Embed Size (px)
DESCRIPTION
Citation preview

Ακτινοθεραπεία Ξ. ΒακάληςΑκτινοθεραπευτής Ογκολόγος Ιατρικού κέντρου Αθηνών

Disclosures
None
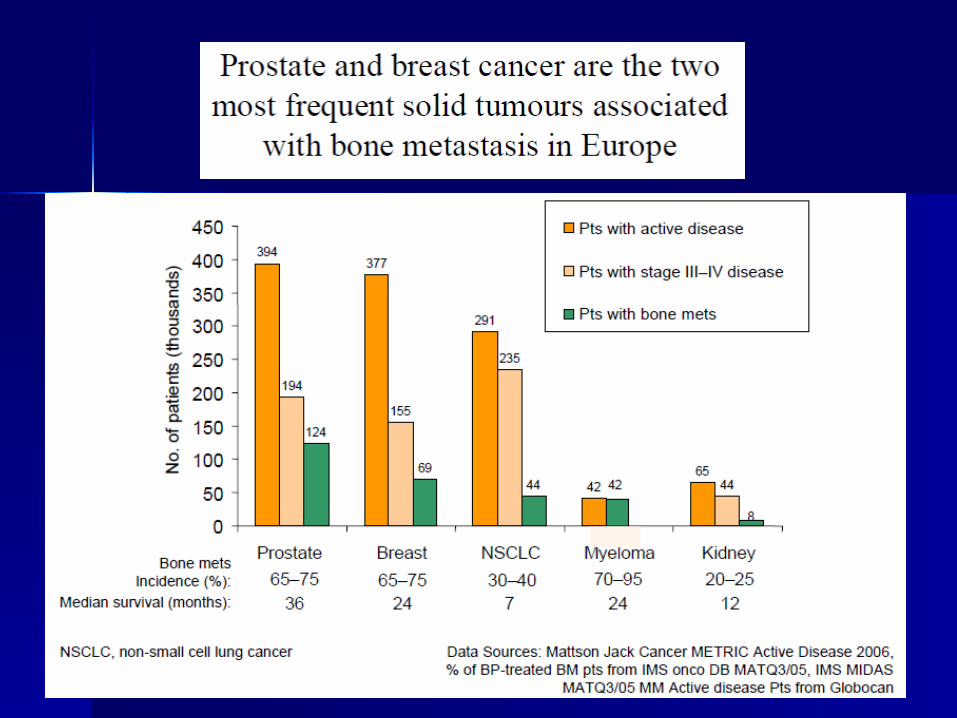
Metastatic Bone DiseaseMetastasis Sites
–Vertebra (69%)–Pelvis (41%)–Femur (25%)–Hip (14%)
Malawer, MM and Delaney, TF. Treatment of Metastatic Cancer to the Bone. In: Devita VT, Hellman S, Rosenberg SA (eds). Cancer: Principles and Practice of Oncology. 4th ed. Philadelphia: JB Lippincott; 1993:2225-2245.
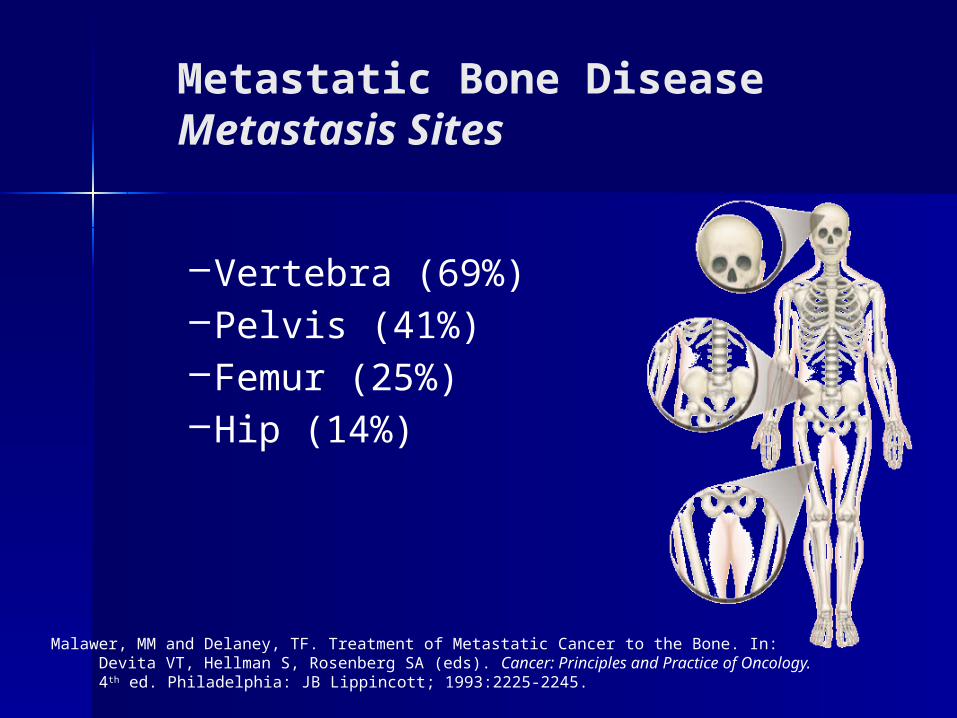
Level of Metastases
Thoracic 70%
Lumbar 20%
Cervical 10%
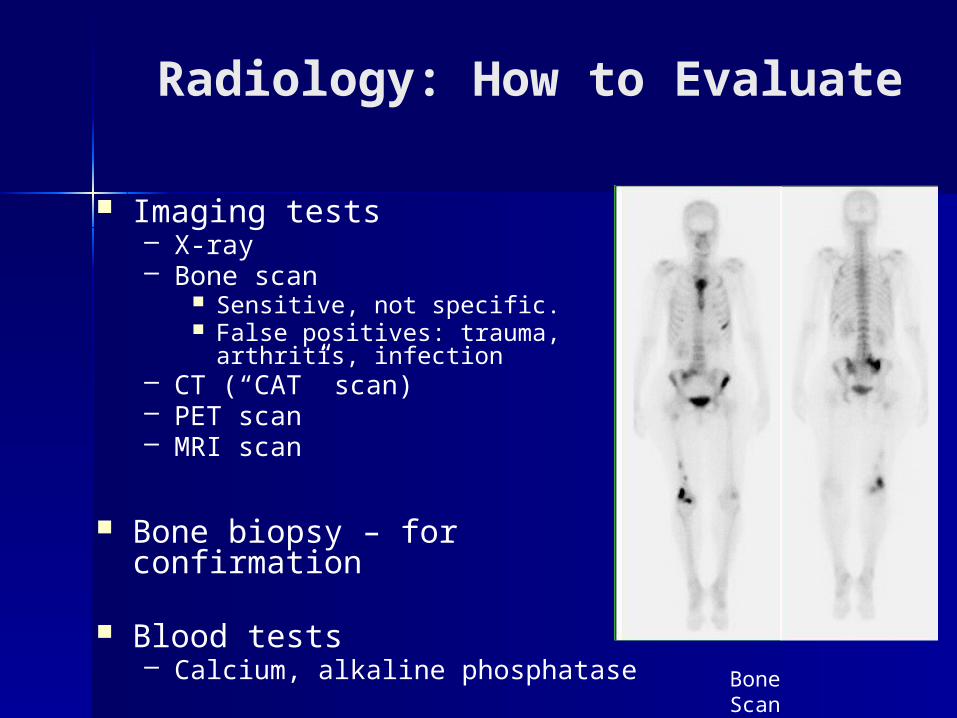
Radiology: How to Evaluate
Imaging tests– X-ray– Bone scan
Sensitive, not specific. False positives: trauma, arthritis,
infection– CT (“CAT” scan)– PET scan– MRI scan
Bone biopsy – for confirmation
Blood tests– Calcium, alkaline phosphatase
Bone Scan
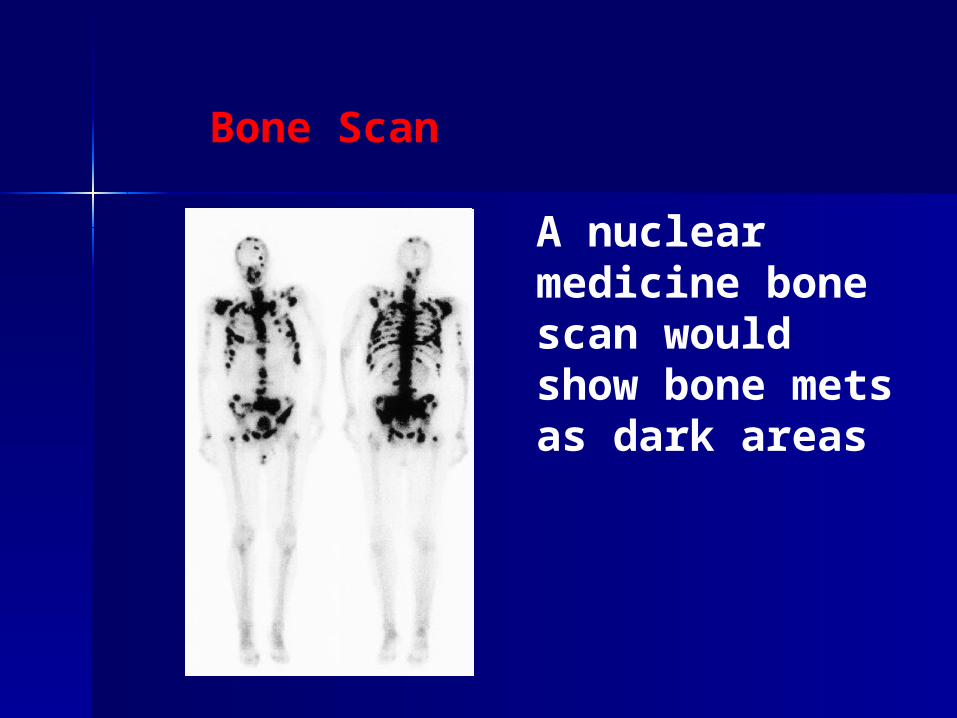
Bone Scan
A nuclear medicine bone scan would show bone mets as dark areas
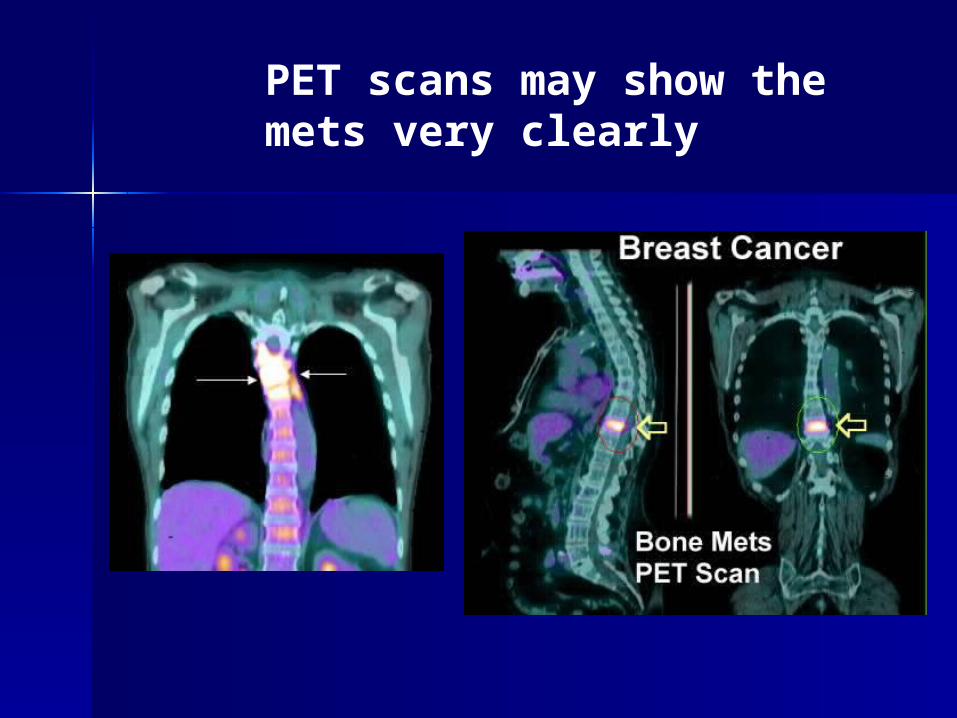
PET scans may show the mets very clearly
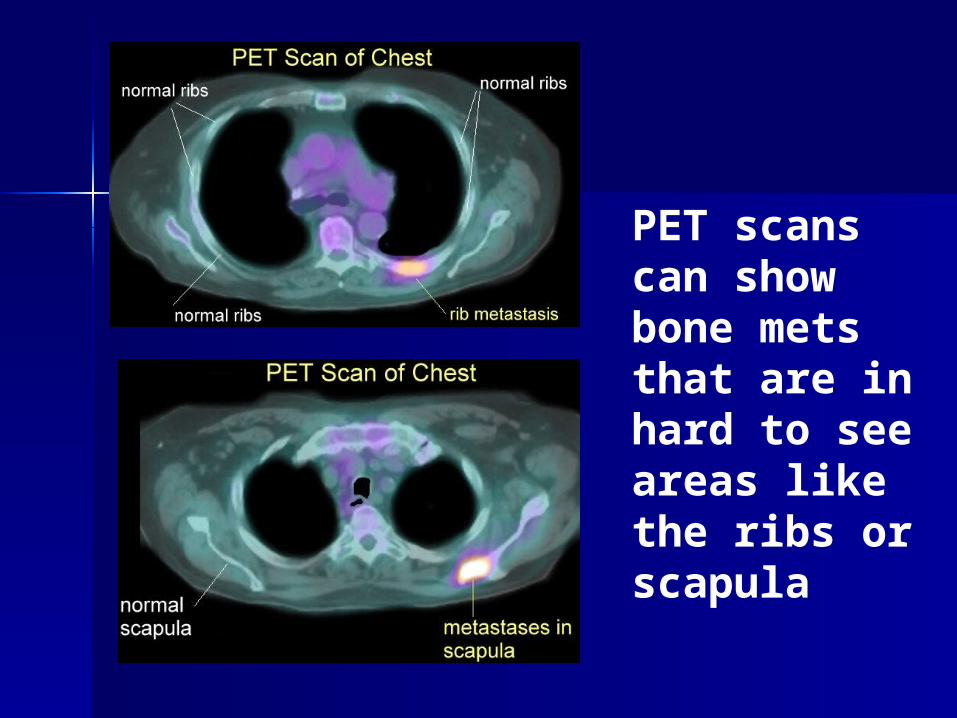
PET scans can show bone mets that are in hard to see areas like the ribs or scapula
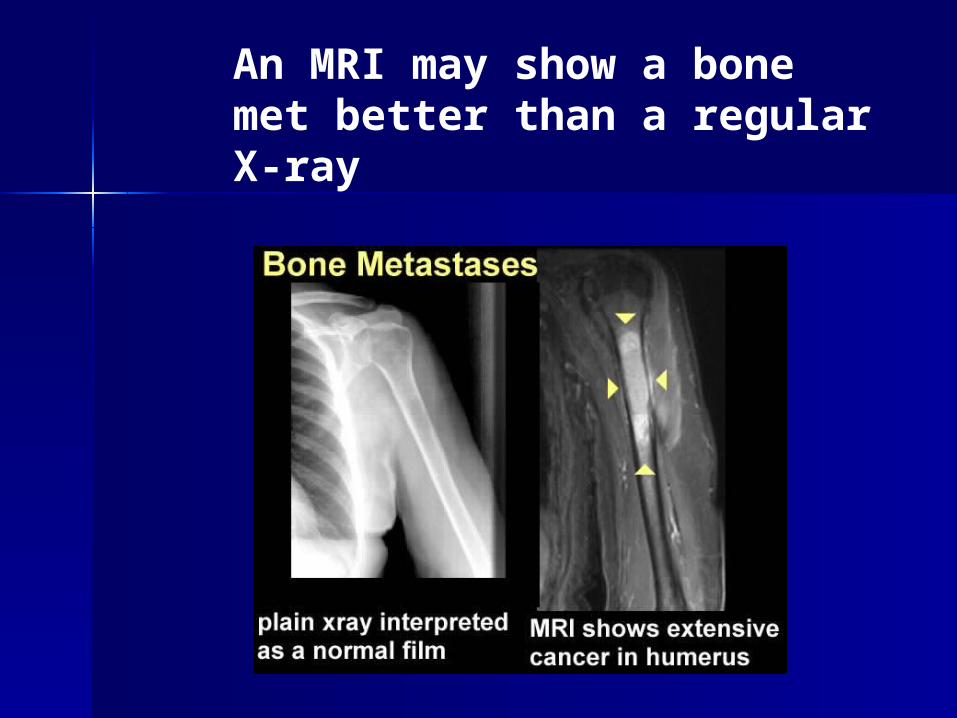
An MRI may show a bone met better than a regular X-ray

MRI imaging
T1 T2
Clinical features of bony metastases
Bone pain Pathological fracture Nerve compression Hypercalcaemia
Life expectancy Biopsy – Histology to predict the
response to non operative management
Stability Clinical presentation – Pain and
Neurological status
APPROACH
Treatment of bone metstasis
Medical. Surgical. Radiotherapy. Radionuclid. Chemotherapy & Hormonal
Therapy
Multi-disciplinary approach
Radiation Therapy
1. Localized irradiation2. Hemibody irradiation
How does RT reduce pain ?
Cell kill – reduced tumor size and pressure effects
Endothelial damage of micro-vasculature – reduced blood flow.
Reduces edema Reduces pain related neuro-transmitter concentrations
Bone – promotes re-mineralisation leading to structural stability.
Indications of Radiotherapy As Primary Treatment
1. Radiosensitive tumor not previously irradiated
2. Widespread spinal metastases with multilevel neural compression
3. Total neurological deficits below the level of compression > 48 hours
4. Patient’s condition (or prognosis) precludes surgery: high surgical risk or short life expectancy
Penas-Prado M, Loghin ME. Spinal cord compression in cancer patients: review of diagnosis and treatment. Curr Oncol Rep. 2008 Jan;10(1):78-85.
Radiotherapy Modalities
Conventional External Beam Radiotherapy (EBRT)
Intensity-modulated radiation therapy (IMRT)
Stereotactic radiotherapy Stereotactic radiosurgery Radioisotopes
Finn MA, Vrionis FD, Schmidt MH. Spinal radiosurgery for metastatic disease of the spine. Cancer Control. 2007 Oct;14(4):405-11.
Radiation Results
•Overall 85% response rate
•Complete relief in 54%
•50% respond by 2 weeks, 80% by 1 month
•Median duration of pain relief 12-15 weeks
•The Xrays or scans may take months to show improvement (Recalcification by 2-3 months)
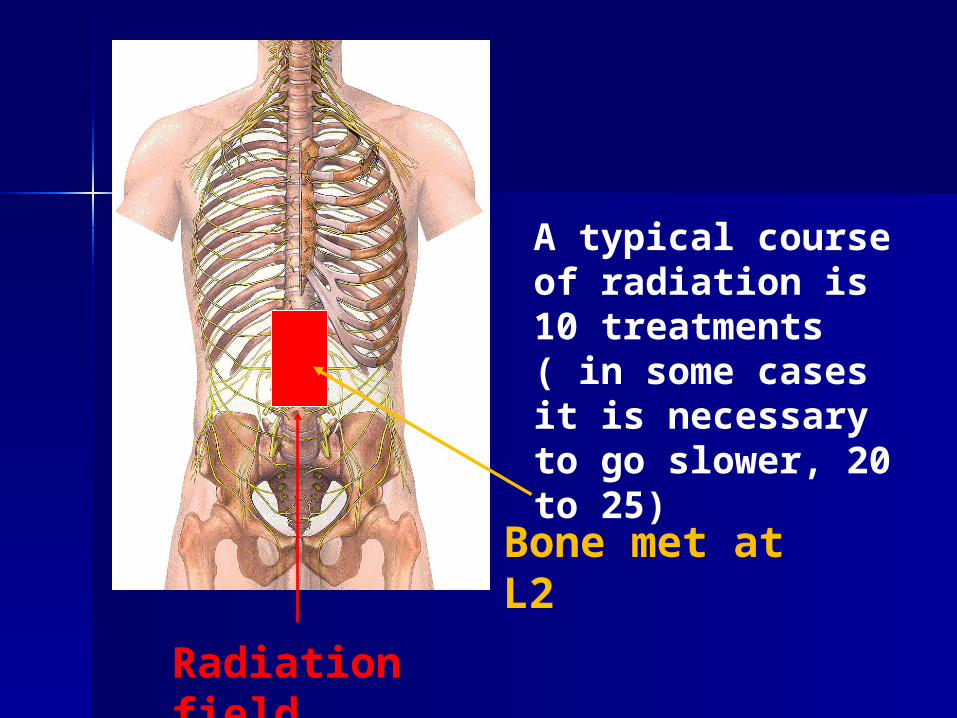
Bone met at L2
Radiation field
A typical course of radiation is 10 treatments ( in some cases it is necessary to go slower, 20 to 25)
M. Raphael Pfeffer,Oncology Institute, Chaim Sheba Medical Center
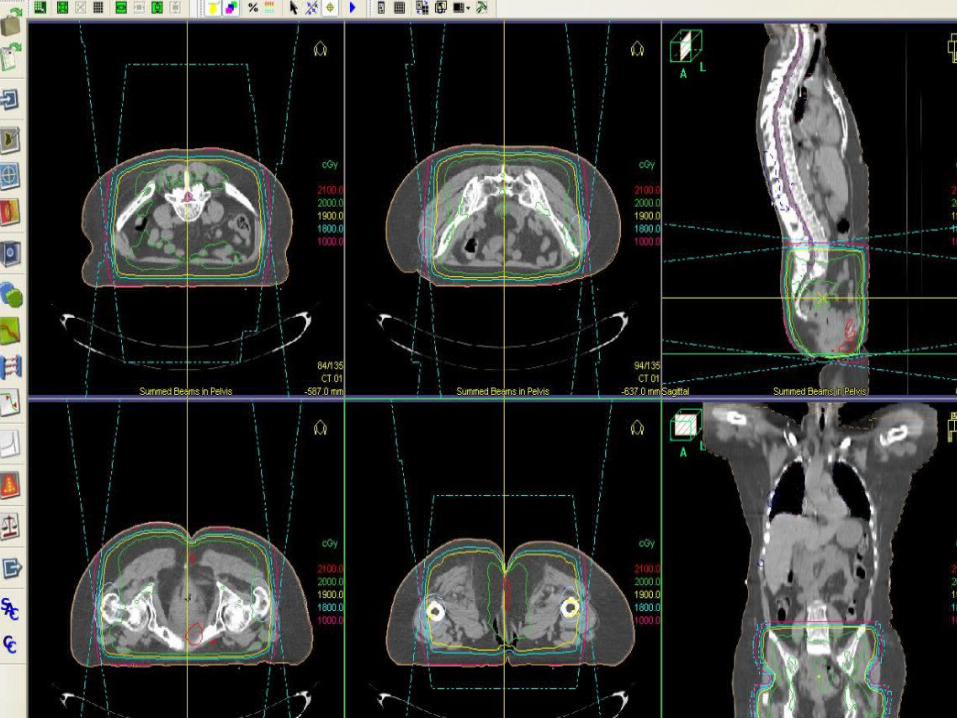
Palliative xrt - bone metastases treatment planning
good margins– e.g. add 1-2 vertebrae on each side
include nearby asymptomatic lesions avoid irradiating entire limb
circumference reduce irradiated volume of
bowel/bladder bone marrow toxicity
Fractionation regimens
8 Gy in 1 fraction 20 Gy in 5 fractions 24 Gy in 6 fractions 30 Gy in 10 fractions
Endpoints using pain relief, narcotic relief and quality of life measures show consistent similarity in the regimens
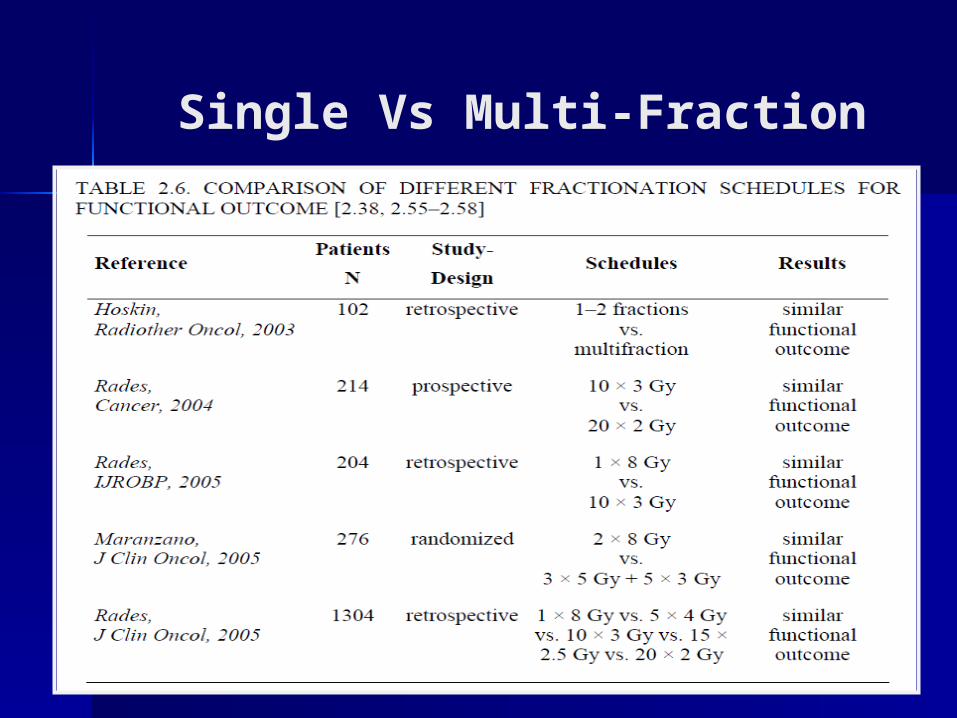
Single Vs Multi-Fraction
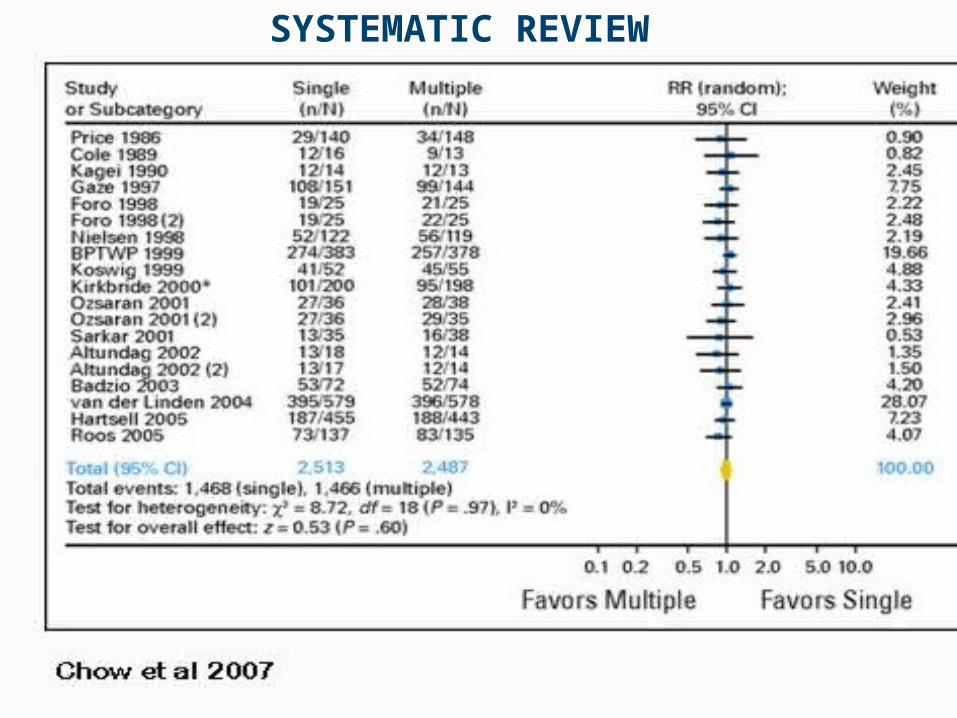
SYSTEMATIC REVIEW
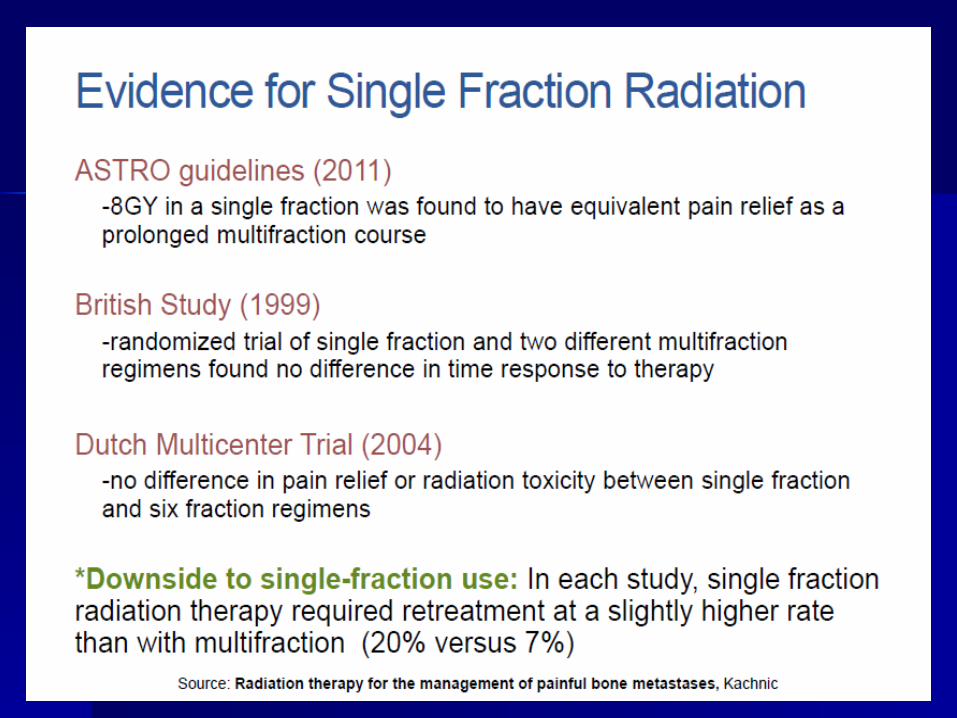
more convenientless costlyshorter time with acute side effects
fear of high doses per fractionhigher retreatment rate( 2-2,5 times higher)concern about toxicity in long-term survivorsflare of bone pain maybe be higher
Single fraction v multifraction
Problematic retreatment Previous treatment to the spine Femoral axial cortical involvment >
3 cm Surgical stabilization procedure Spinal cord compression or
radicular nerve pain
Single fraction v multifraction caution
Re-irradiation
Not covering the spinal cord – 1 x 8 Gy or 5 x 4Gy(Grade C)
Covering the spinal cord – 8 x 2,5 Gy (Grade D)
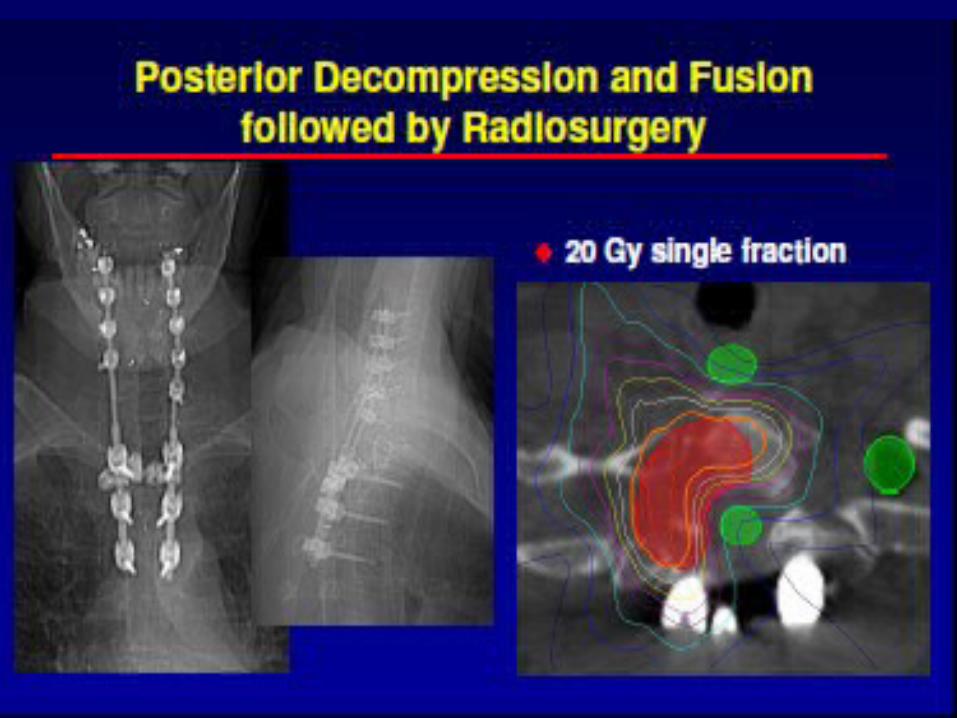
Adjuvant Radiotherapy
Done after operative decompression
Patchell et al study
Wait 3 weeks for wound healing before starting radiation
Post-operative
Patient received 30Gy/10fx
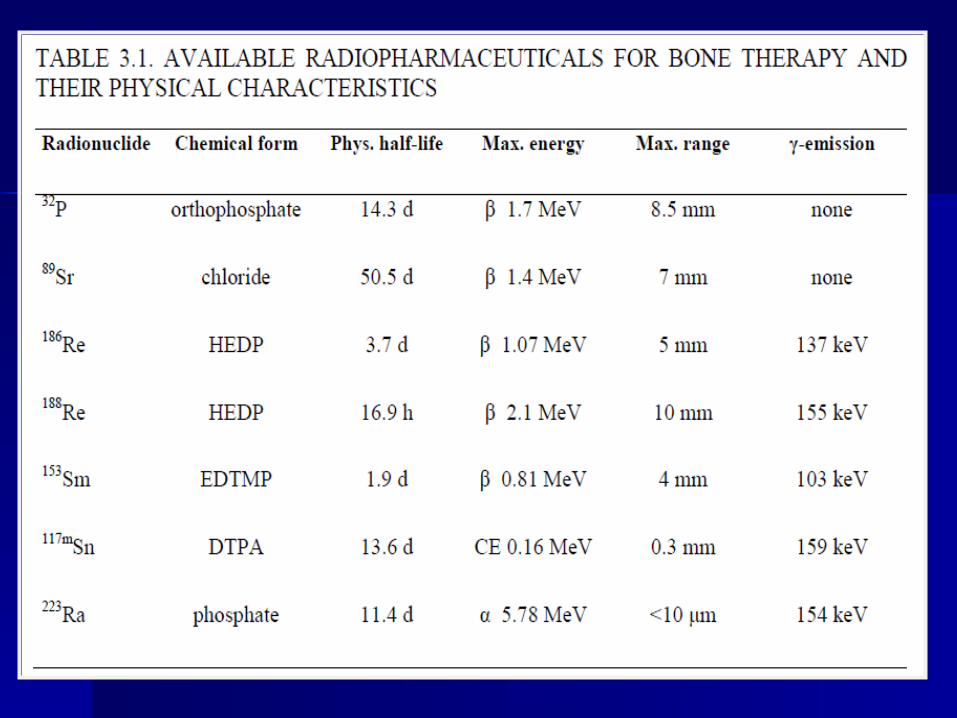
Radiopharmaceuticals
Use of Radiopharmaceuticals does not obviate the need for EBRT.
Ideal for osteoblastic, multi-focal and wide-spread disease.
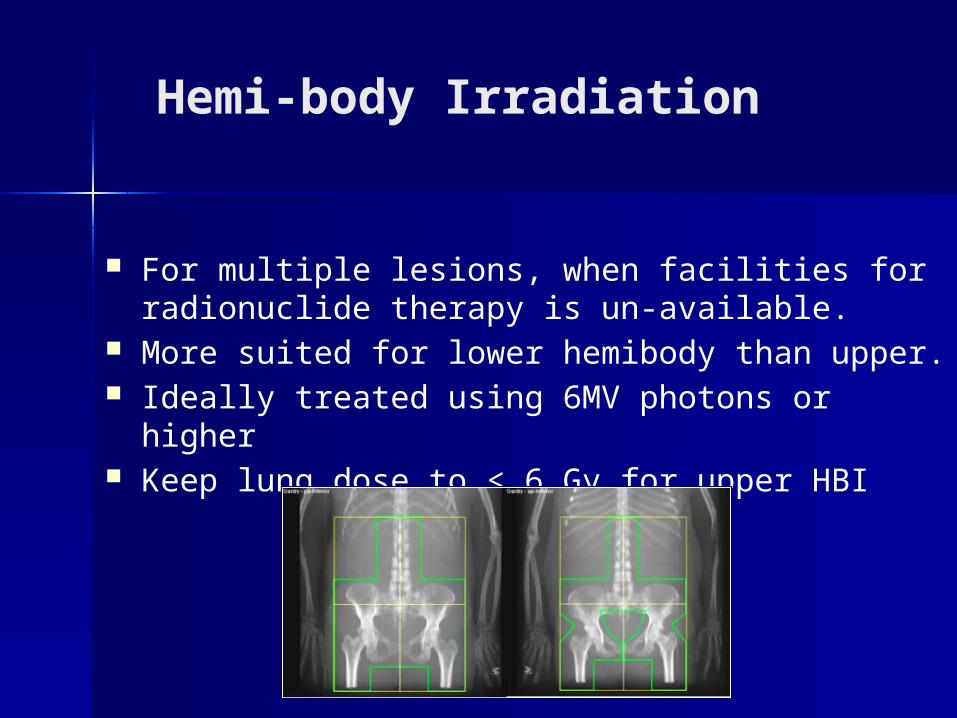
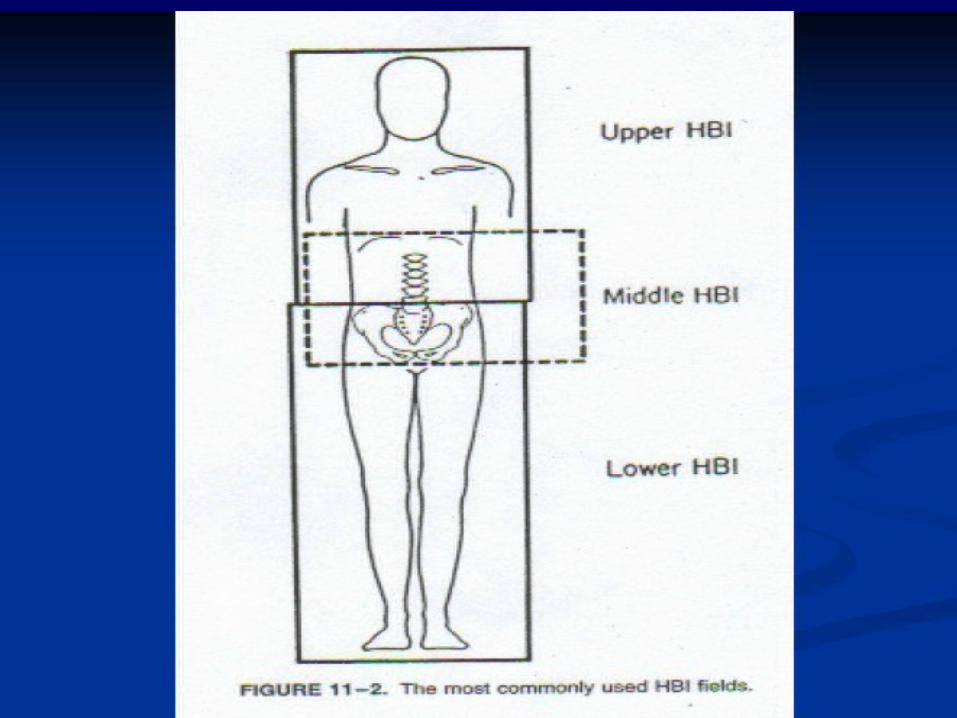
Hemi-body Irradiation
For multiple lesions, when facilities for radionuclide therapy is un-available.
More suited for lower hemibody than upper. Ideally treated using 6MV photons or higher Keep lung dose to < 6 Gy for upper HBI
M. Raphael Pfeffer,Oncology Institute, Chaim Sheba Medical
Center
Palliative xrt -single fraction half body iradiation
lower half body 8 Gy upper half body 6 Gy good short term palliation (~3 months) onset of pain relief
– Half Body xrt 50% @ 3 days, 100% @ 14 days
– Focal XRT 50% @ 7 days, 80% @ 14 days Salazar Cancer 1986
Bisphosphonates and RT
“Bisphosphonates and RT can be given concurrently.”
Synergistic effect – Zoledronic acid pauses the cells in G2M phase.
Use of Bisphosphonates does not obviate the need for RT.
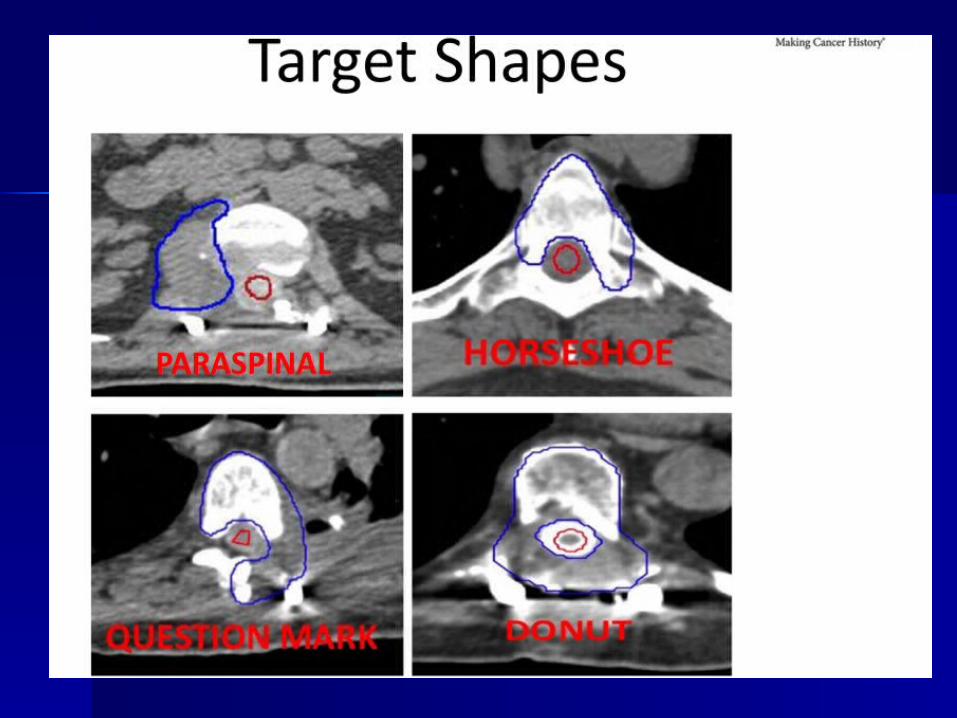
– Deliver high doses safely– Possible to irradiate spine without
affecting spinal cord
IMRT, STEREOTACTIC RADIOSURGERY AND STEREOTACTIC RADIOTHERAPY
*De Salles AA, Pedroso AG, Medin P, Agazaryan N, Solberg T,Cabatan-Awang C, et al: Spinal lesions treated with Novalisshaped beam intensity-modulated radiosurgery and stereotacticradiotherapy. J Neurosurg 101 (3 Suppl):435–440, 2004
Metastatic Spinal Cord Compression (MSCC)
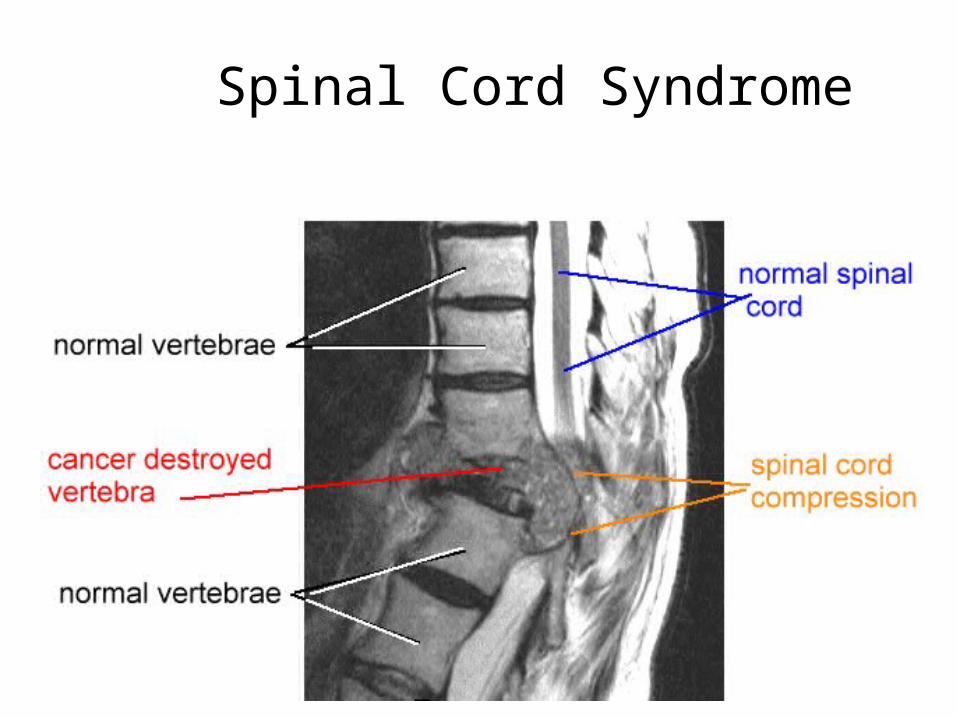
Spinal Cord Syndrome
Epidemiology
40% of all cancer patients will develop metastatic spinal disease– 10-20% of these patients will develop spinal
cord compression
White AP, Kwon BK, Lindskog DM, Friedlaender GE, Grauer JN. Metastatic disease of the spine. J Am Acad Orthop Surg. 2006 Oct;14(11):587-98.
Signs & Symptoms
Presents with as:Collapsed vertebral bodySoft tissue mass in the spinal canal
Symptoms Increasing & unexplained pain in neck or
spine Any numbness/ weakness in arms or legs Difficulty in walking and balancing Problems with controlling & emptying bladder
or bowels Any muscle loss or lack of tendon reflex
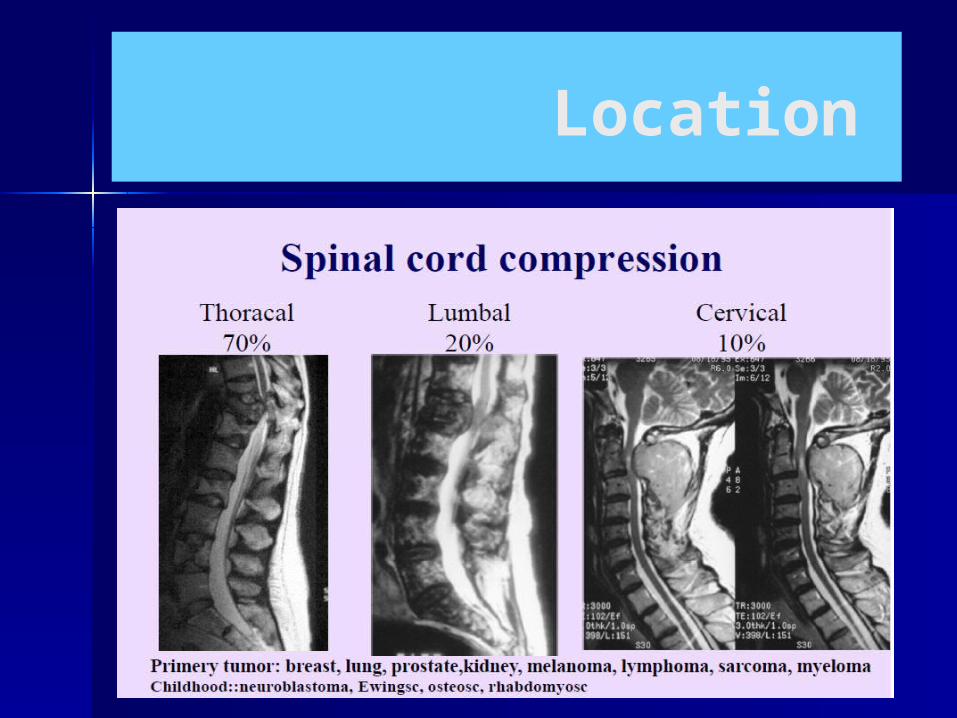
Location
What happens to the patient in hospital?
– they should start dexamethasone 16mg od if not already on it
– urgent MRI scan of spine– if proven, urgent radiotherapy to cord
compression area
It is an oncologic emergency
Success rates of SCC treatment with Radiotherapy
– depends on level of neurological function at presentation to radiotherapist
– if patient is ambulatory – 70% retain ability to walk
– if patient is paraparetic – 35% retain ability to walk
– if patient is paraplegic – 5% retain ability to walk
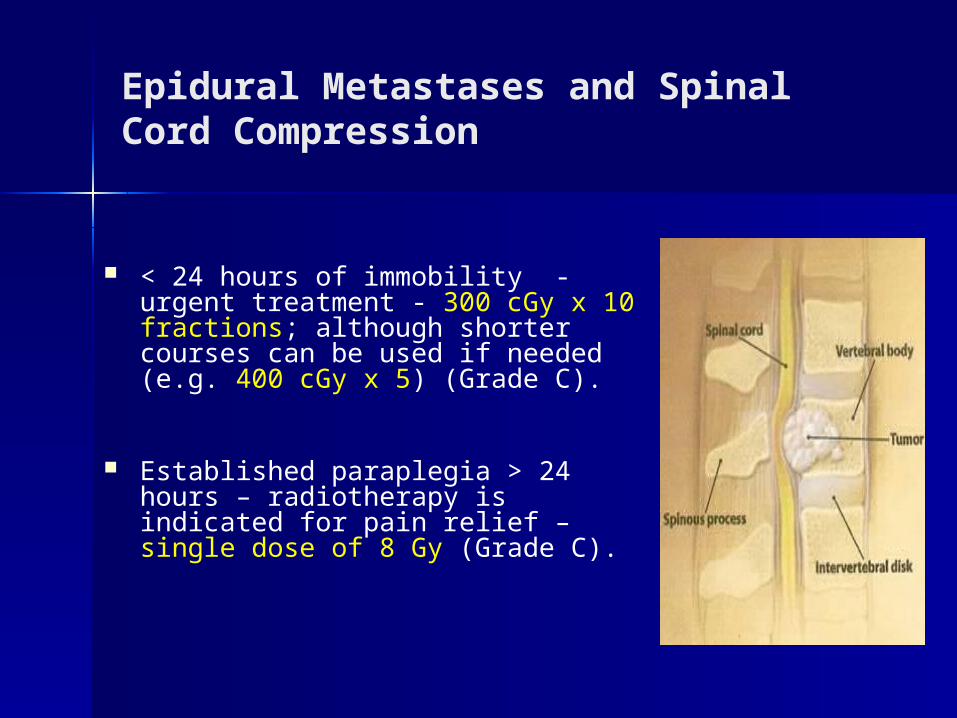
Epidural Metastases and Spinal Cord Compression
< 24 hours of immobility - urgent treatment - 300 cGy x 10 fractions; although shorter courses can be used if needed (e.g. 400 cGy x 5) (Grade C).
Established paraplegia > 24 hours – radiotherapy is indicated for pain relief – single dose of 8 Gy (Grade C).
Multidisciplinary Care NOMS1,2
Neurologic Oncologic Mechanical Stability Systemic disease
Systemic Therapy Radiation Therapy Surgery
vs.
1Bilsky MH, Smith M. Surgical approach to epidural spinal cord compression. Hematology/Oncology Clinics of North America.;20(6):1307-1317, 2006
2Bilsky MH, Azeem S. The NOMS framework for decision making in metastatic cervical spine tumors. Current Opinions in Orthopedics 2007;18(3):263-269.
The role of surgery
Indicated if: previous Radio Rx/ no response Radioresistant tumor life expectancy > three months single site unstable spine no tissue diagnosis
RCT comparing surgery followed by RT vs. RT alone
Improvement in surgery + RT– Able to walk: 84% vs 57%– Median time able to walk: 122 vs 13 days– Continent: 156 vs 17 days– Regained ability to walk: (n= 32) 62% vs 19%– Survival: 126 vs 100 days
Patchell, R, Tibbs, PA, Regine, WF, et al. A randomized trial of direct decompressive surgical resection in the treatment of spinal cord compression caused by metastasis (abstract). proc Am Soc Clin Oncol 2003; 22:1.
The role of surgery + RT
A meta-analysis of surgery versus conventional radiotherapy for the treatment of metastatic spinal epidural disease
Neuro Oncol 2005 Jan. Klimo et al. Department of Neurosurgery, University of Utah, Salt Lake City, USA
surgery 999 patients: radiation 543 patients
surgical patients were 1.3 times more likely to be ambulatory after treatment and twice as likely to regain ambulatory function
overall ambulatory success rates for surgery and radiation were 85% and 64%
surgery should usually be the primary treatment with radiation given as adjuvant therapy
32% in the group that underwent radiotherapy before surgery
12% in the group of patients first treated by
surgery.
PostOp major wound complications (dehiscence or wound infection)
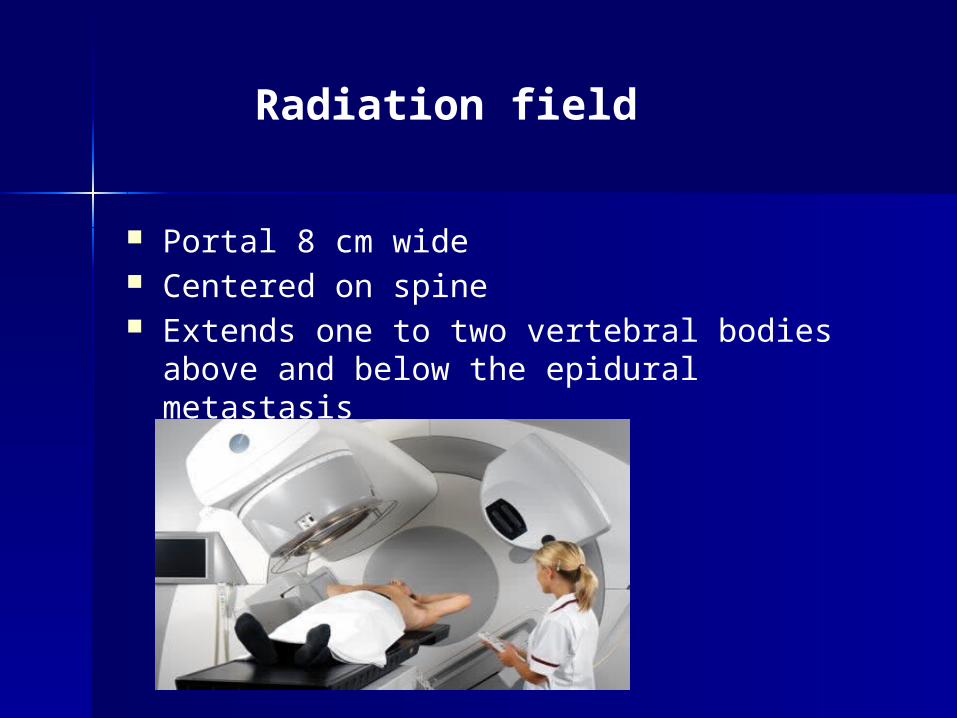
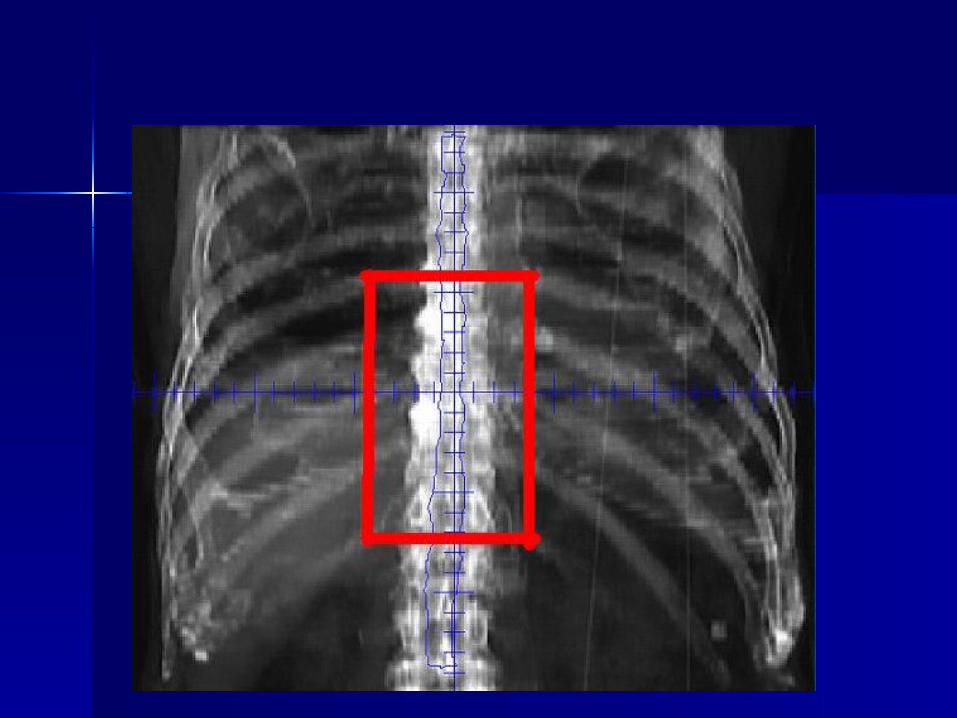
Portal 8 cm wide Centered on spine Extends one to two vertebral bodies above
and below the epidural metastasis
Radiation field
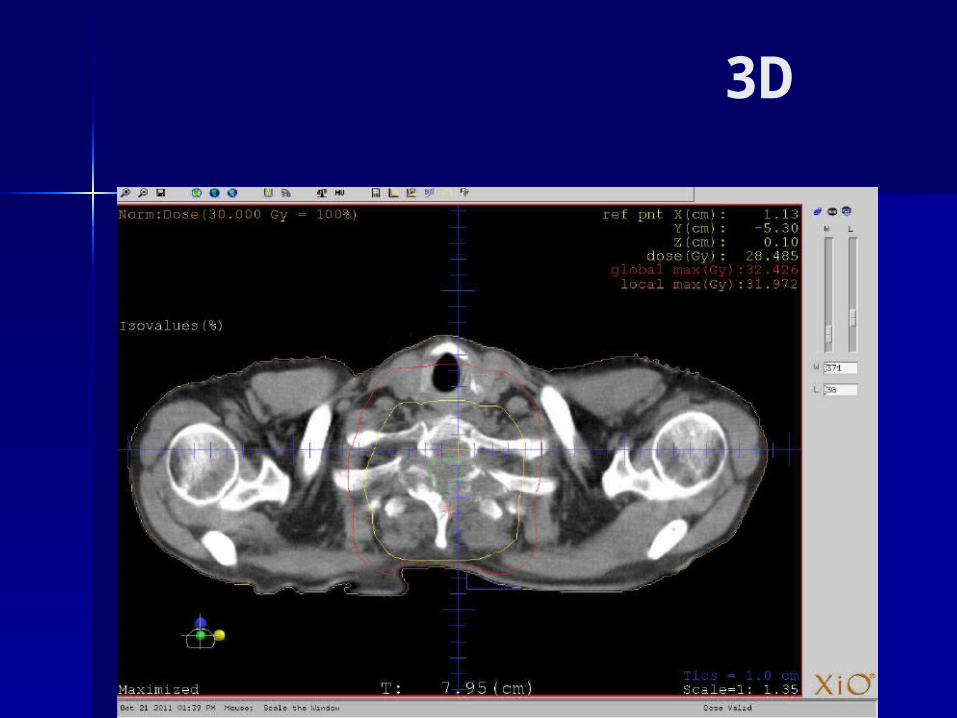
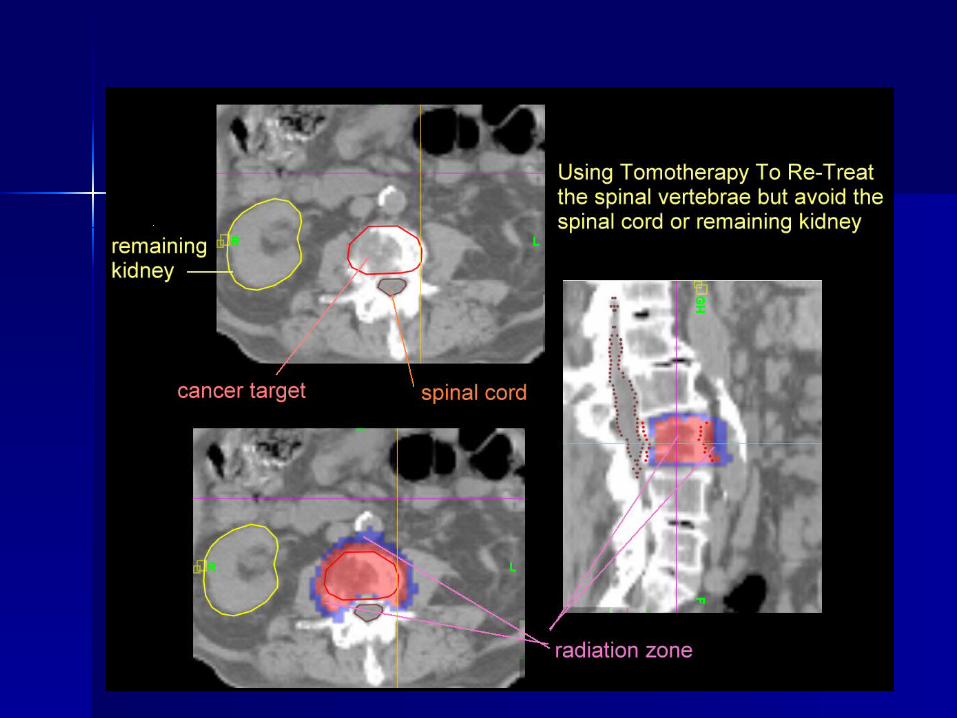
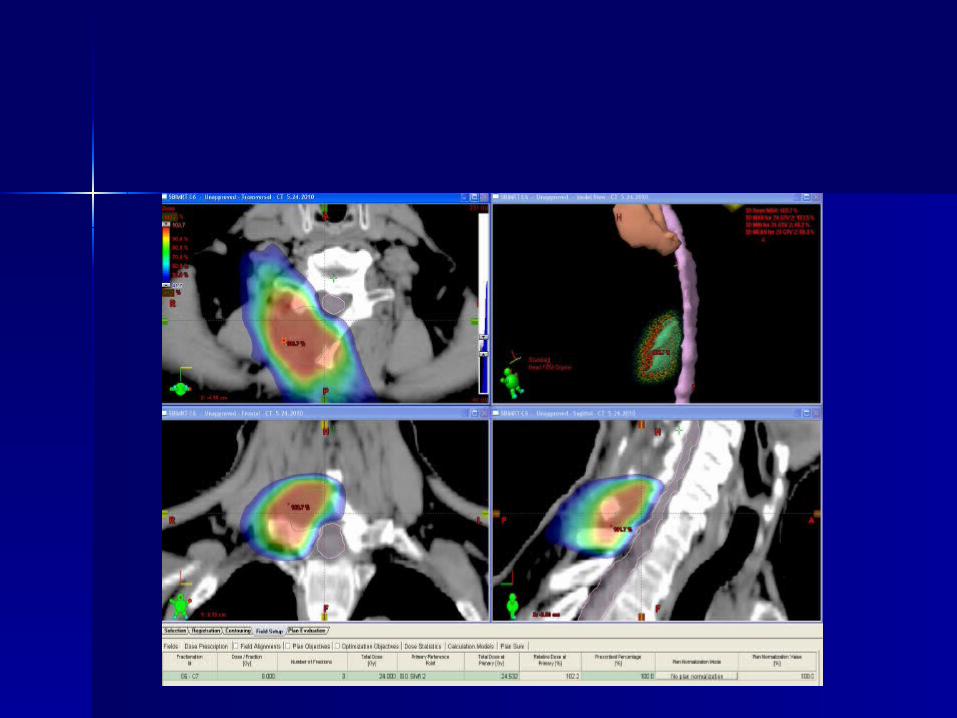
3D
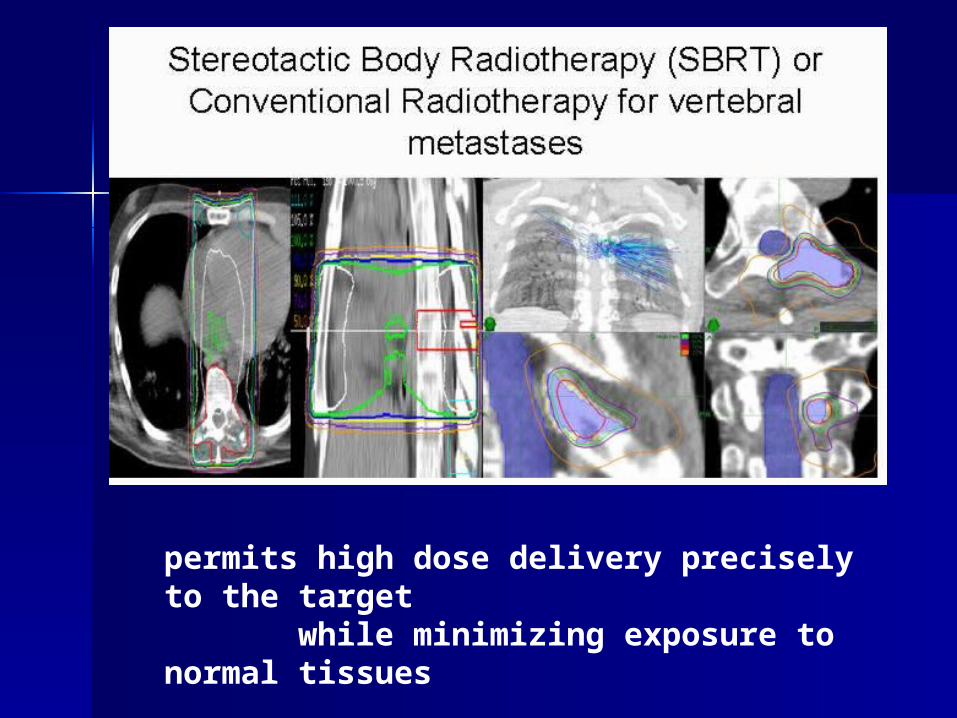
permits high dose delivery precisely to the target while minimizing exposure to normal tissues
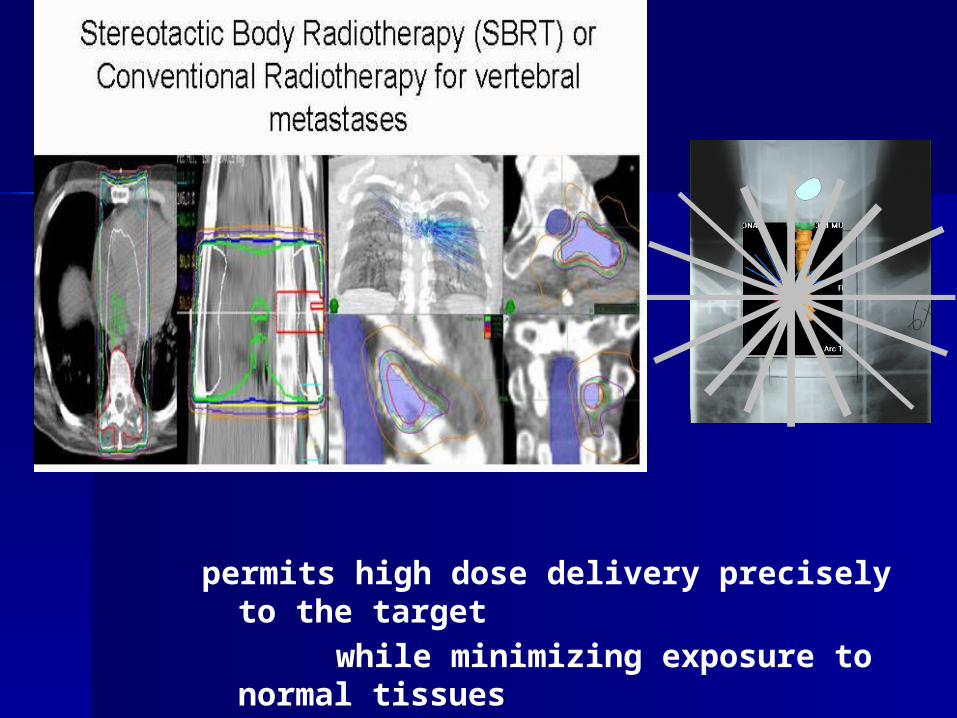
permits high dose delivery precisely to the target
while minimizing exposure to normal tissues
Radiosurgery Recommendations
A strong recommendation can be made with low-quality evidence that radiosurgery should be considered over conventional fractionated radiotherapy for the treatment of solid tumor spine metastases in the setting of oligometastatic disease and/or radioresistant histology in which no relative contraindications exist.
Gerszten PC, Mendel E, Yamada Y. Radiotherapy and radiosurgery for metastatic spine disease: What are the options, indications, and outcomes. Spine 34(22S):S78-92, 2009
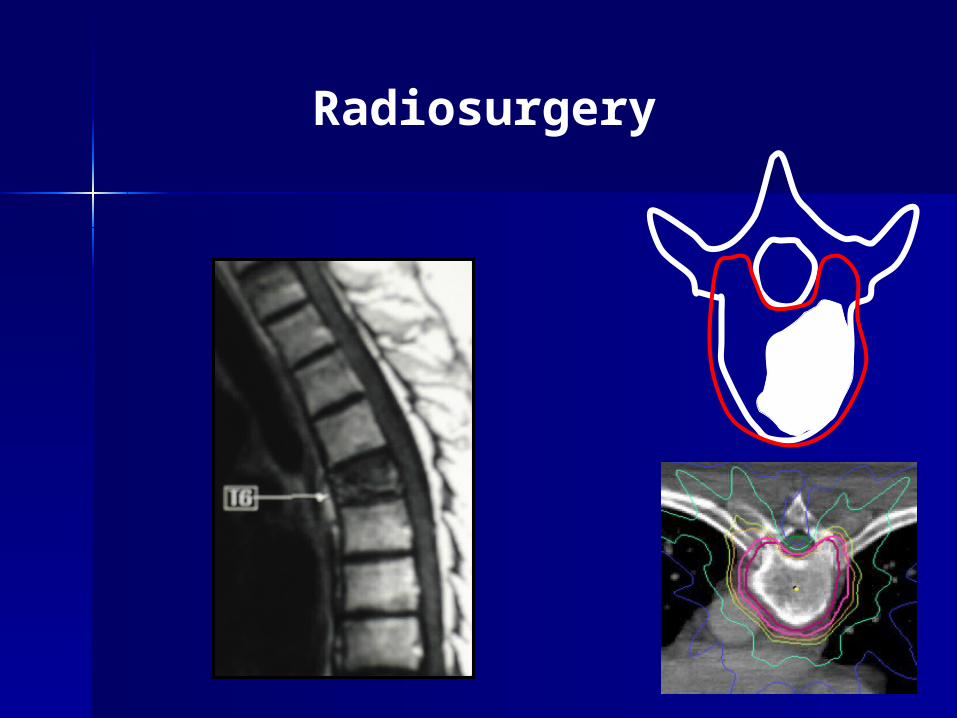
Radiosurgery
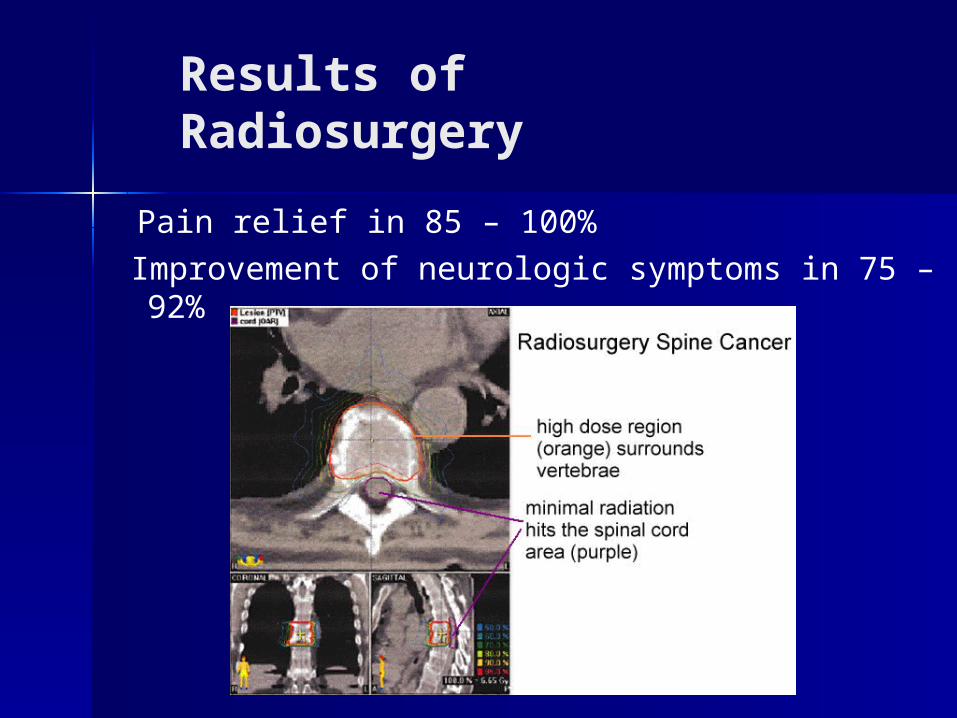
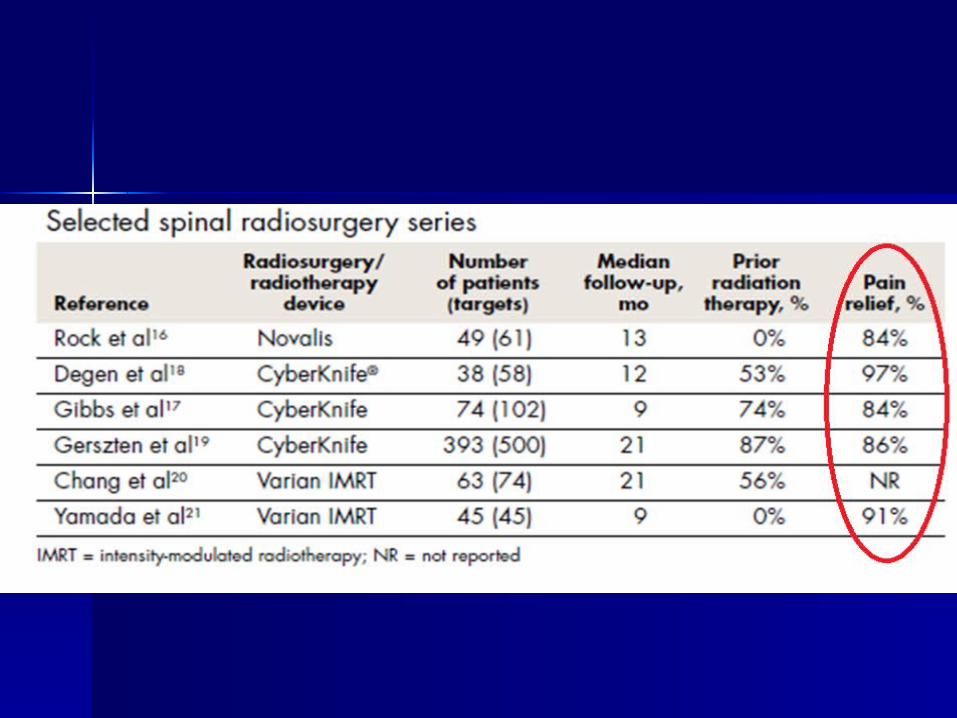
Results of Radiosurgery
Pain relief in 85 – 100%
Improvement of neurologic symptoms in 75 – 92%
Cyberknife
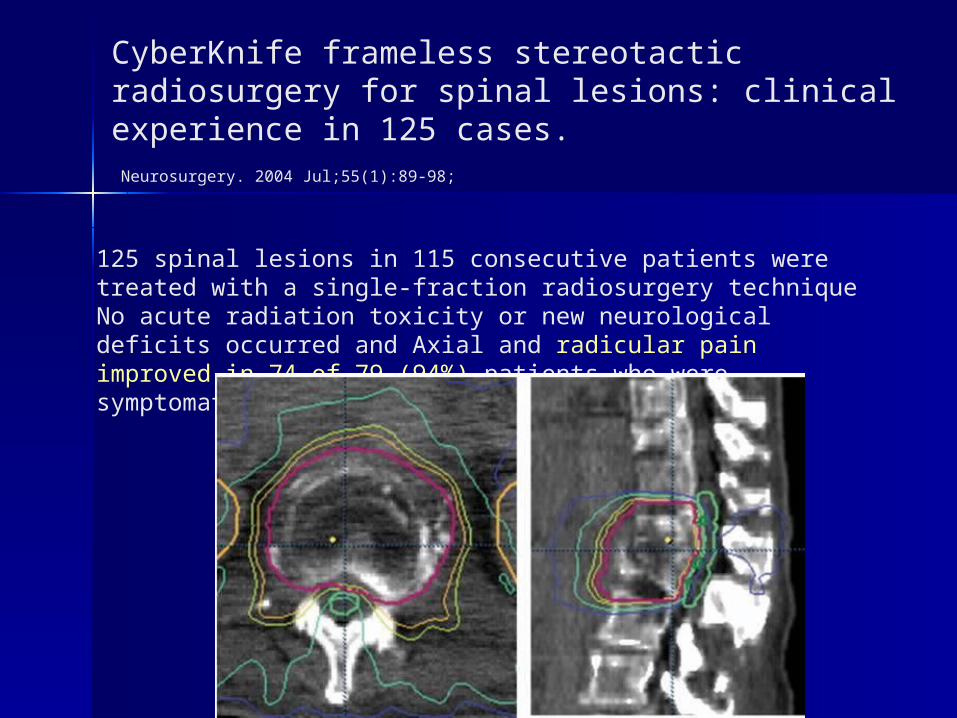
CyberKnife frameless stereotactic radiosurgery for spinal lesions: clinical experience in 125 cases. Neurosurgery. 2004 Jul;55(1):89-98;
125 spinal lesions in 115 consecutive patients were treated with a single-fraction radiosurgery technique No acute radiation toxicity or new neurological deficits occurred and Axial and radicular pain improved in 74 of 79 (94%) patients who were symptomatic before treatment.
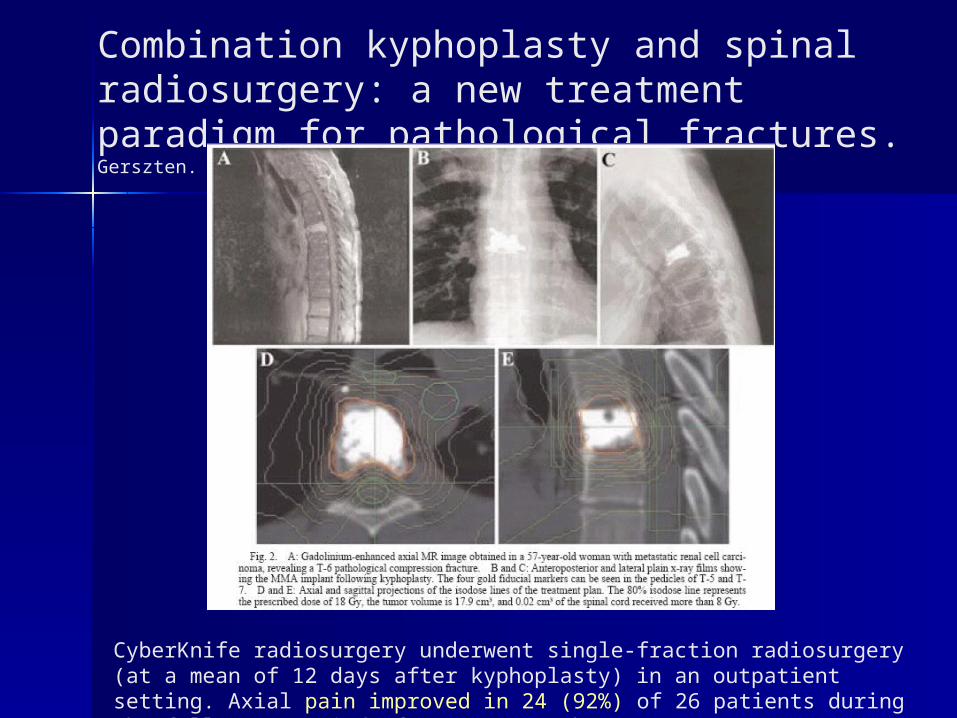
Combination kyphoplasty and spinal radiosurgery: a new treatment paradigm for pathological fractures.Gerszten. Neurosurg Focus 2005 Mar 15;18(3):e8.
CyberKnife radiosurgery underwent single-fraction radiosurgery (at a mean of 12 days after kyphoplasty) in an outpatient setting. Axial pain improved in 24 (92%) of 26 patients during the follow-up period of 7 to 20 months.