Embed Size (px)
Citation preview
Health Informatics & eHealth: Application of ICT for Health
PHID 682 Integration and Innovation of Public HealthMahidol University Faculty of Public Health
November 7, 2014
Nawanan Theera-Ampornpunt, M.D., Ph.D.Department of Community Medicine
Faculty of Medicine Ramathibodi HospitalSlideShare.net/Nawanan
2
Outline
• Health & Health Information• Health IT & eHealth• Health Informatics as a Discipline• Thailand’s eHealth Situation• Current Forces

3
Health & Health Information

4
Let’s take a look at these pictures...

5Image Source: Guardian.co.uk
Manufacturing
6Image Source: http://www.oknation.net/blog/phuketpost/2013/10/19/entry-3
Banking
7ER - Image Source: nj.com
Healthcare (on TV)
8
(At an undisclosed nearby hospital)
Healthcare (Reality)
9
• Life-or-Death• Difficult to automate human decisions
– Nature of business– Many & varied stakeholders– Evolving standards of care
• Fragmented, poorly-coordinated systems• Large, ever-growing & changing body of
knowledge• High volume, low resources, little time
Why Healthcare Isn’t Like Any Others
10
Back to something simple...
11
To treat & to care for their patients to their best abilities, given limited time & resources
Image Source: http://en.wikipedia.org/wiki/File:Newborn_Examination_1967.jpg (Nevit Dilmen)
What Clinicians Want?
12
• Safe• Timely• Effective• Patient-Centered• Efficient• Equitable
Institute of Medicine, Committee on Quality of Health Care in America. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy
Press; 2001. 337 p.
High Quality Care

13
Information is Everywhere in Healthcare
14
“Information” in Medicine
Shortliffe EH. Biomedical informatics in the education of physicians. JAMA. 2010 Sep 15;304(11):1227-8.
15
15
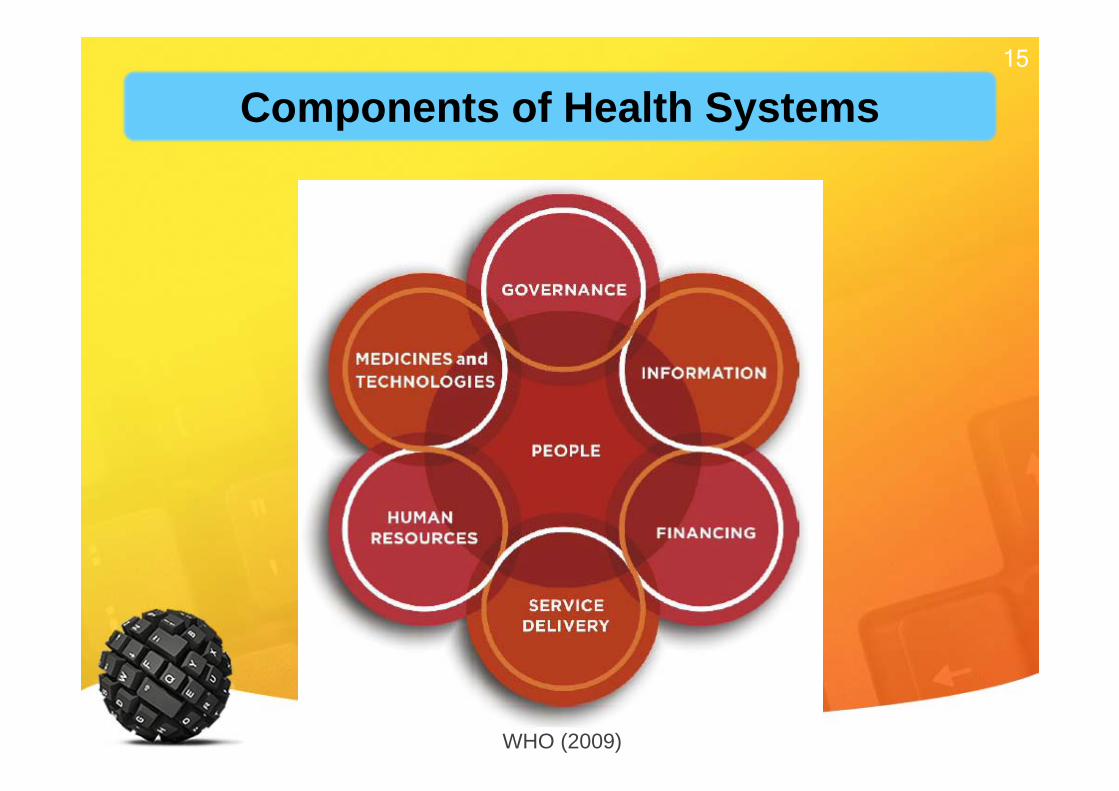
WHO (2009)
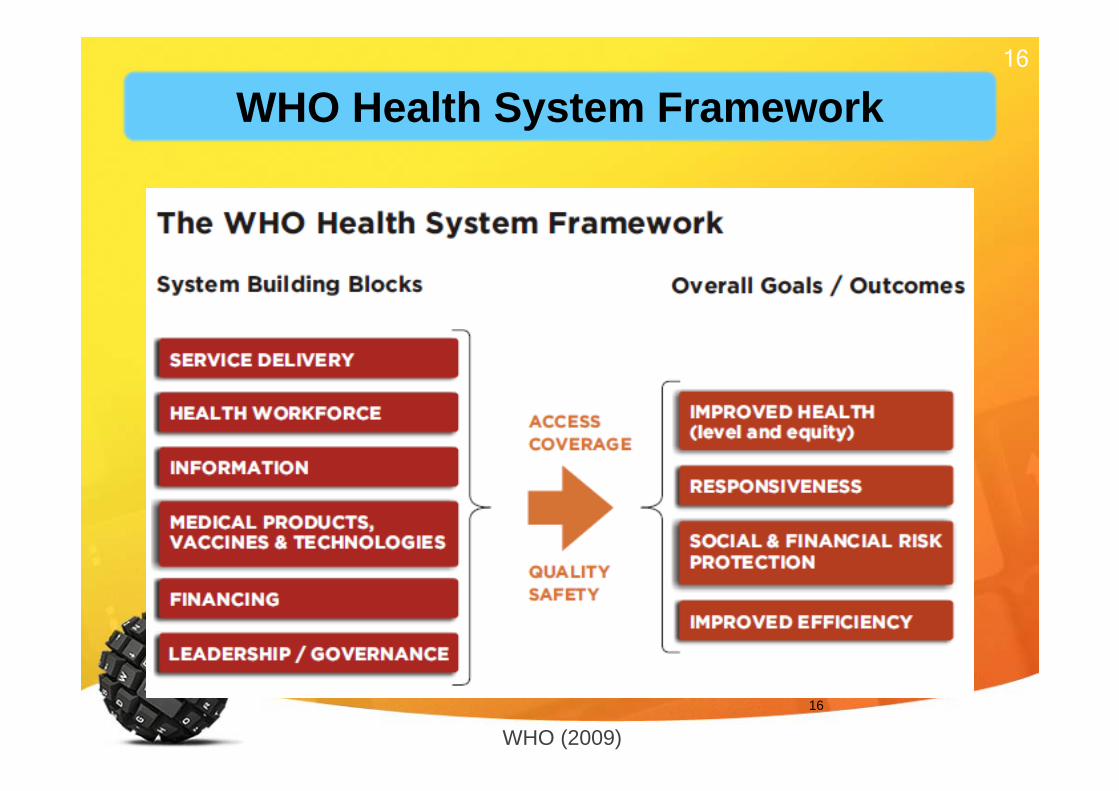
Components of Health Systems
16
16
WHO (2009)
WHO Health System Framework

17
Outline
Health & Health Information• Health IT & eHealth• Health Informatics as a Discipline• Thailand’s eHealth Situation• Current Forces

18
Health IT & eHealth
19
(IOM, 2001)(IOM, 2000) (IOM, 2011)
Landmark IOM Reports
20
• To Err is Human (IOM, 2000) reported that: – 44,000 to 98,000 people die in U.S.
hospitals each year as a result of preventable medical mistakes
– Mistakes cost U.S. hospitals $17 billion to $29 billion yearly
– Individual errors are not the main problem– Faulty systems, processes, and other
conditions lead to preventable errorsHealth IT Workforce Curriculum Version 3.0/Spring 2012 Introduction to Healthcare and Public Health in the US: Regulating Healthcare - Lecture d
Patient Safety
21
• Humans are not perfect and are bound to make errors
• Highlight problems in U.S. health care system that systematically contributes to medical errors and poor quality
• Recommends reform• Health IT plays a role in improving patient
safety
IOM Reports Summary
22Image Source: (Left) http://docwhisperer.wordpress.com/2007/05/31/sleepy-heads/ (Right) http://graphics8.nytimes.com/images/2008/12/05/health/chen_600.jpg
To Err is Human 1: Attention
23Image Source: Suthan Srisangkaew, Department of Pathology, Facutly of Medicine Ramathibodi Hospital
To Err is Human 2: Memory
24
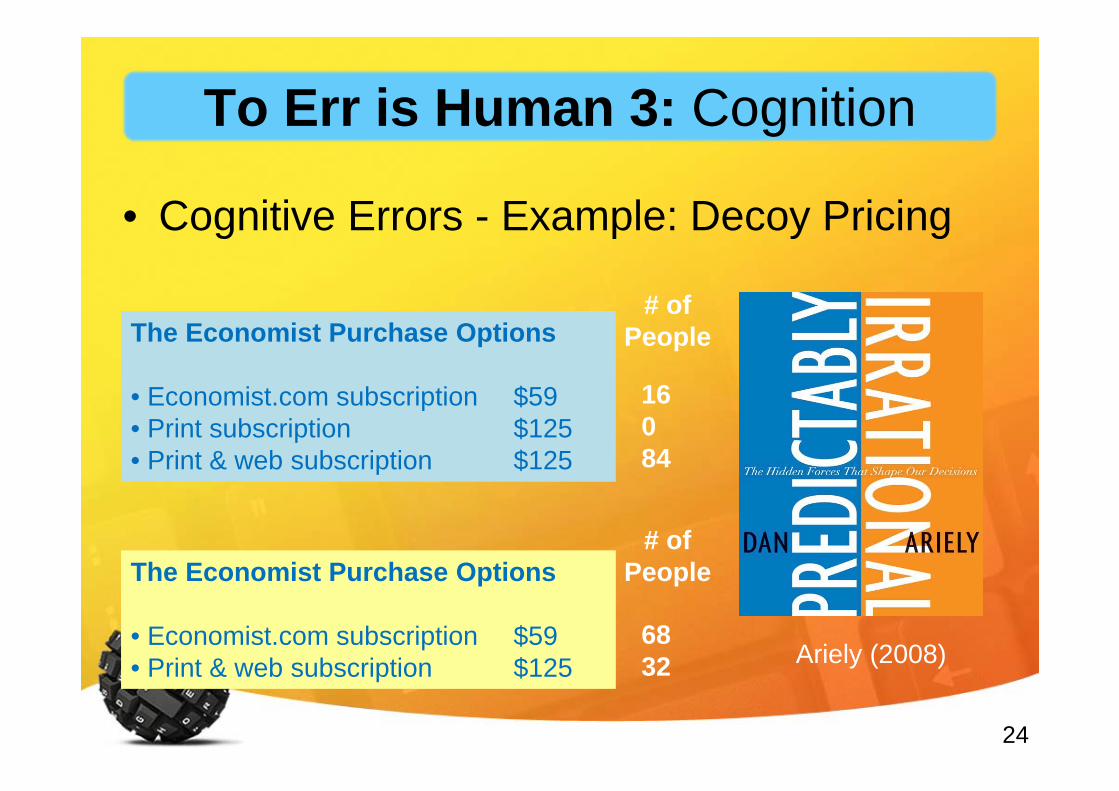
• Cognitive Errors - Example: Decoy Pricing
The Economist Purchase Options
• Economist.com subscription $59• Print subscription $125• Print & web subscription $125
Ariely (2008)
16084
The Economist Purchase Options
• Economist.com subscription $59• Print & web subscription $125
6832
# of People
# of People
To Err is Human 3: Cognition
25
• It already happens....(Mamede et al., 2010; Croskerry, 2003; Klein, 2005; Croskerry, 2013)
What If This Happens in Healthcare?
26
Mamede S, van Gog T, van den Berge K, Rikers RM, van Saase JL, van Guldener C, Schmidt HG. Effect of availability bias and reflective reasoning on diagnostic accuracy
among internal medicine residents. JAMA. 2010 Sep 15;304(11):1198-203.
Cognitive Biases in Healthcare
27
Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them. Acad Med. 2003 Aug;78(8):775-80.
Cognitive Biases in Healthcare
28Klein JG. Five pitfalls in decisions about diagnosis and prescribing. BMJ. 2005 Apr
2;330(7494):781-3.
“Everyone makes mistakes. But our reliance on cognitive processes prone to bias makes treatment errors more likely
than we think”
Cognitive Biases in Healthcare
29
• Medication Errors
– Drug Allergies
– Drug Interactions
• Ineffective or inappropriate treatment
• Redundant orders
• Failure to follow clinical practice guidelines
Common Errors
30
Why We Need ICT in Healthcare?
#1: Because information is everywhere in healthcare

31
Why We Need ICT in Healthcare?
#2: Because healthcare is error-prone and technology
can help

32
Why We Need ICT in Healthcare?
#3: Because access to high-quality patient
information improves care

33
Why We Need ICT in Healthcare?
#4: Because healthcare at all levels is fragmented &
in need of process improvement
34
Use of information and communications technology (ICT) in health & healthcare
settings
Source: The Health Resources and Services Administration, Department of Health and Human Service, USA
Slide adapted from: Dr. Boonchai Kijsanayotin
Health IT
35
Use of information and communications technology (ICT) for health; Including
• Treating patients• Conducting research• Educating the health workforce• Tracking diseases• Monitoring public health.
Sources: 1) WHO Global Observatory of eHealth (GOe) (www.who.int/goe)2) World Health Assembly, 2005. Resolution WHA58.28
Slide adapted from: Mark Landry, WHO WPRO & Dr. Boonchai Kijsanayotin
eHealth
36
eHealth Health IT
Slide adapted from: Dr. Boonchai Kijsanayotin
eHealth & Health IT
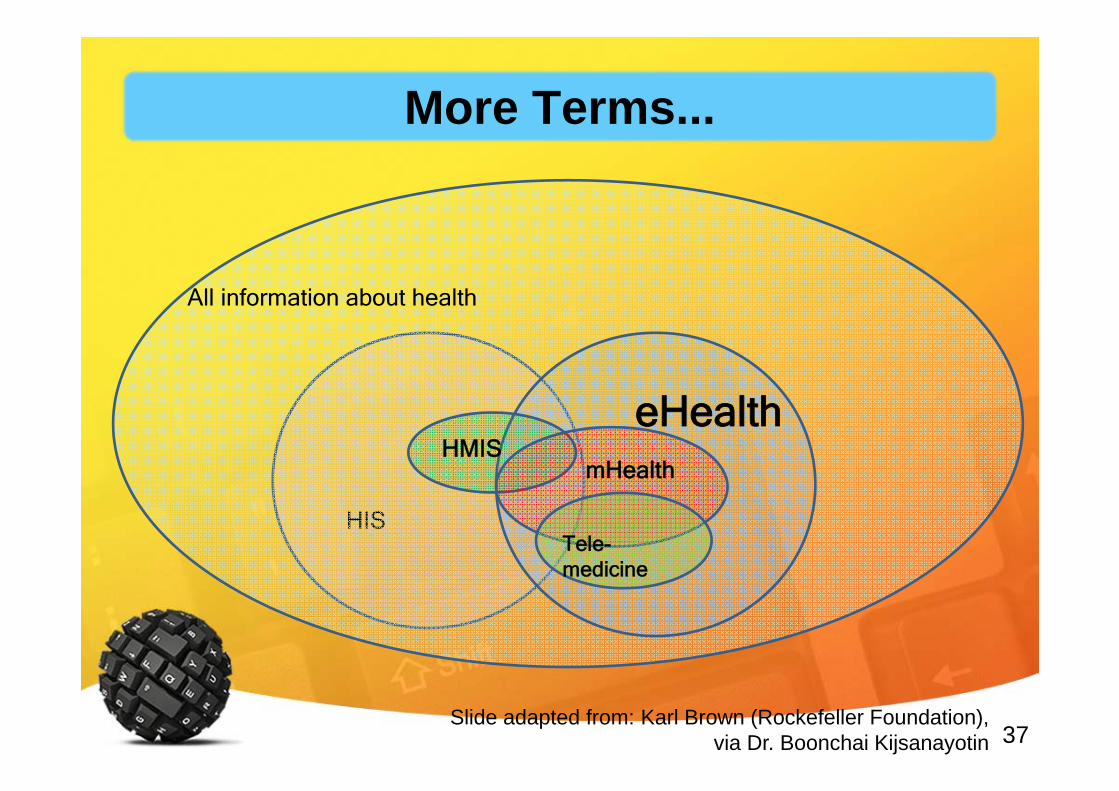
37
HIS
All information about health
eHealthHMIS
mHealth
Tele-medicine
Slide adapted from: Karl Brown (Rockefeller Foundation), via Dr. Boonchai Kijsanayotin
More Terms...
38
Health InformationTechnology
Goal
Value-Add
Tools
Health IT: What’s in a Word?
39
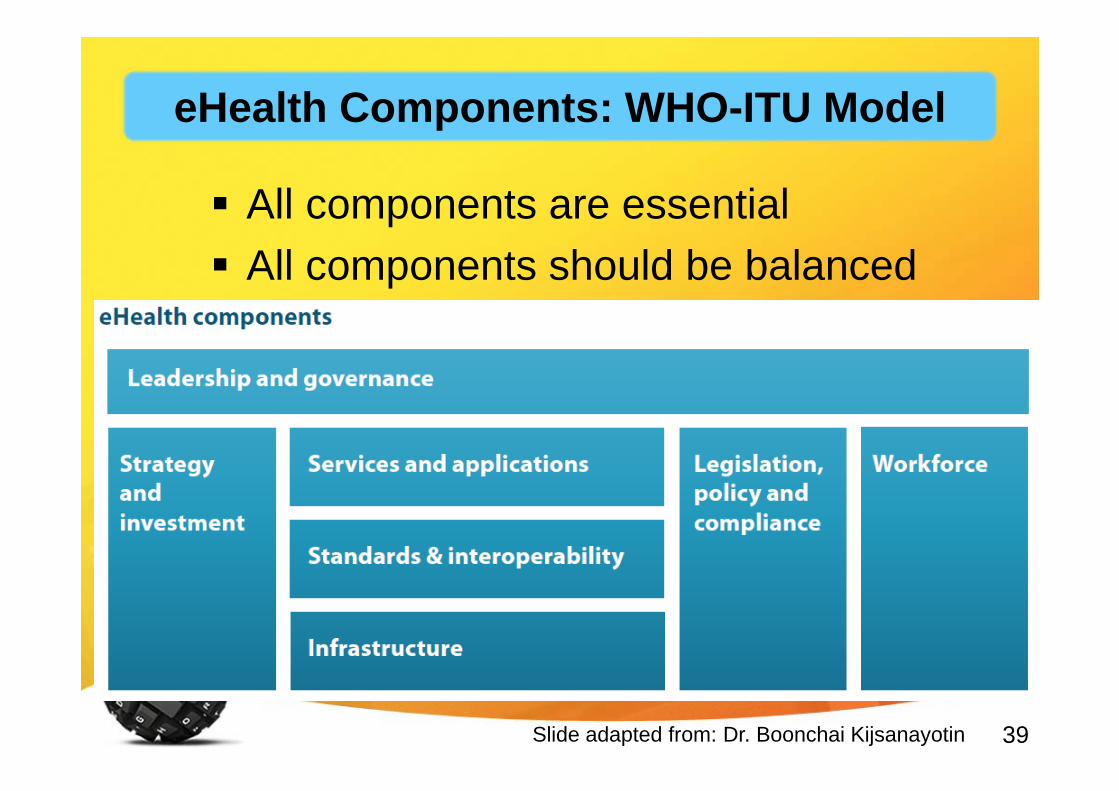
All components are essential All components should be balanced
Slide adapted from: Dr. Boonchai Kijsanayotin
eHealth Components: WHO-ITU Model
40
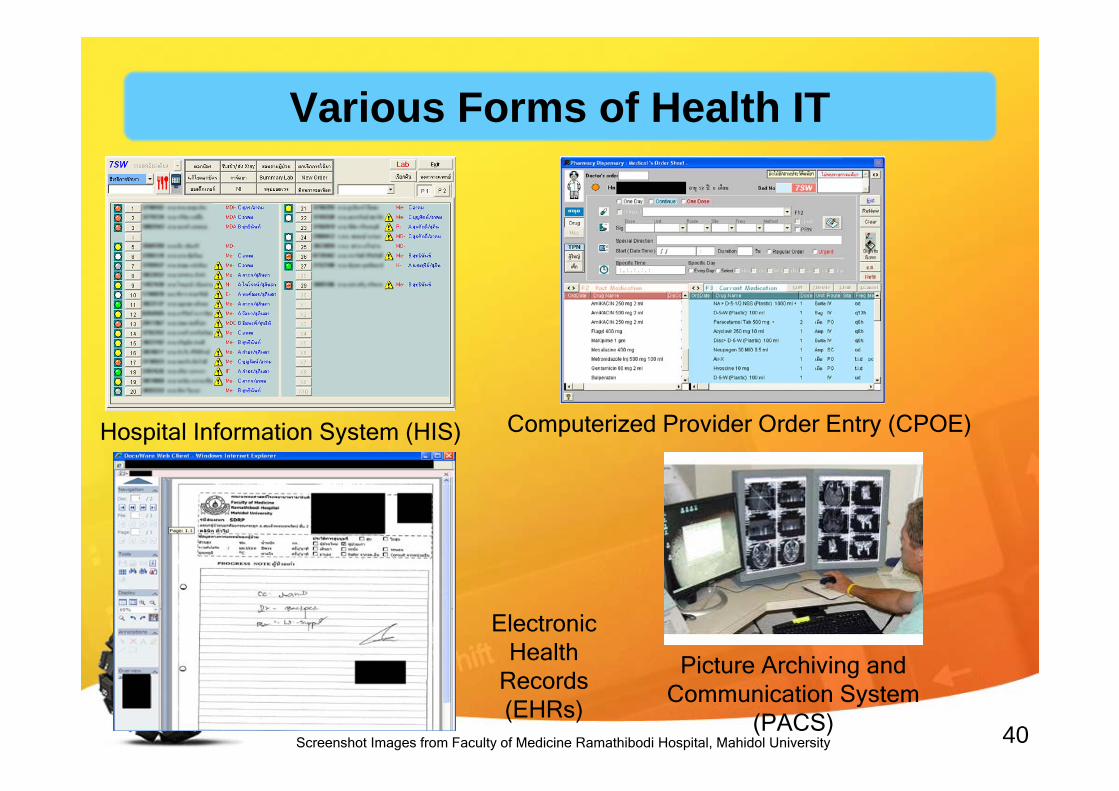
Hospital Information System (HIS) Computerized Provider Order Entry (CPOE)
Electronic Health
Records (EHRs)
Picture Archiving and Communication System
(PACS)Screenshot Images from Faculty of Medicine Ramathibodi Hospital, Mahidol University
Various Forms of Health IT
41
mHealth
Biosurveillance
Telemedicine & Telehealth
Images from Apple Inc., Geekzone.co.nz, Google, HealthVault.com and American Telecare, Inc.
Personal Health Records (PHRs) and Patient Portals
Still Many Other Forms of Health IT
42
• Guideline adherence• Better documentation• Practitioner decision making or
process of care• Medication safety• Patient surveillance & monitoring• Patient education/reminder
Documented Values of Health IT

43
• Master Patient Index (MPI)• Admit-Discharge-Transfer (ADT)• Electronic Health Records (EHRs)• Computerized Physician Order Entry (CPOE)• Clinical Decision Support Systems (CDS)• Picture Archiving and Communication System
(PACS)• Nursing applications• Enterprise Resource Planning (ERP)
Some Hospital IT - Enterprise-wide
44
• Pharmacy applications
• Laboratory Information System (LIS)
• Radiology Information System (RIS)
• Specialized applications (ER, OR, LR, Anesthesia, Critical Care, Dietary Services, Blood Bank)
• Incident management & reporting system
Some Hospital IT - Departmental Systems
45
The Challenge - Knowing What It Means
Electronic Medical Records (EMRs)
Computer-Based Patient Records
(CPRs)
Electronic Patient Records (EPRs)
Electronic Health Records (EHRs)
Personal Health Records (PHRs)
Hospital Information System
(HIS)
Clinical Information System (CIS)
EHRs & HIS
46
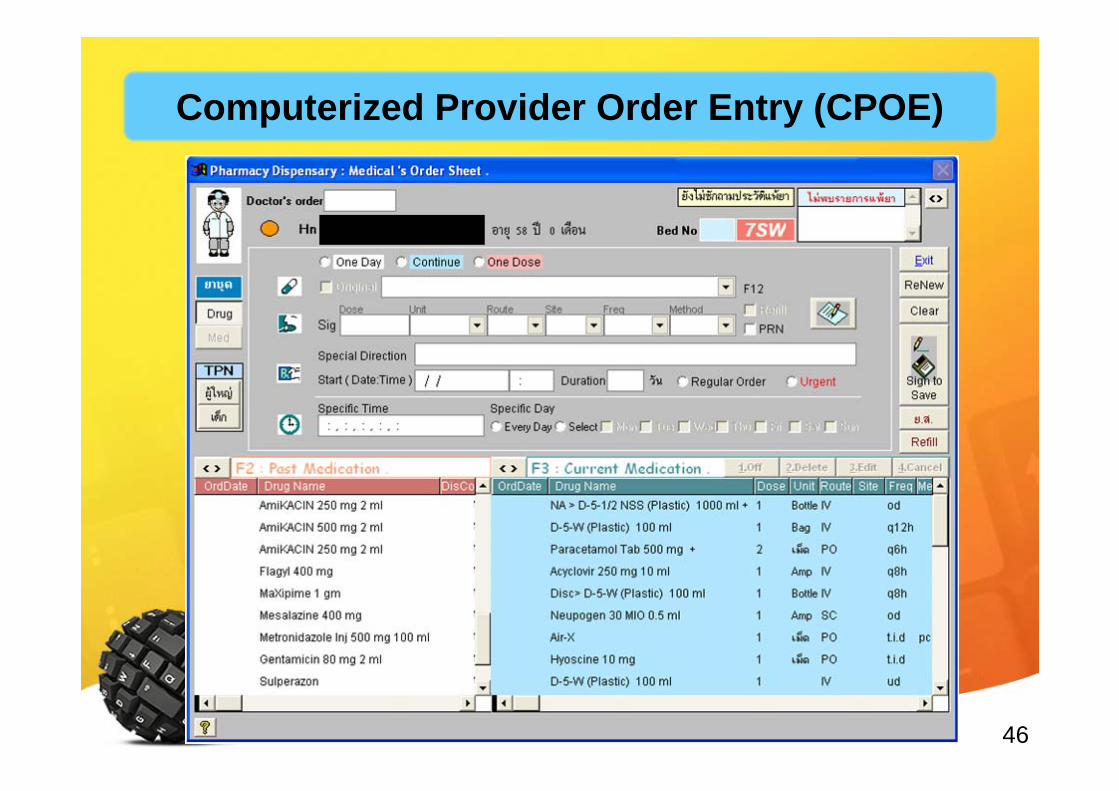
Computerized Provider Order Entry (CPOE)
47
Values
• No handwriting!!!• Structured data entry: Completeness, clarity,
fewer mistakes (?)• No transcription errors!• Streamlines workflow, increases efficiency
Computerized Provider Order Entry (CPOE)
48
• The real place where most of the values of health IT can be achieved
– Expert systems• Based on artificial intelligence,
machine learning, rules, or statistics
• Examples: differential diagnoses, treatment options
(Shortliffe, 1976)
Clinical Decision Support Systems (CDS)
49
– Alerts & reminders• Based on specified logical conditions• Examples:
– Drug-allergy checks– Drug-drug interaction checks– Reminders for preventive services– Clinical practice guideline integration
Clinical Decision Support Systems (CDS)
50
Examples of “Reminders”
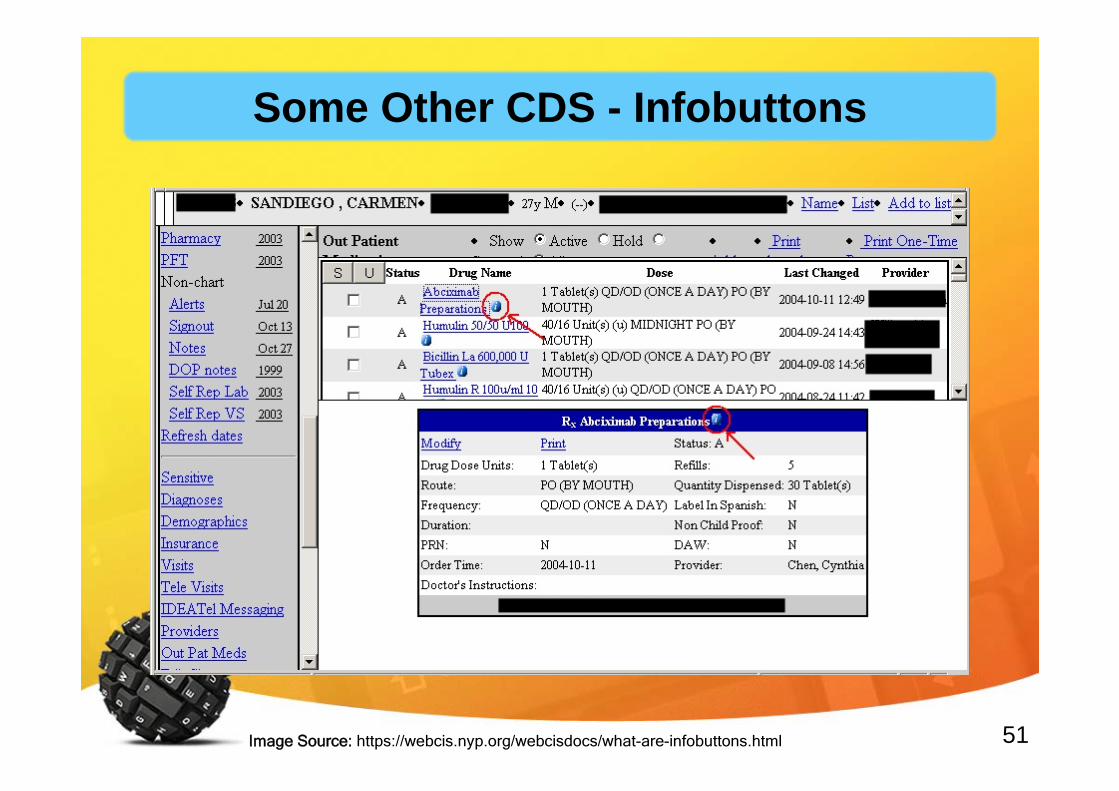
51Image Source: https://webcis.nyp.org/webcisdocs/what-are-infobuttons.html
Some Other CDS - Infobuttons
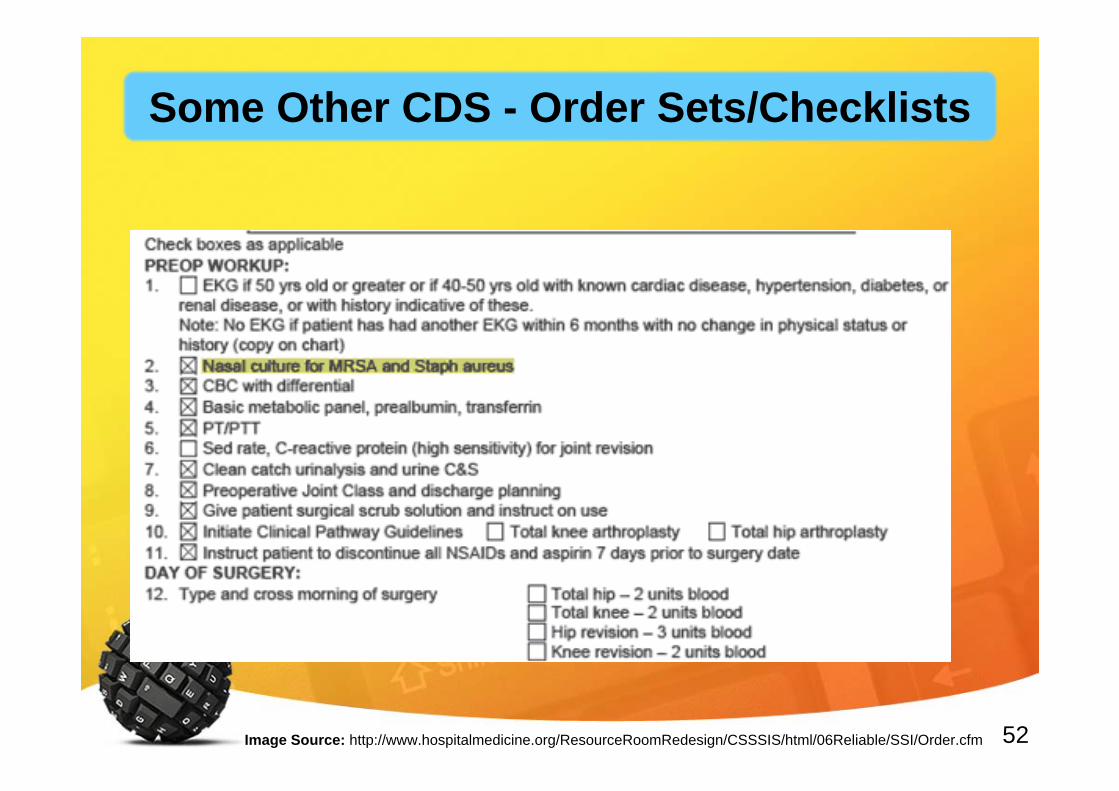
52Image Source: http://www.hospitalmedicine.org/ResourceRoomRedesign/CSSSIS/html/06Reliable/SSI/Order.cfm
Some Other CDS - Order Sets/Checklists
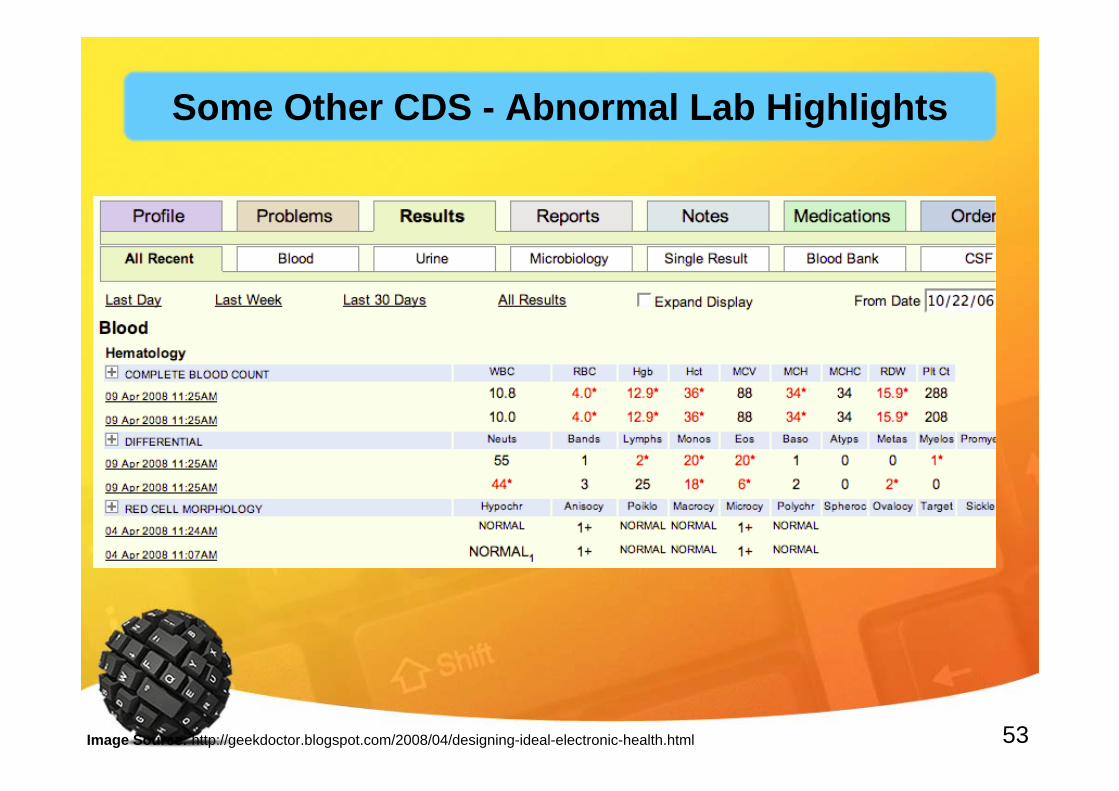
53Image Source: http://geekdoctor.blogspot.com/2008/04/designing-ideal-electronic-health.html
Some Other CDS - Abnormal Lab Highlights
54
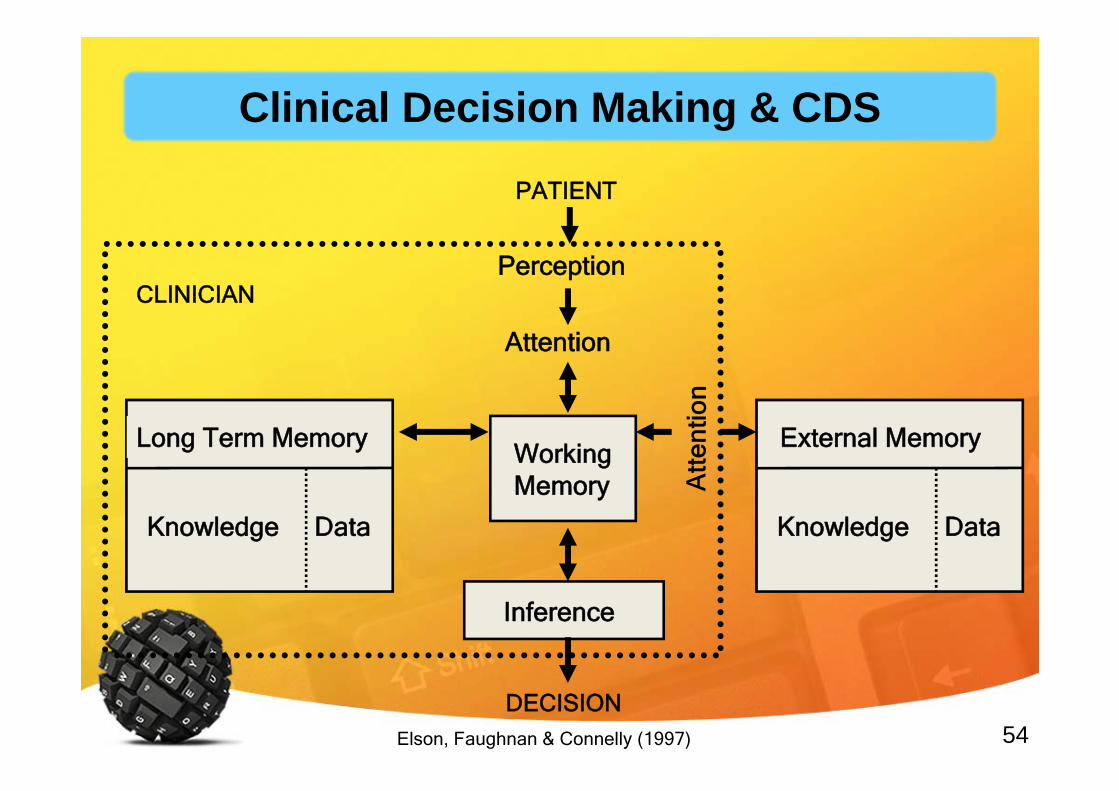
External Memory
Knowledge Data
Long Term Memory
Knowledge Data
Inference
DECISION
PATIENT
Perception
Attention
WorkingMemory
CLINICIAN
Elson, Faughnan & Connelly (1997)
Clinical Decision Making & CDS

55Image Source: socialmediab2b.com
IBM’s Watson

56Image Source: englishmoviez.com
Rise of the Machines
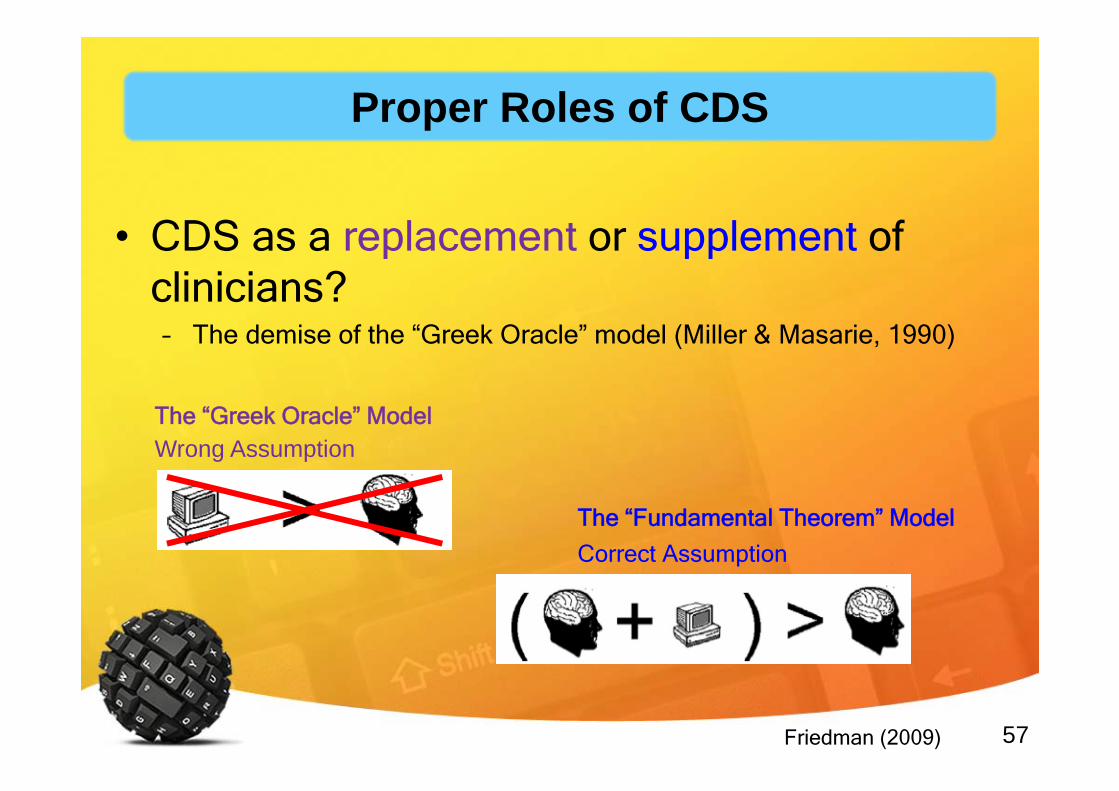
57
• CDS as a replacement or supplement of clinicians?– The demise of the “Greek Oracle” model (Miller & Masarie, 1990)
The “Greek Oracle” Model
The “Fundamental Theorem” Model
Friedman (2009)
Wrong Assumption
Correct Assumption
Proper Roles of CDS
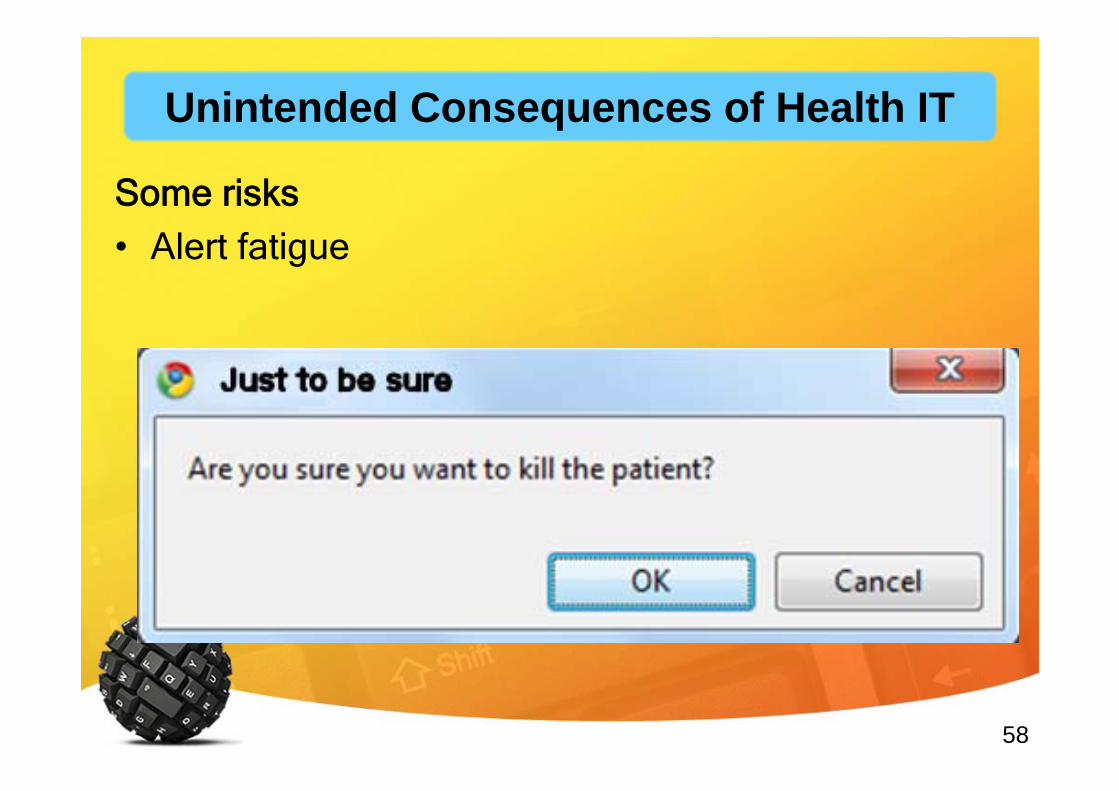
58
Some risks• Alert fatigue
Unintended Consequences of Health IT
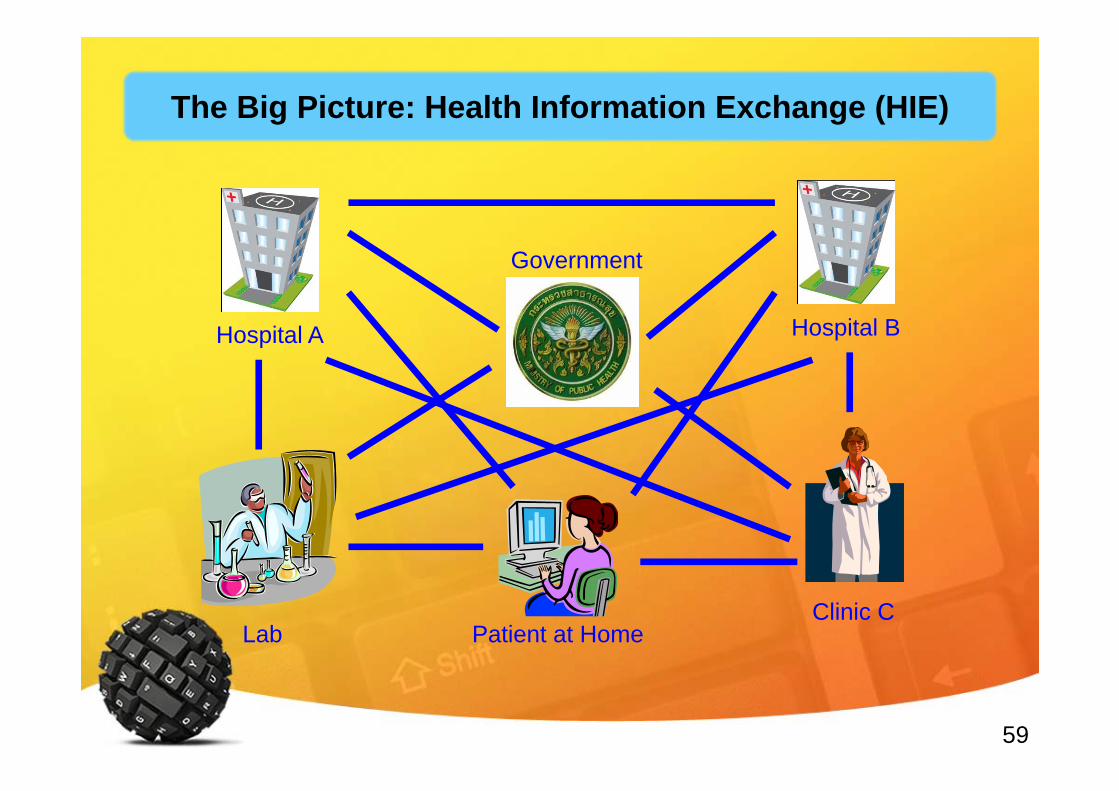
59
Hospital A Hospital B
Clinic C
Government
Lab Patient at Home
The Big Picture: Health Information Exchange (HIE)
60
Outline
Health & Health InformationHealth IT & eHealth• Health Informatics as a Discipline• Thailand’s eHealth Situation• Current Forces
61
Health Informatics as a Discipline
62
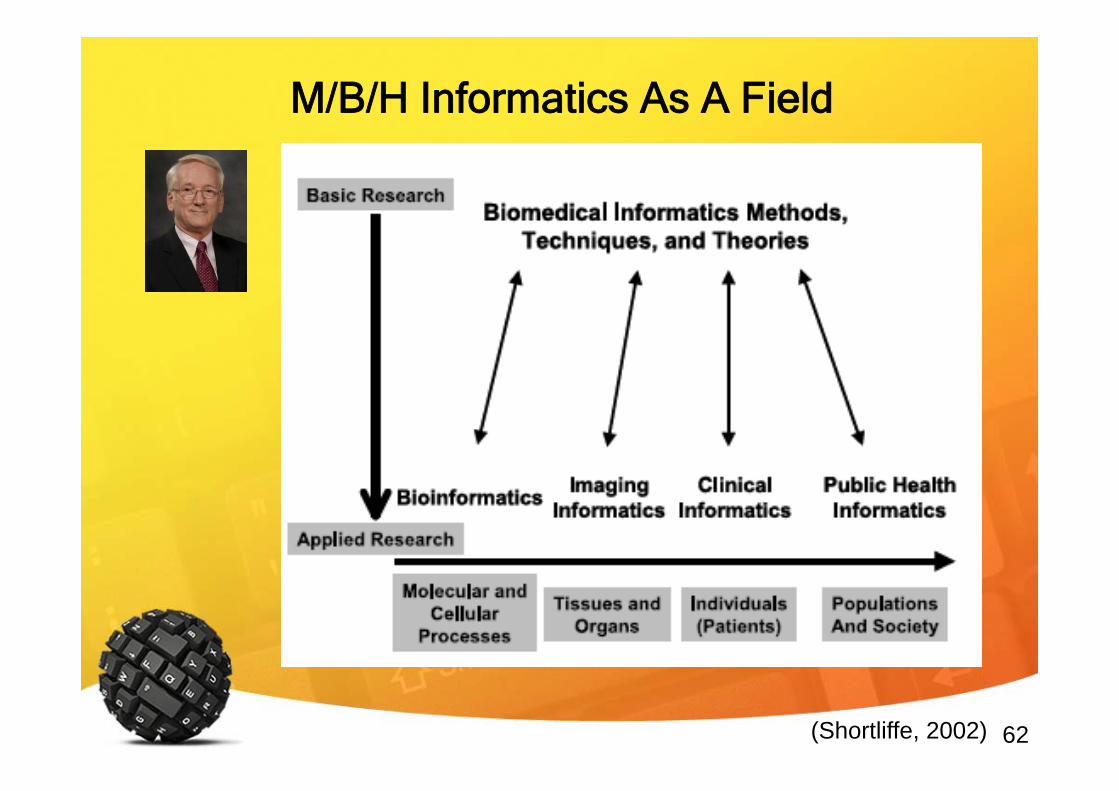
M/B/H Informatics As A Field
(Shortliffe, 2002)
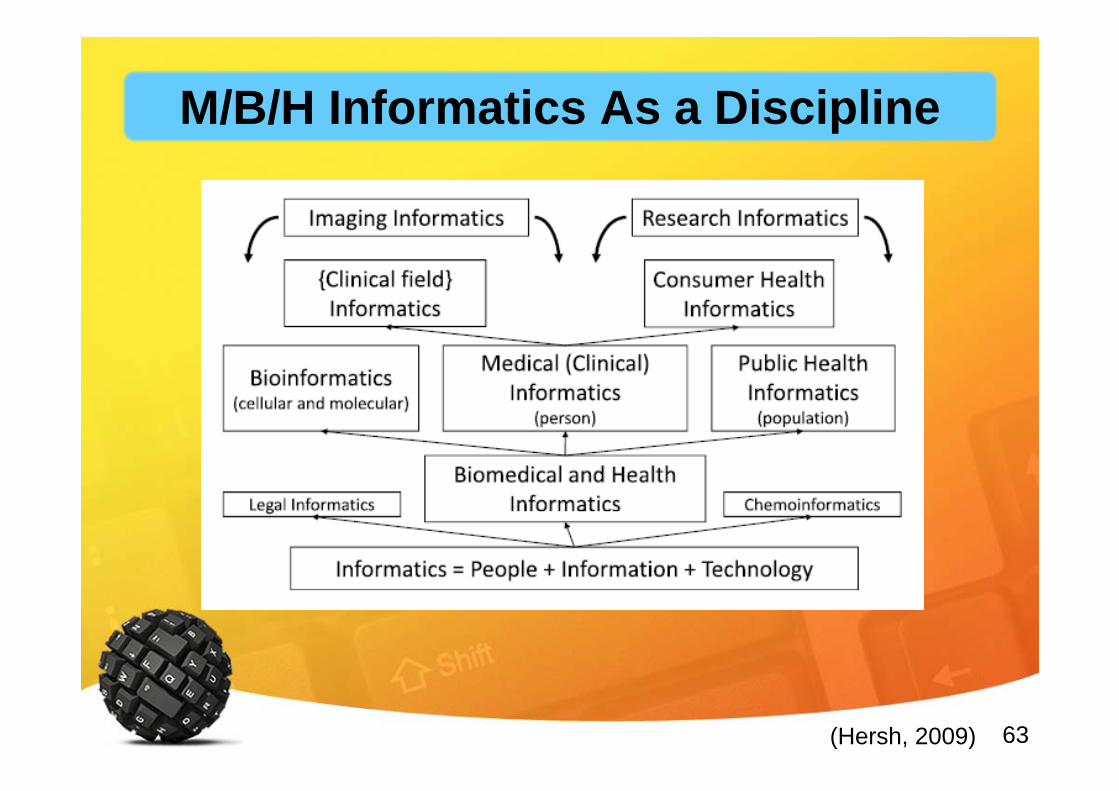
63(Hersh, 2009)
M/B/H Informatics As a Discipline
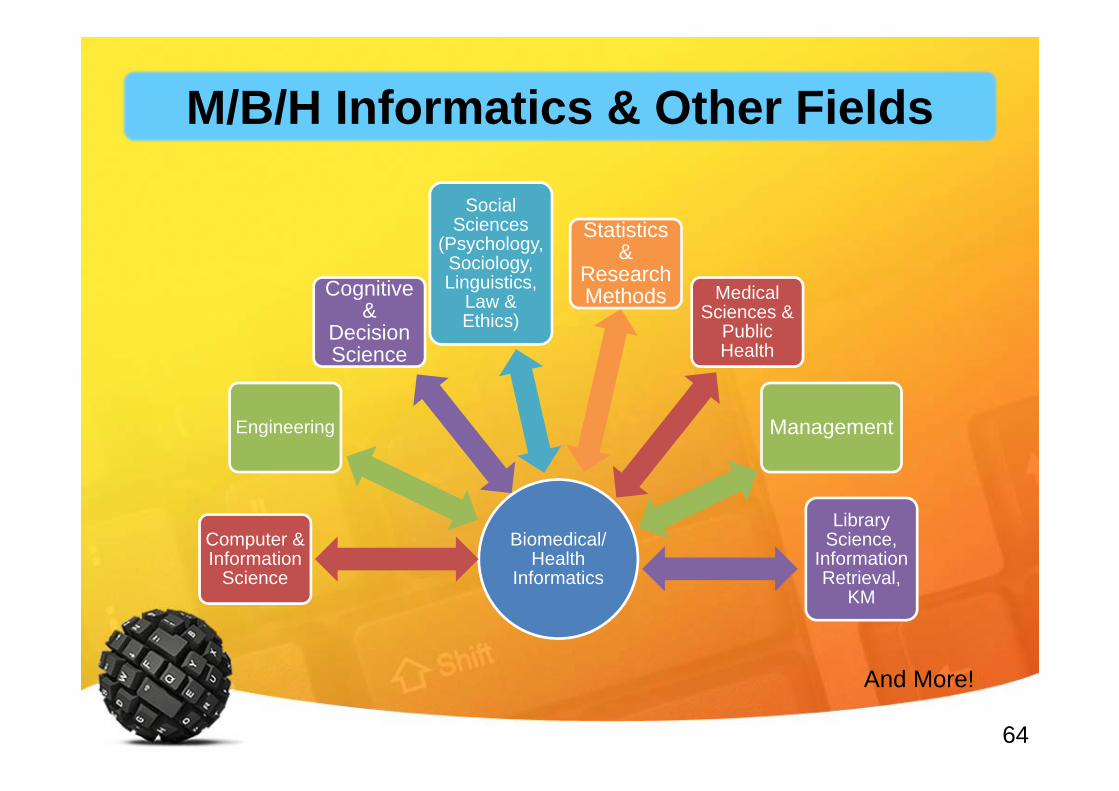
64
Biomedical/Health
Informatics
Computer & Information
Science
Engineering
Cognitive &
Decision Science
Social Sciences
(Psychology, Sociology, Linguistics,
Law & Ethics)
Statistics &
Research Methods Medical
Sciences & Public Health
Management
Library Science,
Information Retrieval,
KM
And More!
M/B/H Informatics & Other Fields
65
Outline
Health & Health InformationHealth IT & eHealthHealth Informatics as a Discipline• Thailand’s eHealth Situation• Current Forces

66
Thailand’s eHealth Situation
67eHealth in Thailand: The current status. Stud Health Technol Inform
2010;160:376–80, Presented at MedInfo2010 South Africa
Thailand’s eHealth: 2010
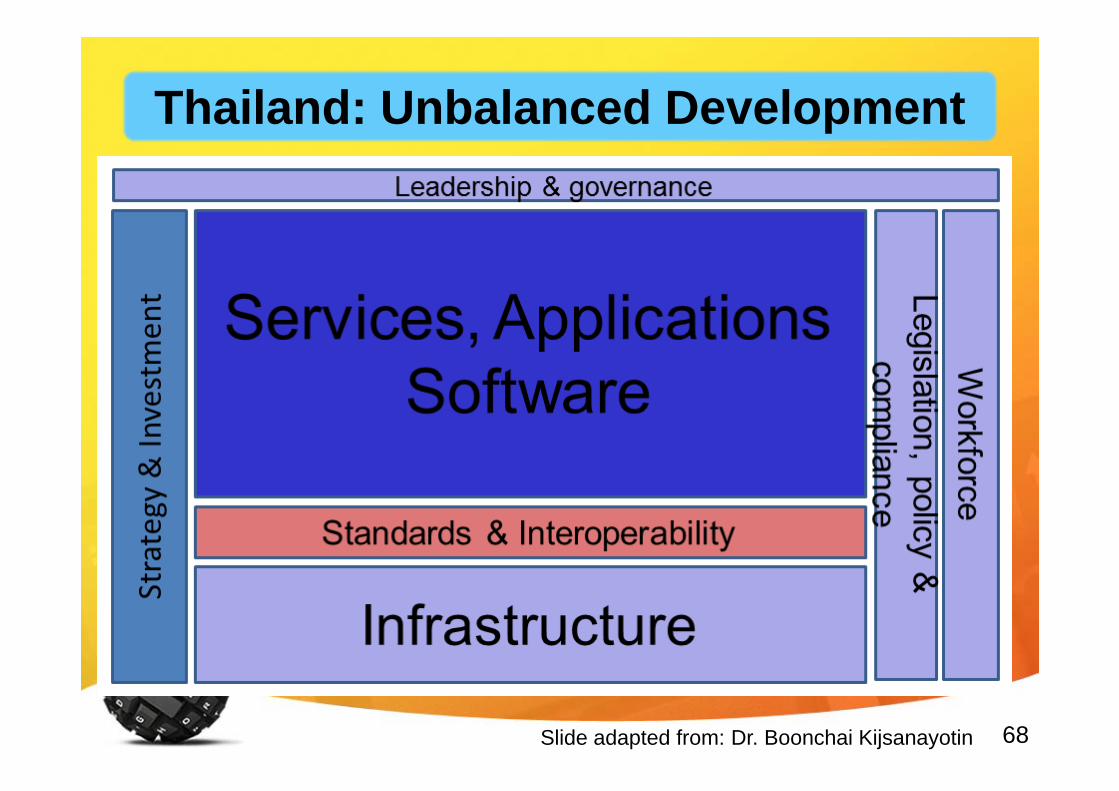
68Slide adapted from: Dr. Boonchai Kijsanayotin
Thailand: Unbalanced Development
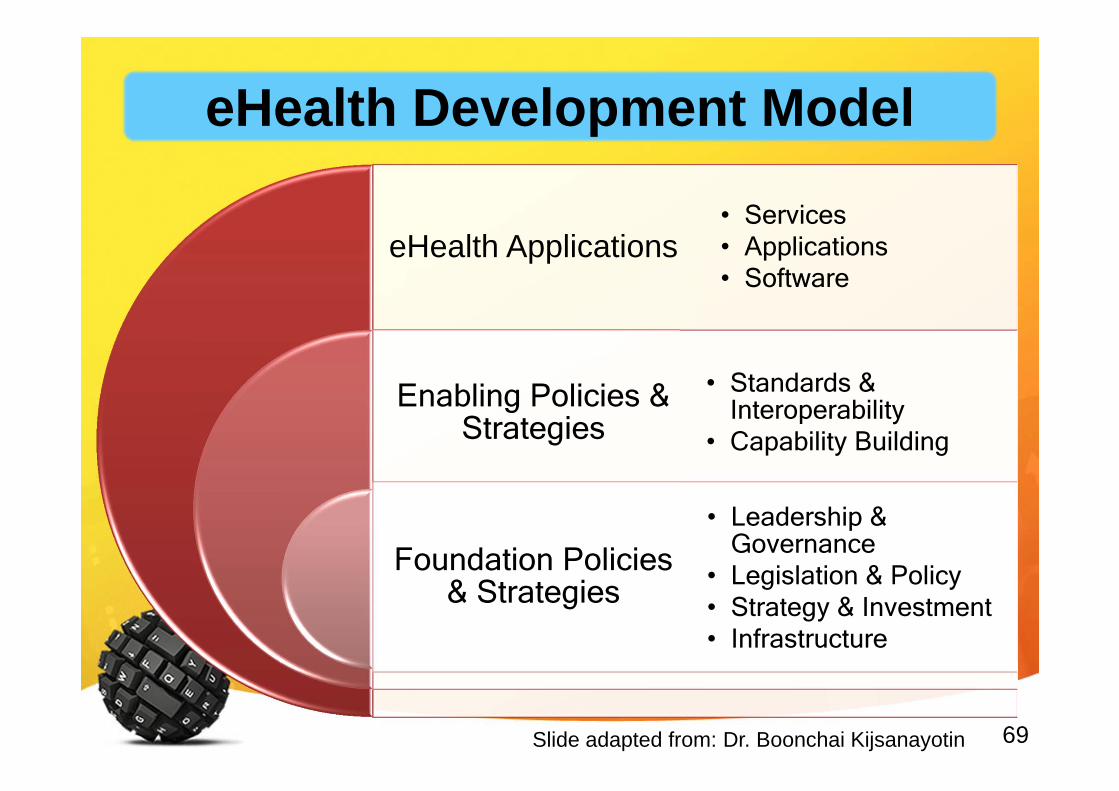
69
eHealth Applications
Enabling Policies & Strategies
Foundation Policies & Strategies
• Services• Applications• Software
• Standards & Interoperability
• Capability Building
• Leadership & Governance
• Legislation & Policy• Strategy & Investment • Infrastructure
Slide adapted from: Dr. Boonchai Kijsanayotin
eHealth Development Model
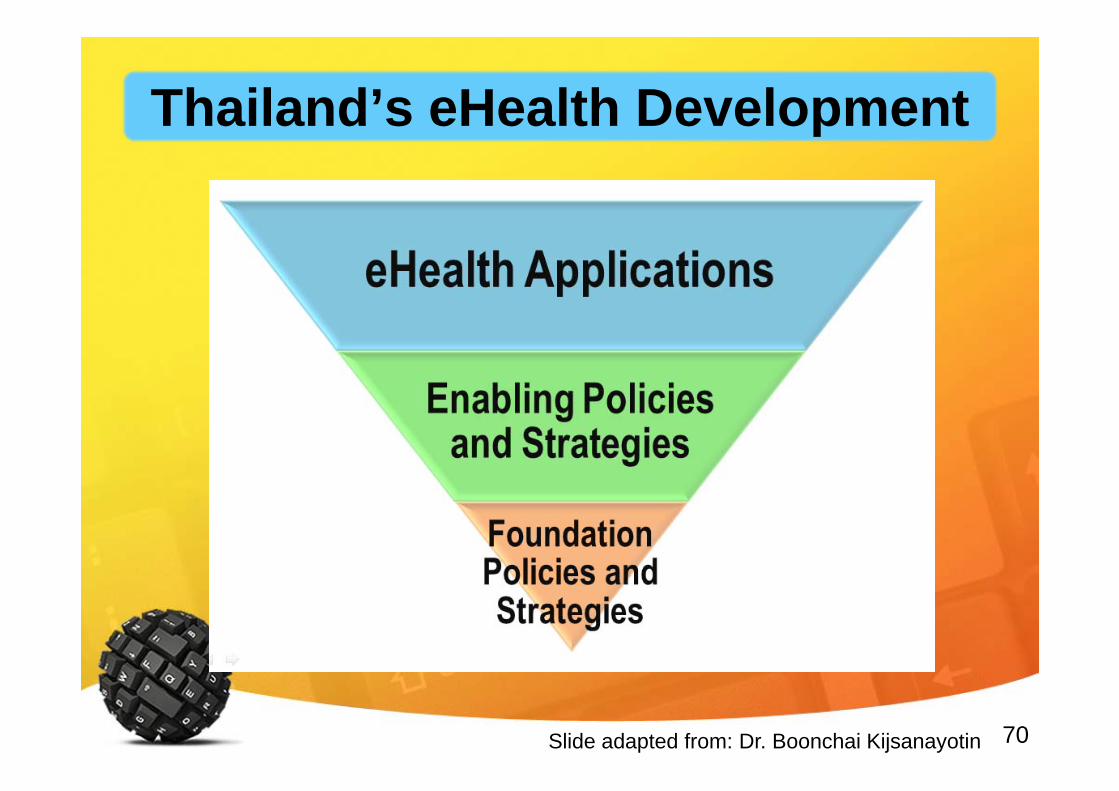
70Slide adapted from: Dr. Boonchai Kijsanayotin
Thailand’s eHealth Development
71
Silo-type systems Little integration and interoperability Mostly aim for administration and management 40% of work-hours spent on managing reports and
documents Lack of national leadership and governance body Inadequate HIS foundations development
Slide adapted from: Boonchai Kijsanayotin
Thailand’s eHealth Situation
72
Section 1 Hospital ProfileSection 2 IT Adoption & Use
ProfileSection 3 Respondent’s
Information
Thailand’s Health IT Adoption
73
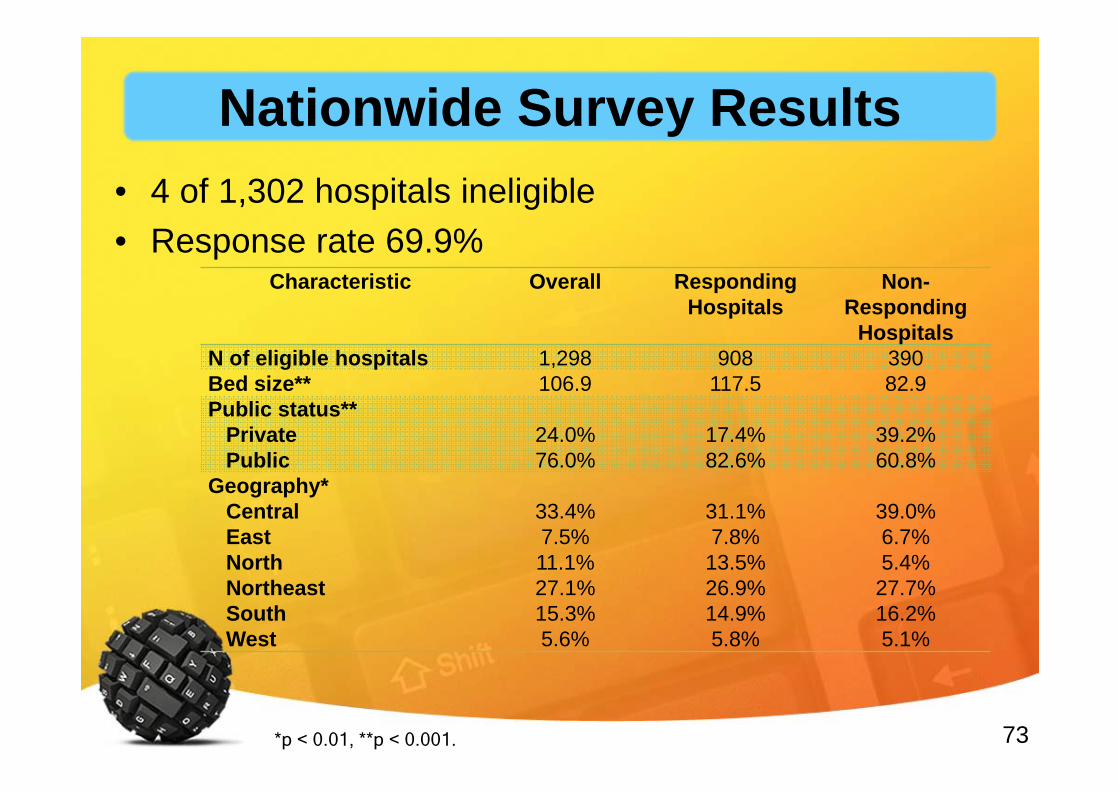
• 4 of 1,302 hospitals ineligible• Response rate 69.9%
Characteristic Overall Responding Hospitals
Non-Responding
HospitalsN of eligible hospitals 1,298 908 390Bed size** 106.9 117.5 82.9Public status**
PrivatePublic
24.0%76.0%
17.4%82.6%
39.2%60.8%
Geography*CentralEastNorthNortheastSouthWest
33.4%7.5%11.1%27.1%15.3%5.6%
31.1%7.8%13.5%26.9%14.9%5.8%
39.0%6.7%5.4%27.7%16.2%5.1%
*p < 0.01, **p < 0.001.
Nationwide Survey Results
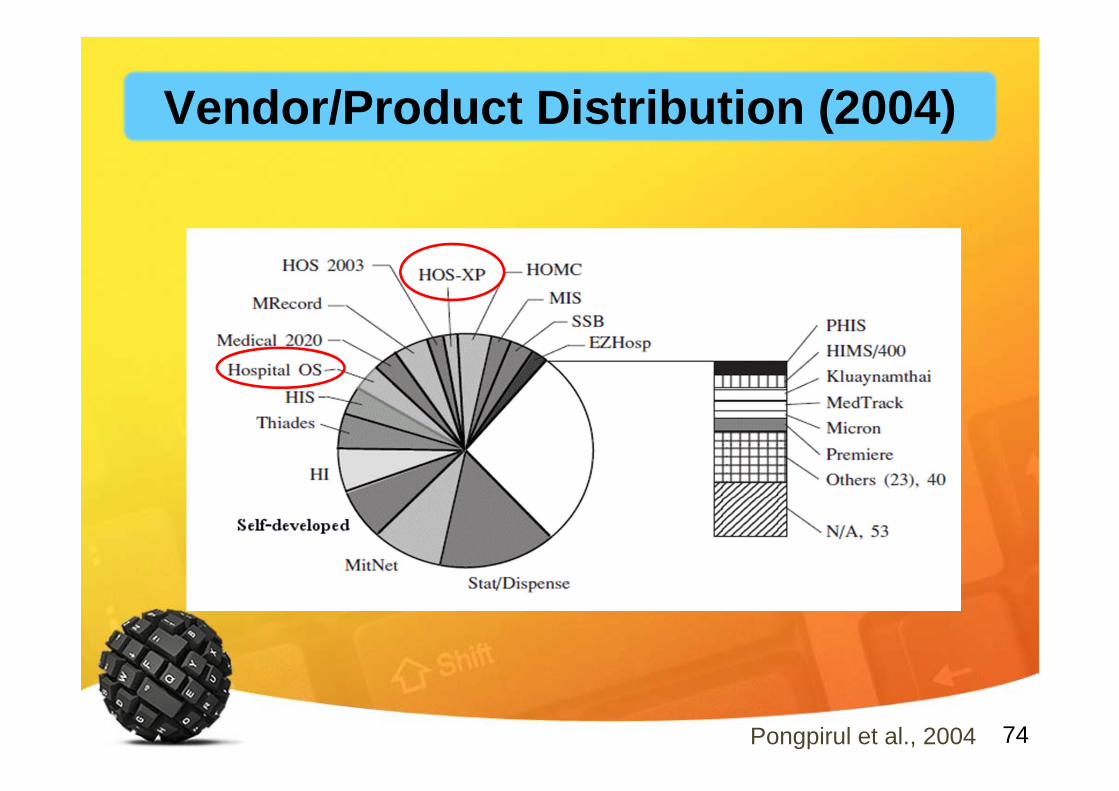
74Pongpirul et al., 2004
Vendor/Product Distribution (2004)
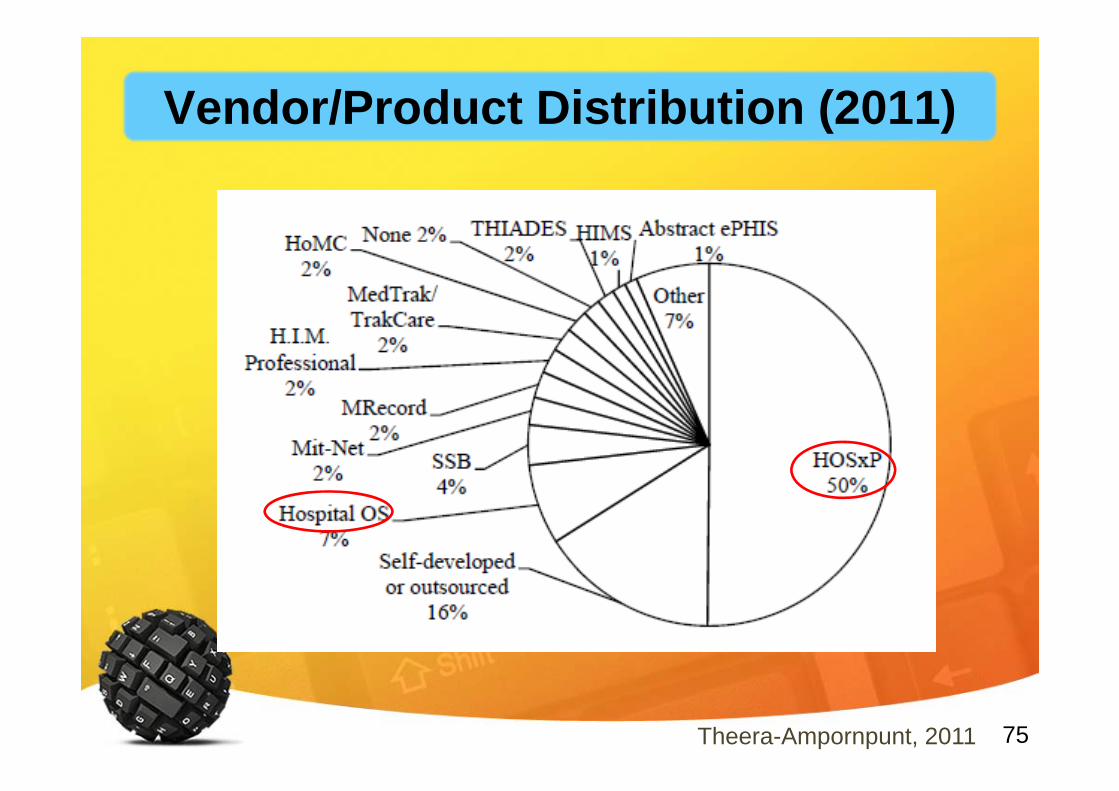
75
Vendor/Product Distribution (2011)
Theera-Ampornpunt, 2011
76
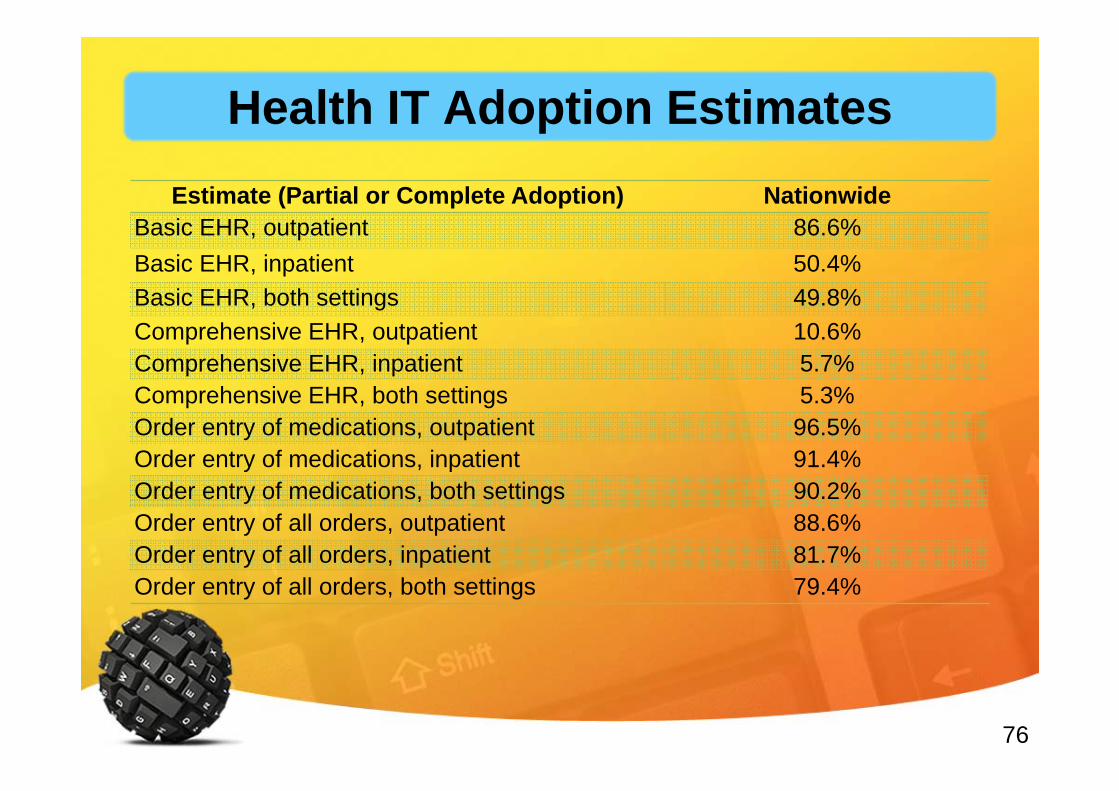
Estimate (Partial or Complete Adoption) NationwideBasic EHR, outpatient 86.6%Basic EHR, inpatient 50.4%Basic EHR, both settings 49.8%Comprehensive EHR, outpatient 10.6%Comprehensive EHR, inpatient 5.7%Comprehensive EHR, both settings 5.3%Order entry of medications, outpatient 96.5%Order entry of medications, inpatient 91.4%Order entry of medications, both settings 90.2%Order entry of all orders, outpatient 88.6%Order entry of all orders, inpatient 81.7%Order entry of all orders, both settings 79.4%
Health IT Adoption Estimates
77
• High IT adoption rates• Drastic changes in adoption landscape• Local context might play a role
– Supply Side– Demand Side
• International Comparison– Relatively higher adoption
THAIS: Discussion
78
Outline
Health & Health InformationHealth IT & eHealthHealth Informatics as a DisciplineThailand’s eHealth Situation• Current Forces
79
Current Forces

80
International• Technology Trends• Standards & Interoperability Trends• eHealth Successes & Failures
– UK NHS– US Meaningful Use– Nordic Countries
• International eHealth Networks– International Medical Informatics Association (IMIA)– American Medical Informatics Association (AMIA)– Asia eHealth Information Network (AeHIN)
Current Forces
81
URGES Member States:(1) to consider, as appropriate, options to collaborate with
relevant stakeholders, including national authorities, relevant ministries, health care providers, and academic institutions, in order to draw up a road map for implementation of ehealth and health data standards at national and subnational levels;
(2) to consider developing, as appropriate, policies and legislative mechanisms linked to an overall national eHealth strategy, in order to ensure compliance in the adoption of ehealth and health data standards by the public and private sectors, as appropriate, and the donor community, as well as to ensure the privacy of personal clinical data;
http://apps.who.int/gb/ebwha/pdf_files/WHA66/A66_R24-en.pdf
World Health Assembly Resolution WHA66.24 (2013) on eHealth Standardization & Interoperability
82
(3) to consider ways for ministries of health and public health authorities to work with their national representatives on the ICANN Governmental Advisory Committee in order to coordinate national positions towards the delegation, governance and operation of health-related global top-level domain names in all languages, including “.health”, in the interest of public health;
http://apps.who.int/gb/ebwha/pdf_files/WHA66/A66_R24-en.pdf
World Health Assembly Resolution WHA66.24 (2013) on eHealth Standardization & Interoperability

83
Domestic• Thailand’s Health Insurance Trends• Increased Hospital IT Adoption• Demands for Data & Information Exchange
in Thailand’s Healthcare• Thailand’s e-Transaction Trends• Consumer IT Behavior Trends
Current Forces
84
Outline
Health & Health InformationHealth IT & eHealthHealth Informatics as a DisciplineThailand’s eHealth SituationCurrent Forces
85Image Source: http://twinstrivia.com/2013/05/20/the-road-to-minnesota-is-long-and-hard/
The Journey Beyond: A Long and Winding Road






![[e-Health] · eHealth Monitor 2017 v Veel kansen zijn voor eHealth ... • Social media • Bekostiging • Overzicht digitale zorg en preventie 11 . Praktijkscan eHealth ... v VIPP](https://img.pdfslide.tips/doc/110x75/600c8895afef3053861cb73c/e-health-ehealth-monitor-2017-v-veel-kansen-zijn-voor-ehealth-a-social-media.jpg)