Embed Size (px)
Citation preview

18-03-16
1
¤ none …but
Ihadnothingtodowithwhathappenedtomylast
Pro-Condebateoponent
¤ AMS-whatisitabout¤ WhyisAgneswrong¤ Whyisitallaboutcosts
AnongoingefforttoopDmizeanDmicrobialuseamonghospitalizedpaDentsinorderto:
¤ ImprovepaDentoutcomes
¤ Ensurecost-effecDvetherapy
¤ ReduceadversesequelaeofanDmicrobialuse(oneofwhichisanDmicrobialresistance)
MacDougal,ClinMicrobiolRev,2005,18:638-656
¤ Consults-‘auditandfeedback’² ReserveanDbioDcs² Risk-paDents
¤ RestricDngchoices² AnDbioDcguideline(adjustedCMreportsandCPdispensing)
¤ Guidelinedevelopment² CAP² UTI
¤ ProjectstoimproveanDmicrobialuse² Switchprogram,5Sprotocol
¤ EducaDon
18-03-16
2
¤ Start:wrongindicaDon,notaccordingtoguideline
¤ Switchivtooralnotdonewhenpossible
¤ Streamlining/adjustmentaccordingtosuscepDbilitynotdone
¤ Safety–disregardinginteracDons
¤ Stop–unneededconDnuaDon
Let’sstartthePro-Condiscussionon:
vs
Resistance Money!
…andsomehelpwithresistance
…havetosaythatbutofcourseit’s
money
Resistance Cochranereview
¤ ‘Interven:onstoimprovean:bio:cprescribinginhospitalsaresuccesfulandcanhelptoreducemicrobiologicalresistance’
¤ 3controlledstudieswithregardtoresistance:
² deMan2000,Lancet(restrictedtoNICU)² Singh2000AJRCC(automaDcstopofAB)² Toltzis2002Pediatrics(cycling)
Brown,2009,Cochranelibrary
Obviouslynot“reduce”,butpreventsomeemergence
¤ InspiteoftheknownassociaDonbetweenanDmicrobialuseandresistance,assumingthatanimprovementinmicrobio-logicaloutcomesfromstudiesthatonlydemonstrateareducDoninanDmicrobialusageishazardous.
HAZARDOUS CONCLUSIONS
Thereareother-probablyevenstronger–factorswithimpactonresistanceratesthanchangesinabsolutequanDDesofanDmicrobialdruguse:¤ DifferencesinpotenDalforselecDonofresistancebetweenanDmicrobials
¤ ImpactofduraDonoftherapyanddosagechanges
¤ Seculartrendsinresistance¤ CultureandliDgaDon,…
18-03-16
3
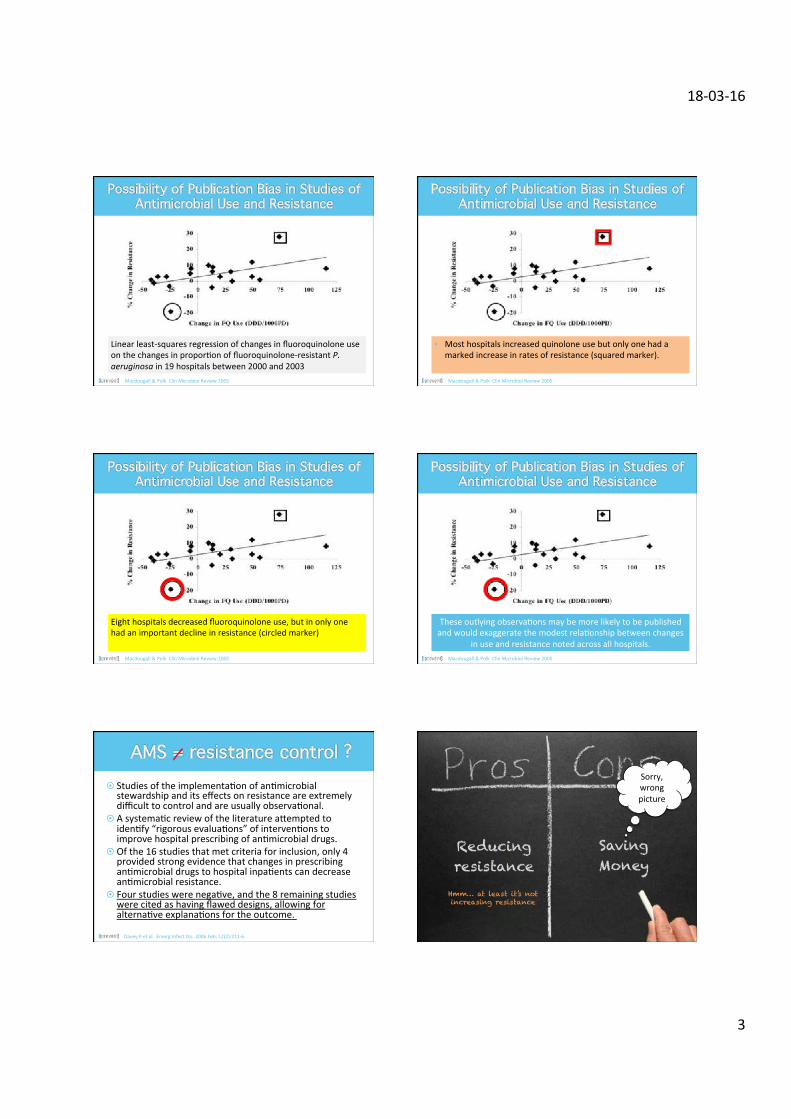
Linearleast-squaresregressionofchangesinfluoroquinoloneuseonthechangesinproporDonoffluoroquinolone-resistantP.aeruginosain19hospitalsbetween2000and2003
Macdougall&PolkClinMicrobiolReview2005
• Mosthospitalsincreasedquinoloneusebutonlyonehadamarkedincreaseinratesofresistance(squaredmarker).
Macdougall&PolkClinMicrobiolReview2005
Eighthospitalsdecreasedfluoroquinoloneuse,butinonlyonehadanimportantdeclineinresistance(circledmarker)
Macdougall&PolkClinMicrobiolReview2005
TheseoutlyingobservaDonsmaybemorelikelytobepublishedandwouldexaggeratethemodestrelaDonshipbetweenchanges
inuseandresistancenotedacrossallhospitals.Macdougall&PolkClinMicrobiolReview2005
¤ StudiesoftheimplementaDonofanDmicrobialstewardshipanditseffectsonresistanceareextremelydifficulttocontrolandareusuallyobservaDonal.
¤ AsystemaDcreviewoftheliteratureahemptedtoidenDfy“rigorousevaluaDons”ofintervenDonstoimprovehospitalprescribingofanDmicrobialdrugs.
¤ Ofthe16studiesthatmetcriteriaforinclusion,only4providedstrongevidencethatchangesinprescribinganDmicrobialdrugstohospitalinpaDentscandecreaseanDmicrobialresistance.
¤ FourstudieswerenegaDve,andthe8remainingstudieswerecitedashavingflaweddesigns,allowingforalternaDveexplanaDonsfortheoutcome.
DaveyPetal.EmergInfectDis.2006Feb;12(2):211-6.
Reducing resistance
Saving Money
Sorry,wrongpicture
Hmm… at least it’s not increasing resistance
18-03-16
4
Reducing resistance
Saving Money
Obviously the organizers let me go first for a reason: They know that this is the
“pro” statement
Gougleditandfoundnothingaboutsaving
money!
ThedataIhaveseenarebiasedorlies
Notonesitemen:oned“An:microbialStewardship”
¤ yes,theremightevenbesome(verylihle)biasinstudiesshowingcost-savings…
AgnesAndreas
¤ Sure,weneededthemforourbusinesscase*tocreatetheA-teaminourhospital
“businesscaseinmedicine”=awellthoughtofandnon-detectablesumofliesandassumpDonstobeabletofinancewhatwebelieveisneededforthesafetyofourpaDents
¤ Sure,weneededthemforourbusinesscase*tocreatetheA-teaminourhospital
¤ SincethefundingofmanyanDmicrobialstewardshipprogramsisconDngentupondemonstraDonofcost-effecDvenessprogramsthatdonotachieveposiDveresultsmaybedisconDnued.
18-03-16
5
¤ PaDentsreceivingoneof10targetanDmicrobialsforgreaterthan3dayswererandomizedtotheintervenDonarmortothestandardofcare.
¤ TheintervenDonconsistedofahavingaclinicalpharmacistandinfecDousdiseasesfellowreviewthemedicalrecordsofpaDentsreceivingthetargetanDmicrobials.IftherewasagreementonaneedtoopDmizeanDmicrobialtherapy(changingorstoppingtherapy,switchingtooralregimen,oranalternaDvedosage),anonpermanentchartnotewaswrihen;85%ofsuggesDonswereimplemented.
¤ Therewasnosignificantdifferenceinclinicalormicrobiolog-icaloutcomesbetweenthegroups,buttotalanDmicrobialcostsweresignificantlylowerintheintervenDonarm;yearlysavingswereesDmatedat$390,000
Fraseretal.Arch.Intern.Med1997;157:1689–1694
¤ 275-bedcommunityhospitalrandomizedpaDentsreceivingpotenDallyinappropriateanDmicrobialstostandardcareortohaveamulDdisciplinaryteamprovidesuggesDonsfortherapy(67).
¤ Eighty-ninepercentofsuggesDonsprovidedintheintervenDonarmwereaccepted.
¤ Themedianlengthofstaywasshorterby3daysintheintervenDonarmthanthecontrolarm,andanoverallcostreduc:onof$2,642perintervenDonwasesDmated.
¤ Otherclinicalandmicrobiologicoutcomesweresimilarbetweenthetwogroups.
Gumsetal.Pharmacotherapy1999;19:1369
¤ RandomizedinpaDentclinicalservicesassigningtotheintervenDonarmandtothecontrolarm.
¤ AllordersforlevofloxacinorcerazidimeintheintervenDongroupwerereviewed.Ifanorderwasnotincompliancewiththeguidelines,amemberoftheA-teamcontactedtheprescribertosuggestalternaDvetherapy.
¤ TheduraDonofinappropriatetherapyofthetargetanDmicrobialswasreducedbyapproximately40%intheintervenDongroup,whileclinicaloutcomesweresimilarbetweenthegroups.
Solomonetal.ArchInternMed2001;161:1897
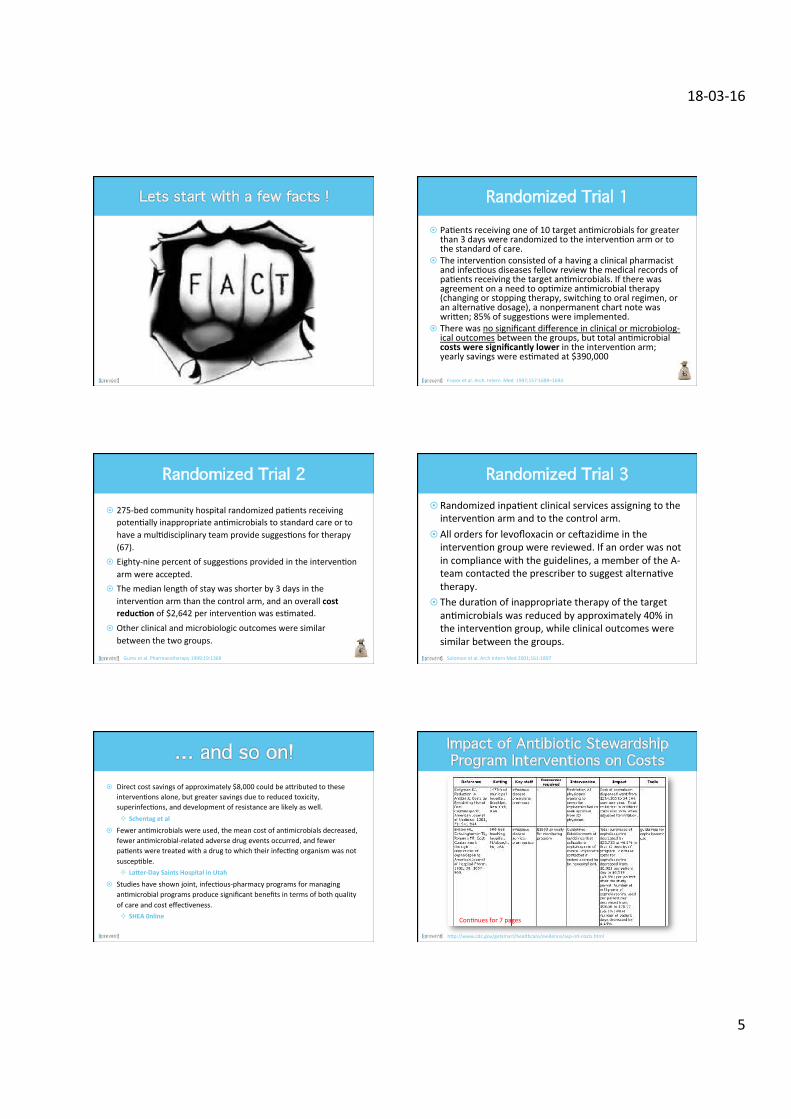
¤ Directcostsavingsofapproximately$8,000couldbeahributedtotheseintervenDonsalone,butgreatersavingsduetoreducedtoxicity,superinfecDons,anddevelopmentofresistancearelikelyaswell.² Schentagetal
¤ FeweranDmicrobialswereused,themeancostofanDmicrobialsdecreased,feweranDmicrobial-relatedadversedrugeventsoccurred,andfewerpaDentsweretreatedwithadrugtowhichtheirinfecDngorganismwasnotsuscepDble.² LaGer-DaySaintsHospitalinUtah
¤ Studieshaveshownjoint,infecDous-pharmacyprogramsformanaginganDmicrobialprogramsproducesignificantbenefitsintermsofbothqualityofcareandcosteffecDveness.² SHEA0nline
hhp://www.cdc.gov/getsmart/healthcare/evidence/asp-int-costs.html
ConDnuesfor7pages

18-03-16
6
PhamD
ClinMicro/ID
ICT
¤ Control/restricteduseofreserve-anDbioDcs¤ SelectandmeasurelocalindicatorsforadequateanDmicrobialuse
¤ Standardizeempirictreatmentandenhance/fosteriv-oralswitch.
¤ EducaDonandtrainingwithregardtoanDmicrobialuse
¤ DefineallpaDentscategoriesthatneedbed-sideIDconsultaDon
¤ Real-Dmesurveillance(includingfeedback)oflocalresistancetrends
¤ all-causemortality
¤ infecDon-relatedmortality
¤ duraDonofhospitalizaDon
¤ ratesofreadmission
Whatwouldyouchoosetotakehome?Whyevendebate!
18-03-16
7
…thusitmutbeaboutthefirst$48million!
Coverslightlymodified
Reducing Resistance
(development)
Money saved to invest in:
• A-team • Patient safety • Infection Control
Reducing resistance
Saving Money
It’snotonlyaboutsavingmoneyand(partly)aboutreducingresistance,it’smainlyaboutadequate
andopDmalAB-treatment
Antimicrobial Stewardship





























