Embed Size (px)
Citation preview

Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 1
Measuring the health-related Sustainable Development Goals in 188 countries: a baseline analysis from the Global Burden of Disease Study 2015GBD 2015 SDG Collaborators*
SummaryBackground In September, 2015, the UN General Assembly established the Sustainable Development Goals (SDGs). The SDGs specify 17 universal goals, 169 targets, and 230 indicators leading up to 2030. We provide an analysis of 33 health-related SDG indicators based on the Global Burden of Diseases, Injuries, and Risk Factors Study 2015 (GBD 2015).
Methods We applied statistical methods to systematically compiled data to estimate the performance of 33 health-related SDG indicators for 188 countries from 1990 to 2015. We rescaled each indicator on a scale from 0 (worst observed value between 1990 and 2015) to 100 (best observed). Indices representing all 33 health-related SDG indicators (health-related SDG index), health-related SDG indicators included in the Millennium Development Goals (MDG index), and health-related indicators not included in the MDGs (non-MDG index) were computed as the geometric mean of the rescaled indicators by SDG target. We used spline regressions to examine the relations between the Socio-demographic Index (SDI, a summary measure based on average income per person, educational attainment, and total fertility rate) and each of the health-related SDG indicators and indices.
Findings In 2015, the median health-related SDG index was 59∙3 (95% uncertainty interval 56∙8–61∙8) and varied widely by country, ranging from 85∙5 (84∙2–86∙5) in Iceland to 20∙4 (15∙4–24∙9) in Central African Republic. SDI was a good predictor of the health-related SDG index (r²=0∙88) and the MDG index (r²=0∙92), whereas the non-MDG index had a weaker relation with SDI (r²=0∙79). Between 2000 and 2015, the health-related SDG index improved by a median of 7∙9 (IQR 5∙0–10∙4), and gains on the MDG index (a median change of 10∙0 [6∙7–13∙1]) exceeded that of the non-MDG index (a median change of 5∙5 [2∙1–8∙9]). Since 2000, pronounced progress occurred for indicators such as met need with modern contraception, under-5 mortality, and neonatal mortality, as well as the indicator for universal health coverage tracer interventions. Moderate improvements were found for indicators such as HIV and tuberculosis incidence, minimal changes for hepatitis B incidence took place, and childhood overweight considerably worsened.
Interpretation GBD provides an independent, comparable avenue for monitoring progress towards the health-related SDGs. Our analysis not only highlights the importance of income, education, and fertility as drivers of health improvement but also emphasises that investments in these areas alone will not be suffi cient. Although considerable progress on the health-related MDG indicators has been made, these gains will need to be sustained and, in many cases, accelerated to achieve the ambitious SDG targets. The minimal improvement in or worsening of health-related indicators beyond the MDGs highlight the need for additional resources to eff ectively address the expanded scope of the health-related SDGs.
Funding Bill & Melinda Gates Foundation.
Copyright The Authors(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license.
BackgroundIn September, 2015, the UN General Assembly adopted “Transforming our World: The 2030 Agenda for Sustainable Development”, a resolution outlining a new framework to form the cornerstone of the sustainable development agenda for the period leading up to 2030.1 This new framework replaced the Millennium Development Goal (MDG) framework that expired in 2015, establishing 17 universal goals and 169 targets referred to as the Sustainable Development Goals (SDGs). The SDGs substantially broaden the development agenda beyond the MDGs and are expected to frame UN member state
policies over the next 15 years. To measure progress towards achieving the goals, the UN Statistical Commission created the Inter-Agency and Expert Group on Sustainable Development Goal Indicators (IAEG-SDGs) with a mandate to draft an indicator framework that aligns with the targets. The IAEG-SDGs announced a total of 230 indicators to measure achievement of the 169 targets.2 Health is a core dimension of the SDGs; goal 3 aims to “ensure healthy lives and promote wellbeing for all at all ages”. Health-related indicators—ie, indicators directly pertaining to health services, health outcomes, and environmental, occupational, behavioural, or metabolic
Published OnlineSeptember 21, 2016http://dx.doi.org/10.1016/S0140-6736(16)31467-2
See Online/Commenthttp://dx.doi.org/10.1016/S0140-6736(16)31635-X
*Collaborators listed at the end of the Article
Correspondence to:Prof Christopher J L Murray, University of Washington, Institute for Health Metrics and Evaluation, 2301 5th Avenue, Suite 600, Seattle, WA 98121, [email protected]
See Online for infographic http://www.thelancet.com/infographics/SDG
Articles
2 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
risks with well established causal connections to health—are also present in ten of the other 16 goals.3,4 Across these 11 goals, there are 28 health-related targets with a total of 47 health-related indicators.
The SDGs were developed through a highly consultative and iterative process that included multiple meetings with expert groups, civil society, and governments. However, the process of developing the SDGs and the accompanying goals, targets, and indicators has not been without its critics. In both scientifi c settings and the news media, the common refrain has been that the SDGs are a long list of vague goals that lack clear, realistic, and measurable targets and indicators,5–11 and that they are not accompanied by a clear theory of change12 articulating how the pieces fi t together.3 In view of the potential importance of the SDGs in directing national policies and donor investments, there has also been intense debate about the selection of targets and indicators;12 despite the lengthy list, some think that the SDGs are missing key areas of development, ranging from prohibition of forced labour13 to improvement of mental health.14–16 Concerns have also been expressed about the feasibility of measuring the 230 proposed indicators.5,6,17 Indeed, measurement of countries’ current status and progress towards meeting the SDG targets will be an enormous task and will require collective action across a range of national and international organisations, both governmental and non-governmental. The diffi culties of measurement are also further compounded by persistent problems of data availability, quality, and comparability across a host of indicators.4,18 Furthermore, measurement of development indicators is accompanied by a high potential for political entanglement, which can lead to distorted estimates.19–22 Independent monitoring of the SDG indicators will be crucial if they are to be used to accurately evaluate progress to ensure accountability and drive national and international development agendas towards meeting the SDGs.4,23–26
Despite these concerns, increasing work has been done in the past decade to generate independent, comparable, valid, and consistent measurements of development indicators.27–32 To measure progress on the SDGs, these existing eff orts will need to be leveraged, particularly those that provide comparable assessments of health outcomes and risks across countries and over time. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) is a primary example of such an initiative. GBD is an open, collaborative, independent study to comprehensively measure epidemiological levels and trends of disease and risk factor burden worldwide, with more than 1870 individual collaborators from 124 countries and three territories across the full range of development. GBD uses a highly standardised approach to overcome challenges of inconsistent coding and indicator defi nitions across countries, missing and confl icting data, and time lags in measurement and estimation. Of the 47 health-related indicators included as part of the SDGs, estimates for 33 indicators are presently included as part of GBD. The GBD study also has several mechanisms to ensure independence, including the GBD Scientifi c Council that meets regularly to review all methods and major data changes, and the Independent Advisory Committee that meets twice yearly to review GBD progress and provide recommendations for strengthening GBD estimates.33
In this analysis, while acknowledging the continued debate about the structure, selection, and construction of SDG indicators, we used the GBD study to assess the current status of these 33 health-related SDG indicators. With this baseline assessment, we developed and estimated a summary indicator for the health-related SDG indicators and documented historical trends for this summary indicator. With the GBD results, we identifi ed countries with the largest improvements between 1990 and 2015 to inform roadmaps and provide a basis for monitoring the health-related SDG indicators.
Research in context
Evidence before this studySince the adoption of the Sustainable Development Goals (SDGs) in September, 2015, demand to establish independent, robust avenues for monitoring progress for the SDGs has escalated. However, substantial challenges exist in undertaking comprehensive and comparable assessments of health-related SDG indicators to monitor and guide development agendas and health policy implementation.
Added value of this studyThe Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) features more than 1870 collaborators from 124 countries and three territories and provides an independent analytical platform through which levels of health-related SDG indicators can be assessed across geographies and over time in a
comparable manner. Drawing from GBD, we provide the measurement of 33 of the 47 health-related SDG indicators and introduce an overall health-related SDG index for 188 countries from 1990 to 2015.
Implications of all the available evidenceGBD and its analytical framework allow detailed analyses of country-level performance across health-related SDG indicators and over time. This information can be used to identify high-performing and low-performing countries, inform policy decisions, guide resource allocation, and monitor progress towards the health-related SDGs. The varied historical progress in improving a subset of health-related SDG indicators and rising prevalence of risks such as child overweight underscores the complex health landscape the world faces in the SDG era.

Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 3
MethodsOverview of GBDGBD is an annual eff ort to measure the health of populations at regional, country, and selected subnational levels.33 GBD produces estimates of mortality and morbidity by cause, age, sex, and country for the period 1990 to the most recent year, refl ecting all available data sources adjusted for bias. GBD also measures many health system characteristics, risk factor exposure, and mortality and morbidity attributable to these risks. In addition to providing highly detailed standardised information for many outcomes and risks, various summary measures are also computed, including disability-adjusted life-years (DALYs) and healthy life expectancy. For the present analysis, we used estimates from GBD 2015 to provide a baseline assessment for 188 countries. Further details on GBD 2015, which covers 1990–2015, are available elsewhere.34–39
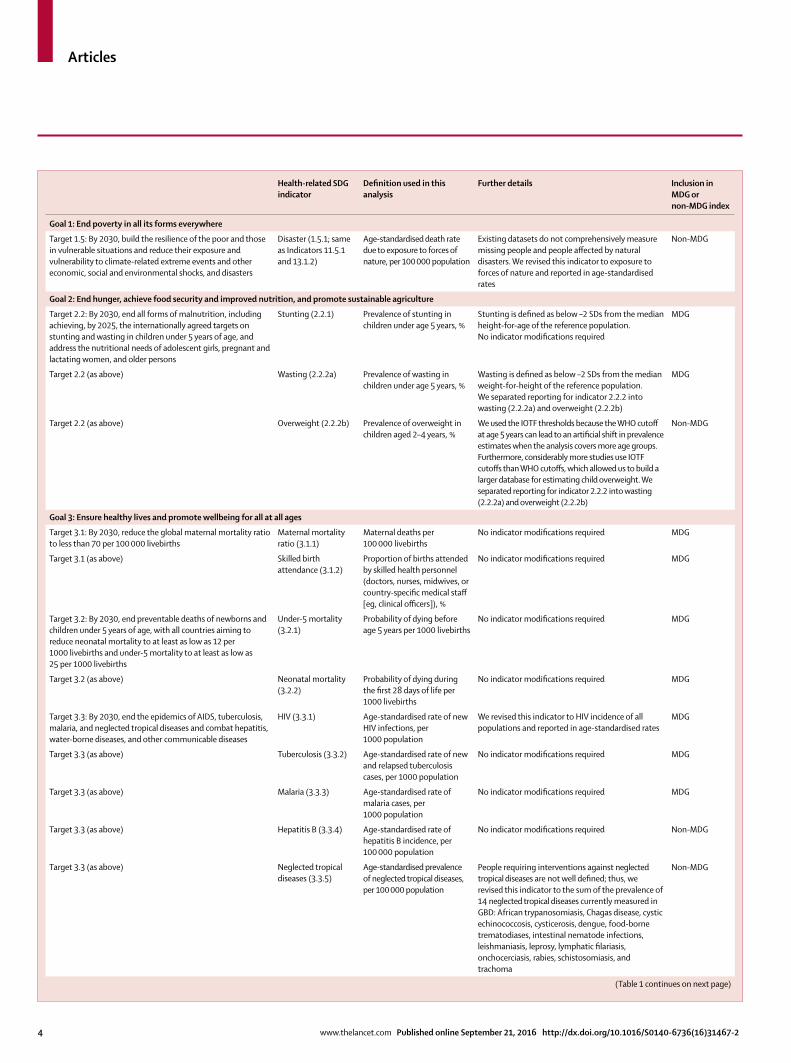
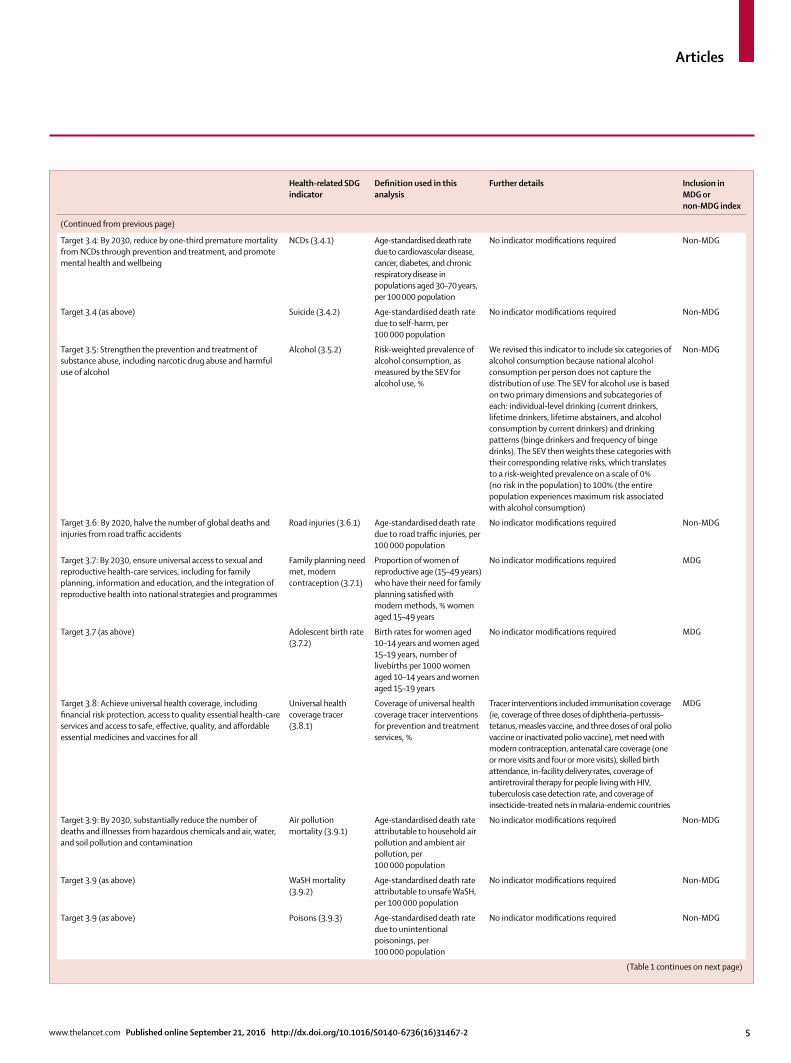
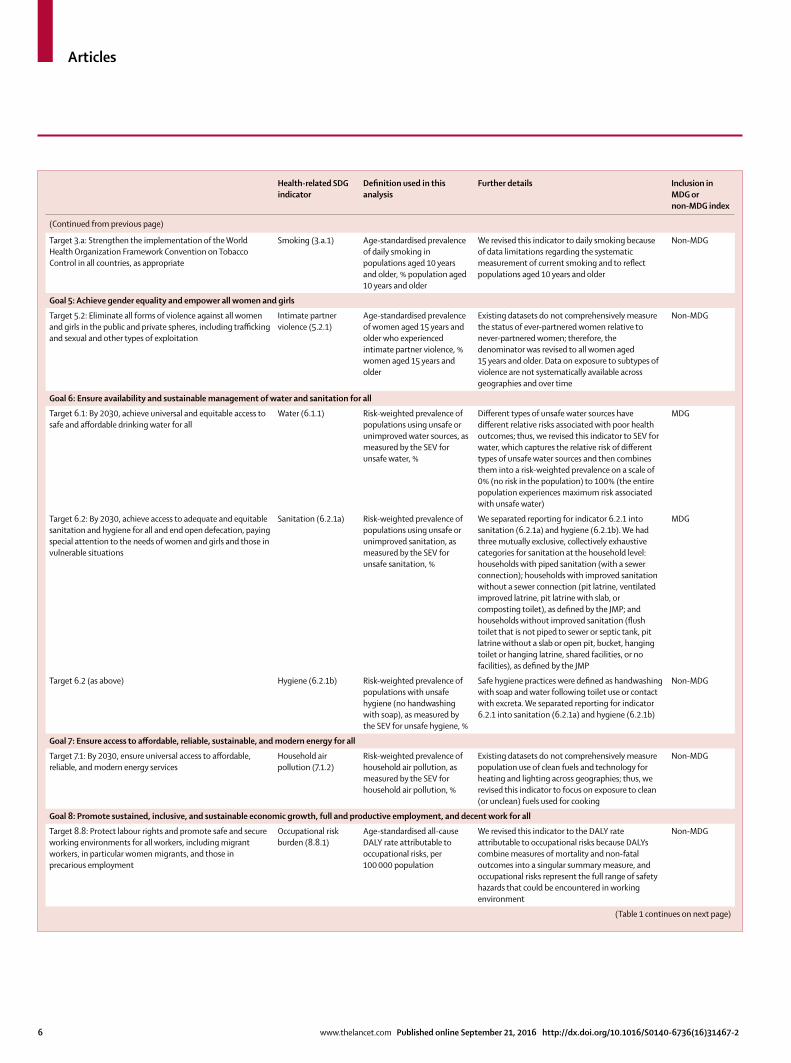
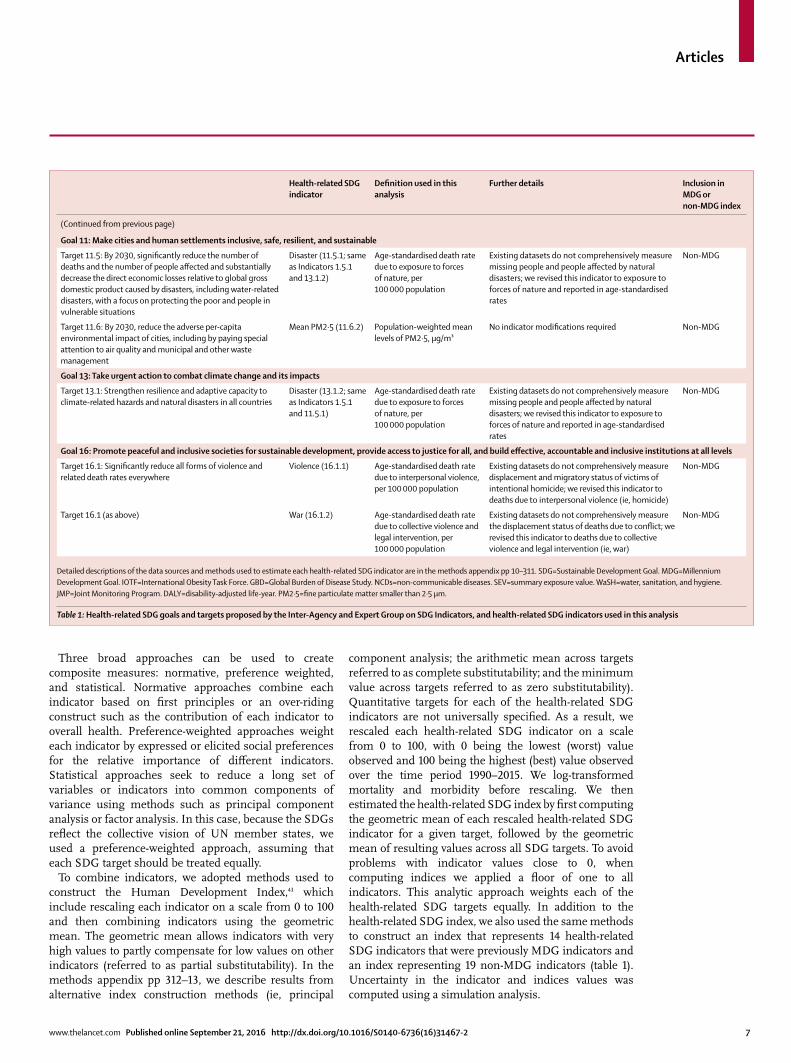
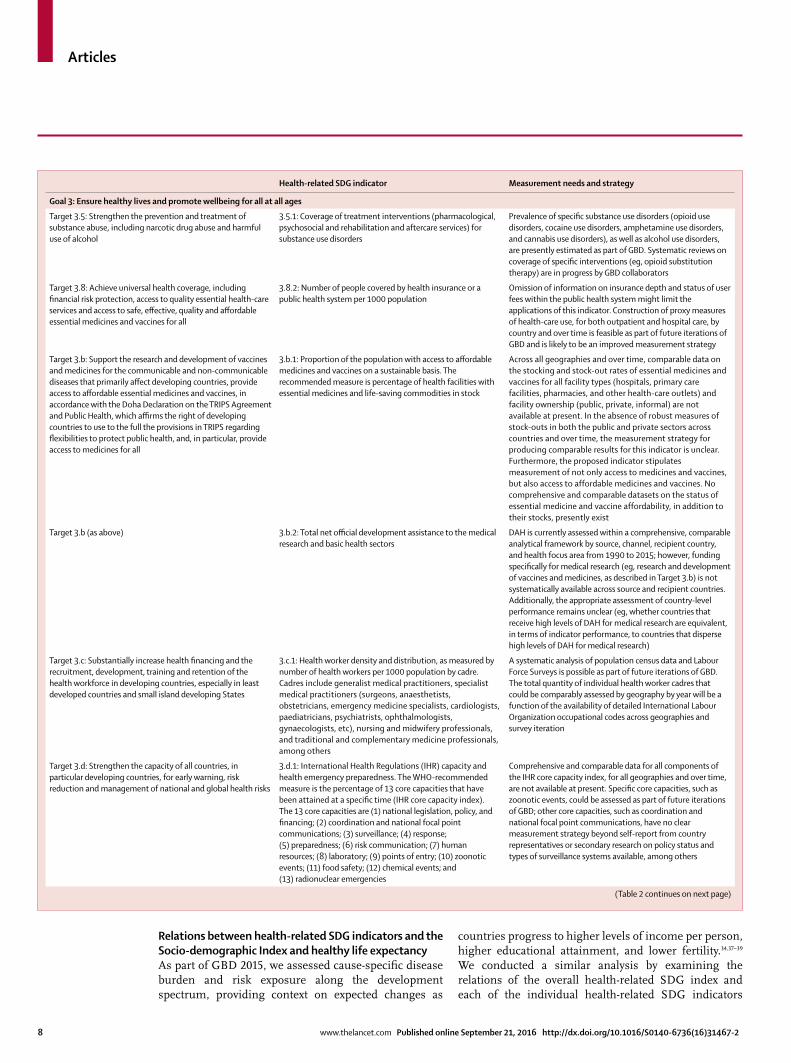
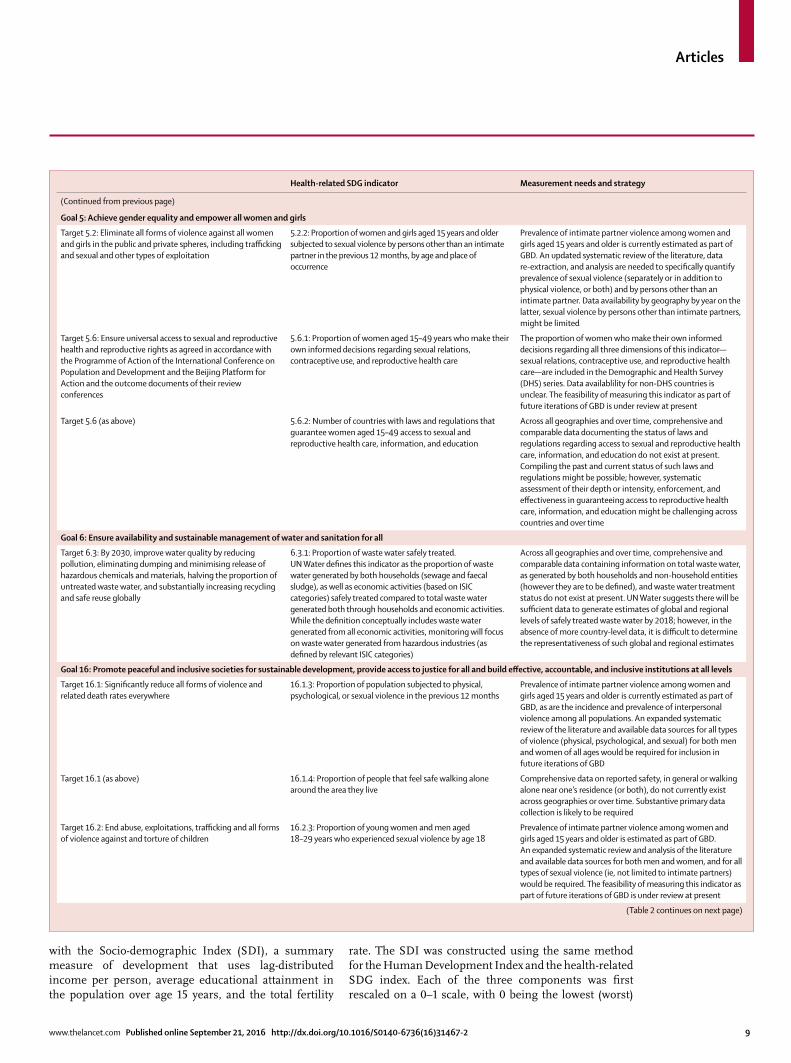
Indicators, defi nitions, and measurement approachWe defi ned health-related SDG indicators as indicators for health services, health outcomes, and environmental, occupational, behavioural, and metabolic risks with well established causal connections to health. Many of the 47 health-related SDG indicators selected by the IAEG-SDGs are produced as part of GBD. Table 1 outlines the ten goals, corresponding to 21 health-related targets and 33 health-related indicators included in this present iteration of GBD. This table also outlines the defi nition of the indicator used in this analysis; detailed descriptions of the estimation methods and data sources are given in the methods appendix pp 10–311. For the 14 health-related indicators that were not included in this analysis, their prospects for measurement in future iterations of GBD are described in table 2.
Direct outputs of GBD that are health-related SDG indicators include mortality disaggregated by age (under-5 and neonatal) and cause (maternal, cardiovascular disease, cancer, diabetes, chronic respiratory diseases, road injuries, self-harm, un inten-tion al poisonings, exposure to forces of nature, inter-personal violence, and collective violence and legal inter vention [ie, deaths due to law enforcement actions, irrespective of their legality]), as well as disease incidence (HIV, malaria, tuberculosis, and hepatitis B) and prevalence (neglected tropical diseases). The GBD comparative risk assessment includes measurement of exposure prevalence included as health-related SDG indicators (under-5 stunting, wasting, and overweight; tobacco smoking; harmful alcohol use; intimate partner violence; unsafe water, sanitation, and hygiene; household air pollution; and ambient particulate matter pollution), as well as deaths or disease burden attributable to risk factors selected as health-related SDG indicators (unsafe water, sanitation, and hygiene; household air pollution and ambient particulate matter pollution; and occupational risks).
Underlying GBD outputs are a range of additional health determinants that contribute to the estimation of morbidity and mortality, for which data are systematically compiled and estimates are produced. For example, GBD comprehensively analyses data from household surveys on vaccine coverage and combines survey estimates with reported administrative data to produce time series of vaccine coverage for all countries from 1990 to 2015. Estimates of vaccine coverage are then included as predictors of vaccine-preventable morbidity and mortality in GBD. Additional health indicators produced as part of GBD and included as health-related SDG indicators in this analysis are: met need with modern contraception among women of reproductive age, adolescent birth rate, skilled birth attendance coverage, and universal health coverage (UHC) tracer interventions. For UHC tracer interventions, we developed an index based on the geometric mean of the coverage of a set of UHC tracer interventions: met need with modern contraception; antenatal care (one or more visits and four or more visits); skilled birth attendance coverage; in-facility delivery rates; vaccination coverage (three doses of diphtheria–pertussis–tetanus, measles vaccine, and three doses of oral polio vaccine or inactivated polio vaccine); tuberculosis case detection rate; coverage of antiretroviral therapy for populations living with HIV, and coverage of insecticide-treated nets for malaria-endemic countries.
For selected indicators proposed by the IAEG-SDGs, we made modifi cations to the defi nition for clarity or on the basis of the defi nition used in GBD (table 1). For example, Indicator 2.2.2 proposes a measure of malnutrition that combined prevalence of wasting and overweight among children under age 5 years. As childhood wasting and overweight have very diff erent determinants, we opted to report them separately. For childhood overweight, we report prevalence in children aged 2–4 years, the defi nition used in GBD based on thresholds set by the International Obesity Task Force.40
Further details on the estimation and data sources used for all indicators, compliant with Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER),41,42 are included in the methods appendix pp 10–311.
Health-related SDG, health-related MDG, and health-related non-MDG indicesTo identify broad patterns and more easily track general progress, we developed an overall health-related SDG index that is a function of the 33 health-related SDG indicators (referred to as the health-related SDG index). We also constructed two related indices: one refl ecting the SDG health-related indicators previously included in the MDG monitoring framework (referred to as the MDG index) and one refl ecting SDG health-related indicators not included in the MDGs (referred to as the non-MDG index).
See Online for appendices
Articles
4 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
Health-related SDG indicator
Defi nition used in this analysis
Further details Inclusion in MDG or non-MDG index
Goal 1: End poverty in all its forms everywhere
Target 1.5: By 2030, build the resilience of the poor and those in vulnerable situations and reduce their exposure and vulnerability to climate-related extreme events and other economic, social and environmental shocks, and disasters
Disaster (1.5.1; same as Indicators 11.5.1 and 13.1.2)
Age-standardised death rate due to exposure to forces of nature, per 100 000 population
Existing datasets do not comprehensively measure missing people and people aff ected by natural disasters. We revised this indicator to exposure to forces of nature and reported in age-standardised rates
Non-MDG
Goal 2: End hunger, achieve food security and improved nutrition, and promote sustainable agriculture
Target 2.2: By 2030, end all forms of malnutrition, including achieving, by 2025, the internationally agreed targets on stunting and wasting in children under 5 years of age, and address the nutritional needs of adolescent girls, pregnant and lactating women, and older persons
Stunting (2.2.1) Prevalence of stunting in children under age 5 years, %
Stunting is defi ned as below –2 SDs from the median height-for-age of the reference population. No indicator modifi cations required
MDG
Target 2.2 (as above) Wasting (2.2.2a) Prevalence of wasting in children under age 5 years, %
Wasting is defi ned as below –2 SDs from the median weight-for-height of the reference population. We separated reporting for indicator 2.2.2 into wasting (2.2.2a) and overweight (2.2.2b)
MDG
Target 2.2 (as above) Overweight (2.2.2b) Prevalence of overweight in children aged 2–4 years, %
We used the IOTF thresholds because the WHO cutoff at age 5 years can lead to an artifi cial shift in prevalence estimates when the analysis covers more age groups. Furthermore, considerably more studies use IOTF cutoff s than WHO cutoff s, which allowed us to build a larger database for estimating child overweight. We separated reporting for indicator 2.2.2 into wasting (2.2.2a) and overweight (2.2.2b)
Non-MDG
Goal 3: Ensure healthy lives and promote wellbeing for all at all ages
Target 3.1: By 2030, reduce the global maternal mortality ratio to less than 70 per 100 000 livebirths
Maternal mortality ratio (3.1.1)
Maternal deaths per 100 000 livebirths
No indicator modifi cations required MDG
Target 3.1 (as above) Skilled birth attendance (3.1.2)
Proportion of births attended by skilled health personnel (doctors, nurses, midwives, or country-specifi c medical staff [eg, clinical offi cers]), %
No indicator modifi cations required MDG
Target 3.2: By 2030, end preventable deaths of newborns and children under 5 years of age, with all countries aiming to reduce neonatal mortality to at least as low as 12 per 1000 livebirths and under-5 mortality to at least as low as 25 per 1000 livebirths
Under-5 mortality (3.2.1)
Probability of dying before age 5 years per 1000 livebirths
No indicator modifi cations required MDG
Target 3.2 (as above) Neonatal mortality (3.2.2)
Probability of dying during the fi rst 28 days of life per 1000 livebirths
No indicator modifi cations required MDG
Target 3.3: By 2030, end the epidemics of AIDS, tuberculosis, malaria, and neglected tropical diseases and combat hepatitis, water-borne diseases, and other communicable diseases
HIV (3.3.1) Age-standardised rate of new HIV infections, per 1000 population
We revised this indicator to HIV incidence of all populations and reported in age-standardised rates
MDG
Target 3.3 (as above) Tuberculosis (3.3.2) Age-standardised rate of new and relapsed tuberculosis cases, per 1000 population
No indicator modifi cations required MDG
Target 3.3 (as above) Malaria (3.3.3) Age-standardised rate of malaria cases, per 1000 population
No indicator modifi cations required MDG
Target 3.3 (as above) Hepatitis B (3.3.4) Age-standardised rate of hepatitis B incidence, per 100 000 population
No indicator modifi cations required Non-MDG
Target 3.3 (as above) Neglected tropical diseases (3.3.5)
Age-standardised prevalence of neglected tropical diseases, per 100 000 population
People requiring interventions against neglected tropical diseases are not well defi ned; thus, we revised this indicator to the sum of the prevalence of 14 neglected tropical diseases currently measured in GBD: African trypanosomiasis, Chagas disease, cystic echinococcosis, cysticerosis, dengue, food-borne trematodiases, intestinal nematode infections, leishmaniasis, leprosy, lymphatic fi lariasis, onchocerciasis, rabies, schistosomiasis, and trachoma
Non-MDG
(Table 1 continues on next page)
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 5
Health-related SDG indicator
Defi nition used in this analysis
Further details Inclusion in MDG or non-MDG index
(Continued from previous page)
Target 3.4: By 2030, reduce by one-third premature mortality from NCDs through prevention and treatment, and promote mental health and wellbeing
NCDs (3.4.1) Age-standardised death rate due to cardiovascular disease, cancer, diabetes, and chronic respiratory disease in populations aged 30–70 years, per 100 000 population
No indicator modifi cations required Non-MDG
Target 3.4 (as above) Suicide (3.4.2) Age-standardised death rate due to self-harm, per 100 000 population
No indicator modifi cations required Non-MDG
Target 3.5: Strengthen the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol
Alcohol (3.5.2) Risk-weighted prevalence of alcohol consumption, as measured by the SEV for alcohol use, %
We revised this indicator to include six categories of alcohol consumption because national alcohol consumption per person does not capture the distribution of use. The SEV for alcohol use is based on two primary dimensions and subcategories of each: individual-level drinking (current drinkers, lifetime drinkers, lifetime abstainers, and alcohol consumption by current drinkers) and drinking patterns (binge drinkers and frequency of binge drinks). The SEV then weights these categories with their corresponding relative risks, which translates to a risk-weighted prevalence on a scale of 0% (no risk in the population) to 100% (the entire population experiences maximum risk associated with alcohol consumption)
Non-MDG
Target 3.6: By 2020, halve the number of global deaths and injuries from road traffi c accidents
Road injuries (3.6.1) Age-standardised death rate due to road traffi c injuries, per 100 000 population
No indicator modifi cations required Non-MDG
Target 3.7: By 2030, ensure universal access to sexual and reproductive health-care services, including for family planning, information and education, and the integration of reproductive health into national strategies and programmes
Family planning need met, modern contraception (3.7.1)
Proportion of women of reproductive age (15–49 years) who have their need for family planning satisfi ed with modern methods, % women aged 15–49 years
No indicator modifi cations required MDG
Target 3.7 (as above) Adolescent birth rate (3.7.2)
Birth rates for women aged 10–14 years and women aged 15–19 years, number of livebirths per 1000 women aged 10–14 years and women aged 15–19 years
No indicator modifi cations required MDG
Target 3.8: Achieve universal health coverage, including fi nancial risk protection, access to quality essential health-care services and access to safe, eff ective, quality, and aff ordable essential medicines and vaccines for all
Universal health coverage tracer (3.8.1)
Coverage of universal health coverage tracer interventions for prevention and treatment services, %
Tracer interventions included immunisation coverage (ie, coverage of three doses of diphtheria–pertussis–tetanus, measles vaccine, and three doses of oral polio vaccine or inactivated polio vaccine), met need with modern contraception, antenatal care coverage (one or more visits and four or more visits), skilled birth attendance, in-facility delivery rates, coverage of antiretroviral therapy for people living with HIV, tuberculosis case detection rate, and coverage of insecticide-treated nets in malaria-endemic countries
MDG
Target 3.9: By 2030, substantially reduce the number of deaths and illnesses from hazardous chemicals and air, water, and soil pollution and contamination
Air pollution mortality (3.9.1)
Age-standardised death rate attributable to household air pollution and ambient air pollution, per 100 000 population
No indicator modifi cations required Non-MDG
Target 3.9 (as above) WaSH mortality (3.9.2)
Age-standardised death rate attributable to unsafe WaSH, per 100 000 population
No indicator modifi cations required Non-MDG
Target 3.9 (as above) Poisons (3.9.3) Age-standardised death rate due to unintentional poisonings, per 100 000 population
No indicator modifi cations required Non-MDG
(Table 1 continues on next page)
Articles
6 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
Health-related SDG indicator
Defi nition used in this analysis
Further details Inclusion in MDG or non-MDG index
(Continued from previous page)
Target 3.a: Strengthen the implementation of the World Health Organization Framework Convention on Tobacco Control in all countries, as appropriate
Smoking (3.a.1) Age-standardised prevalence of daily smoking in populations aged 10 years and older, % population aged 10 years and older
We revised this indicator to daily smoking because of data limitations regarding the systematic measurement of current smoking and to refl ect populations aged 10 years and older
Non-MDG
Goal 5: Achieve gender equality and empower all women and girls
Target 5.2: Eliminate all forms of violence against all women and girls in the public and private spheres, including traffi cking and sexual and other types of exploitation
Intimate partner violence (5.2.1)
Age-standardised prevalence of women aged 15 years and older who experienced intimate partner violence, % women aged 15 years and older
Existing datasets do not comprehensively measure the status of ever-partnered women relative to never-partnered women; therefore, the denominator was revised to all women aged 15 years and older. Data on exposure to subtypes of violence are not systematically available across geographies and over time
Non-MDG
Goal 6: Ensure availability and sustainable management of water and sanitation for all
Target 6.1: By 2030, achieve universal and equitable access to safe and aff ordable drinking water for all
Water (6.1.1) Risk-weighted prevalence of populations using unsafe or unimproved water sources, as measured by the SEV for unsafe water, %
Diff erent types of unsafe water sources have diff erent relative risks associated with poor health outcomes; thus, we revised this indicator to SEV for water, which captures the relative risk of diff erent types of unsafe water sources and then combines them into a risk-weighted prevalence on a scale of 0% (no risk in the population) to 100% (the entire population experiences maximum risk associated with unsafe water)
MDG
Target 6.2: By 2030, achieve access to adequate and equitable sanitation and hygiene for all and end open defecation, paying special attention to the needs of women and girls and those in vulnerable situations
Sanitation (6.2.1a) Risk-weighted prevalence of populations using unsafe or unimproved sanitation, as measured by the SEV for unsafe sanitation, %
We separated reporting for indicator 6.2.1 into sanitation (6.2.1a) and hygiene (6.2.1b). We had three mutually exclusive, collectively exhaustive categories for sanitation at the household level: households with piped sanitation (with a sewer connection); households with improved sanitation without a sewer connection (pit latrine, ventilated improved latrine, pit latrine with slab, or composting toilet), as defi ned by the JMP; and households without improved sanitation (fl ush toilet that is not piped to sewer or septic tank, pit latrine without a slab or open pit, bucket, hanging toilet or hanging latrine, shared facilities, or no facilities), as defi ned by the JMP
MDG
Target 6.2 (as above) Hygiene (6.2.1b) Risk-weighted prevalence of populations with unsafe hygiene (no handwashing with soap), as measured by the SEV for unsafe hygiene, %
Safe hygiene practices were defi ned as handwashing with soap and water following toilet use or contact with excreta. We separated reporting for indicator 6.2.1 into sanitation (6.2.1a) and hygiene (6.2.1b)
Non-MDG
Goal 7: Ensure access to aff ordable, reliable, sustainable, and modern energy for all
Target 7.1: By 2030, ensure universal access to aff ordable, reliable, and modern energy services
Household air pollution (7.1.2)
Risk-weighted prevalence of household air pollution, as measured by the SEV for household air pollution, %
Existing datasets do not comprehensively measure population use of clean fuels and technology for heating and lighting across geographies; thus, we revised this indicator to focus on exposure to clean (or unclean) fuels used for cooking
Non-MDG
Goal 8: Promote sustained, inclusive, and sustainable economic growth, full and productive employment, and decent work for all
Target 8.8: Protect labour rights and promote safe and secure working environments for all workers, including migrant workers, in particular women migrants, and those in precarious employment
Occupational risk burden (8.8.1)
Age-standardised all-cause DALY rate attributable to occupational risks, per 100 000 population
We revised this indicator to the DALY rate attributable to occupational risks because DALYs combine measures of mortality and non-fatal outcomes into a singular summary measure, and occupational risks represent the full range of safety hazards that could be encountered in working environment
Non-MDG
(Table 1 continues on next page)
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 7
Three broad approaches can be used to create composite measures: normative, preference weighted, and statistical. Normative approaches combine each indicator based on fi rst principles or an over-riding construct such as the contribution of each indicator to overall health. Preference-weighted approaches weight each indicator by expressed or elicited social preferences for the relative importance of diff erent indicators. Statistical approaches seek to reduce a long set of variables or indicators into common components of variance using methods such as principal component analysis or factor analysis. In this case, because the SDGs refl ect the collective vision of UN member states, we used a preference-weighted approach, assuming that each SDG target should be treated equally.
To combine indicators, we adopted methods used to construct the Human Development Index,43 which include rescaling each indicator on a scale from 0 to 100 and then combining indicators using the geometric mean. The geometric mean allows indicators with very high values to partly compensate for low values on other indicators (referred to as partial substitutability). In the methods appendix pp 312–13, we describe results from alternative index construction methods (ie, principal
component analysis; the arithmetic mean across targets referred to as complete substitutability; and the minimum value across targets referred to as zero substitutability). Quantitative targets for each of the health-related SDG indicators are not universally specifi ed. As a result, we rescaled each health-related SDG indicator on a scale from 0 to 100, with 0 being the lowest (worst) value observed and 100 being the highest (best) value observed over the time period 1990–2015. We log-transformed mortality and morbidity before rescaling. We then estimated the health-related SDG index by fi rst computing the geometric mean of each rescaled health-related SDG indicator for a given target, followed by the geometric mean of resulting values across all SDG targets. To avoid problems with indicator values close to 0, when computing indices we applied a fl oor of one to all indicators. This analytic approach weights each of the health-related SDG targets equally. In addition to the health-related SDG index, we also used the same methods to construct an index that represents 14 health-related SDG indicators that were previously MDG indicators and an index representing 19 non-MDG indicators (table 1). Uncertainty in the indicator and indices values was computed using a simulation analysis.
Health-related SDG indicator
Defi nition used in this analysis
Further details Inclusion in MDG or non-MDG index
(Continued from previous page)
Goal 11: Make cities and human settlements inclusive, safe, resilient, and sustainable
Target 11.5: By 2030, signifi cantly reduce the number of deaths and the number of people aff ected and substantially decrease the direct economic losses relative to global gross domestic product caused by disasters, including water-related disasters, with a focus on protecting the poor and people in vulnerable situations
Disaster (11.5.1; same as Indicators 1.5.1 and 13.1.2)
Age-standardised death rate due to exposure to forces of nature, per 100 000 population
Existing datasets do not comprehensively measure missing people and people aff ected by natural disasters; we revised this indicator to exposure to forces of nature and reported in age-standardised rates
Non-MDG
Target 11.6: By 2030, reduce the adverse per-capita environmental impact of cities, including by paying special attention to air quality and municipal and other waste management
Mean PM2·5 (11.6.2) Population-weighted mean levels of PM2·5, μg/m³
No indicator modifi cations required Non-MDG
Goal 13: Take urgent action to combat climate change and its impacts
Target 13.1: Strengthen resilience and adaptive capacity to climate-related hazards and natural disasters in all countries
Disaster (13.1.2; same as Indicators 1.5.1 and 11.5.1)
Age-standardised death rate due to exposure to forces of nature, per 100 000 population
Existing datasets do not comprehensively measure missing people and people aff ected by natural disasters; we revised this indicator to exposure to forces of nature and reported in age-standardised rates
Non-MDG
Goal 16: Promote peaceful and inclusive societies for sustainable development, provide access to justice for all, and build eff ective, accountable and inclusive institutions at all levels
Target 16.1: Signifi cantly reduce all forms of violence and related death rates everywhere
Violence (16.1.1) Age-standardised death rate due to interpersonal violence, per 100 000 population
Existing datasets do not comprehensively measure displacement and migratory status of victims of intentional homicide; we revised this indicator to deaths due to interpersonal violence (ie, homicide)
Non-MDG
Target 16.1 (as above) War (16.1.2) Age-standardised death rate due to collective violence and legal intervention, per 100 000 population
Existing datasets do not comprehensively measure the displacement status of deaths due to confl ict; we revised this indicator to deaths due to collective violence and legal intervention (ie, war)
Non-MDG
Detailed descriptions of the data sources and methods used to estimate each health-related SDG indicator are in the methods appendix pp 10–311. SDG=Sustainable Development Goal. MDG=Millennium Development Goal. IOTF=International Obesity Task Force. GBD=Global Burden of Disease Study. NCDs=non-communicable diseases. SEV=summary exposure value. WaSH=water, sanitation, and hygiene. JMP=Joint Monitoring Program. DALY=disability-adjusted life-year. PM2·5=fi ne particulate matter smaller than 2·5 μm.
Table 1: Health-related SDG goals and targets proposed by the Inter-Agency and Expert Group on SDG Indicators, and health-related SDG indicators used in this analysis
Articles
8 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
Relations between health-related SDG indicators and the Socio-demographic Index and healthy life expectancyAs part of GBD 2015, we assessed cause-specifi c disease burden and risk exposure along the development spectrum, providing context on expected changes as
countries progress to higher levels of income per person, higher educational attainment, and lower fertility.34,37–39 We conducted a similar analysis by examining the relations of the overall health-related SDG index and each of the individual health-related SDG indicators
Health-related SDG indicator Measurement needs and strategy
Goal 3: Ensure healthy lives and promote wellbeing for all at all ages
Target 3.5: Strengthen the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol
3.5.1: Coverage of treatment interventions (pharmacological, psychosocial and rehabilitation and aftercare services) for substance use disorders
Prevalence of specifi c substance use disorders (opioid use disorders, cocaine use disorders, amphetamine use disorders, and cannabis use disorders), as well as alcohol use disorders, are presently estimated as part of GBD. Systematic reviews on coverage of specifi c interventions (eg, opioid substitution therapy) are in progress by GBD collaborators
Target 3.8: Achieve universal health coverage, including fi nancial risk protection, access to quality essential health-care services and access to safe, eff ective, quality and aff ordable essential medicines and vaccines for all
3.8.2: Number of people covered by health insurance or a public health system per 1000 population
Omission of information on insurance depth and status of user fees within the public health system might limit the applications of this indicator. Construction of proxy measures of health-care use, for both outpatient and hospital care, by country and over time is feasible as part of future iterations of GBD and is likely to be an improved measurement strategy
Target 3.b: Support the research and development of vaccines and medicines for the communicable and non-communicable diseases that primarily aff ect developing countries, provide access to aff ordable essential medicines and vaccines, in accordance with the Doha Declaration on the TRIPS Agreement and Public Health, which affi rms the right of developing countries to use to the full the provisions in TRIPS regarding fl exibilities to protect public health, and, in particular, provide access to medicines for all
3.b.1: Proportion of the population with access to aff ordable medicines and vaccines on a sustainable basis. The recommended measure is percentage of health facilities with essential medicines and life-saving commodities in stock
Across all geographies and over time, comparable data on the stocking and stock-out rates of essential medicines and vaccines for all facility types (hospitals, primary care facilities, pharmacies, and other health-care outlets) and facility ownership (public, private, informal) are not available at present. In the absence of robust measures of stock-outs in both the public and private sectors across countries and over time, the measurement strategy for producing comparable results for this indicator is unclear. Furthermore, the proposed indicator stipulates measurement of not only access to medicines and vaccines, but also access to affordable medicines and vaccines. No comprehensive and comparable datasets on the status of essential medicine and vaccine affordability, in addition to their stocks, presently exist
Target 3.b (as above) 3.b.2: Total net offi cial development assistance to the medical research and basic health sectors
DAH is currently assessed within a comprehensive, comparable analytical framework by source, channel, recipient country, and health focus area from 1990 to 2015; however, funding specifi cally for medical research (eg, research and development of vaccines and medicines, as described in Target 3.b) is not systematically available across source and recipient countries. Additionally, the appropriate assessment of country-level performance remains unclear (eg, whether countries that receive high levels of DAH for medical research are equivalent, in terms of indicator performance, to countries that disperse high levels of DAH for medical research)
Target 3.c: Substantially increase health fi nancing and the recruitment, development, training and retention of the health workforce in developing countries, especially in least developed countries and small island developing States
3.c.1: Health worker density and distribution, as measured by number of health workers per 1000 population by cadre. Cadres include generalist medical practitioners, specialist medical practitioners (surgeons, anaesthetists, obstetricians, emergency medicine specialists, cardiologists, paediatricians, psychiatrists, ophthalmologists, gynaecologists, etc), nursing and midwifery professionals, and traditional and complementary medicine professionals, among others
A systematic analysis of population census data and Labour Force Surveys is possible as part of future iterations of GBD. The total quantity of individual health worker cadres that could be comparably assessed by geography by year will be a function of the availability of detailed International Labour Organization occupational codes across geographies and survey iteration
Target 3.d: Strengthen the capacity of all countries, in particular developing countries, for early warning, risk reduction and management of national and global health risks
3.d.1: International Health Regulations (IHR) capacity and health emergency preparedness. The WHO-recommended measure is the percentage of 13 core capacities that have been attained at a specifi c time (IHR core capacity index). The 13 core capacities are (1) national legislation, policy, and fi nancing; (2) coordination and national focal point communications; (3) surveillance; (4) response; (5) preparedness; (6) risk communication; (7) human resources; (8) laboratory; (9) points of entry; (10) zoonotic events; (11) food safety; (12) chemical events; and (13) radionuclear emergencies
Comprehensive and comparable data for all components of the IHR core capacity index, for all geographies and over time, are not available at present. Specifi c core capacities, such as zoonotic events, could be assessed as part of future iterations of GBD; other core capacities, such as coordination and national focal point communications, have no clear measurement strategy beyond self-report from country representatives or secondary research on policy status and types of surveillance systems available, among others
(Table 2 continues on next page)
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 9
with the Socio-demographic Index (SDI), a summary measure of development that uses lag-distributed income per person, average educational attainment in the population over age 15 years, and the total fertility
rate. The SDI was constructed using the same method for the Human Development Index and the health-related SDG index. Each of the three components was fi rst rescaled on a 0–1 scale, with 0 being the lowest (worst)
Health-related SDG indicator Measurement needs and strategy
(Continued from previous page)
Goal 5: Achieve gender equality and empower all women and girls
Target 5.2: Eliminate all forms of violence against all women and girls in the public and private spheres, including traffi cking and sexual and other types of exploitation
5.2.2: Proportion of women and girls aged 15 years and older subjected to sexual violence by persons other than an intimate partner in the previous 12 months, by age and place of occurrence
Prevalence of intimate partner violence among women and girls aged 15 years and older is currently estimated as part of GBD. An updated systematic review of the literature, data re-extraction, and analysis are needed to specifi cally quantify prevalence of sexual violence (separately or in addition to physical violence, or both) and by persons other than an intimate partner. Data availability by geography by year on the latter, sexual violence by persons other than intimate partners, might be limited
Target 5.6: Ensure universal access to sexual and reproductive health and reproductive rights as agreed in accordance with the Programme of Action of the International Conference on Population and Development and the Beijing Platform for Action and the outcome documents of their review conferences
5.6.1: Proportion of women aged 15–49 years who make their own informed decisions regarding sexual relations, contraceptive use, and reproductive health care
The proportion of women who make their own informed decisions regarding all three dimensions of this indicator—sexual relations, contraceptive use, and reproductive health care—are included in the Demographic and Health Survey (DHS) series. Data availablility for non-DHS countries is unclear. The feasibility of measuring this indicator as part of future iterations of GBD is under review at present
Target 5.6 (as above) 5.6.2: Number of countries with laws and regulations that guarantee women aged 15–49 access to sexual and reproductive health care, information, and education
Across all geographies and over time, comprehensive and comparable data documenting the status of laws and regulations regarding access to sexual and reproductive health care, information, and education do not exist at present. Compiling the past and current status of such laws and regulations might be possible; however, systematic assessment of their depth or intensity, enforcement, and eff ectiveness in guaranteeing access to reproductive health care, information, and education might be challenging across countries and over time
Goal 6: Ensure availability and sustainable management of water and sanitation for all
Target 6.3: By 2030, improve water quality by reducing pollution, eliminating dumping and minimising release of hazardous chemicals and materials, halving the proportion of untreated waste water, and substantially increasing recycling and safe reuse globally
6.3.1: Proportion of waste water safely treated. UN Water defi nes this indicator as the proportion of waste water generated by both households (sewage and faecal sludge), as well as economic activities (based on ISIC categories) safely treated compared to total waste water generated both through households and economic activities. While the defi nition conceptually includes waste water generated from all economic activities, monitoring will focus on waste water generated from hazardous industries (as defi ned by relevant ISIC categories)
Across all geographies and over time, comprehensive and comparable data containing information on total waste water, as generated by both households and non-household entities (however they are to be defi ned), and waste water treatment status do not exist at present. UN Water suggests there will be suffi cient data to generate estimates of global and regional levels of safely treated waste water by 2018; however, in the absence of more country-level data, it is diffi cult to determine the representativeness of such global and regional estimates
Goal 16: Promote peaceful and inclusive societies for sustainable development, provide access to justice for all and build eff ective, accountable, and inclusive institutions at all levels
Target 16.1: Signifi cantly reduce all forms of violence and related death rates everywhere
16.1.3: Proportion of population subjected to physical, psychological, or sexual violence in the previous 12 months
Prevalence of intimate partner violence among women and girls aged 15 years and older is currently estimated as part of GBD, as are the incidence and prevalence of interpersonal violence among all populations. An expanded systematic review of the literature and available data sources for all types of violence (physical, psychological, and sexual) for both men and women of all ages would be required for inclusion in future iterations of GBD
Target 16.1 (as above) 16.1.4: Proportion of people that feel safe walking alone around the area they live
Comprehensive data on reported safety, in general or walking alone near one’s residence (or both), do not currently exist across geographies or over time. Substantive primary data collection is likely to be required
Target 16.2: End abuse, exploitations, traffi cking and all forms of violence against and torture of children
16.2.3: Proportion of young women and men aged 18–29 years who experienced sexual violence by age 18
Prevalence of intimate partner violence among women and girls aged 15 years and older is estimated as part of GBD. An expanded systematic review and analysis of the literature and available data sources for both men and women, and for all types of sexual violence (ie, not limited to intimate partners) would be required. The feasibility of measuring this indicator as part of future iterations of GBD is under review at present
(Table 2 continues on next page)
Articles
10 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
value observed in the time period 1980–2015 and 1 being the highest (best) value observed. SDI was then computed as the geometric mean of these three rescaled components. To capture average relations, we used a spline regression (ie, piecewise linear regression with so-called knots specifying the intersection between pieces) of the health-related SDG indicators and health-related SDG index on SDI using the full set of data by country from 1990 to 2015. We also compared the health-related SDG indicators with the GBD 2015 estimates of healthy life expectancy38 to explore the relation between the SDGs and overall health achievement for each country.
Role of the funding sourceThe funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had fi nal responsibility for the decision to submit for publication.
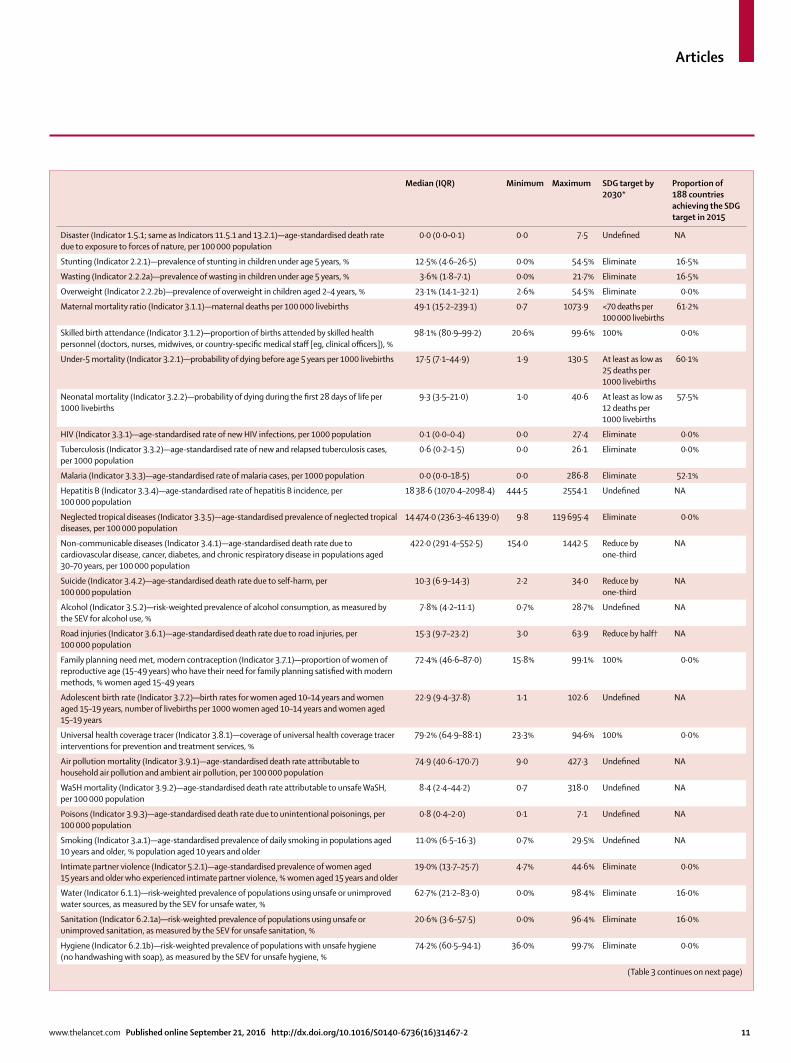
ResultsOf the 33 health-related SDG indicators, 21 were associated with a defi ned target, with 18 of them having an absolute level and three having a target relative to 2015 levels (table 3). The proportion of countries already meeting targets linked to health-related SDG indicators in 2015, as specifi ed by absolute levels to be achieved, ranged from more than 60% for two indicators (maternal mortality ratio and under-5 mortality) to 0% for nine indicators. For these nine indicators, all targets involved full elimination of diseases (eg, tuberculosis, HIV, and neglected tropical diseases), reducing prevalence of health outcomes or risk to 0% (eg, childhood overweight and intimate partner violence), or reaching 100% for intervention coverage or health service provision (eg, skilled birth attendance, met need with modern contraception, and UHC tracer interventions).
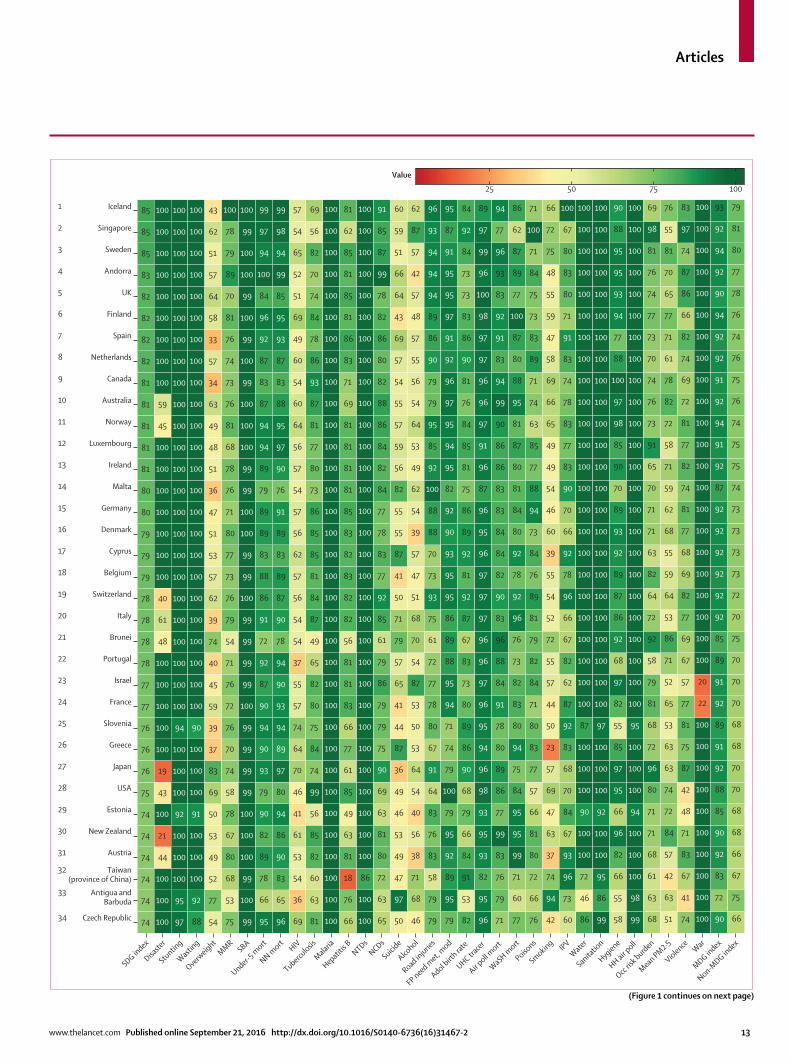
In 2015, the median health-related SDG index was 59∙3 (95% uncertainty interval [UI] 56∙8–61∙8) across all 188 countries. This index was highest in Iceland (85∙5, 84∙2–86∙5), Singapore (85∙3, 84∙1–86∙3), and Sweden (85∙3, 84∙2–86∙2) and lowest in the Central African Republic (20∙4, 15∙9–24∙9), Somalia (21∙6, 16∙0–25∙9), and South Sudan (22∙5, 15∙5–26∙6; fi gure 1). Diff erences in the 95% UI range stem largely from diff erences in the availability and quality of underlying data sources for estimating individual indicators; for example, data were sparser for Somalia than they were for Sweden. Some patterns emerged contrary to what might have been expected. For example, the USA (74∙9, 73∙6–75∙9) ranked 28th, driven by poorer performance on MDG indicators (eg, maternal mortality ratio) than other high-income countries44 and worse performance on non-MDG indicators—most notably, alcohol consumption, childhood overweight, and mortality due to interpersonal violence, self-harm, and unintentional poisoning. India (41∙7, 39∙7–43∙7), despite rapid economic growth, was ranked 143rd, just below Comoros and Ghana.
Levels of the health-related SDG index were highly clustered (fi gure 2), with countries in the highest quintile (≥71·5) located mainly in western Europe, high-income North America, parts of Asia (Japan, South Korea, Singapore, and Brunei), and Australasia. The second highest quintile (62·5–71·5) included countries in southern Latin America, parts of eastern Europe, most of the Caribbean, and a subset of countries across other regions (eg, Mexico, Jordan, Azerbaijan, Malaysia, and Costa Rica), whereas countries in the middle quintile (55·7–62·5) were primarily located in South America; parts of east, central, and southeast Asia; and parts of North Africa and the Middle East. The countries in the fourth quintile (37·8–55·7) were mainly found in south and southeast Asia, southern sub-Saharan Africa, parts of
Health-related SDG indicator Measurement needs and strategy
(Continued from previous page)
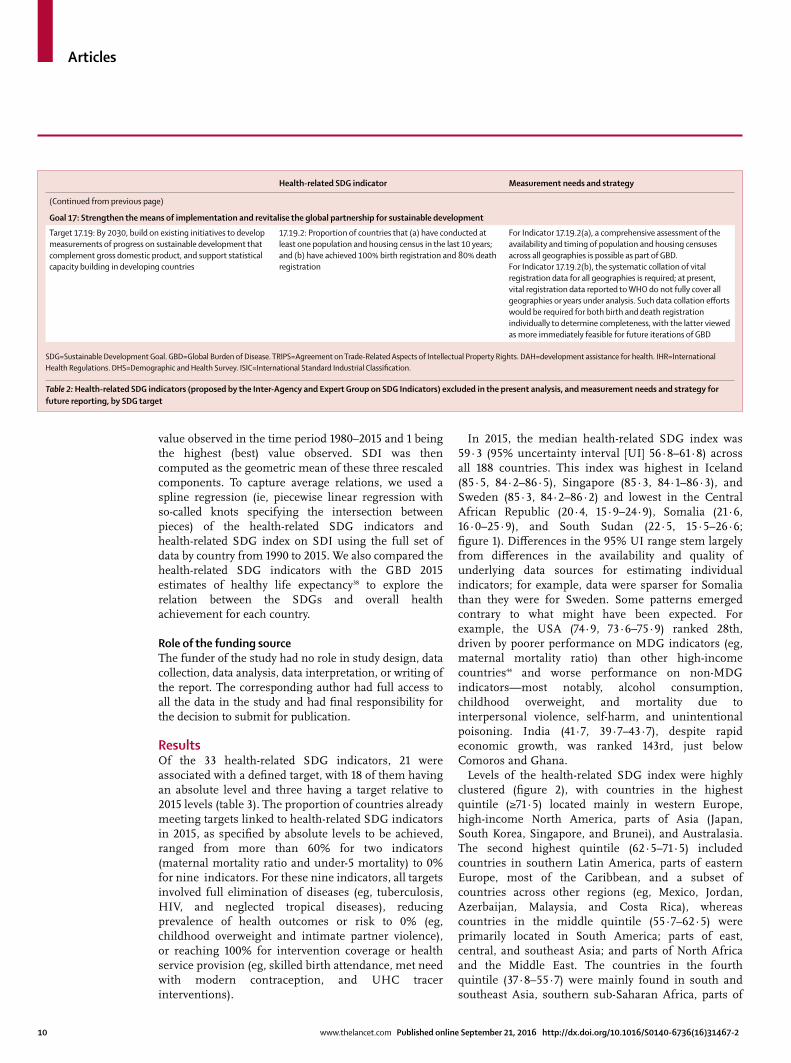
Goal 17: Strengthen the means of implementation and revitalise the global partnership for sustainable development
Target 17.19: By 2030, build on existing initiatives to develop measurements of progress on sustainable development that complement gross domestic product, and support statistical capacity building in developing countries
17.19.2: Proportion of countries that (a) have conducted at least one population and housing census in the last 10 years; and (b) have achieved 100% birth registration and 80% death registration
For Indicator 17.19.2(a), a comprehensive assessment of the availability and timing of population and housing censuses across all geographies is possible as part of GBD. For Indicator 17.19.2(b), the systematic collation of vital registration data for all geographies is required; at present, vital registration data reported to WHO do not fully cover all geographies or years under analysis. Such data collation eff orts would be required for both birth and death registration individually to determine completeness, with the latter viewed as more immediately feasible for future iterations of GBD
SDG=Sustainable Development Goal. GBD=Global Burden of Disease. TRIPS=Agreement on Trade-Related Aspects of Intellectual Property Rights. DAH=development assistance for health. IHR=International Health Regulations. DHS=Demographic and Health Survey. ISIC=International Standard Industrial Classifi cation.
Table 2: Health-related SDG indicators (proposed by the Inter-Agency and Expert Group on SDG Indicators) excluded in the present analysis, and measurement needs and strategy for future reporting, by SDG target
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 11
Median (IQR) Minimum Maximum SDG target by 2030*
Proportion of 188 countries achieving the SDG target in 2015
Disaster (Indicator 1.5.1; same as Indicators 11.5.1 and 13.2.1)—age-standardised death rate due to exposure to forces of nature, per 100 000 population
0·0 (0·0–0·1) 0·0 7·5 Undefi ned NA
Stunting (Indicator 2.2.1)—prevalence of stunting in children under age 5 years, % 12·5% (4·6–26·5) 0·0% 54·5% Eliminate 16·5%
Wasting (Indicator 2.2.2a)—prevalence of wasting in children under age 5 years, % 3·6% (1·8–7·1) 0·0% 21·7% Eliminate 16·5%
Overweight (Indicator 2.2.2b)—prevalence of overweight in children aged 2–4 years, % 23·1% (14·1–32·1) 2·6% 54·5% Eliminate 0·0%
Maternal mortality ratio (Indicator 3.1.1)—maternal deaths per 100 000 livebirths 49·1 (15·2–239·1) 0·7 1073·9 <70 deaths per 100 000 livebirths
61·2%
Skilled birth attendance (Indicator 3.1.2)—proportion of births attended by skilled health personnel (doctors, nurses, midwives, or country-specifi c medical staff [eg, clinical offi cers]), %
98·1% (80·9–99·2) 20·6% 99·6% 100% 0·0%
Under-5 mortality (Indicator 3.2.1)—probability of dying before age 5 years per 1000 livebirths 17·5 (7·1–44·9) 1·9 130·5 At least as low as 25 deaths per 1000 livebirths
60·1%
Neonatal mortality (Indicator 3.2.2)—probability of dying during the fi rst 28 days of life per 1000 livebirths
9·3 (3·5–21·0) 1·0 40·6 At least as low as 12 deaths per 1000 livebirths
57·5%
HIV (Indicator 3.3.1)—age-standardised rate of new HIV infections, per 1000 population 0·1 (0·0–0·4) 0·0 27·4 Eliminate 0·0%
Tuberculosis (Indicator 3.3.2)—age-standardised rate of new and relapsed tuberculosis cases, per 1000 population
0·6 (0·2–1·5) 0·0 26·1 Eliminate 0·0%
Malaria (Indicator 3.3.3)—age-standardised rate of malaria cases, per 1000 population 0·0 (0·0–18·5) 0·0 286·8 Eliminate 52·1%
Hepatitis B (Indicator 3.3.4)—age-standardised rate of hepatitis B incidence, per 100 000 population
18 38·6 (1070·4–2098·4) 444·5 2554·1 Undefi ned NA
Neglected tropical diseases (Indicator 3.3.5)—age-standardised prevalence of neglected tropical diseases, per 100 000 population
14 474·0 (236·3–46 139·0) 9·8 119 695·4 Eliminate 0·0%
Non-communicable diseases (Indicator 3.4.1)—age-standardised death rate due to cardiovascular disease, cancer, diabetes, and chronic respiratory disease in populations aged 30–70 years, per 100 000 population
422·0 (291·4–552·5) 154·0 1442·5 Reduce by one-third
NA
Suicide (Indicator 3.4.2)—age-standardised death rate due to self-harm, per 100 000 population
10·3 (6·9–14·3) 2·2 34·0 Reduce by one-third
NA
Alcohol (Indicator 3.5.2)—risk-weighted prevalence of alcohol consumption, as measured by the SEV for alcohol use, %
7·8% (4·2–11·1) 0·7% 28·7% Undefi ned NA
Road injuries (Indicator 3.6.1)—age-standardised death rate due to road injuries, per 100 000 population
15·3 (9·7–23·2) 3·0 63·9 Reduce by half† NA
Family planning need met, modern contraception (Indicator 3.7.1)—proportion of women of reproductive age (15–49 years) who have their need for family planning satisfi ed with modern methods, % women aged 15–49 years
72·4% (46·6–87·0) 15·8% 99·1% 100% 0·0%
Adolescent birth rate (Indicator 3.7.2)—birth rates for women aged 10–14 years and women aged 15–19 years, number of livebirths per 1000 women aged 10–14 years and women aged 15–19 years
22·9 (9·4–37·8) 1·1 102·6 Undefi ned NA
Universal health coverage tracer (Indicator 3.8.1)—coverage of universal health coverage tracer interventions for prevention and treatment services, %
79·2% (64·9–88·1) 23·3% 94·6% 100% 0·0%
Air pollution mortality (Indicator 3.9.1)—age-standardised death rate attributable to household air pollution and ambient air pollution, per 100 000 population
74·9 (40·6–170·7) 9·0 427·3 Undefi ned NA
WaSH mortality (Indicator 3.9.2)—age-standardised death rate attributable to unsafe WaSH, per 100 000 population
8·4 (2·4–44·2) 0·7 318·0 Undefi ned NA
Poisons (Indicator 3.9.3)—age-standardised death rate due to unintentional poisonings, per 100 000 population
0·8 (0·4–2·0) 0·1 7·1 Undefi ned NA
Smoking (Indicator 3.a.1)—age-standardised prevalence of daily smoking in populations aged 10 years and older, % population aged 10 years and older
11·0% (6·5–16·3) 0·7% 29·5% Undefi ned NA
Intimate partner violence (Indicator 5.2.1)—age-standardised prevalence of women aged 15 years and older who experienced intimate partner violence, % women aged 15 years and older
19·0% (13·7–25·7) 4·7% 44·6% Eliminate 0·0%
Water (Indicator 6.1.1)—risk-weighted prevalence of populations using unsafe or unimproved water sources, as measured by the SEV for unsafe water, %
62·7% (21·2–83·0) 0·0% 98·4% Eliminate 16·0%
Sanitation (Indicator 6.2.1a)—risk-weighted prevalence of populations using unsafe or unimproved sanitation, as measured by the SEV for unsafe sanitation, %
20·6% (3·6–57·5) 0·0% 96·4% Eliminate 16·0%
Hygiene (Indicator 6.2.1b)—risk-weighted prevalence of populations with unsafe hygiene (no handwashing with soap), as measured by the SEV for unsafe hygiene, %
74·2% (60·5–94·1) 36·0% 99·7% Eliminate 0·0%
(Table 3 continues on next page)
Articles
12 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
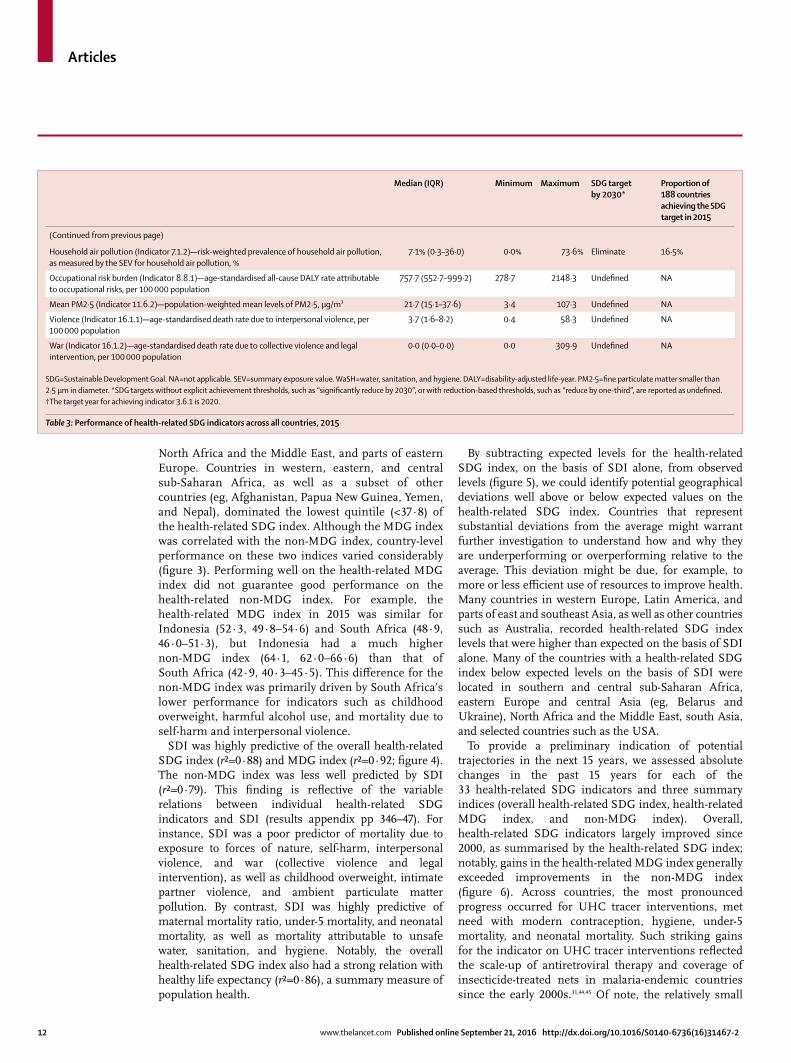
North Africa and the Middle East, and parts of eastern Europe. Countries in western, eastern, and central sub-Saharan Africa, as well as a subset of other countries (eg, Afghanistan, Papua New Guinea, Yemen, and Nepal), dominated the lowest quintile (<37·8) of the health-related SDG index. Although the MDG index was correlated with the non-MDG index, country-level performance on these two indices varied considerably (fi gure 3). Performing well on the health-related MDG index did not guarantee good performance on the health-related non-MDG index. For example, the health-related MDG index in 2015 was similar for Indonesia (52∙3, 49∙8–54∙6) and South Africa (48∙9, 46∙0–51∙3), but Indonesia had a much higher non-MDG index (64∙1, 62∙0–66∙6) than that of South Africa (42∙9, 40∙3–45∙5). This diff erence for the non-MDG index was primarily driven by South Africa’s lower performance for indicators such as childhood overweight, harmful alcohol use, and mortality due to self-harm and interpersonal violence.
SDI was highly predictive of the overall health-related SDG index (r²=0∙88) and MDG index (r²=0∙92; fi gure 4). The non-MDG index was less well predicted by SDI (r²=0∙79). This fi nding is refl ective of the variable relations between individual health-related SDG indicators and SDI (results appendix pp 346–47). For instance, SDI was a poor predictor of mortality due to exposure to forces of nature, self-harm, interpersonal violence, and war (collective violence and legal intervention), as well as childhood overweight, intimate partner violence, and ambient particulate matter pollution. By contrast, SDI was highly predictive of maternal mortality ratio, under-5 mortality, and neonatal mortality, as well as mortality attributable to unsafe water, sanitation, and hygiene. Notably, the overall health-related SDG index also had a strong relation with healthy life expectancy (r²=0∙86), a summary measure of population health.
By subtracting expected levels for the health-related SDG index, on the basis of SDI alone, from observed levels (fi gure 5), we could identify potential geographical deviations well above or below expected values on the health-related SDG index. Countries that represent substantial deviations from the average might warrant further investigation to understand how and why they are underperforming or overperforming relative to the average. This deviation might be due, for example, to more or less effi cient use of resources to improve health. Many countries in western Europe, Latin America, and parts of east and southeast Asia, as well as other countries such as Australia, recorded health-related SDG index levels that were higher than expected on the basis of SDI alone. Many of the countries with a health-related SDG index below expected levels on the basis of SDI were located in southern and central sub-Saharan Africa, eastern Europe and central Asia (eg, Belarus and Ukraine), North Africa and the Middle East, south Asia, and selected countries such as the USA.
To provide a preliminary indication of potential trajectories in the next 15 years, we assessed absolute changes in the past 15 years for each of the 33 health-related SDG indicators and three summary indices (overall health-related SDG index, health-related MDG index, and non-MDG index). Overall, health-related SDG indicators largely improved since 2000, as summarised by the health-related SDG index; notably, gains in the health-related MDG index generally exceeded improvements in the non-MDG index (fi gure 6). Across countries, the most pronounced progress occurred for UHC tracer interventions, met need with modern contraception, hygiene, under-5 mortality, and neonatal mortality. Such striking gains for the indicator on UHC tracer interventions refl ected the scale-up of antiretroviral therapy and coverage of insecticide-treated nets in malaria-endemic countries since the early 2000s.31,44,45 Of note, the relatively small
Median (IQR) Minimum Maximum SDG target by 2030*
Proportion of 188 countries achieving the SDG target in 2015
(Continued from previous page)
Household air pollution (Indicator 7.1.2)—risk-weighted prevalence of household air pollution, as measured by the SEV for household air pollution, %
7·1% (0·3–36·0) 0·0% 73·6% Eliminate 16·5%
Occupational risk burden (Indicator 8.8.1)—age-standardised all-cause DALY rate attributable to occupational risks, per 100 000 population
757·7 (552·7–999·2) 278·7 2148·3 Undefi ned NA
Mean PM2·5 (Indicator 11.6.2)—population-weighted mean levels of PM2·5, μg/m³ 21·7 (15·1–37·6) 3·4 107·3 Undefi ned NA
Violence (Indicator 16.1.1)—age-standardised death rate due to interpersonal violence, per 100 000 population
3·7 (1·6–8·2) 0·4 58·3 Undefi ned NA
War (Indicator 16.1.2)—age-standardised death rate due to collective violence and legal intervention, per 100 000 population
0·0 (0·0–0·0) 0·0 309·9 Undefi ned NA
SDG=Sustainable Development Goal. NA=not applicable. SEV=summary exposure value. WaSH=water, sanitation, and hygiene. DALY=disability-adjusted life-year. PM2·5=fi ne particulate matter smaller than 2·5 μm in diameter. *SDG targets without explicit achievement thresholds, such as “signifi cantly reduce by 2030”, or with reduction-based thresholds, such as “reduce by one-third”, are reported as undefi ned. †The target year for achieving indicator 3.6.1 is 2020.
Table 3: Performance of health-related SDG indicators across all countries, 2015
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 13
Under-5 m
ort
74
74
74
74
74
74
75
76
76
76
77
77
78
78
78
78
79
79
79
80
80
81
81
81
81
81
82
82
82
82
83
85
85
85
100
100
100
44
21
100
43
19
100
100
100
100
100
48
61
40
100
100
100
100
100
100
100
45
59
100
100
100
100
100
100
100
100
100
97
95
100
100
100
92
100
100
100
94
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
88
92
100
100
100
91
100
100
100
90
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
54
77
52
49
53
50
69
83
37
39
59
45
40
74
39
62
57
53
51
47
36
51
48
49
63
34
57
33
58
64
57
51
62
43
75
53
68
80
67
78
58
74
70
76
72
76
71
54
79
76
73
77
80
71
76
78
68
81
76
73
74
76
81
70
89
79
78
100
99
100
99
100
100
100
99
99
99
99
100
99
99
99
99
100
99
99
100
100
99
99
100
100
100
99
100
99
100
99
100
100
99
100
95
66
78
89
82
90
79
93
90
94
90
87
92
72
91
86
88
83
89
89
79
89
94
94
87
83
87
92
96
84
100
94
97
99
96
65
83
90
86
94
80
97
89
94
93
90
94
78
90
87
89
83
89
91
76
90
97
95
88
83
87
93
95
85
99
94
98
99
69
36
54
53
61
41
46
70
64
74
57
55
37
54
54
56
57
62
56
57
54
57
56
64
60
54
60
49
69
51
52
65
54
57
81
63
60
82
85
56
99
74
84
75
80
82
65
49
87
84
81
85
85
86
73
80
77
81
87
93
86
78
84
74
70
82
56
69
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
66
76
18
81
63
49
85
61
77
66
83
81
81
56
82
82
83
82
83
85
81
81
81
81
69
71
83
86
81
85
81
85
62
81
100
100
86
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
65
63
72
80
81
63
69
90
75
79
79
86
79
61
85
92
77
83
78
77
84
82
84
86
88
82
80
86
82
78
99
87
85
91
50
97
47
49
53
46
49
36
87
44
41
65
57
79
71
50
41
87
55
55
82
56
59
57
55
54
57
69
43
64
66
51
59
60
46
68
71
38
56
40
54
64
53
50
53
87
54
70
68
51
47
57
39
54
62
49
53
64
54
56
55
57
48
57
42
57
87
62
79
79
58
83
76
83
64
91
67
80
78
77
72
61
75
93
73
70
88
88
100
92
85
95
79
79
90
86
89
94
94
94
93
96
79
95
89
92
95
79
100
79
74
71
94
95
88
89
86
95
95
93
90
92
82
95
94
95
97
96
92
91
97
95
95
91
87
95
82
53
91
84
66
79
68
90
86
89
80
73
83
67
87
92
81
92
89
86
75
81
85
84
76
81
90
86
83
73
73
84
92
84
96
95
82
93
95
93
98
96
94
95
96
97
96
96
97
97
97
96
95
96
87
96
91
97
96
96
97
97
98
100
96
99
97
89
71
79
76
83
99
77
86
89
80
78
91
84
88
96
83
90
82
84
84
83
83
86
86
90
99
94
83
91
92
83
93
96
77
94
77
60
71
99
95
95
84
75
94
80
83
82
73
76
96
92
78
92
80
84
81
80
87
81
95
88
80
87
100
77
89
87
62
86
76
66
72
80
81
66
57
77
83
80
71
84
82
79
81
89
76
84
73
94
88
77
85
63
74
71
89
83
73
75
84
71
100
71
42
94
74
37
63
47
69
57
23
50
44
57
55
72
52
54
55
39
60
46
54
49
49
65
66
69
58
47
59
55
48
75
72
66
60
73
96
93
67
84
70
68
83
92
87
62
82
67
66
96
78
92
66
70
90
83
77
83
78
74
83
91
71
80
83
80
67
100
86
46
72
100
100
90
100
100
100
87
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
99
86
95
100
100
92
100
100
100
97
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
58
55
66
82
96
66
95
97
85
55
82
97
68
92
86
87
89
92
93
89
70
90
85
98
97
100
88
77
94
93
95
95
88
90
99
98
100
100
100
94
100
100
100
95
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
68
63
61
68
71
71
80
96
72
68
81
79
58
92
72
64
82
63
71
71
70
65
91
73
76
74
70
73
77
74
76
81
98
69
51
63
42
57
84
72
74
63
63
53
65
52
71
86
53
64
59
55
68
62
59
71
58
72
82
78
61
71
77
65
70
81
55
76
74
41
67
83
71
48
42
87
75
81
77
57
67
69
77
82
69
68
77
81
74
82
77
81
72
69
74
82
66
86
87
74
97
83
100
100
100
100
100
100
100
100
100
100
22
20
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
90
72
83
92
90
85
88
92
91
89
92
91
89
85
92
92
92
92
92
92
87
92
91
94
92
91
92
92
94
90
92
94
92
93
66
75
67
66
68
68
70
70
68
68
70
70
70
75
70
72
73
73
73
73
74
75
75
74
76
75
76
74
76
78
77
80
81
791 Iceland
2 Singapore
3 Sweden
4 Andorra
5 UK
6 Finland
7 Spain
8 Netherlands
9 Canada
10 Australia
11 Norway
12 Luxembourg
13 Ireland
14 Malta
15 Germany
16 Denmark
17 Cyprus
18 Belgium
19 Switzerland
20 Italy
21 Brunei
22 Portugal
23 Israel
24 France
25 Slovenia
26 Greece
27 Japan
28 USA
29 Estonia
30 New Zealand
31 Austria
32 Taiwan(province of China)
33 Antigua andBarbuda
34 Czech Republic
SDG index
Disaste
r
Stunting
Wasting
Overweight
MMRSBA
NN mort HIV
Tuberculosis
Malaria
Hepatitis B NTDs
NCDs
Suicide
Alcohol
Road injurie
s
FP need met, m
od
Adol birt
h rate
UHC tracer
Air poll m
ort
WaSH mort
Poisons
Smoking IPVWater
Sanitatio
n
Hygiene
HH air poll
Occ ris
k burden
Mean PM2·5
Violence War
MDG index
Non-MDG in
dex
100755025
Value
(Figure 1 continues on next page)
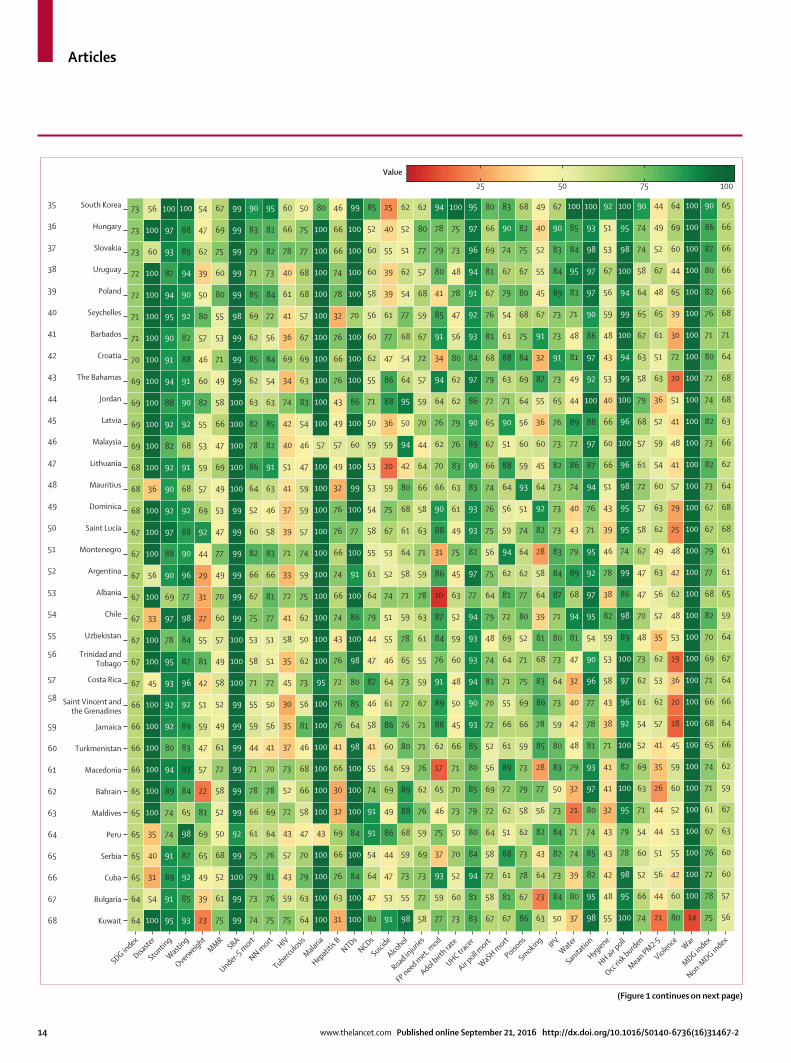
Articles
14 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
100755025
Value
SDG index
Disaste
r
Stunting
Wasting
Overweight
MMRSBA
Under-5 m
ort
NN mort HIV
Tuberculosis
Malaria
Hepatitis B NTDs
NCDs
Suicide
Alcohol
Road injurie
s
FP need met, m
od
Adol birt
h rate
UHC tracer
Air poll m
ort
WaSH mort
Poisons
Smoking IPVWater
Sanitatio
n
Hygiene
HH air poll
Occ ris
k burden
Mean PM2·5
Violence War
MDG index
Non-MDG in
dex
64
64
65
65
65
65
65
66
66
66
66
67
67
67
67
67
67
67
67
68
68
68
69
69
69
69
70
71
71
72
72
73
73
73
100
54
31
40
35
100
100
100
100
100
100
45
100
100
33
100
56
100
100
100
36
100
100
100
100
100
100
100
100
100
100
60
100
56
95
91
89
91
74
74
89
94
80
92
92
93
95
78
97
69
90
88
97
92
90
92
82
92
88
94
91
90
95
94
87
93
97
100
93
85
92
87
98
65
84
93
83
89
92
96
87
84
98
77
96
90
88
92
68
91
68
92
90
91
88
82
92
90
94
89
88
100
23
39
49
65
69
81
22
57
47
59
51
42
81
55
27
31
29
44
92
69
57
59
53
55
82
60
46
57
80
50
39
62
47
54
75
61
52
68
50
52
58
72
61
49
52
58
49
57
60
70
49
77
47
53
49
69
47
66
58
49
71
53
55
80
60
75
69
67
99
99
100
99
92
99
99
99
99
99
99
100
100
100
99
99
99
99
99
99
100
100
100
100
100
99
99
99
98
99
99
99
99
99
74
73
79
75
61
66
78
71
44
59
55
71
58
53
75
67
66
82
60
52
64
86
78
82
63
62
85
62
69
85
71
79
83
90
75
76
81
76
64
69
78
70
41
56
50
72
51
51
77
81
66
83
58
46
63
91
82
85
63
54
84
56
72
84
73
82
82
95
75
59
43
57
43
72
52
73
37
35
30
45
35
58
41
72
33
71
39
37
41
51
40
42
74
34
69
36
41
61
40
78
66
60
64
63
79
70
47
58
66
68
46
81
56
73
62
50
62
75
59
74
57
59
59
47
46
54
83
63
69
67
57
68
68
77
75
50
100
100
100
100
43
100
100
100
100
100
100
95
100
100
100
100
100
100
100
100
100
100
57
100
100
100
100
100
100
100
100
100
100
80
31
63
76
66
69
32
30
66
41
76
76
72
76
43
74
66
74
66
76
76
32
49
57
49
43
76
66
76
32
78
74
66
66
46
100
100
84
100
84
100
100
100
98
64
85
80
98
100
86
100
91
100
77
100
99
100
60
100
86
100
100
100
70
100
100
100
100
99
80
47
64
54
91
91
74
55
41
58
46
87
47
44
79
64
61
55
58
54
53
53
59
50
71
55
62
60
56
58
60
60
52
85
91
53
47
44
86
49
69
64
60
86
61
64
46
55
51
74
52
53
67
75
59
20
59
36
88
86
47
77
61
39
39
55
40
25
98
55
73
59
68
88
89
59
80
76
72
73
65
78
59
71
58
64
61
68
80
42
94
50
95
64
54
68
77
54
62
51
52
62
58
72
73
69
59
76
62
76
71
71
67
59
55
61
63
78
59
71
63
58
66
64
44
70
59
57
72
67
59
68
57
77
80
62
77
59
93
37
75
46
65
17
62
88
89
91
76
84
87
10
86
31
88
90
66
70
62
76
64
94
34
91
85
41
80
79
78
94
73
60
52
70
50
73
70
71
66
45
50
48
60
59
52
63
45
75
49
61
63
83
76
79
62
62
80
56
47
78
48
73
75
100
83
81
94
84
80
79
85
80
85
93
90
94
93
93
94
77
97
82
93
93
83
90
89
90
86
97
84
93
92
91
94
96
97
95
67
58
72
58
64
72
69
56
52
72
70
81
74
48
79
64
75
56
75
76
74
66
67
65
72
79
68
81
76
67
81
69
66
80
67
81
61
88
51
62
72
89
61
66
55
71
64
69
72
81
62
94
59
56
64
88
51
90
71
63
88
61
54
79
67
74
90
83
86
67
78
73
62
58
79
73
59
66
69
75
71
52
80
77
62
64
74
51
93
59
60
56
64
69
84
75
68
80
67
75
82
68
63
23
64
43
82
56
77
28
85
78
86
83
68
81
39
64
58
28
82
92
64
45
60
36
55
87
32
91
67
45
55
52
40
49
50
84
73
82
84
73
50
83
80
59
73
64
73
80
71
87
84
83
73
73
73
82
73
76
65
73
91
73
73
89
84
83
90
67
37
80
39
74
71
21
32
79
48
42
40
32
47
81
94
68
89
79
43
40
74
86
72
89
44
49
81
48
71
83
95
84
85
100
98
95
82
85
74
80
97
93
81
78
77
96
90
54
95
97
92
95
71
76
94
87
97
88
100
92
97
86
90
97
97
98
93
100
55
48
42
43
43
32
41
41
71
38
43
58
53
59
82
38
78
46
39
43
51
66
60
66
40
53
43
48
59
56
67
53
51
92
100
95
98
78
79
95
100
82
100
92
96
97
100
89
98
86
99
74
95
95
98
96
100
96
100
99
94
100
99
94
100
98
95
100
74
66
52
60
54
71
63
69
52
54
61
62
73
48
70
47
47
67
58
57
72
61
57
68
79
58
63
67
65
64
58
74
74
90
21
44
56
51
44
44
26
35
41
57
62
53
62
35
52
56
63
49
62
63
60
54
59
52
36
63
51
61
65
48
67
52
49
44
80
60
42
55
53
52
60
59
45
18
20
36
19
53
48
62
42
48
25
29
57
41
48
41
51
20
72
30
39
65
44
60
69
64
14
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
75
78
72
76
67
61
71
74
65
68
66
71
69
70
82
68
77
79
67
67
73
82
73
82
74
72
80
71
76
82
80
87
86
90
56
57
60
60
63
67
59
62
66
64
66
64
67
64
59
65
61
61
68
68
64
62
66
63
68
68
64
71
68
66
66
66
66
6535 South Korea
36 Hungary
37 Slovakia
38 Uruguay
39 Poland
40 Seychelles
41 Barbados
42 Croatia
43 The Bahamas
44 Jordan
45 Latvia
46 Malaysia
47 Lithuania
48 Mauritius
49 Dominica
50 Saint Lucia
51 Montenegro
52 Argentina
53 Albania
54 Chile
55 Uzbekistan
56 Trinidad andTobago
57 Costa Rica
58 Saint Vincent andthe Grenadines
59 Jamaica
60 Turkmenistan
61 Macedonia
62 Bahrain
63 Maldives
64 Peru
65 Serbia
66 Cuba
67 Bulgaria
68 Kuwait
(Figure 1 continues on next page)
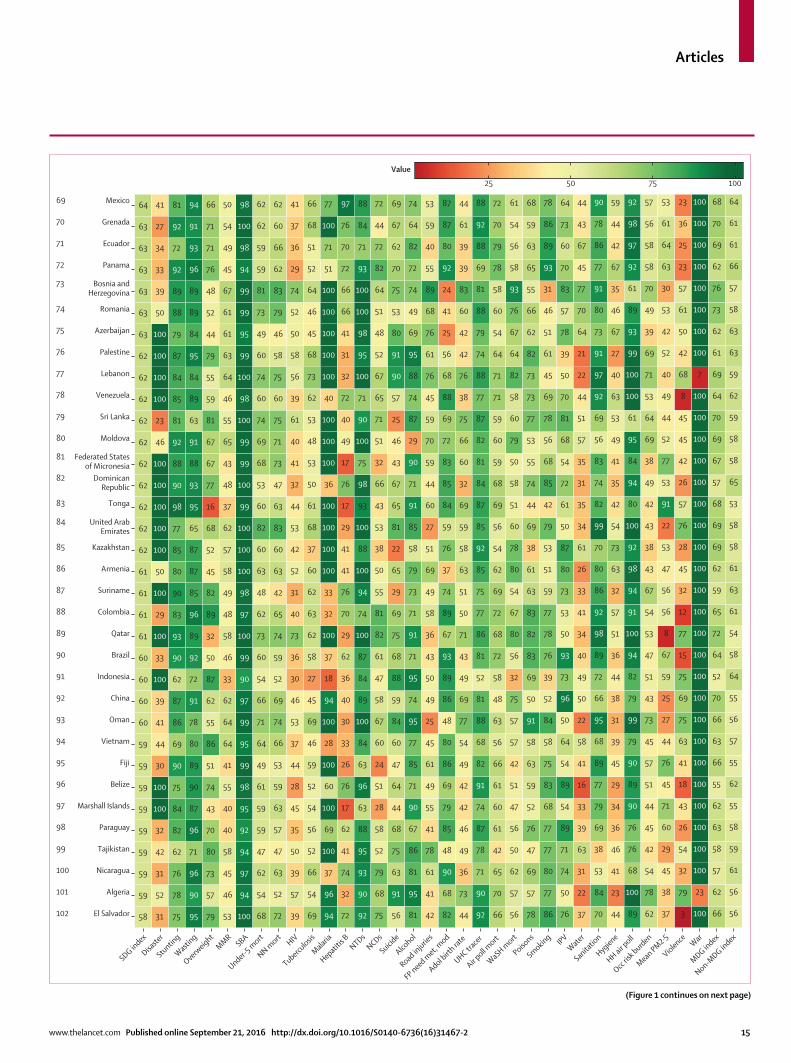
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 15
100755025
Value
SDG index
Disaste
r
Stunting
Wasting
Overweight
MMRSBA
Under-5 m
ort
NN mort HIV
Tuberculosis
Malaria
Hepatitis B NTDs
NCDs
Suicide
Alcohol
Road injurie
s
FP need met, m
od
Adol birt
h rate
UHC tracer
Air poll m
ort
WaSH mort
Poisons
Smoking IPVWater
Sanitatio
n
Hygiene
HH air poll
Occ ris
k burden
Mean PM2·5
Violence War
MDG index
Non-MDG in
dex
58
59
59
59
59
59
59
59
59
60
60
60
60
61
61
61
61
62
62
62
62
62
62
62
62
62
62
63
63
63
63
63
63
64
31
52
31
42
32
100
100
30
44
41
39
100
33
100
29
100
50
100
100
100
100
100
46
23
100
100
100
100
50
39
33
34
27
41
75
78
76
62
82
84
75
90
69
86
87
62
90
93
83
90
80
85
77
98
90
88
92
81
85
84
87
79
88
89
92
72
92
81
95
90
96
71
96
87
90
89
80
78
91
72
92
89
96
85
87
87
65
95
93
88
91
63
89
84
95
84
89
89
96
93
91
94
79
57
73
80
70
43
74
51
86
55
62
87
50
32
89
82
45
52
68
16
77
67
67
81
59
55
79
44
52
48
76
71
71
66
53
46
45
58
40
40
55
41
64
64
62
33
46
58
48
49
58
57
62
37
48
43
65
55
46
64
63
61
61
67
45
49
54
50
100
94
97
94
92
95
98
99
95
99
97
90
99
100
97
98
100
100
100
99
100
99
99
100
98
100
99
95
99
99
94
98
100
98
68
54
62
47
59
59
61
49
64
71
66
54
60
73
62
48
63
60
82
60
53
68
69
74
60
74
60
49
73
81
59
59
62
62
72
52
63
47
57
63
59
53
66
74
69
52
59
74
65
42
63
60
83
63
47
73
71
75
60
75
58
46
79
83
62
66
60
62
39
57
39
50
35
45
28
44
37
53
46
30
36
73
40
31
52
42
53
44
32
41
40
61
39
56
58
50
52
74
29
36
37
41
69
54
66
52
56
54
52
59
46
69
45
27
58
62
63
62
60
37
68
61
50
53
48
53
62
73
68
45
46
64
52
51
68
66
94
96
37
100
69
100
60
100
28
100
94
18
37
100
32
33
100
100
100
100
36
100
100
100
40
100
100
100
100
100
51
71
100
77
72
32
74
41
62
17
76
26
33
30
40
36
62
29
70
76
41
41
29
17
76
17
49
40
72
32
31
41
66
66
72
70
76
97
92
90
93
95
88
63
96
63
84
100
89
84
87
100
74
94
100
88
100
93
98
75
100
90
71
100
95
98
100
100
93
71
84
88
75
68
79
52
58
28
51
24
60
67
58
47
61
82
81
55
50
38
53
43
66
32
51
71
65
67
52
48
51
64
82
72
44
72
56
91
63
75
68
44
64
47
60
84
59
88
68
75
69
29
65
22
81
65
67
43
46
25
57
90
91
80
53
75
70
62
67
69
81
95
81
86
67
90
71
85
77
95
74
95
71
91
71
73
79
58
85
91
71
90
29
87
74
88
95
69
49
74
72
82
64
74
42
41
61
78
41
55
49
61
45
25
49
50
43
36
58
49
69
51
27
60
44
59
70
59
45
76
61
76
68
89
55
40
59
53
82
68
90
48
85
79
69
86
80
48
86
89
93
67
89
74
37
76
59
84
85
83
72
69
88
68
56
25
41
24
92
80
87
87
44
73
36
49
46
42
42
49
54
77
69
49
43
71
50
51
63
58
59
69
32
60
66
75
38
76
42
42
60
83
39
39
61
44
92
90
71
78
87
74
91
82
68
88
81
52
81
86
77
75
85
92
85
87
84
81
82
87
77
88
74
79
88
81
69
88
92
88
66
70
65
42
61
60
61
66
56
63
48
58
72
68
72
69
62
54
56
69
68
59
60
59
71
71
64
54
60
58
78
79
70
72
56
57
62
50
56
47
51
42
57
57
75
32
56
80
67
54
80
78
60
51
58
50
79
60
58
82
64
67
76
93
58
56
54
61
78
57
69
47
76
52
59
63
58
91
50
69
83
82
83
63
61
38
69
44
74
55
53
77
73
73
82
62
66
55
65
63
59
68
86
77
80
77
77
68
83
75
58
84
52
39
76
78
77
59
51
53
79
42
85
68
56
78
69
45
61
51
46
31
93
89
86
78
76
50
74
71
89
54
89
54
64
50
96
73
93
50
53
73
80
87
50
61
72
54
68
81
70
50
39
78
57
83
70
60
73
64
37
22
31
63
39
33
16
41
58
22
50
49
40
34
41
33
26
61
34
35
31
35
57
51
44
22
21
64
70
77
45
67
43
44
70
84
53
38
69
79
77
89
68
95
66
72
89
98
92
86
80
70
99
82
74
83
56
69
92
97
91
73
80
91
77
86
78
90
44
23
41
46
36
34
29
45
39
31
38
44
36
51
57
32
63
73
54
42
35
41
49
53
63
40
27
67
46
35
67
42
44
59
89
100
68
76
76
90
89
90
79
99
79
82
94
100
91
94
98
92
100
80
94
84
95
61
100
100
99
93
89
61
92
97
98
92
62
78
54
42
45
44
51
57
45
73
43
51
47
53
54
67
43
38
43
42
49
38
69
64
53
71
69
39
49
70
58
58
56
57
37
38
45
29
60
71
45
76
44
27
25
59
67
8
56
56
47
53
22
91
53
77
52
44
49
40
52
42
53
30
63
64
61
53
3
79
32
54
26
43
18
41
63
75
69
75
15
77
12
32
45
28
76
57
26
42
45
45
8
68
42
50
61
57
23
25
36
23
100
23
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
100
7
100
100
100
100
100
100
100
100
66
62
57
58
63
62
55
66
63
66
70
52
64
72
65
59
62
69
69
68
57
67
69
70
64
69
61
62
73
76
62
69
70
68
56
56
61
59
58
55
62
55
57
56
55
64
58
54
61
63
61
58
58
53
65
58
58
59
62
59
63
63
58
57
66
61
61
6469 Mexico
70 Grenada
71 Ecuador
72 Panama
73 Bosnia andHerzegovina
74 Romania
75 Azerbaijan
76 Palestine
77 Lebanon
78 Venezuela
79 Sri Lanka
80 Moldova
81 Federated Statesof Micronesia
82 DominicanRepublic
83 Tonga
84 United ArabEmirates
85 Kazakhstan
86 Armenia
87 Suriname
88 Colombia
89 Qatar
90 Brazil
91 Indonesia
92 China
93 Oman
94 Vietnam
95 Fiji
96 Belize
97 Marshall Islands
98 Paraguay
99 Tajikistan
100 Nicaragua
101 Algeria
102 El Salvador
(Figure 1 continues on next page)
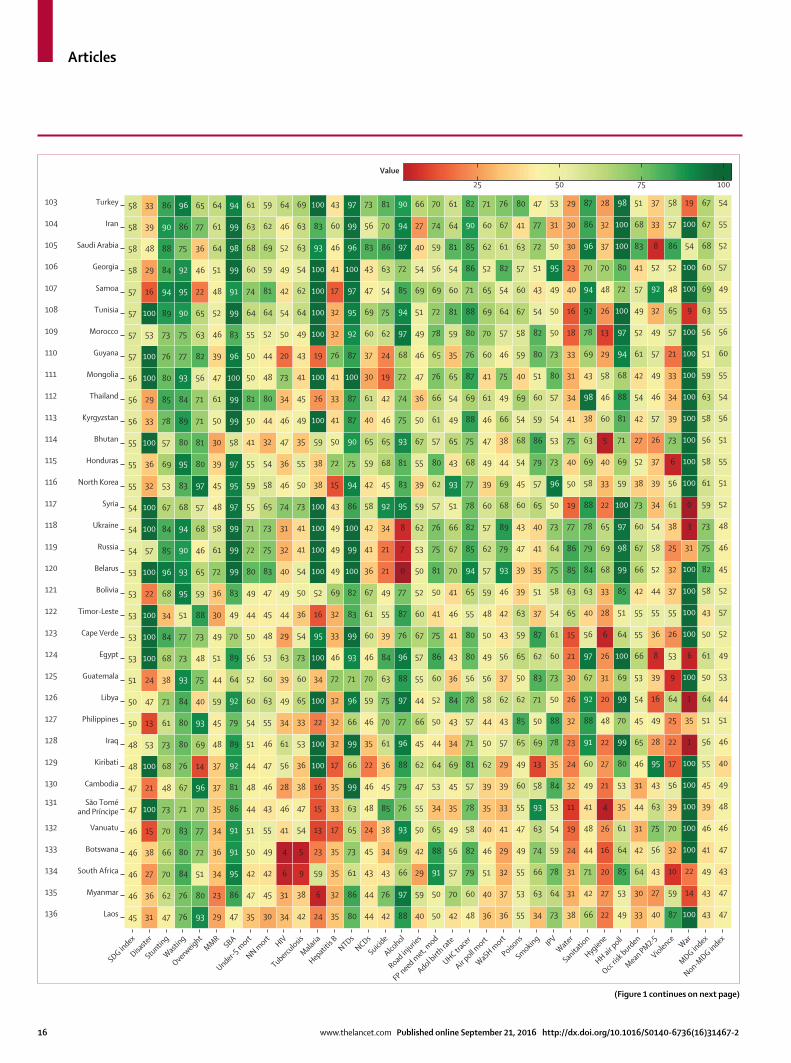
Articles
16 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
100755025
Value
SDG index
Disaste
r
Stunting
Wasting
Overweight
MMRSBA
Under-5 m
ort
NN mort HIV
Tuberculosis
Malaria
Hepatitis B NTDs
NCDs
Suicide
Alcohol
Road injurie
s
FP need met, m
od
Adol birt
h rate
UHC tracer
Air poll m
ort
WaSH mort
Poisons
Smoking IPVWater
Sanitatio
n
Hygiene
HH air poll
Occ ris
k burden
Mean PM2·5
Violence War
MDG index
Non-MDG in
dex
45
46
46
46
46
47
47
48
48
50
50
51
53
53
53
53
53
54
54
54
55
55
55
56
56
56
57
57
57
57
58
58
58
58
31
36
27
38
15
100
21
100
53
13
47
24
100
100
100
22
100
57
100
100
32
36
100
33
29
100
100
53
100
16
29
48
39
33
47
62
70
66
70
73
48
68
73
61
71
38
68
84
34
68
96
85
84
67
53
69
57
78
85
80
76
73
89
94
84
88
90
86
76
76
84
80
83
71
67
76
80
80
84
93
73
77
51
95
93
90
94
68
83
95
80
89
84
93
77
75
90
95
92
75
86
96
93
80
51
72
77
70
96
14
69
93
40
75
48
73
88
59
65
46
68
57
97
80
81
71
71
56
82
63
65
22
46
36
77
65
29
23
34
36
34
35
37
37
48
45
59
44
51
49
30
36
72
61
58
48
45
39
30
50
61
47
39
46
52
48
51
64
61
64
47
86
95
91
91
86
81
92
89
79
92
64
89
70
49
83
99
99
99
97
95
97
58
99
99
100
96
83
99
91
99
98
99
94
35
47
42
50
51
44
48
44
51
54
60
52
56
50
44
49
80
72
71
55
59
55
41
50
81
50
50
55
64
74
60
68
63
61
30
45
42
49
55
43
46
47
46
55
63
60
53
48
45
47
83
75
73
65
58
54
32
44
80
48
44
52
64
81
59
69
62
59
34
31
6
4
41
46
28
56
61
34
49
39
63
29
44
49
40
32
31
74
46
36
47
46
34
73
20
50
54
42
49
52
46
64
42
38
9
5
54
47
38
36
53
33
65
60
73
54
36
50
54
41
41
73
50
55
35
49
45
41
43
49
64
62
54
63
63
69
24
6
59
23
13
15
16
100
100
22
100
34
100
95
16
52
100
100
100
100
38
38
59
100
26
100
19
100
100
100
100
93
83
100
35
32
35
35
17
33
35
17
32
32
32
72
46
33
32
69
49
49
49
43
15
72
50
41
33
41
76
32
32
17
41
46
60
43
80
86
61
73
65
63
99
66
99
66
96
71
93
99
83
82
100
99
100
86
94
75
90
87
87
100
87
92
95
97
100
96
99
97
44
44
43
45
24
48
46
22
35
46
59
70
46
60
61
67
36
41
42
58
42
59
65
40
61
30
37
60
69
47
43
83
56
73
42
76
43
34
38
85
45
36
61
70
75
63
84
39
55
49
21
21
34
92
45
68
65
46
42
19
24
62
75
54
63
86
70
81
88
97
66
69
93
76
79
88
96
77
97
88
96
76
87
77
0
7
8
95
83
81
93
75
74
72
68
97
94
85
72
97
94
90
40
59
29
42
50
55
47
62
45
66
44
55
57
67
60
52
50
53
62
59
39
55
67
50
36
47
46
49
51
69
54
40
27
66
50
50
91
88
65
34
53
64
44
50
52
60
86
75
41
50
81
75
76
57
62
80
57
61
66
76
65
78
72
69
56
59
74
70
42
70
57
56
49
35
45
69
34
43
84
36
43
41
46
41
70
67
66
51
93
43
65
49
54
65
35
59
81
60
54
81
64
61
48
60
79
82
58
78
57
81
71
57
78
56
80
80
55
65
94
85
82
78
77
68
75
88
69
87
76
80
88
71
86
85
90
82
36
40
51
46
40
35
39
62
50
44
58
56
49
50
48
59
57
62
57
60
39
49
47
46
61
41
60
70
69
65
52
62
60
71
36
37
32
29
41
33
39
29
57
43
62
37
56
43
42
46
93
79
89
68
69
44
38
66
49
75
46
57
64
54
82
61
67
76
55
53
55
49
47
55
60
49
65
85
62
50
65
59
63
39
39
47
43
60
45
54
68
54
69
40
59
58
67
60
57
63
41
80
34
63
66
74
63
93
58
13
69
50
71
83
62
87
37
51
35
41
40
65
57
79
86
59
60
51
80
82
54
43
51
72
77
47
73
64
78
59
54
53
84
35
78
88
50
73
60
61
54
58
75
64
73
50
96
73
53
54
57
80
73
50
50
49
95
50
31
53
38
31
31
24
19
11
32
24
23
32
26
30
21
15
65
63
85
86
77
19
50
40
75
41
34
31
33
18
16
40
23
30
30
29
66
42
71
44
48
41
49
60
91
88
92
67
97
56
40
63
84
79
78
88
58
69
63
38
98
43
69
78
92
94
70
96
86
87
22
27
20
16
26
4
21
27
22
48
20
31
26
6
28
33
68
69
65
22
33
40
5
60
46
58
29
13
26
48
70
37
32
28
49
53
85
64
61
35
53
80
99
70
99
69
100
64
51
85
99
98
97
100
59
69
71
81
88
68
94
97
100
72
80
100
100
98
33
30
64
42
31
44
31
46
65
45
54
53
66
55
55
42
66
67
60
73
38
52
27
42
54
42
61
52
49
57
41
83
68
51
40
27
43
56
75
63
43
95
28
49
16
39
8
36
55
44
52
58
54
34
39
37
26
57
46
49
57
49
32
92
52
8
33
37
87
59
10
32
70
39
56
17
22
25
64
9
53
26
55
37
32
25
38
61
56
6
73
39
34
33
21
57
65
48
52
86
57
58
100
14
22
100
100
100
100
100
1
35
1
100
6
100
100
100
100
31
3
0
100
100
100
100
100
100
100
100
9
100
100
54
100
19
43
43
49
41
46
39
45
55
56
51
64
50
61
50
43
58
82
75
73
59
61
58
56
58
63
59
51
56
63
69
60
68
67
67
47
47
43
47
46
48
49
40
46
51
44
53
49
52
57
52
45
46
48
52
51
55
51
56
54
55
60
56
55
49
57
52
55
54103 Turkey
104 Iran
105 Saudi Arabia
106 Georgia
107 Samoa
108 Tunisia
109 Morocco
110 Guyana
111 Mongolia
112 Thailand
113 Kyrgyzstan
114 Bhutan
115 Honduras
116 North Korea
117 Syria
118 Ukraine
119 Russia
120 Belarus
121 Bolivia
122 Timor-Leste
123 Cape Verde
124 Egypt
125 Guatemala
126 Libya
127 Philippines
128 Iraq
129 Kiribati
130 Cambodia
131 São Toméand Príncipe
132 Vanuatu
133 Botswana
134 South Africa
135 Myanmar
136 Laos
(Figure 1 continues on next page)
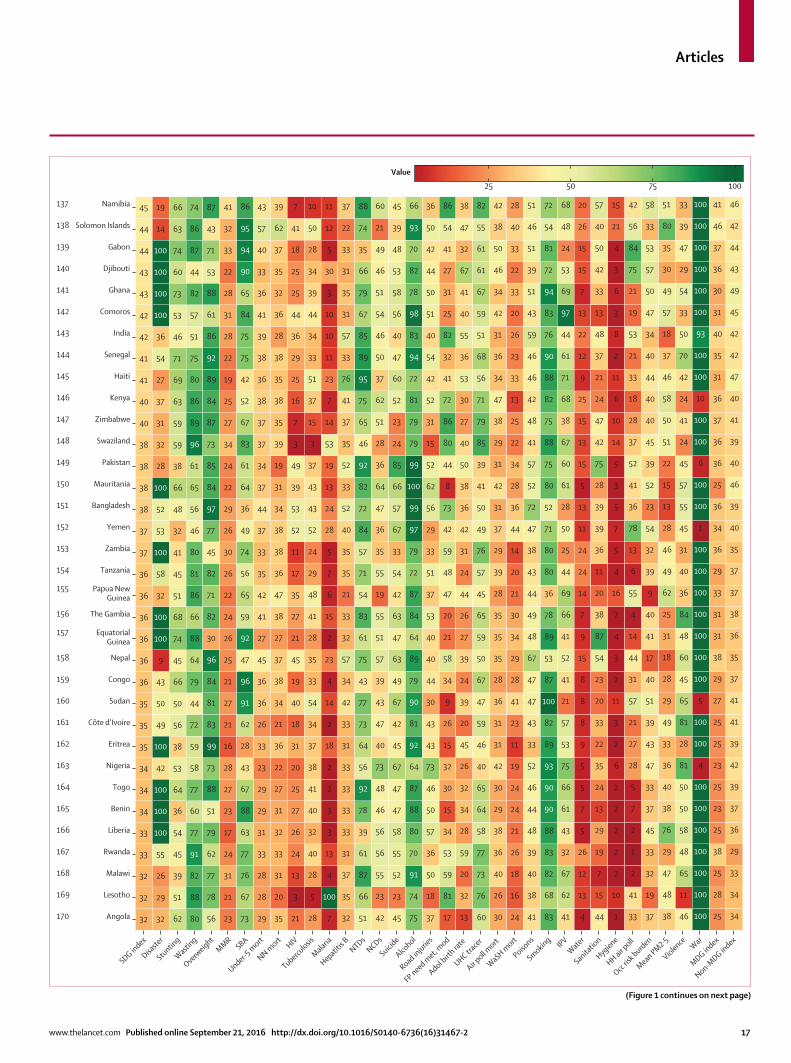
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 17
100755025
Value
SDG index
Disaste
r
Stunting
Wasting
Overweight
MMRSBA
Under-5 m
ort
NN mort HIV
Tuberculosis
Malaria
Hepatitis B NTDs
NCDs
Suicide
Alcohol
Road injurie
s
FP need met, m
od
Adol birt
h rate
UHC tracer
Air poll m
ort
WaSH mort
Poisons
Smoking IPVWater
Sanitatio
n
Hygiene
HH air poll
Occ ris
k burden
Mean PM2·5
Violence War
MDG index
Non-MDG in
dex
32
32
32
33
33
34
34
34
35
35
35
36
36
36
36
36
36
37
37
38
38
38
38
40
40
41
41
42
42
43
43
44
44
45
32
29
26
55
100
100
100
42
100
49
50
43
9
100
100
32
58
100
53
52
100
28
32
31
37
27
54
36
100
100
100
100
14
19
62
51
39
45
54
36
64
53
38
56
50
66
45
74
68
51
45
41
32
48
66
38
59
59
63
69
71
46
53
73
60
74
63
66
80
88
82
91
77
60
77
58
59
72
44
79
64
88
66
86
81
80
46
56
65
61
96
89
86
80
75
51
57
82
44
87
86
74
56
78
77
62
79
51
88
73
99
83
81
84
96
30
82
71
82
45
77
97
84
85
73
87
84
89
92
86
61
88
53
71
43
87
23
21
31
24
17
23
27
28
16
21
27
21
25
26
24
22
26
30
26
29
22
24
34
27
25
19
22
28
31
28
22
33
32
41
73
67
76
77
63
88
67
43
28
62
91
96
47
92
59
65
56
74
49
36
64
61
83
67
52
42
75
75
84
65
90
94
95
86
29
28
28
33
31
29
29
23
33
26
36
36
45
27
41
42
35
33
37
44
37
34
37
37
38
36
38
39
41
36
33
40
57
43
35
20
31
33
32
31
27
22
36
21
34
38
37
27
38
47
36
38
38
34
31
19
39
35
38
35
38
28
36
32
35
37
62
39
21
3
13
24
26
27
25
20
31
18
40
19
45
21
27
35
17
11
52
53
39
49
3
7
16
25
29
36
44
25
25
18
41
7
28
5
28
40
32
40
41
38
37
34
54
33
35
28
41
48
29
24
52
43
43
37
3
15
37
51
33
34
44
39
34
28
50
10
7
100
4
13
3
3
2
2
18
2
14
4
23
2
15
6
7
5
28
24
13
19
53
14
7
23
11
10
10
3
30
5
12
11
32
35
37
31
33
33
33
33
31
33
42
34
57
32
33
21
35
35
40
52
33
52
35
37
41
76
33
57
31
35
31
33
22
37
51
66
87
61
39
78
92
56
64
73
77
43
75
61
83
54
71
57
84
72
82
92
46
65
75
95
89
85
67
79
66
35
74
88
42
23
55
56
56
46
48
73
40
47
43
39
57
51
55
19
55
35
36
47
64
36
28
51
62
37
50
46
54
51
46
49
21
60
45
23
52
55
58
47
47
67
45
42
67
49
63
47
63
42
54
33
67
57
66
85
24
23
52
60
47
40
56
58
53
48
39
45
75
74
91
70
80
88
87
64
92
81
90
79
89
64
84
87
72
79
97
99
100
99
79
79
81
72
94
83
98
78
82
70
93
66
37
18
50
36
57
50
46
73
43
43
30
44
40
40
53
37
51
33
29
56
62
52
15
31
52
42
54
40
51
50
44
42
50
36
17
81
59
53
34
15
30
32
15
26
9
34
58
21
20
47
48
59
42
73
8
44
80
86
72
41
32
82
25
31
27
41
54
86
13
32
20
59
28
34
32
26
45
20
39
24
39
27
26
44
24
31
42
36
38
50
40
27
30
53
36
55
40
41
67
32
47
38
60
76
73
77
58
64
65
40
46
59
47
67
50
59
65
45
57
76
49
50
41
39
85
79
71
56
68
51
59
67
61
61
55
82
30
26
40
36
38
29
30
42
31
31
36
28
35
35
35
28
39
29
37
31
42
31
29
38
47
34
36
31
42
34
46
50
38
42
24
16
18
26
21
24
24
19
11
23
41
28
29
34
30
21
20
14
44
36
28
34
22
25
13
33
23
26
20
33
22
33
40
28
41
38
40
39
48
44
46
52
33
43
47
47
67
48
49
44
43
38
47
72
52
57
41
48
42
46
46
59
43
51
39
51
46
51
83
68
82
83
88
90
90
93
89
82
100
87
53
89
78
36
80
80
71
52
80
75
88
75
82
88
90
76
83
94
72
81
54
72
41
62
67
32
43
61
66
75
53
57
21
41
52
41
66
69
44
25
50
28
61
60
67
38
68
71
61
44
97
69
53
24
48
68
4
13
12
26
5
7
5
5
9
8
8
8
15
9
7
14
24
24
11
13
5
15
13
15
25
9
12
22
13
7
15
15
26
20
44
15
7
19
29
13
24
35
22
33
20
23
54
87
38
20
11
36
39
39
28
75
42
47
24
21
37
48
13
33
42
50
40
57
1
10
2
2
2
2
2
6
2
3
11
2
3
4
2
16
4
5
7
5
3
5
14
10
6
11
2
8
3
6
3
4
21
15
33
41
2
1
2
7
5
28
27
21
57
31
44
14
4
55
6
13
78
36
41
52
37
28
18
33
21
53
19
21
75
84
56
42
37
19
32
33
45
37
33
47
43
39
51
40
17
41
40
9
39
32
54
23
52
39
45
40
40
44
40
34
47
50
57
53
33
58
38
48
47
29
76
38
40
36
33
49
29
28
18
31
25
62
49
46
28
13
15
22
51
50
58
46
37
18
57
49
30
35
80
51
46
11
65
48
58
50
50
81
28
81
65
45
60
48
84
36
40
31
45
55
57
45
24
41
24
42
70
50
33
54
29
47
39
33
100
100
100
100
100
100
100
4
100
100
5
100
100
100
100
100
100
100
1
100
100
6
100
100
10
100
100
93
100
100
100
100
100
100
25
28
25
38
25
23
25
23
25
25
27
29
38
31
31
33
29
36
34
36
25
36
36
37
36
31
35
40
31
30
36
37
46
41
34
34
33
29
36
37
39
42
39
41
41
37
35
36
38
37
37
35
40
39
46
40
39
41
40
47
42
42
45
49
43
44
42
46137 Namibia
138 Solomon Islands
139 Gabon
140 Djibouti
141 Ghana
142 Comoros
143 India
144 Senegal
145 Haiti
146 Kenya
147 Zimbabwe
148 Swaziland
149 Pakistan
150 Mauritania
151 Bangladesh
152 Yemen
153 Zambia
154 Tanzania
155 Papua NewGuinea
156 The Gambia
157 EquatorialGuinea
158 Nepal
159 Congo
160 Sudan
161 Côte d’Ivoire
162 Eritrea
163 Nigeria
164 Togo
165 Benin
166 Liberia
167 Rwanda
168 Malawi
169 Lesotho
170 Angola
(Figure 1 continues on next page)

Articles
18 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
improvement for the indicator on malaria incidence represents the large number of malaria-free countries in both 2000 and 2015.46 Health-related indicators covered by Target 3.3—which aims to end the epidemics of HIV, tuberculosis, malaria, and neglected tropical diseases, and to “combat hepatitis” by 2030—generally saw moderate progress (median absolute change of 2∙7 [IQR –0∙2 to 4∙6] for HIV incidence and 3∙9 [IQR 1∙7 to 5∙7] for tuberculosis incidence), although minimal changes occurred for hepatitis B incidence (–0∙2 [–0∙4 to –0∙05]). In combination, these trends highlight the need for accelerated progress in order to meet Target 3.3. Substantial improvements occurred for childhood stunting (8∙2 [3∙5 to 14∙2]) and, to a more modest extent, wasting (2∙7 [0∙0 to 6∙0]), yet childhood overweight considerably worsened in the past 15 years (–4∙5 [–9∙2 to –0∙7]). This trend occurred across SDI
quintiles, emphasising the need for concerted policy attention to reverse this trend. Alcohol consumption worsened slightly in the past 15 years as well (–0∙4 [–2∙3 to 0∙7]).
Between 2000 and 2015, distinct patterns for absolute changes in health-related SDG indicators surfaced across SDI quintiles (fi gure 6). While the indicator for UHC tracer interventions improved across all SDI quintiles, the most pronounced gains occurred in low-SDI and low-middle-SDI countries. Childhood stunting and wasting also improved at a faster pace for the low-SDI quintile than for other quintiles. Notably, mortality measures from the MDG agenda—maternal mortality ratio, under-5 mortality, and neonatal mortality—progressed at a similar pace across SDI quintiles. By contrast, mortality due to road injuries, non-communicable diseases (NCDs), and interpersonal
Figure 1: Performance of the health-related SDG index, MDG index, and non-MDG index, and 33 individual health-related indicators, by country, 2015Countries are ranked by their health-related SDG index from highest to lowest. Indicators have been scaled from 0 to 100. Defi nitions of health-related SDG indicators are shown in table 1. SDG=Sustainable Development Goal. MDG=Millennium Development Goal. MMR=maternal mortality ratio. SBA=skilled birth attendance. Mort=mortality. NN mort=neonatal mortality. NTDs=neglected tropical diseases. NCDs=non-communicable diseases. FP need met, mod=family planning need met, modern contraception. Adol=adolescent. UHC=universal health coverage. Air poll mort=mortality attributable to air pollution. WaSH=water, sanitation, and hygiene. IPV=intimate partner violence. HH air poll=household air pollution. Occ risk burden=burden attributable to occupational risks. PM2·5=fi ne particulate matter smaller than 2·5 μm.
100755025
Value
SDG index
Disaste
r
Stunting
Wasting
Overweight
MMRSBA
Under-5 m
ort
NN mort HIV
Tuberculosis
Malaria
Hepatitis B NTDs
NCDs
Suicide
Alcohol
Road injurie
s
FP need met, m
od
Adol birt
h rate
UHC tracer
Air poll m
ort
WaSH mort
Poisons
Smoking IPVWater
Sanitatio
n
Hygiene
HH air poll
Occ ris
k burden
Mean PM2·5
Violence War
MDG index
Non-MDG in
dex
20
22
22
23
24
24
26
26
26
27
28
28
29
29
30
31
31
31
100
25
28
31
52
48
30
47
18
42
28
32
100
100
100
53
58
57
45
44
54
36
48
43
21
49
33
46
33
44
54
53
41
55
53
58
71
55
30
42
47
71
78
54
66
67
39
79
77
66
64
82
50
80
84
86
72
90
82
84
92
75
88
68
87
71
71
82
88
82
78
68
12
17
20
24
20
21
24
25
13
15
26
27
21
17
23
28
25
21
61
32
41
32
21
87
63
57
40
61
44
61
39
49
15
68
68
67
19
22
23
22
19
27
30
19
28
20
34
29
20
22
35
32
22
27
17
26
29
34
21
30
32
17
29
21
35
32
20
22
32
34
27
25
15
34
23
34
23
26
24
25
57
26
46
11
18
23
26
15
28
17
24
30
28
35
33
30
34
40
45
36
41
24
30
36
32
29
36
36
3
11
6
3
7
3
6
1
14
2
9
3
10
2
25
5
2
4
34
36
31
33
33
32
35
33
31
34
31
37
33
33
36
33
33
34
68
48
58
97
70
47
79
90
76
78
57
59
74
56
55
85
93
75
26
42
51
57
50
47
47
51
10
45
39
44
46
45
52
46
52
47
35
53
55
61
55
53
49
65
55
54
52
43
53
55
50
43
50
45
85
96
82
96
81
87
71
96
96
73
91
89
82
94
79
58
67
74
23
42
44
59
47
50
37
58
13
47
53
40
48
53
49
35
46
48
9
15
24
29
16
14
29
20
39
35
37
38
20
18
54
41
28
33
33
27
41
5
19
23
53
12
37
25
26
20
33
20
43
24
27
29
45
16
27
46
34
56
65
47
28
64
39
59
52
48
44
69
66
58
15
28
32
30
27
27
31
39
11
28
29
37
26
27
38
33
34
31
14
6
9
16
14
23
16
21
38
21
21
20
19
21
20
22
19
25
32
27
33
42
39
42
34
44
44
42
41
39
39
42
44
37
42
46
86
84
83
91
85
84
89
88
66
71
77
78
87
92
92
87
81
90
74
53
53
61
79
12
53
50
50
23
53
42
61
61
27
18
84
23
2
5
6
2
2
3
4
4
9
3
19
6
3
7
8
26
4
7
9
26
8
3
8
15
11
13
28
17
4
11
24
20
7
20
11
24
0
1
1
1
2
0
1
1
4
2
3
1
1
1
1
3
1
5
2
1
1
2
3
3
2
2
49
2
2
4
3
2
4
2
6
24
21
43
42
40
33
30
29
49
43
39
20
31
35
35
37
31
30
40
31
53
40
23
31
31
32
32
30
54
53
54
40
50
38
24
35
21
34
26
31
53
48
47
74
55
11
65
60
37
38
49
38
37
80
53
3
1
2
4
6
7
5
7
1
100
12
28
100
33
17
100
100
4
15
19
18
13
15
20
23
18
26
20
23
22
21
21
23
33
21
26
24
24
24
28
30
25
27
30
27
30
29
30
33
33
32
29
35
34171 Cameroon
172 Burkina Faso
173 Uganda
174 Ethiopia
175 Guinea
176 Guinea-Bissau
177 Mozambique
178 Madagascar
179 Sierra Leone
180 Afghanistan
181 Mali
182 Burundi
183 DemocraticRepublic ofthe Congo
184 Chad
185 Niger
186 South Sudan
187 Somalia
188 Central AfricanRepublic
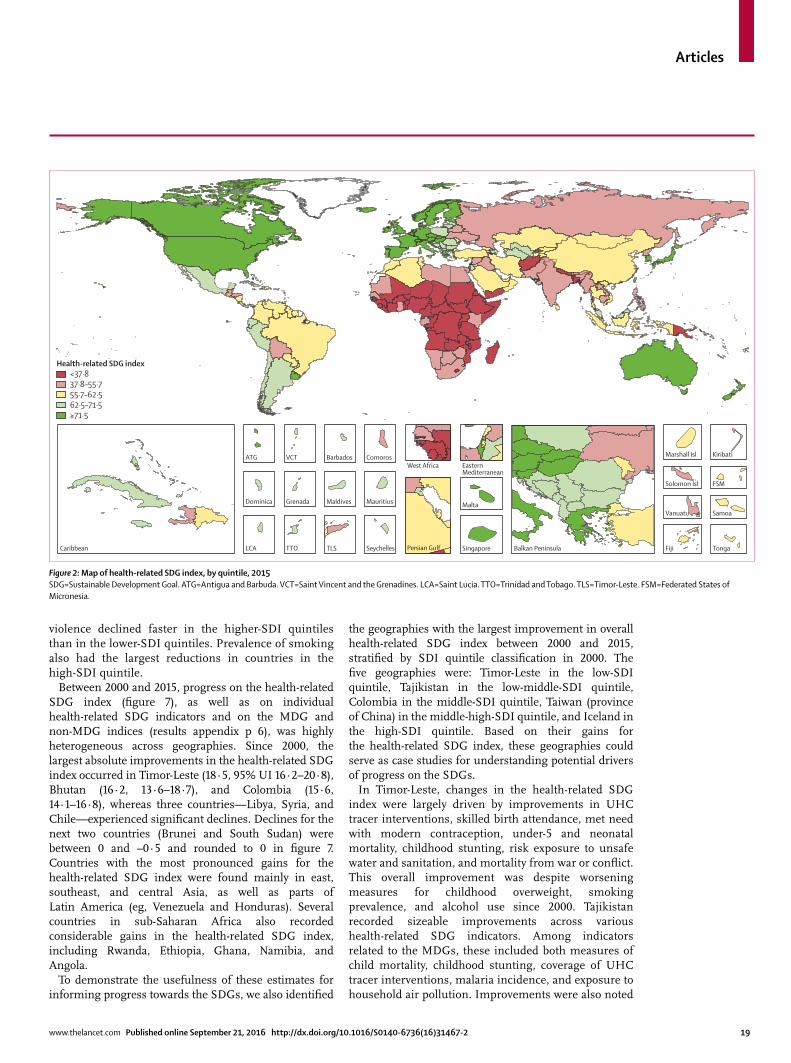
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 19
violence declined faster in the higher-SDI quintiles than in the lower-SDI quintiles. Prevalence of smoking also had the largest reductions in countries in the high-SDI quintile.
Between 2000 and 2015, progress on the health-related SDG index (fi gure 7), as well as on individual health-related SDG indicators and on the MDG and non-MDG indices (results appendix p 6), was highly heterogeneous across geographies. Since 2000, the largest absolute improve ments in the health-related SDG index occurred in Timor-Leste (18∙5, 95% UI 16∙2–20∙8), Bhutan (16∙2, 13∙6–18∙7), and Colombia (15∙6, 14∙1–16∙8), whereas three countries—Libya, Syria, and Chile—experienced signifi cant declines. Declines for the next two countries (Brunei and South Sudan) were between 0 and –0∧5 and rounded to 0 in fi gure 7. Countries with the most pronounced gains for the health-related SDG index were found mainly in east, southeast, and central Asia, as well as parts of Latin America (eg, Venezuela and Honduras). Several countries in sub-Saharan Africa also recorded considerable gains in the health-related SDG index, including Rwanda, Ethiopia, Ghana, Namibia, and Angola.
To demonstrate the usefulness of these estimates for informing progress towards the SDGs, we also identifi ed
the geographies with the largest improvement in overall health-related SDG index between 2000 and 2015, stratifi ed by SDI quintile classifi cation in 2000. The fi ve geographies were: Timor-Leste in the low-SDI quintile, Tajikistan in the low-middle-SDI quintile, Colombia in the middle-SDI quintile, Taiwan (province of China) in the middle-high-SDI quintile, and Iceland in the high-SDI quintile. Based on their gains for the health-related SDG index, these geographies could serve as case studies for understanding potential drivers of progress on the SDGs.
In Timor-Leste, changes in the health-related SDG index were largely driven by improvements in UHC tracer interventions, skilled birth attendance, met need with modern contraception, under-5 and neonatal mortality, childhood stunting, risk exposure to unsafe water and sanitation, and mortality from war or confl ict. This overall improvement was despite worsening measures for childhood overweight, smoking prevalence, and alcohol use since 2000. Tajikistan recorded sizeable improvements across various health-related SDG indicators. Among indicators related to the MDGs, these included both measures of child mortality, childhood stunting, coverage of UHC tracer interventions, malaria incidence, and exposure to household air pollution. Improvements were also noted
Figure 2: Map of health-related SDG index, by quintile, 2015SDG=Sustainable Development Goal. ATG=Antigua and Barbuda. VCT=Saint Vincent and the Grenadines. LCA=Saint Lucia. TTO=Trinidad and Tobago. TLS=Timor-Leste. FSM=Federated States of Micronesia.
Persian GulfCaribbean LCA
Dominica
ATG
TTO
Grenada
VCT
TLS
Maldives
Barbados
Seychelles
Mauritius
ComorosWest Africa Eastern
Mediterranean
Malta
Singapore Balkan Peninsula Tonga
Samoa
FSM
Fiji
Solomon Isl
Marshall Isl
Vanuatu
Kiribati
Health-related SDG index <37·8 37·8–55·7 55·7–62·5 62·5–71·5 ≥71·5
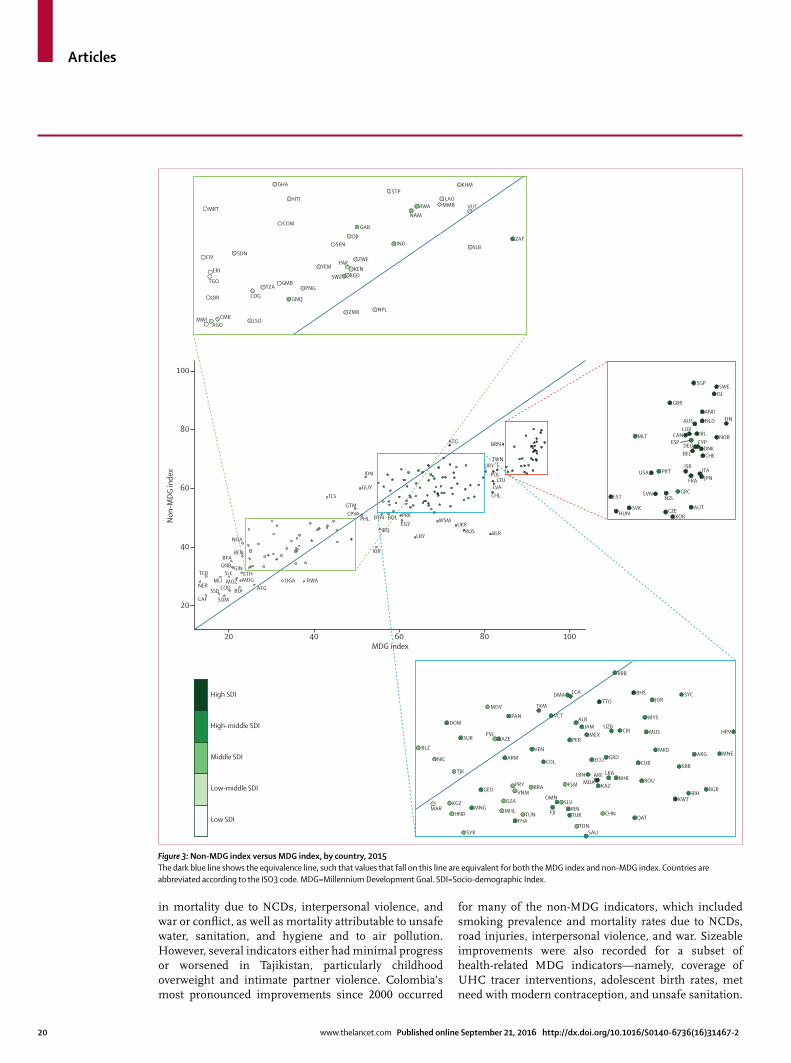
Articles
20 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
in mortality due to NCDs, interpersonal violence, and war or confl ict, as well as mortality attributable to unsafe water, sanitation, and hygiene and to air pollution. However, several indicators either had minimal progress or worsened in Tajikistan, particularly childhood overweight and intimate partner violence. Colombia’s most pronounced improvements since 2000 occurred
for many of the non-MDG indicators, which included smoking prevalence and mortality rates due to NCDs, road injuries, interpersonal violence, and war. Sizeable improvements were also recorded for a subset of health-related MDG indicators—namely, coverage of UHC tracer interventions, adolescent birth rates, met need with modern contraception, and unsafe sanitation.
Figure 3: Non-MDG index versus MDG index, by country, 2015The dark blue line shows the equivalence line, such that values that fall on this line are equivalent for both the MDG index and non-MDG index. Countries are abbreviated according to the ISO3 code. MDG=Millennium Development Goal. SDI=Socio-demographic Index.
20 40 60 80 100
20
40
RWA
MDV
PANDOM
SUR
BLZ
NIC
TJK
MARKGZ
HND
SYR
MNG
GEO
DZA
MHL
THATUN
PRY
ARMVEN
COL
VNMBRA
FJI
SLVOMN
IRNTUR CHN
QATTON
SAU
AZEPSE
TKM
LCA
VCT
BRB
TTOBHS
JORSYC
MYS
MUS HRVCRIMEX
PER
ECU GRDCUB
MKD
SRB
KWTBIH
BGR
ARG MNE
ROULBN ARE
KAZBHR
LKA
MDAFSM
JAMALB
UZB
DMA
UGAAFG
CAF SOMSSD
NERMLI
SLE ETHMDG
BDI
MOZTCD
COD
NGA
TLS
IDN
GUY
GTMCPV
PHL BTN
IRQ
KIR
PRKBOLEGY
LBY
WSMUKR
RUS BLR
ATG
SGPSWE
ISLGBR
ANDNLDAUS
NORIRL
BELDEU CYP
DNKCHE
LUXCAN
ESPMLT
USA PRT ITAJPNFRA
ISR
GRC
AUTKOR
CZE
NZLSVN
SVKHUN
EST
FIN
MRT
GHA
HTI
GAB
IND
NAMBWA
STPKHM
LAOMMB VUT
SLBZAFDJI
SEN
COM
SDNCIV
ERI
TGO
LBR
CMRAGO
MWI LSO
COGTZA
GMBPNG
ZMB NPL
YEMZWE
KENBGDSWZ
PAK
GNQ
LTUPOL
URYTWN
BRN
LVACHL
BENBFA
GNB GIN
60
80
100
Non
-MDG
inde
x
MDG index
High SDI
High-middle SDI
Middle SDI
Low-middle SDI
Low SDI
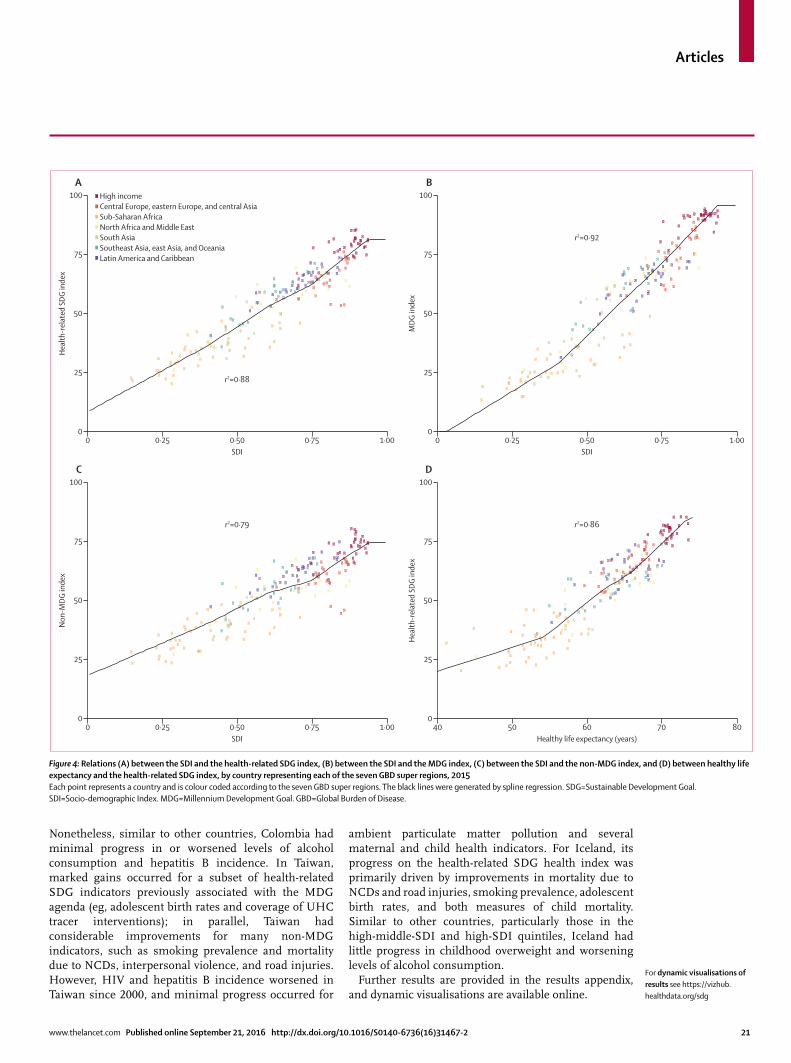
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 21
Nonetheless, similar to other countries, Colombia had minimal progress in or worsened levels of alcohol consumption and hepatitis B incidence. In Taiwan, marked gains occurred for a subset of health-related SDG indicators previously associated with the MDG agenda (eg, adolescent birth rates and coverage of UHC tracer interventions); in parallel, Taiwan had considerable improvements for many non-MDG indicators, such as smoking prevalence and mortality due to NCDs, interpersonal violence, and road injuries. However, HIV and hepatitis B incidence worsened in Taiwan since 2000, and minimal progress occurred for
ambient particulate matter pollution and several maternal and child health indicators. For Iceland, its progress on the health-related SDG health index was primarily driven by improvements in mortality due to NCDs and road injuries, smoking prevalence, adolescent birth rates, and both measures of child mortality. Similar to other countries, particularly those in the high-middle-SDI and high-SDI quintiles, Iceland had little progress in childhood overweight and worsening levels of alcohol consumption.
Further results are provided in the results appendix, and dynamic visualisations are available online.
Figure 4: Relations (A) between the SDI and the health-related SDG index, (B) between the SDI and the MDG index, (C) between the SDI and the non-MDG index, and (D) between healthy life expectancy and the health-related SDG index, by country representing each of the seven GBD super regions, 2015 Each point represents a country and is colour coded according to the seven GBD super regions. The black lines were generated by spline regression. SDG=Sustainable Development Goal. SDI=Socio-demographic Index. MDG=Millennium Development Goal. GBD=Global Burden of Disease.
0 0·25 0·50 0·75 1·000
25
50
75
100
Hea
lth-r
elat
ed S
DG in
dex
SDI
r2=0·88
0 0·25 0·50 0·75 1·000
25
50
75
100
MDG
inde
x
SDI
r2=0·92
�
�
�
�
�
�
�
�
�
�
�
�
�
�
� �
�
�
�
�
�
�
�
�
��
�
�
� �
�
�� �
� �
�
��
��
�
��
�
�
�
�
��
�
��
�
��
�
�
�
�
�
�
�� �
�
�
�
�
�
�
� �
��� �
�
�
�
�
�
�
� �
�
�
��
��
�
�
�
��
�
�
���
�
�
�
��
�
�
�
�
�
�
�
�
��
���
�
�
�
�
�
�
��
�
�
�
��
�
�
� �
�
�
�
�
�
�
�
��
�
�
�
�
�
�
�
� �
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
��
�
��
�
� �
�
�
��
�
� �
�
�
�
�
�
�
�
�
�
�
�
A B
0 0·25 0·50 0·75 1·000
25
50
75
100
Non
-MDG
inde
x
SDI
r2=0·79
40 50 60 70 800
25
50
75
100
Hea
lth-r
elat
ed S
DG in
dex
Healthy life expectancy (years)
r2=0·86
C D
High incomeCentral Europe, eastern Europe, and central AsiaSub-Saharan AfricaNorth Africa and Middle EastSouth AsiaSoutheast Asia, east Asia, and OceaniaLatin America and Caribbean
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
� ��
�
��
�
�
�
�
��
�
�
�
�
�
�
�
�
��
�
�
��
�
��
�
��� ��
���� ��
� ��
���
� �
�
��
�
��
�
�
�
��
�
�
���
�
�
�
�
�
�
�
� ��
�
�
�
���
�
�
�
�
�
�
���
��
�
�
�
�
��
�
�
�
�
�
�
�
�
�
��
�
�
�
�
��
�
�
�
�
�
�
�
�
�
�
��
�
��
�
�
�
�
�
�
�
�
�
�
�
�
��
�
�
�
�
�
�
� �
� �
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
��
�
�
�
�
� ��
�
�
�
�
�
�
�
�
��
� �� �
�
�� �
� �
���
� �
�
��
��
�
�
��
�
��
�
�
�
�
�
�
�
�
�� �
�
�
�
�
�
�
� �
���
�
�
�
�
�
�
��
�
�
�
�
��
��
�
�
��
�
�
��
�
�
�
��
�
�
�
��
�
�
�
�
���
�
�
�
�
�
�
�
�
�
�
��
��� �
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
��
�
�
�
�
�
�
��
�
�
�
�
�
�
�
�
�
��
��
�
�
�
�
�
�
� �
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
��
�
�
�
�
�
�
�
�
��
�
�
��
�
� � �
��
�
��
��
�
��
�
�
�
�
��
�
� �
��
�
�
�
�
�
�
� ��
�
�
�
�
�
�
��
��� �
�
�
�
�
�
� �
�
�
��
��
�
�
�
��
�
�
��
�
�
�
�
��
�
�
�
�
�
�
�
��
�� �
�
�
�
�
�
��
�
�
�
��
�
�
� �
�
�
�
�
�
�
��
�
�
�
�
�
�
�
��
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
��
��
�
��
�
�
� �
�
��
�
�
�
�
�
�
�
�
�
�
�
For dynamic visualisations of results see https://vizhub.healthdata.org/sdg
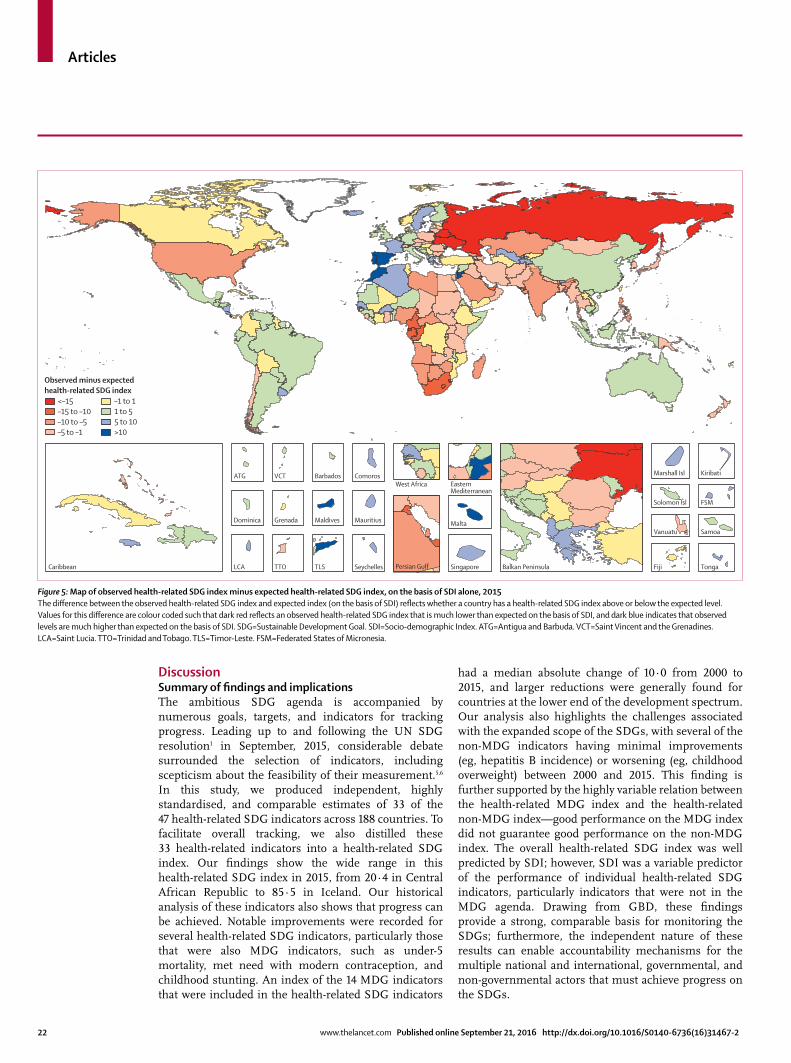
Articles
22 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
DiscussionSummary of fi ndings and implicationsThe ambitious SDG agenda is accompanied by numerous goals, targets, and indicators for tracking progress. Leading up to and following the UN SDG resolution1 in September, 2015, considerable debate surrounded the selection of indicators, including scepticism about the feasibility of their measurement.5,6 In this study, we produced independent, highly standardised, and comparable estimates of 33 of the 47 health-related SDG indicators across 188 countries. To facilitate overall tracking, we also distilled these 33 health-related indicators into a health-related SDG index. Our fi ndings show the wide range in this health-related SDG index in 2015, from 20∙4 in Central African Republic to 85∙5 in Iceland. Our historical analysis of these indicators also shows that progress can be achieved. Notable improvements were recorded for several health-related SDG indicators, particularly those that were also MDG indicators, such as under-5 mortality, met need with modern contraception, and childhood stunting. An index of the 14 MDG indicators that were included in the health-related SDG indicators
had a median absolute change of 10∙0 from 2000 to 2015, and larger reductions were generally found for countries at the lower end of the development spectrum. Our analysis also highlights the challenges associated with the expanded scope of the SDGs, with several of the non-MDG indicators having minimal improvements (eg, hepatitis B incidence) or worsening (eg, childhood overweight) between 2000 and 2015. This fi nding is further supported by the highly variable relation between the health-related MDG index and the health-related non-MDG index—good performance on the MDG index did not guarantee good performance on the non-MDG index. The overall health-related SDG index was well predicted by SDI; however, SDI was a variable predictor of the performance of individual health-related SDG indicators, particularly indicators that were not in the MDG agenda. Drawing from GBD, these fi ndings provide a strong, comparable basis for monitoring the SDGs; furthermore, the independent nature of these results can enable accountability mechanisms for the multiple national and international, governmental, and non-governmental actors that must achieve progress on the SDGs.
Figure 5: Map of observed health-related SDG index minus expected health-related SDG index, on the basis of SDI alone, 2015The diff erence between the observed health-related SDG index and expected index (on the basis of SDI) refl ects whether a country has a health-related SDG index above or below the expected level. Values for this diff erence are colour coded such that dark red refl ects an observed health-related SDG index that is much lower than expected on the basis of SDI, and dark blue indicates that observed levels are much higher than expected on the basis of SDI. SDG=Sustainable Development Goal. SDI=Socio-demographic Index. ATG=Antigua and Barbuda. VCT=Saint Vincent and the Grenadines. LCA=Saint Lucia. TTO=Trinidad and Tobago. TLS=Timor-Leste. FSM=Federated States of Micronesia.
Caribbean LCA
Dominica
ATG
Persian GulfTTO
Grenada
VCT
TLS
Maldives
Barbados
Seychelles
Mauritius
ComorosWest Africa Eastern
Mediterranean
Malta
Singapore Balkan Peninsula Tonga
Samoa
FSM
Fiji
Solomon Isl
Marshall Isl
Vanuatu
Kiribati
Observed minus expected health-related SDG index
<–15–15 to –10–10 to –5–5 to –1
–1 to 11 to 55 to 10>10

Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 23
Figure 6: Median absolute change for health-related SDG index, MDG index, and 33 individual health-related SDG indicators (rescaled), (A) across all countries and in the (B) low-SDI quintile, (C) low-middle-SDI quintile, (D) middle-SDI quintile, (E) high-middle-SDI quintile, and (F) high-SDI quintile, 2000–15Positive values indicate improvements between 2000–15, and negative values point to worsening performance for a given indicator during this time. Black stripes represent median absolute change and boxes represent IQR. Health-related indicators are colour coded according to the health-related goals they represent. Defi nitions of health-related SDG indicators are shown in table 1. SDG=Sustainable Development Goal. MDG=Millennium Development Goal. SDI=Socio-demographic Index. MMR=maternal mortality ratio. SBA=skilled birth attendance. Mort=mortality. NN mort=neonatal mortality. NTDs=neglected tropical diseases. NCDs=non-communicable diseases. FP need met, mod=family planning need met, modern contraception. Adol=adolescent. UHC=universal health coverage. Air poll mort=mortality attributable to air pollution. WaSH=water, sanitation, and hygiene. IPV=intimate partner violence. HH air poll=household air pollution. Occ risk burden=burden attributable to occupational risks. PM2·5=fi ne particulate matter smaller than 2·5 μm.
–15–10
0–5
1520
30
40
50
60
70
105
25
35
45
55
65
75
Med
ian
abso
lute
chan
ge fo
r the
resc
aled
indi
cato
r
A All countries
SDG index
D
isaste
r
Stuntin
g
W
asting
O
verweight
MMR
SBA
Under-5
mort
NN m
ort
HIV
T
uberculosis
M
alaria
Hepatitis B
NTDs
NCDs
S
uicide
A
lcohol
R
oad injurie
s
FP need m
et, mod
A
dol birt
h rate
UHC tracer
A
ir poll m
ort
WaSH mort
P
oisons
Smoking
IP
V
Water
Sanitatio
n
Hygiene
HH air poll
O
cc ris
k burden
M
ean PM2·5
Violence
War
MDG in
dex
Non-MDG in
dex
SDG index
D
isaste
r
Stuntin
g
W
asting
O
verweight
MMR
SBA
Under-5
mort
NN m
ort
HIV
T
uberculosis
M
alaria
Hepatitis B
NTDs
NCDs
S
uicide
A
lcohol
R
oad injurie
s
FP need m
et, mod
A
dol birt
h rate
UHC tracer
A
ir poll m
ort
WaSH mort
P
oisons
Smoking
IP
V
Water
Sanitatio
n
Hygiene
HH air poll
O
cc ris
k burden
M
ean PM2·5
Violence
War
MDG in
dex
Non-MDG in
dex
B Low SDI
–15–10
0–5
1520
30
40
50
60
70
105
25
35
45
55
65
75
Med
ian
abso
lute
chan
ge fo
r the
resc
aled
indi
cato
r
C Low-middle SDI D Middle SDI
–15–10
0–5
1520
30
40
50
60
70
105
25
35
45
55
65
75
Med
ian
abso
lute
chan
ge fo
r the
resc
aled
indi
cato
r
E High-middle SDI F High SDI
Indices Goal 1Goal 2Goal 3
Goal 5Goal 6Goal 7
Goal 8Goal 11Goal 16
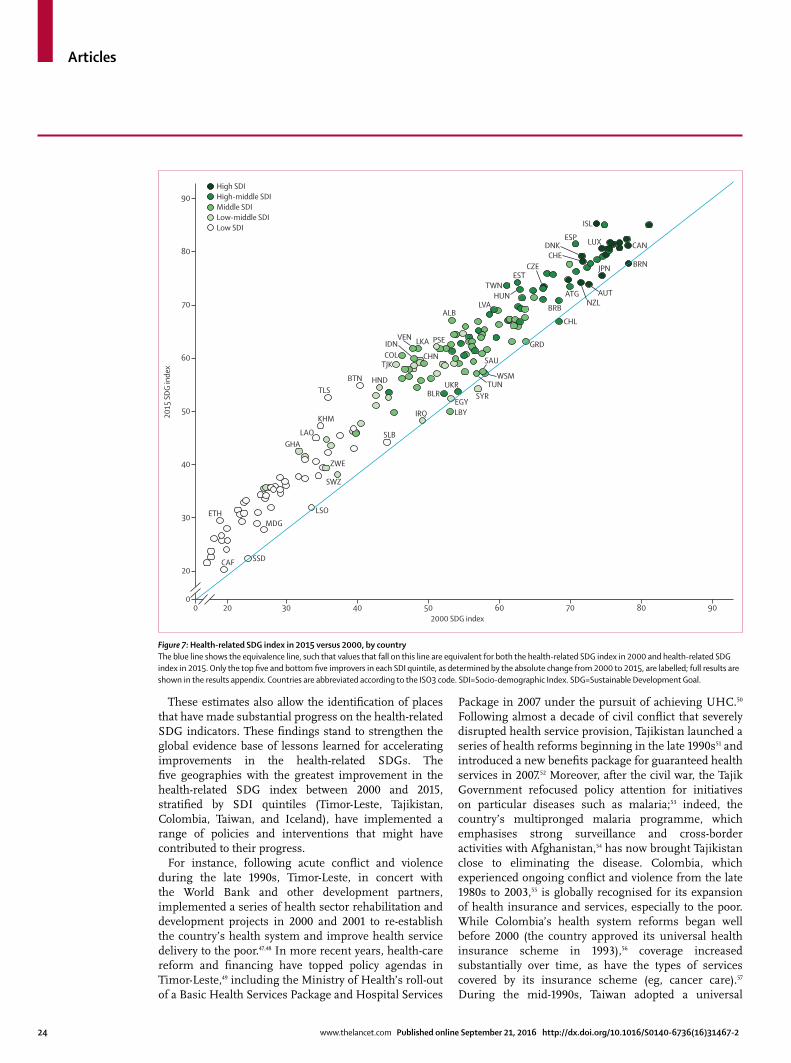
Articles
24 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
These estimates also allow the identifi cation of places that have made substantial progress on the health-related SDG indicators. These fi ndings stand to strengthen the global evidence base of lessons learned for accelerating improvements in the health-related SDGs. The fi ve geographies with the greatest improvement in the health-related SDG index between 2000 and 2015, stratifi ed by SDI quintiles (Timor-Leste, Tajikistan, Colombia, Taiwan, and Iceland), have implemented a range of policies and interventions that might have contributed to their progress.
For instance, following acute confl ict and violence during the late 1990s, Timor-Leste, in concert with the World Bank and other development partners, implemented a series of health sector rehabilitation and development projects in 2000 and 2001 to re-establish the country’s health system and improve health service delivery to the poor.47,48 In more recent years, health-care reform and fi nancing have topped policy agendas in Timor-Leste,49 including the Ministry of Health’s roll-out of a Basic Health Services Package and Hospital Services
Package in 2007 under the pursuit of achieving UHC.50 Following almost a decade of civil confl ict that severely disrupted health service provision, Tajikistan launched a series of health reforms beginning in the late 1990s51 and introduced a new benefi ts package for guaranteed health services in 2007.52 Moreover, after the civil war, the Tajik Government refocused policy attention for initiatives on particular diseases such as malaria;53 indeed, the country’s multipronged malaria programme, which emphasises strong surveillance and cross-border activities with Afghanistan,54 has now brought Tajikistan close to eliminating the disease. Colombia, which experienced ongoing confl ict and violence from the late 1980s to 2003,55 is globally recognised for its expansion of health insurance and services, especially to the poor. While Colombia’s health system reforms began well before 2000 (the country approved its universal health insurance scheme in 1993),56 coverage increased substantially over time, as have the types of services covered by its insurance scheme (eg, cancer care).57 During the mid-1990s, Taiwan adopted a universal
Figure 7: Health-related SDG index in 2015 versus 2000, by countryThe blue line shows the equivalence line, such that values that fall on this line are equivalent for both the health-related SDG index in 2000 and health-related SDG index in 2015. Only the top fi ve and bottom fi ve improvers in each SDI quintile, as determined by the absolute change from 2000 to 2015, are labelled; full results are shown in the results appendix. Countries are abbreviated according to the ISO3 code. SDI=Socio-demographic Index. SDG=Sustainable Development Goal.
0 20 30 40 50 60 70 80 900
20
30
40
50
60
70
80
90
ISL
ESP LUX
BRNJPN
AUTNZL
DNKCHE
TWNHUN
WSM
SAU
LKAVEN
TJK
HNDBTNTLS
KHM
LAOGHA
ZWE
SWZ
LSOMDG
SSDCAF
ETH
SLB
SYR
LBYIRQ
BLRUKR
EGY
LVA
TUN
PSE
CHN
ESTCZE
CAN
ATG
BRB
CHL
GRD
ALB
COL
2015
SDG
inde
x
2000 SDG index
High SDIHigh-middle SDIMiddle SDILow-middle SDILow SDI
IDN

Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 25
health insurance system,58 which is viewed as one of its most successful public entities. Taiwan also enacted many road safety laws between the mid-1990s and early 2000s, including mandatory helmet laws for motorcyclists in 1996 and an extension of seat belt laws to general roads in 2001.59 Iceland’s tobacco control policies have been viewed as some of the world’s most comprehensive,60 and the country’s long-standing publicly funded health system provides UHC,61 a factor that might have contributed to its declines in NCD mortality.
Such progress also highlights important interactions between development goals and wider contextual factors, such as post-confl ict experiences in Timor-Leste, Tajikistan, and Colombia, as well as a rebound in health following the dissolution of Soviet rule for Tajikistan. Furthermore, Taiwan’s gains underscore the interplay between advancing economic development and deliberate investments in improving UHC. These vignettes highlight only a fraction of the possible learning for informing action towards improving the health-related SDGs. An important future area of work will be to understand in detail how these and other high-performing geographies have achieved substantial improvements in key SDG indicators.
Besides showing the feasibility and value of measuring many of the health-related SDGs, our fi ndings also affi rm concerns voiced during the SDG development process and following the UN resolution. One criticism of the SDGs was the incredibly ambitious nature of some of the targets,5 such as Target 3.3, which calls for the end of the epidemics of HIV, tuberculosis, and malaria by 2030. Our analysis of these indicators in the past 15 years suggests that a substantial change in the present trajectory of HIV and tuberculosis incidence will be needed to meet this target, and major technological leaps coupled with universal delivery are likely to be necessary. The vague nature of many of the SDG targets has also been a common criticism;4,8,10,62 Of the 33 health-related SDG indicators in our study, we identifi ed specifi c targets for only 21 of them. The absence of specifi c and attainable targets for SDG indicators, health related or otherwise, undermines the usefulness of the SDGs in driving development agendas, a limitation that can and should be addressed at this early stage of the SDG period.
Our analysis also represents a step towards producing a more cohesive understanding of the interactions between diff erent SDG goals, targets, and indicators—a widely noted criticism.3,4 We show the potential for quantifying these interactions by comparing the relations between education, income, and fertility—components of the SDI—and the 33 health-related SDG indicators and accompanying health-related SDG, MDG, and non-MDG indices. Although we acknowledge the ecological nature of this analysis and its usual caveats, SDI was a strong predictor of the overall
health-related SDG and MDG indices, highlighting the general importance of income, education, and fertility, as well as intersectoral action for health-related development. However, SDI was a weaker predictor of the non-MDG index, particularly for indicators such as violence (intimate partner, interpersonal, and collective violence) and ambient particulate matter pollution. This fi nding shows that a sole focus on increasing income and education and decreasing fertility is probably insuffi cient to meet the SDG targets. It also raises questions about whether other common drivers, analogous to income, education, and fertility, can be determined and their relations with SDG indicators assessed. Combining this initial assessment of the 33 health-related SDG indicators with an expanded quantifi cation and analysis of other potential drivers is an important future area of work that could help to create a more concise, cohesive, and actionable monitoring framework for the SDGs.
Future directions for GBD monitoring eff ortsIn this report, we focused on measuring indicators proposed by the IAEG-SDGs. In future years, we plan to address three related sets of issues: fi rst, improved assessment of the health-related SDG indicators measured at present; second, inclusion of the 14 currently excluded health-related indicators in the annualised GBD study; and third, potential expansion of indicators consistent with the framing of the targets. We address each of these issues in turn.
Improving the measurement of currently included health-related indicatorsWith the present analysis, we made several modifi cations that we believe improve several health-related indicators for the purposes of measuring progress towards each health-related SDG target. Future iterations are likely to incorporate further modifi cations to these and other indicators. First, as noted in the Methods section, rather than reporting on the combined prevalence of childhood wasting and overweight, we assessed and measured them separately. Our results support this decision, since they had divergent relations over time (ie, childhood wasting improved for most countries, whereas the prevalence of childhood overweight generally increased) and with SDI (ie, childhood wasting and overweight were negatively and positively correlated with SDI, respectively).
Second, the IAEG-SDGs’ proposed indicator for harmful use of alcohol is the average national-level consumption per person in litres of pure alcohol. The health and non-health risks associated with harmful alcohol use are a function of not only average consumption at the population level but also use patterns (ie, amount consumed at a given time and frequency of consumption). For this analysis, we reported on the summary exposure value of harmful alcohol use, which

Articles
26 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
takes into account the distribution of consumption and the prevalence of binge drinking.39
Third, we made two modifi cations to the measurement of disaster (Indicators 1.5.1, 11.5.1, and 13.1.2). For mortality attributable to disasters, we chose to report on the lagged 5 year average of disaster mortality. One of the corresponding health-related SDG targets (Target 1.5) is to “build the resilience of the poor and those in vulnerable situations and reduce their exposure and vulnerability to climate-related extreme events and other economic, social and environmental shocks and disasters”. Focusing solely on the observed mortality caused by natural disaster ignores the role of chance in the occurrence of natural disasters; for example, nations with weak resilience to natural disasters might not experience a natural disaster during a given period of time, whereas those with strong resilience might encounter them more frequently. Taking the moving average of disaster mortality lessens the contribution of chance in assessing progress for this indicator. Nonetheless, this adjustment cannot account for background risk of natural disasters, which varies by geography, and future research eff orts could include developing a risk-standardised version of the indicator. For natural disasters, data on missing people and people aff ected by disaster are not readily available across countries and over time.
Fourth, for occupational health (Indicator 8.8.1), we reported on age-standardised all-cause DALY rate attributable to occupational risks rather than the suggested indicator, which is limited to fatal and non-fatal occupational injuries. This revision captures a wider set of occupational risks instead of only those that result in injuries, which supports the stated target of promotion of “safe and secure working environments for all workers” (Target 8.8). Fifth, for tobacco use prevalence (Indicator 3.a.1), GBD does not presently assess smokeless tobacco use. Furthermore, smokeless tobacco use has a notably diff erent risk profi le to smoked tobacco use,63 and thus it might warrant a subindicator akin to childhood malnutrition. Sixth, for clean fuels and technology (Indicator 7.1.2), we presently use a more limited defi nition that covers fuels used primarily for household cooking. Seventh, for homicide (Indicator 16.1.1), GBD does not measure this indicator by displacement or migratory status, and similarly for confl ict-related deaths (Indicator 16.1.2), we do not measure deaths by displacement status or by more specifi ed causes.
Eighth, data gaps also account for limitations in the estimation of the UHC tracer indicator (Indicator 3.8.1). We used a set of tracer interventions that were restricted to reproductive, maternal, and child health, as well as a subset of infectious diseases. There is a paucity of data for the coverage of NCD interventions in particular64–67 and for higher-level care. Furthermore, the UHC tracer indicator only captures the use of interventions and not the quality of the intervention provided.68,69 As more data
become available on the delivery of interventions for NCDs and the modifi cation of key risk factors, this information will be incorporated into revisions of the UHC tracer indicator. Finally, data gaps mean that, in this initial assessment, we have also not been able to include a measure of fi nancial risk protection. Substantial investments are needed in this area to address data gaps to be able to track the central role of health system delivery in improving health.
Indicators not presently measuredOf the 14 health-related SDG indicators that were not included in this analysis, there are several that the GBD does not currently measure but that could be assessed in the future through GBD (table 2). These indicators include the coverage of treatment interventions for substance use disorders (Indicator 3.5.1), which would leverage the work on quantifying incidence, prevalence, and mortality for these conditions. Estimating the proportion of women and girls aged 15 years and older who are subjected to sexual violence by people other than an intimate partner (Indicator 5.2.2) would leverage work already undertaken by GBD on measuring prevalence of intimate partner violence. As part of GBD, we have also assembled a host of population-level data that would facilitate measurement of the coverage of health insurance or public health systems (Indicator 3.8.2), health worker density and distribution (Indicator 3.c.1), and completeness of death registration (Indicator 17.19.2). Other indicators are more diffi cult to measure because of data gaps or unclear defi nitions. For example, data sources to measure the proportion of people that feel safe walking alone around the area they live (Indicator 16.1.4) are not readily available for most countries.
Strengthening the indicators for selected targetsVarious commentaries have pointed out the absence of indicators for key health outcomes and determinants. Proponents have argued for indicators for mental health that go beyond substance abuse disorders and suicide;14–16 other NCDs beyond cardiovascular diseases, cancer, diabetes, and chronic respiratory diseases;70 diseases related to ageing, including osteoarthritis and Alzheimer’s disease;71,72 non-fatal disorders that lead to substantial morbidity (eg, sensory disorders); and a host of major risk factors. Another example is Target 3.3, which aims to combat hepatitis—the indicator only tracks hepatitis B, although the data for hepatitis C monitoring are as robust as those for hepatitis B and a highly eff ective cure for hepatitis C is available. As shown in this report, our GBD collaboration provides the basis for measuring many of these indicators. The danger is that an exhaustive laundry list of indicators, a criticism already levelled at the present SDG list, would dilute the value of the SDGs in focusing attention on where it is most needed.

Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 27
Comparison with other assessmentsThere are several important similarities and diff erences between our assessment of the health-related SDGs and those produced by WHO18 and the Sustainable Development Solutions Network (SDSN).17 Like WHO, we focused on the health-related SDG indicators and did not cover indicators across all goals as SDSN does. With our focus on health, we covered 33 health-related indicators, compared with 21 by SDSN and 32 by WHO. Similar to SDSN, we produced a summary measure for the health-related SDG indicators included in the analysis. Most importantly, GBD uses standardised and internally consistent approaches to generate estimates across causes, risk factors, and underlying indicators. For example, we constrain the aggregation of cause-specifi c deaths to equal all-cause deaths. Furthermore, GBD also produces a complete set of estimates for 188 countries and for individual years from 1990 to 2015. By contrast, WHO and SDSN draw on disparate sources and methods for estimation and, as a result, report on an incomplete set of estimates by country. SDSN provides estimates for 149 countries, whereas estimates for health-related SDG indicators produced by WHO range from 194 countries for under-5 mortality and neonatal mortality to 109 countries for HIV incidence. WHO and SDSN also do not generate estimates for a consistent set of years. WHO reports 2015 estimates for only seven indicators and combines data from a range of years for ten indicators; for example, WHO combined skilled birth attendance estimates by country ranging from 2006 to 2014. SDSN reports 2015 estimates for only four indicators and combines data from a range of years for eight indicators; for example, country estimates for smoking prevalence from the SDSN report range from 2006 to 2013. Complete, consistent, comparable, and contemporary estimates of health-related SDG indicators are necessary to properly track progress on the SDGs.
LimitationsThis study has several limitations in addition to the ones we already described. First, all the limitations of GBD relevant to the 33 indicators used here apply.34,37–39 Second, we tried to summarise the complexity of the 33 indicators using a summary measure for the health-related SDGs. Many approaches are available for developing summary measures. Since the SDGs are the outcome of a political consensus building process, we opted to use the stated targets as preferences of UN member states that have agreed to the SDG declaration. Our sensitivity analysis shows that using alternative weighting schemes produces broadly similar results (methods appendix pp 312–13). Our sensitivity analysis also highlights the limitation of the statistical approach (ie, principal component analysis) for constructing an index for this purpose, with the fi rst principal component including both positive correlations with indicators such as maternal mortality ratio and negative correlations with indicators such as alcohol use.
An alternative could be to weight each indicator by their contribution to healthy life expectancy. Third, we opted to construct the summary measure using the Human Development Index method of rescaling each component on a scale of 0 to 100, and then taking the geometric mean of the components. We chose to use the minimum and maximum observed values to rescale, as targets for all indicators are not clearly specifi ed; however, the limitation of this approach is that minimum and maximum values might change in the future. In the next iteration of this analysis, we will use targets for all indicators and rescale them accordingly; to establish targets for indicators currently lacking explicit ones, we will determine plausible targets based on forecasts of trends through 2030. Fourth, a clear limitation, as highlighted by the UHC tracer indicator, is the need for broad investment in data systems in countries to properly assess progress on key health and development indicators such as the SDGs. As an example, there remains considerable uncertainty about levels and age patterns of mortality and the cause of death structure.34 Investments in high-quality vital registration systems and other related data collection systems, from censuses and household surveys to health management information systems, are crucial to the proper monitoring of progress towards the SDGs.
Our GBD collaboration aims to address several of the limitations noted above in future reporting of the health-related SDGs on an annual cycle. As noted, we will also leverage work that is underway to forecast country-specifi c disease burden, which will additionally provide information on the future trajectory of health-related SDG indicators based on historical trends and provide an explicit way to understand how those trajectories could be changed with diff erent policy adoption. We will also address, in a staged manner, the absence of measures of geographical and socioeconomic inequality in the health-related SDG indicators.
ConclusionsThe measurement of 33 health-related SDG indicators presented here is the product of an extensive, open collaboration that represents many countries across a broad range of development. We invite others to join in this eff ort to produce an independent, robust basis for monitoring and assessing progress towards the SDGs. Independent measurement is a crucial component of accountability, but it is not the only component. These results should ideally be used as the basis for review and action at the country level. We hope that this collaboration is a major contribution to creating a culture of accountability for the SDGs. Other actors, especially governments, civil society organisations, donors, and global development institutions, need to participate in the process of using this information to enhance accountability through open and transparent review and action.
Articles
28 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
GBD 2015 SDG CollaboratorsStephen S Lim, Kate Allen, Zulfi qar A Bhutta, Lalit Dandona, Mohammad H Forouzanfar, Nancy Fullman, Peter W Gething, Ellen M Goldberg, Simon I Hay, Mollie Holmberg, Yohannes Kinfu, Michael J Kutz, Heidi J Larson, Xiaofeng Liang, Alan D Lopez, Rafael Lozano, Claire R McNellan, Ali H Mokdad, Meghan D Mooney, Mohsen Naghavi, Helen E Olsen, David M Pigott, Joshua A Salomon, Theo Vos, Haidong Wang, Amanuel Alemu Abajobir*, Kalkidan Hassen Abate*, Cristiana Abbafati*, Kaja M Abbas*, Foad Abd-Allah*, Abdishakur M Abdulle*, Biju Abraham*, Ibrahim Abubakar*, Laith J Abu-Raddad*, Niveen M E Abu-Rmeileh*, Gebre Yitayih Abyu*, Tom Achoki*, Akindele Olupelumi Adebiyi*, Isaac Akinkunmi Adedeji*, Kossivi Agbelenko Afanvi*, Ashkan Afshin*, Arnav Agarwal*, Anurag Agrawal*, Aliasghar Ahmad Kiadaliri*, Hamid Ahmadieh*, Kedir Yimam Ahmed*, Ali Shafqat Akanda*, Rufus Olusola Akinyemi*, Tomi F Akinyemiju*, Nadia Akseer*, Ziyad Al-Aly*, Khurshid Alam*, Uzma Alam*, Deena Alasfoor*, Fadia S AlBuhairan*, Saleh Fahed Aldhahri*, Robert William Aldridge*, Zewdie Aderaw Alemu*, Raghib Ali*, Ala’a Alkerwi*, Mohammad AB Alkhateeb*, François Alla*, Peter Allebeck*, Christine Allen*, Rajaa Al-Raddadi*, Khalid A Altirkawi*, Elena Alvarez Martin*, Nelson Alvis-Guzman*, Azmeraw T Amare*, Alemayehu Amberbir*, Adeladza Kofi Amegah*, Heresh Amini*, Walid Ammar*, Stephen Marc Amrock*, Hjalte H Andersen*, Benjamin O Anderson*, Gregory M Anderson*, Carl Abelardo T Antonio*, Palwasha Anwari*, Johan Ärnlöv*, Al Artaman*, Hamid Asayesh*, Rana Jawad Asghar*, Suleman Atique*, Euripide Frinel G Arthur Avokpaho*, Ashish Awasthi*, Beatriz Paulina Ayala Quintanilla*, Peter Azzopardi*, Umar Bacha*, Alaa Badawi*, Kalpana Balakrishnan*, Amitava Banerjee*, Aleksandra Barac*, Ryan Barber*, Suzanne L Barker-Collo*, Till Bärnighausen*, Lope H Barrero*, Tonatiuh Barrientos-Gutierrez*, Sanjay Basu*, Tigist Assefa Bayou*, Shahrzad Bazargan-Hejazi*, Justin Beardsley*, Neeraj Bedi*, Ettore Beghi*, Yannick Béjot*, Michelle L Bell*, Aminu K Bello*, Derrick A Bennett*, Isabela M Bensenor*, Habib Benzian*, Adugnaw Berhane*, Eduardo Bernabé*, Oscar Alberto Bernal*, Balem Demtsu Betsu*, Addisu Shunu Beyene*, Neeraj Bhala*, Samir Bhatt*, Sibhatu Biadgilign*, Kelly A Bienhoff *, Boris Bikbov*, Agnes Binagwaho*, Donal Bisanzio*, Espen Bjertness*, Jed Blore*, Rupert R A Bourne*, Michael Brainin*, Michael Brauer*, Alexandra Brazinova*, Nicholas J K Breitborde*, David M Broday*, Traolach S Brugha*, Rachelle Buchbinder*, Zahid A Butt*, Leah E Cahill*, Ismael Ricardo Campos-Nonato*, Julio Cesar Campuzano*, Hélène Carabin*, Rosario Cárdenas*, Juan Jesus Carrero*, Austin Carter*, Daniel Casey*, Valeria Caso*, Carlos A Castañeda-Orjuela*, Jacqueline Castillo Rivas*, Ferrán Catalá-López*, Fiorella Cavalleri*, Pedro Cecílio*, Hsing-Yi Chang*, Jung-Chen Chang*, Fiona J Charlson*, Xuan Che*, Alan Zian Chen*, Peggy Pei-Chia Chiang*, Mirriam Chibalabala*, Vesper Hichilombwe Chisumpa*, Jee-Young Jasmine Choi*, Rajiv Chowdhury*, Hanne Christensen*, Liliana G Ciobanu*, Massimo Cirillo*, Matthew M Coates*, Megan Coggeshall*, Aaron J Cohen*, Graham S Cooke*, Cyrus Cooper*, Leslie Trumbull Cooper*, Benjamin C Cowie*, John A Crump*, Solomon Abrha Damtew*, Rakhi Dandona*, Paul I Dargan*, José das Neves*, Adrian C Davis*, Kairat Davletov*, E Filipa de Castro*, Diego De Leo*, Louisa Degenhardt*, Liana C Del Gobbo*, Kebede Deribe*, Sarah Derrett*, Don C Des Jarlais*, Aniruddha Deshpande*, Gabrielle A deVeber*, Subhojit Dey*, Samath D Dharmaratne*, Preet K Dhillon*, Eric L Ding*, E Ray Dorsey*, Kerrie E Doyle*, Tim R Driscoll*, Leilei Duan*, Manisha Dubey*, Bruce Bartholow Duncan*, Hedyeh Ebrahimi*, Aman Yesuf Endries*, Sergey Petrovich Ermakov*, Holly E Erskine*, Babak Eshrati*, Alireza Esteghamati*, Saman Fahimi*, Talha A Farid*, Carla Sofi a e Sa Farinha*, André Faro*, Maryam S Farvid*, Farshad Farzadfar*, Valery L Feigin*, Manuela Mendonca Felicio*, Seyed-Mohammad Fereshtehnejad*, Jeff erson G Fernandes*, Joao C Fernandes*, Alize J Ferrari*, Florian Fischer*, Joseph R A Fitchett*, Christina Fitzmaurice*, Nataliya Foigt*, Kyle Foreman*, F Gerry R Fowkes*, Elisabeth Barboza Franca*,
Richard C Franklin*, Maya Fraser*, Joseph Friedman*, Joseph Frostad*, Thomas Fürst*, Belinda Gabbe*, Alberto L Garcia-Basteiro*, Teshome Gebre*, Tsegaye Tewelde Gebrehiwot*, Amanuel Tesfay Gebremedhin*, Alemseged Aregay Gebru*, Bradford D Gessner*, Richard F Gillum*, Ibrahim Abdelmageem Mohamed Ginawi*, Ababi Zergaw Giref*, Maurice Giroud*, Melkamu Dedefo Gishu*, William Godwin*, Philimon Gona*, Amador Goodridge*, Sameer Vali Gopalani*, Carolyn C Gotay*, Atsushi Goto*, Hebe N Gouda*, Nicholas Graetz*, Karen Fern Greenwell*, Max Griswold*, Yuming Guo*, Rahul Gupta*, Rajeev Gupta*, Vipin Gupta*, Reyna A Gutiérrez*, Bishal Gyawali*, Juanita A Haagsma*, Annie Haakenstad*, Nima Hafezi-Nejad*, Demewoz Haile*, Gessessew Bugssa Hailu*, Yara A Halasa*, Randah Ribhi Hamadeh*, Samer Hamidi*, Mouhanad Hammami*, Graeme J Hankey*, Hilda L Harb*, Josep Maria Haro*, Mohammad Sadegh Hassanvand*, Rasmus Havmoeller*, Ileana Beatriz Heredia-Pi*, Hans W Hoek*, Masako Horino*, Nobuyuki Horita*, H Dean Hosgood*, Damian G Hoy*, Aung Soe Htet*, Guoqing Hu*, Hsiang Huang*, Kim Moesgaard Iburg*, Bulat T Idrisov*, Manami Inoue*, Farhad Islami*, Troy A Jacobs*, Kathryn H Jacobsen*, Nader Jahanmehr*, Mihajlo B Jakovljevic*, Peter James*, Henrica A F M Jansen*, Mehdi Javanbakht*, Achala Upendra Jayatilleke*, Sun Ha Jee*, Panniyammakal Jeemon*, Vivekanand Jha*, Ying Jiang*, Tariku Jibat*, Ye Jin*, Jost B Jonas*, Zubair Kabir*, Yogeshwar Kalkonde*, Ritul Kamal*, Haidong Kan*, Amit Kandel*, André Karch*, Corine Kakizi Karema*, Chante Karimkhani*, Palitha Karunapema*, Amir Kasaeian*, Nicholas J Kassebaum*, Anil Kaul*, Norito Kawakami*, Jeanne Françoise Kayibanda*, Peter Njenga Keiyoro*, Laura Kemmer*, Andrew Haddon Kemp*, Andre Pascal Kengne*, Andre Keren*, Chandrasekharan Nair Kesavachandran*, Yousef Saleh Khader*, Abdur Rahman Khan*, Ejaz Ahmad Khan*, Gulfaraz Khan*, Young-Ho Khang*, Tawfi k Ahmed Muthafer Khoja*, Ardeshir Khosravi*, Jagdish Khubchandani*, Christian Kieling*, Cho-il Kim*, Daniel Kim*, Sungroul Kim*, Yun Jin Kim*, Ruth W Kimokoti*, Niranjan Kissoon*, Miia Kivipelto*, Luke D Knibbs*, Yoshihiro Kokubo*, Dhaval Kolte*, Soewarta Kosen*, Georgios A Kotsakis*, Parvaiz A Koul*, Ai Koyanagi*, Michael Kravchenko*, Hans Krueger*, Barthelemy Kuate Defo*, Ricardo S Kuchenbecker*, Ernst J Kuipers*, Xie Rachel Kulikoff *, Veena S Kulkarni*, G Anil Kumar*, Gene F Kwan*, Hmwe H Kyu*, Aparna Lal*, Dharmesh Kumar Lal*, Ratilal Lalloo*, Hilton Lam*, Qing Lan*, Sinead M Langan*, Anders Larsson*, Dennis Odai Laryea*, Asma Abdul Latif*, Janet L Leasher*, James Leigh*, Mall Leinsalu*, Janni Leung*, Ricky Leung*, Miriam Levi*, Yichong Li*, Yongmei Li*, Margaret Lind*, Shai Linn*, Steven E Lipshultz*, Patrick Y Liu*, Shiwei Liu*, Yang Liu*, Belinda K Lloyd*, Loon-Tzian Lo*, Giancarlo Logroscino*, Paulo A Lotufo*, Robyn M Lucas*, Raimundas Lunevicius*, Mohammed Magdy Abd El Razek*, Carlos Magis-Rodriguez*, Mahdi Mahdavi*, Marek Majdan*, Azeem Majeed*, Reza Malekzadeh*, Deborah Carvalho Malta*, Chabila C Mapoma*, David Joel Margolis*, Randall V Martin*, Jose Martinez-Raga*, Felix Masiye*, Amanda J Mason-Jones*, João Massano*, Richard Matzopoulos*, Bongani M Mayosi*, John J McGrath*, Martin McKee*, Peter A Meaney*, Alem Mehari*, Alemayehu B Mekonnen*, Yohannes Adama Melaku*, Peter Memiah*, Ziad A Memish*, Walter Mendoza*, Gert B M Mensink*, Atte Meretoja*, Tuomo J Meretoja*, Yonatan Moges Mesfi n*, Francis Apolinary Mhimbira*, Renata Micha*, Ted R Miller*, Edward J Mills*, Mojde Mirarefi n*, Awoke Misganaw*, Philip B Mitchell*, Charles N Mock*, Alireza Mohammadi*, Shafi u Mohammed*, Lorenzo Monasta*, Jonathan de la Cruz Monis*, Julio Cesar Montañez Hernandez*, Marcella Montico*, Maziar Moradi-Lakeh*, Lidia Morawska*, Rintaro Mori*, Ulrich O Mueller*, Michele E Murdoch*, Brighton Murimira*, Joseph Murray*, Gudlavalleti Venkata Satyanarayana Murthy*, Srinivas Murthy*, Kamarul Imran Musa*, Jean B Nachega*, Gabriele Nagel*, Kovin S Naidoo*, Luigi Naldi*, Vinay Nangia*, Bruce Neal*, Chakib Nejjari*, Charles R Newton*, John N Newton*, Frida Namnyak Ngalesoni*, Peter Nguhiu*, Grant Nguyen*,
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 29
Quyen Le Nguyen*, Muhammad Imran Nisar*, Patrick Martial Nkamedjie Pete*, Sandra Nolte*, Marika Nomura*, Ole F Norheim*, Bo Norrving*, Carla Makhlouf Obermeyer*, Felix Akpojene Ogbo*, In-Hwan Oh*, Olanrewaju Oladimeji*, Pedro R Olivares*, Bolajoko Olubukunola Olusanya*, Jacob Olusegun Olusanya*, John Nelson Opio*, Eyal Oren*, Alberto Ortiz*, Richard H Osborne*, Erika Ota*, Mayowa O Owolabi*, Mahesh PA*, Eun-Kee Park*, Hye-Youn Park*, Charles D Parry*, Mahboubeh Parsaeian*, Tejas Patel*, Vikram Patel*, Angel J Paternina Caicedo*, Snehal T Patil*, Scott B Patten*, George C Patton*, Deepak Paudel*, João Mário Pedro*, David M Pereira*, Norberto Perico*, Konrad Pesudovs*, Max Petzold*, Michael Robert Phillips*, Frédéric B Piel*, Julian David Pillay*, Christine Pinho*, Farhad Pishgar*, Suzanne Polinder*, Richie G Poulton*, Farshad Pourmalek*, Mostafa Qorbani*, Rynaz H S Rabiee*, Amir Radfar*, Vafa Rahimi-Movaghar*, Mahfuzar Rahman*, Mohammad Hifz Ur Rahman*, Sajjad Ur Rahman*, Rajesh Kumar Rai*, Sasa Rajsic*, Murugesan Raju*, Usha Ram*, Saleem M Rana*, Chhabi Lal Ranabhat*, Kavitha Ranganathan*, Puja C Rao*, Amany H Refaat*, Marissa B Reitsma*, Giuseppe Remuzzi*, Serge Resnikoff *, Antonio L Ribeiro*, Maria Jesus Rios Blancas*, Hirbo Shore Roba*, Bayard Roberts*, Alina Rodriguez*, David Rojas-Rueda*, Luca Ronfani*, Gholamreza Roshandel*, Gregory A Roth*, Dietrich Rothenbacher*, Ambuj Roy*, Nobhojit Roy*, Ben Benasco Sackey*, Rajesh Sagar*, Muhammad Muhammad Saleh*, Juan R Sanabria*, Damian F Santomauro*, Itamar S Santos*, Rodrigo Sarmiento-Suarez*, Benn Sartorius*, Maheswar Satpathy*, Miloje Savic*, Monika Sawhney*, Susan M Sawyer*, Josef Schmidhuber*, Maria Inês Schmidt*, Ione J C Schneider*, Aletta E Schutte*, David C Schwebel*, Soraya Seedat*, Sadaf G Sepanlou*, Edson E Servan-Mori*, Katya Shackelford*, Amira Shaheen*, Masood Ali Shaikh*, Teresa Shamah Levy*, Rajesh Sharma*, Jun She*, Sara Sheikhbahaei*, Jiabin Shen*, Kevin N Sheth*, Muki Shey*, Peilin Shi*, Kenji Shibuya*, Mika Shigematsu*, Min-Jeong Shin*, Rahman Shiri*, Kawkab Shishani*, Ivy Shiue*, Inga Dora Sigfusdottir*, Naris Silpakit*, Diego Augusto Santos Silva*, Jonathan I Silverberg*, Edgar P Simard*, Shireen Sindi*, Abhishek Singh*, Gitanjali M Singh*, Jasvinder A Singh*, Om Prakash Singh*, Prashant Kumar Singh*, Vegard Skirbekk*, Amber Sligar*, Samir Soneji*, Kjetil Søreide*, Reed J D Sorensen*, Joan B Soriano*, Sergey Soshnikov*, Luciano A Sposato*, Chandrashekhar T Sreeramareddy*, Hans-Christian Stahl*, Jeff rey D Stanaway*, Vasiliki Stathopoulou*, Nadine Steckling*, Nicholas Steel*, Dan J Stein*, Caitlyn Steiner*, Heidi Stöckl*, Saverio Stranges*, Mark Strong*, Jiandong Sun*, Bruno F Sunguya*, Patrick Sur*, Soumya Swaminathan*, Bryan L Sykes*, Cassandra E I Szoeke*, Rafael Tabarés-Seisdedos*, Karen M Tabb*, Roberto Tchio Talongwa*, Mohammed Rasoul Tarawneh*, Mohammad Tavakkoli*, Bineyam Taye*, Hugh R Taylor*, Bemnet Amare Tedla*, Worku Tefera*, Teketo Kassaw Tegegne*, Dejen Yemane Tekle*, Girma Temam Shifa*, Abdullah Sulieman Terkawi*, Gizachew Assefa Tessema*, J S Thakur*, Alan J Thomson*, Andrew L Thorne-Lyman*, Amanda G Thrift*, George D Thurston*, Taavi Tillmann*, Ruoyan Tobe-Gai*, Marcello Tonelli*, Roman Topor-Madry*, Fotis Topouzis*, Bach Xuan Tran*, Zacharie Tsala Dimbuene*, Abera Kenay Tura*, Emin Murat Tuzcu*, Stefanos Tyrovolas*, Kingsley Nnanna Ukwaja*, Eduardo A Undurraga*, Chigozie Jesse Uneke*, Olalekan A Uthman*, Aaron van Donkelaar*, Yuri Y Varakin*, Tommi Vasankari*, Ana Maria Nogales Vasconcelos*, J Lennert Veerman*, Narayanaswamy Venketasubramanian*, Raj Kumar Verma*, Francesco S Violante*, Vasiliy Victorovich Vlassov*, Patricia Volkow*, Stein Emil Vollset*, Gregory R Wagner*, Mitchell T Wallin*, Linhong Wang*, Valentine Wanga*, David A Watkins*, Scott Weichenthal*, Elisabete Weiderpass*, Robert G Weintraub*, Daniel J Weiss*, Andrea Werdecker*, Ronny Westerman*, Harvey A Whiteford*, James D Wilkinson*, Charles Shey Wiysonge*, Charles D A Wolfe*, Ingrid Wolfe*, Sungho Won*, Anthony D Woolf*, Shimelash Bitew Workie*, Mamo Wubshet*, Gelin Xu*, Ajit Kumar Yadav*, Bereket Yakob*, Ayalnesh Zemene Yalew*, Lijing L Yan*, Yuichiro Yano*, Mehdi Yaseri*, Pengpeng Ye*, Paul Yip*,
Naohiro Yonemoto*, Seok-Jun Yoon*, Mustafa Z Younis*, Chuanhua Yu*, Zoubida Zaidi*, Maysaa El Sayed Zaki*, Carlos Zambrana-Torrelio*, Tomas Zapata*, Elias Asfaw Zegeye*, Yi Zhao*, Maigeng Zhou*, Sanjay Zodpey*, David Zonies*, Christopher J L Murray†. *Authors listed alphabetically. †Corresponding author.
Affi liationsInstitute for Health Metrics and Evaluation (Prof S S Lim PhD, K Allen BA, Prof L Dandona MD, M H Forouzanfar MD, N Fullman MPH, E M Goldberg BSc, Prof S I Hay DSc, M Holmberg BS, M J Kutz BS, H J Larson PhD, Prof A D Lopez PhD, C R McNellan BA, Prof A H Mokdad PhD, M D Mooney BS, Prof M Naghavi PhD, H E Olsen MA, D M Pigott DPhil, Prof T Vos PhD, H Wang PhD, T Achoki MD, A Afshin MD, C Allen BA, G M Anderson MSEE, R Barber BS, K A Bienhoff MA, J Blore PhD, Prof M Brauer ScD, A Carter BS, D Casey BA, F J Charlson PhD, A Z Chen BS, M M Coates MPH, M Coggeshall BA, A J Cohen DSc, A Deshpande MPH, H E Erskine PhD, A J Ferrari PhD, C Fitzmaurice MD, K Foreman PhD, M Fraser BA, J Friedman BA, J Frostad MPH, W Godwin BS, N Graetz MPH, M Griswold MS, J A Haagsma PhD, A Haakenstad MA, N J Kassebaum MD, L Kemmer PhD, X R Kulikoff BA, H H Kyu PhD, J Leung PhD, M Lind BS, P Y Liu BA, F Masiye PhD, M Mirarefi n MPH, A Misganaw PhD, M Moradi-Lakeh MD, G Nguyen MPH, C Pinho BA, P C Rao MPH, M B Reitsma BS, G A Roth MD, D F Santomauro PhD, K Shackelford BA, N Silpakit BS, A Sligar MPH, R J D Sorensen MPH, J D Stanaway PhD, C Steiner MPH, P Sur BA, Prof S E Vollset DrPH, V Wanga MS, Prof H A Whiteford PhD, Y Zhao MS, Prof M Zhou PhD, Prof C J L Murray DPhil), School of Dentistry (G A Kotsakis DDS), Harborview Injury Prevention and Research Center (C N Mock PhD), University of Washington, Seattle, WA, USA (Prof B O Anderson MD, D A Watkins MD); Centre of Excellence in Women and Child Health (Z A Bhutta PhD), Aga Khan University, Karachi, Pakistan (M I Nisar MSc); Centre for Global Child Health, The Hospital for Sick Children, Toronto, ON, Canada (Z A Bhutta PhD, N Akseer MSc, G A deVeber MD); Centre for Control of Chronic Conditions (P Jeemon PhD), Public Health Foundation of India, New Delhi, India (Prof L Dandona MD, R Dandona PhD, G A Kumar PhD); Department of Zoology (P W Gething PhD), Nuffi eld Department of Medicine (D Bisanzio PhD), NIHR Musculoskeletal Biomedical Research Centre (Prof C Cooper FMedSci), University of Oxford, Oxford, UK (R Ali FRCP, D A Bennett PhD, Prof V Jha DM, D J Weiss PhD); Centre for Research & Action in Public Health, Faculty of Health, University of Canberra, Canberra, ACT, Australia (Y Kinfu PhD); Department of Infectious Disease Epidemiology (H J Larson PhD), Centre for Global Mental Health (Prof V Patel PhD), London School of Hygiene and Tropical Medicine, London, UK (S M Langan PhD, Prof M McKee DSc, Prof G V S Murthy MD, B Roberts PhD, H Stöckl DPhil); National Center for Chronic and Noncommunicable Disease Control and Prevention (L Duan MD, Y Jin MS, Y Li MPH, S Liu PhD, Prof L Wang MD, P Ye MPH, Prof M Zhou PhD), Chinese Center for Disease Control and Prevention, Beijing, China (Prof X Liang MD); Melbourne School of Population and Global Health (Prof A D Lopez PhD), Department of Paediatrics (P Azzopardi MEpi), The Peter Doherty Institute for Infection and Immunity (Prof B C Cowie PhD), Department of Medicine (A Meretoja PhD), Murdoch Childrens Research Institute (Prof G C Patton MD, K Alam PhD, P Azzopardi MEpi, R G Weintraub MBBS), Department of Pediatrics (Prof S M Sawyer MD), Institute of Health and Ageing (Prof C E I Szoeke PhD), The University of Melbourne, Melbourne, VIC, Australia (K Alam PhD, Prof H R Taylor AC, R G Weintraub MBBS); National Institute of Public Health, Cuernavaca, Mexico (R Lozano MD, T Barrientos-Gutierrez PhD, I R Campos-Nonato PhD, J C Campuzano PhD, I B Heredia-Pi PhD, J C Montañez Hernandez MSc, M J Rios Blancas MPH, Prof E E Servan-Mori MSc, T Shamah Levy PhD); Department of Global Health and Population, Harvard T H Chan School of Public Health (Prof J A Salomon PhD), Department of Global Health and Social Medicine, Harvard Medical School (Prof A Binagwaho PhD), Department of Epidemiology (P James ScD) Harvard T H Chan School of Public Health (Prof T Bärnighausen MD, L E Cahill PhD,
Articles
30 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
I R Campos-Nonato PhD, E L Ding ScD, M S Farvid PhD, A Haakenstad MA, G R Wagner MD), Department of Nutrition, Harvard T H Chan School of Public Health (A L Thorne-Lyman ScD), Channing Division of Network Medicine, Brigham & Women’s Hospital, Harvard Medical School (P James ScD), Harvard University, Boston, MA, USA (J R A Fitchett MD); School of Public Health (A A Abajobir MPH, F J Charlson PhD, H E Erskine PhD, A J Ferrari PhD, L D Knibbs PhD, J Leung PhD, D F Santomauro PhD, J L Veerman PhD, Prof H A Whiteford PhD), School of Dentistry (Prof R Lalloo PhD), University of Queensland, Brisbane, QLD, Australia (H N Gouda PhD, Y Guo PhD, Prof J J McGrath MD); Jimma University, Jimma, Ethiopia (K H Abate MS, T T Gebrehiwot MPH, A T Gebremedhin MPH); La Sapienza, University of Rome, Rome, Italy (C Abbafati PhD); Virginia Tech, Blacksburg, VA, USA (Prof K M Abbas PhD); Department of Neurology, Cairo University, Cairo, Egypt (Prof F Abd-Allah MD); New York University Abu Dhabi, Abu Dhabi, United Arab Emirates (A M Abdulle PhD); NMSM Government College Kalpetta, Kerala, India (Prof B Abraham MPhil); Institute for Global Health (Prof I Abubakar PhD, R W Aldridge PhD), Centre for Public Health Data Science, Institute of Health Informatics (R W Aldridge PhD), Farr Institute of Health Informatics Research (R W Aldridge PhD, A Banerjee DPhil), Department of Epidemiology and Public Health (H Benzian PhD, T Tillmann MSc), University College London, London, UK; Infectious Disease Epidemiology Group, Weill Cornell Medical College in Qatar, Doha, Qatar (L J Abu-Raddad PhD); Institute of Community and Public Health, Birzeit University, Ramallah, Palestine (N M Abu-Rmeileh PhD); School of Public Health (Y A Melaku MPH), Mekelle University, Mekelle, Ethiopia (Prof G Y Abyu MS, T A Bayou BS, B D Betsu MS, A A Gebru MPH, G B Hailu MSc, D Y Tekle MS, A Z Yalew MS); College of Medicine (A O Adebiyi MD), Department of Medicine (M O Owolabi Dr Med), University of Ibadan, Ibadan, Nigeria (R O Akinyemi PhD); University College Hospital, Ibadan, Nigeria (A O Adebiyi MD); Olabisi Onabanjo University, Ago-Iwoye, Nigeria (I A Adedeji MS); Direction du District Sanitaire de Haho, Notse, Togo (K A Afanvi MD); Faculte des Sciences de Sante, Universite de Lome, Lome, Togo (K A Afanvi MD); Friedman School of Nutrition Science and Policy (A Afshin MD, R Micha PhD), Tufts University, Boston, MA, USA (P Shi PhD, G M Singh PhD); Dalla Lana School of Public Health (N Akseer MSc), Department of Nutritional Sciences, Faculty of Medicine (A Badawi PhD), University of Toronto, Toronto, ON, Canada (A Agarwal BHSc); McMaster University, Hamilton, ON, Canada (A Agarwal BHSc); CSIR Institute of Genomics and Integrative Biology, Delhi, India (A Agrawal PhD); Department of Internal Medicine, Baylor College of Medicine, Houston, TX, USA (A Agrawal PhD); Department of Clinical Sciences Lund, Orthopedics, Clinical Epidemiology Unit (A Ahmad Kiadaliri PhD), Skane University Hospital, Department of Clinical Sciences Lund (Prof B Norrving PhD), Lund University, Lund, Sweden; Health Services Management Research Center, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran (A Ahmad Kiadaliri PhD); Ophthalmic Research Center (H Ahmadieh MD, M Yaseri PhD), School of Public Health (N Jahanmehr PhD), Shahid Beheshti University of Medical Sciences, Tehran, Iran; Department of Ophthalmology, Labbafi nejad Medical Center, Tehran, Iran (H Ahmadieh MD); Debre Markos University, Debre Markos, Ethiopia (K Y Ahmed MPH, Z A Alemu MPH, T K Tegegne MPH); University of Rhode Island, Kingston, RI, USA (A S Akanda PhD); Newcastle University, Newcastle upon Tyne, UK (R O Akinyemi PhD); Department of Epidemiology (T F Akinyemiju PhD), University of Alabama at Birmingham, Birmingham, AL, USA (D C Schwebel PhD, J A Singh MD); Washington University in Saint Louis, St Louis, MO, USA (Z Al-Aly MD); Sydney School of Public Health (Prof T R Driscoll PhD), The University of Sydney, Sydney, NSW, Australia (K Alam PhD, J Leigh PhD, A B Mekonnen MS, Prof B Neal PhD); International Center for Humanitarian Aff airs, Nairobi, Kenya (U Alam PhD); Ministry of Health, Al Khuwair, Oman (D Alasfoor MSc); King Abdullah Specialized Children’s Hospital, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia (F S AlBuhairan MD); King Abdullah International Medical Research Center, Riyadh, Saudi Arabia (F S AlBuhairan MD); King Khalid University Hospital (M A Alkhateeb BA), King Saud University, Riyadh, Saudi Arabia
(S F Aldhahri MD, K A Altirkawi MD); Department of Anesthesiology (A S Terkawi MD), King Fahad Medical City, Riyadh, Saudi Arabia (S F Aldhahri MD); Luxembourg Institute of Health (LIH), Strassen, Luxembourg (A Alkerwi PhD); School of Public Health, University of Lorraine, Nancy, France (Prof F Alla PhD); Department of Public Health Sciences (P Allebeck PhD, R H S Rabiee MPH, N Roy MD), Aging Research Center (Prof M Kivipelto PhD), Department of Clinical Science, Intervention and Technology (Prof J J Carrero PhD), Department of Neurobiology, Care Sciences and Society (NVS) (S M Fereshtehnejad PhD), Department of Medical Epidemiology and Biostatistics (E Weiderpass PhD), Karolinska Institutet, Stockholm, Sweden (R Havmoeller PhD, S Sindi PhD); Ministry of Health, Jeddah, Saudi Arabia (R Al-Raddadi PhD); Government, Madrid, Spain (E Alvarez Martin PhD); Universidad de Cartagena, Cartagena, Colombia (Prof N Alvis-Guzman PhD, A J Paternina Caicedo MD); School of Medicine (A T Amare MPH, Y A Melaku MPH), University of Adelaide, Adelaide, SA, Australia (L G Ciobanu MS, G A Tessema MPH); College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia (A T Amare MPH); Dignitas International, Zomba, Malawi (A Amberbir PhD); University of Cape Coast, Cape Coast, Ghana (A K Amegah PhD); Environmental Health Research Center, Kurdistan University of Medical Sciences, Sanandaj, Iran (H Amini MSPH); Department of Epidemiology and Public Health (H Amini MSPH, T Fürst PhD), Swiss Tropical and Public Health Institute, Basel, Switzerland (C K Karema MSc); Ministry of Public Health, Beirut, Lebanon (W Ammar PhD, H L Harb MPH); Oregon Health & Science University, Portland, OR, USA (S M Amrock MD); Center for Sensory-Motor Interaction, Department of Health Science and Technology, Faculty of Medicine, Aalborg University, Aalborg, Denmark (H H Andersen MSc); Department of Health Policy and Administration, College of Public Health, University of the Philippines Manila, Manila, Philippines (C A T Antonio MD); Self-employed, Kabul, Afghanistan (P Anwari MD); Department of Medical Sciences, Uppsala University, Uppsala, Sweden (Prof J Ärnlöv PhD, Prof A Larsson PhD); Dalarna University, Falun, Sweden (Prof J Ärnlöv PhD); University of Manitoba, Winnipeg, MB, Canada (A Artaman PhD); Department of Medical Emergency, School of Paramedic, Qom University of Medical Sciences, Qom, Iran (H Asayesh PhD); South Asian Public Health Forum, Islamabad, Pakistan (R J Asghar MD); Graduate Institute of Biomedical Informatics, Taipei Medical University, Taipei, Taiwan (S Atique MS); Institut de Recherche Clinique du Bénin, Cotonou, Benin Republic (E F G A Avokpaho MPH); Laboratoire d’Etudes et de Recherche-Action en Santé (LERAS Afrique), Parakou, Benin Republic (E F G A Avokpaho MPH); Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India (A Awasthi MSc); The Judith Lumley Centre for Mother, Infant and Family Health Research, La Trobe University, Melbourne, VIC, Australia (B P Ayala Quintanilla PhD); Peruvian National Institute of Health, Lima, Peru (B P Ayala Quintanilla PhD); Wardliparingga Aboriginal Research Unit, South Australian Health and Medical Research Institute, Adelaide, SA, Australia (P Azzopardi MEpi); Centre for International Health, Burnet Institute, Melbourne, VIC, Australia (P Azzopardi MEpi); School of Health Sciences, University of Management and Technology, Lahore, Pakistan (U Bacha PhD); Public Health Agency of Canada, Toronto, ON, Canada (A Badawi PhD); Department of Environmental Health Engineering, Sri Ramachandra University, Chennai, India (K Balakrishnan PhD); Faculty of Medicine, University of Belgrade, Belgrade, Serbia (A Barac PhD); School of Psychology, University of Auckland, Auckland, New Zealand (S L Barker-Collo PhD); Africa Health Research Institute, Mtubatuba, South Africa (Prof T Bärnighausen MD); Institute of Public Health, Heidelberg University, Heidelberg, Germany (Prof T Bärnighausen MD, S Mohammed PhD); Department of Industrial Engineering, School of Engineering, Pontifi cia Universidad Javeriana, Bogotá, Colombia (L H Barrero ScD); Stanford University, Stanford, CA, USA (S Basu PhD, L C Del Gobbo PhD); College of Medicine, Charles R Drew University of Medicine and Science, Los Angeles, CA, USA (Prof S Bazargan-Hejazi PhD); David Geff en School of Medicine, University of California, Los Angeles, Los Angeles, CA, USA (Prof S Bazargan-Hejazi PhD); Kermanshah University of Medical Science, Kermanshah, Iran (Prof S Bazargan-Hejazi PhD); Oxford University, Ho Chi Minh City, Vietnam (J Beardsley MBChB);
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 31
College of Public Health and Tropical Medicine, Jazan, Saudi Arabia (N Bedi MD); IRCCS - Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy (E Beghi MD); University Hospital and Medical School of Dijon, University of Burgundy, Dijon, France (Prof Y Béjot PhD); School of Medicine (K N Sheth MD), Yale University, New Haven, CT, USA (Prof M L Bell PhD); University of Alberta, Edmonton, AB, Canada (A K Bello PhD); Internal Medicine Department (Prof I S Santos PhD), University of São Paulo, São Paulo, Brazil (I M Bensenor PhD, Prof P A Lotufo DrPH); Department of Epidemiology and Health Promotion, College of Dentistry (H Benzian PhD), New York University, New York, NY, USA; Debre Berhane University, Debre Berhan, Ethiopia (A Berhane PhD); Division of Health and Social Care Research (Prof C D Wolfe MD), King’s College London, London, UK (E Bernabé PhD, I Wolfe PhD); University Andes, Bogotá, Colombia (O A Bernal PhD); College of Health and Medical Sciences (H S Roba MPH), Haramaya University, Harar, Ethiopia (A S Beyene MPH, Y M Mesfi n MPH); Queen Elizabeth Hospital Birmingham, Birmingham, UK (N Bhala DPhil); University of Otago Medical School, Wellington, New Zealand (N Bhala DPhil); Imperial College, London, UK (S Bhatt DPhil); Independent Public Health Consultants, Addis Ababa, Ethiopia (S Biadgilign MPH); Department of Nephrology Issues of Transplanted Kidney, Academician V I Shumakov Federal Research Center of Transplantology and Artifi cial Organs, Moscow, Russia (B Bikbov MD); Department of Pediatrics & The Dartmouth Institute for Health Policy and Clinical Practice, Geisel School of Medicine (Prof A Binagwaho PhD), Dartmouth College, Hanover, NH, USA (S Soneji PhD); The University of Global Health Equity, Kigali, Rwanda (Prof A Binagwaho PhD); Department of Community Medicine (Prof E Bjertness PhD), University of Oslo, Oslo, Norway (A S Htet MPhil); Vision & Eye Research Unit, Anglia Ruskin University, Cambridge, UK (Prof R R A Bourne FRCOphth); Danube-University Krems, Krems, Austria (Prof M Brainin PhD); School of Population and Public Health (H Krueger PhD), University of British Columbia, Vancouver, BC, Canada (Prof M Brauer ScD, C C Gotay PhD, Prof N Kissoon MD, S Murthy MD, F Pourmalek PhD); Faculty of Health Sciences and Social Work, Department of Public Health, Trnava University, Trnava, Slovakia (A Brazinova PhD, M Majdan PhD); International Neurotrauma Research Organization, Vienna, Austria (A Brazinova PhD); College of Medicine (J Shen PhD), The Ohio State University, Columbus, OH, USA (Prof N J K Breitborde PhD); Technion, Haifa, Israel (Prof D M Broday DSc); University of Leicester, Leicester, UK (Prof T S Brugha MD); Monash Department of Clinical Epidemiology, Cabrini Institute, Melbourne, VIC, Australia (Prof R Buchbinder PhD); Department of Epidemiology and Preventive Medicine (Prof R Buchbinder PhD), School of Public Health and Preventive Medicine (Prof B Gabbe PhD), Department of Medicine, School of Clinical Sciences at Monash Health (Prof A G Thrift PhD), Monash University, Melbourne, VIC, Australia; Al Shifa Trust Eye Hospital, Rawalpindi, Pakistan (Z A Butt PhD); Department of Physics and Atmospheric Science (A van Donkelaar PhD), Dalhousie University, Halifax, NS, Canada (L E Cahill PhD, Prof R V Martin PhD); Department of Biostatistics and Epidemiology, University of Oklahoma Health Sciences Center, Oklahoma City, OK, USA (H Carabin PhD); Metropolitan Autonomous University, Mexico City, Mexico (R Cárdenas ScD); Stroke Unit, University of Perugia, Perugia, Italy (V Caso MD); Colombian National Health Observatory, Instituto Nacional de Salud, Bogotá, Colombia (C A Castañeda-Orjuela MSc); Epidemiology and Public Health Evaluation Group, Public Health Department, Universidad Nacional de Colombia, Bogotá, Colombia (C A Castañeda-Orjuela MSc); Caja Costarricense de Seguro Social, San Jose, Costa Rica (Prof J Castillo Rivas MPH); Universidad de Costa Rica, San Pedro, Montes de Oca, Costa Rica (Prof J Castillo Rivas MPH); Department of Medicine, University of Valencia/INCLIVA Health Research Institute and CIBERSAM, Valencia, Spain (F Catalá-López PhD); Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, ON, Canada (F Catalá-López PhD); Faculty of Medicine, University of the Republic, Montevideo, Uruguay (F Cavalleri BS); i3S - Instituto de Investigação e Inovação em Saúde (P Cecílio MS, J das Neves PhD); Pharmacy Faculty (P Cecílio MS), INEB - Instituto de Engenharia Biomédica (J das Neves PhD), Faculty of Medicine (J Massano MD), EPIUnit - Institute of Public Health
(J M Pedro MS), University of Porto, Porto, Portugal; National Health Research Institutes, Zhunan Town, Taiwan (Prof H Chang DrPH); National Yang-Ming University, Taipei, Taiwan (Prof H Chang DrPH); School of Nursing, College of Medicine, National Taiwan University, Taipei, Taiwan (Prof J Chang PhD); Queensland Centre for Mental Health Research, Brisbane, QLD, Australia (F J Charlson PhD, H E Erskine PhD, A J Ferrari PhD, J Leung PhD, D F Santomauro PhD, Prof H A Whiteford PhD); African Centre for Statistics, United Nations Economic Commission for Africa, Addis Ababa, Ethiopia (X Che PhD); Clinical Governance Unit, Gold Coast Health, Southport, QLD, Australia (P P Chiang PhD); Crowd Watch Africa, Lusaka, Zambia (M Chibalabala BS); University of Zambia, Lusaka, Zambia (V H Chisumpa MPhil, C C Mapoma PhD, F Masiye PhD); University of Witwatersrand, Johannesburg, South Africa (V H Chisumpa MPhil); Seoul National University Medical Library, Seoul, South Korea (J J Choi PhD); Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK (R Chowdhury PhD); Bispebjerg University Hospital, Copenhagen, Denmark (Prof H Christensen DMSCi); University of Salerno, Baronissi, Italy (Prof M Cirillo MD); Health Eff ects Institute, Boston, MA, USA (A J Cohen DSc); Department of Infectious Disease Epidemiology (T Fürst PhD), Department of Epidemiology and Biostatistics (F B Piel PhD), Department of Epidemiology and Biostatistics, School of Public Health (Prof A Rodriguez PhD), Imperial College London, London, UK (G S Cooke DPhil, Prof A Majeed MD, Prof B Neal PhD); MRC Lifecourse Epidemiology Unit, University of Southampton, Southampton, UK (Prof C Cooper FMedSci); NIHR Biomedical Research Centre, University of Southampton and University Hospital Southampton NHS Foundation Trust, Southampton, UK (Prof C Cooper FMedSci); Mayo Clinic, Jacksonville, FL, USA (L T Cooper MD); WHO Collaborating Centre for Viral Hepatitis, Victorian Infectious Diseases Reference Laboratory, Melbourne, VIC, Australia (Prof B C Cowie PhD); Centre for International Health, Dunedin School of Medicine (Prof J A Crump MD), Injury Prevention Research Unit, Department of Preventive and Social Medicine, Dunedin School of Medicine (Prof S Derrett PhD), University of Otago, Dunedin, New Zealand (Prof R G Poulton PhD); Wolaita Sodo University, Wolaita Sodo, Ethiopia (S A Damtew MPH, S B Workie MPH); School of Public Health (K Deribe MPH), College of Health Sciences, School of Public Health (W Tefera MPH), Addis Ababa University, Addis Ababa, Ethiopia (S A Damtew MPH, A Z Giref PhD, D Haile MPH, G Temam Shifa MPH); Guy’s and St Thomas’ NHS Foundation Trust, London, UK (Prof P I Dargan FRCP); Public Health England, London, UK (Prof A C Davis PhD, Prof J N Newton FRCP, Prof N Steel PhD); School of Public Health, Kazakh National Medical University, Almaty, Kazakhstan (K Davletov PhD); National Institute of Public Health, Mexico City, Mexico (E F de Castro PhD); Griffi th University, Brisbane, QLD, Australia (Prof D De Leo DSc); National Drug and Alcohol Research Centre (Prof L Degenhardt PhD), Brien Holden Vision Institute (Prof S Resnikoff MD), School of Optometry and Vision Science (Prof S Resnikoff MD), University of New South Wales, Sydney, NSW, Australia (Prof P B Mitchell MD); Brighton and Sussex Medical School, Brighton, UK (K Deribe MPH); Mount Sinai Beth Israel, New York, NY, USA (Prof D C Des Jarlais PhD); Icahn School of Medicine at Mount Sinai, New York, NY, USA (Prof D C Des Jarlais PhD); Indian Institute of Public Health-Delhi (S Dey PhD, Prof G V S Murthy MD), Centre for Control of Chronic Conditions (P Jeemon PhD), Centre for Chronic Conditions and Injuries (Prof V Patel PhD), Public Health Foundation of India, Gurgaon, India (P K Dhillon PhD, D K Lal MD, Prof S Zodpey PhD); Department of Community Medicine, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka (S D Dharmaratne MD); University of Rochester Medical Center, Rochester, NY, USA (E R Dorsey MD); RMIT University, Bundoora, VIC, Australia (Prof K E Doyle PhD); The University of Sydney, Camperdown, NSW, Australia (Prof A H Kemp PhD); International Institute for Population Sciences, Mumbai, India (M Dubey MPhil, M H U Rahman MPhil, Prof U Ram PhD, A Singh PhD, R K Verma MPhil, A K Yadav MPhil); Federal University of Rio Grande do Sul, Porto Alegre, Brazil (B B Duncan PhD, C Kieling MD, Prof M I Schmidt MD); University of North Carolina, Chapel Hill, NC, USA (B B Duncan PhD); Non-Communicable Diseases Research Center,
Articles
32 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
Endocrinology and Metabolism Population Sciences Institute (H Ebrahimi MD, Prof A Esteghamati MD, F Farzadfar MD, N Hafezi-Nejad MD, A Kasaeian PhD, M Parsaeian PhD, F Pishgar MD, S Sheikhbahaei MD), Liver and Pancreaticobiliary Diseases Research Center, Digestive Disease Research Institute, Shariati Hospital (H Ebrahimi MD), Digestive Diseases Research Institute (S Fahimi PhD, Prof R Malekzadeh MD, G Roshandel PhD, S G Sepanlou PhD), Center for Air Pollution Research, Institute for Environmental Research (M S Hassanvand PhD), Hematology-Oncology and Stem Cell Transplantation Research Center (A Kasaeian PhD), Non-Communicable Diseases Research Center (A Khosravi PhD), Department of Epidemiology and Biostatistics, School of Public Health (M Parsaeian PhD), Uro-Oncology Research Center (F Pishgar MD), Sina Trauma and Surgery Research Center (Prof V Rahimi-Movaghar MD), Tehran University of Medical Sciences, Tehran, Iran (M Yaseri PhD); Arba Minch University, Arba Minch, Ethiopia (A Y Endries MPH, G Temam Shifa MPH); The Institute of Social and Economic Studies of Population, Russian Academy of Sciences, Moscow, Russia (Prof S P Ermakov DSc); Federal Research Institute for Health Organization and Informatics, Ministry of Health of the Russian Federation, Moscow, Russia (Prof S P Ermakov DSc, S Soshnikov PhD); Ministry of Health and Medical Education, Tehran, Iran (B Eshrati PhD); Arak University of Medical Sciences, Arak, Iran (B Eshrati PhD); University of Louisville, Louisville, KY, USA (T A Farid MD, A R Khan MD); DGS Directorate General of Health, Lisboa, Portugal (C S E S Farinha MSc); Universidade Aberta, Lisboa, Portugal (C S E S Farinha MSc); Federal University of Sergipe, Aracaju, Brazil (Prof A Faro PhD); Harvard/MGH Center on Genomics, Vulnerable Populations, and Health Disparities, Mongan Institute for Health Policy, Massachusetts General Hospital, Boston, MA, USA (M S Farvid PhD); National Institute for Stroke and Applied Neurosciences, Auckland University of Technology, Auckland, New Zealand (V L Feigin PhD); ARS Norte, I P, Departamento Saúde Pública, Porto, Portugal (M M Felicio MD); Institute of Education and Sciences, German Hospital Oswaldo Cruz, São Paulo, Brazil (Prof J G Fernandes PhD); Centre for Experimental Medicine & Rheumatology, William Harvey Research Institute, Barts and The London School of Medicine & Dentistry, Queen Mary University of London, London, UK (J C Fernandes PhD); Bielefeld University, Bielefeld, Germany (F Fischer MPH); Institute of Gerontology, Academy of Medical Science, Kyiv, Ukraine (N Foigt PhD); Alzheimer Scotland Dementia Research Centre (I Shiue PhD), University of Edinburgh, Edinburgh, UK (Prof F G R Fowkes PhD); Federal University of Minas Gerais, Belo Horizonte, Brazil (Prof E B Franca PhD); James Cook University, Townsville, QLD, Australia (R C Franklin PhD); University of Basel, Basel, Switzerland (T Fürst PhD); Manhiça Health Research Center, Manhiça, Mozambique (A L Garcia-Basteiro MSc); Barcelona Institute for Global Health, Barcelona, Spain (A L Garcia-Basteiro MSc); The Task Force for Global Health, Decatur, GA, USA (T Gebre PhD); Ludwig Maximilians University, Munich, Germany (A T Gebremedhin MPH); Kilte Awlaelo Health and Demographic Surveillance System, Mekelle, Ethiopia (A A Gebru MPH, G B Hailu MSc); Agence de Medecine Preventive, Paris, France (B D Gessner MD); College of Medicine, Howard University, Washington, DC, USA (R F Gillum MD, A Mehari MD); College of Medicine, University of Hail, Hail, Saudi Arabia (I A Ginawi MD); University Hospital of Dijon, Dijon, France (Prof M Giroud MD); College of Health and Medical Sciences (H S Roba MPH), Haramaya University, Dire Dawa, Ethiopia (M D Gishu MS, A K Tura MPH); Kersa Health and Demographic Surveillance System, Harar, Ethiopia (M D Gishu MS); University of Massachusetts Boston, Boston, MA, USA (Prof P Gona PhD); Instituto de Investigaciones Cientifi cas y Servicios de Alta Tecnologia - INDICASAT-AIP, Ciudad del Saber, Panamá (A Goodridge PhD); Department of Health and Social Aff airs, Government of the Federated States of Micronesia, Palikir, Federated States of Micronesia (S V Gopalani MPH); Division of Epidemiology, Center for Public Health Sciences (A Goto PhD), National Cancer Center, Tokyo, Japan (M Inoue MD); Stattis LLC, Chisinau, Moldova (K F Greenwell PhD); West Virginia Bureau for Public Health, Charleston, WV, USA (R Gupta MD); Eternal Heart Care Centre and Research Institute, Jaipur,
india (R Gupta PhD); Department of Anthropology, University of Delhi, Delhi, India (V Gupta PhD); National Institute of Psychiatry Ramon de la Fuente, Mexico City, Mexico (R A Gutiérrez PhD); Aarhus University, Aarhus, Denmark (B Gyawali MPH, K M Iburg PhD); Department of Public Health, Erasmus MC, University Medical Center, Rotterdam, Netherlands (J A Haagsma PhD); Brandeis University, Waltham, MA, USA (Y A Halasa MS, E A Undurraga PhD); Arabian Gulf University, Manama, Bahrain (Prof R R Hamadeh DPhil); Hamdan Bin Mohammed Smart University, Dubai, United Arab Emirates (S Hamidi PhD); Wayne County Department of Health and Human Services, Detroit, MI, USA (M Hammami MD); School of Medicine and Pharmacology, University of Western Australia, Perth, WA, Australia (Prof G J Hankey MD); Harry Perkins Institute of Medical Research, Nedlands, WA, Australia (Prof G J Hankey MD); Western Australian Neuroscience Research Institute, Nedlands, WA, Australia (Prof G J Hankey MD); Parc Sanitari Sant Joan de Déu - CIBERSAM, Sant Boi de Llobregat (Barcelona), Spain (J M Haro MD); Universitat de Barcelona, Barcelona, Spain (J M Haro MD); Department of Psychiatry, University Medical Center Groningen (Prof H W Hoek MD), University of Groningen, Groningen, Netherlands (A K Tura MPH); Department of Epidemiology, Mailman School of Public Health (Prof H W Hoek MD), Columbia University, New York, NY, USA (Prof V Skirbekk PhD); Nevada Division of Public and Behavioral Health, Department of Health and Human Services, Carson City, NV, USA (M Horino MPH); Department of Pulmonology, Yokohama City University Graduate School of Medicine, Yokohama, Japan (N Horita MD); Albert Einstein College of Medicine, Bronx, NY, USA (Prof H D Hosgood PhD); Public Health Division, The Pacifi c Community, Noumea, New Caledonia (D G Hoy PhD); International Relations Division, Ministry of Health, Nay Pyi Taw, Myanmar (A S Htet MPhil); Department of Epidemiology and Health Statistics, School of Public Health, Central South University, Changsha, China (G Hu PhD); Cambridge Health Alliance, Cambridge, MA, USA (H Huang MD); Boston Medical Center (B T Idrisov MD), School of Medicine (G F Kwan MD), Boston University, Boston, MA, USA; Graduate School of Medicine (M Inoue MD), School of Public Health (Prof N Kawakami MD), University of Tokyo, Tokyo, Japan (K Shibuya MD); American Cancer Society, Atlanta, GA, USA (F Islami PhD); MCH Division, USAID - Global Health Bureau, HIDN, Washington, DC, USA (T A Jacobs MD); Department of Global and Community Health, George Mason University, Fairfax, VA, USA (K H Jacobsen PhD); Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia (Prof M B Jakovljevic PhD); UNFPA Asia and the Pacifi c Regional Offi ce, Bangkok, Thailand (H A F Jansen Drs); University of Aberdeen, Aberdeen, UK (M Javanbakht PhD); Postgraduate Institute of Medicine, Colombo, Sri Lanka (A U Jayatilleke PhD); Institute of Violence and Injury Prevention, Colombo, Sri Lanka (A U Jayatilleke PhD); Graduate School of Public Health (Prof S H Jee PhD), Yonsei University, Seoul, South Korea; Centre for Chronic Disease Control, New Delhi, India (P Jeemon PhD); George Institute for Global Health India, New Delhi, India (Prof V Jha DM); Department of Health Development, Institute of Industrial Ecological Sciences, University of Occupational and Environmental Health, Kitakyushu, Japan (Y Jiang PhD); School of Public Health (K Deribe MPH), College of Health Sciences, School of Public Health (W Tefera MPH), Addis Ababa University, Debre Zeit, Ethiopia (T Jibat MS,); Wageningen University, Wageningen, Netherlands (T Jibat MS); Department of Ophthalmology, Medical Faculty Mannheim, Ruprecht-Karls-University Heidelberg, Mannheim, Germany (Prof J B Jonas MD); University College Cork, Cork, Ireland (Z Kabir PhD); Society for Education, Action and Research in Community Health, Gadchiroli, India (Y Kalkonde MD); CSIR - Indian Institute of Toxicology Research, Lucknow, India (R Kamal MSc, C N Kesavachandran PhD); Department of Pulmonary Medicine, Zhongshan Hospital (J She MD), Fudan University, Shanghai, China (H Kan MD); University at Buff alo, Buff alo, NY, USA (A Kandel MBBS); Epidemiological and Statistical Methods Research Group, Helmholtz Centre for Infection Research, Braunschweig, Germany (A Karch MD); Hannover-Braunschweig Site, German Center for Infection Research, Braunschweig, Germany (A Karch MD); Quality and Equity Health Care, Kigali, Rwanda (C K Karema MSc); Case Western University Hospitals,
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 33
Cleveland, OH, USA (C Karimkhani MD); Ministry of Health, Colombo, Sri Lanka (P Karunapema MD); Oklahoma State University, Tulsa, OK, USA (A Kaul MD); Institut de recherche de l’hôpital de Monttfort, Ottawa, ON, Canada (J F Kayibanda PhD); Institute of Tropical and Infectious Diseases, Nairobi, Kenya (P N Keiyoro PhD); School of Continuing and Distance Education, Nairobi, Kenya (P N Keiyoro PhD); Swansea University, Swansea, UK (Prof A H Kemp PhD); Burden of Disease Research Unit (R Matzopoulos PhD), Alcohol, Tobacco & Other Drug Research Unit (Prof C D Parry PhD), South African Medical Research Council, Cape Town, South Africa (A P Kengne PhD, Prof C S Wiysonge PhD); School of Public Health and Family Medicine (R Matzopoulos PhD), Department of Psychiatry (Prof D J Stein PhD), University of Cape Town, Cape Town, South Africa (A P Kengne PhD, Prof B M Mayosi DPhil, M Shey PhD, D A Watkins MD); Assuta Hospitals, Assuta Hashalom, Tel Aviv, Israel (Prof A Keren MD); Jordan University of Science and Technology, Irbid, Jordan (Prof Y S Khader ScD); Health Services Academy, Islamabad, Pakistan (E A Khan MPH); Department of Microbiology and Immunology, College of Medicine & Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates (G Khan PhD); College of Medicine (Prof Y H Khang MD), Graduate School of Public Health (Prof S Won PhD), Seoul National University, Seoul, South Korea; Executive Board of the Health Ministers’ Council for Cooperation Council States, Riyadh, Saudi Arabia (Prof T A M Khoja FRCP); Iranian Ministry of Health and Medical Education, Tehran, Iran (A Khosravi PhD); Ball State University, Muncie, IN, USA (J Khubchandani PhD); Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil (C Kieling MD); Korea Health Industry Development Institute, Cheongju-si, South Korea (C Kim PhD); Department of Health Sciences, Northeastern University, Boston, MA, USA (Prof D Kim DrPH); Soonchunhyang University, Seoul, South Korea (S Kim PhD); Southern University College, Skudai, Malaysia (Y J Kim PhD); Simmons College, Boston, MA, USA (R W Kimokoti MD); Department of Preventive Cardiology, National Cerebral and Cardiovascular Center, Suita, Japan (Y Kokubo PhD); Division of Cardiology, Brown University, Providence, RI, USA (D Kolte MD); Center for Community Empowerment, Health Policy and Humanities, NIHRD, Jakarta, Indonesia (S Kosen MD); Sher-i-Kashmir Institute of Medical Sciences, Srinagar, India (Prof P A Koul MD); Research and Development Unit, Parc Sanitari Sant Joan de Deu (CIBERSAM), Barcelona, Spain (A Koyanagi MD); Research Center of Neurology, Moscow, Russia (M Kravchenko PhD, Prof Y Y Varakin MD); Department of Demography and Public Health Research Institute (Prof B Kuate Defo PhD), Department of Social and Preventive Medicine, School of Public Health (Prof B Kuate Defo PhD), University of Montreal, Montreal, QC, Canada; Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil (Prof R S Kuchenbecker PhD); Erasmus MC, University Medical Center Rotterdam, Rotterdam, Netherlands (Prof E J Kuipers PhD); Arkansas State University, State University, AR, USA (V S Kulkarni PhD); National Centre for Epidemiology and Population Health, The Australian National University, Canberra, ACT, Australia (A Lal PhD, Prof R M Lucas PhD); Institute of Health Policy and Development Studies, National Institutes of Health, Manila, Philippines (Prof H Lam PhD); National Cancer Institute, Rockville, MD, USA (Q Lan PhD); Komfo Anokye Teaching Hospital, Kumasi, Ghana (D O Laryea MD); Department of Zoology, Lahore College for Women University, Lahore, Pakistan (A A Latif PhD); College of Optometry, Nova Southeastern University, Fort Lauderdale, FL, USA (J L Leasher OD); National Institute for Health Development, Tallinn, Estonia (M Leinsalu PhD); Stockholm Centre for Health and Social Change, Södertörn University, Stockholm, Sweden (M Leinsalu PhD); State University of New York, Albany, Rensselaer, NY, USA (R Leung PhD); Tuscany Regional Centre for Occupational Injuries and Diseases, Florence, Italy (M Levi PhD); San Francisco VA Medical Center, San Francisco, CA, USA (Y Li PhD); University of Haifa, Haifa, Israel (Prof S Linn MD); School of Medicine, Wayne State University, Detroit, MI, USA (Prof S E Lipshultz MD, Prof J D Wilkinson MD); Children’s Hospital of Michigan, Detroit, MI, USA (Prof S E Lipshultz MD); Rollins School of Public Health (E P Simard PhD), Emory University, Atlanta, GA, USA (Prof Y Liu PhD, Prof M R Phillips MD); Eastern Health Clinical School (B K Lloyd PhD), Monash University, Fitzroy, VIC, Australia; Turning Point, Eastern
Health, Melbourne, VIC, Australia (B K Lloyd PhD); UnionHealth Associates, LLC, St Louis, MO, USA (L Lo MD); Alton Mental Health Center, Alton, IL, USA (L Lo MD); University of Bari, Bari, Italy (Prof G Logroscino PhD); Aintree University Hospital National Health Service Foundation Trust, Liverpool, UK (Prof R Lunevicius PhD); School of Medicine, University of Liverpool, Liverpool, UK (Prof R Lunevicius PhD); Aswan University Hospital, Aswan Faculty of Medicine, Aswan, Egypt (M Magdy Abd El Razek MBBCh); National Center for the Prevention and Control of HIV/AIDS, Secretariat of Health, Mexico City, Mexico (C Magis-Rodriguez PhD); Social Security Organization Research Institute, Tehran, Iran (M Mahdavi PhD); Institute of Health Policy and Management, Erasmus University Rotterdam, Rotterdam, Netherlands (M Mahdavi PhD); Universidade Federal de Minas Gerais, Belo Horizonte, Brazil (Prof D C Malta PhD); Perelman School of Medicine (P A Meaney MD), University of Pennsylvania, Philadelphia, PA, USA (D J Margolis PhD); University Hospital Doctor Peset, University of Valencia, Valencia, Spain (J Martinez-Raga PhD); CEU Cardenal Herrera University, Moncada (Valencia), Spain (J Martinez-Raga PhD); Department of Health Sciences, University of York, York, UK (A J Mason-Jones PhD); Hospital Pedro Hispano/ULS Matosinhos, Matosinhos, Portugal (J Massano MD); Children’s Hospital of Philadelphia, Philadelphia, PA, USA (P A Meaney MD); University of Gondar, Gondar, Ethiopia (A B Mekonnen MS, B A Tedla BS); University of West Florida, Pensacola, FL, USA (P Memiah PhD); Saudi Ministry of Health, Riyadh, Saudi Arabia (Prof Z A Memish MD); College of Medicine, Alfaisal University, Riyadh, Saudi Arabia (Prof Z A Memish MD); United Nations Population Fund, Lima, Peru (W Mendoza MD); Robert Koch Institute, Berlin, Germany (G B M Mensink PhD); Department of Neurology, Helsinki University Hospital, Helsinki, Finland (A Meretoja PhD); Helsinki University Hospital, Comprehensive Cancer Center, Breast Surgery Unit, Helsinki, Finland (T J Meretoja PhD); University of Helsinki, Helsinki, Finland (T J Meretoja PhD); Ifakara Health Institute, Bagamoyo, Tanzania (F A Mhimbira MS); Pacifi c Institute for Research & Evaluation, Calverton, MD, USA (T R Miller PhD); Centre for Population Health, Curtin University, Perth, WA, Australia (T R Miller PhD); University of Ottawa, Ottawa, ON, Canada (E J Mills PhD); Neuroscience Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran (A Mohammadi PhD); Health Systems and Policy Research Unit, Ahmadu Bello University, Zaria, Nigeria (S Mohammed PhD); Institute for Maternal and Child Health, IRCCS “Burlo Garofolo”, Trieste, Italy (L Monasta DSc, M Montico MSc, L Ronfani PhD); Bureau of International Health Cooperation, Manila City, Philippines (J D Monis MSc); Department of Community Medicine, Gastrointestinal and Liver Disease Research Center, Preventive Medicine and Public Health Research Center, Iran University of Medical Sciences, Tehran, Iran (M Moradi-Lakeh MD); International Laboratory for Air Quality and Health (L Morawska PhD), School of Public Health and Social Work (J Sun PhD), Queensland University of Technology, Brisbane, QLD, Australia; National Center for Child Health and Development, Setagaya, Japan (R Mori PhD); Competence Center Mortality-Follow-Up of the German National Cohort (A Werdecker PhD), Federal Institute for Population Research, Wiesbaden, Germany (Prof U O Mueller PhD, R Westerman PhD); West Herts Hospitals NHS Trust, Watford, UK (M E Murdoch FRCP); AIDS & TB Unit, Ministry of Health and Child Care, Bindura, Zimbabwe (B Murimira MS); Zimbabwe National Family Planning Council, Harare, Zimbabwe (B Murimira MS); Federal University of Pelotas, Pelotas, Brazil (Prof J Murray PhD); School of Medical Sciences, University of Science Malaysia, Kubang Kerian, Malaysia (K I Musa MD); Graduate School of Public Health (Prof J B Nachega PhD), Public Health Dynamics Laboratory (A J Paternina Caicedo MD), University of Pittsburgh, Pittsburgh, PA, USA; Department of Psychiatry (Prof C D Parry PhD), Stellenbosch University, Cape Town, South Africa (Prof J B Nachega PhD, Prof S Seedat PhD, Prof C S Wiysonge PhD); Bloomberg School of Public Health (Prof J B Nachega PhD), Johns Hopkins University, Baltimore, MD, USA (B X Tran PhD); Institute of Epidemiology and Medical Biometry, Ulm University, Ulm, Germany (Prof G Nagel PhD, Prof D Rothenbacher MD); University of KwaZulu-Natal, Durban, South Africa (Prof K S Naidoo PhD, O Oladimeji MD, Prof B Sartorius PhD, E A Zegeye MS); Azienda
Articles
34 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
Ospedaliera Papa Giovanni XXIII, Bergamo, Italy (Prof L Naldi MD, Prof G Remuzzi MD); Suraj Eye Institute, Nagpur, India (V Nangia MD); The George Institute for Global Health, Sydney, NSW, Australia (Prof B Neal PhD); Royal Prince Alfred Hospital, Sydney, NSW, Australia (Prof B Neal PhD); Faculty of Medicine, Fez, Morocco (Prof C Nejjari PhD); KEMRI Wellcome Trust, Kilifi , Kenya (Prof C R Newton MD); Ministry of Health and Social Welfare, Dar es Salaam, Tanzania (F N Ngalesoni MSc); KEMRI - Wellcome Trust Research Program, Nairobi, Kenya (P Nguhiu BPharm); Institute for Global Health Innovations, Duy Tan University, Da Nang, Vietnam (Q L Nguyen MD); Institute For Research, Socio-Economic Development and Communication, Yaoundé, Cameroon (P M Nkamedjie Pete MS); Department of Psychosomatic Medicine, Center for Internal Medicine and Dermatology, Charité Universitätsmedizin, Berlin, Germany (S Nolte PhD); Population Health Strategic Research Centre, School of Health and Social Development (S Nolte PhD), Deakin University, Geelong, VIC, Australia (Prof R H Osborne PhD); National Institute of Public Health, Saitama, Japan (M Nomura PhD); Department of Global Public Health and Primary Care (Prof S E Vollset DrPH), University of Bergen, Bergen, Norway (Prof O F Norheim PhD); Center for Research on Population and Health, Faculty of Health Sciences, American University of Beirut, Beirut, Lebanon (Prof C M Obermeyer DSc); Centre for Health Research, Western Sydney University, Sydney, NSW, Australia (F A Ogbo MPH); Department of Preventive Medicine, School of Medicine, Kyung Hee University, Seoul, South Korea (Prof I Oh PhD); Human Sciences Research Council, Durban, South Africa (O Oladimeji MD); Universidad Autonoma de Chile, Talca, Chile (Prof P R Olivares PhD); Center for Healthy Start Initiative, Lagos, Nigeria (B O Olusanya PhD, J O Olusanya MBA); Lira District Local Government, Lira Municipal Council, Uganda (J N Opio MPH); University of Arizona, Tucson, AZ, USA (Prof E Oren PhD); IIS-Fundacion Jimenez Diaz-UAM, Madrid, Spain (Prof A Ortiz PhD); St Luke’s International University, Tokyo, Japan (E Ota PhD); JSS Medical College, JSS University, Mysore, India (Prof Mahesh PA DNB); Department of Medical Humanities and Social Medicine, College of Medicine, Kosin University, Busan, South Korea (E Park PhD); California Air Resources Board, Sacramento, CA, USA (H Park PhD); Mount Sinai Health System, New York, NY, USA (T Patel MD); Sangath, Goa, India (Prof V Patel PhD); Krishan Institute of Medical Sciences, Deemed University, School of Dental Sciences, Karad, India (S T Patil MDS); Department of Community Health Sciences (Prof S B Patten PhD), University of Calgary, Calgary, AB, Canada (Prof M Tonelli MD); UK Department for International Development, Lalitpur, Nepal (D Paudel PhD); Health Research Centre of Angola, Caxito, Angola (J M Pedro MS); REQUIMTE/LAQV, Laboratório de Farmacognosia, Departamento de Química, Faculdade de Farmácia, Universidade do Porto, Porto, Portugal (Prof D M Pereira PhD); IRCCS - Istituto di Ricerche Farmacologiche Mario Negri, Bergamo, Italy (N Perico MD, Prof G Remuzzi MD); Flinders University, Adelaide, SA, Australia (Prof K Pesudovs PhD); Health Metrics Unit, University of Gothenburg, Gothenburg, Sweden (Prof M Petzold PhD); University of the Witwatersrand, Johannesburg, South Africa (Prof M Petzold PhD); Shanghai Jiao Tong University School of Medicine, Shanghai, China (Prof M R Phillips MD); Durban University of Technology, Durban, South Africa (J D Pillay PhD); Department of Public Health, Erasmus University Medical Center, Rotterdam, Netherlands (S Polinder PhD); Department of Community Medicine, School of Medicine, Alborz University of Medical Sciences, Karaj, Iran (M Qorbani PhD); A T Still University, Kirksville, MO, USA (A Radfar MD); Research and Evaluation Division, BRAC, Dhaka, Bangladesh (M Rahman PhD); Hamad Medical Corporation, Doha, Qatar (S U Rahman FCPS); Society for Health and Demographic Surveillance, Suri, India (R K Rai MPH); ERAWEB Program, University for Health Sciences, Medical Informatics and Technology, Hall in Tirol, Austria (S Rajsic MD); University of Missouri, Columbia, MO, USA (M Raju PhD); Contech School of Public Health, Lahore, Pakistan (Prof S M Rana PhD); Contech International Health Consultants, Lahore, Pakistan (Prof S M Rana PhD); Department of Preventive Medicine, Wonju College of Medicine (C L Ranabhat PhD), Yonsei University, Wonju, South Korea; University of Michigan Health Systems, Ann Arbor, MI, USA (K Ranganathan MD); Walden University, Minneapolis, MN, USA (Prof A H Refaat PhD); Suez Canal University,
Ismailia, Egypt (Prof A H Refaat PhD); Department of Biomedical and Clinical Sciences L Sacco, University of Milan, Milan, Italy (Prof G Remuzzi MD); Hospital das Clinicas da Universidade Federal de Minas Gerais, Belo Horizonte, Brazil (Prof A L Ribeiro MD); School of Psychology, University of Lincoln, Lincoln, UK (Prof A Rodriguez PhD); (ISGlobal) Instituto de Salud Global de Barcelona, Barcelona, Spain (D Rojas-Rueda PhD); Golestan Research Center of Gastroenterology and Hepatology, Golestan University of Medical Sciences, Gorgan, Iran (G Roshandel PhD); All India Institute of Medical Sciences, New Delhi, India (A Roy DM, R Sagar MD, M Satpathy PhD); BARC Hospital, HBNI University, Mumbai, India (N Roy MD); World Health Organization, Accra, Ghana (B B Sackey MS); All India Institute of Medical Sciences, New Delhi, India (R Sagar MD, M Satpathy PhD); Development Research and Projects Center, Abuja, Nigeria (M M Saleh MPH); Marshall University J Edwards School of Medicine, Huntington, WV, USA (J R Sanabria MD); Case Western Reserve University, Cleveland, OH, USA (J R Sanabria MD); Universidad Ciencias Aplicadas y Ambientales, Bogotá, Colombia (R Sarmiento-Suarez MPH); Centre for Disease Burden (Prof S E Vollset DrPH), Norwegian Institute of Public Health, Oslo, Norway (M Savic PhD, Prof V Skirbekk PhD); Marshall University, Huntington, WV, USA (M Sawhney PhD); Global Perspective Studies Unit, Food and Agriculture Organization, Rome, Italy (J Schmidhuber PhD); Federal University of Santa Catarina, Florianópolis, Brazil (I J C Schneider PhD, D A S Silva PhD); Hypertension in Africa Research Team (HART), North-West University, Potchefstroom, South Africa (Prof A E Schutte PhD); Burden of Disease Research Unit (R Matzopoulos PhD), Alcohol, Tobacco & Other Drug Research Unit (Prof C D Parry PhD), South African Medical Research Council, Potchefstroom, South Africa (Prof A E Schutte PhD); Department of Public Health, An-Najah University, Nablus, Palestine (A Shaheen PhD); Independent Consultant, Karachi, Pakistan (M A Shaikh MD); Indian Institute of Technology Ropar, Rupnagar, India (R Sharma MA); Research Institute at Nationwide Children’s Hospital, Columbus, OH, USA (J Shen PhD); National Institute of Infectious Diseases, Tokyo, Japan (M Shigematsu PhD); Sandia National Laboratories, Albuquerque, NM, USA (M Shigematsu PhD); Department of Public Health Science, Graduate School (Prof M Shin PhD), Department of Preventive Medicine, College of Medicine (S Yoon PhD), Korea University, Seoul, South Korea; Work Organizations, Work Disability Prevention, The Finnish Institute of Occupational Health, Helsinki, Finland (R Shiri PhD); Washington State University, Spokane, WA, USA (K Shishani PhD); Faculty of Health and Life Sciences, Northumbria University, Newcastle upon Tyne, UK (I Shiue PhD); Reykjavik University, Reykjavik, Iceland (I D Sigfusdottir PhD); Feinberg School of Medicine (J I Silverberg MD), Department of Preventive Medicine (Y Yano MD), Northwestern University, Chicago, IL, USA; Department of Medicine, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India (O P Singh PhD); Institute for Human Development, New Delhi, India (P K Singh PhD); Stavanger University Hospital, Stavanger, Norway (K Søreide PhD); Instituto de Investigación Hospital Universitario de la Princesa, Universidad Autónoma de Madrid, Madrid, Spain (Prof J B Soriano PhD); Department of Clinical Neurological Sciences, Western University, London, ON, Canada (L A Sposato MD); Department of Community Medicine, International Medical University, Kuala Lumpur, Malaysia (C T Sreeramareddy MD); Institute of Public Health, University Hospital Heidelberg, Heidelberg, Germany (H Stahl PhD); University Medical Centre Freiburg, Freiburg, Germany (H Stahl PhD); Attikon University Hospital, Athens, Greece (V Stathopoulou PhD); Institute and Outpatient Clinic for Occupational, Social and Environmental Medicine, University Hospital Munich, Munich, Germany (N Steckling MSc); University of East Anglia, Norwich, UK (Prof N Steel PhD); South African Medical Research Council Unit on Anxiety & Stress Disorders, Cape Town, South Africa (Prof D J Stein PhD); Luxembourg Institute of Health, Strassen, Luxembourg (S Stranges PhD); School of Health and Related Research, University of Sheffi eld, Sheffi eld, UK (M Strong PhD); Institute for Resilient Regions, University of Southern Queensland, Springfi eld, QLD, Australia (J Sun PhD); Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania (B F Sunguya PhD); Indian Council of Medical Research, New Delhi, India (S Swaminathan MD);
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 35
Departments of Criminology, Law & Society, Sociology, and Public Health, University of California, Irvine, Irvine, CA, USA (Prof B L Sykes PhD); Department of Medicine, University of Valencia, INCLIVA Health Research Institute and CIBERSAM, Valencia, Spain (Prof R Tabarés-Seisdedos PhD); School of Social Work, University of Illinois at Urbana-Champaign, Champaign, IL, USA (K M Tabb PhD); Ministry of Health, MINSANTE, Yaoundé, Cameroon (R T Talongwa MD); Ministry of Health, Amman, Jordan (M R Tarawneh MPH); New York Medical College, Valhalla, NY, USA (M Tavakkoli MD); Department of Biology, Colgate University, Hamilton, NY, USA (B Taye PhD); James Cook University, Cairns, QLD, Australia (B A Tedla BS); Department of Anesthesiology, University of Virginia, Charlottesville, VA, USA (A S Terkawi MD); Outcomes Research Consortium (A S Terkawi MD), Cleveland Clinic, Cleveland, OH, USA (Prof E M Tuzcu MD); University Of Gondar, Gondar, Ethiopia (G A Tessema MPH); School of Public Health, Post Graduate Institute of Medical Education and Research, Chandigarh, India (Prof J Thakur MD); Adaptive Knowledge Management, Victoria, BC, Canada (A J Thomson PhD); WorldFish, Penang, Malaysia (A L Thorne-Lyman ScD); Nelson Institute of Environmental Medicine, School of Medicine, New York University, Tuxedo, NY, USA (Prof G D Thurston ScD); National Center for Child Health and Development, Tokyo, Japan (R Tobe-Gai PhD); Institute of Public Health, Faculty of Health Sciences, Jagiellonian University Medical College, Kraków, Poland (R Topor-Madry PhD); Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland (R Topor-Madry PhD); Aristotle University of Thessaloniki, Thessaloniki, Greece (Prof F Topouzis PhD); Hanoi Medical University, Hanoi, Vietnam (B X Tran PhD); Department of Population Sciences and Development, Faculty of Economics and Management, University of Kinshasa, Kinshasa, Democratic Republic of the Congo (Z Tsala Dimbuene PhD); African Population and Health Research Center, Nairobi, Kenya (Z Tsala Dimbuene PhD); Parc Sanitari Sant Joan de Déu, Fundació Sant Joan de Déu, Universitat de Barcelona, CIBERSAM, Barcelona, Spain (S Tyrovolas PhD); Department of Internal Medicine, Federal Teaching Hospital, Abakaliki, Nigeria (K N Ukwaja MD); Ebonyi State University, Abakaliki, Nigeria (C J Uneke PhD); Warwick Medical School, University of Warwick, Coventry, UK (O A Uthman PhD); UKK Institute for Health Promotion Research, Tampere, Finland (Prof T Vasankari PhD); University of Brasilia, Brasília, Brazil (Prof A M N Vasconcelos PhD); Raffl es Neuroscience Centre, Raffl es Hospital, Singapore, Singapore (N Venketasubramanian FRCP); University of Bologna, Bologna, Italy (Prof F S Violante MD); National Research University Higher School of Economics, Moscow, Russia (Prof V V Vlassov MD); National Cancer Institute, Mexico City, Mexico (P Volkow MD); National Autonomous University of Mexico, Mexico City, Mexico (P Volkow MD); National Institute for Occupational Safety and Health, Washington, DC, USA (G R Wagner MD); VA Medical Center, Washington, DC, USA (M T Wallin MD); Neurology Department, Georgetown University, Washington, DC, USA (M T Wallin MD); McGill University, Montreal, QC, Canada (S Weichenthal PhD); Department of Research, Cancer Registry of Norway, Institute of Population-Based Cancer Research, Oslo, Norway (E Weiderpass PhD); Department of Community Medicine, Faculty of Health Sciences, University of Tromsø, The Arctic University of Norway, Tromsø, Norway (E Weiderpass PhD); Genetic Epidemiology Group, Folkhälsan Research Center, Helsinki, Finland (E Weiderpass PhD); Royal Children’s Hospital, Melbourne, VIC, Australia (R G Weintraub MBBS); German National Cohort Consortium, Heidelberg, Germany (R Westerman PhD); Children’s Hospital of Michigan, Detroit, MI, USA (Prof J D Wilkinson MD); National Institute for Health Research Comprehensive Biomedical Research Centre, Guy’s & St Thomas’ NHS Foundation Trust and King’s College London, London, UK (Prof C D Wolfe MD); Evelina London Children’s Healthcare, St Thomas’ Hospital, London, UK (I Wolfe PhD); Royal Cornwall Hospital, Truro, UK (Prof A D Woolf FRCP); St Paul’s Hospital, Millennium Medical College, Addis Ababa, Ethiopia (M Wubshet PhD); Department of Neurology, Jinling Hospital, Nanjing University School of Medicine, Nanjing, China (Prof G Xu PhD); Discipline of Public Health Medicine, School of Nursing and Public Health, University of KwaZulu Natal, Durban, South Africa (B Yakob PhD); Global Health Research Center, Duke Kunshan
University, Kunshan, China (Prof L L Yan PhD); Social Work and Social Administration Department and The Hong Kong Jockey Club Centre for Suicide Research and Prevention, University of Hong Kong, Hong Kong, China (Prof P Yip PhD); Department of Biostatistics, School of Public Health, Kyoto University, Kyoto, Japan (N Yonemoto MPH); Jackson State University, Jackson, MS, USA (Prof M Z Younis DrPH); Department of Epidemiology and Biostatistics, School of Public Health (Prof C Yu PhD), Global Health Institute (Prof C Yu PhD), Wuhan University, Wuhan, China; University Hospital, Setif, Algeria (Prof Z Zaidi PhD); Faculty of Medicine, Mansoura University, Mansoura, Egypt (Prof M E Zaki PhD); EcoHealth Alliance, New York, NY, USA (C Zambrana-Torrelio MS); Instituto de Ecologia-Bolivia, La Paz, Bolivia (C Zambrana-Torrelio MS); World Health Organization, Windhoek, Namibia (T Zapata MD); Ethiopian Public Health Institute, Addis Ababa, Ethiopia (E A Zegeye MS); Oregon Health and Science University, Portland, OR, USA (D Zonies MD)
ContributorsStephen S Lim, Nancy Fullman, and Christopher J L Murray prepared the fi rst draft. Michael J Kutz, Ellen M Goldberg, and David M Pigott constructed the indices. Claire R McNellan, Nancy Fullman, and Kate Allen constructed the UHC tracer intervention indicator. Stephen S Lim and Christopher J L Murray provided overall guidance. Meghan D Mooney managed the project. Stephen S Lim, Nancy Fullman, Christopher J L Murray, and Meghan D Mooney fi nalised the manuscript based on comments from other authors and reviewer feedback. Helen E Olsen managed the appendices. All other authors provided data or developed models for SDG indicators, reviewed results, initiated modelling infrastructure, or reviewed and contributed to the report.
Declaration of interestsBruce Bartholow Duncan and Maria Inês Schmidt have received additional funding from the Brazilian Ministry of Health (Process number 25000192049/2014-14). Itamar S Santos reports grants from FAPESP (Brazilian public agency) outside the submitted work. Rafael Tabarés-Seisdedos was supported in part by grant PROMETEOII/2015/021 from Generalitat Valenciana and the national grand PI14/00894 from ISCIII-FEDER. Ai Koyanagi’s work is supported by the Miguel Servet contract fi nanced by the CP13/00150 and PI15/00862 projects, integrated into the National R + D + I and funded by the ISCIII—General Branch Evaluation and Promotion of Health Research—and the European Regional Development Fund (ERDF-FEDER). Benjamin C Cowie acknowledges funding support from the Australian Government Department of Health and the Royal Melbourne Hospital Research Funding Program. Elisabeth Barboza Franca acknowledges funding from the Brazilian Ministry of Health (Project number 25000192049/2014-14). Aletta E Schutte is funded by the Medical Research Council of South Africa, and the South African Research Chair Initiative by the National Research Foundation. Amador Goodridge acknowledges funding from Sistema Nacional de Investigadores de Panamá-SNI. José das Neves was supported in his contribution to this work by a Fellowship from Fundação para a Ciência e a Tecnologia, Portugal (SFRH/BPD/92934/2013). Thomas Fürst has received fi nancial support from the Swiss National Science Foundation (SNSF; project number P300P3-154634). Jost B Jonas reports personal fees from being a consultant for Mundipharma and a patent holder with Biocompatibles UK (title: Treatment of eye diseases using encapsulated cells encoding and secreting neuroprotective factor and/or anti-angiogenic factor; patent number: 20120263794), and has applied for patent with University of Heidelberg (title: Agents for use in the therapeutic or prophylactic treatment of myopia or hyperopia; Europäische Patentanmeldung 15 000 771.4) outside the submitted work. Stefanos Tyrovolas’s work is supported by the Foundation for Education and European Culture (IPEP), the Sara Borrell postdoctoral programme (reference number CD15/00019) from the Instituto de Salud Carlos III (ISCIII), Spain, and the Fondos Europeo de Desarrollo Regional (FEDER). Beatriz Paulina Ayala Quintanilla acknowledges the institutional support of PRONABEC (National Program of Scholarship and Educational Loan), provided by the Peruvian Government, while studying for her doctoral course at the

Articles
36 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
Judith Lumley Centre of La Trobe University funded by PRONABEC. Manami Inoue is the benefi ciary of a fi nancial contribution from the AXA Research fund as chair holder of the AXA Department of Health and Human Security, Graduate School of Medicine, The University of Tokyo from Nov 1, 2012; the AXA Research Fund has no role in this work. Olanrewaju Oladimeji is an African Research Fellow at Human Sciences Research Council (HSRC) and a Doctoral Candidate at the University of KwaZulu-Natal (UKZN), South Africa, and acknowledges the institutional support by leveraging on the existing organisational research infrastructure at HSRC and UKZN. Sun Ha Jee has been funded by a grant of the Korean Health Technology R&D project (HI14C2686), South Korea. Dan J Stein reports personal fees from Lundbeck, Novartis, AMBRF, Biocodex, Sevier, SUN, and CIPLA; and grants from NRGF and MRC outside the submitted work. Mayowa O Owolabi’s work is supported by U54 HG007479 from the US National Institutes of Health. All other authors declare no competing interests.
AcknowledgmentsWe thank the countless individuals who have contributed to the Global Burden of Disease Study 2015 in various capacities. The data used in this paper came from the 2009–10 Ghana Socioeconomic Panel Study Survey, which is a nationally representative survey of more than 5000 households in Ghana. The survey is a joint eff ort undertaken by the Institute of Statistical, Social and Economic Research (ISSER) at the University of Ghana, and the Economic Growth Centre (EGC) at Yale University. It was funded by the Economic Growth Center. At the same time, ISSER and the EGC are not responsible for the estimations reported by the analyst(s). HBSC is an international study carried out in collaboration with WHO/EURO. A list of principal investigators in each country can be found online. The Panel Study of Income Dynamics is primarily sponsored by the National Science Foundation, the National Institute on Aging, and the National Institute of Child Health and Human Development and is conducted by the University of Michigan. This analysis uses data or information from the LASI Pilot micro data and documentation. The development and release of the LASI Pilot Study was funded by the National Institute on Ageing/National Institute of Health (R21AG032572, R03AG043052, and R01 AG030153). Collection of these data was made possible by the US Agency for International Development (USAID) under the terms of cooperative agreement GPO-A-00-08-000_D3-00. The opinions expressed are those of the authors and do not necessarily refl ect the views of USAID or the US Government. Data for this research were provided by MEASURE Evaluation, funded by the USAID. Views expressed do not necessarily refl ect those of USAID, the US Government, or MEASURE Evaluation. The Palestinian Central Bureau of Statistics granted the researchers access to relevant data in accordance with licence number SLN2014-3-170, after subjecting data to processing aiming to preserve the confi dentiality of individual data in accordance with the General Statistics Law—2000. The researchers are solely responsible for the conclusions and inferences drawn upon available data. We thank the Russia Longitudinal Monitoring Survey, RLMS-HSE, conducted by the National Research University Higher School of Economics and ZAO “Demoscope” together with Carolina Population Center, University of North Carolina at Chapel Hill and the Institute of Sociology RAS for making these data available. This research used data from the National Health Survey 2009–10, and we gratefully acknowledge the Ministry of Health, Survey copyright owner, for use of the database. All results of the study are those of the authors and in no way committed to the ministry. The following individuals acknowledge various forms of institutional support: Amanda G Thrift is supported by a fellowship from the Australian National Health and Medical Research Council (GNT1042600). Panniyammakal Jeemon is supported by the Wellcome Trust–DBT India Alliance, Clinical and Public Health, Intermediate Fellowship (2015–20). Boris Bikbov, Giuseppe Remuzzi, and Norberto Perico acknowledge that their contribution to this paper has been on behalf of the International Society of Nephrology (ISN) as a follow-up of the activities of the GBD 2010 Genitourinary Diseases Expert Group. Tonatiuh Barrientos-Gutierrez and E Filipa de Castro acknowledge that the data shared on Water and Sanitation for Mexico, was derived from the “Encuesta Nacional de Niños, Niñas y Mujeres en México 2015”, which is the implementation in Mexico of the Multiple Indicators Cluster Survey (MICS) carried out with the fi nancial support of UNICEF. Miriam Levi would like to acknowledge the
institutional support received from CeRIMP, Regional Centre for Occupational Diseases and Injuries, Tuscany Region, Florence, Italy. Charles Wolfe’s research was funded/supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. No individuals acknowledged receiving additional compensation for their eff orts.
References1 UN. Transforming our world: the 2030 Agenda for Sustainable
Development. New York: United Nations, 2015. https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed Sept 14, 2015).
2 IAEG-SDGs. Report of the Inter-Agency and Expert Group on the Sustainable Development Goal Indicators. New York, NY: Economic and Social Council, 2016. http://unstats.un.org/unsd/statcom/47th-session/documents/2016-2-SDGs-Rev1-E.pdf (accessed July 15, 2016).
3 Nilsson M, Griggs D, Visbeck M. Policy: map the interactions between Sustainable Development Goals. Nature 2016; 534: 320–22.
4 International Council for Science, International Social Science Council. Review of targets for the Sustainable Development Goals: the science perspective. Paris: International Council for Science, 2015.
5 Horton R. Offl ine: Why the Sustainable Development Goals will fail. Lancet 2014; 383: 2196.
6 Yamey G, Shretta R, Binka FN. The 2030 sustainable development goal for health. BMJ 2014; 349: g5295.
7 Hák T, Janoušková S, Moldan B. Sustainable Development Goals: a need for relevant indicators. Ecol Indic 2016; 60: 565–73.
8 Hickel J. The problem with saving the world. Jacobin (New York), Aug 8, 2015. https://www.jacobinmag.com/2015/08/global-poverty-climate-change-sdgs/ (accessed July 16, 2016).
9 The 169 commandments. The Economist (New York), March 28, 2015. http://www.economist.com/news/leaders/21647286-proposed-sustainable-development-goals-would-be-worse-useless-169-commandments (accessed July 16, 2016).
10 Unsustainable goals. The Economist (New York), March 26, 2015. http://www.economist.com/news/international/21647307-2015-will-be-big-year-global-governance-perhaps-too-big-unsustainable-goals (accessed July 16, 2016).
11 The good, the bad and the hideous. The Economist (New York), March 26, 2015. http://www.economist.com/news/international/21647316-which-mdgs-did-some-good-and-which-sdgs-might-work-good-bad-and-hideous (accessed July 16, 2016).
12 “Transforming our World by 2030” Some thoughts on the post 2015 zero draft. Permanent Observer. June 3, 2015. http://blogs.shu.edu/unstudies/2015/06/03/transforming-our-world-by-2030-some-thoughts-on-the-post-2015-zero-draft/ (accessed July 16, 2016).
13 Muchhala B, Sengupta M. A critique of the emerging post-2015 agenda. New Delhi: Centre for Development and Human Rights, 2015. http://www.cdhr.org.in/post-2015-agenda/ a-critique-of-the-emerging-post-2015-agenda (accessed July 16, 2016).
14 Tsai AC, Tomlinson M. Inequitable and ineff ective: exclusion of mental health from the post-2015 development agenda. PLoS Med 2015; 12: e1001846.
15 Izutsu T, Tsutsumi A, Minas H, Thornicroft G, Patel V, Ito A. Mental health and wellbeing in the Sustainable Development Goals. Lancet Psychiatry 2015; 2: 1052–54.
16 Gureje O, Thornicroft G. Health equity and mental health in post-2015 sustainable development goals. Lancet Psychiatry 2015; 2: 12–14.
17 Sachs J, Schmidt-Traub G, Kroll C, Durand-Delacre D, Teksoz K. SDG Index and dashboards—a global report. New York: Bertelsmann Stiftung and Sustainable Development Solutions Network (SDSN), 2016.
18 WHO. World health statistics: monitoring health for the SDGs. Geneva: World Health Organization, 2016.
19 Lim SS, Stein DB, Charrow A, Murray CJL. Tracking progress towards universal childhood immunisation and the impact of global initiatives: a systematic analysis of three-dose diphtheria, tetanus, and pertussis immunisation coverage. Lancet 2008; 372: 2031–46.
For HBSC principal investigators see http://www.hbsc.org
Articles
www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2 37
20 Hogan MC, Foreman KJ, Naghavi M, et al. Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium Development Goal 5. Lancet 2010; 375: 1609–23.
21 Horton R. Maternal mortality: surprise, hope, and urgent action. Lancet 2010; 375: 1581–82.
22 Murray CJL, Lopez AD, Wibulpolprasert S. Monitoring global health: time for new solutions. BMJ 2004; 329: 1096–100.
23 Friedman E. An independent review and accountability mechanism for the Sustainable Development Goals: the possibilities of a framework convention on global health. Rochester, NY: Social Science Research Network, 2016. http://papers.ssrn.com/abstract=2726226 (accessed July 16, 2016).
24 International Organizations Clinic, NYU School of Law, UNDP. Follow-up and review of the Sustainable Development Goals under the high level political forum. New York, NY: New York University School of Law, United Nations Development Programme, 2016.
25 Horton R. Offl ine: the “chronic pandemic” that just won’t go away. Lancet 2015; 385: 758.
26 UN Department of Economic and Social Aff airs. Transitioning from the MDGs to the SDGs: accountability for the post-2015 era. New York, NY: United Nations, 2015.
27 Lozano R, Wang H, Foreman KJ, et al. Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet 2011; 378: 1139–65.
28 Wang H, Liddell CA, Coates MM, et al. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014; 384: 957–79.
29 Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014; 384: 980–1004.
30 Murray CJL, Ortblad KF, Guinovart C, et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014; 384: 1005–70.
31 Bhatt S, Weiss DJ, Cameron E, et al. The eff ect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015; 526: 207–11.
32 Bhutta ZA, Chopra M, Axelson H, et al. Countdown to 2015 decade report (2000–10): taking stock of maternal, newborn, and child survival. Lancet 2010; 375: 2032–44.
33 Murray CJ, Frenk J, Piot P, Mundel T. GBD 2.0: a continuously updated global resource. Lancet 2013; 382: 9–11.
34 GBD Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause and cause-specifi c mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (in press).
35 GBD 2015 Child Mortality Collaborators. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (in press).
36 GBD 2015 Maternal Mortality Collaborators. Maternal mortality 1990 to 2015: a systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors 2015 Study. Lancet (in press).
37 GBD 2015 Diseases and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries during 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (in press).
38 GBD 2015 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2015: a systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors 2015 Study. Lancet (in press).
39 GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 195 countries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (in press).
40 Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014; 384: 766–81.
41 Stevens GA, Alkema L, Black RE, et al. Guidelines for Accurate and Transparent Health Estimates Reporting: the GATHER statement. Lancet 2016; published online June 28. http://dx.doi.org/10.1016/S0140-6736(16)30388-9.
42 Stevens GA, Alkema L, Black RE, et al. Guidelines for Accurate and Transparent Health Estimates Reporting: the GATHER statement. PLoS Med 2016; 13: e1002056.
43 Human Development Index (HDI). UN Development Programme Human Development Reports. http://hdr.undp.org/en/content/human-development-index-hdi (accessed July 16, 2016).
44 GBD 2015 HIV Collaborators. Estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2015: the Global Burden of Disease Study 2015. Lancet HIV 2016; 3: e361–87.
45 Bhatt S, Weiss DJ, Mappin B, et al. Coverage and system effi ciencies of insecticide-treated nets in Africa from 2000 to 2017. eLife 2015; 4: e09672.
46 Newby G, Bennett A, Larson E, et al. The path to eradication: a progress report on the malaria-eliminating countries. Lancet 2016; 387: 1775–84.
47 Asante AD, Price J, Hayen A, et al. Assessment of equity in healthcare fi nancing in Fiji and Timor-Leste: a study protocol. BMJ Open 2014; 4: e006806.
48 World Bank. The World Bank’s projects in Timor-Leste: the political economy of eff ective aid. Washington, DC: World Bank, 2015.
49 Ly C, Lee Y-K, Hou X. Timor-Leste—health equity and fi nancial protection report. Washington, DC: World Bank, 2016.
50 Ministry of Health of Timor-Leste. Basic services package for primary health care and hospitals: achieving the MDGs by improved service delivery. Dili, Timor-Leste: Ministry of Health, 2007.
51 Ministry of Health, Republic of Tajikistan. National President Program of health sector reforms in the Republic of Tajikistan 2000–2010. Dushanbe, Tajikistan: Ministry of Health, 1999.
52 Khodjamurodov G, Rechel B. Tajikistan: Health system review. Copenhagen, Denmark: European Observatory on Health Systems and Policies, 2010
53 Matthys B, Sherkanov T, Karimov SS, et al. History of malaria control in Tajikistan and rapid malaria appraisal in an agro-ecological setting. Malar J 2008; 7: 217.
54 WHO/EURO. Joint statement on cross-border cooperation on malaria in Tajikistan and Afghanistan. Kurgan Tube: World Health Organization Regional Offi ce for Europe, 2010
55 Restrepo J, Spagat M. Civilian casualties in the Colombian confl ict: a new approach to human security. London: Royal Holloway College, University of London, 2004. http://personal.rhul.ac.uk/uhte/014/HS%20in%20Colombia%20Civil%20Confl ict.pdf (accessed Aug 12, 2016).
56 Giedion U, Uribe MV. Colombia’s universal health insurance system. Health Aff (Millwood) 2009; 28: 853–63.
57 Farmer P, Frenk J, Knaul FM, et al. Expansion of cancer care and control in countries of low and middle income: a call to action. Lancet 2010; 376: 1186–93.
58 Wu T-Y, Majeed A, Kuo KN. An overview of the healthcare system in Taiwan. Lond J Prim Care 2010; 3: 115–19.
59 International Association of Traffi c and Safety Sciences. Changes in traffi c safety policies and regulations in 7 countries (1950–2010). Tokyo, Japan: International Association of Traffi c and Safety Sciences, 2012.
60 Iceland: a pioneer’s saga. Tob Control 2007; 16: 364.61 Sigurgeirsdóttir S, Waagfjörð J, Maresso A. Iceland: health system
review. Health Syst Transit 2014; 16: 1–182.62 Horton R. Offl ine: Let’s celebrate rhetoric-based development.
Lancet 2015; 386: 1324.63 WHO International Agency for Research on Cancer.
IARC monographs on the evaluation of carcinogenic risks to humans: volume 89. smokeless tobacco and some tobacco-specifi c N-nitrosamines. Lyon, France: WHO International Agency for Research on Cancer, 2007.
64 Gakidou E, Mallinger L, Abbott-Klafter J, et al. Management of diabetes and associated cardiovascular risk factors in seven countries: a comparison of data from national health examination surveys. Bull World Health Organ 2011; 89: 172–83.

Articles
38 www.thelancet.com Published online September 21, 2016 http://dx.doi.org/10.1016/S0140-6736(16)31467-2
65 Farzadfar F, Murray CJ, Gakidou E, et al. Eff ectiveness of diabetes and hypertension management by rural primary health-care workers (Behvarz workers) in Iran: a nationally representative observational study. Lancet 2012; 379: 47–54.
66 Gakidou E, Nordhagen S, Obermeyer Z. Coverage of cervical cancer screening in 57 countries: low average levels and large inequalities. PLoS Med 2008; 5: e132.
67 Gabert R, Thomson B, Gakidou E, Roth G. Identifying high-risk neighborhoods using electronic medical records: a population-based approach for targeting diabetes prevention and treatment interventions. PLoS One 2016; 11: e0159227.
68 Ng M, Fullman N, Dieleman JL, Flaxman AD, Murray CJL, Lim SS. Eff ective coverage: a metric for monitoring universal health coverage. PLoS Med 2014; 11: e1001730.
69 WHO, World Bank. Monitoring progress towards universal health coverage at country and global levels: framework, measures and targets. Geneva, Switzerland, and Washington, DC: World Health Organization and the World Bank, 2014.
70 Minas H, Tsutsumi A, Izutsu T, Goetzke K, Thornicroft G. Comprehensive SDG goal and targets for non-communicable diseases and mental health. Int J Ment Health Syst 2015; 9: 12.
71 Lloyd-Sherlock P, Ebrahim S, McKee M, Prince M. A premature mortality target for the SDG for health is ageist. Lancet 2015; 385: 2147–48.
72 Lloyd-Sherlock PG, Ebrahim S, McKee M, Prince MJ. Institutional ageism in global health policy. BMJ 2016; 354: i4514.