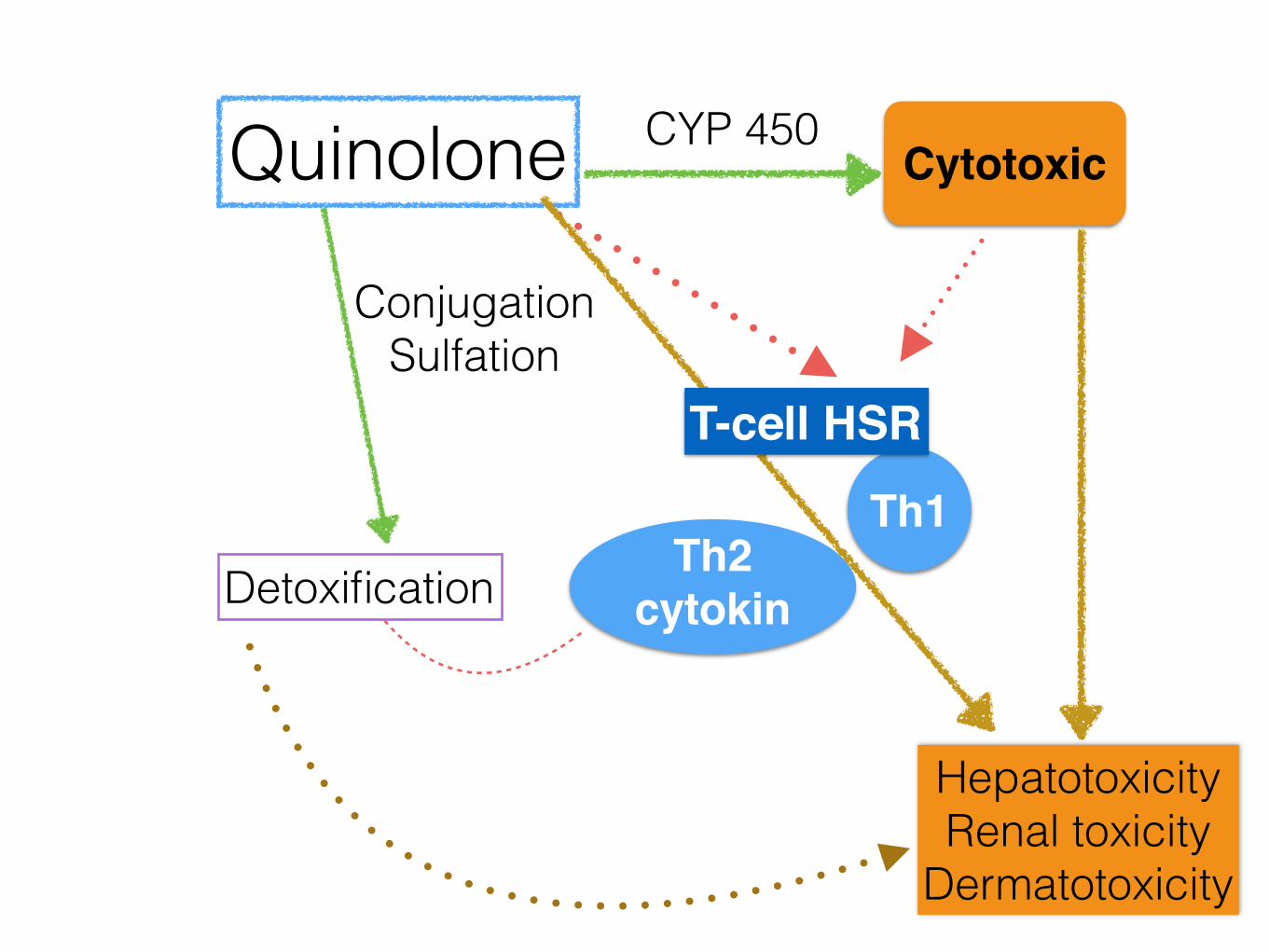
• Quinolone- induced toxicity
• Parent compound of quinolones (chemically not reactive) -> directly bind to the MHC-peptide/T cell receptors and stimulate T cells by pharmaceutical interaction (p–i)
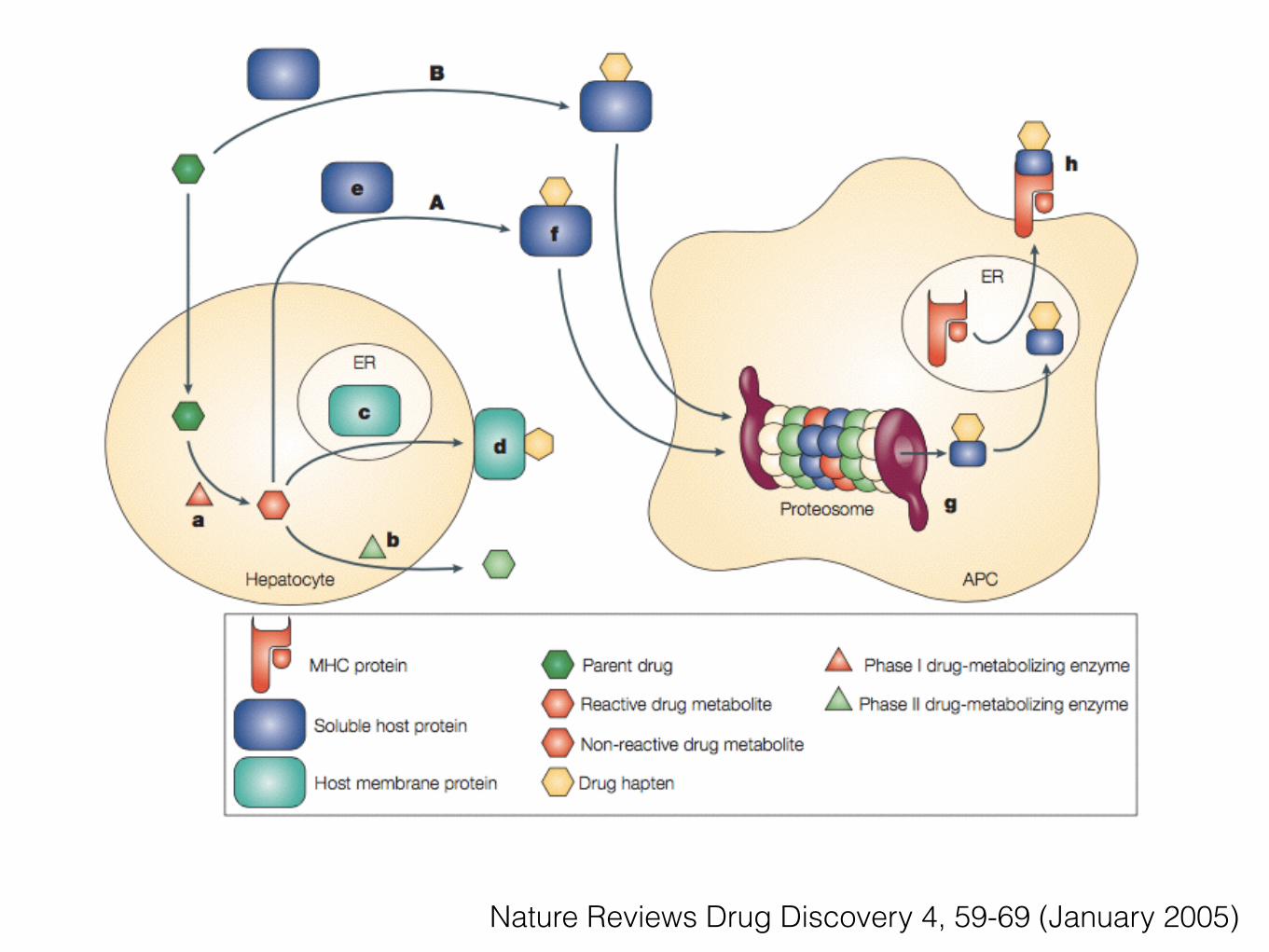
Nature Reviews Drug Discovery 4, 59-69 (January 2005)

http://www.antimicrobe.org/new/d17.asp#t1
Mechanisms and cross-reactivity• In vivo : patch test
• In vitro : lymphocyte proliferation test (LTT)
• Investigated through the generation and analysis (flow cytometry and proliferation assays) of quinolone-specific T cell clones (TCC).
• Results :
• The LTT confirmed the involvement of T cells because peripheral blood mononuclear cells (PBMC) mounted an enhanced in vitro proliferative response to CPFX and/or NRFX or MXFX in all patients.
• Patch tests were positive after 24 and 48 h in three out of the six patients.
• From two patients, CPFX- and MXFX-specific CD41/CD81 T cell receptor (TCR) ab1 TCC were generated to investigate the nature of the drug-T cell interaction as well as the cross-reactivity with other quinolones.
Clinical and Experimental Allergy,2006; 36, 59–69
T cell-mediated hypersensitivity to quinolones: mechanisms and cross-reactivity
• The use of 8 different quinolones as antigens (Ag) revealed three patterns of cross-reactivity:
• Clones exclusively reacting with the eliciting drug
• Clones with a limited cross-reactivity
• Clones showing a broad cross-reactivity
• The TCC recognized quinolones directly without need of processing and without covalent association with the major histocompatability complex (MHC)–peptide complex
• Glutaraldehyde-fixed Ag-presenting cells (APC) could present the drug and washing quinolone-pulsed APC removed the drug, abrogating the reactivity of quinolone-specific TCC.
Clinical and Experimental Allergy,2006; 36, 59–69
In Vitro (Ex Vivo)• Lymphocyte Transformation Testing (LTT)
• Lymphocytes isolated from peripheral blood mononuclear cells (PBMCs) of a patient with a specific delayed HSR
• Cultured with pharmacologic concentrations of the culprit drug
• After 5–7 days the amount of incorporated 3H-thymidine is determined and the result is expressed as a stimulation index.
• Enhanced proliferative responses in the presence of a drug are interpreted as drug-specific T-cell sensitisation.
• Most quinolone hypersensitivity study reported this technique
In Vitro (Ex Vivo)• ELISpot and Intracellular Cytokine Staining
• Similar to LTT, the enzyme-linked immunospot (ELISpot) assay and intracellular cytokine staining (ICS) have been used in the research
• Both ELISpot and ICS are ex vivo assays that are used to measure the production and release of a target cytokine(s) by a population of T-cells in relation to exposure to pharmacological concentrations of the suspected drug or drug metabolite
• Only 2 study showed ELISpot technique (Immediate type)

Take home message
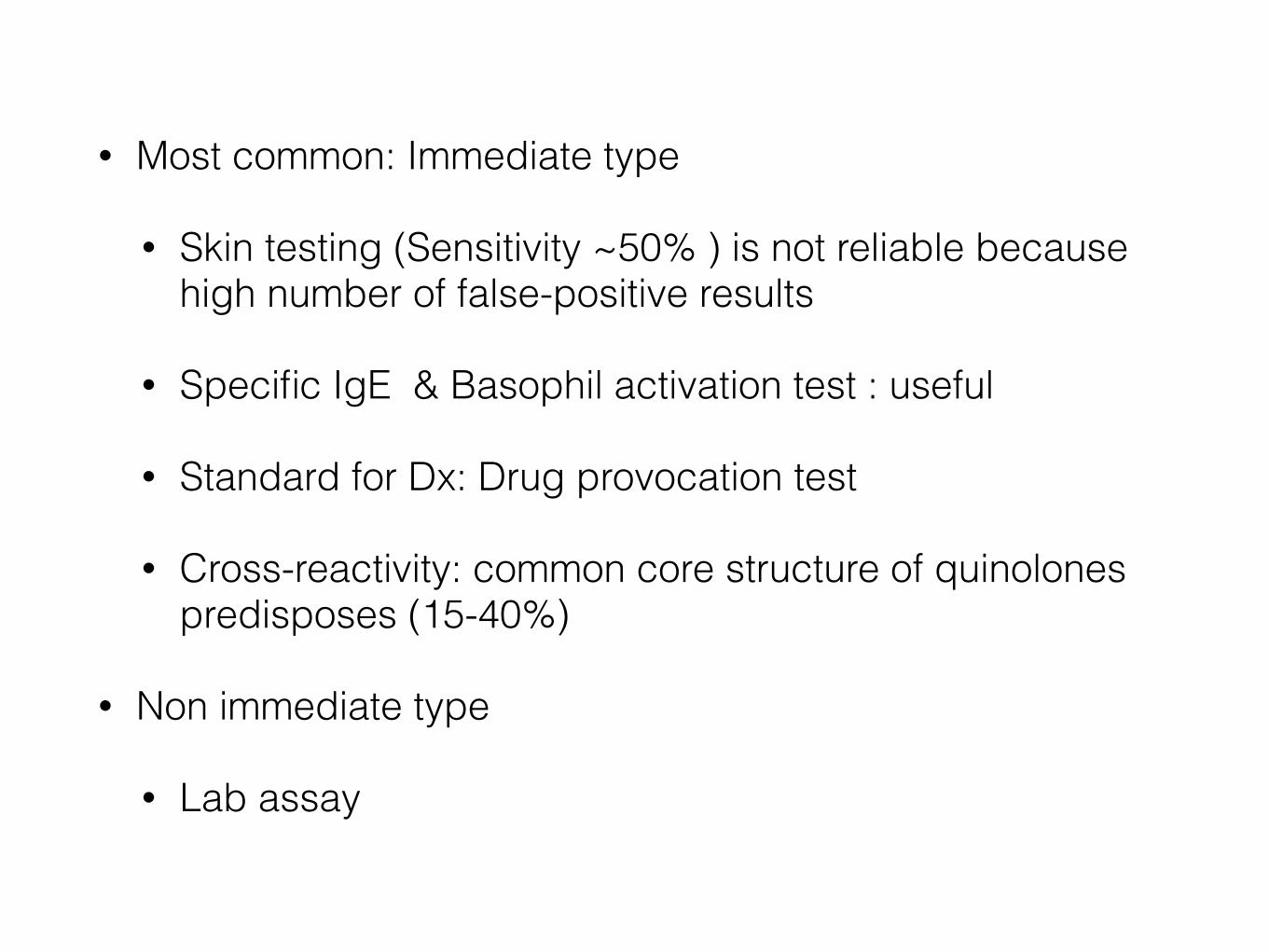
• Most common: Immediate type
• Skin testing (Sensitivity ~50% ) is not reliable because high number of false-positive results
• Specific IgE & Basophil activation test : useful
• Standard for Dx: Drug provocation test
• Cross-reactivity: common core structure of quinolones predisposes (15-40%)
• Non immediate type
• Lab assay
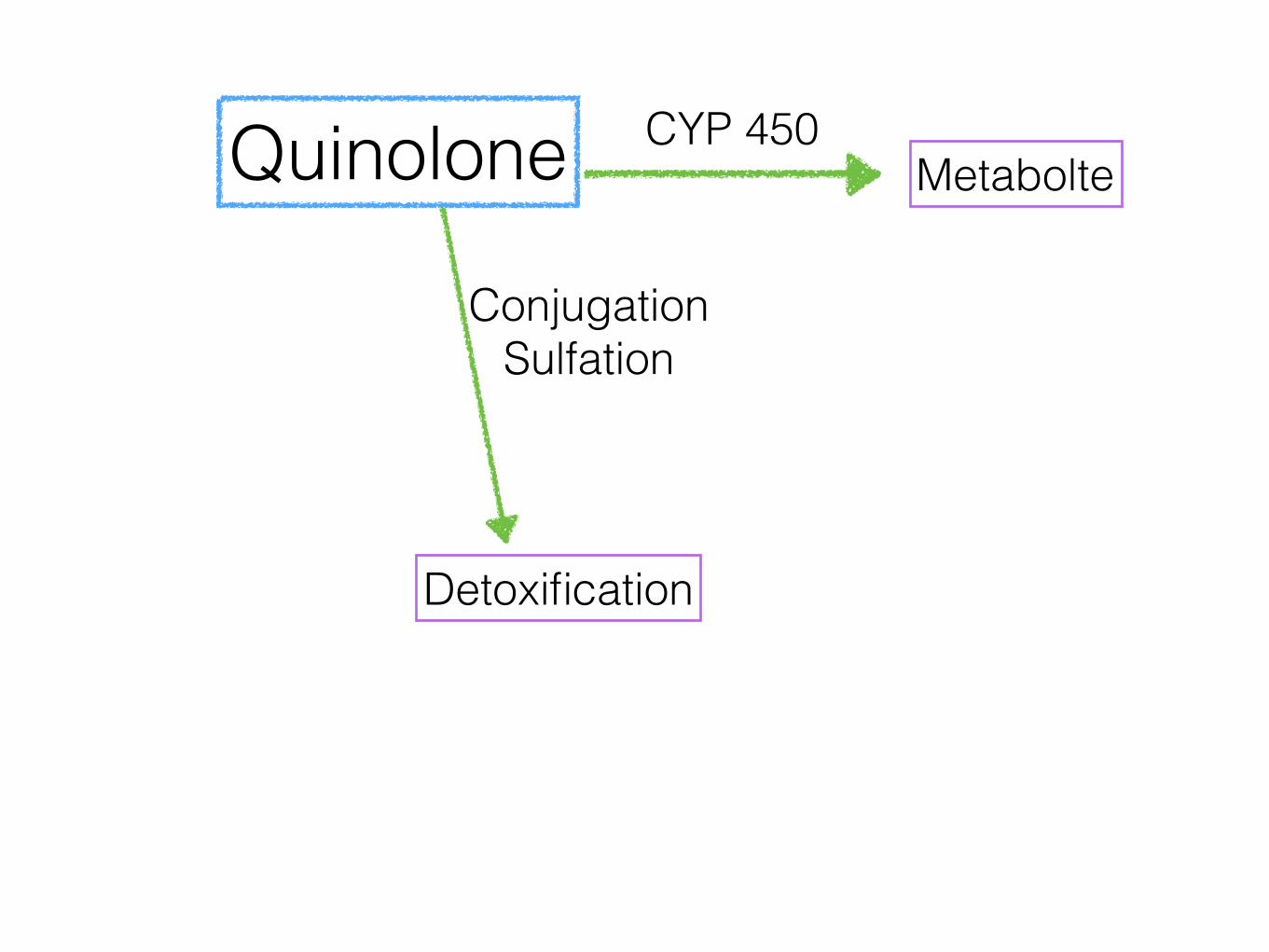
Quinolone CYP 450Metabolte
Conjugation Sulfation
Detoxification
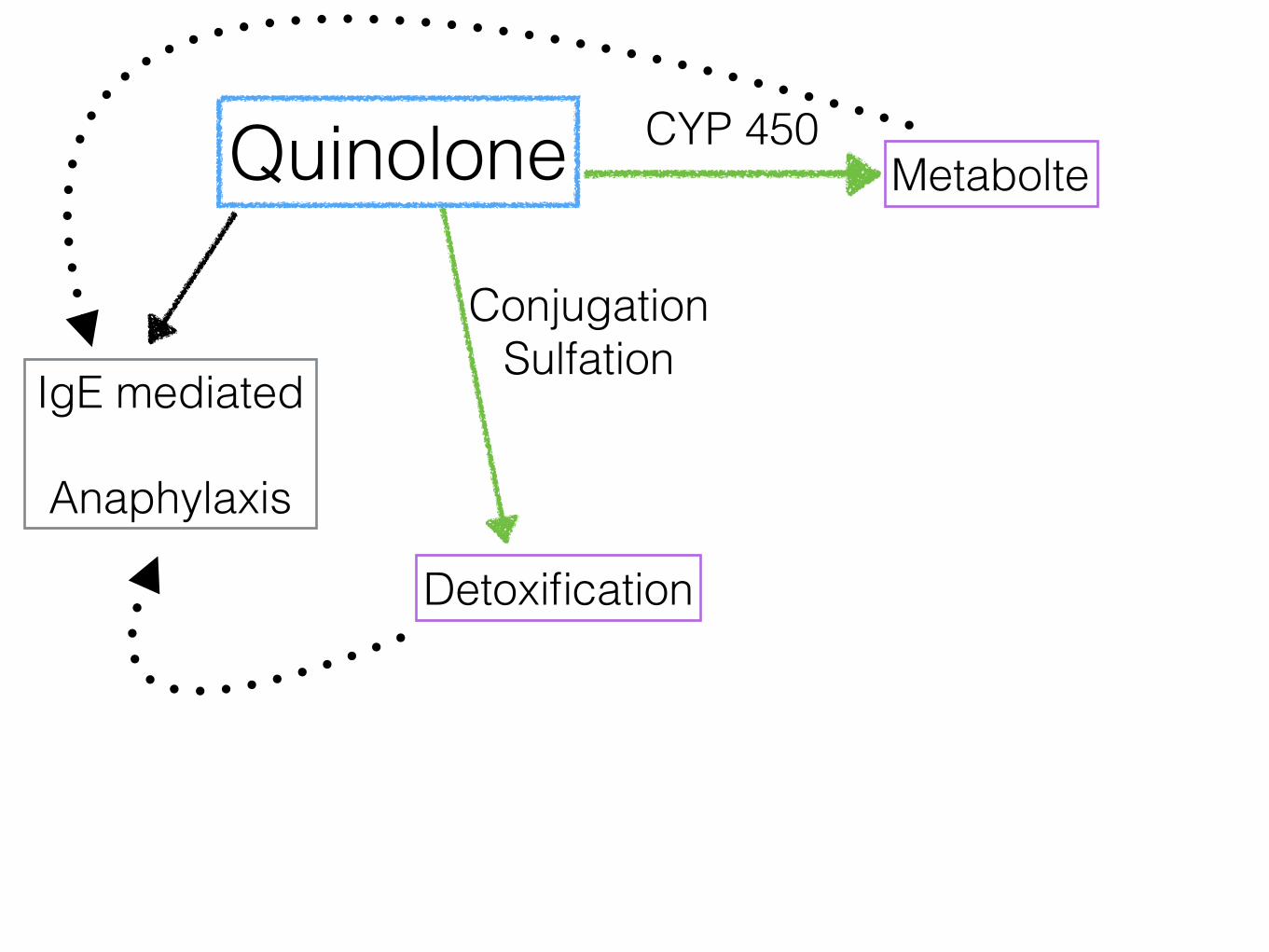
Quinolone CYP 450Metabolte
IgE mediated
Anaphylaxis
Conjugation Sulfation
Detoxification
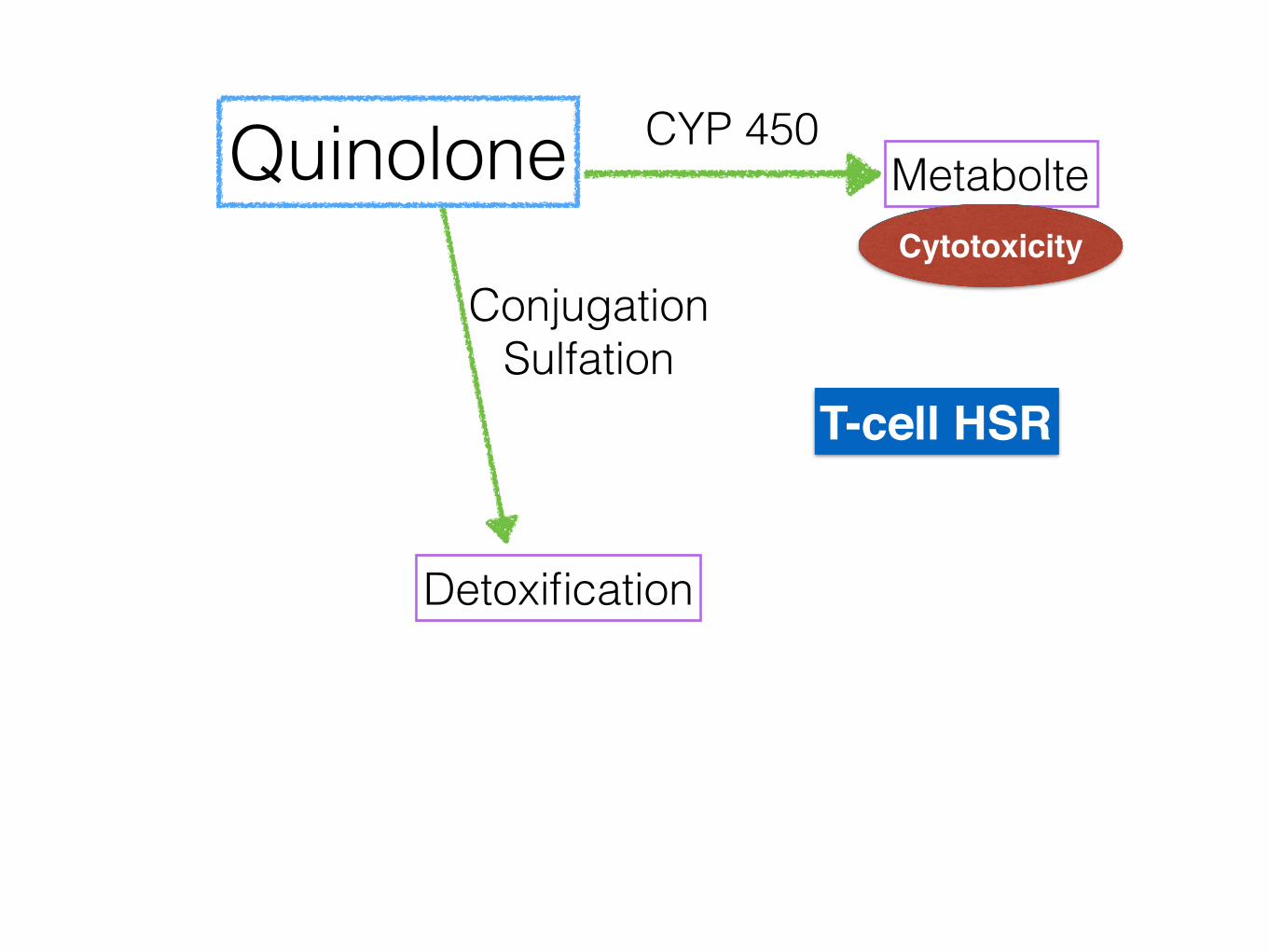
Quinolone CYP 450Metabolte
Conjugation Sulfation
Detoxification
T-cell HSR
Cytotoxicity
Quinolone CYP 450Metabolte
Conjugation Sulfation
Detoxification
T-cell HSR
Th2 cytokin
Th1
Hapten
Hapten&pro hapten
Pi-concept
Quinolone CYP 450Metabolte
Conjugation Sulfation
DetoxificationTh2
cytokin
Th1
Hepatotoxicity Renal toxicity
Dermatotoxicity
Cytotoxic
T-cell HSR
“Thank you”



![Targeting prokineticin system counteracts hypersensitivity ......thermal hypersensitivity, the PKRs antagonist PC1 [23] was subcutaneously administered, in a therapeutic way, at the](https://img.pdfslide.tips/doc/110x75/6092e439b685a76c2800e8e5/targeting-prokineticin-system-counteracts-hypersensitivity-thermal-hypersensitivity.jpg)

![[PPT]Hypersensitivity type I - bpumsparamed.bpums.ac.ir/.../Copy_of_type_I__3c5fe061.ppt · Web viewTitle Hypersensitivity type I Author Michael Jackson Last modified by acadpm01](https://img.pdfslide.tips/doc/110x75/5aa9eb4b7f8b9a7c188d728a/ppthypersensitivity-type-i-viewtitle-hypersensitivity-type-i-author-michael.jpg)