Embed Size (px)
Citation preview

La qualità del sonno e le alterazioni di quest’ultimo, nella realtà lavorativa, vengono spesso poste in secondo piano data la complessità degli interventi e la gravità dei
pazienti che occupano le terapie intensive.
Ma anche il sonno è importante.Ma anche il sonno è importante.E’ uno bei bisogni fondamentali per la salute degli esseri viventi.E’ uno bei bisogni fondamentali per la salute degli esseri viventi.
Sulla base di questionari (ove possibile) e/o di registrazioni di determinati parametri anche a seguito di stimolazione, sono stati portati a termine molti studi che hanno dimostrato che la causa primaria di disturbo sembra provenire dall’ambiente che circonda il degente: luci, allarmi dei dispositivi medici sono tra i tanti incriminati…
il rumore risulta esser la causa di disturbo più importante.il rumore risulta esser la causa di disturbo più importante.
Ma da chi è generato il rumore più intenso o prolungato o chi crea gli stimoli più frequenti nel paziente? Coloro che si trovano più frequentemente ad assisterlo:
gli infermieri
POSSIAMO FARE QUALCOSA?*

Perché dormiamo?
La funzione del sonno non è ancora del tutto chiarita.
E’ generalmente accettato che il sonno è necessario per mantenere un adeguato stato di salute, sia fisica che
psichica delle specie viventi.
Il bisogno di sonno aumenta durante gli stati patologiciMeccanismo Immunitario
Il sonno profondo è considerato un periodo di riparazione tissutale e di conservazione energetica.
“Scan Disk del SNC e funzioni di salvataggio su HD”

Effetti della OSPEDALIZZAZIONE sul SONNO
QUANTITATIVIcirca 2 ore TST/prime 48h in ICU
QUALITATIVIriduzione del sonno profondo N-REM (st. 3-4) + riduzione-assenza REM/prime 48h ICU
Ne possono derivareNe possono derivare
DISTURBI ENDOCRINIMelatinina Cortisolo
PSICOSI FUNZIONALI
DELIRIUM
AUMENTO DELLA MORTALITA’

Metodi di valutazione del SONNO
SOGGETTIVIQUESTIONARI
PAIN Assessment: Visual, Numeric, GraficRamsay
STRUMENTALIPOLISONNOGRAFIA
ACTIGRAFIA
OSSERVAZIONALICOMPORTAMENTO/BPS

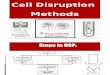
POLISONNOGRAFIA
Esempio di risveglio indotto da un rumore.La FRECCIA indica un improvviso aumento del rumore (68dB) dovuto ad un allarme, seguito da modificazioni EEG della Fase2 N-REM del sonno e della EOG dx e sx .
Jonathan Y. Gabor, Andrew B. Cooper, Shelley A. Crombach – University Of TORONTO: Contribution of the ICU environment to sleep disruption in meccanically ventilated pantient( American Journal Of Respiratory and Critical Care Medicine, 2003)


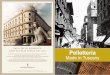
Rappresentazioni grafiche POLISONNOGRAFICHE di 5 differenti pazienti

ES. POLISONNOGRAFICO DI UN PAZIENTE SETTICO

Sleep in the ICU questionnaire
1. Rate the overall quality of your sleep at home 1 2 3 4 5 6 7 8 9 10
Use a scale of 1 to 10 (1 is poor; 10 is exellent)
2. Rate the overall quality of your sleep in the ICU 1 2 3 4 5 6 7 8 9 10 Use a scale of 1 to 10 (1 is poor; 10 is exellent)
3. Rate the overall quality of your sleep in the ICU on the following days (1 is no sleep; 10 is exellent)
a) On the first night in the ICU 1 2 3 4 5 6 7 8 9 10
b) During the middle of your ICU stay 1 2 3 4 5 6 7 8 9 10
c) At the end of your ICU stay 1 2 3 4 5 6 7 8 9 10
4. Rate the overall degree of the daytime sleeping during your ICU stay 1 2 3 4 5 6 7 8 9 10 (1 unable to stay awake; 10 fully alert and awake)
5. Rate the overall degree of the daytime sleeping during on the following days (1 is unable to stay awake; 10 is fully alert and awake)
a) On the first night in the ICU 1 2 3 4 5 6 7 8 9 10
b) During the middle of your ICU stay 1 2 3 4 5 6 7 8 9 10 c) At the end of your ICU stay 1 2 3 4 5 6 7 8 9
10
Neil S. Freedman, University. Of Pennsylvania: Patient perception of sleep quality and etiology of sleep disruption in ICU (American Journal Of Resp. And Critical care Medicine, 1999)

6. Rate how disruptive the following activities were to your sleep during ICU stay Use a scale of 1 to 10 (1 is no disruption; 10 is significant disruption)
Noise 1 2 3 4 5 6 7 8 9 10 Light 1 2 3 4 5 6 7 8 9 10 Nursing interventions (i.e. bath) 1 2 3 4 5 6 7 8 9 10 Diagnostic testing (i.e. chest x-rays) 1 2 3 4 5 6 7 8 9 10 Vital Signs 1 2 3 4 5 6 7 8 9 10 Blood samples 1 2 3 4 5 6 7 8 9 10 Administration of medications 1 2 3 4 5 6 7 8 9 10
7. Rate how disruptive the following noises were to your sleep during ICU stay (1 is no disruption; 10 is significant disruption)
Heart Monitor Alarm 1 2 3 4 5 6 7 8 9 10 Ventilator 1 2 3 4 5 6 7 8 9 10 Ventilator Alarm 1 2 3 4 5 6 7 8 9 10 I.V. Pumps Alarm 1 2 3 4 5 6 7 8 9 10 Suctioning 1 2 3 4 5 6 7 8 9 10 Talking 1 2 3 4 5 6 7 8 9 10 Nebulizer 1 2 3 4 5 6 7 8 9 10 Telephone 1 2 3 4 5 6 7 8 9 10 Beepers 1 2 3 4 5 6 7 8 9 10 TV 1 2 3 4 5 6 7 8 9 10
Neil S. Freedman, University. Of Pennsylvania: Patient perception of sleep quality and etiology of sleep disruption in ICU
(American Journal Of Resp. And Critical care Medicine, 1999)

SLEEP QUALITY: HOME Vs ICU
Neil S. Freedman, University. Of Pennsylvania: Patient perception of sleep quality and etiology of sleep disruption in ICU (American Journal Of Resp. And Critical care Medicine, 1999)

SLEEP DISRUPTION FROM THE ICU ENVIROMENT
Neil S. Freedman, University. Of Pennsylvania: Patient perception of sleep quality and etiology of sleep disruption in ICU (American Journal Of Resp. And Critical care Medicine, 1999)

SLEEP DISRUPTION BY SPECIFIC ENVIRONMENT NOISES
Neil S. Freedman, University. Of Pennsylvania: Patient perception of sleep quality and etiology of sleep disruption in ICU (American Journal Of Resp. And Critical care Medicine, 1999)

Open ICU Single Room
Mean (night) dB 5151 43
Mean (day) dB 56 44
Mean maximum (night) dB 6161 49
Mean maximum (day) dB 67 55
Mean (wakefulness) dB 55 48
Mean (sleep) dB 52 43
Sleep > 60 dB 5 0.02
Sleep > 70 dB 0.3 none
Jonathan Y. Gabor, Andrew B. Cooper, Shelley A. Crombach – University Of TORONTO: Contribution of the ICU environment to sleep disruption in meccanically ventilated pantient( American Journal Of Respiratory and Critical Care Medicine, 2003)
Il livello massimo di rumore espresso in dB, per consentire ad un soggetto sanoIl livello massimo di rumore espresso in dB, per consentire ad un soggetto sanodi attraversare tutte le fasi del sonno fino a quello paradosso è di 40dB.di attraversare tutte le fasi del sonno fino a quello paradosso è di 40dB.
Una normativa edilizia prevede una rilevazione max di 36dB tra una unità immobiliare e l’altra.Una normativa edilizia prevede una rilevazione max di 36dB tra una unità immobiliare e l’altra.
SOUND INTENSITY IN CARE UNIT LOCATIONS

Open ICU Single Room
Total Sleep Time, hr 6.5 9.5
Night Sleep, hr 3 6.4
Day Sleep, hr 3.5 3.1
Day Sleep, % 54 32
AROUSALS per hr 11 4.6
Jonathan Y. Gabor, Andrew B. Cooper, Shelley A. Crombach – University Of TORONTO: Contribution of the ICU environment to sleep disruption in meccanically ventilated pantient( American Journal Of Respiratory and Critical Care Medicine, 2003)
SLEEP ARCHITECTURE IN INTENSIVE CARE UNIT LOCATIONS

Open ICU Single Room
Sound-arousal from ICU activities 25 87
Sound-arousal from alarms 32 7
Sound-arousal from talking 42 6
IMPACT OF NOISE ON SLEEP DISRUPTION
Jonathan Y. Gabor, Andrew B. Cooper, Shelley A. Crombach – University Of TORONTO: Contribution of the ICU environment to sleep disruption in meccanically ventilated pantient( American Journal Of Respiratory and Critical Care Medicine, 2003)

POSSIAMO FARE QUALCOSA?*POSSIAMO FARE QUALCOSA?*
modelli incentrati sui bisogni della persona
modelli incentrati sui risultati
La pratica infermieristica, deve basarsi su un approccio scientifico per essere metodologicamente corretta. Adotta il procedimento del problem solving:
individuazione del problema la pianificazione
attuazione del piano la valutazione
ma anchema anche

MODI DI AGIRE
PROFESSIONALE e METODICORAZIONALIZZAZIONE degli INTERVENTIRAZIONALIZZAZIONE degli INTERVENTI
RISPETTO DEI CICLI SonnoVegliaRISPETTO DEI CICLI SonnoVegliaOSSERVAZIONE DEL PAZIENTEOSSERVAZIONE DEL PAZIENTE
PAIN & SLEEP AssessmentPAIN & SLEEP AssessmentPROMUOVERE il senso di sicurezzaPROMUOVERE il senso di sicurezza
ma ancheETICO
e
CONSAPEVOLEI TUOI BISOGNI SONO ANCHE I LORO

E’ compito dell’infermiere attuare una serie di interventi finalizzati a favorire un adeguato riposo mediante: una adeguata informazione, una idonea rassicurazione, mediante la disponibilità all’aiuto, sperimentando metodi alternativi ai farmaci che favoriscono il sonno (lettura, tisane). Altri interventi infermieristici saranno finalizzati a creare un ambiente rilassante ed una comoda posizione nel letto in modo da favorire positivamente questo bisogno fondamentale.L’assistenza infermieristica si impegna dunque, mediante un rapporto più umano, a trasformare l’immagine spesso fredda dell’ospedale in modo da farlo diventare un luogo di cura e di riposo.