Embed Size (px)
Citation preview

Central Hospital Reform in Malawi 1
Establishment of Public Trust Hospitals in Malawi:Expert Panel on Reforms
Report
Ministry of Health
SWAp mid-year Review meeting
27th April 2015

Central Hospital Reform in Malawi 2
Outline of presentation Introduction Findings by Consultancy on Establishment of Public Trust
Hospitals (What has been done / Progress on Reforms) Challenges Why Reforms Proposed Reforms
Efficient & Effective Central Hospitals (QECH, KCH, MCH, ZCH)
Efficient & Effective District Health Services - (Blantyre, Lilongwe, Mzuzu & Zomba
Considerations Conclusions

Central Hospital Reform in Malawi 3
Introduction Hospital Reforms were initiated in Malawi health system
(National Health Policy Framework) – 1995 (20 years to-date)
Starting 1997, the MOH Working Group on Hospital Autonomy prepared a draft policy which proposed goals and strategies for hospital autonomy including the decentralisation of hospitals and new roles for hospital boards, management and the MOH. – 4th National Health Plan, and– Program of Work, both made provision for reforms.
– Program implemented by PHR Plus and from early 2003,
– Program implemented by MSH (both funded by USAID).

Central Hospital Reform in Malawi 4
2015 - Key Findings
Only Gate way clinic established in Blantyre operated by DHO – KCH (efforts made)
Assessment of Blantyre health facilities done – Ndirande, Bangwe, Chilomoni & Zingwangwa (to look at report
Selected systems in place i.e. HMIS system in QECH
By pass fee in place in QECH & KCH
Special paying ward in KCH
Hospitals accessing funds from paying services (60%?)

Central Hospital Reform in Malawi 5
Challenge
• ‘The inability of central hospitals to provide equitable access to tertiary quality health care to all Malawians’ • (Draft Hospital Reform Policy: September 2006 and
Cabinet Paper on Reforms: 2004)
• Central hospitals’ failure to deliver their core functions - including provision of quality specialist care, professional training, research and district support

Central Hospital Reform in Malawi 6
Challenges• All urban (City) districts including Blantyre, Zomba, Lilongwe
and Mzuzu do not have district.
• Urban districts have very large populations served by very limited hospital services including Central hospitals, CHAM and private hospitals / clinics - 4 central hospitals, 2 Mental hospitals, 23 district hospitals, 37 community hospitals and 21 CHAM hospitals.
• Most CHAM hospitals and community hospitals are not operating at optimum capacity. CHAM hospitals are affected by funding / resources while community hospitals have serious lack of equipment, and human resources

Central Hospital Reform in Malawi 7
Why Reforms?
• Need to make the hospitals run more effectively and efficiently
• Giving more control to the hospitals to manage their own affairs
• That the hospitals will have greater power to manage themselves
• That the hospitals can appoint their own staff directly
• That the hospitals can manage their own finances

Central Hospital Reform in Malawi 8
Why Reforms?
Inadequate policy, regulatory and institutional framework
Gross under-management of public central hospitals
An inefficient health referral system
MSH 2007

Central Hospital Reform in Malawi 9
Why Reforms? HR situationCentral hospital QECH KCH ZCH MCH
Medical Doctors 16 31 4 4
Intern Medical Doctors 79 61 1 2
Paediatrician 1 1 0 0
Specialist[3] // Surgeons 3 4 2 2
Internal Medicine 0 1 0 0
Obstetrics & Gynaecology 3 2 0 0
Ophthalmologist 1 2 1 0
Pathologists 0 0 0 0
Dental Specialist 1 0
Radiologist 0 1 0 0
Oncologist 1 0 0 0
Orthopaedic Surgeon 0 0 0 0
104 104 8 8
Source: Hospitals Staff Returns - 2015

Central Hospital Reform in Malawi 10
Mzuzu Central Hospital
Grade Staff CategoryAuthorized Posts
Filled Posts
Vacant Posts
D Chief Specialists / Hospital Director 15 2 13E Principal Specialists /Deputy Hospital Director 36 1 35
FSpecialists /Chief Officers - Clinical, Nursing, Clinical Support, Administrator, Accountant 53 13 40
GPrincipal Officers - Clinical, Nursing, Clinical Support, Administrator, Accountant, Medical Doctors 66 12 54
HSenior Officers - Clinical, Nursing, Clinical Support, Administrator, Accountant, Medical Doctors 54 5 49
IOfficers - Clinical, Nursing, Clinical Support, Administrator, Accountant 97 72 25
J Senior Technicians - Clinical, Nursing, Clinical Support 112 22 90K Technicians - Clinical, Nursing, Clinical Support 223 179 44
LSenior - Ward / Data Clerks/Nurse Auxilliaries / Clerical Officers / Catering / Accounts Assistants 43 10 33
MWard / Data Clerks/Nurse Auxilliaries / Clerical Officers/ Catering / Accounts Assistants 100 41 59
N Operators /Hospital / Patient Attendants 29 8 21O Hospital / Patient Attendants 42 76 -34P Guards 154 38 116
1024 479 545

Central Hospital Reform in Malawi 11
Queen Elizabeth Central Hospital - As of December 2014
Grade Staff CategoryAuthorized Posts Filled Posts Vacant Posts
D Chief Specialists / Hospital Director 17 6 11
E Principal Specialists /Deputy Hospital Director 34 10 24
FSpecialists /Chief Officers - Clinical, Nursing, Clinical Support, Administrator, Accountant 58 23 35
GPrincipal Officers - Clinical, Nursing, Clinical Support, Administrator, Accountant, Medical Doctors 71 28 43
HSenior Officers - Clinical, Nursing, Clinical Support, Administrator, Accountant, Medical Doctors 60 111 -51
I Officers - Clinical, Nursing, Clinical Support, Administrator, Accountant 110 150 -40
J Senior Technicians - Clinical, Nursing, Clinical Support 122 32 90
K Technicians - Clinical, Nursing, Clinical Support 235 339 -104
LSenior - Ward / Data Clerks/Nurse Auxilliaries / Clerical Officers / Catering / Accounts Assistants 50 21 29
MWard / Data Clerks/Nurse Auxilliaries / Clerical Officers/ Catering / Accounts Assistants 120 87 33
N Operators /Hospital / Patient Attendants 42 58 -16
O Hospital / Patient Attendants 48 209 -161
P Guards 164 162 2
Q Cooks 12 10 2
R Ground Labourer 15 10 5
1158 1256 -98

Central Hospital Reform in Malawi 12
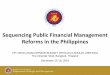
Why Reforms? Patients seen in Central Hospitals
Q1 (Jul-Sep 13) Q2 (Oct - Dec 13) Q3 (Jan - Mar 14) Q4 (Apr - Jun 14) Q5 (Jul - Sep 14) Q6 (Oct -Dec 14)0
10000
20000
30000
40000
50000
60000
KCH Attendance
OPD attendance Seen by Specialist Admissions all Discharges - tot

Central Hospital Reform in Malawi 13
Why Reforms? HR situation
• Number of Specialists very low (Grades F- D)
• Highest number of staff are subordinates employees and professional staff grades – (M to I) – not the required staff for Central Hospitals
• Numbers of Doctors high where there are Interns
• Translating into poor quality of care and limited specialist services

Central Hospital Reform in Malawi 14
Why Reforms? District Support function
• One of the critical roles for public trust hospitals is to provide district support to ensure provision of quality clinical care in all districts in the country.
• The ability by public trust hospitals to attract and retain well - qualified personnel including Medical Specialists, Specialist nurses and para-medicals will have the potential of revitalizing the Malawi health system through this function.
• Enabling districts receive technical support from those that are responsible for managing cases that the districts refers– Undertaking Specialist visits for district specialist clinics– Mentorship and clinical couching visits– Organizing clinical camps in public trust hospitals for district staff, – Providing referrals feedback– Making recommendations and identifying potential district staff for Specialist training– Facilitating clinical and Specialist trainings are the important functions that the public
trust hospitals are to undertake.

Central Hospital Reform in Malawi 15
Why Reforms? Strengthening urban health services
Construction of district hospitals - Long term Establishment of City / Urban District Health Offices /
integrate the office with the Directorate of Health and Social Services for the City Councils
Up grading of urban health centres to become urban (community) hospitals:
Construction of Gate Way Clinics and urban health centres Establishment of Urban Health Outreach programs Urban (City) District Health offices agreements with CHAM
to operate district hospitals services in CHAM hospitals Promote Public – Private Partnerships (Community Health
Partnerships).

Central Hospital Reform in Malawi
EPOS 2010

Central Hospital Reform in Malawi 17
Proposed Reforms
Recommended change in Policy:Governance structure change through
establishment of Public Trust Hospitals
Legal precedents are National AIDS Commission (NAC), Malawi Blood Transfusion Service (MBTS), Small Medium Entrepreneur Development Institute (SMEDI), Central Medical Stores Trust (CMST)

Central Hospital Reform in Malawi 18
Proposed Reforms
Recommended change in Policy:Governance structure change through
establishment of Public Trust Hospitals
Legal precedents are National AIDS Commission (NAC), Malawi Blood Transfusion Service (MBTS), Small Medium Entrepreneur Development Institute (SMEDI), Central Medical Stores Trust (CMST)

Central Hospital Reform in Malawi 19
Proposed Reforms : Objectives of Public Trust Hospitals• Establish authority and accountability of public trust hospital boards and
management• Improve the quality and availability of public hospital care, especially for
priority conditions• Ensure equitable access to essential public hospital services • Establish an effective referral system• Ensure hospitals are accountable to the people they serve• Introduce modern hospital management practices for efficient care
delivery• Ensure sustainable public hospital financing • Provide support for training health workers and for research• Provide effective district support• Strengthen urban health services

Central Hospital Reform in Malawi 20
Proposed Reforms : Features of Public Trust Hospitals Hospitals remain in public ownership therefore state assets
are not alienated
No change in fee policy
Public Trust Hospitals need necessary policies, procedures, systems and staff to implement decentralized management
Legislation

Central Hospital Reform in Malawi 21
Proposed Reforms : Features of Public Trust Hospitals
Separation of Primary, Secondary & Tertially (central hospital) services
City Councils to be responsible for primary and secondary health services in cities
Public Trust hospitals be ‘National Resources’ and thus to become “Autonomous” Hospitals responsible to a Management Board

Central Hospital Reform in Malawi 22
Proposed Reforms : Features of Public Trust Hospitals (2)
Decentralization of management controlled through a performance management agreement between MOH and hospital boards
Hospital focus on performance improvement measured by outputs as well as inputs
Introduction of a business management approach (commercial accounting system, business planning, marketing department, business IT system)

Central Hospital Reform in Malawi 23
Proposed Reforms : Features of Public Trust Hospitals (3) New cadre of professional hospital managers:
– CEO
– Finance, HR, Physical Assets and Pharmaceutical Services Directors
Allowed to attract new sources of finance
- public – private partnerships
- grants & direct donations
- Fees (service, research, training etc.)
Continue to bid for Government capital funds (Purpose built paying units, Specialized OPD units, HDU etc.)

Central Hospital Reform in Malawi 24
Proposed reforms: Roadmap for public trust hospitals reforms process
The Roadmap (14 steps outlined) :• Agree to the specific content for establishment of public
trust hospitals as outlined in this report• Identification of governing structure and board composition• Development of the advocacy and communication strategy
and communicating the objectives of the process• Drafting cabinet paper and seeking cabinet approval• Determining personnel policies and transition arrangements• Developing systems procedures and plans• Communication to stakeholders including staff and the
public

Central Hospital Reform in Malawi 25
Proposed reforms: Roadmap for public trust hospitals reforms process
• Preparation of service plans• Registering public trust hospitals under public trust act• Developing service agreements and performance
management systems• Selecting and training key managers and board members• Start operating Public Trust Hospitals (1st July 2016)• Drafting legislation and obtaining parliament endorsement• Reviewing implementation of the preparatory phase (April
to June 2016), transition phase (July 2016 to June 2018) and final evaluation of the implementation period (after June 2020).

Central Hospital Reform in Malawi 26
Proposed Reforms: Recommendations (Financing) Proposed mechanisms to fund Public Trust
hospitals:
Public Trust Hospitals FundTo benefit from Health Fund / Government funding
arrangementProposing 25% from Health Fund to finance the 5 PTH’s Independently managedSource additional Funding / get donationsGovernment funding based on Referral budgets for
Districts & CHAM Hospitals

Central Hospital Reform in Malawi 27
Proposed Reforms: Recommendations (Financing 2)
Proposed mechanisms to fund Central hospitals:
By Pass fees (OPD I) – In-place In – Patient paying services – In placeCharges for training / student levy charged to
teaching institutions (per student)Charges for student research / student levy
charged to teaching institutions (per student)Charges for research / researchers levy charged to
individual researchers & research institutions

Central Hospital Reform in Malawi 28
Proposed Reforms: Recommendations - Financing Proposed mechanisms to fund Public Trust
hospitals: Government ORT for management during
transitionTransition period (3 years)MOH support
Donor support - Financing of Independent facilitator for reforms
Finances managed / mobilized through the Public Trust Hospitals Fund

Central Hospital Reform in Malawi 29
Challenges to address:
Problems with the term “autonomy”:negative public perceptionsequated with privatisation, fee for service,
limitation of access to central hospital services and alienation of public assets
none of these issues are fundamental to the policy on introduction of public trust hospitals

Central Hospital Reform in Malawi 30
ConclusionsNeed to address a wide array of policy,
management and devolution issues
Considerable vested interests in status quo at all levels
Advocacy & Communication essential
Policy changes, systems strengthening and structural adjustments take time to develop and implement (facilitates preparations & acceptance)