Embed Size (px)
Citation preview
嬰兒室之感染管制
中華民國防疫學會
王任賢 理事長
Normal Newborn Care
Advances in Maternal and Neonatal Health

Session Objective• Define essential elements of early
newborn care• Discuss best practices and technologies
for promoting newborn health• Use relevant data and information to
develop appropriate essential newborn recommendations

9.4
11.9 12.310.8 10.1
7.6
0
4
8
12
1981 1991 2001 2003 2007 2010
Preterm Births United States
Percent
Healthy People Objective
March of Dimes Objective
27 percent increase from 1981 to 2001

Newborn Deaths
• 8.1 million infant deaths (1993)
• 3.9 million (48%) newborn deaths
• 2.8 million (67%) early newborn deaths
• Major causes of newborn deaths– Birth asphyxia: 21%– Infections: 42% (tetanus,
sepsis, meningitis, pneumonia, diarrhea)

Newborn Deaths (continued)• Birth process was the antecedent cause of
2/3 of deaths due to infections– Lack of hygiene at childbirth and during newborn
period– Home deliveries without skilled birth attendants
• Birth asphyxia in developing countries– 3% of newborns suffer mild to moderate birth
asphyxia– Prompt resuscitation is often not initiated or
procedure is inadequate or incorrect

Newborn Deaths (continued)• Hypothermia and newborn deaths
– Significant contribution to deaths in low birth weight infants and preterm newborns
– Social, cultural and health practices delaying care to the newborn
• Countries with high STD prevalence and inconsistent prophylactic practices– Ophthalmia neonatorum is a common cause of
blindness

Newborn Deaths (continued)• Low birth weight
– An extremely important factor in newborn mortality• Place of childbirth
– At least 2 out 3 childbirths in developing countries occur at home
– Only half are attended by skilled birth attendants– Strategies for improving newborn health should
target• Birth attendant, families and communities• Healthcare providers within the formal health system
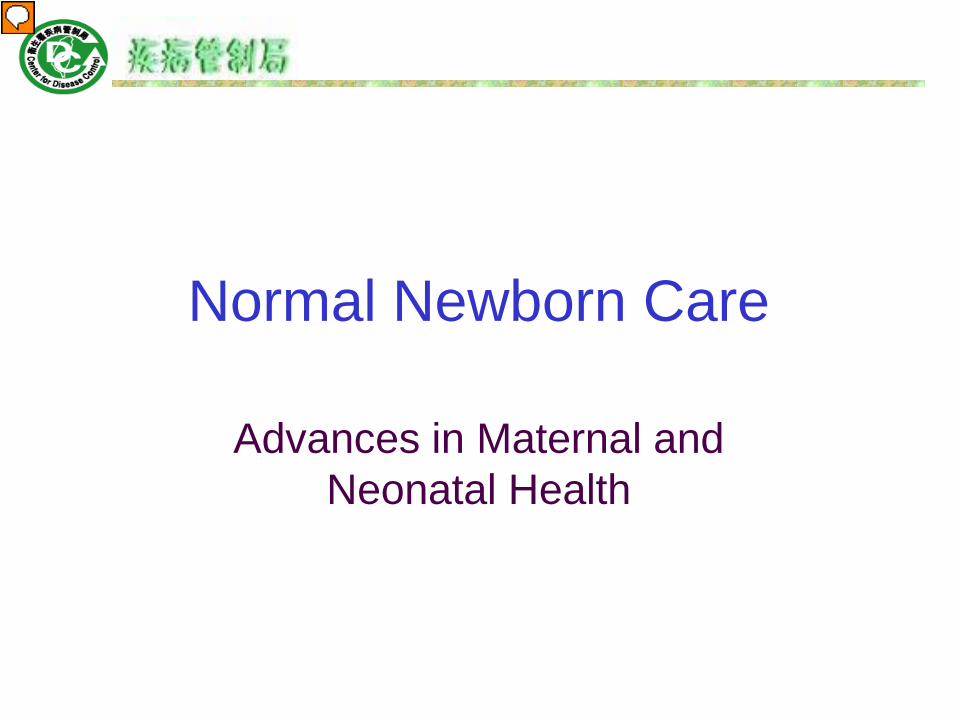
Characteristics of Neonatal Sepsis
Early Onset<7 days
Late Onset ≥ 7 days to 3 months
Late, Late Onset>3 months
Intrapartum complications
Often present Usually absent Varies
Transmission Vertical; organisms often acquired from mother’s genital tract
Vertical or via postnatal environment
Usually postnatal environment
Clinical manifestations
Fulminant course, multisystem involvement, pneumonia
Insidious, focal infection, meningitis common
Insidious
Case-fatality rate
5 percent to 20 percent 5 percent LowM.S. Edwards, 2002a. Reprinted with permission.
Prevention of Nosocomial Infections in NICUs
• Increased compliance with hand-hygiene standards
• Improved accuracy of the diagnosis of bacteremia
• Reduced line and line connection (hub) bacterial contamination

• Maximal barrier precautions for central line placement
• Decreased – Number of skin punctures– Duration of IV lipid infusion– Duration of central venous line use
Prevention of Nosocomial Infections in NICUs

Essential Newborn Care Interventions
• Clean childbirth and cord care– Prevent newborn infection
• Thermal protection– Prevent and manage newborn hypo/hyperthermia
• Early and exclusive breastfeeding– Started within 1 hour after childbirth
• Initiation of breathing and resuscitation– Early asphyxia identification and management

Essential Newborn Care Interventions (continued)
• Eye care– Prevent and manage ophthalmia neonatorum
• Immunization– At birth: bacille Calmette-Guerin (BCG) vaccine, oral
poliovirus vaccine (OPV) and hepatitis B virus (HBV) vaccine (WHO)
• Identification and management of sick newborn• Care of preterm and/or low birth weight newborn

Standard Operating Procedure
• Patients• Waste• Sharps• Equipment• Environment• Parents• Health care workers

Standard Operating Procedure
• Patients– Closed incubators– Minimal movement
• Waste– Infectious– Non infectious

Standard Operating Procedure
• Sharps
• Equipment– No sharing– Labelling of
incubators
• Environment– Clean (+) rooms last
– Separate equipment
– New cloths daily
– Soap & water – damp dusting surfaces & floors
– Wipe surfaces 95% ethyl alcohol

Standard Operating Procedure• Parents
– Hand washing & spray
– Masks– Reporting loose
stools– Their baby only– Pamphlets– Limit visitors
• Health Care Workers– Limit staff exposure– Limit students– Hand washing &
spray– PPE per procedure

Personal Protective EquipmentProcedure Mask Gloves Apron
Nappy change √ √ √
NG feeds √ √
Medication √ √
Insert IV √ √
Draw blood √ √
Hold baby √ √ √
Examine baby √ √
Do dressing √ √
Wash baby √ √ √

Assessment of Ward Ventilation – smoke test
1. No proper mechanical ventilation in rooms. Some air outlets closed.
2. Circulation of air b/w the incubators - ↑ likelihood of aerosol transmission of the rotavirus.
3. Smoke particles remained suspended in far corners of the rooms, ↑ the risk of aerosol transmission in these areas.
4. There was no real movement of air from the rooms into the passages.

General Hygiene and Care• Skin care
– Bathing• Oral hygiene, prevent thrush• Hair care• Feeding• Hyperthermia with antipyretics• Analgesics, stool softeners, antiemetics• Antibiotics

Cleanliness to Prevent Infection
• Principles of cleanliness essential in both home and health facilities childbirths
• Principles of cleanliness at childbirth– Clean hands– Clean perineum– Nothing unclean introduced vaginally– Clean delivery surface– Cleanliness in cord clamping and cutting– Cleanliness for cord care
• Infection prevention/control measures at healthcare facilities

Umbilical Cord• Apply alcohol with each diaper change
• Fold diaper below cord
• Will fall off in 10-14 days
• Do not give full bath until it falls off

Circumcision• Is done at 24 hours of age
• Cleanse with soap & water, apply petroleum jelly
• Plastibell ring will fall off 5-8 days

Bathing• Sponge bath 3 times/wk• Tub bath when cord and circumcision heal• Wash face and genitals daily with plain
water• Use mild soap on genitals if needed• Avoid baby wipes with alcohol or perfume

Thermal Protection• Newborn physiology
– Normal temperature: 36.5–37.5°C– Hypothermia: < 36.5°C– Stabilization period: 1st 6–12 hours after birth
• Large surface area• Poor thermal insulation• Small body mass to produce and conserve heat• Inability to change posture or adjust clothing to respond to
thermal stress
• Increase hypothermia– Newborn left wet while waiting for delivery of placenta– Early bathing of newborn (within 24 hours)

Hypothermia Prevention• Deliver in a warm room• Dry newborn thoroughly and wrap in dry, warm cloth• Keep out of draft and place on a warm surface• Give to mother as soon as possible
– Skin-to-skin contact first few hours after childbirth– Promotes bonding– Enables early breastfeeding
• Check warmth by feeling newborn’s feet every 15 minutes
• Bathe when temperature is stable (after 24 hours)

Breastfeeding• Benefits to baby
– Protects against allergies
– Easily digested– Decreases diaper
rash– Encourages bonding– Decrease diarrhea or
constipation
• Benefits to mother – Convenient– Promotes weight
loss– Less expensive– Promotes bonding

Bottle Feeding Basics• NEVER MICROWAVE! – use warm water to warm
formula• Hold your baby for every feeding• Keep baby’s head higher than their body• Brush baby’s lips lightly with bottle nipple• Place nipple gently in baby’s mouth• Keep milk in the nipple by tilting the bottle down
towards the baby• NEVER PROP A BOTTLE, YOUR BABY MAY
CHOKE!
Bottle Feeding• Supplies needed:
– 8 (4 ounce) baby bottles and caps– 8 nipples– Bottle and nipple brush for cleaning– 1 quart measuring cup
• Formula– Wait until you see what type of formula your baby
likes before buying a lot• Plan on around 70 ounces of formula to start

Early and Exclusive Breastfeeding• Early contact between mother and newborn
– Enables breastfeeding– Rooming-in policies in health facilities prevents
nosocomial infection• Best practices
– No prelacteal feeds or other supplement– Giving first breastfeed within one hour of birth– Correct positioning to enable good attachment of
the newborn– Breastfeeding on demand– Psycho-social support to breastfeeding mother

Breathing Initiation and Resuscitation• Spontaneous breathing (> 30 breaths/min.) in most
newborns– Gentle stimulation, if at all
• Effectiveness of routine oro-nasal suctioning is unknown– Biologically plausible advantages – clear airway– Potentially real disadvantages – cardiac arrhythmia– Bulb suctioning preferred
• Newborn resuscitation may be needed– Fetal distress– Thick meconium staining– Vaginal breech deliveries– Preterm

Diaper Care• Cloth vs. Disposable
– Cloth diapers, diaper service, disposable
• Diaper rash– Dermatitis vs. Yeast
• Cleansing– Wipe front to back– Avoid wipes as they may irritate skin– Use warm water to wash skin– Use ointment as needed
Well Baby Check Up• Regularly scheduled visits
– Physical exam– Interview
• Immunizations are scheduled at these visits– Ask for advice on caring for immunization
site
Stools• Meconium – the first stool
– Sticky, greenish-black
• Normal – yellow-green seedy, mustard-like, soft stool
• Diarrhea stools > 3 times/hour, watery with no consistency
• Constipation – infrequent, hard, pellet-like
Safety• Use good handwashing
– Protect your baby from infection
• Shaken baby syndrome– Never handle your baby roughly
• Second hand smoke – Limit exposure

Eye Care To Prevent or Manage Ophthalmia Neonatorum
• Ophthalmia neonatorum– Conjunctivitis with discharge during first 2 weeks of life– Appears usually 2–5 days after birth– Corneal damage if untreated – Systemic progression if not managed
• Etiology– N. gonorrhea
• More severe and rapid development of complications• 30–50% mother-newborn transmission rate
– C. trachomatis

Eye Care To Prevent or Manage Ophthalmia Neonatorum (continued)• Prophylaxis
– Clean eyes immediately– 1% Silver nitrate solution
• Not effective for chlamydia– 2.5% Povidone-iodine solution– 1% Tetracycline ointment
• Not effective vs. some N. gonorrhea strains
• Common causes of prophylaxis failure– Giving prophylaxis after first hour– Flushing of eyes after silver nitrate application– Using old prophylactic solutions

Efficacy of Prophylaxis for Conjunctivitis in China
• Objective: To assess etiology of newborn conjunctivitis and evaluate the efficacy of regimens in China
• Design: November 1989 to October 1991 rotated regimens monthly: tetracycline, erythromycin, silver nitrate
• 302 (6.7%) infants developed conjunctivitis, most S. aureus (26.2%) and chlamydia (22.5%)
• Silver nitrate, tetracycline: fewer cases than no prophylaxis (p < 0.05), erythromycin: not significant

Prophylaxis for Conjunctivitis: Objective and Design
• Objective: To compare efficacy in prevention of nongonococcal conjunctivitis
• Design: Randomized control trial to compare erythromycin, silver nitrate, no prophylaxis– Examined with test for leukocyte esterase and
chlamydia trachomatis antibody probe 30–48 hours postpartum, 13–15 days later, and telephone contact up to 60 days of life
• Main outcome measured: conjunctivitis within 60 days of life and nasolacrimal duct patency

Prophylaxis for Conjunctivitis: Results and Conclusion
• Results: 630 infants• 109 with conjunctivitis
– Silver nitrate vs. no prophylaxis: Hazard ratio 0.61 (0.39-0.97)
• Chemical conjunctivitis with silver nitrate resolves within 48 hours
– Erythromycin vs. no prophylaxis: Hazard ratio 0.69 (not significant)
• Conclusion: Parental choice of prophylaxis, including no prophylaxis, is reasonable IF antenatal care and STD screening

Povidone-Iodine for Conjunctivitis: Objective and Design
• Objective: To determine incidence and type of conjunctivitis after povidone-iodine in Kenya
• Design: Rotate regimen weekly: erythromycin, silver nitrate, povidone iodine
• Results: – Conjunctivitis:
• Chlamydia in 50.5%• S. aureus in 39.7%
– More infections in silver nitrate than povidone-iodine, OR 1.76, p < 0.001
– More infections in erythromycin OR 1.38, p=0.001

Povidone-Iodine for Conjunctivitis: Conclusion
Povidone-iodine:– Is good prophylaxis– Has wider antibacterial spectrum– Causes greater reduction in colony-forming units
and number of bacterial species– Is active against viruses– Is inexpensive

Immunization
• BCG vaccinations in all population at high risk of tuberculosis infection
• Single dose of OPV at birth or in the two weeks after birth
• HBV vaccination as soon as possible where perinatal infections are common

Intrapartum prophylaxis not indicated
• Previous pregnancy with positive GBS screening culture (unless a culture was also positive during the current pregnancy)
• Planned cesarean delivery performed in the absence of labor or membrane rupture (regardless of maternal GBS culture status)
• Negative vaginal and rectal GBS screening culture in late gestation during the current pregnancy, regardless of intrapartum risk factors
Intrapartum Antibiotic Prophylaxis to Prevent Perinatal GBS
Intrapartum prophylaxis indicated• Previous infant with invasive GBS
disease• GBS bacteriuria during current
pregnancy• Positive GBS screening culture during
current pregnancy (unless a planned cesarean delivery, in the absence of labor or amniotic membrane rupture, is performed)
• Unknown GBS status (culture not done, incomplete or results unknown) and any of the following:
– Delivery at <37 weeks gestation– Amniotic membrane rupture ≥18 hours– Intrapartum temperature ≥100.4°F
(≥38.0°C)†
Vaginal and rectal GBS screening cultures at 35 to 37 weeks gestation for all pregnant women (unless patient had GBS bacteriuria during the current pregnancy or a previous infant with invasive GBS disease).

GBS Prophylaxis for Women with Threatened Preterm Delivery

Prevention of Early-Onset GBS Disease in the Newborn

SummaryThe essential components of normal newborn
care include:• Clean delivery and cord care• Thermal protection• Early and exclusive breastfeeding• Monitoring• Eye care• Immunization

懇請賜教