PowerPoint Presentation
BRAIN VASCULAR ANATOMY ANATOMICAL VARIANT& VASCULAR
LESIONSDR SOUMITRA HALDERDEPT. OF RADIOLOGYMEDICAL
COLLEGE,KOLKATA
1
BRAIN VASCULAR LESIONS..
PART-2
AneurysmVascular malformations
Aneurysm
Abnormal bulge of an arterial wall .
Develops where the blood vessel wall is weakened. Aneurysm
ACQABNORMAL VASCULAR HEMODYNAMCICS AND SHEAR FORSE.,Genetetic
alterationAnomalous vsAcq.abnormal vascular hemodynamics.shearing
stress.5
2. Sizes of Aneurysm.1.
By size-
. Small aneurysm diameter females> 40 years: females >
males The sites different from gender: female supraclinoid segment
of the internal carotid artery. male anterior communicating complex
Age: rupture is most common between 40 and 60 years but can occur
in any age, even in old age.Lateralized in 30 percent of patients,
predominantly to the side of the aneurysm associated with a brief
loss of consciousness
9
IMAGING
An unenhanced CT scan is the preferred procedure for detection
of SAH is positive in more than 90% of patients in the first 24
hours .
The location of the SAH may frequently suggest the site of the
aneurysm
Rarely, the aneurysm itself might be visible.
CTA ..Sensitivity > 90%
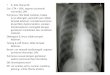
DSA is gold standart.Right MCA aneurysm with subarachnoid
hemorrhage.
12
Giant vertebral aneurysm in the vertebral artery tip with nausea
and vomiting due to brain stem compression.
14
Treatment
ObservationSurgical clipping Endovascular occlusion.
Watchful waiting with serial scan for asymptomatic >
SAH29
MR
T1W1 tightly packed mass or honeycomb of flow voidsT2W1
serpiginous honeycomb of flow voids adjacent high signal tissue
gliosisFLAIR- flow voids +/- surrounding high signalGRE - blooming
(Hagic residua)Left parital wedge shaped serpentine flow
voids.30
ANGIOGRAPHY
Internal angioarchitecture best depiction
Depicts 3 components of AVM
Enlarged arteries+/- aneurysmNidusEarly draining veins
Feeding arteries Dilated and tortuous Flow related angiopathy
dilatation , stenosis or thrombosisPedicle
aneurysm(10-15%cases)Nidus Tightly packed tangle of abnormal
arteries and veins with no intervening capillary bed/brain
parenchym Intranidal aneurysm(50% cases)Draining Veins Opacify in
mid-late arterial phase(Early draining vein) Enlarged , tortuous
and may form varices exerting local mass effectStenosis can cause
AVM Hage by intranidal pressure
33
TREATMENT
Surgical excision for nidusAcute and emergent surgical
intervention in life threatening ICH.
STEREOTACTIC RADIOSURGERY
Focussed irradiation to nidus Indication Unresectable because of
locationSize < 3.5cms Risk of hage till it disappears
completely
ENDOVASCULAR RX
Adjunct to Sx/ RadioSxUsed in small AVMs or 1-2 feeding
arteriesEmbolisation Precedes surgery /radiosx reduce size of
nidusComplete cure if : small AVM , few feeders , single draining
vein
1Complete obliteration of nidus for cure.2 STEREOTACTIC
RADIOSURGERYFocussed irradiation to nidusIndication Unresectable
because of locationSize < 3.5cmsAdv : Non invasiveDisadv :Effect
takes yearsRisk of hage till it disappears completely
34
DURAL AV FISTULATiny crack like vessels that shunt blood b/w
meningeal arteries and small venules within dural sinus wall.
ETIOLOGY : Acquired angiogenesis within dural sinus wall after
thrombosis
Local hypoeperfusion in thrombosed dural venous sinus increased
intrasinsu pressure
thrombosed transverse sinus with multiple tiny arteriovenous in
the dural wall(thickarrow) . Lesion is mostly supplied
bytransosseous feeders(curved arrow) from the external carotid
artery.35
DURAL AV FISTULA
LOCATION: Trans Sinus>Sig sinus>Cav sinus(adults) Sup
Saggital sinus (Children)SIZE : Tiny single vessel shunts to
massive complex lesions with multiple feedersNUMBER : Multiple
lesions are uncommon.
Malignant dAVF aggressive clinical course with Hage and
NDMultiple dAVF poor clinical prognosis
36
CLINICAL FEATURE
Mostly in adults(40-60yrs)
C/F varies with location and drainage patternTS-SigS - Bruit and
tinnitusCav S Pulsatile proptosis , chemsois , retroorbital
pain
Lesions with cortical venous drainage(Malignant dAVF) :
seizures, dementia ,FND
40-60 yr. 20 y older than avmFND focal neurological
deficitsPROGNOSIS98% w/o cortical venous drainage - benign
courseTREATMENTConservative Observation +/- carotid compression
techniqueIf rsk of HageEndovascular Embolisation of arterial
feeders with particulate or liquid agents , coil embolization of
venous sinus Surgical resection of involved dural venous
sinusStereotactic RadioSx- 2-3 years for obliteration
37
CT
CTA source ,right-sided tinnitus shows no obvious abnormality,
although the right sigmoid sinus looks peculiar. 7-11B.Bone CT in
the same patient shows multiple enlarged transosseous vascular
channels
Ct.Normal to strikingEnlarged dural sinus or draining
vein/transosseous venous channelsCECT Enlarged feeding arteries and
draining veins Dural sinus may be thrombosed or stenotic
38
MRI
Contrast-enhanced MRA dural sinus thrombosis , multiple
enhancing vascular channels 7-11D. MRA innumerable tiny feeding
arteries(bold arrow) supplying a dAVF at the transverse-sigmoid
sinus junction. The sinushas partially recanalized , and the distal
sigmoid sinus and jugular bulb are partially opacified.(curved
arrow)
Dilated cortical vein without nidus adjacent to normal appearing
brain MC finding thrombosed dural venous sinus with flow voids
39
ANGIOGRAPHY
Best imaging toolDSA with superselective catheterization of
dural and transosseous feeders requiredPresence of dural sinus
thrombosis, flow reversal with drainage into cortical veins and
engorged tortuous pial veins
Dural branches arise from ECA , ICA and vertebral arteries
40
ECA
DSA of the external carotid artery in a patient with tinnitus,
dAVF in the occluded transverse sinus(bold arrow) supplied by the
middle meningeal artery (curved arrow), transosseous
branches(straight) from the ECA.ANGIOGRAPHYHigh flow venopathy can
cause stenosis . Occlusion or hemorrhageDysplastic venous pouches
may cause HageIncreased Hage with cortical venous drainage and
dysplastic venous dilatation
41
TREATMENT
Conservative Observation
Endovascular Embolisation of arterial feeders with particulate
or liquid agents , coil embolization of venous sinus .
Surgical resection of involved dural venous sinus
Stereotactic RadioSx- 2-3 years for obliteration
+/- carotid compression techniqueIf rsk of Hage
42
CAROTID CAVERNOUS FISTULAAV shunting developing within cavernous
sinus
The right cavernous sinus is enlarged by numerous dilated
arterial and venouschannels.43
ETIOLOGY
Almost always acquired
DirectTraumatic: central skull base #Non-Traumatic: Preexisting
cavernous ICA aneurysm
IndirectDegenerative sequelae of dural sinus thrombosis
Skull base# - stretch injury of ica /puncture from bony
segmentDirectHigh FlowRupture of cavernous ICAIndirectSlow flow ,
low pressureFistula b/w dural br of ICA and the CS
44
Dilated CS (Direct) Enlarged crack like vessels(Indirect)
GROSS PATHOLOGY
CLINICAL FEATURES
DIRECTINDIRECTEPIDEMIOLOGYLess commonMore
commonDEMOGRAPHICSM=FAny ageWomen40-60yrsPRESENTATIONBruitPulsatile
xophthalmosOrbital edemavisionGlaucomaPainless proptosis Vision
changes
CTMild or striking proptosisProminent CSEnlarged SOV Enlarged
ExOcMs
CECT The right cavernous sinus is enlarged , and the ipsilateral
superior ophthalmic vein is more than 4 times the size of the left
superior ophthalmic vein .
47
MRI
T2WI enlarged right cavernous sinus containing numerous abnormal
flow voidsT1 Bulging SOV and CS with flow voidsT2 Asymmetric flow
related signal loss in the affected veins48
ANGIOGRAPHY
DIRECT CCFRapid flow with early opacification of CSFistula may
be noted in ICA segment
INDIRECT CCFMultiple dural feeders from Cavernous br of ICA and
deep br of ECAAnastomoses b/w ICA and ECA feeders are common
Narrowed ICA before terminating in a large venous pouch.Venous
reflux into SOV and IOV is present.Direct CCF. LAT DSA in post
trauma with multiple skull base fracture.Treatment..balloon
embolization.50
VEIN OF GALEN ANEURYSMAL MALFORMATIONDirect AV fistula b/w deep
choroidal arteries and persistent embryonic precursor of VOG
Large midline venous pouch behind the 3rd ventricle
Enlarged choroidal veins(staright arrow) draining directly to
dilated MPV (median procencephalic vn)and to torcu via falcine
culcus.Torcular heterophili(venous sinus confluence) enlarged.
Primary malformation in development of vein of Galen-AV shunts
involving embryologic venous precursors (median vein of
prosencephalon)-Choroidal arteriovenous fistula with no
nidus-Absence of normal vein of Galen-Median vein of prosencephalon
does not drain normal brain tissue-Manifests as high-output
congestive heart failure (CHF) in infants and hydrocephalus in
older children
51
EtiologyIn normal fetal dvpt : arterial supply of choroid plexus
drains via single transient midline vein median prosencephalic vein
.
Internal cerebral vein drains fetal chorid plexus as MPV
regresses
Persistent high flow fistula prevents regression
Absence of normal vein of Galen
Median vein of prosencephalon does not drain normal brain
tissue
Manifests as high-output congestive heart failure (CHF) in
infants and hydrocephalus in older children
Primary malformation in development of vein of Galen-AV shunts
involving embryologic venous precursors (median vein of
prosencephalon)-Choroidal arteriovenous fistula with no
nidus-Absence of normal vein of Galen-Median vein of prosencephalon
does not drain normal brain tissue-Manifests as high-output
congestive heart failure (CHF) in infants and hydrocephalus in
older children
52
CLINICAL FEATURES
>30% of symptomatic VoGM in childrenRare in adultsNeonates
high output CCF with cranial bruitOlder infants macrocrania +
hydrocephalus +/- CCFOlder Children Developmental delay and
seizuresYoung adults - Headache
Large VGAMS cerebral ischemia and dystrophic changesLeft
untreated Die of progressive brain damage andintracatable CCF
53
CTNECTEnlarged well delineated hyperdense mass at tentorial
apexObstructive hydrocephalusHage and calcification may be
present.
CECT Strong uniform enhancement
CECT scan massive VGAM(bold) draining into an enlarged falcine
sinus (staright), causing obstructive hydrocephalus.54
MRI
Sagittal T2WI shows prominent arteries supplying an enlarged
median prosencephalic vein . Note enlarged falcine sinus(curved )
.Enlarged serpentine arterial feeders adjacent to the lesion
55
DSA in the same patient shows that the VGAM(bold arrow) is
supplied by multiple direct arterial fistulas .2 forms based on
angioarchitectureChoroidal Multiple br from pericallosal choroidal
and thalamoperforate arteries drain into dilated midline venous
sacMural single or few enlarged collicular or post choridal
arteries drain into sinus wallVenous drainage into persistent
embryonic FALCINE SINUS
56
ULTRASOUNDAntenatallyHypoechoic to mild echogenic midline mass
behind the third ventricle Bidirectional turbulent flow
Neonatal transcranial US shows a large VGAM posterior to the 3rd
ventricle. Prominent vessels with arterial flow(staright) supply
the lesion.57
CVMS WITHOUT AV SHUNTING
DEVELOPMENTAL VENOUS ANOMALYUmbrella shaped CVM with mature
venous part.No arterial componentMay represent anatomic variant of
otherwise normal venous drainage
enlarged medullary veins(BOLD) draining into a single
transmantle collector vein .Also called VENOUS ANGIOMA/VENOUS
MALFORMATION
DVA is an abnormal vein that provides functional venous drainage
to normal brain .The presice etiology is unknown.Some investigator
depict that it is due to arressted medullary vein devoploment
between 8-11 wks.-
59
CLINICAL FEATURES
DVA is a DO NOT Touch lesion
Usually asymptomaticHeadache/seizuresHage with FND ( if a/w
cavernous malformation)MC vascular malformation at autopsy
Venous angiomas per se do not hemorrhage but are associated with
cavernous malformation (30%) which do bleed-DVA is a DO NOT Touch
lesion, if resected, the patient will suffer a debilitating venous
infarct, the DVA must be preserved if an adjacent cavernous
malformation is resectedLEAVE ME ALONE60
IMAGINGLocation : MC near the frontal horn of ventricle. (Deep
WM)Size < 3cmUsually solitary
2ND MC4TH VENTRICLE.61
CTNECTNormal .enlarged draining vein may appear hyperdense
CECT
CECT , CTA classic DVA in left cerebellar hemisphere .
COLLECTOR VEINCECTNumerous linear or punctate enhancing foci and
converge on single enlarged tubular draining vein
63
MRT1 Normal if DVA is small Hage if mixed malformationsT1 C+ -
stellate collection of linear enhancement structures joining
subependymal collector vein.GRE if H;age in coexisting cavernous
malformation - Occasionally hypo Not Hage but deoxyHb within venous
bloodclassic DVA with enlarged WM veins(bold) and a collector vein
draining into the anterior aspect of the superior
sagittalsinus.
64
MRA- MRV- DSANormal arterial and capillary phaseVenous phase
Medusa head appearance
CAVERNOUS MALFORMATIONIntralesional hemorrhages into thin walled
angiogenically immature blood filled locules called CAVERNS
Acquired /Inherited
Subacute(curved) , classic popcorn ball appearances of CCMs.
Microhemorrhages are seen as multifocal blooming black dots .
CAVERNOUS ANGIOMA/CAVERNOMa
Dilated endothelial cell-lined spaces with no normal brain
within lesion-Usually detectable because cavernous malformation
contains blood degradation products of different stages
ACQUIRED BY POST RADIATION THERAPY.
66
Gross patholgyDark blue well circumscribed lobulated lesion with
raspberry /POPCORN like configCCMs do not contain brain
parenchymaHemosiderin depositionMicro Hg
BLOOD FILLED COLLECTION67
CLINICAL FEATURES
2/3 are solitary Peak presentn : 40-60yrsMC presentn :
Seizures(50%) Headache FNDHage risk More if DVACan occur anywhere
in CNS.
3RD mc(AFTER DVA,CAPPILARY HEMANGIOMA)Can occur anywhere in
CNS.FROM TINY TO GIANT Can occupy whole lobe.Small hemorrhages
(usually not associated with large hemorrhages)
TREATMENT OPTIONS
Total surgical removal via microsurgical resexn for symptomatic
lesions with recurrent HageStereotactic Radiosx = for inaccessible
lesions
68
CT
IMAGINGCT Norma if small.In large lesion Hyperdense lesion with
scatteres intralesional calcification at post limb of int
capsule
69
T2WI shows classic popcorn ball appearance with locules of blood
in different stages of evolution surrounded by hemosiderin rim
MRIMR DIAGNOSTICFocal central heterogeneity(varying hemorrhage
within caverns)- POPCORN appearance on T2WI Circumferential
hypointense ring of hemosiderin form around high intense central
areas
T2 : Popcorn lesion : bright lobulated center with black
(hemosiderin) rim-Subacute hemorrhage and degraded blood products
within the lesion produce a halo of signal hyperintensity around
the lesion on T1-weighted images, a useful finding for
differentiating cavernous malformations from hemorrhagic tumors and
other intracranial hemorrhages-Always obtain susceptibility
sequences to detect coexistent smaller lesions
70
Cavernoma in the [post central gyrus.
Axial T2 shows a large left parietal mass that resembles a
popcorn ball with a hypointense hemosiderin rim (arrows) and
loculated hyperintense compartments(b) Axial T1 at the same level
shows multiple high signal intensity compartments in the lesion ,
findings suggestive of subacute hemorrhage , a faint halo of high
signal intensity also is visible around the lesion (arrowheads)
T2 & T2* gradient echo show multiple cavernomas , notice the
popcorn appearance with peripheral rim of hemosiderin on the T2 ,
the lesions are almost completely black on the gradient echo due to
blooming artefacts , T2* and susceptibility weighted imaging (SWI)
markedly increase the sensitivity of MRI to detect small cavernomas
, the five black dots in the left cerebral hemisphere on the T2*
are also cavernomas and are not visible on the T2WI
71
Based on imaging72
ANGIOGRAPHY
No identifiable feeding arteries/veinsNegative unless mixed with
other lesions
CAPILLARY TELANGIECTASIACAPILLARY ANGIOMACollection of enlarged
thin walled vessels resembling capillaries.Vessels surrounded by
normal brain parenchymaProbably congenital lesionsMC sites : Pons ,
cerebellum(can occur anywhere)
Graphic depicts pontine capillary telangiectasia with tiny
dilated capillaries interspersed with normal brain
Cranial irradiation cause vascular damage thar induce
devolpoment of talengiectasia.76
CLINICAL FEATURES
Peak Presentation : 30-40 yearsUsually silent, discovered
incidentally at imaging
A few cases vertigo,headache,tinnitus77
IMAGING
CT Usually Normal
MRT1W1 usually normalT2 50% normal -50 % show stippled foci of
hyperintensityT1+C BRUSH LIKE
T2* - Best sequence for demonstrating the lesion(poorly
delineated greyish hypointensity)FLAIRGRE
Usually