Embed Size (px)
DESCRIPTION
재발성 자연 유산
Citation preview
Recurrent Spontaneous Abortion (RSA)
- How to manage genetic cause?
관동대학교 의과대학 제일병원 산부인과불임 생식내분비 분과 ∙
양 광 문
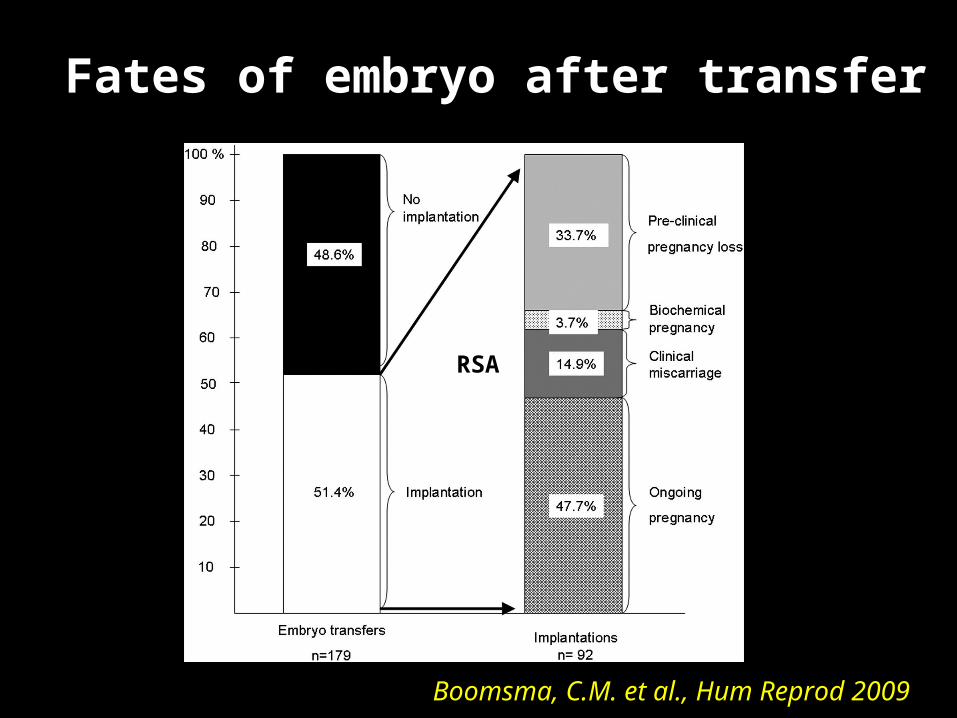
Fates of embryo after transfer
Boomsma, C.M. et al., Hum Reprod 2009
RSA
Definition of RSA (I)• Traditionally, ≥ 3 clinical pregnancy losses
before 20 weeks from the last menstrual period
- occurs in about 1/300 pregnancies. Novak 15th ed., WILCOX et al, 1988
• Risk of subsequent pregnancy loss– 24% after 2 clinical losses– 30% after 3 losses– 40~50% after 4 losses Novak 15th ed., Regan et al, 1989
Definition of RSA (II)
• In 2008, the American Society for Reproductive Medicine (ASRM) defined RPL by two or more failed pregnancies, and pregnancy must be clinical
: documented by ultrasound or histopathologic
examination
Indications of clinical Indications of clinical investigationinvestigation
• Clinical investigation may be initiated after 2 consecutive SA
especially,
• when fetal heart activity is identified • when the women is older than 35 years old• when the couple has had difficulty conceiving
-1% of pregnant women
Novak 15th ed., Alberman et al, 1988
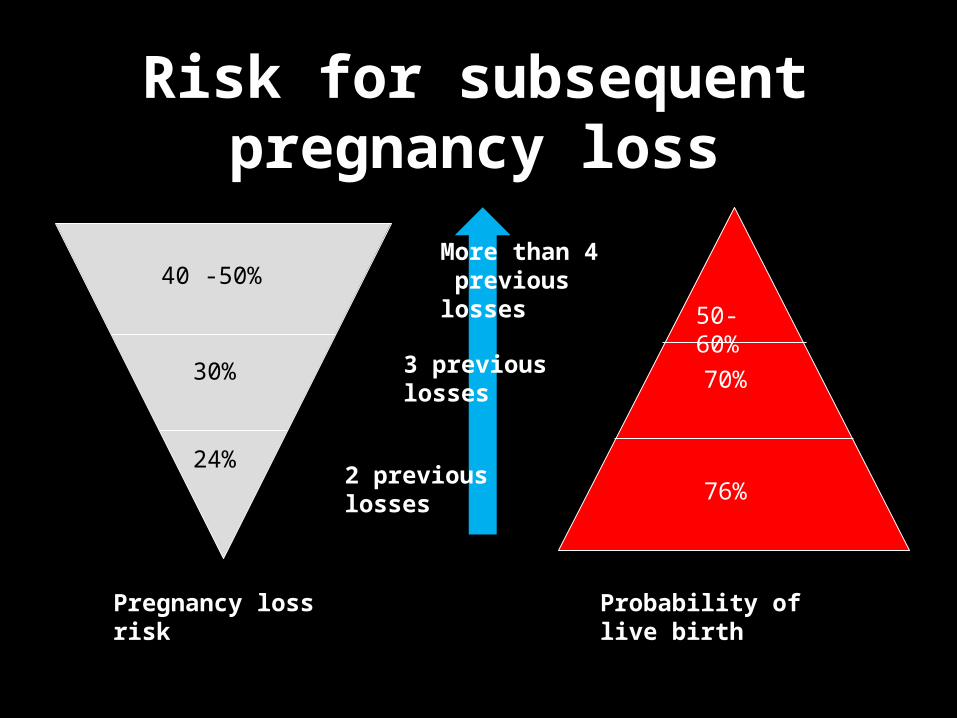
Risk for subsequent pregnancy loss
Pregnancy loss risk
Probability of live birth
24%
30%
40 -50%
76%
70%
50- 60%
3 previous losses
More than 4 previous losses
2 previous losses
Regan et al., 1989
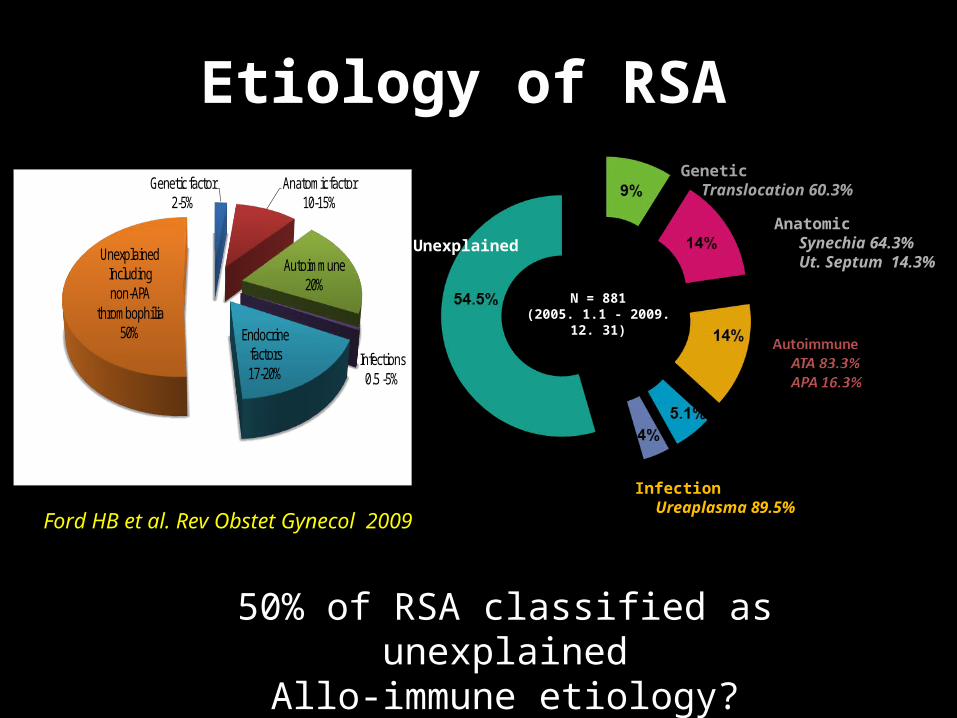
Etiology of RSA
Genetic factor2-5%
Anatomic factor10-15%
Autoimmune 20%
Infections0.5 -5%
Endocrine factors17-20%
UnexplainedIncluding non-APA
thrombophilia50%
Ford HB et al. Rev Obstet Gynecol 2009
Unexplained
Genetic Translocation 60.3%
Anatomic Synechia 64.3% Ut. Septum 14.3%
Endocrine Hyperthyroidism 71.4%Infection
Ureaplasma 89.5%
N = 881(2005. 1.1 - 2009. 12. 31)
50% of RSA classified as unexplained Allo-immune etiology?
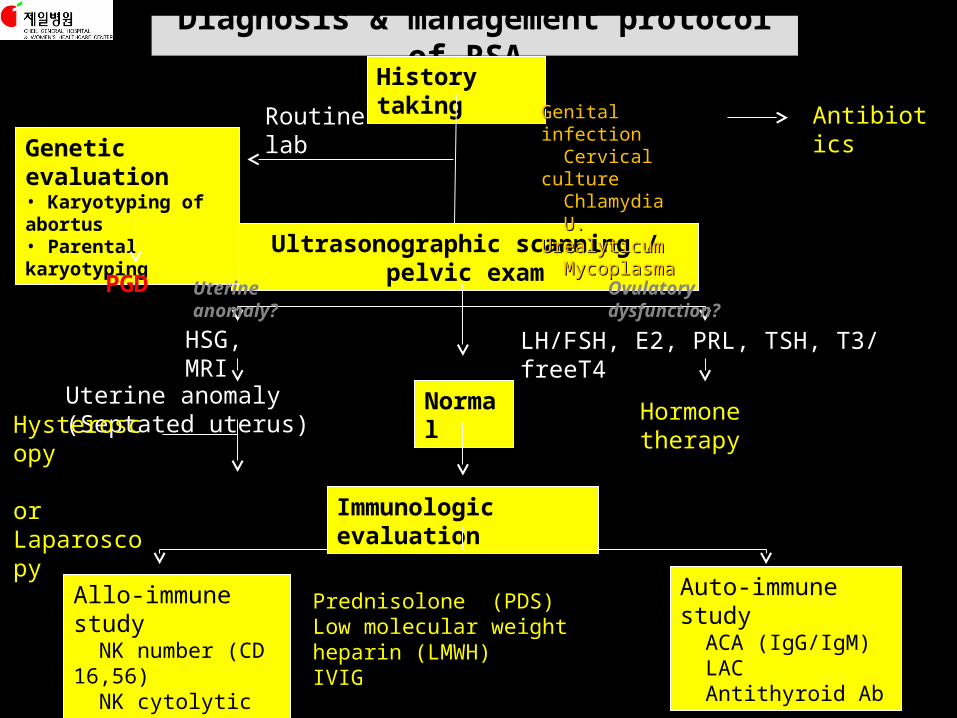
Diagnosis & management protocol of RSA History taking
Ultrasonographic scanning / pelvic exam
Normal
Genetic evaluation• Karyotyping of abortus• Parental karyotyping
Immunologic evaluation
Routine lab Genital infectionGenital infection Cervical cultureCervical culture ChlamydiaChlamydia U. UrealyticumU. Urealyticum MycoplasmaMycoplasma
HSG, MRI LH/FSH, E2, PRL, TSH, T3/ freeT4
Uterine anomaly (Septated uterus)Hysteroscopy orLaparoscopy
Hormone therapy
Allo-immune study NK number (CD 16,56) NK cytolytic activity
Auto-immune study ACA (IgG/IgM) LAC Antithyroid Ab
PGD
AntibioticsAntibiotics
Surgery
Prednisolone (PDS)Low molecular weight heparin (LMWH)IVIGIVIG
Uterine anomaly? Ovulatory dysfunction?
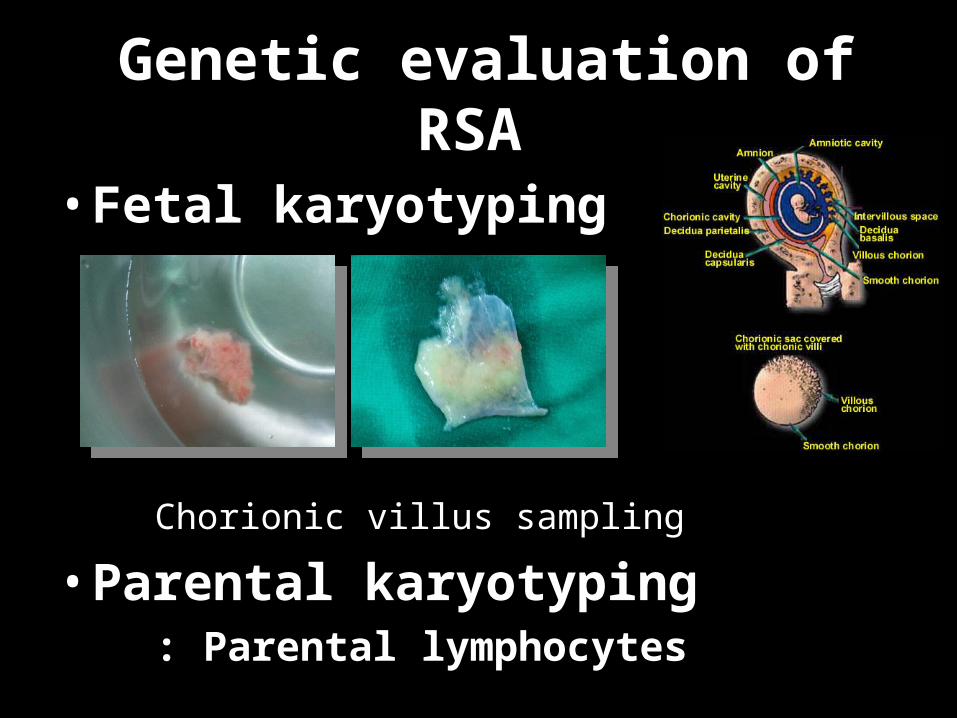
Genetic evaluation of RSA
• Fetal karyotyping
Chorionic villus sampling
• Parental karyotyping : Parental lymphocytes
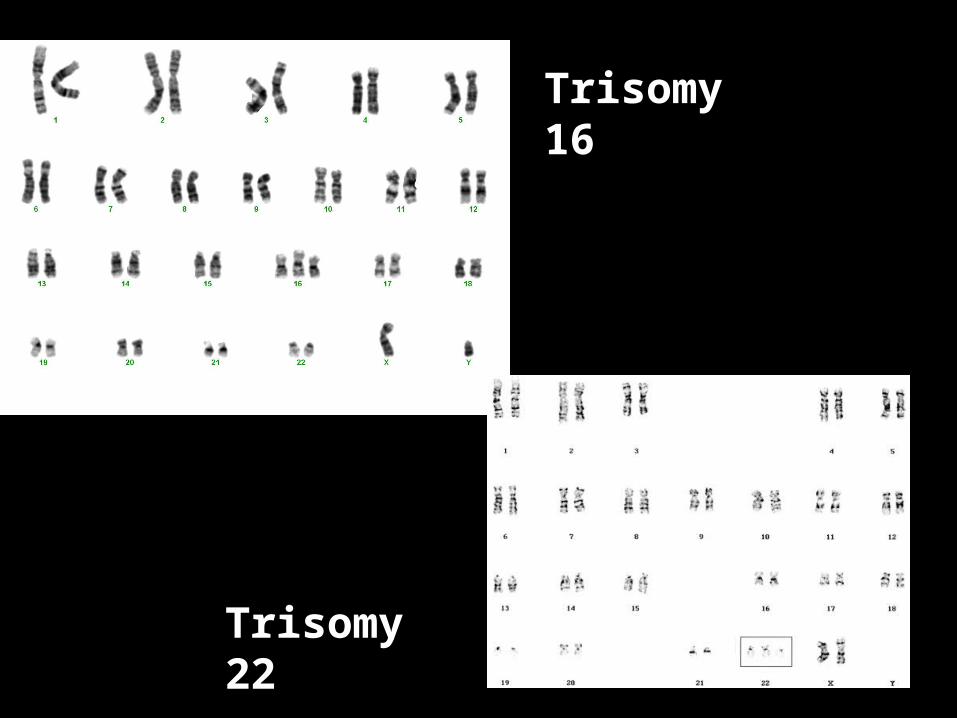
Trisomy 16
Trisomy 22
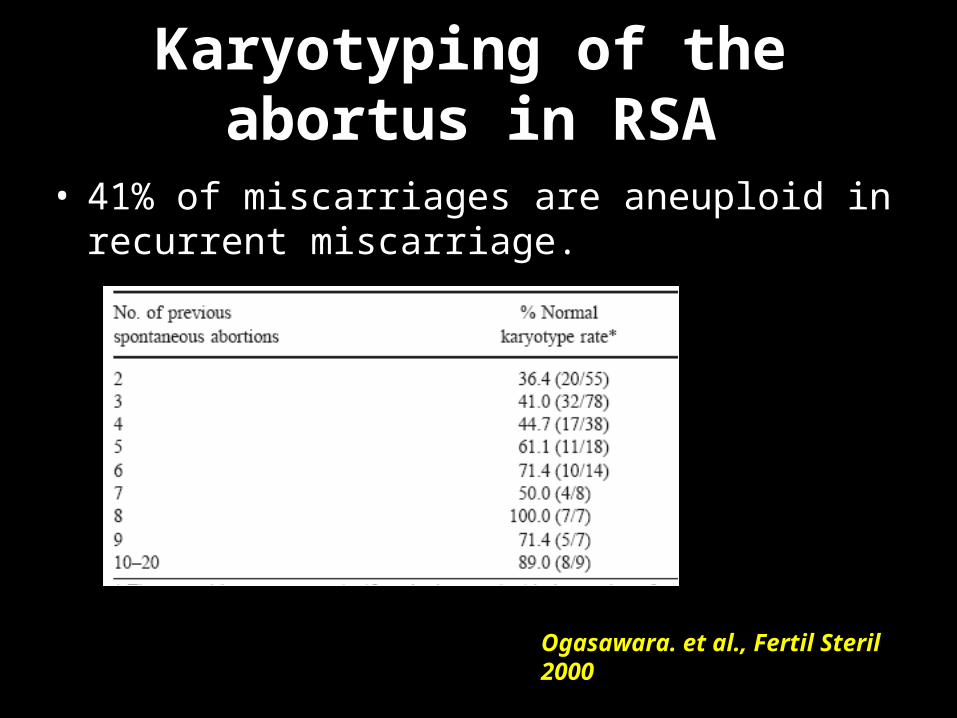
Karyotyping of the abortus in RSA
• 41% of miscarriages are aneuploid in recurrent miscarriage.
Ogasawara. et al., Fertil Steril 2000
• The prognosis is better after an aneuploid abortion than a euploidy miscarriage.• 15% of patients will have repeat
aneuploidy. : can be offered pre-implantation genetic
screening (PGS).
Karyotyping of the abortus
- Howard et al., IMAJ 2008
• The value of parental karyotyping is limited in recurrent miscarriage. • Seeks balanced translocations and inversions
rather than the more common numerical aberrations such as trisomy.
• Parental karyotypic aberrations have been found in
3–10% of couples with recurrent miscarriage. : PGD is indicated
Parental karyotyping
- Howard et al., IMAJ 2008
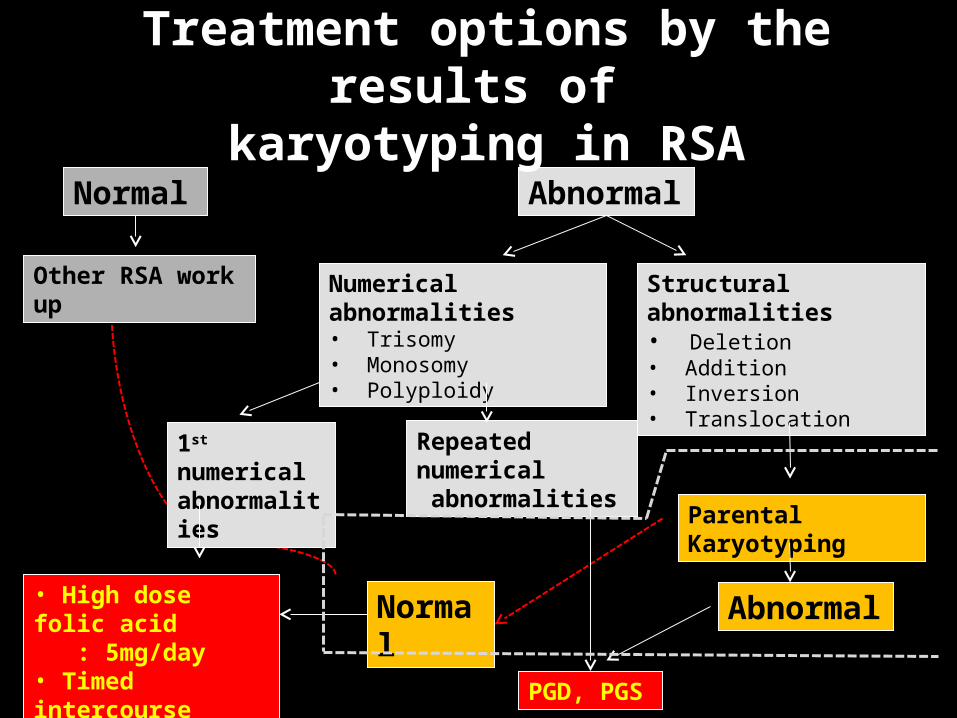
Normal
Other RSA work up
Parental Karyotyping
Abnormal
PGD, PGS
Normal
Abnormal
Numerical abnormalities• Trisomy• Monosomy• Polyploidy
1st numerical abnormalities
Repeated numerical abnormalities
Structural abnormalities• Deletion• Addition• Inversion• Translocation
• High dose folic acid : 5mg/day• Timed intercourse
Treatment options by the results of
karyotyping in RSA
1. Supplement of high dose folic acid2. Timed intercourse3. Prenatal Genetic Screening (PGS)
Prevention of repeated aneuploidy pregnancy
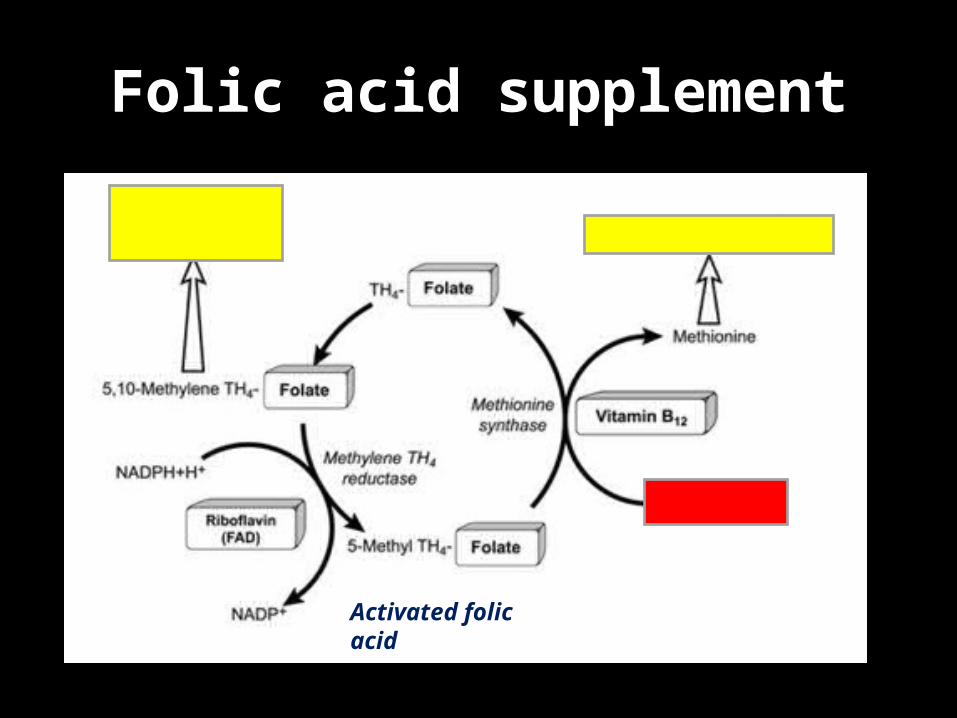
Folic acid supplement
Activated folic acid
Folic acid supplementation in
RSA patients • Abnormal folate and methyl metabolism can lead to DNA hypo-methylation, instability, abnormal segregation and aneuploidy. - Fenech M. Mutat Res 2001, Wang X,
Mutat Res. 2004
• Genomic instability is minimized when the plasma folate level
exceeds about 34 nmol/l and the Hcy level is less than 7.5 μmol/l. • These levels can only be achieved when folic acid intake is above 5mg per day. - Fenech M.
Mutat Res 2001
MTHFR gene mutation and folic acid supplement
• MTHFR (methylenetetrahydrofoloate reductase) gene
C677T
A1298C
• MTHFR gene mutation heterozygous MTHFR carriers - activate folate at 60-70% homozygous carriers - activate folate at 10% • Activated folic acid or high dose folic acid supplement
are recommended
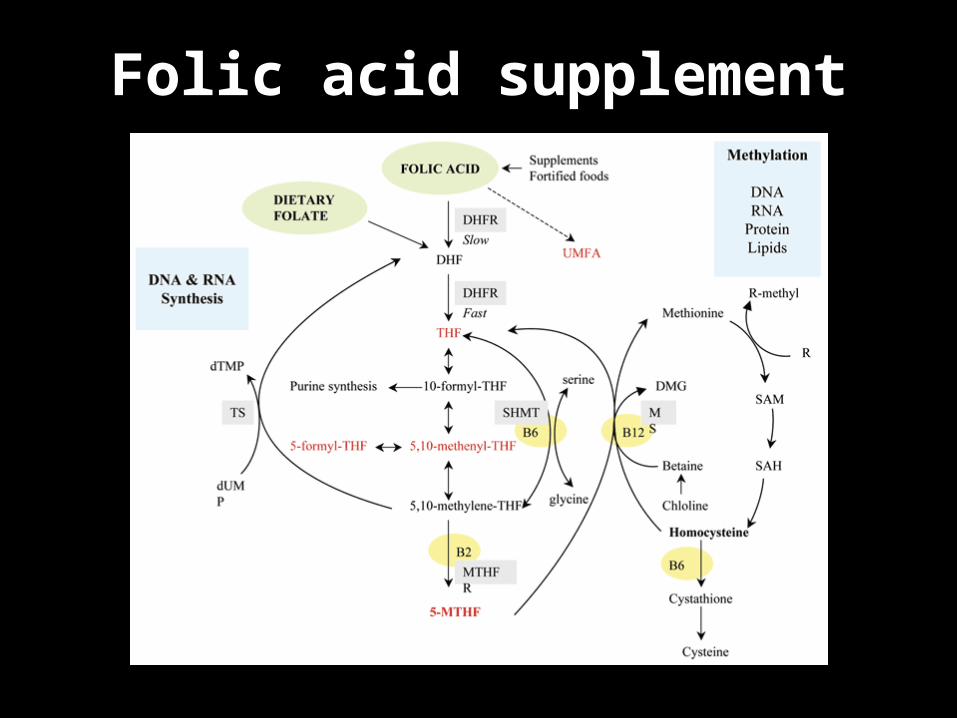
Folic acid supplement
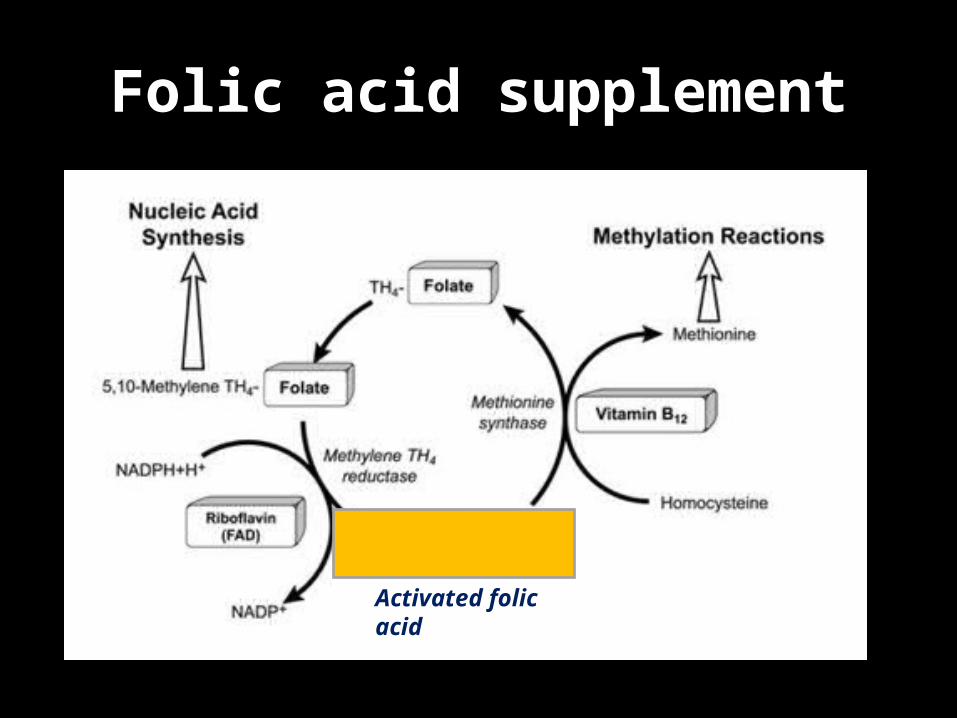
Folic acid supplement
Activated folic acid
Timed intercourse for prevention of repeated
aneuploidy• Prevention of delayed fertilization Secondary oocyte remains in MII metaphase in the fallopian tube until it is fertilized. Ageing or over-ripeness of these cells could lead to a higher incidence of spindle defects and so increase the
chance of non-disjunction. Chromosomal errors increase with delayed fertilization, although it is difficult to distinguish this from the
maternal age effect.
Ishikawa H et al., Hum Reprod 1995
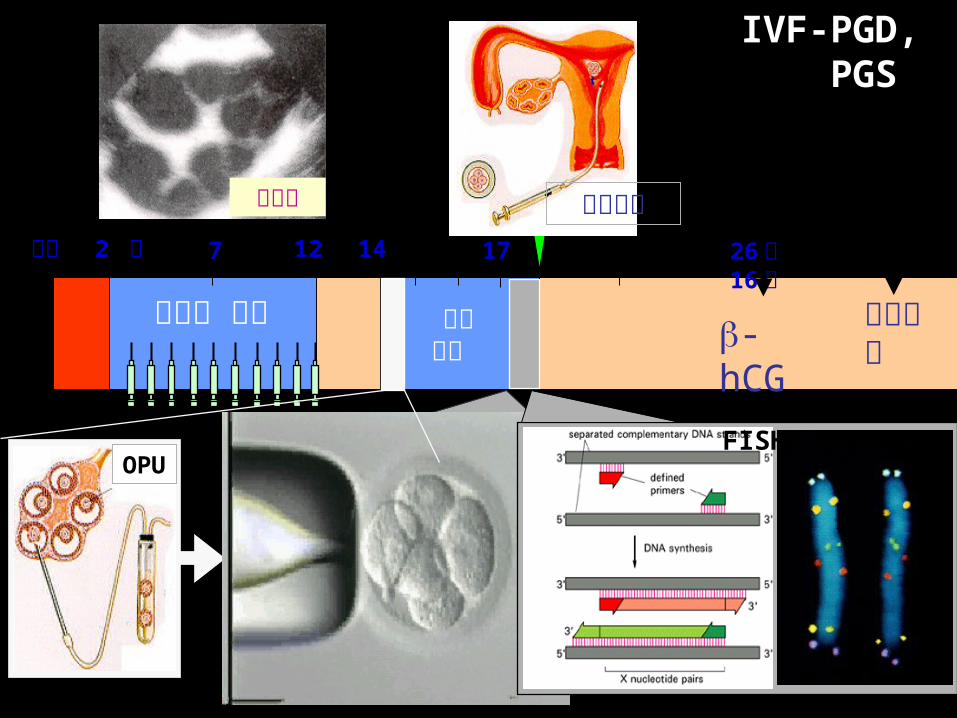
OPU수정
IVF-PGD, PGS
PCR
FISH
배아 배양
26 일 16주
17141272 일생리
과배란 유도
초음파 배아이식
-hCG양수천자
PCR FISH
Embryo 7
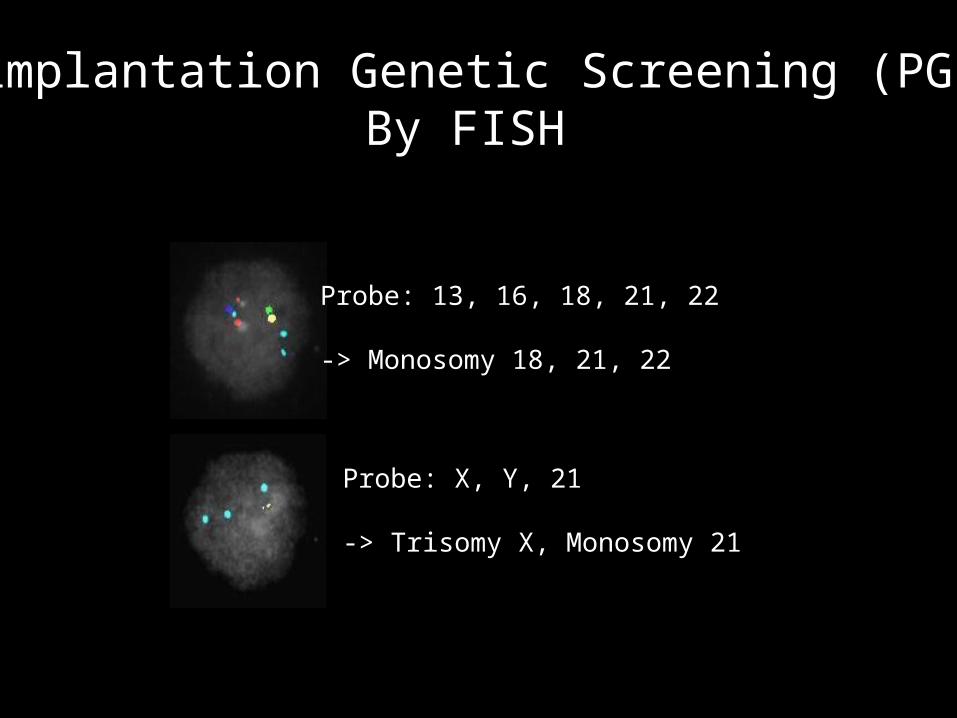
Probe: 13, 16, 18, 21, 22
-> Monosomy 18, 21, 22
Probe: X, Y, 21
-> Trisomy X, Monosomy 21
A.Handyside, RBM Online 2011;23:686-91
Preimplantation Genetic Screening (PGS) By FISH
The first techniques used for PGS were polar body biopsy or cleavage-stage blastomere biopsy followed by fluorescence in situ hybridization (FISH) analysis -> first-generation PGS
Initial studies with first-generation PGS suggested that implantation rates increased and loss rates decreased.
However, other studies, including several randomized controlled trials (RCTs), showed no benefit or, worse, a negative impact on implantation, pregnancy, or loss rates.
Preimplantation Genetic Screening (PGS) By FISH
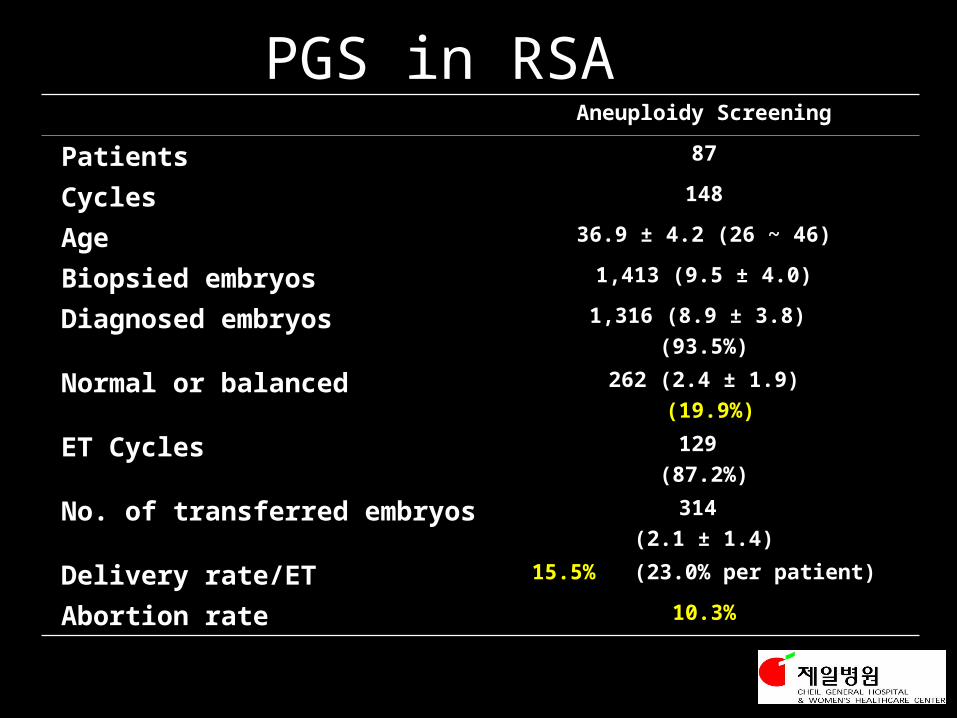
PGS in RSA Aneuploidy Screening
Patients 87
Cycles 148
Age 36.9 ± 4.2 (26 ~ 46)
Biopsied embryos 1,413 (9.5 ± 4.0)
Diagnosed embryos 1,316 (8.9 ± 3.8)
(93.5%)
Normal or balanced 262 (2.4 ± 1.9)
(19.9%)
ET Cycles 129
(87.2%)
No. of transferred embryos 314
(2.1 ± 1.4)
Delivery rate/ET 15.5% (23.0% per patient)
Abortion rate 10.3%
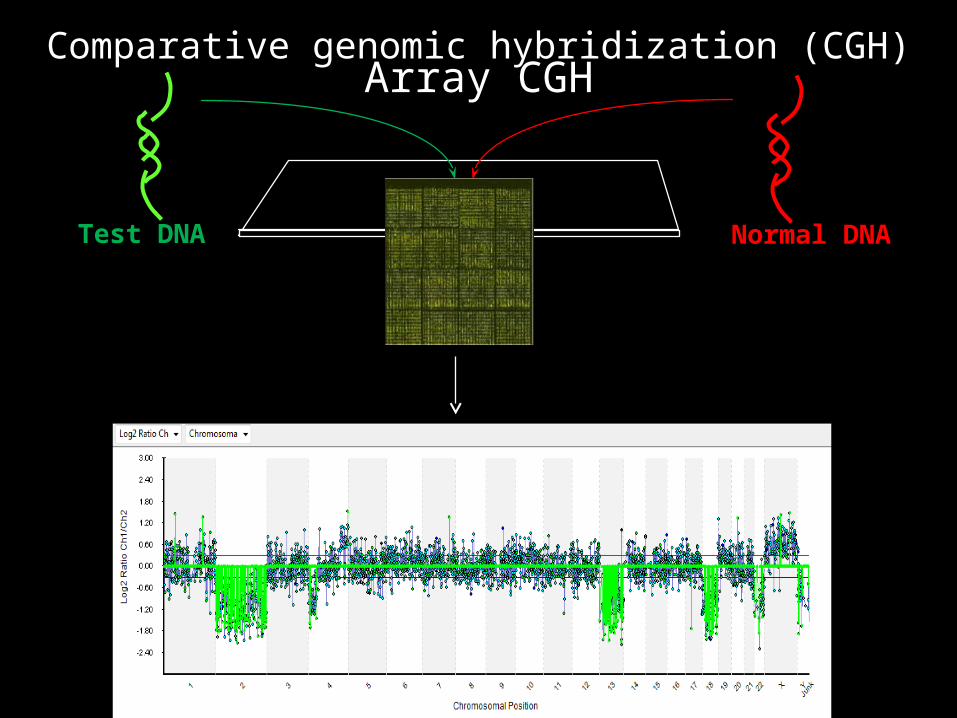
Comparative genomic hybridization (CGH)
Normal DNANormal DNATest DNATest DNA
MonosomyMonosomyTrisomyTrisomyNormalNormal
Array CGH
27
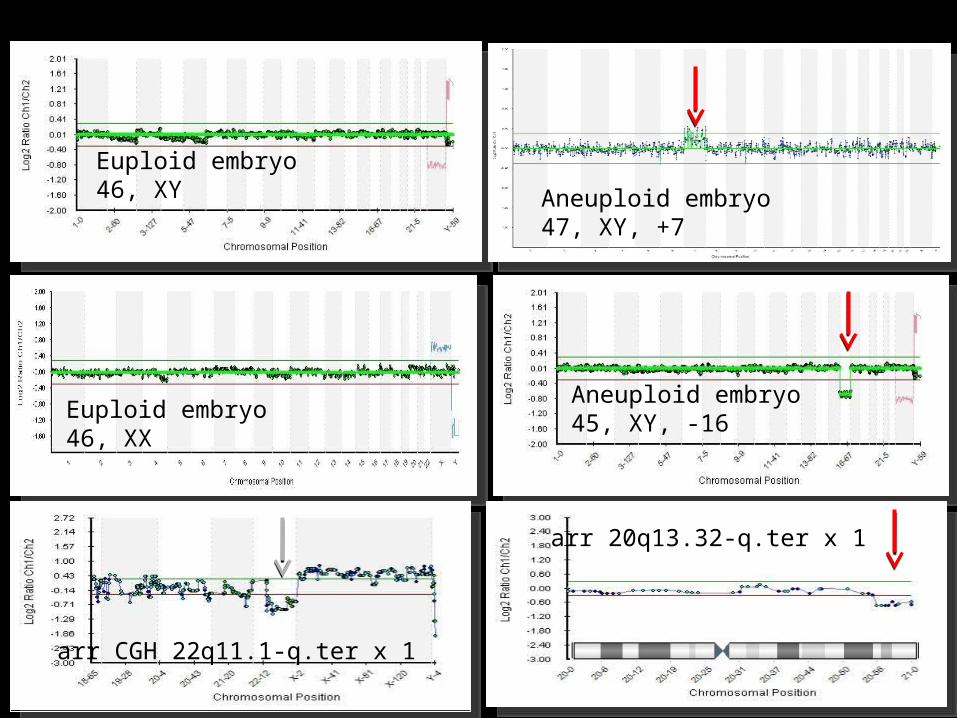
Euploid embryo46, XY Aneuploid embryo
47, XY, +7
Euploid embryo46, XX
Aneuploid embryo45, XY, -16
arr CGH 22q11.1-q.ter x 1
arr 20q13.32-q.ter x 1
An ideal technique would allow for the simultaneous analysis of all 24 chromosomes (autosomes 1–22, X, and Y) and less prone to technical issues that could lead to errors and misdiagnosis than earlier FISH methods.
The first comprehensive analysis technique appearing after FISH was comparative genomic hybridization (CGH), but it was challenging to put into clinical practice because it needed at least three full days for the analysis to be completed.
Finally, the advent of vitrification, which permitted the safe cryopreservation of biopsied embryos, allowed all the components for second-generation PGS to be assembled: complete chromosome screening (via CGH); less damaging embryo biopsy (at the blastocyst stage); and enough time to carry out the test (afforded by vitrification).
CGH was later displaced by more automated techniques, such as aCGH, single-nucleotide polymorphism (SNP) arrays, and quantitative fluorescent polymerase chain reaction (qPCR).
Of these techniques, aCGH and qPCR have been shown in RCTs to improve pregnancy rates.
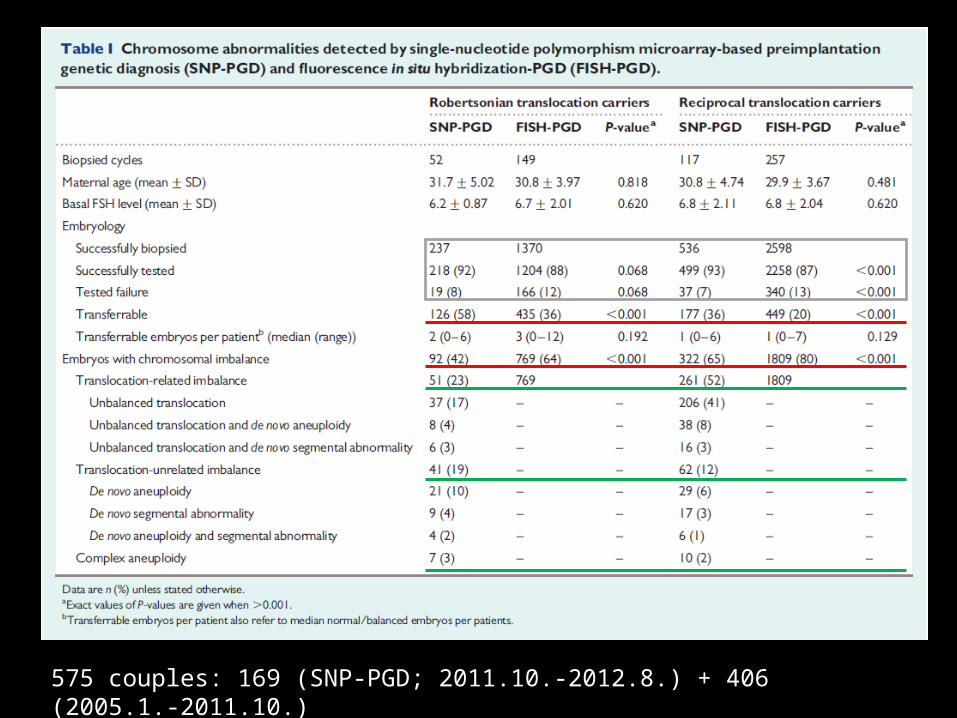
575 couples: 169 (SNP-PGD; 2011.10.-2012.8.) + 406 (2005.1.-2011.10.)

Early Diagnosis for Early Cure!
KFDA Certification
‘BAC Chip H1440’ was approved from the Korea Food and Drug Administration(KFDA) in March 2006
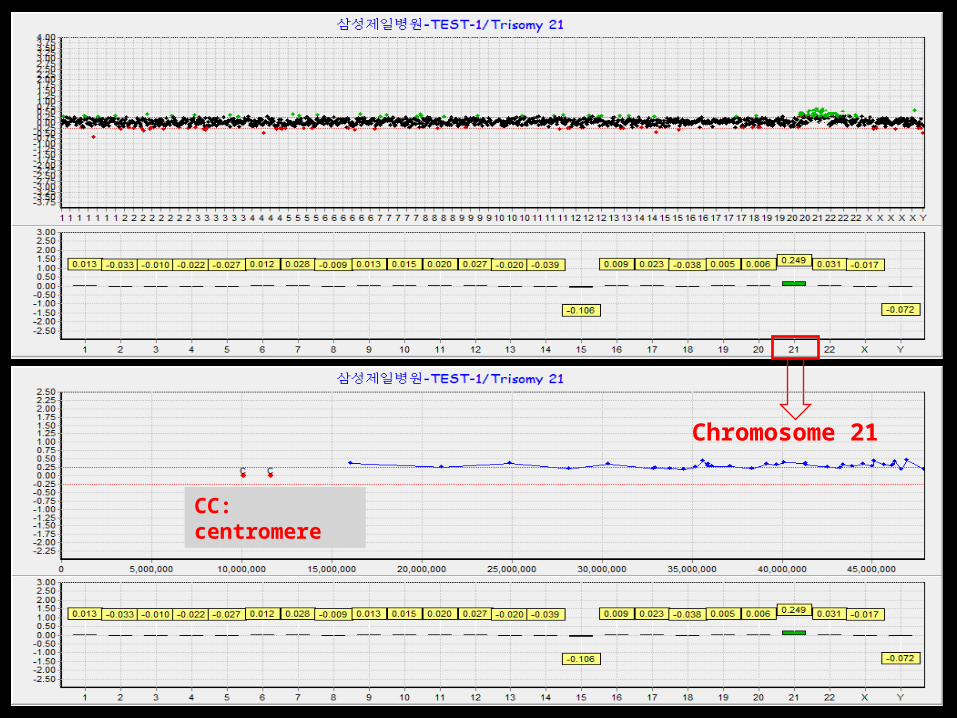
CC: centromere
Chromosome 21
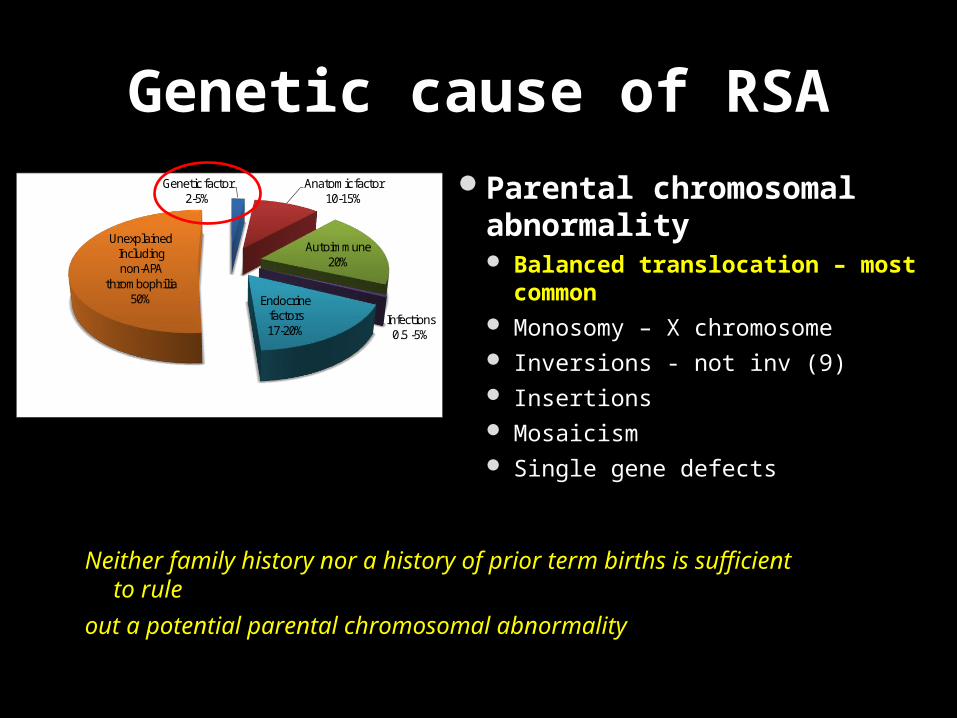
Parental chromosomal abnormality Balanced translocation – most common Monosomy – X chromosome Inversions - not inv (9) Insertions Mosaicism Single gene defects
Genetic factor2-5%
Anatomic factor10-15%
Autoimmune 20%
Infections0.5 -5%
Endocrine factors17-20%
UnexplainedIncluding non-APA
thrombophilia50%
Genetic cause of RSA
Neither family history nor a history of prior term births is sufficient to rule
out a potential parental chromosomal abnormality
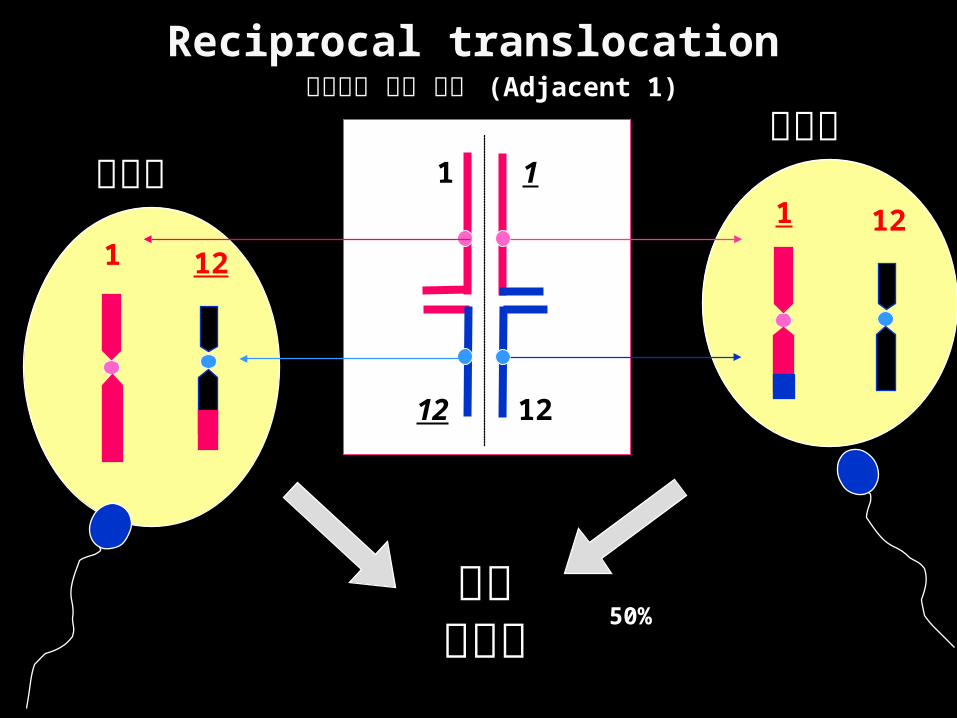
비정상적 감수 분열 (Adjacent 1)
비정상12
1
1
12
비정상1 1
12 12
유산기형아
Reciprocal translocation
50%
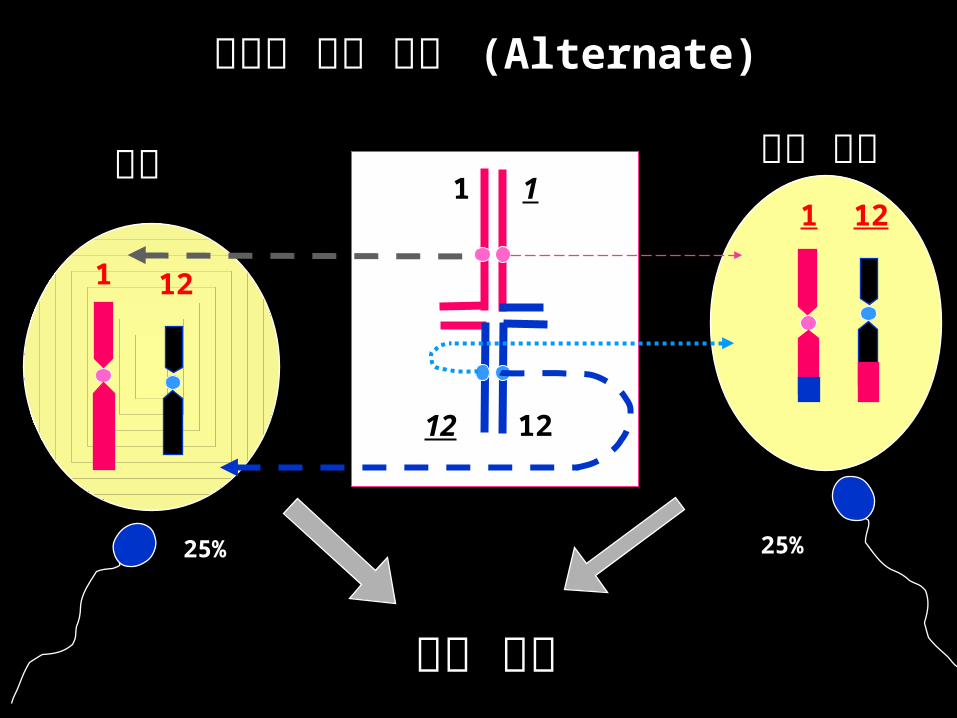
정상적 감수 분열 정상적 감수 분열 (Alternate)(Alternate)
균형 전좌정상1 1
12 12
121
1 12
정상 임신
25% 25%
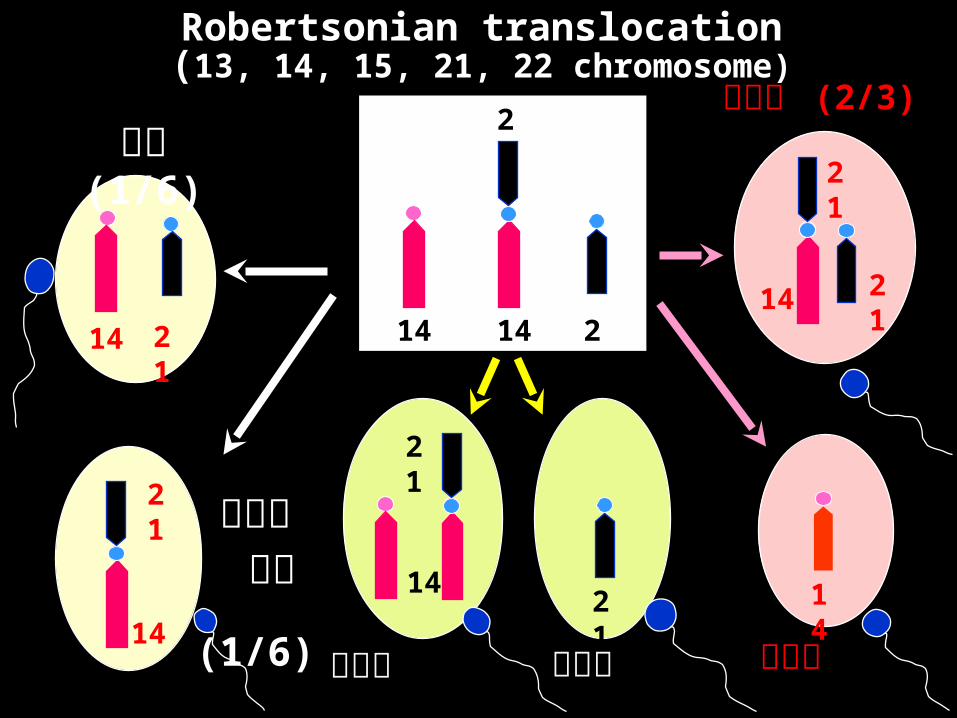
Robertsonian translocation(13, 14, 15, 21, 22 chromosome)
14 21
21
1421
21
14
21
14
21
14
정상 (1/6)
로벗슨 전좌 (1/6)
비정상 비정상
14
21
14
비정상 (2/3)
비정상
21
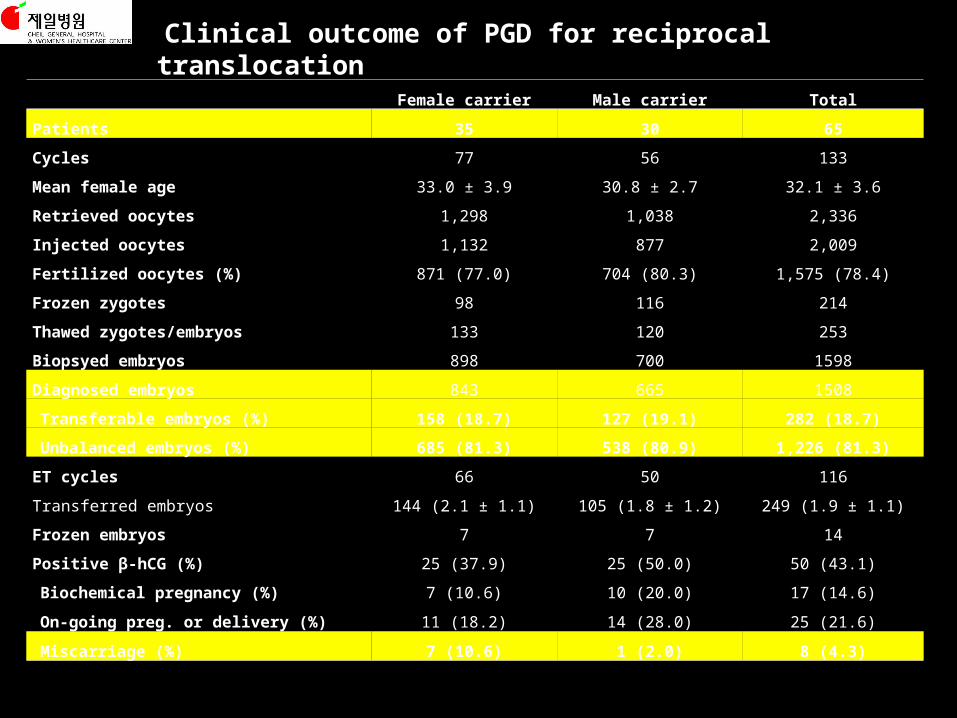
Female carrier Male carrier Total
Patients 35 30 65
Cycles 77 56 133
Mean female age 33.0 ± 3.9 30.8 ± 2.7 32.1 ± 3.6
Retrieved oocytes 1,298 1,038 2,336
Injected oocytes 1,132 877 2,009
Fertilized oocytes (%) 871 (77.0) 704 (80.3) 1,575 (78.4)
Frozen zygotes 98 116 214
Thawed zygotes/embryos 133 120 253
Biopsyed embryos 898 700 1598
Diagnosed embryos 843 665 1508
Transferable embryos (%) 158 (18.7) 127 (19.1) 282 (18.7)
Unbalanced embryos (%) 685 (81.3) 538 (80.9) 1,226 (81.3)
ET cycles 66 50 116
Transferred embryos 144 (2.1 ± 1.1) 105 (1.8 ± 1.2) 249 (1.9 ± 1.1)
Frozen embryos 7 7 14
Positive β-hCG (%) 25 (37.9) 25 (50.0) 50 (43.1)
Biochemical pregnancy (%) 7 (10.6) 10 (20.0) 17 (14.6)
On-going preg. or delivery (%) 11 (18.2) 14 (28.0) 25 (21.6)
Miscarriage (%) 7 (10.6) 1 (2.0) 8 (4.3)
Clinical outcome of PGD for reciprocal translocation
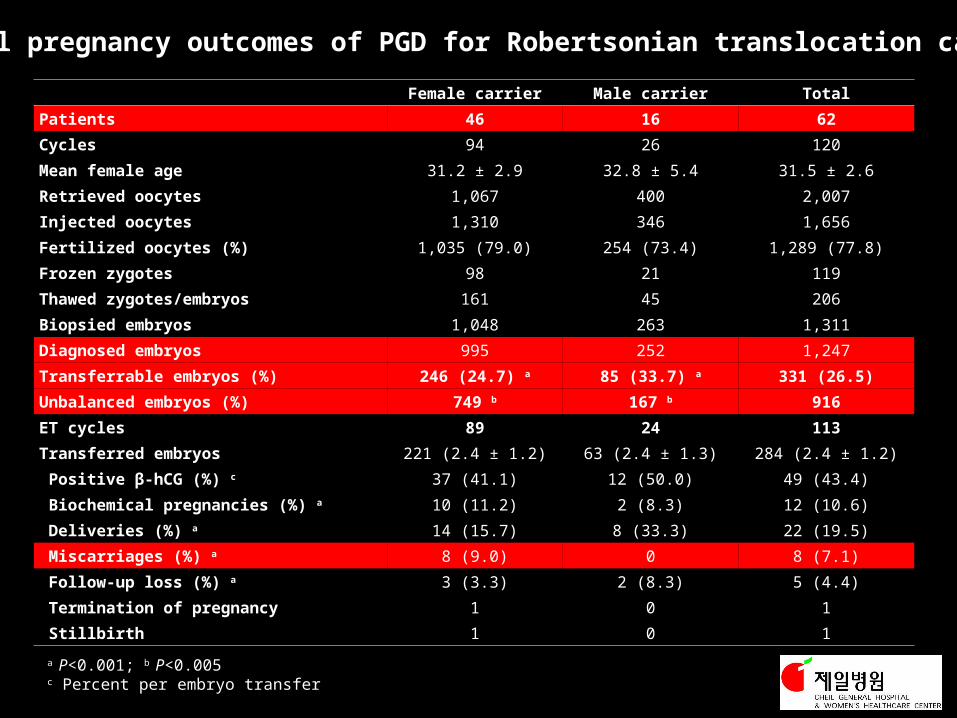
Female carrier Male carrier Total
Patients 46 16 62
Cycles 94 26 120
Mean female age 31.2 ± 2.9 32.8 ± 5.4 31.5 ± 2.6
Retrieved oocytes 1,067 400 2,007
Injected oocytes 1,310 346 1,656
Fertilized oocytes (%) 1,035 (79.0) 254 (73.4) 1,289 (77.8)
Frozen zygotes 98 21 119
Thawed zygotes/embryos 161 45 206
Biopsied embryos 1,048 263 1,311
Diagnosed embryos 995 252 1,247
Transferrable embryos (%) 246 (24.7) a 85 (33.7) a 331 (26.5)
Unbalanced embryos (%) 749 b 167 b 916
ET cycles 89 24 113
Transferred embryos 221 (2.4 ± 1.2) 63 (2.4 ± 1.3) 284 (2.4 ± 1.2)
Positive β-hCG (%) c 37 (41.1) 12 (50.0) 49 (43.4)
Biochemical pregnancies (%) a 10 (11.2) 2 (8.3) 12 (10.6)
Deliveries (%) a 14 (15.7) 8 (33.3) 22 (19.5)
Miscarriages (%) a 8 (9.0) 0 8 (7.1)
Follow-up loss (%) a 3 (3.3) 2 (8.3) 5 (4.4)
Termination of pregnancy 1 0 1
Stillbirth 1 0 1
Overall pregnancy outcomes of PGD for Robertsonian translocation carriers
a P<0.001; b P<0.005c Percent per embryo transfer
Summary
• Benefits of high dose folic acid
• Efficacy of timed intercourse
• MTHFR gene mutation needs activated or high dose folic acid
• CGH in patients with repeated aneuploidy
• PGD in patients with inheritable chromosome abnormalities

Thank you for your attention!





























