Embed Size (px)
Citation preview
SEROTONIN : DISEASES AND THERAPEUTICS
By: Dr. Gaurav Yadav
Source & Chemistry 3-(β-aminoethyl)-5-hydroxyindole Widely distributed in animals and plants. Present in sea food, meat, nuts, seeds, various grains. It is also present in venoms; common stinging nettles
and of wasps and scorpions. In humans it is found in high concentrations in
enterochromaffin cells throughout the gastrointestinal tract, in storage granules in platelets and broadly throughout the CNS.
HISTORY 1930s Erspamer studied distribution of enterochromaffin cells.
1948 Page and colleagues isolated and chemically characterized vasoconstrictor substance from platelets as 5-HT.
1957 Gaddum and Piccarelli classified 5-HT receptors into M and D type.
1959 Udenfriend discovered biosynthetic and degradative pathways.
1976 Page coined term SEROTONIN.
1979 Peroutka &Snyder identified 5HT1 and 5HT2 receptors by radioligand binding studies.
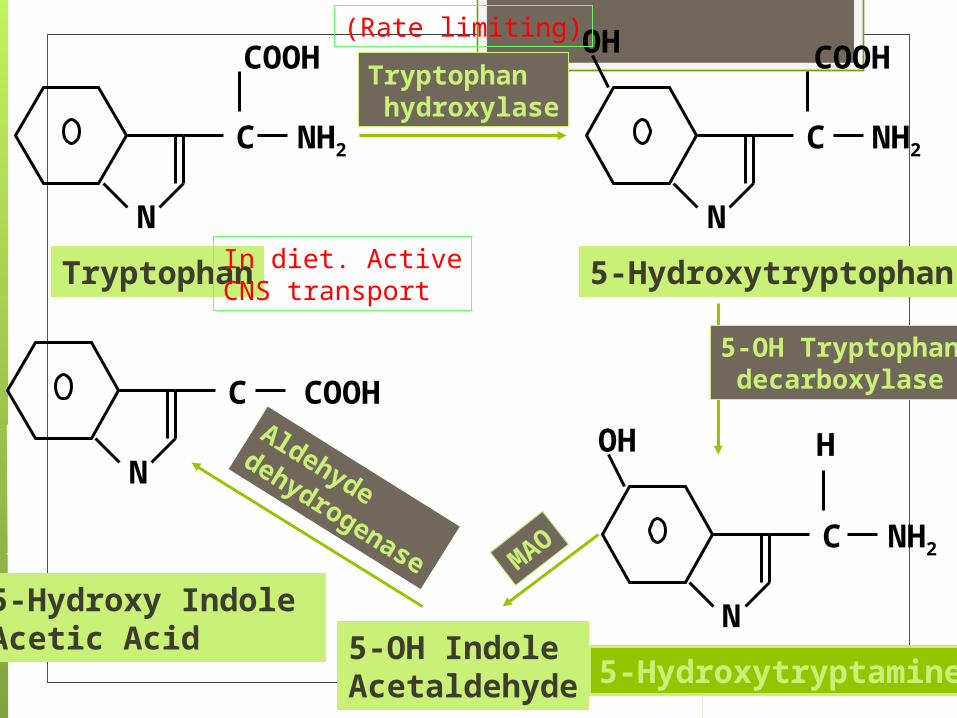
Synthesis and Metabolism 5-HT is synthesized by a two step pathway from the
essential amino acid tryptophan. Tryptophan is actively transported into the brain by a
carrier protein. Tryptophan hydroxylase is rate limiting enzyme . Rate limiting enzyme not saturated by substrate. 5-OHTr decarboxylase same as DOPA decarboxylase Breakdown mainly by MAO (MAO-A and MAO-B) 5-HIAA actively extruded from CNS and excreted in
urine.
N
C
N
C NH2
COOH COOH
NH2
OH
N
C NH2
OH H
Tryptophan 5-Hydroxytryptophan
5-Hydroxytryptamine
N
C COOH
5-OH Indole Acetaldehyde
5-Hydroxy Indole Acetic Acid
Tryptophan hydroxylase
5-OH Tryptophan decarboxylase
MAO
Aldehyde dehydrogenase
(Rate limiting)
In diet. ActiveCNS transport
Serotonin Receptors
There are 7 families (5-HT1-7) with further subtypes of 5-HT1(A,B,D,E,F) and 5-HT2(A-C)Multiple transduction mechanismsAll are G-protein coupled receptors, except 5-HT3 which is a ligand gated cation channel5-HT1 acts by decreasing cAMP, while 5-HT4-7 act by increasing cAMP.5-HT2 acts by phospholipase C/inositol triphosphate pathway.
5-HT1 receptorSubtype
Transduction mechanism
Location Physiological roles and therapeutic applications
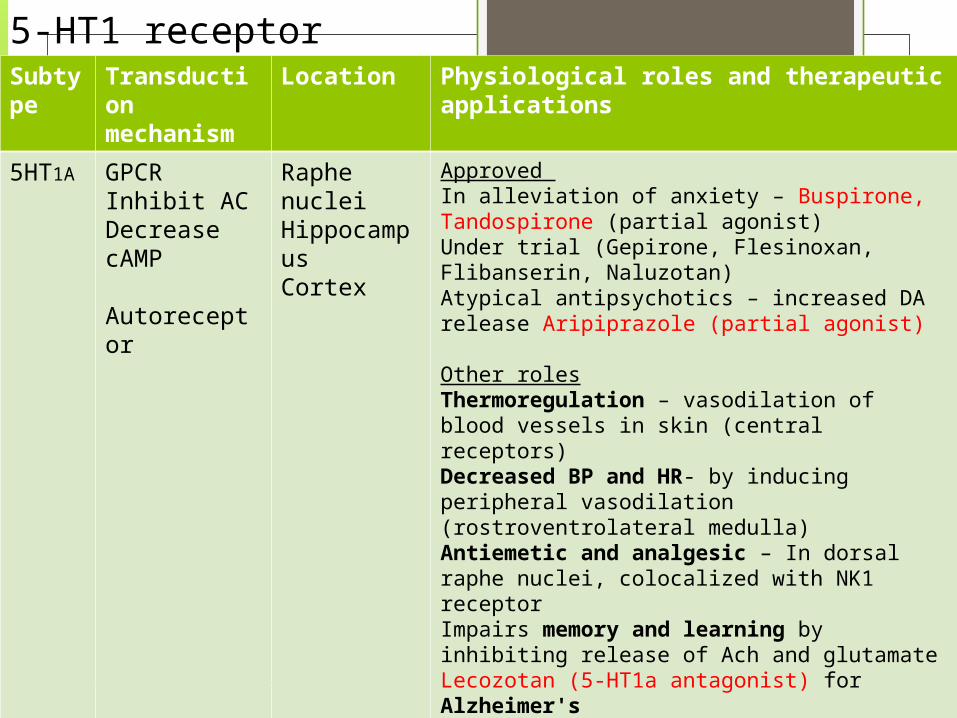
5HT1A GPCRInhibit ACDecrease cAMP
Autoreceptor
Raphe nucleiHippocampusCortex
Approved In alleviation of anxiety – Buspirone, Tandospirone (partial agonist)Under trial (Gepirone, Flesinoxan, Flibanserin, Naluzotan)Atypical antipsychotics – increased DA release Aripiprazole (partial agonist)
Other rolesThermoregulation – vasodilation of blood vessels in skin (central receptors)Decreased BP and HR- by inducing peripheral vasodilation (rostroventrolateral medulla)Antiemetic and analgesic – In dorsal raphe nuclei, colocalized with NK1 receptorImpairs memory and learning by inhibiting release of Ach and glutamate Lecozotan (5-HT1a antagonist) for Alzheimer'sVilazodone Vortioxetine– SERT inhibitor with 5HT1a partial agonist activity ; novel antidepressantIncreased secretion of oxytocin- prosocial, antiaggressive β endorphins- antidepressant, anxiolytic & analgesic.
5-HT1 receptorSubtype
Transduction mechanism
Location Physiological roles and therapeutic applications
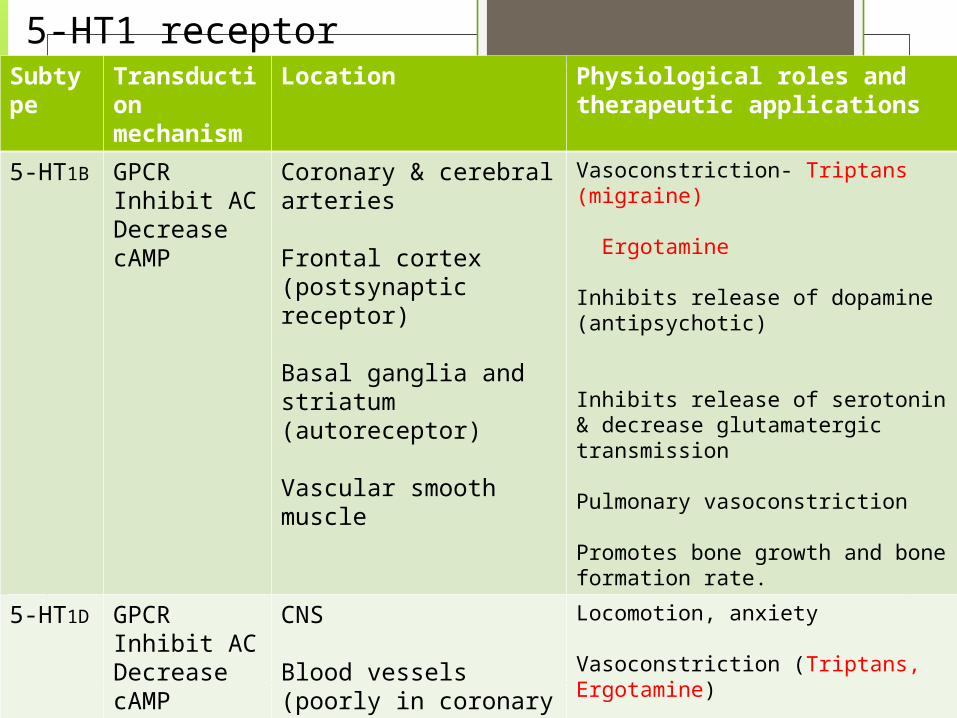
5-HT1B GPCRInhibit ACDecrease cAMP
Coronary & cerebral arteries
Frontal cortex (postsynaptic receptor)
Basal ganglia and striatum (autoreceptor)
Vascular smooth muscle
Vasoconstriction- Triptans (migraine) Ergotamine
Inhibits release of dopamine (antipsychotic)
Inhibits release of serotonin & decrease glutamatergic transmission
Pulmonary vasoconstriction
Promotes bone growth and bone formation rate.
5-HT1D GPCRInhibit ACDecrease cAMP
CNS
Blood vessels (poorly in coronary circulation)
Trigeminal ganglion
Locomotion, anxiety
Vasoconstriction (Triptans, Ergotamine)
Inhibit release of proinflammatory neuropeptides
5-HT1 receptorSubtype
Transduction mechanism
Location Physiological roles and therapeutic applications
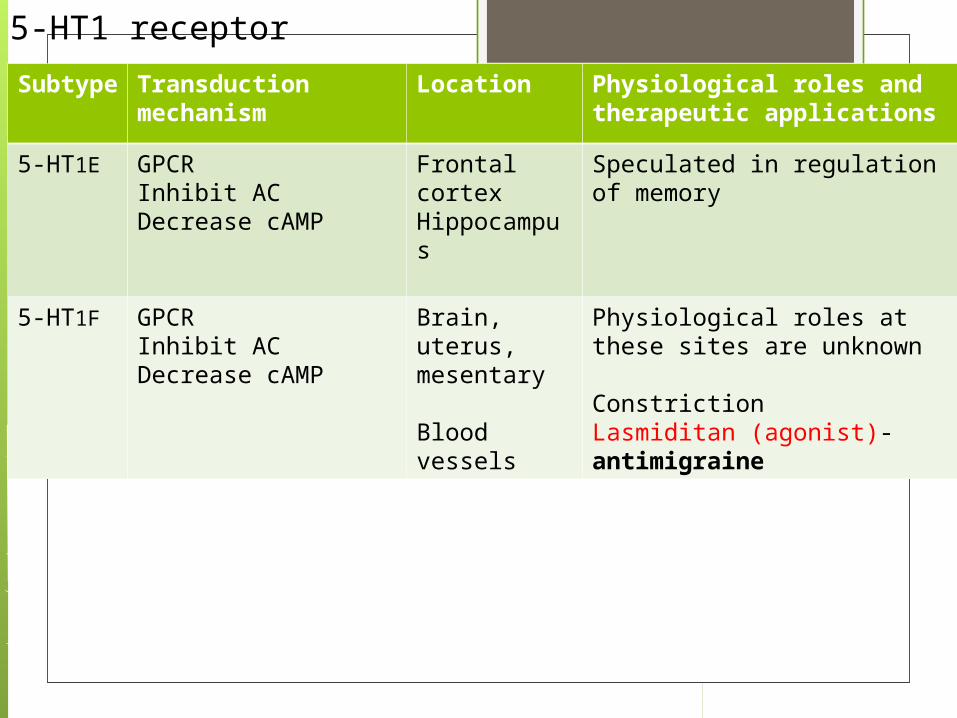
5-HT1E GPCRInhibit ACDecrease cAMP
Frontal cortexHippocampus
Speculated in regulation of memory
5-HT1F GPCRInhibit ACDecrease cAMP
Brain, uterus, mesentary
Blood vessels
Physiological roles at these sites are unknown
Constriction Lasmiditan (agonist)- antimigraine
5-HT2 receptorsSubtype
Transduction mechanism
Location Physiological roles and therapeutic applications
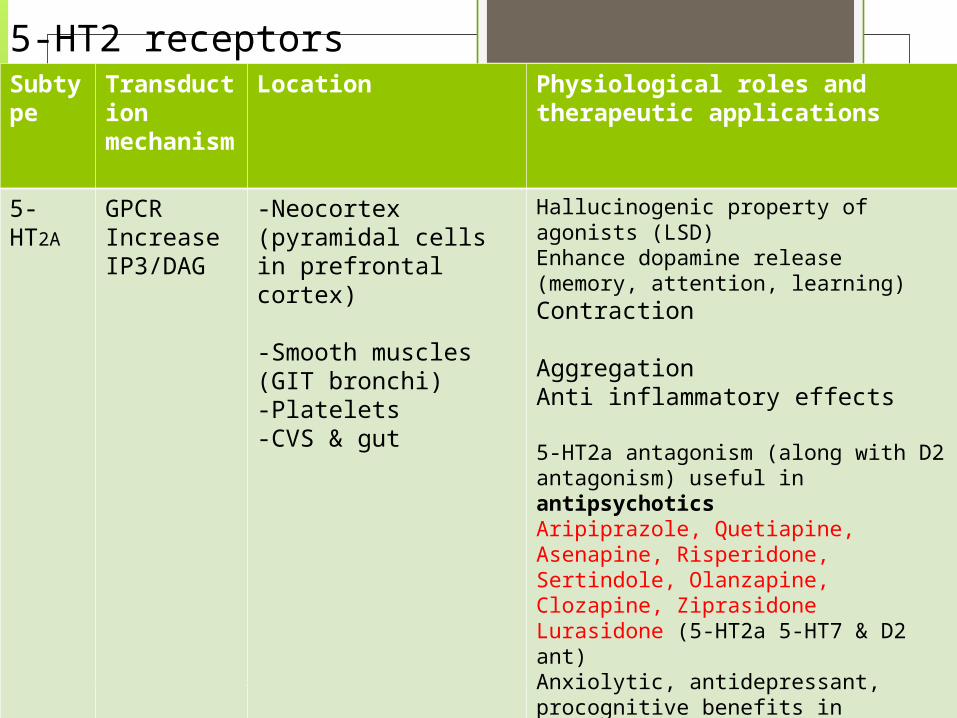
5-HT2A
GPCRIncrease IP3/DAG
-Neocortex (pyramidal cells in prefrontal cortex)
-Smooth muscles (GIT bronchi)-Platelets -CVS & gut
Hallucinogenic property of agonists (LSD)Enhance dopamine release (memory, attention, learning)Contraction
Aggregation Anti inflammatory effects
5-HT2a antagonism (along with D2 antagonism) useful in antipsychoticsAripiprazole, Quetiapine, Asenapine, Risperidone, Sertindole, Olanzapine, Clozapine, ZiprasidoneLurasidone (5-HT2a 5-HT7 & D2 ant)Anxiolytic, antidepressant, procognitive benefits in schizophrenia patients. AntidepressantsNefazodone (5-HT2a & SERT ant)Amoxapine
AL34662 possible role in glaucomaVolinanserin(5-HT2a inv agonist) insomnia
5-HT2 receptorSubtype
Transduction mechanism
Location Physiological roles and therapeutic applications
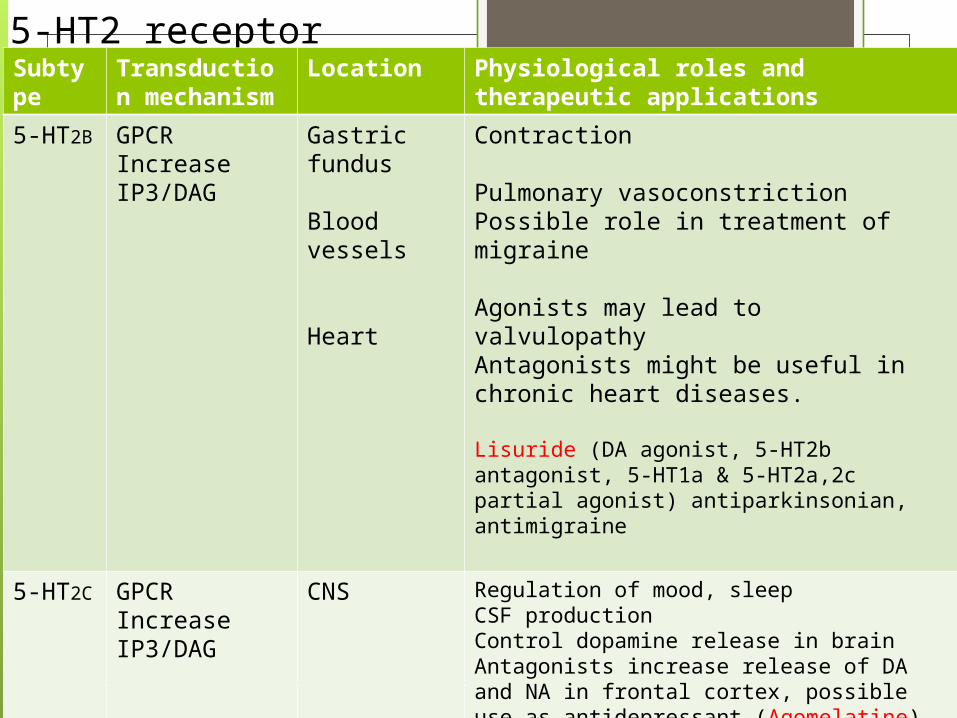
5-HT2B GPCRIncrease IP3/DAG
Gastric fundus
Blood vessels
Heart
Contraction
Pulmonary vasoconstrictionPossible role in treatment of migraine
Agonists may lead to valvulopathyAntagonists might be useful in chronic heart diseases.
Lisuride (DA agonist, 5-HT2b antagonist, 5-HT1a & 5-HT2a,2c partial agonist) antiparkinsonian, antimigraine
5-HT2C GPCRIncrease IP3/DAG
CNS Regulation of mood, sleepCSF productionControl dopamine release in brainAntagonists increase release of DA and NA in frontal cortex, possible use as antidepressant (Agomelatine)
Antipsychotics 5-HT2c antagonism (Sertindole, Ziprasidone)Lorcaserin 5HT2c selective agonist – anti obesity drug
Type Transduction mechanism
Location Physiological roles and therapeutic applications
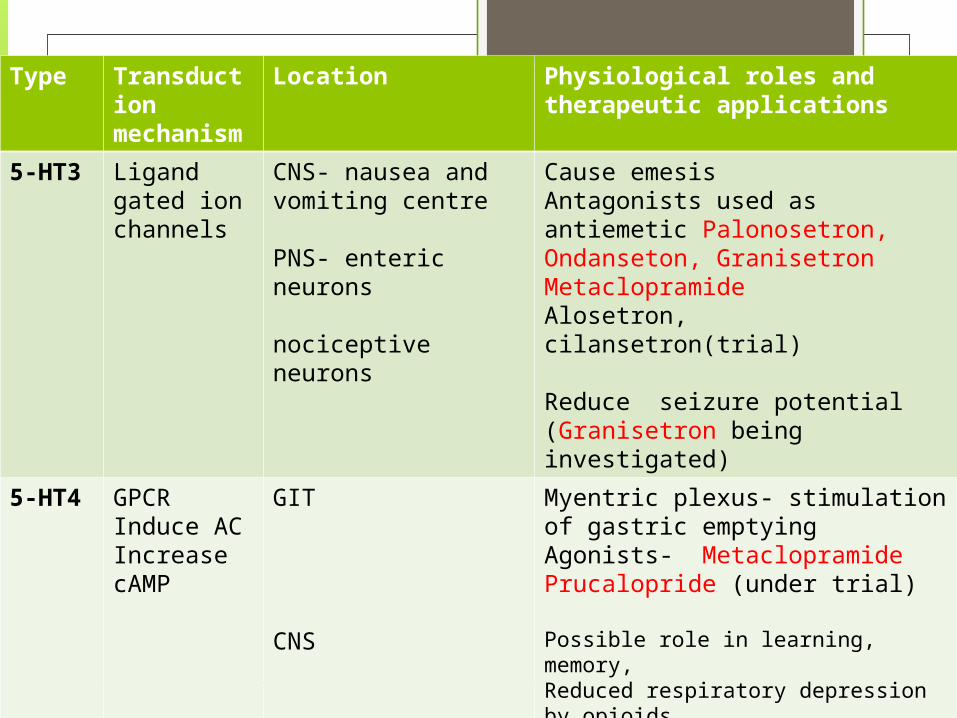
5-HT3 Ligand gated ion channels
CNS- nausea and vomiting centre
PNS- enteric neurons nociceptive neurons
Cause emesisAntagonists used as antiemetic Palonosetron, Ondanseton, GranisetronMetaclopramideAlosetron, cilansetron(trial)
Reduce seizure potential (Granisetron being investigated)
5-HT4 GPCRInduce ACIncrease cAMP
GIT
CNS
Myentric plexus- stimulation of gastric emptyingAgonists- MetaclopramidePrucalopride (under trial)
Possible role in learning, memory,Reduced respiratory depression by opioidsStimulation of aldosterone secretion from adrenal cortexReducing susceptibility to seizures
Type Transduction mechanisms
Location Physiological roles and therapeutic applications
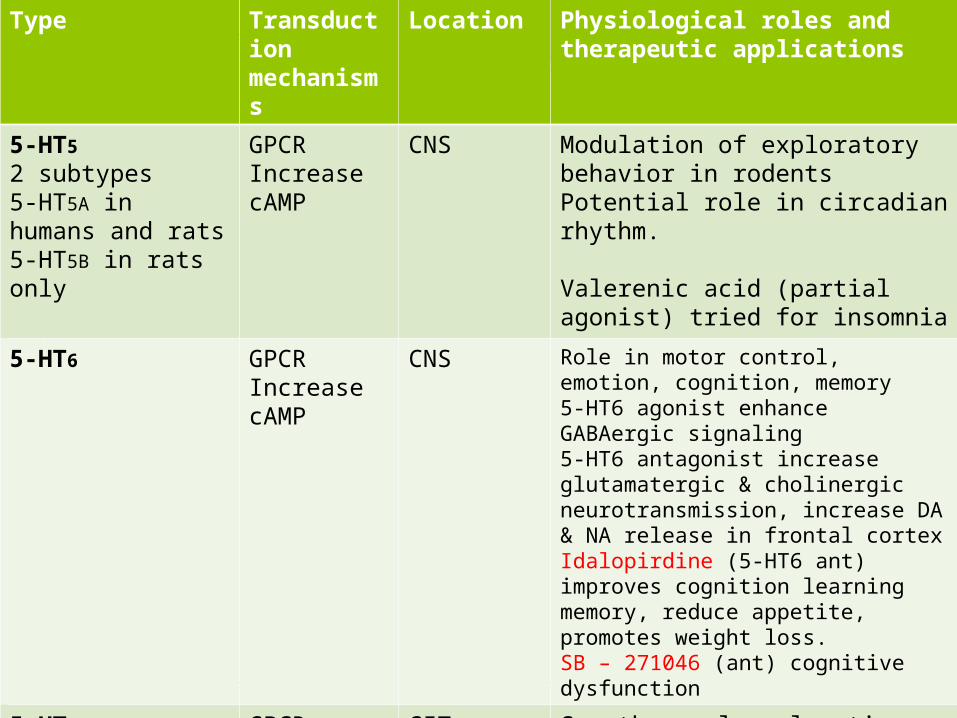
5-HT52 subtypes5-HT5A in humans and rats5-HT5B in rats only
GPCRIncrease cAMP
CNS Modulation of exploratory behavior in rodentsPotential role in circadian rhythm.
Valerenic acid (partial agonist) tried for insomnia
5-HT6 GPCRIncrease cAMP
CNS Role in motor control, emotion, cognition, memory5-HT6 agonist enhance GABAergic signaling5-HT6 antagonist increase glutamatergic & cholinergic neurotransmission, increase DA & NA release in frontal cortexIdalopirdine (5-HT6 ant) improves cognition learning memory, reduce appetite, promotes weight loss.SB – 271046 (ant) cognitive dysfunction
5-HT7 GPCRIncrease cAMP
GITBlood vesselsBrain
Smooth muscle relaxation5-HT7 ant – IBD Thermoregulation, circadian rhythm, learning, memory, sleep.
Migraine Various theories proposed Vascular theory by Wolff suggests initially humorally mediated
intracerebral vasoconstriction causing aura, followed by extracerebral vasodilation causing headache.
Neural hypothesis by Lauritzen “cortical spreading depression”
Inflammation hypothesis by Waeber & Moskowitz activation of trigeminal nerve terminals & release of inflammatory neuropeptides. (CGRP; telcagepant)
2 important factors that implicate 5-HT in its pathogenesis are - there is a sharp increase in the urinary excretion of the main 5-HT metabolite, 5-HIAA, during the attack. - Several drugs that modulate the serotonin system are effective in migraine.
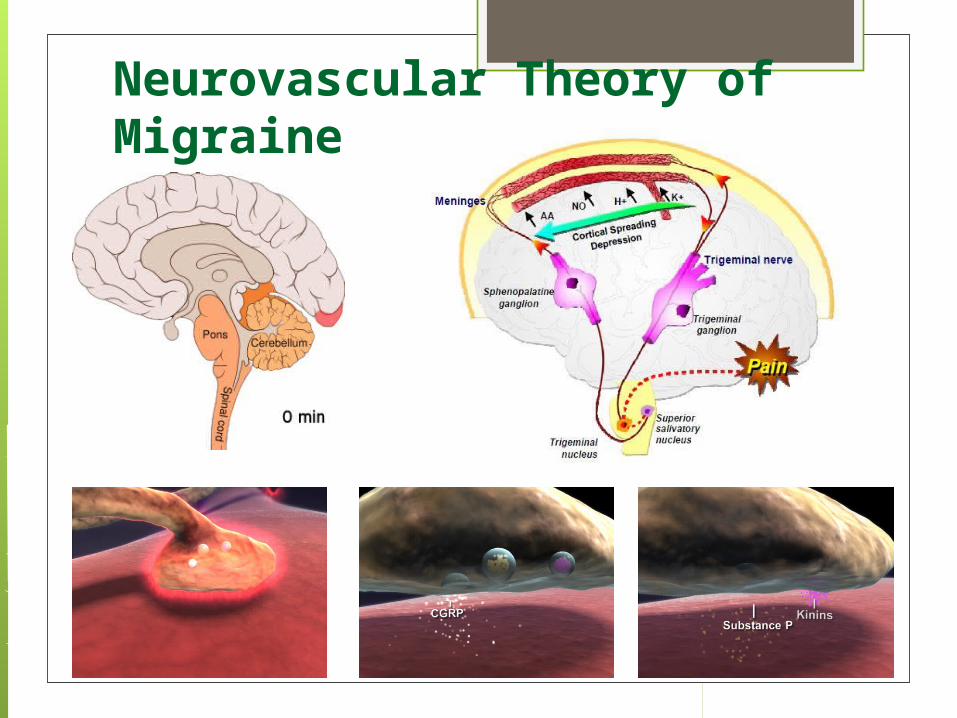
Neurovascular Theory of Migraine
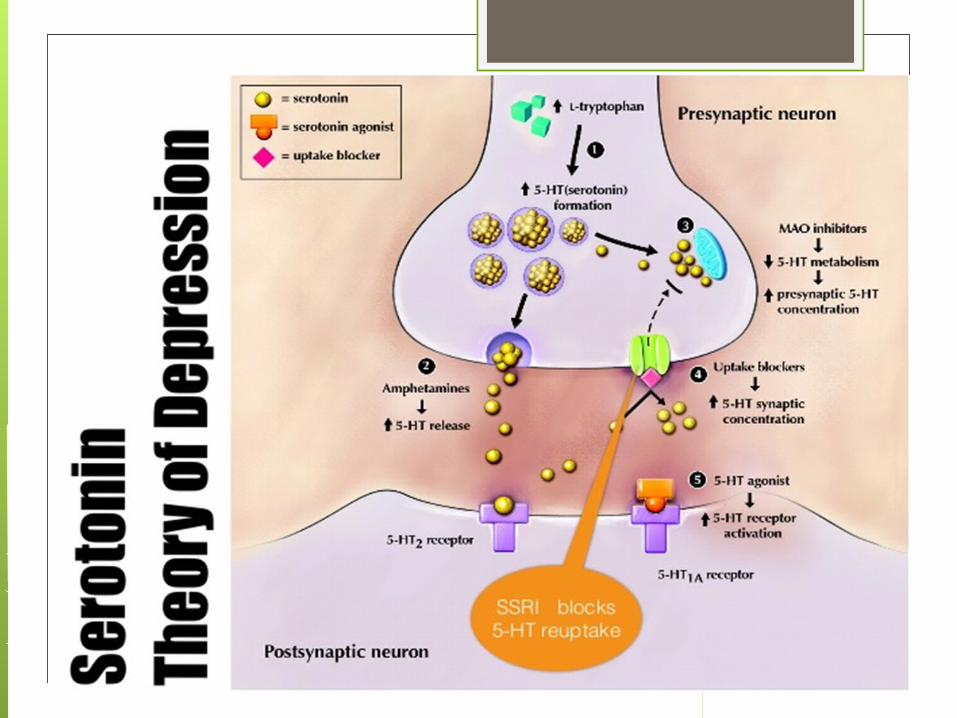
Depression Monoamine theory of depression which was first proposed in
1965 by Schildkraut suggests that depression results from deficient monoaminergic (5-HT or NA) transmission in the CNS.
Noradrenaline depletion may be due to inhibition of tyrosine hydroxylase, whereas reduced synthesis of serotonin may be due to depletion of dietary tryptophan or mutations of tryptophan hydroxylase
Based on the ability of known antidepressant drugs TCAs, SSRIs and MAO inhibitors to facilitate monoaminergic transmission.
Recent approaches show that depression may be associated with neurodegeneration and reduced neurogenesis in the hippocampus.
Stress & hypothalamic-pituitary-adrenal axis -The hypothalamic-pituitary-cortisol hypothesis
postulates that depression is associated with elevated cortisol levels in response to stress.
Other possible disease mechanisms - Reduced level GABA & dopamine - Melatonin dysfunction - Abnormal circadian rhythms - Neuronal loss and reduced neurogenesis
SSRIs Selectively block 5-HT reuptake by the neurons Include Citalopram, Fluoxetine, Paroxetine, Sertraline and
Fluvoxamine Increase synaptic 5-HT availability stimulates post-synaptic
neurons and contributes to mood elevating and anxiolytic properties
Other uses OCD, Panic disorder , social phobia , PTSD.
Other new drugs for depression Newer mixed 5-HT and noradrenaline reuptake inhibitors Venlafaxine Desvenlafaxine Duloxetine Milnacipran
5-HT2a receptor antagonist – Trazodone, Mianserin
Other Drugs affecting 5-HT system Precursors of serotonin- - s-adenyl-l-methionine, tryptophan Inhibit synthesis
p-chlorophenylalanine (irreversible) Inhibit neuronal re-uptake
SSRI (e.g. fluoxetine), TCA (e.g. imipramine) Inhibit storage-deplete:
Reserpine Inhibit metabolism:
MAO inhibitors Promote release:
p-chloroamphetamine (e.g. fenfluramine to ↓ appetite)
Serotonin syndrome Serotonin syndrome is a symptom complex of varying drug
interactions which may lead to excess serotonin in body. These are toxic and potentially fatal effects. Require a combination of serotonergic drugs such as SSRIs
with MAO inhibitors. Other drugs implicated are TCAs, meperidine, MDMA. Symptoms- mental status changes, confusion, agitation,
hypomania, myoclonus, hyperreflexia, diaphoresis, shivering, tremor, diarrhoea, incoordination, fever.
Treatment Remove suspected agent BZDs Propranolol
THANK YOU


























![VEDLEGG I PREPARATOMTALE · serotonin-norepinefrin-reopptakshemmere (SNRIs), samt med legemidler som forringer metabolismen av serotonin (inkludert monoaminoksidasehemmere [MAO-hemmere])](https://img.pdfslide.tips/doc/110x75/5e52a2565bd51d52a71b872b/vedlegg-i-preparatomtale-serotonin-norepinefrin-reopptakshemmere-snris-samt-med.jpg)