Embed Size (px)
Citation preview

962 Japanese Journal of Lung Cancer―Vol 56, Supplement, Dec 1, 2016―www.haigan.gr.jp
講演 6
新しい肺癌分類谷田部恭1
はじめに
肺癌の罹患率は依然として高い水準にあり,多くのがんの中でも死亡率の高い腫瘍の一つに居座り続けている.それ故に,治療法に対する多くの臨床治験が試みられると同時に,治癒に継がる新規薬剤が開発されている.それに対応するかのごとく,腫瘍であるかどうかの判断のみならず,組織型など病理診断医による診断がなくては治療方針が決定できないまでになっている.その理由として,現在の標準治療に組み入れられているベバシズマブとペメトレキセドが,それぞれ重篤な副作用および有効性の点で,腺癌が対象になっているためである.また,近年承認された免疫チェックポイント阻害剤であるニボルマブでは,その治療効果に扁平上皮癌と腺癌では差があることから,両者を区別して考える必要がある.この組織型による治療戦略決定はすでに確立されたエビデンスになっており,治療方針を決定するのに重要な因子となっている.そこで,ここでは 2015 年に改定された新しい肺癌分類1について,前分類との違いに焦点を当て,概説する.2015 年 4 月にWHOによる肺癌・胸腺・胸膜腫瘍・
心臓腫瘍についての分類が変更された.この分類は第 4版にあたるが,以前の紫がかった青の表紙を有していたことからブルーブックと称されることも多い.第 3版は新旧 2つのバージョンがあるが,2,3 これまでの変遷をTable 2 にまとめた.第 4版では 2011 年に提唱されたIASLC/ATS/ERS 肺腺癌分類4をもとにし,それに対応するように他の組織型も改変された.それぞれの組織型ごとに解説を進めたい.
腺 癌
1.上皮内腺癌の定義の確立
これまで肺腺癌における上皮内癌の定義は明瞭ではな
かった.第 3版では preinvasive lesion として扁平上皮内癌の他,異型腺腫様過形成(AAH)を挙げているが,細気管支肺胞上皮癌は腺癌の上皮内癌であると文章のみに記載していた.3 2015 分類では,上皮内癌の定義を定め(Table 2),明示的に preinvasive lesion として記載した(Table 1).これに伴って「細気管支肺胞上皮癌」という用語を使わないことにしている.これは後述する浸潤性粘液腺癌もこの疾患に含まれるとする歴史的背景があり,大きな混乱を生じたためである.2.微少浸潤腺癌の概念の導入
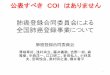
乳癌をはじめとする多くの癌腫では微少浸潤癌の概念が確立されており,肺腺癌においても放射線画像との対比や予後の点において明らかな浸潤癌とは異なることが明らかになった.これは本邦の野口分類に基づく研究成果が大きく貢献した.5 微少浸潤癌の定義についてはTable 3 にまとめ,典型的な微少浸潤腺癌をFigure 1 に示した.3.優位型による亜型分類
これまでの腺癌の組織亜型として,乳頭型,腺胞型,充実型,混合型にわけられていたが,肺腺癌は多様性の高い癌腫の 1つであり,その大多数(>90%)は混合型に分類されていた.6 そこで,その特徴を最もよく表すであろう優位組織型で分類を行うことにした.この組織亜型については,新たに微小乳頭状型(micropapillary)および肺胞置換性(lepidic)増殖型が加わった.微小浸潤型は,肺腺癌のみならず多くの癌腫で高い侵襲性との関連が指摘されている.7
4.充実性腺癌の定義変更
充実性腺癌の定義はこれまで粘液染色によりなされていた.すなわち,すべてが充実型腺癌の形態を取っていた場合,少なくとも 2高視野で 5細胞以上の粘液染色陽性細胞がないと大細胞癌に分類することになっていた.新分類では,粘液染色もしくは免疫組織学的に腺癌と確
1愛知県がんセンター遺伝子病理診断部. 論文責任者:谷田部恭.
(肺癌.2016;56:962-968) � 2016 The Japan Lung Cancer Society

Update for the NewWHO Classification of the Lung―Yatabe
Japanese Journal of Lung Cancer―Vol 56, Supplement, Dec 1, 2016―www.haigan.gr.jp 963
Table 1. The 2015 WHO Classifications of Lung Cancer
Histological Types and Subtypes ICDO CodeEpithelial tumorsAdenocarcinoma 8140/3Lepidic adenocarcinomae 8250/3dAcinar adenocarcinoma 8551/3dPapillary adenocarcinoma 8260/3Micropapillary adenocarcinomae 8265/3Solid adenocarcinoma 8230/3Invasive mucinous adenocarcinomae 8253/3dMixed invasive mucinous andnonmucinous adenocarcinoma 8254/3d
Colloid adenocarcinoma 8480/3Fetal adenocarcinoma 8333/3Enteric adenocarcinomae 8144/3Minimally invasive adenocarcinomaeNonmucinous 8256/3dMucinous 8257/3d
Preinvasive lesionsAtypical adenomatous hyperplasia 8250/0dAdenocarcinoma in situe
Nonmucinous 8250/2dMucinous 8253/2d
Squamous cell carcinoma 8070/3Keratinizing squamous cell carcinomae 8071/3Nonkeratinizing squamous cell carcinomae 8072/3Basaloid squamous cell carcinomae 8083/3Preinvasive lesion
Squamous cell carcinoma in situ 8070/2Neuroendocrine tumorsSmall cell carcinoma 8041/3Combined small cell carcinoma 8045/3
Large cell neuroendocrine carcinoma 8013/3Combined large cell neuroendocrine carci-noma
8013/3
Carcinoid tumorsTypical carcinoid tumor 8240/3Atypical carcinoid tumor 8249/3
Preinvasive lesionDiffuse idiopathic pulmonary neuroendocrine cell hyperplasia
8040/0d
Large cell carcinoma 8012/3Adenosquamous carcinoma 8560/3Sarcomatoid carcinomasPleomorphic carcinoma 8022/3Spindle cell carcinoma 8032/3Giant cell carcinoma 8031/3Carcinosarcoma 8980/3Pulmonary blastoma 8972/3
Other and Unclassified carcinomasLymphoepithelioma-like carcinoma 8082/3NUT carcinomae 8023/3d
Salivary gland-type tumorsMucoepidermoid carcinoma 8430/3Adenoid cystic carcinoma 8200/3Epithelial-myoepithelial carcinoma 8562/3Pleomorphic adenoma 8940/0
Histological Types and Subtypes ICDO CodePapillomasSquamous cell papilloma 8052/0
Exophytic 8052/0Inverted 8053/0
Glandular papilloma 8260/0Mixed squamous and glandular papilloma 8560/0
AdenomasSclerosing pneumocytomae 8832/0Alveolar adenoma 8251/0Papillary adenoma 8260/0Mucinous cystadenoma 8470/0Mucous gland adenoma 8480/0
Mesenchymal tumorsPulmonary hamartoma 8992/0dChondroma 9220/0PEComatous tumorseLymphangioleiomyomatosis 9174/1PEComa, benigne 8714/0
Clear cell tumor 8005/0PEComa, malignante 8714/3
Congenital peribronchial myofibroblastic tumor Diffuse pulmonary
8827/1
lymphangiomatosisInflammatory myofibroblastic tumor 8825/1Epithelioid hemangioendothelioma 9133/3Pleuropulmonary blastoma 8973/3Synovial sarcoma 9040/3Pulmonary artery intimal sarcoma 9137/3Pulmonary myxoid sarcoma with EWSR1-CREB1 translocatione
8842/3d
Myoepithelial tumorseMyoepithelioma 8982/0Myoepithelial carcinoma 8982/3
Lymphohistiocytic tumorsExtranodal marginal zone lymphomas of mucosa-associated
9699/3
Lymphoid tissue (MALT lymphoma) Diffuse large cell lymphoma
9680/3
Lymphomatoid granulomatosis 9766/1Intravascular large B cell lymphomae 9712/3Pulmonary Langerhans cell histiocytosis 9751/1Erdheim-Chester disease 9750/1
Tumors of ectopic originGerm cell tumorsTeratoma, mature 9080/0Teratoma, immature 9080/1
Intrapulmonary thymoma 8580/3Melanoma 8270/3Meningioma, NOS 9530/0Metastatic tumors

Update for the NewWHO Classification of the Lung―Yatabe
964 Japanese Journal of Lung Cancer―Vol 56, Supplement, Dec 1, 2016―www.haigan.gr.jp
Table 2. The Definition of Adenocarcinoma in Situ
Diagnostic criteria
•Small tumor <_3 cm•Solitary adenocarcinoma•Pure lepidic growth•No stromal, vascular or pleural invasion• No pattern of invasive adenocarcinoma (such as acinar, papil-lary, micropapillary, solid, colloid, enteric, fetal or invasive mu-cinous adenocarcinoma).
•No spread through air spaces• Cell type mostly nonmucinous (type II pneumocytes or Clara cells), rarely may be mucinous (tall columnar cells with basal nuclei and abundant cytoplasmic mucin, sometimes resembling goblet cells).•Nuclear atypia is absent or inconspicuous• Septal widening with sclerosis/elastosis is common, particular-ly in nonmucinous adenocarcinoma in situ
Table 3. The Definition of Minimally Invasive Adenocar-cinoma
•Small tumor <_3 cm•Solitary adenocarcinoma•Predominantly lepidic growth• <_0.5 cm invasive component in greatest dimension in any one focus•Invasive component to be measured includes◦ Any histological subtype other than a lepidic pattern (such as acinar, papillary, micropapillary, solid, colloid, fetal or invasive mucinous adenocarcinoma)
◦Tumor cells infiltrating myofibroblastic stroma• The diagnosis of minimally invasive adenocarcinoma is exclud-ed if the tumor◦Invades lymphatics, blood vessels, air spaces or pleura◦Contains tumor necrosis,◦Spreads through air spaces• The cell type is mostly nonmucinous (type II pneumocytes or Clara cells), but may rarely be mucinous (tall columnar cells with basal nuclei and abundant cytoplasmic mucin, sometimes resembling goblet cells).
Figure 1. A representative figure of minimally invasive adenocarcinoma. This adenocarcinoma has two invasive foci (3 mm and 1 mm in size), thus the tumor was diag-nosed as minimally invasive adenocarcinoma with 3-mm invasion.
3mm
1mm
認できれば腺癌と考えるようになった(Figure 2).そのため,これまでの大細胞癌のおよそ 1/2~2/3 が新分類では充実性腺癌に分類されることになる.8
5.浸潤性粘液腺癌の独立
浸潤性粘液腺癌は,特異な臨床病理学的特徴を示し,KRAS遺伝子変異が 75%以上で見出されることから独立した腺癌として扱うようになった.その特徴をTable4 に示す.肺炎様の陰影や大量の粘液性喀痰の他,細胞生物学的にも発現マーカーが異なり,KRAS遺伝子変異が本邦においても高い頻度で見いだされる.形態学的には,豊富な粘液産生と高円柱上皮が肺胞性置換性増殖を背景に微小な浸潤巣を形成する(Figure 3).
扁平上皮癌
1.扁平上皮癌の定義の変更
新しい分類では生物学的な腫瘍の性格を重視する方針となったため,これまで細胞間橋もしくは角化を有する腫瘍という定義から,これらの組織学的特徴および免疫組織化学的に扁平上皮癌マーカー陽性の腫瘍までを含めることになった.そのため,充実性腺癌と同様に,充実性増殖を示し,扁平上皮癌マーカー陽性の腫瘍も非角化型扁平上皮癌と診断するようになった(Figure 4).このため,少なからずの大細胞癌もこれからは扁平上皮癌に分類されることになる.2.亜型分類の変更
旧分類では,乳頭型,淡明細胞型,小細胞型などの組織亜型が含まれていたが,これら細胞学的特徴を基にした亜型はすべて削除された.類基底細胞型は例外で,旧分類では大細胞癌にもその組織亜型は存在したが,扁平上皮癌の 1亜型であることが明らかとなり,扁平上皮癌の亜型として再編されることになった.
大細胞癌
1.大細胞癌の定義の変更
上記のごとく,生物学的特徴をもって分類するようになったため,これまで大細胞癌と診断されていた腫瘍の多くは腺癌もしくは扁平上皮癌に分類されるようになる.新分類での大細胞癌は,Table 5 に掲げる 3タイプのみとなった.
神経内分泌癌
カルチノイド腫瘍,神経内分泌大細胞癌,小細胞癌は神経内分泌性格を有する腫瘍であることが知られていた

Update for the NewWHO Classification of the Lung―Yatabe
Japanese Journal of Lung Cancer―Vol 56, Supplement, Dec 1, 2016―www.haigan.gr.jp 965
Table 4. The Clinicopathological Characteristics of Invasive Mucinous Adenocarcinoma
Invasive Mucinous ADC (Historical Mucinous BAC)
AIS/MIA/LPA (Historical Non-mucinous BAC)
Female 49/84 (58%) 101/140 (72%) Smoker 38/87 (45%) 75/165 (46%) Clinical symptoms Mucinous sputa Mostly asymptomaticRadiographic appearance Majority consolidation;
Air-bronchogramMajority ground-glass attenuation
Frequent multifocal & multi-lobar presentation
Cell type Mucin-filled, columnar and/or goblet
Type II pneumocyte and/or Clara cell
PhenotypeCK7 Mostly positive ( ~ 88%) Positive ( ~ 98%) CK20 Positive ( ~ 54%) Negative ( ~ 5%) TTF-1 Mostly negative ( ~ 17%) Positive ( ~ 67%) CDX2 Possible to be positive Negative
GenotypeKRAS Frequent ( ~ 76%) Some ( ~ 13%) EGFR Almost none ( ~ 3%) Frequent ( ~ 46%)
Figure 2. A representative figure of solid adenocarcinoma. The tumor shows no morphologi-cal differentiation, but the immunohistochemical findings (TTF-1-positive and p40-negative) suggest the biological features of adenocarcinoma. Under the previous classification, this tumor used to be diagnosed as large cell carcinoma.
TTF-1
p40

Update for the NewWHO Classification of the Lung―Yatabe
966 Japanese Journal of Lung Cancer―Vol 56, Supplement, Dec 1, 2016―www.haigan.gr.jp
Figure 3. A typical case of invasive mucinous adenocarcinoma. Distinct pneumonia-like infiltration (left) and pneumonia-like consolidation (middle) are the characteristic features of this type of adenocarcinoma. Histologi-cally, the tumor cells grow along the alveolar wall (lepidic growth) with invasive foci scattered in the lesion.
Figure 4. A representative figure of non-keratinizing squamous cell carcinoma. The tumor shows no morphological differentiation, but the immunohistochemical findings (TTF-1-negative and p40-positive) suggest the biological features of squamous cell carcinoma. Under the previ-ous classification, this tumor used to be diagnosed as large cell carcinoma.
TTF-1
p40

Update for the NewWHO Classification of the Lung―Yatabe
Japanese Journal of Lung Cancer―Vol 56, Supplement, Dec 1, 2016―www.haigan.gr.jp 967
Table 5. The Subtypes of Large Cell Carcinoma
Large cell carcinoma with no immunohistochemical features
Negative for lineage-specific markers and mucin
Large cell carcinoma with unclear immunohistochemical features
Unclear immunoprofiles (such as TTF-1+and p40+) and negative for mucin
Large cell carcinoma with no stains available
No immunohistochemical stains or mucin available
Table 6. The Terminology and Criteria for Adenocarcinoma, Squamous Cell Carcinoma, and NSCC NOS in Small Biopsies and Cytology in Comparison to the Terms in Resection Specimens
New Small Biopsy/Cytology Terminology Morphology/Staining 2015 WHO Classification of Resection Specimens
Adenocarcinoma (describe identifiable patterns present)
Morphologic adenocarcinoma pat-terns clearly present
Adenocarcinoma-predominant pattern: lepidic, acinar, papillary, solid, and micropapillary
Adenocarcinoma with lepidic pattern (if pure, add note: an invasive component can-not be excluded)
Minimally invasive adenocarcinoma, adenocarci-noma in situ, or an invasive adenocarcinoma with a lepidic component
Invasive mucinous adenocarcinoma (describe patterns present; use term mucinous adenocarcinoma with lepidic pattern if pure lepidic pattern)
Invasive mucinous adenocarcinoma
Adenocarcinoma with colloid features Colloid adenocarcinomaAdenocarcinoma with fetal features Fetal adenocarcinomaAdenocarcinoma with enteric featuresb Enteric adenocarcinomaNSCC, favor adenocarcinomac Morphologic adenocarcinoma patterns
not present but supported by special staining (i.e., TTF-1 positive)
Adenocarcinoma (solid pattern may be just one component of the tumor)
Squamous cell carcinoma Morphologic squamous cell patterns clearly present
Squamous cell carcinoma
NSCC, favor squamous cell carcinomac Morphologic squamous cell patterns not present but supported by staining (i.e., p40-positive)
Squamous cell carcinoma (nonkeratinizing pattern may be a component of the tumor)
NSCC NOS No clear adenocarcinoma, squamous or neuroendocrine morphology or staining
Large cell carcinoma
Table 7. The Diagnostic Terminology for Small Biopsy/Cytology in Comparison to the 2015 WHO Terms in Resected Small Cell Carcinoma, LCNEC, Adenosquamous Carcinoma, and Sarcomatoid Carcinoma Specimens
Small Biopsy/Cytology Termlnology/Criteria 2015 WHO Classification of Resection SpecimensSmall cell carcinoma Small cell carcinomaNSCC with NE morphology and positive NE markers, possible LCNEC NSCC with NE morphology. If negative NE markers comment: This is an NSCC where LCNEC is suspected, but stains failed to demonstrate NE differentiation.
LCNEC Large cell carcinoma with NE morphology (LCNEM)
Morphologic squamous cell and adenocarcinoma patterns pres-ent: NSCC, NOS (comment that adenocarcinoma and squamous components are present and this could represent adenosquamous carcinoma). Morphologic squamous cell or adenocarcinoma patterns not present but immunostaining favors separate glandu-lar and adenocarcinoma components: NSCC, NOS (specify the results of immunohistochemical staining and interpretation and comment that this could represent adenosquamous carcinoma).
Adenosquamous carcinoma (if both components ≥10%) Adenocarcinoma, squamous cell carcinoma, adenosquamous carci-noma or large cell carcinoma with unclear immunohistochemical features
NSCC with spindle cell and/or giant cell carcinoma (mention if adenocarcinoma or squamous carcinoma are present)
Pleomorphic, spindle cell, and/or giant cell carcinoma
が,旧分類では神経内分泌大細胞癌は大細胞癌の亜型とされていた.新分類ではこれらの腫瘍をまとめて,神経
内分泌癌として統一した.これは多くの臓器,特に膵を含む消化管では統一した分類となっており,neuroendo-crine tumor(NET)Grade 1 から NET Grade 3 とすることが一般に受け入れられている.しかしながら,肺ではカルチノイド腫瘍,小細胞癌ともに確立した概念であり,標準的な臨床的対応がこの分類をもとにしていることや,典型的カルチノイド=NET grade 1,異型カルチノイド=NET grade 2,小細胞癌および神経内分泌癌=NETgrade 3 と対応が明瞭で,単なる用語の置き換えをする利益は少ないと考えられるからである.9 また,カルチノイド腫瘍と小細胞癌および神経内分泌癌との間には大き

Update for the NewWHO Classification of the Lung―Yatabe
968 Japanese Journal of Lung Cancer―Vol 56, Supplement, Dec 1, 2016―www.haigan.gr.jp
な隔たりがあり,中間形が多い消化管とは異なることもその要因として挙げることができる.
その他
1.生検・細胞診での用語統一
これまでWHO分類はすべて切除組織に対する分類であった.しかしながら,肺癌患者のおよそ 2/3 は進行肺癌として発症し,治療としては薬物治療,放射線治療が対象となることから,生検・細胞診での分類は重要と考えられる.そこで,新分類では用語を統一し,実臨床で混乱のない分類を提唱している(Table 6,7).そのほか,生検診断・細胞診のための良い診療ガイドラインなどについても言及されている.10
2.新しい疾患の導入
2004 年以降,新たに独立した疾患と同定されたNutcarcinoma,pulmonary myxoid sarcoma や,生物学的特性が明らかになったために名称が変更された sclerosingpneumocytoma,PEComa などが挙げられる.これらについての詳細は他の文献を当たられたい.11
終わりに
紙面の関係もあり,概要しか記載できなかったが,新しいWHO分類にそった新しい取扱規約も発刊される予定であり,また詳細はその他の雑誌10,11においても特集が組まれているので興味がある方はそれらを参照されたい.
本論文内容に関連する著者の利益相反:なし
REFERENCES
1.Travis WD, Brambilla E, Burke A, Marx A, NicholsonAG. WHO Classification of Thumours of the lung, pleura, thy-
mus and heart. Lyon: IARC; 2015.2.Travis WD, Colby TV, Corrin B, Shimosato Y, Brambilla
E. HIstological typing of lung and pleural tumours. Berlin :Springer; 1999.
3.Travis WD, Brambilla E, Müller-Hermelink HK, HarrisCC. Pathology and Genetics. Tumours of the Lung, Pleura,
Thymus and Heart. Lyon: IARC Press; 2004.4.Travis WD, Brambilla E, Noguchi M, Nicholson AG,Geisinger KR, Yatabe Y, et al. International associationfor the study of lung cancer/american thoracic society/european respiratory society international multidiscipli-nary classification of lung adenocarcinoma. J Thorac On-
col. 2011;6:244-285.5.Travis WD, Garg K, Franklin WA, Wistuba II, Sabloff B,Noguchi M, et al. Evolving concepts in the pathology andcomputed tomography imaging of lung adenocarcinomaand bronchioloalveolar carcinoma. J Clin Oncol. 2005;23:3279-3287.
6.Motoi N, Szoke J, Riely GJ, Seshan VE, Kris MG, RuschVW, et al. Lung adenocarcinoma : modification of the2004 WHO mixed subtype to include the major his-tologic subtype suggests correlations between papillaryand micropapillary adenocarcinoma subtypes, EGFRmutations and gene expression analysis. Am J Surg Pathol.
2008;32:810-827.7.Amin MB, Tamboli P, Merchant SH, Ordóñez NG, Ro J,Ayala AG, et al. Micropapillary component in lung ade-nocarcinoma: a distinctive histologic feature with possi-ble prognostic significance. Am J Surg Pathol. 2002;26:358-364.
8.Rekhtman N, Tafe LJ, Chaft JE, Wang L, Arcila ME,Colanta A, et al. Distinct profile of driver mutations andclinical features in immunomarker-defined subsets ofpulmonary large-cell carcinoma. Mod Pathol. 2013;26:511-522.
9.Caplin ME, Baudin E, Ferolla P, Filosso P, Garcia-YusteM, Lim E, et al. Pulmonary neuroendocrine (carcinoid)tumors : European Neuroendocrine Tumor Society ex-pert consensus and recommendations for best practicefor typical and atypical pulmonary carcinoids. Ann Oncol.
2015;26:1604-1620.10.谷田部恭,野口雅之.肺癌 I.病理と臨床.2016:34.11.谷田部恭,野口雅之.肺癌 II.病理と臨床.2016:34.