Embed Size (px)
DESCRIPTION
Target: UG students of medicine.
Citation preview

RBC Disorders - 2
Dr.CSBR.Prasad, M.D.,

Iron Deficiency Anemia

Importance of iron
Iron is quantitatively the most important bioactive element in human enzymology with roles in:
–Oxygen transport and storage
–Oxidative metabolism
–Cellular growth and proliferation

Haem - Proteins
• Hemoglobin 70% • Myoglobin 5% • Tissue specific haem proteins
– Cytochromes Eg: P450 – Oxygenases – Hydroxylases – Peroxidase – Catalase – Ribonucleotide reductase – Aconitase

Proteins of iron TRANSPORT & STORAGE
• TRANSFERRIN: Single chain glycoprotein with two iron binding sites, responsible for iron transport in plasma and extra-cellular fluid
• TRANSFERRIN RECEPTOR: Transmembrane glycoprotein with two transferrin binding sites
• FERRITIN: Spherical protein of 24 subunits which binds 4500 atoms of iron
• IRP: four domine cluster protein which co-ordinates translocational regualtion of iron proteins

Iron Distribution in Healthy
Young Adults (mg)
Pool Men Women Total 3450 2450
Functional
Hemoglobin 2100 1750
Myoglobin 300 250
Enzymes 50 50
Storage
Ferritin, hemosiderin 1000 400

Iron metabolism

Iron balance
Absorption
• 7mg/1000kcal
• 20-30% of haem iron is absorbed
• <5% of non haem iron is absorbed
• Absorption is increased by aminoacids & ascorbic acid
• Absorption is decreased by phytates, phosphates and tannates
Excretion
• Exfoliated epithelial cells of the GI tract
• Exfoliated cells of the skin
• Bile
• Urine
• Menstrual blood loss
NO MECHANISM FOR INCREASING IRON EXCRETION

Free iron is highly toxic
Hence, storage iron is sequestered
– Ferritin or
–Hemosiderin

Ferritin & Hemosiderin
• Ferritin is a ubiquitous protein-iron complex • Highest levels :
– liver, spleen, bone marrow, and skeletal muscles
• In the liver, most ferritin is stored within the parenchymal cells
• Partially degraded protein shells of ferritin aggregate into hemosiderin granules
• Since plasma ferritin is derived largely from the storage pool of body iron, its levels correlate well with body iron stores

Iron requirements
MEN
• Daily basal iron loss <1mg/day
• 10mg of iron in the diet with 10% absorption is sufficient to maintain iron balance
WOMEN
• Menstruating: 1.5mg/day
• Pregnancy: 2mg/day or 500mg for 280days of gestation

Regulation of iron absorption

Iron absorption is regulated by HEPCIDIN
• Nature: Small peptide
• Source: Liver
• Stimulus: Intrahepatic iron level dictates Hepcidin synthesis
• Action:
– Inhibits ferroportin
– Hence, inhibits iron transfer from the enterocyte to plasma

Diseases with abnormal iron metabolism Basis: Alterations in hepcidin
• Anemia of chronic disease
• Mutations that disable TMPRSS6
• Primary and secondary hemochromatosis
– Associated with mutations in hepcidin or the genes that regulate hepcidin expression
• Ineffective erythropoiesis suppresses hepatic hepcidin production, even when iron stores are high (unknown mechanim)

Prevalence of iron deficiency in India
• Pregnant women 70-90%
• Pre-school children 50%

Causes of iron deficiency
• Nutrional
– Decreased dietary intake
– Increased physiological demand
• Pregnancy
• Lactation
• Iron malabsorption
• Blood loss
Chase the cause

Causes of blood loss
• Gastrointestinal
• Pulmonary
– Hemosiderosis
• Urinary
– Hematuria
– Hemoglobinuria
• Uterine
– Menorrhagia

Causes of GI blood loss
• Esophagus – web
– Varices
– Reflux
– Carcinoma
• Stomach – Ulcer
– Carcinoma
– Leiomyoma
– Gastritis
• Small intestine – Meckel’s divrticulum
– Duodenal ulcer
– Crohn’s
• Large intestine – Polyps
– AV malformations
– Carcinoma
– Ulcerative colitis
– Amebiasis
– Tuberculosis
– Hemorrhoids

Iron deficiency in children
• Most common between 1.5 to 4yrs
• Iron deficiency in children is so important because of the possibility that there may be irreversible impairment of cognitive skills

Blood and BM findings in IDA
Peripheral blood
• <HGB
• <MCV
• <MCH
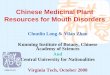
• Microcytic hypochromic
• Aniospoikilocytosis
• Pencil shaped cells
• Tailed poikilocytes
• There may be Thrombocytosis
Bone marrow
• Erythroid hyperplasia
• Micronormoblastic maturation
• Leucocytes and MKc may be normal

Microcytic hypochromic anemia of iron deficiency (peripheral blood smear)

Why anisocytosis in iron deficiency?
It’s due to differences in availability of iron in different areas of the bone marrow

Diagnosis of IDA

Laboratory evaluation of iron status
• Serum iron and iron binding capacity
• Serum ferritin
• Bone marrow iron status (Perl’s stain)
• Serum transferrin
• Plasma transferrin receptor
• RBC protoporphyrin

Serum transferrin receptor levels
• Good correlation with erythron mass
– Increased in hemolytic anemia
• Good correlation with iron deficiency in which it’s increased
• Not increased in anemia of chronic disease

Important points

Regulation of fe balance is mainly by absorption

Ferritn levels < 12 is indicative of fe deficiency

“Chase the cause in bleeding”

Weakness in IDA is disproportionate to HGB levels

Iron loss is mainly thru…..
• Hair growth
• Skin desquamation
• Menstruation / blood loss

Role of acid in fe absorption

Common cause of anemia in children

How gastrectomy causes anemia?
• Low or no acid secretion

How GJ causes anemia (IDA)

Causes for chronic blood loss

External bleeding Vs bleeding in to the tissues and Fe deficiency

Occult colonic carcinoma -
• Ask for occult blood test on stool

Main causes for microcytic hypochromic anemia
• Iron deficiency anemia
• Thalassemia
• Sideroblastic anemia
• Anemia of chronic disease

Sequence of events in iron deficiency
At presentation
• Disappearance of iron stores
• Drop in hgb
• Microcytosis
With treatment
• Disappearance of microcytosis
• Raise in hgb
• Restoration of body iron pool

E N D

Dr.CSBR.Prasad, M.D.,
Associate Professor of Pathology,
Sri Devaraj Urs Medical College,
Kolar-563101,
Karnataka,
INDIA.