Embed Size (px)
Citation preview
XXXIII°°°°Congresso Nazionale della Società Italiana di Cardiologi a InvasivaPorto Antico di Genova, Centro Cogressi
3 ottobre 2012
Treatment of iatrogenic artery pseudoaneurysm
by ultrasound guided fibrin glue injection: a single
center experience
Francesca Faresin a; Francesca Franz a; Marco Zennaro b;
Enrico Favaretto b; Luigi Pedon b; Salvatore Ronsivalle a
aDivision of Vascular Surgery, bDivision of Cardiology,
Cittadella Hospital, Padua, Italy
Disclosure statement
The authors have nothing to disclose with regard to the conduction of this study.
Background
A pseudoaneurysm (PSA) is a contained rupture; disr uption in all 3 layers of the arterial wall.
Postcatheterization PSA is one of the most common va scular complication of cardiac and peripheral angiographic procedures.
Incidence of PSA: - after diagnostic catheterization: 0.05 – 2 %;- after coronary and peripheral intervention: 2.0 – 6 .0 %.
Causes: 1) after catheterization2) at the site of native artery and synthetic graft anastomosis (i.e. aortofemoral bypass graft)3) trauma4) infection (eg. Mycotic PSA)
Webber G et al. Circulation 2007
Background
Factors associated with PSA formation are: obesity; hypertension; peripheral arterial disease; CKD requiring hemodialysis; age ( >65 years); simultaneous artery and vein catheterization; large sheath size (> 8F); complex interventions; low or high puncture sites; poor pos tprocedural compression; antiplatelet and anticoagulation therapy;
Treatment:- Surgical management (vascular anastomosis; spontan eously occuringPSA; compression on underlying structures wich caus es claudication,neuropathy o critical ischemia)- Ultrasound-guided compression (USGC);- Ultrasound-guided thrombin injection (USGTI);- Other techniques (FemStop devices; coil insertion; fibrin adhesives; balloon occlusion)
Webber G et al. Circulation 2007
Objective
We sought to evaluate the safety and efficacy of th e treatment of
iatrogenic pseudoaneurysms by ultrasound guided fib rin glue
injection (USFGI) in the PSA chamber.
Methods
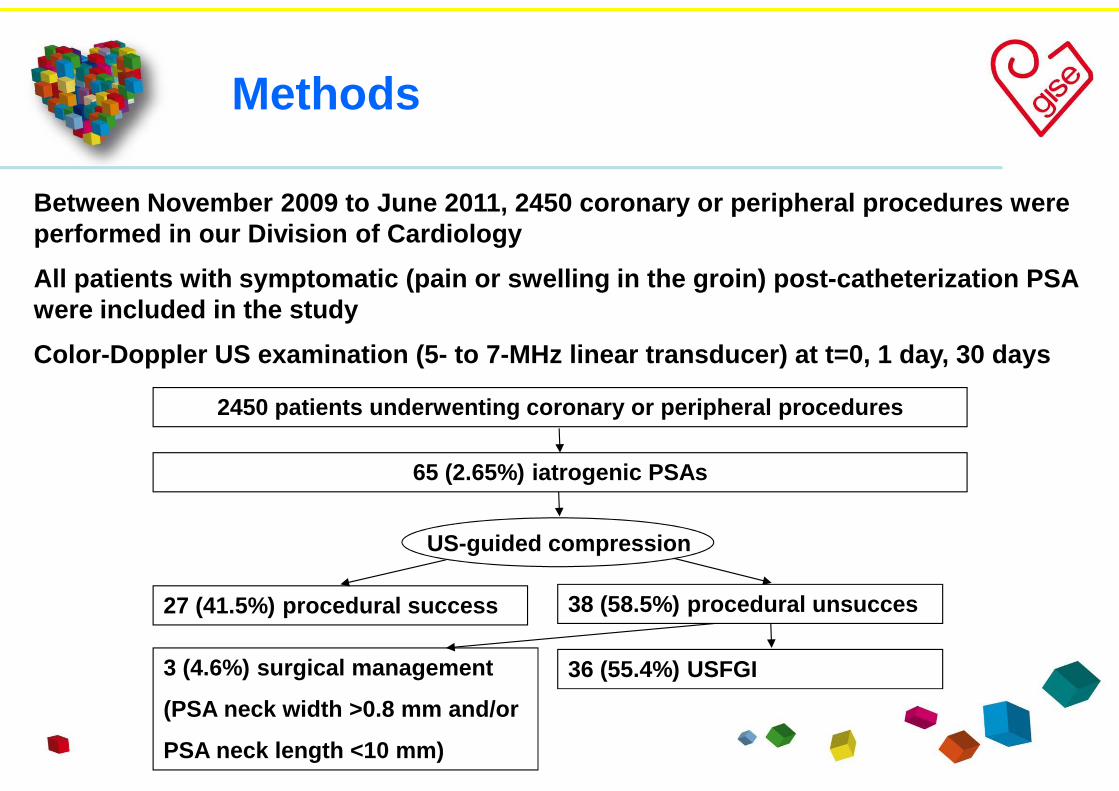
Between November 2009 to June 2011, 2450 coronary o r peripheral procedures were performed in our Division of Cardiology
All patients with symptomatic (pain or swelling in the groin) post-catheterization PSA were included in the study
Color-Doppler US examination (5- to 7-MHz linear tran sducer) at t=0, 1 day, 30 days
2450 patients underwenting coronary or peripheral p rocedures
US-guided compression
38 (58.5%) procedural unsucces27 (41.5%) procedural success
65 (2.65%) iatrogenic PSAs
3 (4.6%) surgical management
(PSA neck width >0.8 mm and/or
PSA neck length <10 mm)
36 (55.4%) USFGI
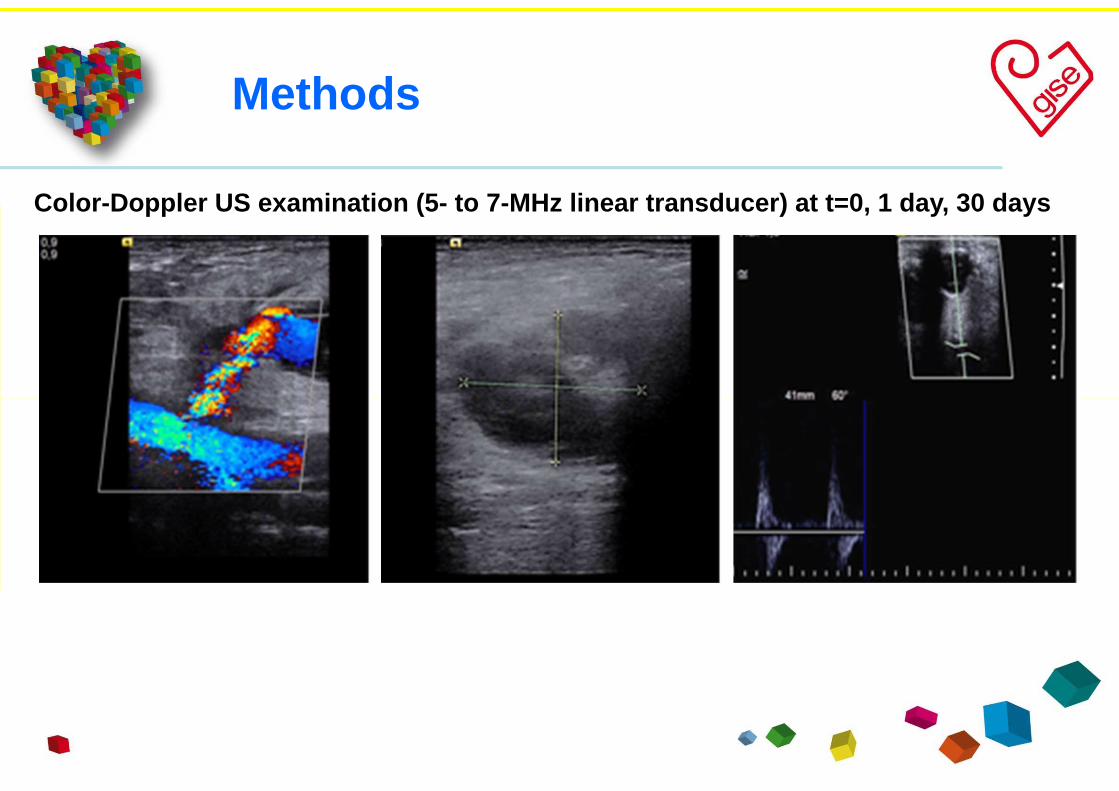
Methods
Color-Doppler US examination (5- to 7-MHz linear tran sducer) at t=0, 1 day, 30 days
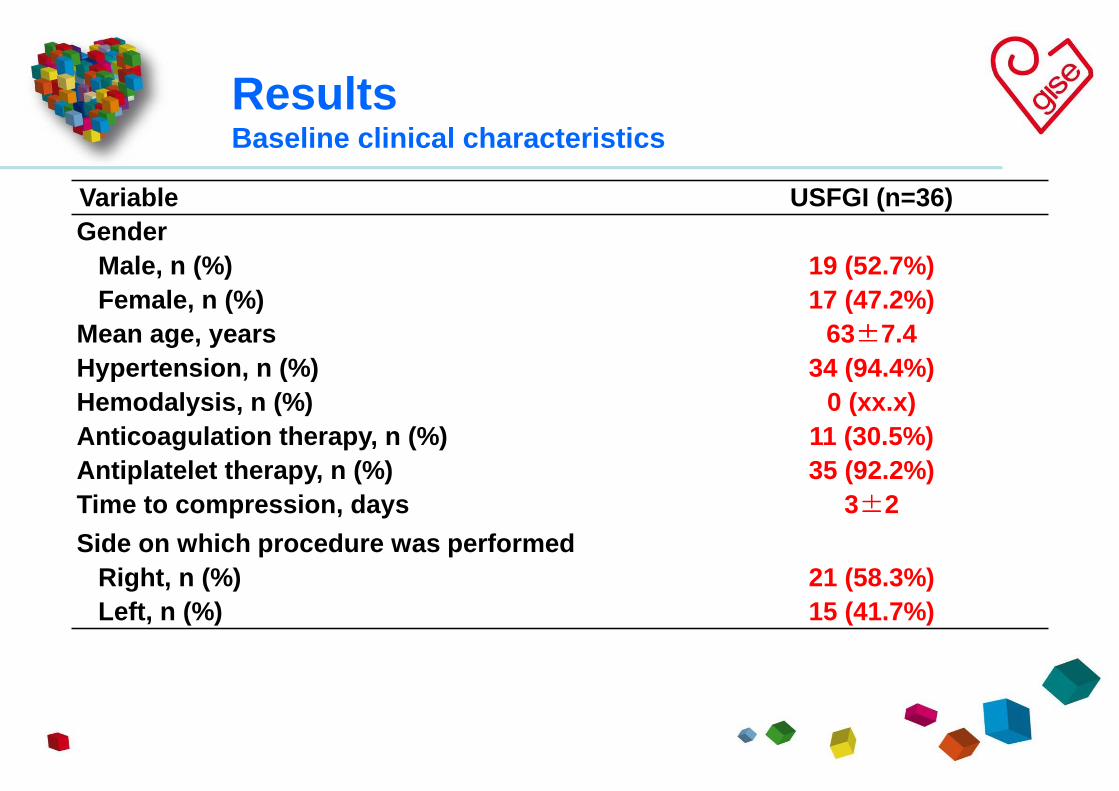
ResultsBaseline clinical characteristics
Variable USFGI (n=36)Gender
Male, n (%) 19 (52.7%)Female, n (%) 17 (47.2%)
Mean age, years 63±±±±7.4Hypertension, n (%) 34 (94.4%)Hemodalysis, n (%) 0 (xx.x)Anticoagulation therapy, n (%) 11 (30.5%)Antiplatelet therapy, n (%) 35 (92.2%)Time to compression, days 3±±±±2
Side on which procedure was performedRight, n (%) 21 (58.3%)Left, n (%) 15 (41.7%)
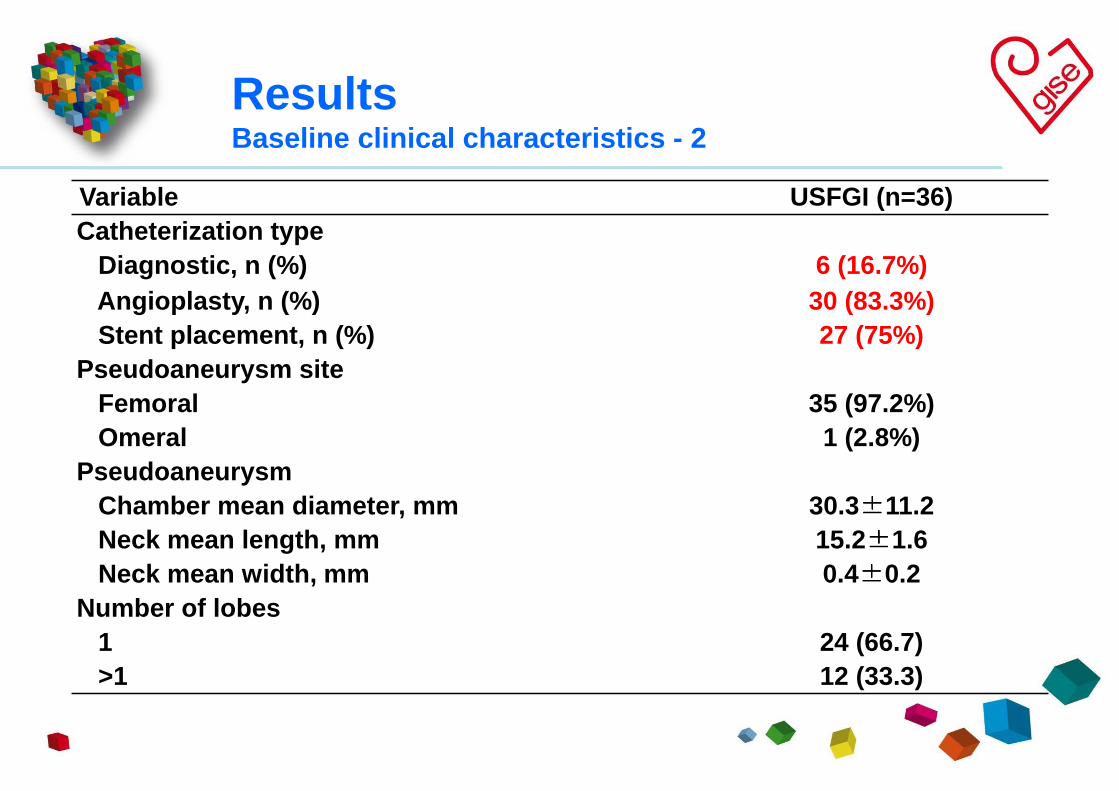
ResultsBaseline clinical characteristics - 2
Variable USFGI (n=36)Catheterization type
Diagnostic, n (%) 6 (16.7%)Angioplasty, n (%) 30 (83.3%)Stent placement, n (%) 27 (75%)
Pseudoaneurysm siteFemoral 35 (97.2%)Omeral 1 (2.8%)
PseudoaneurysmChamber mean diameter, mm 30.3 ±±±±11.2Neck mean length, mm 15.2±±±±1.6Neck mean width, mm 0.4±±±±0.2
Number of lobes1 24 (66.7)>1 12 (33.3)
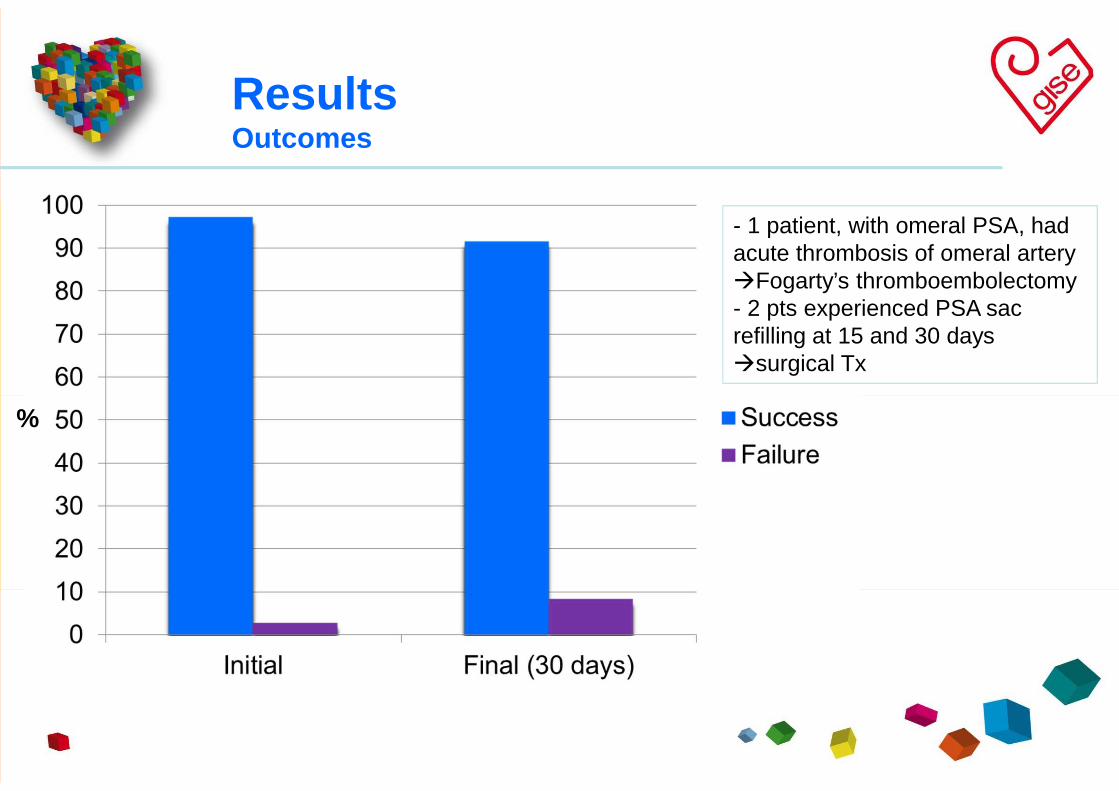
ResultsOutcomes
%
- 1 patient, with omeral PSA, had acute thrombosis of omeral artery �Fogarty’s thromboembolectomy- 2 pts experienced PSA sac refilling at 15 and 30 days �surgical Tx
Conclusions
Our results suggest that the treatment of iatrogeni c PSA by USGFI seems safe and effective, after an accurate pre-operative echo color Doppler ultrasound evaluation
PSAs with short and wide necks seem to be at higher risk of downstream embolization
Further, larger studies are needed to refine indica tions, limitations and complication of this technique
[email protected] you for your attention



















![06-06-17: A696-04: [4] T.84.4-86.5: NCIS Iatrogenic AIDS Docs & AIDS Corr](https://img.pdfslide.tips/doc/110x75/568c553c1a28ab4916c1f800/06-06-17-a696-04-4-t844-865-ncis-iatrogenic-aids-docs-aids-corr.jpg)








