Embed Size (px)
Citation preview
Kor J Oral Maxillofac Pathol 2012;36(4):243-250
하악 전방부에 발생한 거대 중심성 골화성 섬유종
문성용1)*, 김수관1), 김학균2), 윤정훈3)**
조선대학교 치과대학 구강악안면외과학교실1), 충남대학교 의과대학 치과학교실 구강악안면외과2)
원광대학교 치과대학 대전치과병원 구강병리과3)
<Abstract>
Huge Central Ossifying Fibroma on the Anterior Mandible
: A Case Report
Seong Yong Moon1)*, Su Gwan Kim1), Hak Kyun Kim2), Jung Hoon Yoon3)**
Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University Dental Hospital1),
Department of Oral and Maxillofacial Surgery, School of Medicine, Chungnam National University Hospital2),
Department of Oral & Maxillofacial Pathology, College of Dentistry, Daejeon Dental Hospital, Wonkwang University3)
The ossifying fibroma (OF), with the microscopic features of trabuclae or spherules of bone or cementum-like material in a cellular
fibrous connective tissue stroma, is one of the most common benign fibro-osseous lesions in the jaw bones. The OF often occurs in
patients from 20 to 40 years of age, which is a definite female predilection. The mandibles are involved far more often than the
maxillas, especially the pre-molar and molar regions. It is slow-growing, bone producing, asymptomatic and well-demarcated. The OF
is a disorder of odontogenesis or osteogenesis ascribed to bone marrow stroma cells (BMSCs) abnormality. However, the detailed
mechanisms of OF’s oncogenesis, cytodifferentiation, and tumor progression remain unknown. In this article, we reported a huge cen-
tral OF on the anterior mandible. The lesion was enucleated and peripheral ostectomy was done via intraoral approach and re-
constructed with vascularized iliac block bone graft. After 25 months of follow up, the tumor had not recurred. This case shows that
OF may be successfully treated by conservative surgical enucleation and peripheral ostectomy.
Key words:Ossifying fibroma, Mandible, Surgical enucleation
*Correspondence: Seong-Yong Moon, Department of Oral and Maxillofacial Surgery, Chosun University Dental Hospital, Philmoondaero 303, Seo-seok Dong, Dong-gu, Gwang-Ju, 501-759, South Korea. Tel: 82-62-220-3810, E-mail: [email protected]
** Correspondence: Jung-Hoon Yoon, Department of Oral and Maxillofacial Pathology, Wonkwang University Daejeon Dental Hospital, Doonsan-Ro 77.Tel: 82-42-366-1146, E-mail: [email protected]
본 연구는 2012년 조선대학교 치과병원 연구비 지원으로 이루어진 것임.
Received: Jun 13, 2012; Revised: Jun 18, 2012; Accepted: Jun 27, 2012
Ⅰ. Introduction
Ossifying fibroma (OF) is a relatively rare benign neo-
plasm of the jaws, composed of connective tissue of mixed
and variable cellularity, with a mineralized component that
consists of trabecular or woven bone1). OF is one of the be-
nign fibro-osseous lesions included in a heterogeneous
group of bone disorders affecting the craniofacial bones2).
OF was first described by Menzel in 1872 and the term
‘ossifying fibroma’ was subsequently coined by Montgomery
in 19273). This lesion was then thought to be a histological
variant of fibrous dysplasia, but it was later separated into
a distinct clinico-pathological entity.
The OF and cementifying fibroma have been grouped
under a single designation as cemento-ossifying fibroma in
the 1992 World Health Organization (WHO) classification4).

244
The tumor is defined as a demarcated, occasionally
encapsulated lesion consisting of fibrous tissue that contains
variable amounts of mineralized material resembling bone or
cementum4,5). It shows a female predilection, and most cases
are seen at the third and fourth decades of life. The
premolar and molar region of the mandible is the most
common site1). Most cases of active OF are asymptomatic,
as is reflected in the present case, and the first clinical
manifestation is a swelling of the mandibular cortical layer,
which produces a marked extra-oral facial asymmetry6). The
essential characteristics of this clinical entity are as follows:
the early age of onset, the bone pattern, the high tendency
to recurrence and the aggressive local behavior. Sometimes,
these tumors may reach a very large size7). Such cases may
require additional reconstructive surgery because of some
aesthetic and functional problems, especially when teeth are
removed8,9).
Radiographically, The lesions most often are well defined
and unilocular, and are either completely radiolucent or
mixed, depending on the amount of calcification, or are
completely radiopaque and surrounded by a radiolucent rim.
In each type, there is a sclerotic border around the lesion.
Multilocularity is rare. Root divergence and resorption are
not uncommon10)
.
The treatment of choice is always surgery. Small lesions
are treated with conservative excision and the circumscribed
nature of the lesion permits complete local enucleation or
curettage. Whereas larger lesions that have destroyed a
considerable amount of bone, especially those in the
maxilla, may show a more aggressive pattern and require
radical surgery as segmental resection11). Mandibular lesions
have a recurrence rate of 28% after curettage1). To avoid or
minimize the chance of recurrence, en bloc resection or
partial resection of the jaw is generally preferred1,8,12,13).
In this report, aggressive large ossifying fibroma on the
mandible shows that OF could be diagnosed by combination
of clinical and radiologic and histopathologic examination.
And OF cloud be treated by surgical enucleation and
peripheral ostectomy successfully, and immediate
reconstruction was performed.
Ⅱ. Case report
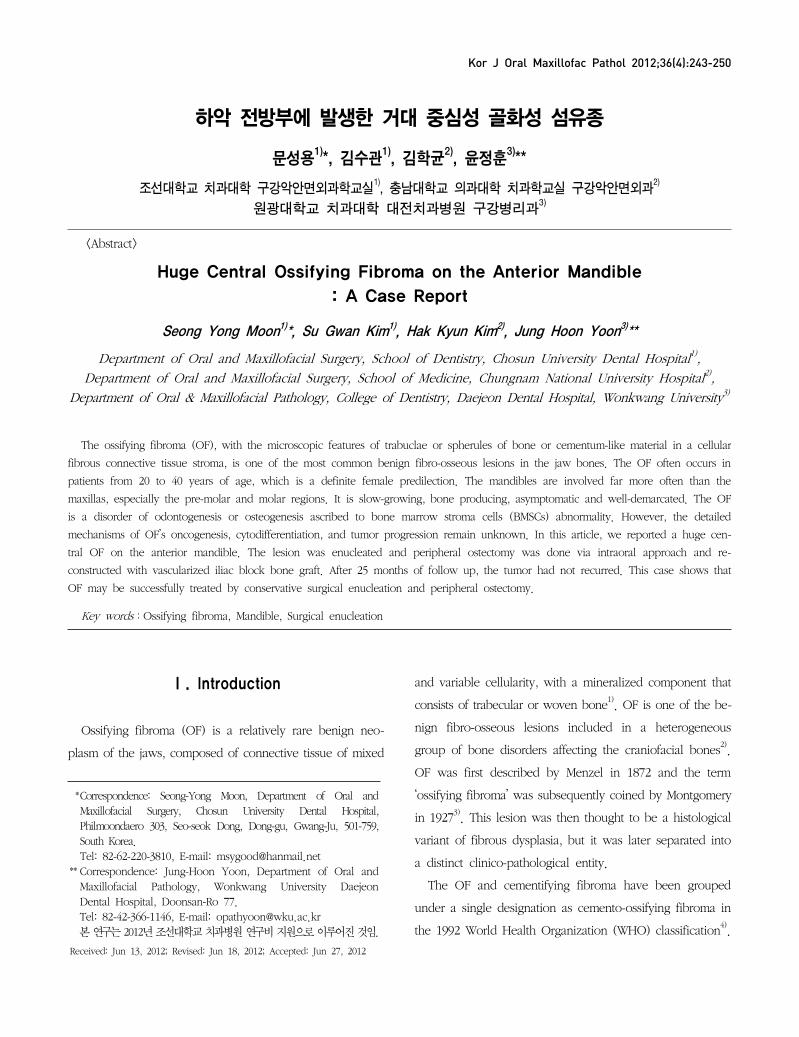
A 38-year-old woman taken the panorama in local clinic
and she referred to our department because of facial
swelling on the anterior mandibular area. In panoramic and
CT view, she had radiolucent-radiopaque mixed lesion
surrounded by radiolucent rim from #36 to #45 area, and
loss of lamina dura of from #33 to #43 teeth, and expansion
and thinning of buccal and lingual cortical bone (Fig 1). The
CT findings favor an OF (Fig 2). The patient was not aware
of its presence until an examination. The surrounding soft
tissue did not show any pathologic appearance.
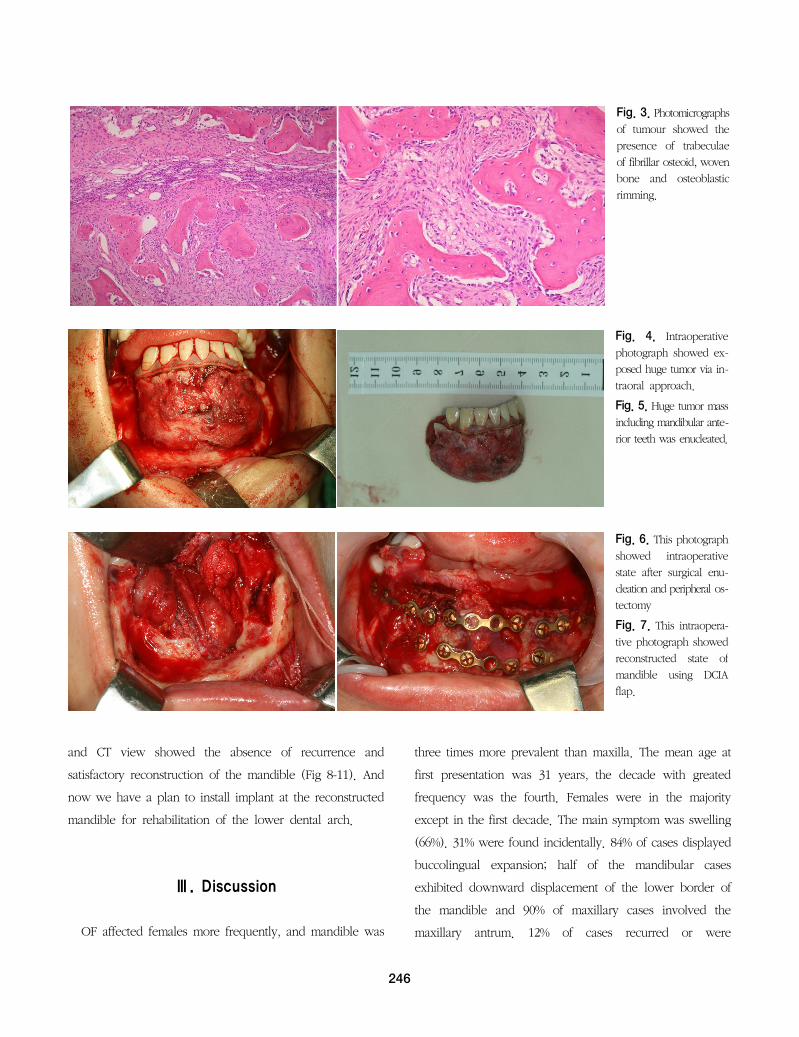
The lesion was biopsied by sulcular and vertical releasing
incision on the mandibular symphyseal area; the results of
which showed an OF, that showed bony trabeculae with
osteoblastic rimming and fascicular proliferation of spindle
cell (Fig 3). In September 4th, 2008, under general
anesthesia, a subperiosteal surgical enucleation was
performed and peripheral ostectomy about 1 mm at the all
enucleated area with piezosurgery (Fig 4-6). The immediate
reconstruction was performed with a deep circumflex iliac
arterial osseous iliac crestal flap harvested from the left ilium
and positioned through intraoral approach (Fig 7). A small
incision of the skin at the left submandibular area for
exposing the facial vessel used for the anastomosis.
The subsequent histologic examination showed the lesion
to be characterized by a dense cellular proliferation of
polyhedral and spindle-shaped cells arranged in a whorled
pattern in which trabuculae of primary bone with occasional
osteoblastic rims and granules of cells of the osteclastic type
were also present. The overall picture led to the diagnosis
of an OF. 1 year and 2 year after the surgery, panoramic
245
Fig. 1. An initial lesion
of the panoramic radio-
graph.
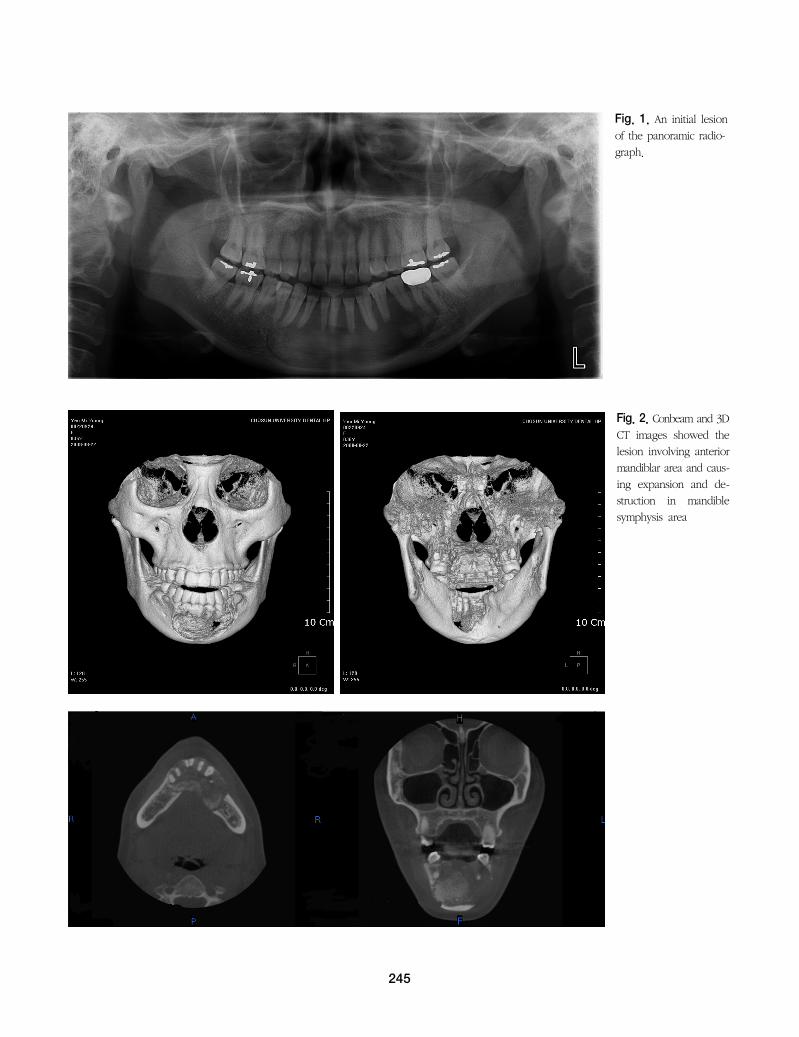
Fig. 2. Conbeam and 3D
CT images showed the
lesion involving anterior
mandiblar area and caus-
ing expansion and de-
struction in mandible
symphysis area
246
Fig. 3. Photomicrographs
of tumour showed the
presence of trabeculae
of fibrillar osteoid, woven
bone and osteoblastic
rimming.
Fig. 4. Intraoperative
photograph showed ex-
posed huge tumor via in-
traoral approach.
Fig. 5. Huge tumor mass
including mandibular ante-
rior teeth was enucleated.
Fig. 6. This photograph
showed intraoperative
state after surgical enu-
cleation and peripheral os-
tectomy
Fig. 7. This intraopera-
tive photograph showed
reconstructed state of
mandible using DCIA
flap.
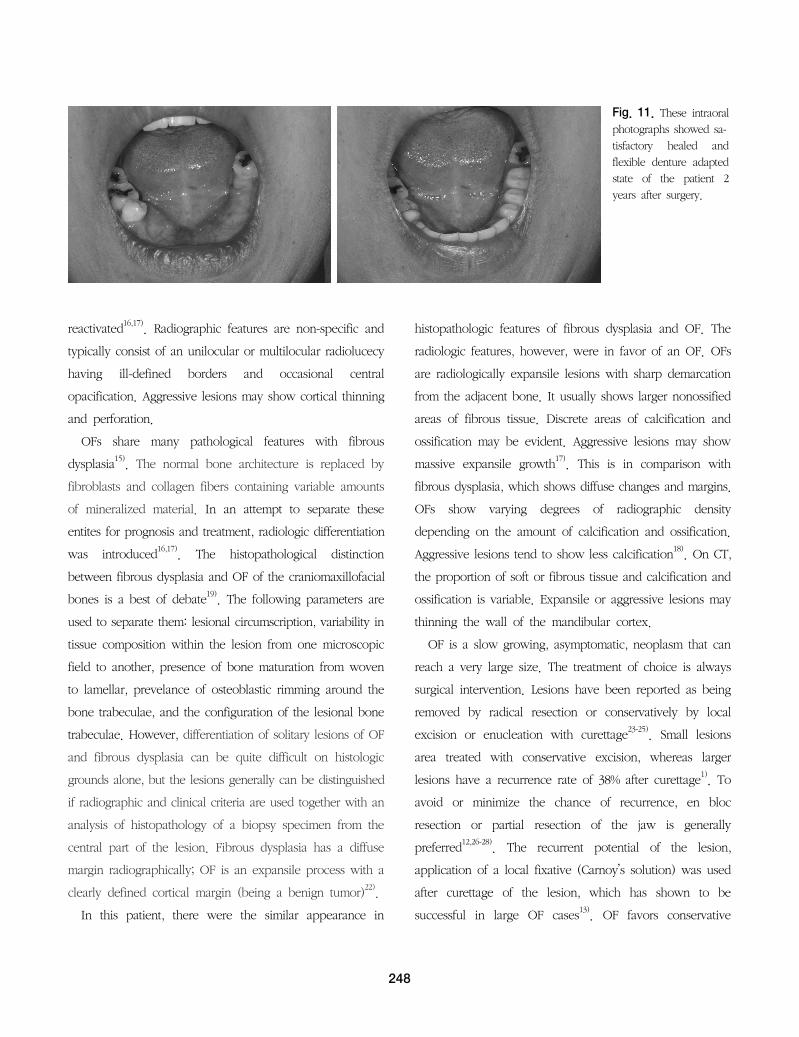
and CT view showed the absence of recurrence and
satisfactory reconstruction of the mandible (Fig 8-11). And
now we have a plan to install implant at the reconstructed
mandible for rehabilitation of the lower dental arch.
Ⅲ. Discussion
OF affected females more frequently, and mandible was
three times more prevalent than maxilla. The mean age at
first presentation was 31 years, the decade with greated
frequency was the fourth. Females were in the majority
except in the first decade. The main symptom was swelling
(66%). 31% were found incidentally. 84% of cases displayed
buccolingual expansion; half of the mandibular cases
exhibited downward displacement of the lower border of
the mandible and 90% of maxillary cases involved the
maxillary antrum. 12% of cases recurred or were

247
Fig. 8. This is panoramaic radiograph of 1 year after surgery.
There was no evidence of recurrence.
Fig. 9. This is panoramaic radiograph of 2 year after surgery.
There was no evidence of recurrence.
Fig. 10. These con-
ebeam and 3D CT images
showed reconstructed
mandible with DCIA flap
2 years after surgery.
248
Fig. 11. These intraoral
photographs showed sa-
tisfactory healed and
flexible denture adapted
state of the patient 2
years after surgery.
reactivated16,17). Radiographic features are non-specific and
typically consist of an unilocular or multilocular radiolucecy
having ill-defined borders and occasional central
opacification. Aggressive lesions may show cortical thinning
and perforation.
OFs share many pathological features with fibrous
dysplasia15). The normal bone architecture is replaced by
fibroblasts and collagen fibers containing variable amounts
of mineralized material. In an attempt to separate these
entites for prognosis and treatment, radiologic differentiation
was introduced16,17). The histopathological distinction
between fibrous dysplasia and OF of the craniomaxillofacial
bones is a best of debate19). The following parameters are
used to separate them: lesional circumscription, variability in
tissue composition within the lesion from one microscopic
field to another, presence of bone maturation from woven
to lamellar, prevelance of osteoblastic rimming around the
bone trabeculae, and the configuration of the lesional bone
trabeculae. However, differentiation of solitary lesions of OF
and fibrous dysplasia can be quite difficult on histologic
grounds alone, but the lesions generally can be distinguished
if radiographic and clinical criteria are used together with an
analysis of histopathology of a biopsy specimen from the
central part of the lesion. Fibrous dysplasia has a diffuse
margin radiographically; OF is an expansile process with a
clearly defined cortical margin (being a benign tumor)22).
In this patient, there were the similar appearance in
histopathologic features of fibrous dysplasia and OF. The
radiologic features, however, were in favor of an OF. OFs
are radiologically expansile lesions with sharp demarcation
from the adjacent bone. It usually shows larger nonossified
areas of fibrous tissue. Discrete areas of calcification and
ossification may be evident. Aggressive lesions may show
massive expansile growth17). This is in comparison with
fibrous dysplasia, which shows diffuse changes and margins.
OFs show varying degrees of radiographic density
depending on the amount of calcification and ossification.
Aggressive lesions tend to show less calcification18). On CT,
the proportion of soft or fibrous tissue and calcification and
ossification is variable. Expansile or aggressive lesions may
thinning the wall of the mandibular cortex.
OF is a slow growing, asymptomatic, neoplasm that can
reach a very large size. The treatment of choice is always
surgical intervention. Lesions have been reported as being
removed by radical resection or conservatively by local
excision or enucleation with curettage23-25). Small lesions
area treated with conservative excision, whereas larger
lesions have a recurrence rate of 38% after curettage1). To
avoid or minimize the chance of recurrence, en bloc
resection or partial resection of the jaw is generally
preferred12,26-28)
. The recurrent potential of the lesion,
application of a local fixative (Carnoy’s solution) was used
after curettage of the lesion, which has shown to be
successful in large OF cases13)
. OF favors conservative

249
surgery rather than en block resection in well demarcated
with radiolucent rim29). In these lesions are usually having
definite radiolucent rim, it means that it can be separated
easily from surrounding tissue and well encapsulated lesion.
In this case, the lesion was enucleated via intra-oral
approach with involved teeth, and peripheral ostectomy was
performed approximately 1 mm at entire surface of the
margin, and also shaped the rectangular form for
reconstruction with free vascularized iliac bone. The defect
was larger than 5cm, so free vascularized bone graft using
deep circumflex iliac arterial osseous flap (7*2 cm) was
performed immediately. The relationship between histologic
features and clinical behavior is not sufficiently30). We have
not been able to trace any documented report of a case of
aggressive OF transforming into osteosarcoma, a possibility
mentioned by Hoffman et al31).
Ⅳ. Conclusion
OF is a relatively rare benign neoplasm of the jaws,
composed of connective tissue of mixed and variable
cellularity with a mineralized component that consists of
trabecular or woven bone. The essential characteristics of
this clinical entity are as follows : the early age of onset, the
bone pattern, the high tendency to recurrence and the
aggressive local behavior. The diagnosis of OF is
radiologically expansile lesions with sharp demarcation from
the adjacent bone. Surgical excision is usually selected for
treatment to avoid recurrence, but peripheral ostectomy or
partial mandibulectomy of the jaw is sometimes preferred.
In this case, aggressive large OF on the anterior mandible
was treated by surgical enucleation and peripheral
ostectomy about 1mm using piezosurgery and simultaneous
reconstruction was done with iliac crestal osseous flap.
Successful result was obtained with no reccurrence during
2 years follow up. This study intend to report this case with
systemic reviews.
Ⅳ. Reference
1. Eversole LR, Leider AS, Nelson K: Ossifying fibroma: a
clinicopathologic study of sixty-four cases. Oral Surg Oral
Med Oral Pathol 1985;60:505-511.
2. Mintz S, Velez I: Central ossifying fibroma: an analysis of
20 cases and review of the literature. Qunitessence Int
2007;38:221-227.
3. Sciubba JJ, Younai F: Ossifying fibroma of the mandible
and maxilla: review of 18 cases. J Oral Pathol Med
1989;18:315-321.
4. Jones AC, Alderson G, McGuff HS: Oral and Maxillofacial
pathology cases of the month. Central ossifying fibroma.
Tex Dent J 2003;120:371-377.
5. Slootweg PJ: Lesions of the jaws. Histopathology
2009;54:401-418.
6. Brannon RB, Fowler CB: Benign fibro-osseous lesions: a
review of current concepts. Adv Anat Pathol
2001;8:126-143.
7. Montgomery AH: Ossifying fibroma of the jaw. Arch Surg
1927;15:30-44.
8. Krammer IRH, Pindborg JJ, Shear M: Histologic typing of
odontogenic tumors (ed2). New York, NY, Springer-
Verlag, World Health Organization, 1992;1927.
9. Waldron CA: Fibro-osseous lesions of the jaws. J Oral
Maxillofac Surg 1993;51:828.
10. Corrado Toro, Werner Millesi, Nicoletta Zerman,
Massimo Robiony, Massimo Politi: A case of aggressive
ossifying fibroma with massive involvement of the
mandible: Differential diagnosis and management
options. Int J Pediatric Otorhionolaryngol Extra 2006;
1:167-172.
11. Kristensen S, Tveteras K: Aggressive ossifying fibroma of
the maxilla. Arch Otorhinolaryngol 1986;243:102-105.
12. Kreutziger KL, Weiss LS: Ossifying fibroma: Resection of
recurrent mandibular lesion with microsurgical
250
preservation of inferior alveolar nerve and immediate
reconstruction. South Med J 1994;87:653-658.
13. M.Gurol, S.Uckan, N.Guler, PI Yatmax: Surgical and
reconstructive treatment of a large ossifying fibroma of
the mandible in a retrognathic patient. J Oral Maxillofac
Surg 2001;59:1097-1100.
14. MacDonald-Jankowski DS: Ossifying fibroma: a
systematic review. Dentomaxillofac Radiol 2009; 38:
495-513.
15. Montgomery AH: Ossifying fibroma of the jaw. Arch
Surg 1927;15:40-55.
16. Sherman RS, Waldermar CA: The roentgen apperace of
ossifying fibroma of bone. Radiology 1948;50:595-609.
17. Cook BDE: Benign fibro-osseous enlargement of the
jaws. Part I and II. Br Dent J 1957;102:1-14,49-59.
18. Sciubba JJ, Younai F: Ossifying fibroma of the mandible
and maxilla. Review of 18 cases. J Oral Pathol Med
1989;18:315-321.
19. Van heerden WFP, Raubenheimer EJ, Weier RG, et al:
Giant ossifying fibroma. A clinicopathologic study of 8
tumors. J Oral Pathol Med 1989;18:506-509.
20. Voytek TM, Ro JY, Edeiken J, et al: Fibrous dysplasia
and cement-ossifying fibroma. A histologic spectrum.
Am J Surg Pathol 1995;19:775-781.
21. Chong VF, Tan LH: Maxillary sinus ossifying fibroma.
Am J Otolaryngol 1997;18:419-424.
22. LR: Eversole Benign tumors of the oral cavity. M.S.
Greenberg, M. Glick (Eds.), Oral medicine diagnosis &
treatment (10th ed.), BC Decker Inc. 2003;152
23. Smith AG, Zavaleta A: Osteoma, ossifying fibroma, and
fibrous dysplasia of facial and cranial bones. AMA Arch
Pathol 1952;54:507-527.
24. Test D, Schow C, Cohen D, Tilson H: Juvenile ossifying
fibroma. J Oral Surg 1976;34:907-910.
25. Reaume CE, Schmid RW, Welsey RK: Aggressive
ossifying fibroma of the mandible. J Oral Surg 1985;
43:631-635.
26. Jacobs JB, Berg HM: Destructive cemento-ossifying
fibroma of the maxilla. Ear Nose Throat J 1990; 69:
805-808.
27. Wu PC, Leung PK, Ma KM: Recurrent cementifying
fibroma. J Oral Maxillofac Surg 1986;44:229-234.
28. Sweet RM, Bryarly RC, Kornblut AD, Corio RL.Recurrent
cementifying fibroma of the jaws. Laryngoscope
1981;91:1137-1144.
29. Toro C, Millesi W, Zerman N, et al: A case of aggressive
ossifying fibroma with massive involvement of the
mandible: Differential diagnosis and management
options. International Journal of Pediatric Otorhinol-
arhgology Extra 2006;1:167-172.
30. A Zupy, AM Ruggiero, L Insabato, et al: Aggressive
cement-ossifying fibroma of the jaws. Oral Oncol
2000;36:129-133.
31. Hoffman S, Jacoway JR, Krolls SO: Intraosseous and
periosteal rumors of the jwas. Atlas of Tumor
Pathology. 2nd series Washington: Armed Force
Institute of Pathology. 2nd series Washington: AFIP,
1987;208-211.


























